
Abstract
Introduction
Dementia is a global health priority in the aging population, and the factors that lead to favorable treatment outcomes are currently unknown. Previous studies have reported that patients with dementia nearly 24.3 million globally in 2005. Approximately 50 million people worldwide currently live with dementia, and this number is expected to triple by 2050.1,2 In the World Health Organization European region, the total number of disability-adjusted life-years attributable to neurological disorders is 41.1 million. Furthermore, there are 2.55 million cases of Alzheimer's disease (AD) and other dementias in the U.S..3,4 Global annual costs are estimated to exceed US$800 billion for care systems. 5 This is the most important aspect of dementia that cannot be modified by current intervention. Therefore, there has been a major significant rise in disease burden associated with dementia.
Diagnosis of dementia was when cognitive impaired severely to influence social and/or occupational function, using the Diagnostic and Statistical Manual of Mental Disorders (5th Edition). 6 Memory damage is due to diminution of a change of cognitive or general cognitive decline, not only memory impairment.7–9 Dementia is recognized as any development of cognition decline that is sufficient to significantly interfere with independent daily functioning. 10 There are numerous causes of dementia, including neurological, neuropsychiatric, and medical conditions. In the elderly, the most common forms of neurodegenerative dementia are AD and dementia with Lewy bodies. The dementia incidence increases gradually till the age of 85 or 90 years and women is major population. Specific age-group rates vary annually from 0.1% to 8.6%. 11 In a previous study, the dementia cumulative incidence of 10-year was 22.20%, and time range was 5.4 ± 3.9 years presence to dementia diagnosis. 12 The odds of developing dementia are higher in older adults with incident epilepsy. A higher comorbidity burden is a risk factor for dementia, and prevalent dementia and increasing frailty are associated with mortality. 13 As knowledgeable, the mechanisms underlying this association were amyloid-β (Aβ) deposition, hippocampal damage, or chronic infection. 14 Recently, it has been suggested that dementia can be prevented by tackling risk factors, including unwarranted alcohol use, traumatic brain injury (TBI), air pollution, etc. Some robust observational studies have suggested that various pathological pathways are implicated in dementia; these pathways are notionally correctable via physical exercise and education.15,16
Epilepsy and dementia co-occurrence frequently and induce worse medical outcomes and boosted healthcare burden. One retrospective cohort study found that dementia in patients with epilepsy who are older than 40 years was associated with extended hospital stays (15%, 95% confidence interval [CI] 10–20%) and higher possibility of re-admission (odds ratio 1.11, 95% CI 1.05–1.17). 17 Epilepsy is characterized by long-term tendency of the brain to develop seizures. Epileptic seizures are clinical manifestations of abnormal and excessive discharge of neurons, with sudden onset and varied and temporary symptoms. The condition includes various consciousness, motor, sensory, and psychiatric events.18,19 According to several studies, the expected epilepsy incidence of developed countries per 100,000 people is 43 cases and approximately double rates of the developing countries.20,21 Epilepsy affects nearly 50 million people universally. 22 It is the third most popular cause of neurological disability worldwide, and it advances the development of dementia by inducing neuropathological changes. Not only TBI is a main risk factor for the development of epilepsy, but it also increases the risk of dementia development, and dementia hazard is enlarged by apolipoprotein E ε4 alleles (APOE ε4) inheritance in both cases. 23 The relationship between TBI and the risk of dementia remains controversial. During a 5-year follow-up period, a study found that TBI was associated with 1.68 (range 1.57–1.80) times greater risk of dementia after adjusting for sociodemographic features and particular comorbidities independently. 14 The dementia incidence around 5% and nearly 20% prevalence among people with epilepsy might be due to previous history of TBI.24,25 Some studies of animal models have validated that AD accumulated Aβ peptide, which leads to repeated seizure. The parallel mechanisms have been proposed for AD in humans. Lesional epilepsy comprises subcategories of focal epilepsy indicating attribution of original etiologies, including hippocampal sclerosis and TBI. 26 Dementia rises the hazard of subsequent epilepsy, especially onset AD among young population.27,28 Epilepsy induced risen morbidity and mortality that can worse the quality of life.29,30
Several mechanisms may explain the link between epilepsy and dementia, with trauma being one of the most frequently mentioned. TBI is a common event, and it can cause a wide spectrum of motor and cognitive disabilities. More studies have revealed that long-term brain damage and accumulation of pathological biomarkers (e.g., amyloid and tau proteins) are related to history of moderate-to-severe TBI. In addition, moderate-to-severe TBI patients develop greater odds of dementia.31–33 Secondary damage due to TBI may cause noticeable mechanisms of neuroinflammation and cytokine destruction. Many progressions after TBI could initiate variant changes resulting in epilepsy. 34 Ishigaki et al. reported that chronically epilepsy, especially mesial temporal lobe epilepsy with hippocampal sclerosis, would be related to cognition impairment, which can be uncontrolled seizures secondarily to the underlying biological abnormality. 35
Studies have reported that epilepsy as a familiar symptom of dementia caused impairment cognition. Limited evidence has shown that the contribution of systemic factors to the development of dementia induces secondary damage, resulting in conditions associated with prominent mechanisms of neuro-inflammation and cytokine damage, such as epilepsy, with or without TBI. To date, no study has specifically distinguished the relationship of dementia and epilepsy in patients without a previous history of TBI. Some studies have noted the relationship concerning dementia and epilepsy, but patients without a previous history of TBI in the elderly population have not been considered. There are no recognized causes concerning to post-injury destruction and age-related brain damage with respect to decline cognitive and dementia. 36 Therefore, the risk of dementia in populations with or without epilepsy and no history of TBI is controversial. This study aimed to determine the association between dementia and epilepsy in patients without history of TBI, using a population-based claims dataset.
Methods
Database
This data-driven population-based research selected samples for case-control study from the Taiwan Longitudinal Health Insurance Database 2000 (LHID2000). LHID2000 contains all the fundamental medical claims dataset of 2,000,000 people who were randomly sampled from patient registration files of over twenty-three million enrollees of the Administration Health Insurance (AHI) research claim dataset in Taiwan. In 1995, the AHI operation in Taiwan and the AHI research claim dataset provided a remarkable model tracing healthcare use for enrollees. More than 23 million individuals are included in this registry dataset. Moreover, the Ministry of Health and Welfare and many other researchers have validated the LHID2000. The Department of AHI stated that there were no differences in gender, age, or measurement magnitude of typical payroll payments among the LHID2000 individuals. The data can be used for research, and numerous peer-reviewed academic journal papers based on the data have been published.37,38
Ethics
Based-on the Declaration of Helsinki, our study permitted by the Taipei Medical University Institutional Review Board (TMU-JIRB NO. N202109070).
Study sample
The Health and Welfare Data Science Center, Ministry of Health and Welfare, provided the dataset from 2000 to 2018. This case-control cohort study selected first-time patients who had no history of TBI including ICD-9-CM codes 800.**∼804.** and 850.**∼854.** who presented at clinics and hospital departments from January 1, 2000, to December 31, 2018. The case group included participants who had their first epilepsy diagnosis (ICD-9-CM code 345) during a healthcare visit to a clinic or hospital between January 1, 2001, and December 31, 2013. To ensure homogeneous sample based on clinically, we composed this sample of people older than 18 years. We were exclusive of those had epilepsy diagnosis within 1 year before their first-time had the same diagnosis. All 6143 individuals with their first diagnosis of epilepsy assigned as the index date were included in the case group. To ensure comparability and diminish the effect of confounding factors, the control group was composed from the remaining payees of the LHID2000 who did not have an epilepsy diagnosis between January 1, 2001, and December 31, 2013. Initially, participants who had prior AHI claim dataset records a diagnosis of dementia were excluded from January 1, 2001, to December 31, 2013, before their index date, and those younger than 18 years (n = 60,922). Subsequently, we randomly selected 24,572 individuals (four comparison subjects versus every individual without epilepsy and no history of TBI) who were matched by sex and age group (every 5 years) from January 1, 2001, to December 31, 2013. For controls, we further matched the first clinic and hospital departments visits within the index year of utilizing healthcare resources. All individuals in the study sample (n = 30,715) were followed up for 5 years or until they developed dementia. In addition, all diagnoses of dementia were made using the ICD-9-CM 290, 330–331 codes, and ICD-10-CM F00, F01, F02, F03, G30-G31 codes (due to the AHI alter the ICD-9 and −10 codes in 2016). Since dementia was long-term care payment according to degree of disability under the AHI guidelines, patients with severe disability proceeded to use any healthcare resource without added self-payment for healthcare resource access. Conditional situations increased patient's healthcare costs for the creation of medical access when needed. To reduce overuse of healthcare resources, the correct diagnostic dementia is administered and inspected by the AHI. Therefore, validity of dementia diagnostic, error of clinical procedures, and up-coding of diagnostic in the AHI claims dataset were considered forceful.
Statistical analysis
SAS system (V.9.2, SAS Institute Inc.) was used for all statistical analyses. The main endpoint of this study was approach to medical care visiting or hospital stay for dementia. We stratified all administrative areas in Taiwan into five sets (urbanization levels from the ranges of level I [highest] to the level IV [lowest]). Chi-square test analyzed differences between the study and comparison groups with respect to socio-demographic features (including monthly income, geographic area, and urbanization level) and medical comorbidities (according to ICD-9-CM codes: stroke [430–438], coronary heart disease [410–414], heart failure [428], atrial fibrillation [427], diabetes [250], hyperlipidemia [272], and hypertension [40-405]). These certain medical comorbidities are potential risk factors of dementia, and they were included while diagnosed prior the index date. Furthermore, stratified Cox proportional hazard regression calculated the association between dementia and previously diagnosed epilepsy in patients without TBI until the development of dementia for up to 5 years from their index date of medical consumption. In addition, we investigated the connection of epilepsy and dementia in different gender groups. This study compared the incidence rates of dementia patients who were epilepsy onset or not. We calculated hazard ratios (HRs) and 95% confidence intervals CIs with significance level of 0.05.
Results
We identified 1,568,265 patients with or without epilepsy and who had no history of TBI in LHID2000. The cohort population analyses were based on a random sample of 30,715 patients who met all the study criteria, including 6143 patients with epilepsy and 24,572 patients without epilepsy. Table 1 shows the sociodemographic characteristics and medical comorbidities of the two groups. This study was composed of 56.6% males and stratified into four age groups (18–54, 55–64, 65–74, and ≥75 years). The mean (± standard deviation) ages of both groups were 48.6 ± 18.87 years. There were significant differences (p < 0.0001) in monthly income and geographic region between the cases and controls. Moreover, cases had higher likelihood of stroke, hypertension, diabetes, coronary heart disease, atrial fibrillation, and heart failure than controls (p < 0.0001).
Demographic features of non-TBI patients with and without epilepsy (n = 30,715).
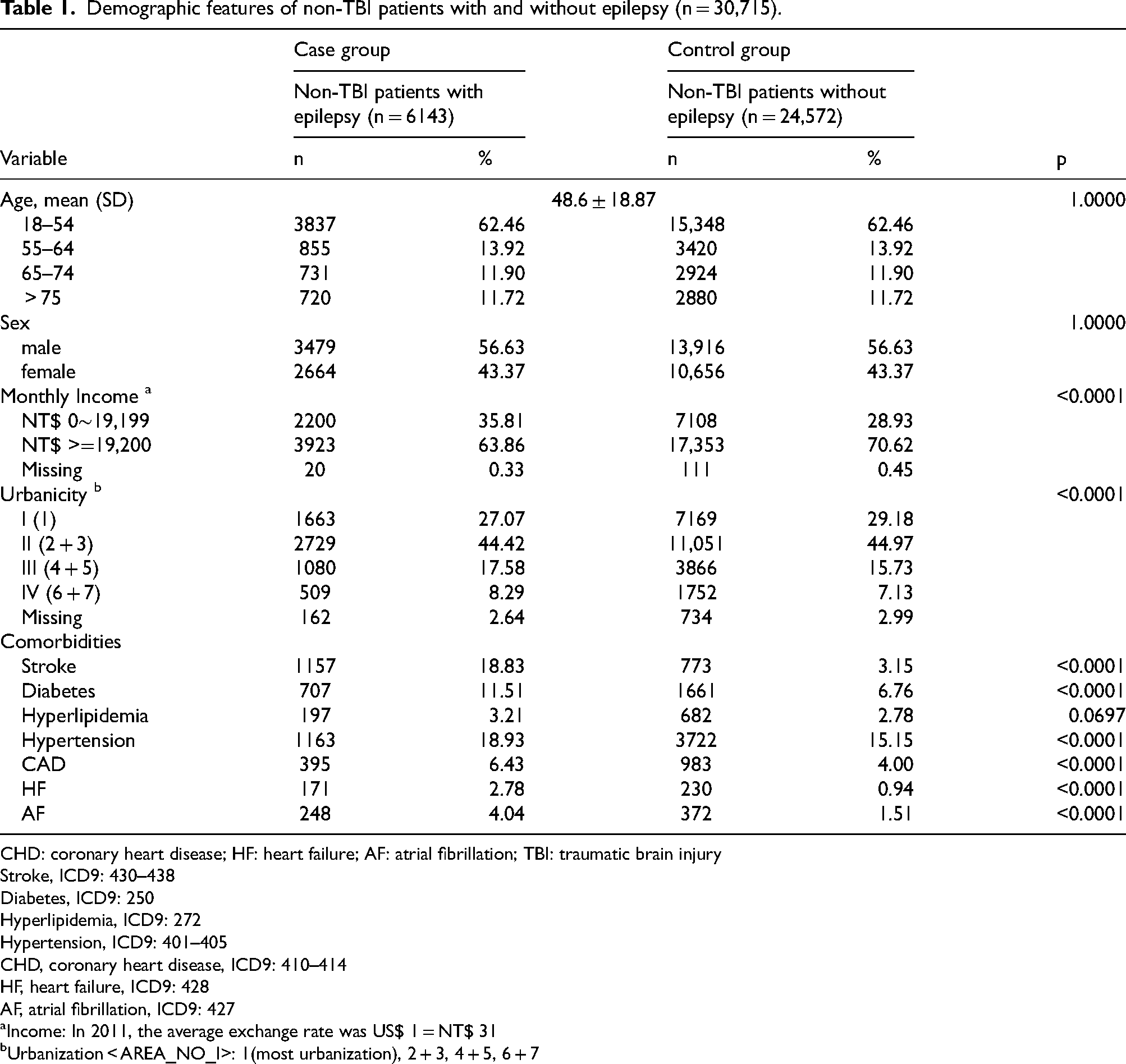
CHD: coronary heart disease; HF: heart failure; AF: atrial fibrillation; TBI: traumatic brain injury
Stroke, ICD9: 430–438
Diabetes, ICD9: 250
Hyperlipidemia, ICD9: 272
Hypertension, ICD9: 401–405
CHD, coronary heart disease, ICD9: 410–414
HF, heart failure, ICD9: 428
AF, atrial fibrillation, ICD9: 427
Income: In 2011, the average exchange rate was US$ 1 = NT$ 31
Urbanization < AREA_NO_I>: 1(most urbanization), 2 + 3, 4 + 5, 6 + 7
Table 2 shows the HR for dementia among cases and controls, determined using stratified Cox regression. Among the 30,715 patients who were diagnosed with dementia follow-up period under 5 years, the dementia onset period was 1.55 year per beneficiaries with epilepsy (the study cohort) and 2.31 year per beneficiaries for patients without epilepsy (the control cohort). In comparison with the control group, the study group was higher possibility of dementia development within the 5-year follow-up period (crude HR: 1.99). After adjustment (including patients’ age, gender, revenue, geographic location, and comorbidities), the HR of dementia patients with epilepsy were 1.84 (95% CI: 1.49–2.26, p < 0.05), and compared to non-epilepsy patients. For both males and females, the study group had higher HR of dementia than the control group: the adjusted HR of the study group was 1.91 (95% CI 1.45–2.53) for males and 1.77 (95% CI 1.29–2.43) for females.
HR for development of dementia during the 5-year follow-up period, starting from the date of index medical utilization.
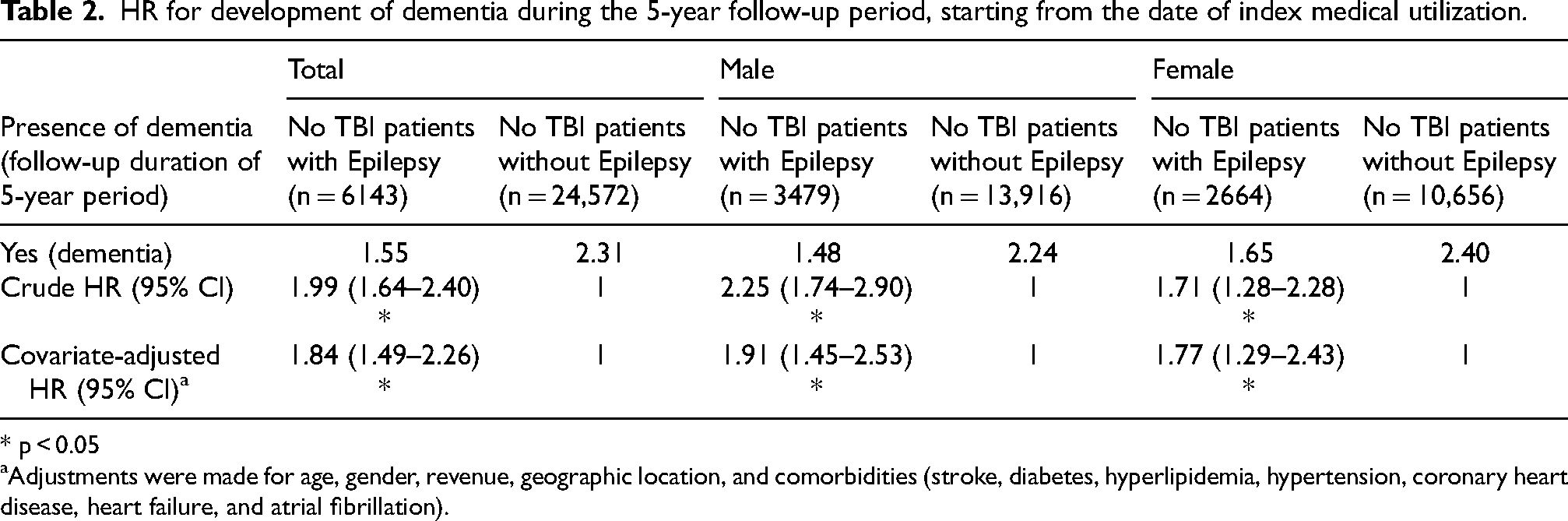
* p < 0.05
Adjustments were made for age, gender, revenue, geographic location, and comorbidities (stroke, diabetes, hyperlipidemia, hypertension, coronary heart disease, heart failure, and atrial fibrillation).
Table 3 presents the adjusted HR of dementia during the 5-year follow-up period after stratifying the patients by age group (18–54, 55–64, 65–74, and ≥75 years). In comparison to patients without epilepsy, the adjusted HR of patients with epilepsy was 2.92 (p < 0.05) in the 18–54 years subgroup and 5.37 (p < 0.05) in the 55–64 years subgroup. Moreover, the adjusted HR of dementia patients with epilepsy in the 65–74 years subgroup was 1.92 (p < 0.05), while it was 1.45 (p < 0.05) in the ≥75 years subgroup. Similar patterns of crude or adjusted HR were found in both males and females dementia patients with epilepsy in different age group, except in the 55–64 years subgroup. However, the highest HR of dementia were found in the 55–64 years female subgroup, with a crude HR of 16.12 (p < 0.05) and adjusted HR of 13.61 (p < 0.05). In addition, the crude HR was 5.81 (p < 0.05) and adjusted HR was 3.02 (p < 0.05) in the 55–64 years male subgroup. Furthermore, there were no significant statistical differences between the case and control groups for the 18–54 years female (HR = 4.23, 95% CI 0.86–21.09; adjusted HR = 1.78, 95% CI 0.22–14.13), 65–74 years female (adjusted HR = 1.42, 95% CI 0.76–2.65), and ≥75 years male (adjusted HR = 1.42, 95% CI 0.96–2.08) subgroups. Additionally, this study revealed that risk of dementia among above 75-year population lowest than other age subgroups (HR = 1.70, 95% CI 1.31- 2.20; adjusted HR = 1.45, 95% CI 1.10–1.92).
HR for the likelihood of dementia among different age groups.
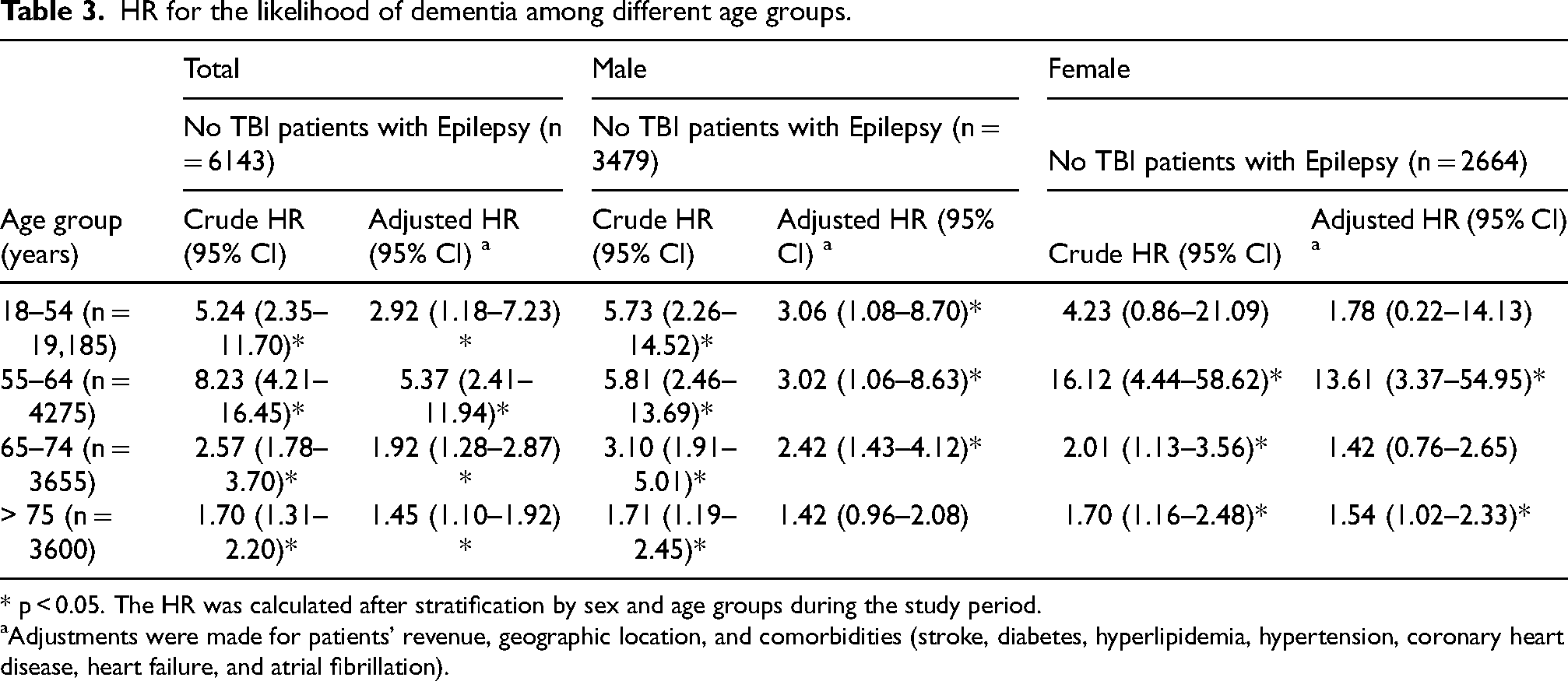
* p < 0.05. The HR was calculated after stratification by sex and age groups during the study period.
Adjustments were made for patients’ revenue, geographic location, and comorbidities (stroke, diabetes, hyperlipidemia, hypertension, coronary heart disease, heart failure, and atrial fibrillation).
Discussion
This study found that epilepsy was strongly associated with elevated hazard of dementia in people with no history of TBI, after controlling for age, gender, revenue, geographic location, and comorbidities. In this random sample of LHID2000 beneficiaries, we investigated the relationship between epilepsy and dementia. The explanatory power of our study is supported by the 18-year observation period and a large database containing a representative cohort of 23,000,000 enrollees. Moreover, only a few studies have investigated the relationship between dementia and epilepsy in patients without TBI. Our results provide a compelling reason for similar hazard patterns of dementia that were consistently associated with the negative impact of dementia in all age groups after adjusting for HR in both males and females with epilepsy. The most notable finding was that among the 55–64 years subgroup diagnosed with epilepsy without history of TBI, the female population had 4.5-fold greater risk of dementia than the male population during the 5-year follow-up period. In contrast, in comparison of the study and control groups, the 18–54 years male subgroup had a higher HR, but no statistically significant differences were observed for the same age subgroup in the female population.
It is generally accepted that the development of dementia involves various systemic elements. A previous study found equal connection of epilepsy and dementia, in terms of either the risk of developing epilepsy among participants with dementia or the risk of developing dementia among participants with epilepsy. Young population, male group, stroke, brain trauma, brain tumors, and low cognitive stage (check by Mini-Mental State Examination score) much risen the risk of dementia. There was also a strong positive association of epilepsy with dementia (OR: 1.72; 95% CI: 1.47–2.01). 39 In comparison with controls who did not have epilepsy, some studies revealed approximately double risk of evolving dementia in patients with epilepsy.27,28,40 A comparable result was found in another study after stratifying for sex (adjusted HR in males = 2.95; adjusted HR in females = 2.66). 41 The Lancet Commission added possible adjustable risk factors for dementia, with updated convincing research evidence with respect to extreme alcohol use, TBI, and air pollution. 16 In the present study, to investigate the association of dementia with epilepsy, we excluded one of the major risk factors for dementia with or without epilepsy, which is history of TBI. Our results showed that compared with patients in the non-TBI without epilepsy cohort, those in the non-TBI with epilepsy cohort tended to have a higher risk of comorbidities.
Previous studies have shown that aging and gender play an important role in neurodegenerative diseases. The development of epilepsy correlates with age as aging advancement would be a risk factor for epilepsy.42,43 The same as previous studies, we found substantial age and gender differences between dementia and epilepsy without TBI. However, the risk of dementia in persons with epilepsy, compared to those without epilepsy among females, appears to be different. This study revealed no statistically significant differences between females aged 18–54 years with and without epilepsy. Furthermore, we found that the risk of dementia in middle-aged females was higher than in males; females aged 55–64 years diagnosed with epilepsy without a history of TBI had 4.5-fold higher risk of dementia than the male subgroup during the 5-year follow-up period. These were in accordance with several long-term follow-up and case-control studies. Studies have also found sex differences in marital status, with a larger percentage of women being married or in stable relationships.44,45 In another study, psychopathology was more common in women (p = 0.007) who were older than 40 years (p = 0.038) and had partial epilepsy (p = 0.017). 46
One more important factor between epilepsy and dementia was age. Several mechanisms support the connection of aging and epilepsy, including involvement of indication pathways, differential expression of enzymes during aging and various neurological and psychiatric diseases, and oxidative and nitrosative stress (as seen in stroke, TBI, AD, and cognitive impairment). 47 A recent study showed that the elderly population with epilepsy is higher likelihood to experience cognition impairment, which maybe a fundamental bidirectional association between epilepsy and dementia. 48 In this large population-based study, we described the frequency of dementia as well as groups of disorders in a claim dataset cohort of adults with and without epilepsy, stratified by age and sex. As expected, conditions common in the adult population with dementia, and the highest HR was found in the 55–64 years subgroup with epilepsy and no history of TBI. However, the HRs of the male and female populations aged ≥75 years had no statistically significant differences after adjustment. It is important to pay attention to males aged 18–54 years who have epilepsy without history of TBI; the HR for dementia was higher in this age group than in other male subgroups after adjustment.
The explanation of the association of epilepsy with aging may be the prevalence of brain diseases with epileptogenic potential (stroke and dementia mostly) and effects of aging on molecular mechanisms that involve neuron networks. 49 Some studies have clarified the connection between aging and epilepsy in neurodegenerative diseases where free radicals are characteristic, such as dementia.47,50,51 In addition, many studies have proved a relationship of epilepsy and dementia, mainly in elderly populations.12,35,52,53 Some studies showed that among patients aged more than 65 years with epilepsy, 20.2% had an underlying disease such as dementia, and epilepsy may have a broader effect on elderly social or healthcare system in developed countries.35,53 Epilepsy is a prevalent brain disorder, and oxidative stress is a possible mechanism involved in epileptogenesis. 50 Inflammation is a key factor in the pathogenesis of both dementia and epilepsy. However, the correlation of epilepsy and dementia remain unclear. 41
This study used a large sample population and proper statistic work to assess the correlation of dementia and epilepsy in patients without a history of TBI. National sampling like this can reduce the selection bias. However, our research has a few limitations. First, some selection dataset which may be connected to both dementia and epilepsy without history of TBI, such as patterns of eating, alcohol consumption, obesity, and tobacco usage, were unobtainable in this study. These confounding factors maybe influence the study outcomes between dementia and epilepsy that was found in this study. Second, the diagnoses of dementia and epilepsy without history of TBI using ICD codes from AHI claims data may not be as precise as those made using clinical diagnosis tests. However, regular validations carry out by the Administration Health Insurance could prevent inappropriate medical coding or improper medical claims; this process includes multiciliary measurements. Third, this population study was mainly Chinese; thus, the generalizability of the findings to the other populations maybe not certified. Fourth, we did not add in individuals with dementia or epilepsy patients without a history of TBI or dementia earlier than 2000, because the AHI claims dataset operated only delivered the medical histories of samples from 1996 until the present, and our study utilized a 5-year follow-up period. Finally, the secondary data obtained from the AHI operation did not have enough information about patient's status to enable us to define dementia and epilepsy without history of TBI or dementia severity. In addition, the subtype of epilepsy and dementia was not included in this study; these need to be studied in the future. Above limitations may affect the validity of this research, and further research is needed to report the limitations.
This study revealed that great proportion of individuals with epilepsy and no history of TBI were diagnosed with dementia compared to controls with no epilepsy. This relationship between dementia and epilepsy in patients with no TBI was particularly pronounced in patients aged 55–64 years, especially in the female population. And it is important to pay attention to males aged 18–54 years who have epilepsy without history of TBI; the HR for dementia was higher in this age group than in other male subgroups after adjustment. There is a need for improved prevention and control of epilepsy patients without TBI, and psychotic indicators after epilepsy should be assessed for possible secondary problems. This research may benefit from greater focus on genetic markers, genetic predisposition to specific sequelae, and potential routes related to epilepsy without a history of TBI-linked appearances. Therefore, more studies are essential in order to address these problems and assess whether appropriate monitoring of patients with epilepsy is efficient in reducing the risk of dementia.
Footnotes
Acknowledgments
This work was supported academically by Taipei Medical University (TMU109-AE1-B28). In addition, a short text would like to acknowledge the contributions of specific colleagues Mr Van-We Lee, Taipei Medical University that aided the efforts of the authors.
Author contributions
Shu-Fen Chu (Conceptualization; Formal analysis; Investigation; Methodology; Writing – original draft); Cheng-Hua Ni (Data curation; Formal analysis; Visualization; Writing – original draft); Kuo-Hsing Liao (Conceptualization; Project administration; Supervision; Writing – review & editing); Ya-Ting Wen (Conceptualization; Investigation; Methodology; Supervision; Writing – review & editing).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data supporting the findings of this study are available on request from the Health and Welfare Data Science Center, Ministry of Health and Welfare. The data are not publicly available due to privacy or ethical restrictions.