
Abstract
Background
Variability of finger tapping speeds, especially in the non-dominant hand, has been reported in individuals with amnestic mild cognitive impairment (MCI-A) and dementia of the Alzheimer's type (AD). An explanation of this finding, however, has not appeared.
Objective
The aim of this study was to investigate possible motor correlates of finger tapping variability in normal older healthy controls (HC), persons with subjective memory complaints (SMC), MCI-A and probable AD.
Methods
Using a modified version of the Halstead Finger Tapping Test (HFTT), individual finger tapping movements were classified as “valid” (i.e., advanced the number on a mechanical counter) or “invalid” (i.e., did not advance the number). Failures at selective motor inhibition and learning and fatigue effects were also measured.
Results
Finger tapping variability was significantly greater in the non-dominant hand in probable AD patients compared to HC and SMC patients. MCI-A and probable AD patients did not differ on this measure. Finger tapping variability was significantly correlated (ρ = + 0.65) with the number of invalid tapping responses but not with selective motor inhibition failures. A small but significant correlation of dominant hand learning effect with finger tapping variability was found. Invalid tapping responses were significantly greater in MCI and probable AD groups compared to HC and SMC groups.
Conclusions
Frequency of invalid tapping responses strongly correlated with finger tapping variability. The number of invalid tapping responses may have diagnostic and prognostic significance when evaluating older individuals with known or suspected memory impairment of a neurodegenerative type.
Keywords
Introduction
Traditionally, finger tapping has been considered “a basic sensorimotor measure largely independent of higher-order cognition.”1 Compatible with this view were early findings which reported no differences between persons with early stages of Alzheimer's disease (AD) and normal older controls when comparing mean speed of finger tapping scores on the traditional Halstead Finger Tapping Test (HFTT).2,3 Those findings reinforced the view that finger tapping performance was not clinically helpful when evaluating older individuals with memory impairments. Large scale studies that attempted to track neuropsychological performance in healthy older individuals as they age (e.g., Jonaitis et al.4) or to identify behavioral biomarkers of cognitive decline in persons suspected of having the beginnings of a dementing condition typically have not included measures of speed of finger tapping.5,6
More recent studies, however, have reported that the variability of finger tapping speeds is substantially greater in persons with amnestic mild cognitive impairment (MCI-A) and early AD compared to normal functioning older controls.7–13 This variability effect is most often observed in the non-dominant hand8 and is supported by both mechanical7 and computerized8,11 tapping assessments. It has also been reported that cognitively normal individuals with amyloid-β positivity (as measured by cerebrospinal fluid biomarkers) have greater intra-subject variability of tapping speeds.14 These findings appear especially robust given that the specific measures of finger tapping variability and techniques for recording finger tapping have varied. Suggested mechanisms for these findings have included loss of tactile sensation,15 disruption of inherent timing mechanisms,11 loss of central processing,9,16 and/or executive/attention dysfunction,12,17 as well as AD-related pathology.14 To date, no neuropsychological or motor explanation has appeared to definitively explain the finger tapping variability findings.
Kinematic recordings obtained while performing a modified version of the HFTT in healthy adults ranging in ages from 21 to 80 years18 revealed that finger tapping variability of “valid” tapping scores was significantly and positively correlated with the number of “invalid” tapping responses (r= + 0.50, p = 0.001). A valid tapping score was simply defined as an index finger tapping movement that advanced the number on a mechanical counter. An invalid response was defined as an index finger movement that did not advance the number on the mechanical counter when attempting to depress the tapping key and then release it. Visual inspection of finger movements associated with invalid responses frequently revealed small perseverative or repetitive movements that were not of sufficient finger extension and/or release to advance the number on the mechanical counter when a finger tapping response was attempted. Interestingly, time to initiate or stop the finger movement response did not correlate with finger tapping variability, nor did the age, educational level, or sex of the individual.
A subsequent study demonstrated that normal individuals in the 60–80 age range showed increased selective motor inhibition failures, particularly in the dominant hand, while performing the modified HFTT task.19 A selective motor inhibition failure was defined as the inability to keep the adjacent fingers (especially the middle finger) from lifting off the tapping board while performing the index finger tapping movement. The relationship of selective motor inhibition failures and finger tapping variability has not been reported.
In addition to the kinematic recordings, behavioral assessments of “learning” and “fatigue” effects were obtained in normal adults while performing the modified version of the HFTT.18 Learning effects (e.g., higher tapping scores with practice) were observed in both hands in healthy functioning individuals, with a greater amount of improved performance in the dominant hand. In contrast, fatigue effects (e.g., lower tapping scores after repetitive finger tapping performances) were observed primarily in the non-dominant hand. The relationship of these two measures to finger tapping variability was also not reported.
In the present study, we measured the mean valid index finger tapping scores, variability of valid finger tapping scores (i.e., the range of scores while performing the task), the frequency of invalid finger tapping movements, the frequency of selective motor inhibition failures, and learning and fatigue effects in normal healthy controls (HC), individuals with subjective memory complaints (SMC), MCI-A and probable AD. We predicted that finger-tapping variability would be greater in the two groups who objectively demonstrated memory impairments (i.e., MCI-A and probable AD) compared to the older individuals with SMC but no objective memory impairments and normal functioning individuals without SMC (i.e., HC). Based on our previous research findings18 with healthy older individuals, we also predicted that variability of valid finger tapping scores would positively and significantly correlate with the number of invalid tapping responses when compared across all four groups. We explored whether selective motor inhibition failures and learning and fatigue effects would correlate with finger tapping variability findings in older individuals with abnormal memory performance (i.e., MCI-A and probable AD). Finally, we predicted that the frequency of invalid tapping responses, using the modified HFTT, would be significantly greater in persons with MCI-A and probable AD compared to the HC and persons with SMC.
Methods
Subjects
The research participants for this investigation were recruited primarily from the clinical practice of the first author between the years 2019–2023. These were older individuals who were referred for a clinical neuropsychological examination because of concern over possible memory impairment by either the patient, family members or referring physician. Clinical neuropsychological testing was performed as a part of their clinical evaluation. The battery included the BNI Screen for Higher Cerebral Functions20 (BNIS), Wechsler Adult Intelligence Scale-IV Edition21 (WAIS-IV), Rey Auditory Verbal Learning Test22 (RAVLT), Brief Visual Memory Test-Revised Form23 (BVMT-R), Trail Making Test Parts A and B,24 and the modified HFTT.18 The battery was performed by a single clinical neuropsychologist (G.P.P., > 50 years of experience) as part of the clinical workflow. Based on a clinical consensus between the referring physician (A.B., > 20 years of experience as a geriatric psychiatrist) and clinical neuropsychologist (G.P.P., > 50 years of experience), three clinical groups were identified.
Participants were classified as SMC if they complained of memory impairment, but psychometric testing showed average levels of performance on a test of intellectual ability and two memory tests. More specifically, SMC participants had a score of at least 90 on the WAIS-IV Full-Scale Intelligence Quotient (FSIQ) and memory scores within 1.5 standard deviation (SD) of demographically-adjusted normative values on at least two measures of memory (from the WAIS-IV, RAVLT, and BVMT-R).
The classification of participants as MCI-A was informed by the Petersen 2004 criteria.25 The specific criteria used for MCI-A was memory scores at least 1.5 SD below demographically-adjusted normative values on two tests of memory while demonstrating a FSIQ score of at least 90. While some of these individuals showed mild difficulties on non-memory neuropsychological measures (defined as scores at least 1 SD below normative values in a non-memory cognitive domain), their primary difficulties were in the domain of memory functioning. This group was functioning independently in everyday life activities by their own report and the reports of family members.
A third group of individuals performed below normal limits on tests of memory and intellectual functioning (i.e., scores at least 1.5 SD below normative values and FSIQ less than 90) with additional clinically significant impairments in at least two other cognitive domains (e.g., impaired language and “executive” functions). This group was dependent on others to help them meet their daily needs. Their neuropsychological test performance was compatible with the mild to moderate stages of a dementing condition, most likely of the Alzheimer's type (AD) according to the criteria suggested by McKhann et al.26
In addition to these three clinical research groups, similar age- and education-matched healthy controls (HC) were recruited to participate in this study from ongoing research projects by the last author of this paper; more specifically, participants were recruited from local research databases (n = 5) and word-of-mouth referrals (n = 7). They consisted of older individuals who were primarily retired and who were functioning normally in everyday life via their reports.
Subject recruitment
Potential research participants were first identified by their performance when undergoing a clinical neuropsychological examination. If their neuropsychological test performance suggested one of the three clinical conditions noted above, the examining clinical neuropsychologist asked if they would be interested in participating in a research project investigating the relationship between finger tapping performance and memory function. If they expressed a potential willingness to participate, research nurses or other study personnel contacted them to explain the study in more detail and obtained informed consent once they understood the details of their potential participation. Informed consent was obtained according to the requirements of the Institutional Research Board (IRB) of St Joseph's Hospital and Medical Center and the Barrow Neurological Institute (BNI) in Phoenix, Arizona, USA.
Inclusion criteria were (1) that the person agreed to participate in the study and informed consent obtained, (2) was between the ages of 60–84, and (3) English was their primary language. Exclusion criteria were (1) after learning more about the study, the individual chose not to participate; (2) the individual's medical history was positive for a neurological or psychiatric condition that could potentially influence neuropsychological test performance (e.g., severe traumatic brain injury, brain tumor, cerebral vascular accident, multiple sclerosis, history of psychosis, history of drug addiction, etc.); (3) the person had a history of learning disability and (4) neuropsychological, neurological or any neuroimaging findings suggesting non-AD-related brain pathology (e.g., the presence of severe cerebral vascular disease (defined by the presence of infarcts or extensive white matter hyperintensity burden), Lewy body dementia, frontotemporal dementia, or parkinsonism).
Neuropsychological measures
All research participants (clinical and non-clinical) were administered the BNIS20 and the modified HFTT.18 The BNIS is a standardized test of higher integrative brain functions that samples both cognitive and non-cognitive abilities.27 The HFTT is a well-established neuropsychological measure of finger tapping speed.28 A modified version of the HFTT test was previously characterized and standardized,18 and this version of the HFTT was administered to each of the four research groups. Briefly, it employed the same mechanical counter (Veeder-Root counter, model # 0727235-001) originally used by Halstead.29 To avoid possible hand biasing effects, each counter was mounted on two separate boards. On one board, the lever (i.e., tapping key) was mounted on the left side of the counter when measuring left index finger movement movements. The tapping lever or key was mounted on the right side to measure right index finger movements.18 Each person was instructed to tap 10 s for three consecutive trials with their dominant hand followed by three consecutive trials of 10 s with their non-dominant hand. This was repeated with three additional trials with first the dominant hand and then the non-dominant hand. Then, one final trial with the dominant hand was performed followed by one final trial of the non-dominant hand. The original version of the HFTT involved obtaining five 10-s tapping scores within 5 taps of each other; this reduced the variability of scores but often resulted in a different number of trials for each hand. The modification to the HFTT18 was developed to capture potential variability of tapping scores in both hands, to ensure the same number of trials were obtained to measure tapping performances (i.e., seven trials) in both hands and to measure possible fatigue and learning effects.
Measures of finger tapping behaviors
After verbally instructing and physically demonstrating to the research participant how to perform the modified HFTT, the examiner administered the test and recorded the following: the number of valid taps (i.e., the number of taps in which the index finger movement produced the next number on the mechanical counter), the number of invalid taps (i.e., the number of up and down index finger movements that did not produce the next number appearing on the mechanical counter), the variability of number of valid tapping responses over the seven trials (i.e., the range score obtained by subtracting the highest score from the lowest score on the seven trials) and the number of selective motor inhibition failures (i.e., the number of times when any of the adjacent fingers next to the index finger lifted off the tapping board when the index finger movement was attempted (further details can be found in Prigatano et al.19). In addition, measures of learning and fatigue effects were calculated. Fatigue effects were assessed by subtracting the finger tapping score on Trial 6 from Trial 4. Learning effects were assessed by subtracting the finger tapping score on Trial 4 from Trial 1 (see Prigatano et al.19 for further details). The same finger tapping apparatus employed in our previous studies which included kinematic recordings was used, but no kinematic recorders were obtained in the present study. The present study was done in the United States and the finger tapping studies using kinematic recorders were done in Brazil where a motor detection laboratory using the VICOB movement analysis system was available.18
Finger tapping measures were obtained for both the dominant and non-dominant hand. Handedness was determined by the subjective report of the individual and the hand used to write their name. None of the research participants had difficulty following the instructions of the task nor did they report any unusual motor weaknesses. The Veeder-Root counter requires a force of 8 oz per inch, and the lever extends for approximately ¾ inch, resulting in an estimated force of 170 g per tap.
Statistical analyses
The analyses were conducted through a custom script developed in R (Version 3.3.3) and RStudio (Version 1.3.1093). The demographic characteristics of each of the four groups (i.e., age, education level, race, ethnicity, handedness and sex) were summarized and compared using analysis of variance (ANOVA), Fisher's Exact test, and chi square as appropriate to the variable studied. Small but statistically reliable differences in age were observed across groups, and therefore group comparisons using the BNI Screen and finger tapping measures were assessed using analysis of covariance (ANCOVA) with age held constant. When group differences (p < 0.05) were found, pairwise post-hoc analyses were conducted to determine specific group differences on the BNI Screen and the various finger tapping measures with Tukey HSD to correct for multiple comparisons. Spearman rank-order correlations were performed to further assess the relationship of invalid tapping responses with variability of valid finger tapping responses. The correlational analyses included all participants. The neuropsychological test scores obtained during clinical evaluations were scored according to age and educational based norms. ANOVA was used when testing for group differences on these measures. Effect sizes were calculated for all ANOVA, ANCOVA, and corresponding pairwise post-hoc comparisons. Eta squared (η2) and partial eta squared (η2p) were used to estimate the effect size for ANOVA and for ANCOVA, respectively. For post-hoc comparisons between groups, Hedge's g was used to estimate effect size.
Results
Demographic and psychometric testing findings
Sixty-five (65) research participants were enrolled in the study. Twelve (12) were healthy normal controls; 23 were SMC; 19 were MCI; and 11 were probable AD with mild to moderate dementia. The mean age for HC was 72.2 years and 70.3 years for SMC group. The mean age for MCI-A participants was 74.6 years and 75.3 years for the probable AD group. The SMC group was slightly, but significantly, younger than the other three groups (p = 0.05). The groups did not different in their mean level of education (p = 0.76), race (p = 0.93), ethnicity (p = 0.57), or sex distribution (p = 0.55). They also did not significantly differ in terms of handedness (p = 0.17). However, three of the 11 probable AD individuals were left-handed (27.3%; Table 1). Consequently, all analyses of finger movements compared dominant hand (DH) to non-dominant hand (NDH) instead of right versus left hand.
Demographic and psychometric test findings.
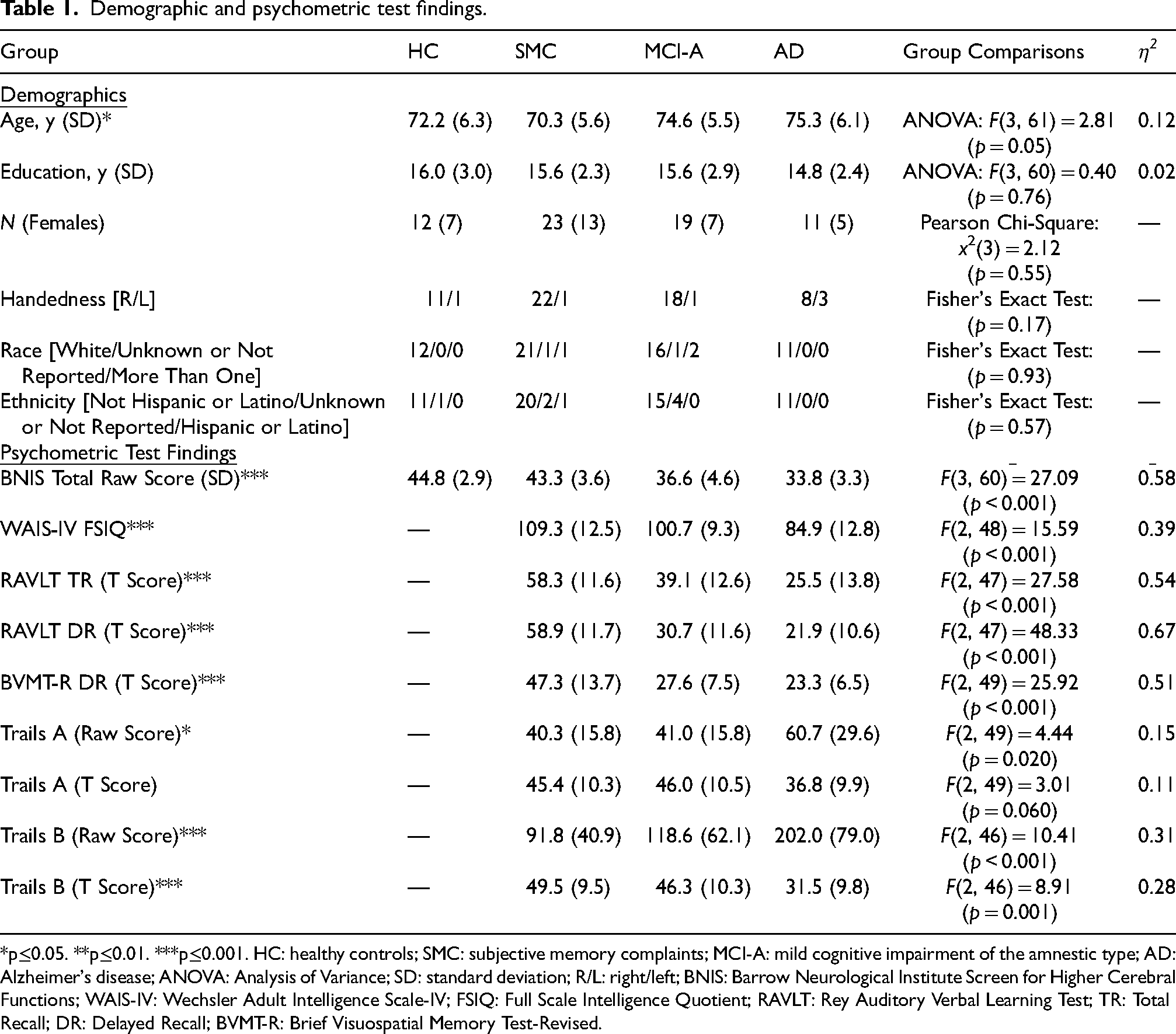
*p≤0.05. **p≤0.01. ***p≤0.001. HC: healthy controls; SMC: subjective memory complaints; MCI-A: mild cognitive impairment of the amnestic type; AD: Alzheimer's disease; ANOVA: Analysis of Variance; SD: standard deviation; R/L: right/left; BNIS: Barrow Neurological Institute Screen for Higher Cerebral Functions; WAIS-IV: Wechsler Adult Intelligence Scale-IV; FSIQ: Full Scale Intelligence Quotient; RAVLT: Rey Auditory Verbal Learning Test; TR: Total Recall; DR: Delayed Recall; BVMT-R: Brief Visuospatial Memory Test-Revised.
The BNIS mean total raw score was significantly different between groups (p < 0.001, η2 = 0.58). Normal HC and SMC groups did not differ on their BNIS total raw score, but the SMC group performed significantly higher than the MCI-A (p < 0.001, g = 1.62) and probable AD groups (p < 0.001, g = 2.64). The MCI-A and probable AD groups did not differ in their overall level of performance on this measure (p = 0.24, g = 0.64).
The three clinical groups significantly differed in terms of their FSIQ estimates (p < 0.001, η2 = 0.39), level of performance on each of the memory tests (p < 0.001, η2 > 0.51; Table 1) and a brief measure of “executive functions” (i.e., Trail Making Test Part B T-score: p < 0.001, η2 = 0.28; Table 1). The direction of these differences between groups was compatible with their clinical diagnosis, with the probable AD group performing at a lower level than the MCI-A and the MCI-A group performing lower than the SMC group on each of these psychometric measures.
Finger tapping findings: valid finger tapping scores and variability of finger tapping
Mean valid finger tapping scores were not different across groups in the DH (p = 0.08, η2p = 0.13) but were significantly different in the NDH (p = 0.002, η2p = 0.24). The major group differences found were that SMC patients and MCI-A patients had higher NDH scores than the probable AD patients (p < 0.001, g = 1.48 and p = 0.02, g = 0.96, respectively). The variability of finger tapping speeds (i.e., the range scores) was also not statistically different across groups in the DH (p = 0.09, η2p = 0.14) but was in the NDH (p = 0.02, η2p = 0.19) (Table 2). The major group differences were that HC and SMC research participants had smaller variability scores in the NDH compared to probable AD participants (p = 0.02, g = −1.13 and p = 0.04, g = −1.07, respectively). MCI-A patients had smaller variability (range scores) than probable AD participants (p = 0.04, g = −0.96) in the NDH.
Finger tapping findings across groups (ANCOVA analyses).
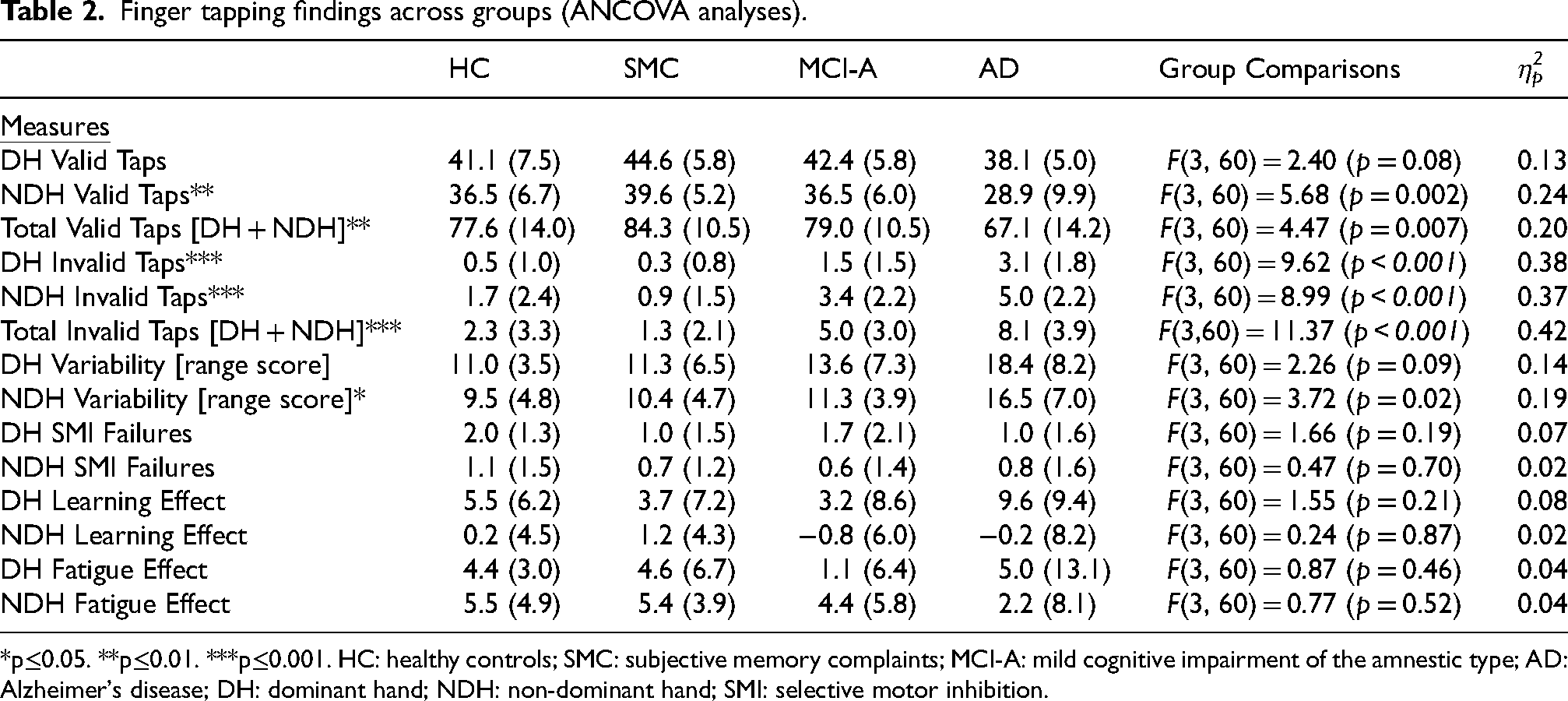
*p≤0.05. **p≤0.01. ***p≤0.001. HC: healthy controls; SMC: subjective memory complaints; MCI-A: mild cognitive impairment of the amnestic type; AD: Alzheimer's disease; DH: dominant hand; NDH: non-dominant hand; SMI: selective motor inhibition.
There were no reliable differences between groups in the number of selective motor inhibition failures, learning effects or fatigue effects for both the DH and the NDH (Table 2).
Finger tapping findings: invalid finger tapping responses and variability of finger tapping
Using age as a covariate, group differences were found for the number of invalid finger tapping responses in both the DH (p < 0.001, η2p = 0.38) and the NDH (p < 0.001, η2p = 0.37; see Table 2). Both HC (p < 0.001, g = −1.69) and SMC (p < 0.001, g = −2.16) research participants had fewer invalid tapping responses than probable AD patients in the DH. Importantly, MCI-A patients also had fewer invalid tapping responses in the DH than the probable AD group (p = 0.007, g = −0.96). In the NDH, HC and SMC participants had fewer invalid responses than the probable AD group (p = 0.004, g = −1.31 and p < 0.001, g = −2.24, respectively). MCI-A participants did not have significantly fewer invalid tapping responses in the NDH than the probable AD group (p = 0.23, g = −0.66). However, MCI-A patients had significantly greater NDH invalid responses compared to SMC patients (p = 0.006, g = 1.35).
The HC and SMC groups did not differ in their total number of invalid tapping responses (i.e., adding the DH and NDH invalid tapping responses; p = 0.88, g = 0.39). However, SMC participants had fewer total invalid tapping responses than the MCI-A (p = 0.009, g = −1.39) and the probable AD group participants (p < 0.001, g = −2.37). Importantly, MCI-A had fewer total invalid tapping responses than the probable AD group (p = 0.04, g = −0.91). Figure 1 demonstrates differences in total invalid tapping responses across groups.
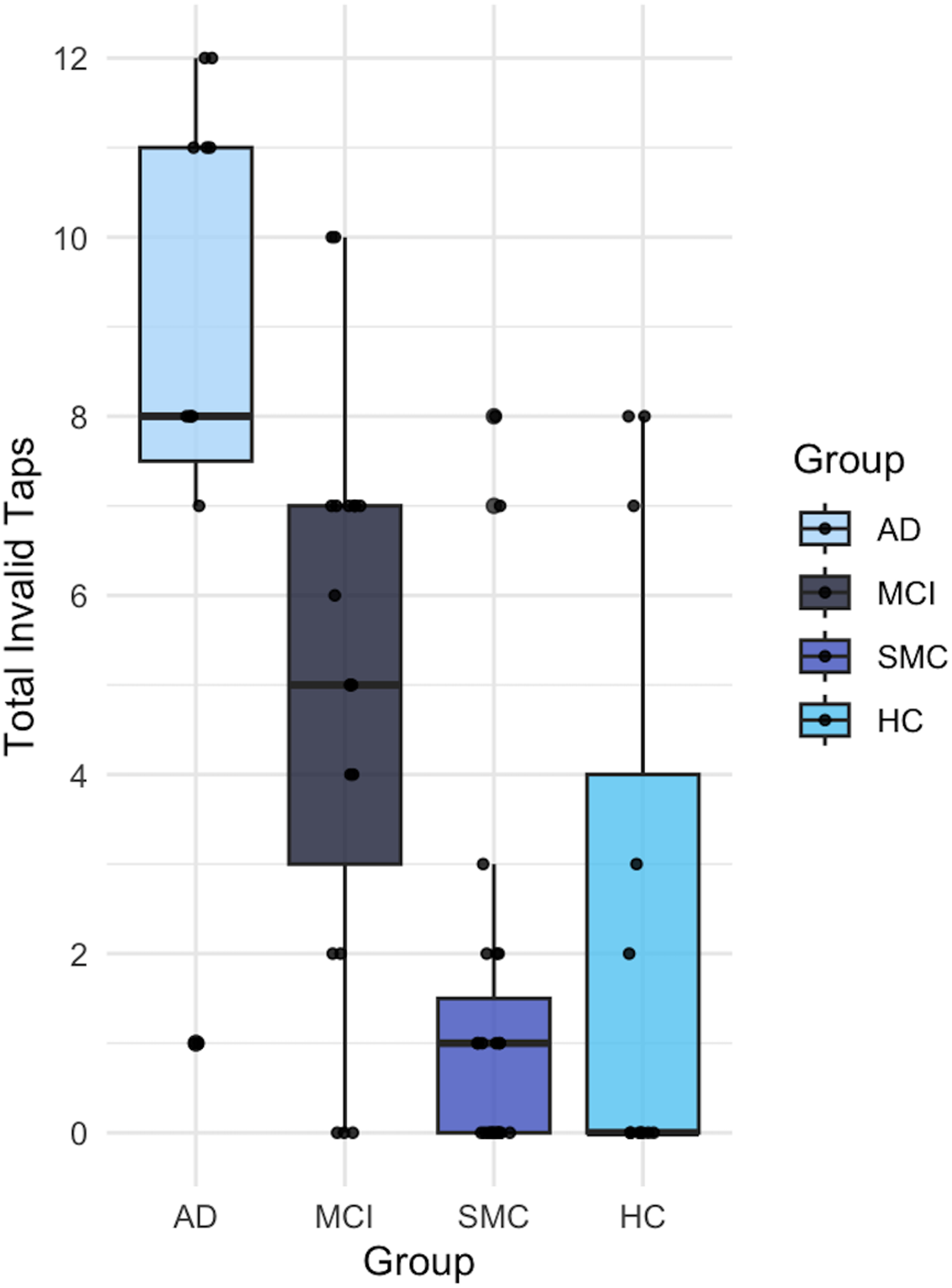
Box plot of total invalid taps (dominant hand + non-dominant hand) per group.
Motor correlates of finger tapping variability
The correlation between DH valid finger tapping variability (e.g., range scores) and invalid tapping responses was ρ = + 0.56, (p < 0.001) with a similar level of correlation for the NDH (ρ = + 0.54, p < 0.001). However, the correlation between the combined range scores of both hands with the total number of invalid responses of both hands was ρ = + 0.65 (p < 0.001).
There were mild to moderate correlations between age and total invalid tapping scores (ρ=+0.47, p < 0.001; Table 3) and the total variability (range) scores (ρ=+0.38, p = 0.002). No relationships were observed between selective motor inhibition responses in the DH or the NDH with the total invalid tapping scores or the total variability scores. A mild learning effect was observed between the DH and total invalid taps (ρ=+0.31, p = 0.01), and a mild correlation was found between DH learning effect and the combined range of finger tapping scores (ρ=+0.45, p < 0.001).
Correlations with total invalid taps and combined range scores.
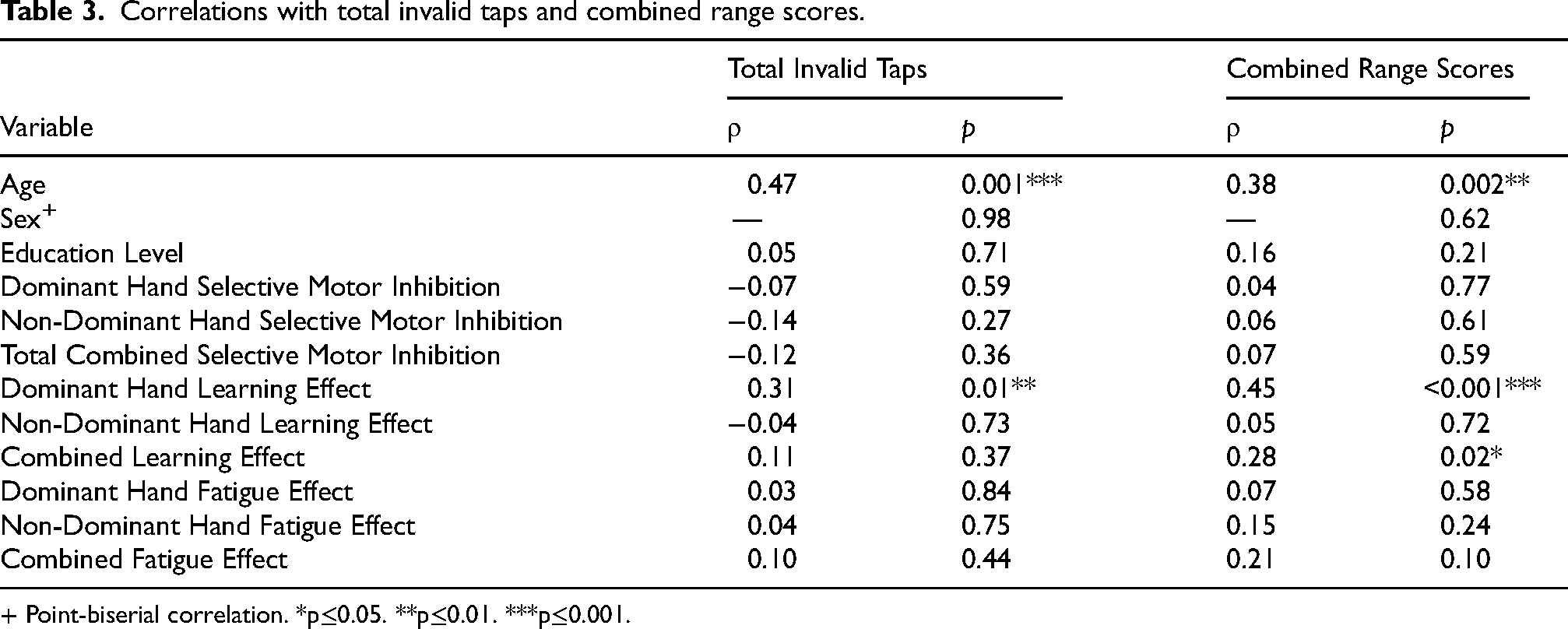
+ Point-biserial correlation. *p≤0.05. **p≤0.01. ***p≤0.001.
Discussion
It has long been recognized that motor slowing may precede cognitive impairments in older individuals30 with either pyramidal31,32 and/or extrapyramidal motor signs.33 Speed of finger tapping has not consistently been identified as an early marker of impaired fine motor functions in persons with mild dementia of the Alzheimer's type (e.g., positive findings reported by Camicioli et al.30 and negative findings reported by Hom2 and Goldman et al.32). Older individuals generally perform tasks more slowly than younger individuals,34 and several variables may contribute to this phenomenon including cognitively reduced speed of information processing16 as well as a decline in vision35 and tactile discrimination/sensitivity.15 Additionally, several studies using different methods of measuring motor function have suggested that motor changes may be uniquely impacted across different forms of dementia, including frontotemporal dementia36,37 and dementia with Lewy bodies.38 Thus, the diagnostic and even prognostic significance of finger tapping behaviors may well depend on how finger tapping is measured.
Clearly, the traditional HFTT test had inherent limitations as a diagnostic and prognostic tool. It limited the measurement of tapping responses to only the dominant hand29 and required that five trials had to have scores within five points of each other before the mean value was calculated. Older normally functioning individuals were often observed to fatigue when performing this task, producing great variability in scores and therefore not easily meeting the criteria originally proposed by Halstead.29 This variability was initially considered unwanted “error variance”, and the test fell out of favor with many clinical neuropsychologists. With time, it was recognized that finger tapping should be measured in both the DH and NDH to aid its diagnostic significance,38 and modification of the administration of the test was needed to capture the various sources of variability observed in clinical practice.18 One advantage of Halstead's29 original finger tapping apparatus was that it required a certain mechanical force to depress the finger tapping lever and a certain finger length extension to release the tapping key so the next tapping movement could be adequately depressed to achieve the next number on a mechanical counter (see Methods section). This simple device thus potentially could be used to also measure learning and fatigue effects in addition to differences in speed of lateralized motor performances.18
With these considerations in mind, we used a modified version of the HFTT to measure mean finger tapping speeds and variability of finger tapping speeds in older individuals with and without neurodegenerative memory impairments. We replicated a reported finding in the literature.8 Non-dominant valid finger tapping variability is significantly larger in persons with MCI-A and AD compared to both HC and SMC groups. The first prediction of this study was, therefore, supported. While a trend for greater finger tapping variability was also observed in the DH (η2p = 0.14), the finding was more robust in the NDH (η2p = 0.19).
Koppelmans et al.8(p1245) have suggested several possible explanations for this phenomenon (i.e., progressive increases in finger tapping variability in the NDH across the AD spectrum), including “accelerated asymmetric cortical thinning” in AD patients and less “motor reserve on non-dominant hand.” They also reported a moderate correlation between hippocampal volume and finger tapping variability, but no differential correlations were reported between the right or left hippocampi volumes and dominant and non-dominant hand finger tapping variability scores to help explain this laterality effect. Jutten et al.17 recently showed that reaction times (which have been shown to significantly correlate with finger tapping variability8) on computerized assessments may reveal incipient cognitive decline in otherwise healthy older adults, possibly reflecting executive dysfunction. While handedness has not been associated with corpus callosum size, reaction time speed and variability in persons with MCI have been found to relate to corpus callosum size.39 Disruption of white matter tracts via the corpus callosum may help explain less efficient lateralized brain processes,40 which in turn may ultimately help explain differences in (valid) finger tapping speeds in MCI-A and AD patients. Bimanual finger-tapping may be more sensitive to disruptions in interhemispheric communication than the more common unimanual version (as implemented herein).8,41 A more recent study also demonstrated white matter microstructural damage in the corpus callosum, as well as in the fornix, in MCI-A and AD patients compared to SMC and HC cohorts.42 These changes may contribute to impaired interhemispheric communication and cognitive deficits.
The findings of the present study also supported the second hypothesis, namely that the number of invalid tapping responses significantly and positively correlated with the variability of finger tapping speed. While both DH and NDH invalid taps were correlated with variability unilaterally, the combined invalid tapping responses were more strongly correlated with combined variability (ρ=+0.65). Moderate age effects (ρ=+0.47 and ρ=+0.38) and DH learning effects (ρ=+0.31 and ρ=+0.45) were also noted for both total invalid taps and combined range scores, respectively. The number of selective motor inhibition failures did not correlate with variability of finger tapping responses. It is interesting to note that dominant hand performance may mildly contribute to total finger tapping variability, further suggesting a role of inter-cerebral hemisphere communication disturbances contributing to finger tapping variability.
Behaviorally, an invalid response simply reflects the fact that the individual moves the index finger without sufficient amplitude (i.e., pressing the lever adequately down or allowing the lever to adequately extend upward) so the next index finger movement could produce the next number on the mechanical counter. Visual inspection of patients while performing this task revealed that many of the invalid tapping responses were associated with small, rapid, repetitive, irregular index finger movements in which the individual felt there was something wrong with the apparatus rather than their ability to perform the task. The “rhythm” of repetitive, synchronistic index finger movements was lost. Luria43(p176) several years ago described such a phenomenon as a breakdown in the “kinetic melodies” of the brain. He noted that the premotor regions of the brain (Brodmann's Areas 6 and 8) as well as postcentral cortical zones played a special role in maintaining this type of motor control. Using somewhat more contemporary terminology, a disturbance of the Default Mode Network might underlie the emergence of invalid tapping responses when performing a modified version of the HFTT. The Default Mode Network has been linked to self-awareness in normal functioning individuals44 and anosognosia in persons with MCI-A and AD,45 suggesting that the altered perception observed during invalid tapping responses may be related to changes in this network. In this regard, future studies should investigate the relationship between invalid finger tapping and self-awareness, including neuroimaging studies of the Default Mode Network to understand the underlying mechanisms of invalid finger tapping.
The final prediction of this study that the frequency of invalid tapping responses would be significantly greater in persons with MCI-A and probable AD compared to HC and SMC groups was also supported. Not only were the HC and SMC groups essentially equal in terms of the frequency of invalid tapping response, but MCI-A patients had fewer invalid tapping responses than the probable AD patients. If a disturbance of frontoparietal components of the Default Mode Network underlies or contributes to the presence of invalid index finger tapping movements, then this finding may have potential prognostic as well as diagnostic significance when evaluating older individuals with memory complaints. Jung et al.,46 for example, have reported that persons with MCI-A who convert to dementia often show early signs of frontal-executive dysfunction in addition to their memory impairments at baseline. Invalid tapping responses, as measured by the modified HFTT, may be a motor manifestation of such early dysfunction.
Limitations of the present study
A major limitation of the present study is the smaller sample size. Larger groups are needed to determine the diagnostic significance of total invalid tapping responses as a discriminator of persons with and without neurodegenerative memory disorders. To mitigate this limitation, we have included effect sizes for all analyses. A second limitation is that the nature of the invalid tapping responses may vary across individual subjects and groups. Detailed kinematic recordings will be necessary to capture the exact motor features that contribute to invalid tapping responses in different groups. A third limitation is that data were obtained by clinical administration and hand scoring of the research participants’ finger tapping responses during their clinical examinations. Computerized administration and scoring of finger tapping behaviors would potentially increase the reliability and validity of the findings. However, for individuals with significant memory and related cognitive impairment, clinical administration is often necessary considering their difficulties verbally following instructions presented to them via a computer. Additionally, the HFTT in the present study was administered and scored by a single rater to remove concerns over inter-rater reliability. A fourth limitation of this study was the absence of biomarkers confirming the diagnosis of AD.47 This study was conducted during a time when AD biomarkers were not yet financially covered by Medicare or private insurance. We therefore identified our AD group as probable AD since clear biomarker evidence of this disease was not present in our sample, and the diagnosis of probable AD was made on the basis of their total neurological evaluation.
Supplemental Material
sj-docx-1-alz-10.1177_13872877241312984 - Supplemental material for Motor correlates of finger tapping variability in subjective memory complaints, mild cognitive impairment and probable Alzheimer's disease
Supplemental material, sj-docx-1-alz-10.1177_13872877241312984 for Motor correlates of finger tapping variability in subjective memory complaints, mild cognitive impairment and probable Alzheimer's disease by George P Prigatano, Lucia W Braga, Molly McElvogue, Katelyn Coddaire, Lori Steffes, Anna Burke and Ashley M Stokes in Journal of Alzheimer's Disease
Footnotes
Acknowledgments
The authors have no acknowledgments to report.
Author contributions
George P Prigatano (Conceptualization; Data curation; Formal analysis; Methodology; Writing – original draft; Writing – review & editing; Project design); Lucia W Braga (Conceptualization; Writing – review & editing); Molly McElvogue (Formal analysis; Review); Katelyn Coddaire (Formal analysis; Writing – review & editing); Lori Steffes (Project administration; Coordinator); Anna Burke (Conceptualization; Data curation; Funding acquisition); Ashley M Stokes (Conceptualization; Data curation; Funding acquisition; Project administration; Writing – review & editing).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Barrow Neurological Foundation and the Arizona Alzheimer's Consortium.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.