
Abstract
Background
Carrying the Apolipoprotein (APOE) ε4 allele lowers age of onset and increases Alzheimer's disease (AD) risk. Neuropathological findings suggest a mixed etiology in many AD patients, and vascular pathology is common.
Objective
This study tested the interactive effect of APOE status and multiple vascular comorbidities on white matter (WM) microstructure in aging and early AD.
Methods
195 participants from the VPH-DARE@IT dataset were stratified in low/high vascular burden based on the Framingham Risk Score (BMI version). Tract-based spatial statistics was used for WM analyses.
Results
There was a main effect of APOE, with APOE ɛ4 carriers having higher fractional anisotropy (FA) and lower axial diffusivity (AxD), mean diffusivity (MD), and radial diffusivity (RD) than non-carriers. There was a main effect of vascular burden with lower FA and higher AxD, MD, and RD in the high-burden than the low-burden group. A significant interaction between APOE genotype and vascular burden was also found for all diffusion indices. Post-hoc comparisons revealed lower left hemisphere WM integrity when comparing the low risk group (i.e., non-carriers low burden) to intermediate risk groups (i.e., non-carriers high burden or ɛ4 carriers low burden). The contrasts between the two intermediate risk groups showed altered WM integrity bilaterally. Only the non-carriers high burden showed greater alterations in WM integrity when compared with the high risk group (i.e., ɛ4 carriers high burden) mainly in right hemisphere tracts.
Conclusions
These findings indicate an interactive effect of a risk gene and vascular comorbidities on WM integrity in aging and early AD.
Introduction
Alzheimer's disease (AD) primarily affects the brain's gray matter as a result of the topographical distribution of two of its key pathological features: amyloid-β (Aβ) and phosphorylated tau. 1 Neuropathological examinations have confirmed that comorbidity with vascular pathology seems to be a common finding in AD patients. 2 There is a large amount of evidence to suggest that vascular damage may be a contributing factor to both gray matter atrophy, as well as chronic white matter (WM) degeneration. Findings from brain imaging studies have highlighted widespread WM microstructural alterations (which add on to gray matter abnormalities) in individuals who are carriers of an autosomal dominant mutation causative of AD and in cases of sporadic young onset AD with onset of symptoms before the age of 65.3,4
A recent histopathological study also seems to confirm that parietal WM lesions (WML) in normal aging are different in their pathological composition relative to parietal WML seen in AD patients. 5 WML in controls tend to be related to ischemic injury, whereas those observed in AD patients could reflect Wallerian degeneration-related axonal loss and demyelination, typically due to AD pathology. 5 Furthermore, WML appearing as WM hyperintensities (WMH) on T2-weighted or fluid-attenuated inversion recovery (FLAIR) sequences have been associated with greater risk of cognitive impairment as well as clinical progression towards AD dementia 6 with midlife vascular risk factors being known to increase WMH volume. 7
Apolipoprotein E (APOE) and WM integrity
The Apolipoprotein E (APOE) is a major cholesterol carrier and is also involved in lipid transport. 8 This apolipoprotein (coded by the homonymous gene) exists in three major isoforms, and carrying one or two ε4 alleles is the strongest genetic risk factor for the late-onset form of AD. 8 Moreover, this risk factor has been found to anticipate the onset of AD symptoms to an earlier age. 9 Different isoforms of APOE are associated with differences in the regulation of Aβ deposition and clearance, tau hyperphosphorylation and neuroinflammation. 8 Moreover, the APOE ε4 allele has also been associated with an increased risk of cardiovascular disease, 10 with evidence from autopsies indicating a possible effect of APOE on cerebrovascular integrity. 11 It is also noteworthy to examine how the APOE ε4 allele might influence WM integrity because both cholesterol and lipids are key components needed to build myelin sheaths. 10
One of the earliest studies that looked at the effects of APOE status on WM microstructure has found distinct findings between younger and older adults. 12 Whole-brain WM analysis using tract-based spatial statistics (TBSS) showed lower fractional anisotropy (FA) in younger APOE ɛ4 carriers in tracts that included limbic association fibers such as the cingulum and superior longitudinal fasciculus, commissural fibers such as the corpus callosum (CC) as well as projection fibers such as the corona radiata, and external and internal capsules. 12 In older adults, on the other hand, only mean diffusivity (MD) was higher among ɛ4 carriers in these areas, without any differences to FA, axial diffusivity (AxD) or radial diffusivity (RD). The authors suggested that the observed differences between APOE ɛ4 carriers and non-carriers could be influenced by age, such that in young adulthood WM structural alterations may be already present years before any clinical symptoms, stabilizing then over the rest of the lifespan.
Another study found that healthy older ɛ4 carriers had significantly lower FA in the CC, bilateral internal and external capsules, bilateral inferior fronto-occipital fasciculi, bilateral inferior longitudinal fasciculi and the anterior section of the cingulum than non-carriers. 13 Higher MD related to ɛ4 was found in the callosal genu (located along the midline) but otherwise had a right predominance in tracts such as the internal capsule, corona radiata and superior longitudinal fasciculus. 13 Higher ɛ4-related RD emerged in the CC (genu and splenium), but also, bilaterally, in the internal capsule, inferior fronto-occipital fasciculus, inferior longitudinal fasciculus, cingulum (mainly in the anterior and posterior regions) and external capsule. 13 These findings suggest that, in cognitively-normal adults, the presence of the ɛ4 allele is associated with lower FA and higher MD/RD, without any visible difference in AxD.
Vascular burden and WM microstructural integrity
Cardiovascular risk factors such as diabetes, dyslipidemia, hypertension and midlife smoking are all associated with an increase of 20–40% in incidence of all-cause dementia. 14 Both cardiovascular risk factors and cardiovascular diseases have been found to influence the etiology of AD, and some of these are based on mechanisms that are linked to those of AD, most of which are complex and still not fully clarified. 15
A study carried out on the Whitehall-II cohort found that increased dementia risk is strongly associated with earlier onset of diabetes, with this association being even stronger among those with a history of diabetes and stroke. 16 Late-onset diabetes, however, was not associated with an increased risk of dementia. In addition, the study found that the combination of diabetes and other cardiovascular comorbidities (i.e., a history of coronary heart disease, heart failure, and stroke) was associated with an even greater risk of dementia. 16
The presence of vascular diseases (e.g., carotid artery atherosclerosis) and related biomarker positivity have been associated with ischemic changes in the brain, such as a bigger WMH volume. 17 Consistently, multiple studies have shown that the presence of two or more vascular risk factors/comorbidities was associated with poorer WM microstructural integrity, generally manifesting as lower FA and higher MD values.18–21
The literature on the effect of APOE variability on WM microstructural integrity suggests mixed and inconsistent findings, and the interactive effect of APOE and clinical indices of vascular burden has been understudied.
Only two studies have explored the interactive effects of APOE status and vascular burden on WM microstructure.19,21 However, only one study 19 found an interaction effect between APOE status and vascular burden in a cohort of cognitively unimpaired (healthy controls) older adults. Having ≥ 2 or more risk factors showed lower FA and higher MD in model 1 (adjusted for age, APOE status, education, high cholesterol, obesity, physical inactivity, and sex) and model 2 (same covariates as model 1 with the addition of WMH). Whereas this similar trend in non-carriers became insignificant after adjusting for WMH volume. 19
To date no study has investigated the interactive effect of APOE status and vascular burden in the AD continuum. To address this gap, this study aimed at examining the interactive impact of APOE status, and specifically the robust effects of the ɛ4 allele, and multiple vascular comorbidities (vascular burden) on WM microstructure in a sample of older adults that covered the pre-clinical and clinical AD spectrum, ranging from cognitively unimpaired controls, to mild cognitive impairment (MCI) and early AD dementia. We conservatively hypothesized that there would be no difference in WM integrity between ɛ4 carriers and non-carriers in any of the diffusion-weighted indices. Secondly, we hypothesized that individuals with high vascular burden will have lower FA values and higher AxD, MD, and RD values compared with those with low vascular burden across projection and association fibers. In addition, damage would be most notable in limbic tracts and tracts traversing through the periventricular regions previously suggested to be vulnerable to vascular pathology 22 with a right predominance indicative of an additive effect. Since the focus of the investigation is the interplay between APOE variability and presence of vascular burden, we also hypothesized that there would be an interaction effect between APOE ɛ4 status and vascular burden, such that the ɛ4 carriers with high burden would show the greatest white matter alterations.
Methods
Participants
A total of 253 participants were initially considered for inclusion. These participants had been recruited as part of the Virtual Physiological Human: Dementia Research Enabled by IT (VPH-DARE@IT) initiative, a multicenter project funded by the EU. All experimental procedures were carried out following the Declaration of Helsinki guidelines. All participants agreed to provide written informed consent. Ethical approval was granted by the regional ethics committee of Yorkshire and Humber, UK (Ref No: 12/YH/0474) for all participants recruited in Sheffield, United Kingdom and by the ethics committee of the Northern Savonia Hospital District (Ref No: 77/2013) for all participants recruited in Kuopio, Finland. Patients were recruited from consecutive referrals to tertiary memory clinics across the centers participating in this project. Exclusion criteria were specified to ensure that these patients were representative instances of the early stage of AD. Controls were also recruited as part of this initiative and were not patients but an opportunity sample of healthy volunteers recruited via word of mouth or among patients’ spouses.
Participants underwent an extensive clinical examination before they were deemed eligible to participate in the study. MCI due to AD was diagnosed based on the criteria from the National Institute on Aging and the Alzheimer's Association. 23 The National Institute of Neurological and Communicative Disorders and Stroke Alzheimer's Disease and Related Disorders Association (NINCDS-ADRDA) criteria were used to classify patients with dementia due to AD. 24 Out of the 253 participants considered for inclusion in this study, 58 had to be excluded due to unavailable APOE genotype, poor quality MRI scans, or missing measurements at the basis of body mass index and blood pressure profiles. In total, the final sample counted 195 participants, including 68 cognitively unimpaired controls, 80 patients with MCI due to AD, and 47 patients with mild dementia of the AD type. All patients have had clinical follow-ups of at least 6 years to confirm diagnosis. A proportion (∼ 70%) of the sample had either cerebrospinal fluid or plasma biomarkers measurements to support clinical diagnosis. In line with standard diagnostic criteria patients and unimpaired controls were not included in the study if they had a Hachinski score greater than 2. In addition, T2-weighted and FLAIR images were used to exclude participants with severe vascular pathology (included participants had deep WMH scores below 2 on the Fazekas scale). Participants included in this study are primarily of Caucasian descent except for two participants (1 Control and 1 AD) who are of Afro-Caribbean descent.
APOE ɛ4 genotype
Each participant had donated a sample of blood as part of the VPH-DARE@IT data collection. This was processed following a standardized polymerase chain reaction (PCR)-based procedure to identify the six main APOE genotypes, i.e., following the same analytical procedure as in De Marco et al. 25 The APOE genotype distribution of our sample included: 0 ε2ε2 (0%), 18 ε2ε3 (9.2%), 99 ε3ε3 (50.8%), 8 ε4ε2 (4.1%), 55 ε4ε3 (28.2%), 15 ε4ε4 (7.7%). Due to the low number of ε2 alleles and unequal distribution by groups, we did not examine the effects of APOE ɛ2 and only focused on ɛ4.
Vascular burden
Vascular burden was quantified using the algorithm of the Framingham General Cardiovascular Risk Profile. 26 The Framingham algorithm provides a sex-specific risk score based on models derived from Cox Proportional Hazard regressions. It gives an overall estimate of the probability of developing a cardiovascular disease within a span of 10 years, based on variables such as age, body mass index, diabetes, smoking regime and a treated or untreated high systolic blood pressure. Three risk groups can be identified based on the Framingham risk scores, as follows: 1) low – less than 10%, 2) intermediate – between 10% and 20% and 3) high – above 20%. Due to the scarce number of participants in the low-risk condition in the cohort included in this study (n = 20), the low and intermediate risks were combined in a “low” vascular burden group (n = 76), while the high-risk scores were labelled as “high” vascular burden (n = 119).
MRI data acquisition
Three-dimensional T1-weighted anatomical images were acquired using a Philips Ingenia 3 T scanner. The specific parameters consisted of: voxel size: 0.94 mm × 0.94 mm × 1.00 mm; repetition time: 8.2 s; echo delay time: 3.8 s; field of view: 256 mm; matrix size: 256 × 256 × 170. In this study, T1-weighted images were used to calculate individual indices of total intracranial volume (TIV) and to support clinical diagnosis.
Three-dimensional T2-weighted anatomical images (voxel size: 1.00 mm × 0.53 mm × 0.53 mm) and FLAIR images (voxel size: 1.00 mm × 0.56 mm × 0.56 mm) were used to assess the presence of severe vascular pathology not compatible with the diagnostic entities of interest and to calculate WMH volume respectively. An automated toolbox was used to extract individual WMH volumes (Table 1).
Demographic characteristics.
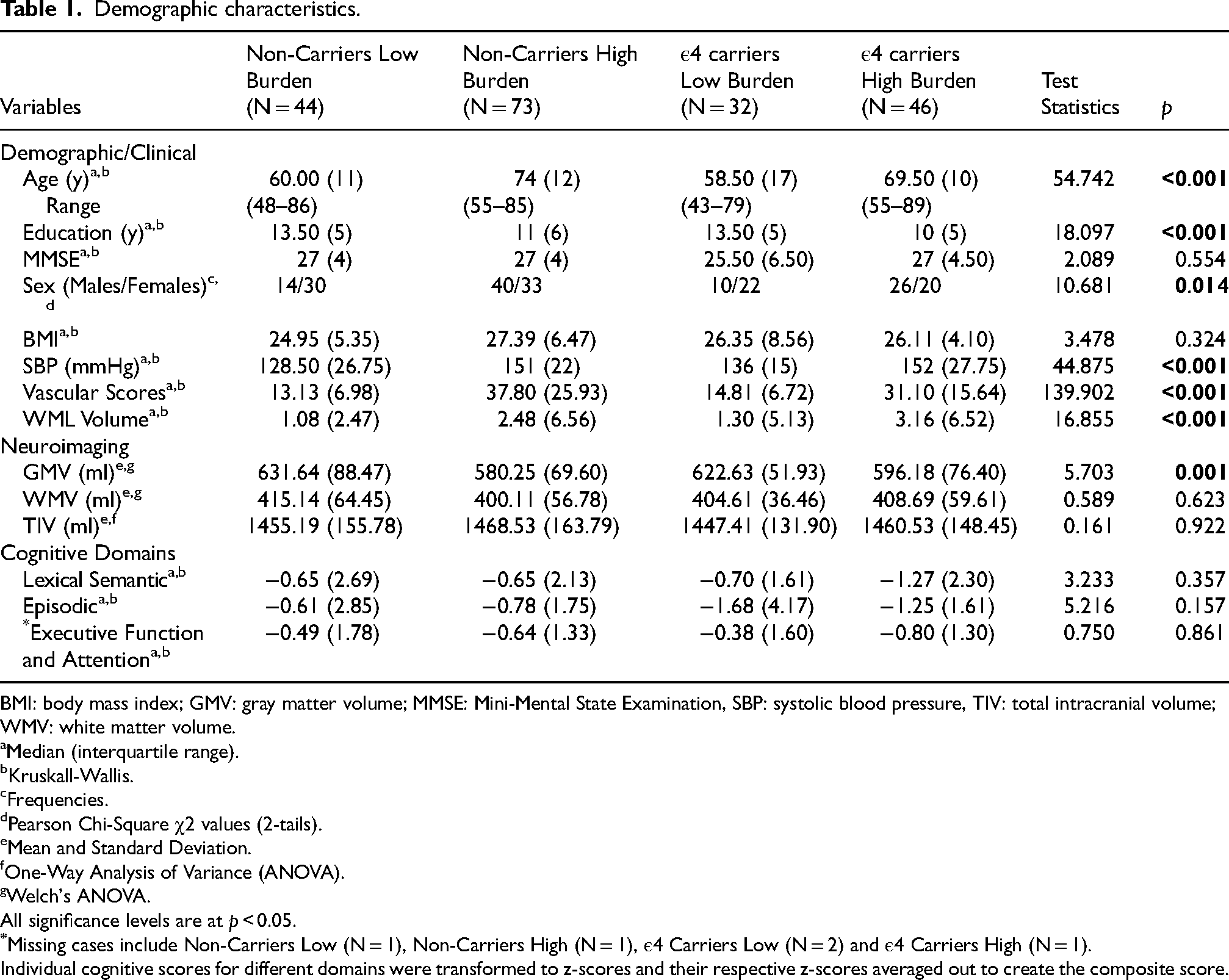
BMI: body mass index; GMV: gray matter volume; MMSE: Mini-Mental State Examination, SBP: systolic blood pressure, TIV: total intracranial volume; WMV: white matter volume.
Median (interquartile range).
Kruskall-Wallis.
Frequencies.
Pearson Chi-Square χ2 values (2-tails).
Mean and Standard Deviation.
One-Way Analysis of Variance (ANOVA).
Welch's ANOVA.
All significance levels are at p < 0.05.
Individual cognitive scores for different domains were transformed to z-scores and their respective z-scores averaged out to create the composite score.
Diffusion-weighted images were acquired with 32 directions, with the following specifications: voxel size 2.5 mm3 isotropic, matrix size 96 × 94 mm2, repetition time 3 s, echo delay time 98 ms, flip angle 90° and field of view 240 × 120 × 240 mm.
Timing of data collection
All data collection for each participant in this study was done on the same day and for a small proportion (5%) of the sample for whom this was not possible, within one week from MRI acquisition.
Imaging analysis
Pre-processing was carried out via the Functional MRI of the Brain Software Library (FSL, https://fsl.fmrib.ox.ac.uk/fsl/fslwiki/), version 6.0.4. Firstly, images were corrected for eddy currents and motion artefacts. The second step served to remove non-brain tissue, via the Brain Extraction Tool. The FMRIB Diffusion Toolbox (DTIFIT program) was used to calculate the diffusion tensor that subsequently resulted in the creation of the FA, AxD, MD, and RD images.
The TBSS procedure was used to complete image pre-processing. Image registration was carried out using non-linear registration of FA images to the standard FMRIB58_FA template. A group-averaged mean FA skeleton mask was created, representing the center of all WM tracts of the entire cohort. FA images were then projected onto this skeletonized mask, and a threshold of 0.2 was applied to remove signal variability from gray matter and cerebrospinal fluid. An analogous procedure was applied to AxD, MD, and RD images.
WMH segmentation
WML volumes were segmented using the Lesion Segmentation Toolbox (LST) version 3.0. 27 Using the lesion growth algorithm, FLAIR images were co-registered to their corresponding T1-Weighted MRI images using the default Kappa of 0.3 with the Markov Random Field parameter set to 1 with the maximum number of iterations set to 50. The output is a bias corrected version of the FLAIR image, a lesion probability map and a HTML report with the volumes.
Statistical analyses
Descriptive statistics for demographic variables were analyzed using IBM SPSS Statistics for Windows, version 28 (IBM Corp., Armonk, NY, USA). Normality of the distribution of continuous variables was checked with the Shapiro-Wilk test. Non-normally distributed variables were compared across groups using Kruskal-Wallis tests. A One-Way Analysis of Variance (ANOVA) was used for normally distributed variables, and Welch's F correction was applied if the data did not meet the homogeneity of variance assumption. Binary and categorical variables were analyzed using Pearson's χ2 tests. The significance level was set at p < 0.05 (two-tailed), and post hoc tests were run to identify group-to-group differences in more detail, using independent sample t-test for normally-distributed variables and Mann-Whitney U test for any variable violating the normality assumption (Supplemental Tables 1–4).
TBSS voxel-wise analysis
Voxel-wise statistical analyses were performed on the skeletonized maps for each of the diffusion indices. The randomise command in FSL was used, with a set rate of 5000 permutations per contrast and a threshold-free cluster enhancement (TFCE) correction, to identify significant clusters at a p < 0.05 threshold corrected for multiple comparisons. 28 A 2-by-2 factorial design was used to investigate both the main effect and the interaction of two factors: APOE status (ε4 carriers versus non-carriers) and vascular burden (low versus high burden). Clusters that survived the significance threshold corrected for multiple comparisons were labelled using the John Hopkins University (JHU) ICBM-DTI-81 white-matter labels atlas 29 and the JHU white-matter tractography atlas. 30 Regions that remained undefined were labelled using the Talairach Daemon atlas. 31 All analyses were adjusted for years of education, clinical diagnosis, site of recruitment and TIV. It is worth noting that age and sex were not included as covariates as these were already adjusted for in the Framingham index formula. The analytical models were, however, also run including age and sex as a check for our methodological choice. Since the goal of the study was to disentangle the independent and interactive effects of APOE status and vascular burden on diffusion-weighted indices, the three clinical groups were combined in single inferential models, in order to maximize variability of our outcome variables.
In anticipation of a potentially significant interaction term, post-hoc analyses were devised for planned post-hoc contrasts that included 4 primary contrasts of interest:
Non-Carriers Low Burden versus Non-Carriers High Burden ɛ4 Carriers Low Burden versus ɛ4 Carriers High Burden Non-Carriers Low Burden versus ɛ4 Carriers Low Burden Non-Carriers High Burden versus ɛ4 Carriers High Burden
A Bonferroni correction was applied to the FWE-corrected p for all the four contrasts (p = 0.05/4 = 0.0125). For all other post-hoc comparisons, a p < 0.05 threshold was used.
Two additional post-hoc contrasts were also carried out:
Non-Carriers High Burden versus ɛ4 Carriers Low Burden Non-Carriers Low Burden versus ɛ4 Carriers High Burden
Results
Significant differences across groups were observed for the following variables: age, education, gray matter volume, sex and vascular scores (See Table 1). Post-hoc analyses were performed for all variables showing significant differences at p < 0.05 restricted to the contrasts that were tested (See Supplemental Information).
Main effect of APOE genotype on WM microstructural integrity
APOE ɛ4 carriers had higher FA than non-carriers in association tracts and WM of the right hemisphere such as the right inferior longitudinal fasciculus, anterior corona radiata, as well as in the frontal, temporal and parietal WM. Similarly, higher FA was also seen in association tracts of the left inferior fronto-occipital fasciculus, left superior longitudinal fasciculus, and more generally for left hemisphere projection tracts (see Supplemental Table 5 and Figure 1). When the analysis was repeated with all Framingham variables accounted for simultaneously, only the main effect of APOE for FA survived, where ɛ4 carriers had higher FA in right hemisphere projection tracts only (see Supplemental Table 10).
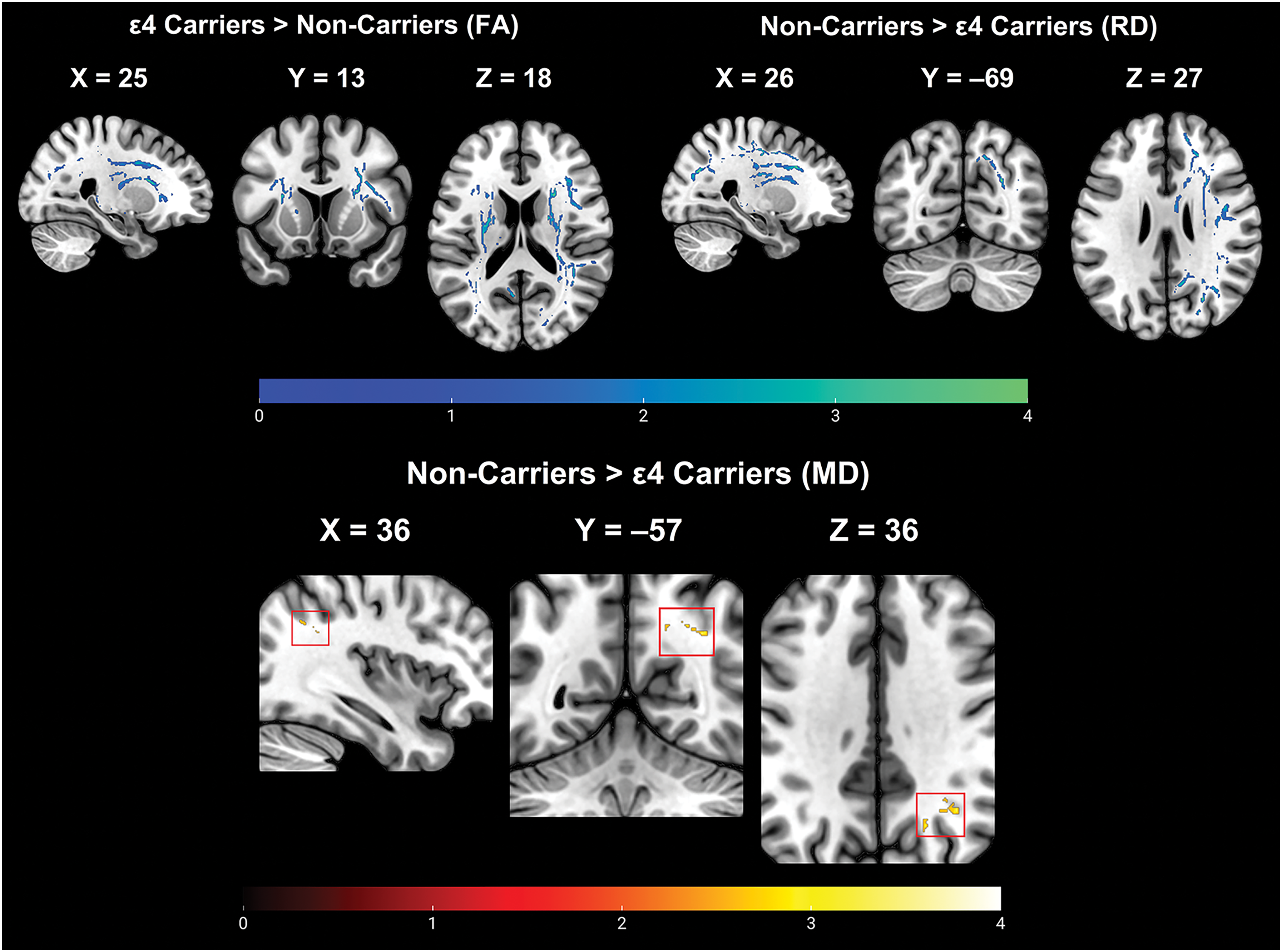
A main effect of APOE status shows that the non-carriers have worse WM integrity across FA, MD, and RD than the ε4 carriers (FWE-p < 0.05). The color bar reflects t-statistics. APOE: Apolipoprotein E; FA: fractional anisotropy; FWE: family-wise error; MD: mean diffusivity; RD: radial diffusivity; WM: white matter.
APOE ɛ4 carriers also had lower MD than non-carriers in the right superior longitudinal fasciculus and the right parietal precuneal WM, lower RD values predominantly in right-lateralized association tracts (i.e., inferior fronto-occipital fasciculus and inferior longitudinal fasciculus) as well as in frontal and temporal areas (see Supplemental Table 5 and Figure 1).
Main effect of vascular burden on WM microstructural integrity
Participants with a low vascular burden had higher FA values in left hemisphere projection tracts (i.e., anterior corona radiata), commissural tracts (i.e., forceps minor and major) and also in the right hemisphere projection and association tracts including WM of the right frontal and limbic lobes (see Supplemental Table 6 and Figure 2).
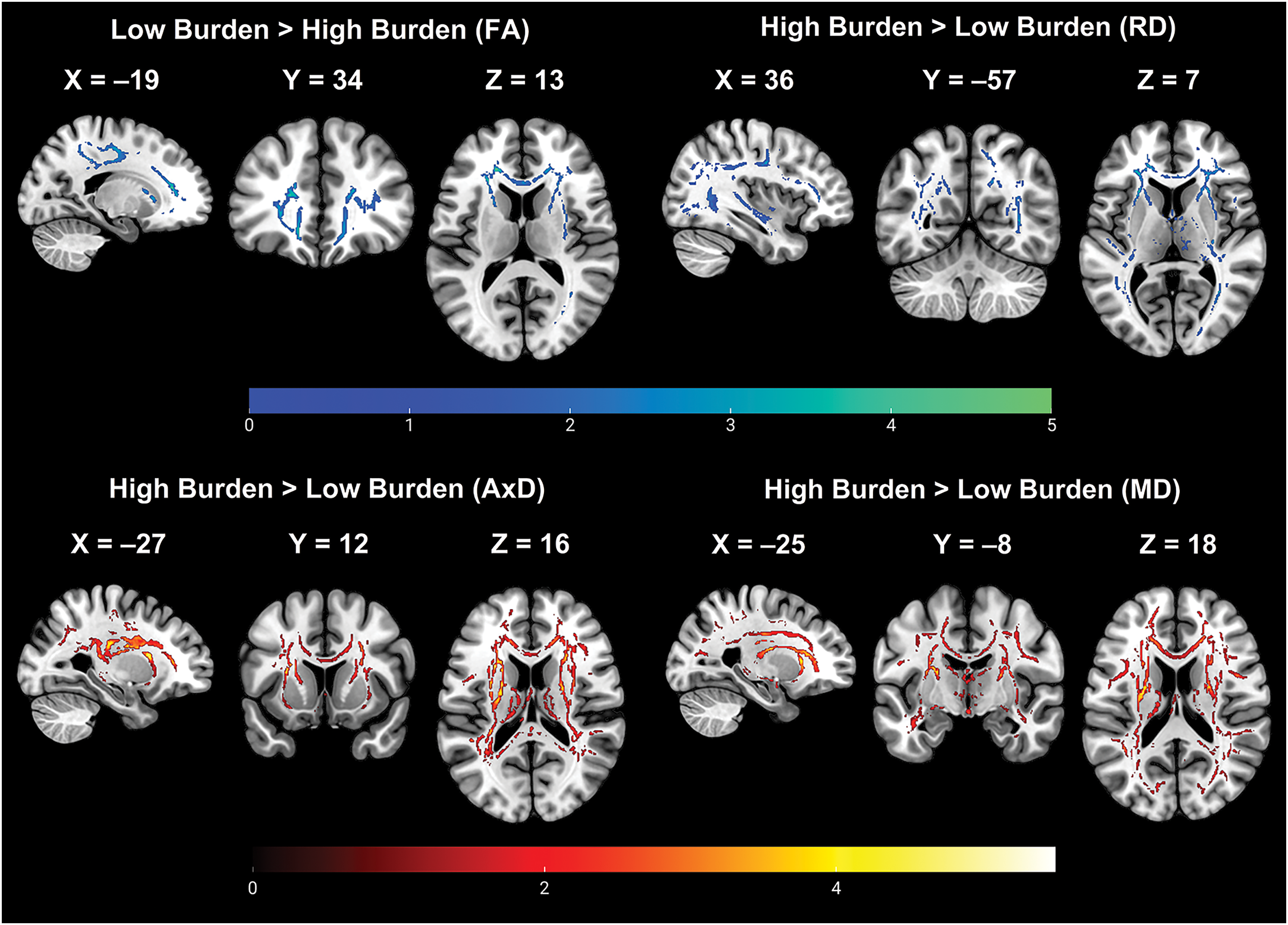
A main effect of vascular burden shows that low burden participants have better WM integrity across all DTI indices than the high burden participants. (FWE-p < 0.05). DTI: diffusion tensor imaging; FWE: family-wise error; WM: white matter.
Participants with high vascular burden had higher AxD in the left hemisphere projection tracts as well and in the commissural tracts. Higher vascular burden had higher MD mainly in the left hemisphere projection tracts and for RD primarily in the left association and projection tracts (see Supplemental Table 6 and Figure 2).
Interaction effects between APOE genotype and vascular burden
A significant APOE status-by-vascular burden interaction effect was found for all diffusion indices: for FA, this was seen in the left limbic tract and parietal WM, bilateral projection, right association and commissural tracts (Table 2, Figure 3); for AxD, this emerged in the right projection tracts; for MD, this was detectable in the right limbic and projection tracts as well as in the commissural tracts; for RD, this was observed in the left limbic WM, commissural tracts, right projection tracts and right frontal and temporal WM.
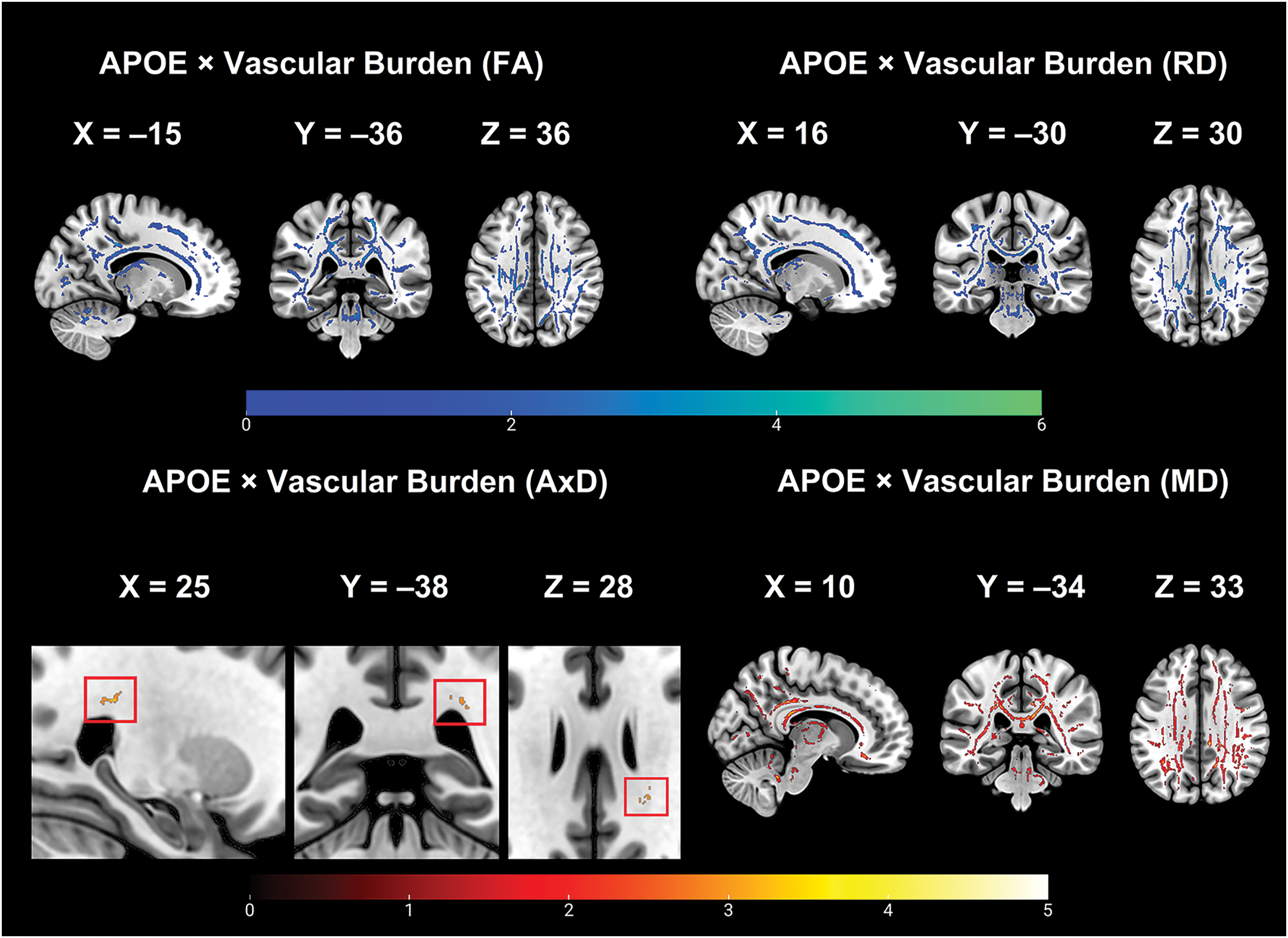
APOE ɛ4 status-by-vascular burden interaction effect on FA, AxD, MD, and RD (FWE-p < 0.05). APOE: Apolipoprotein E; AxD: axial diffusivity; FA: fractional anisotropy; FWE: family-wise error; MD: mean diffusivity; RD: radial diffusivity.
Interactive effects of APOE Status × vascular burden on FA (FWE p < 0.05).
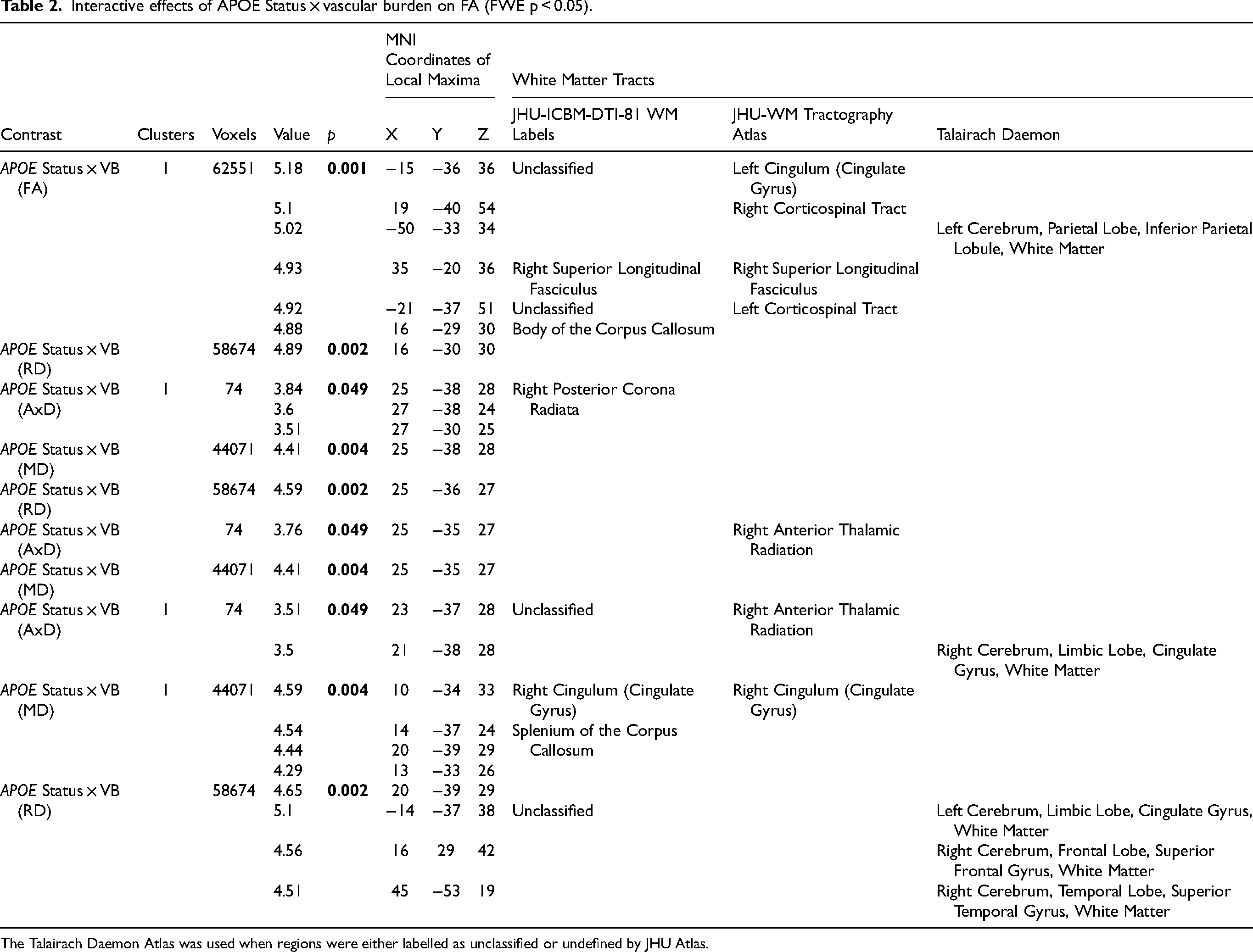
The Talairach Daemon Atlas was used when regions were either labelled as unclassified or undefined by JHU Atlas.
Planned post-hoc analysis contrast 1: non-carriers with low vascular burden versus non-carriers with high vascular burden
Non-carriers with low vascular burden had higher FA in left hemisphere projection tracts and commissural tracts. Non-carriers with high vascular burden had higher AxD in the left hemisphere projection and association tracts. MD alterations were primarily in the left and right hemisphere projection tracts. RD alterations were a combination of bilateral association and projection tracts along with right limbic tracts (see Supplemental Table 7).
Planned post-hoc analysis contrast 2: ɛ4 carriers with low burden versus ɛ4 carriers with high burden
There were no significant results for contrast 2 across any of the diffusion tensor imaging (DTI) indices.
Planned post-hoc analysis contrast 3: non-carriers with low vascular burden versus ɛ4 carriers with low vascular burden
There were no significant results for contrast 3 across any of the DTI indices.
Planned post-hoc analysis contrast 4: non-carriers with high vascular burden versus ɛ4 carriers with high vascular burden
ɛ4 carriers with high-burden had higher FA than the non-carriers with high burden in the left hemisphere limbic tract and parietal lobe WM, and also in the right hemisphere projection and commissural tracts and the right limbic lobe.
The non-carriers with high-burden had higher MD in the right hemisphere such as the parietal and frontal lobe WM, as well right limbic tracts. Alterations in RD were primarily observed in the right hemisphere limbic tracts, frontal lobe WM and association tracts as well as in the left hemisphere projection tracts (See Supplemental Table 7).
Additional post hoc analysis 1: non-carriers with high vascular burden versus ɛ4 carriers with low vascular burden
ɛ4 carriers with low burden had higher FA than the non-carriers with high burden in the right hemisphere association tracts and temporal, parietal and limbic WM. The non-carriers with high burden had higher AxD than ɛ4 carriers with low burden primarily in the left hemisphere projection and commissural tracts. For MD, the alterations were mainly observed in the left hemisphere projection tracts. For RD, the alterations were observed in right hemisphere frontal and parietal WM and left hemisphere projection tracts (see Supplemental Table 8).
Additional post hoc analysis 2: non-carriers with low vascular burden versus ɛ4 carriers with high vascular burden
ɛ4 carriers with high burden had higher AxD than the non-carriers with low burden primarily in the left hemisphere projection and association tracts (see Supplemental Table 8).
Overall, a tract-based overview of all the findings above can be found in Supplemental Table 9.
Discussion
The findings of this study show that participants with at least one APOE ɛ4 allele, independently of their clinical diagnosis and vascular burden status, presented with alterations in WM microstructural integrity: APOE ɛ4 carriers had clusters of higher FA and lower AxD, MD, and RD than non-carriers. This pattern of findings might not be related to neurodegeneration but potentially explained by inherent divergent developmental trajectories in maturational rates of myelination for APOE ɛ4 carriers and non-carriers. A study on children found that ε4 carriers may myelinate earlier, however, their rate of myelination is slower than the non-carriers and this allows the non-carriers to catch up and subsequently surpass them. 32 This differential rate of myelination, therefore, might affect microstructural properties (axon diameter/distribution, packing density, membrane permeability and degree of myelination) resulting in differences in FA. 33
An alternative explanation might be related to and intertwined with the greater effects of AD neuropathology in ɛ4 carriers. Racine and colleagues found that FA was higher in the limbic tracts of Aβ+ individuals. 34 Additionally, Aβ- participants with a modest peptidic load (i.e., with a standardized uptake value of amyloid tracer on imaging between 1 and 1.17) had higher FA in the right medial and posterior cingulum. 34 In an additional study carried out in community-dwelling adults, participants with a limited amount of pathology (i.e., significantly less intense than Aβ+) showed higher diffusion restriction (i.e., higher FA and lower RD), while the pattern was reversed (i.e., lower FA and higher RD) in Aβ+ participants. 35 During the early phase of Aβ deposition, peptidic aggregation is positively associated with FA and negatively associated with AxD, MD, and RD. 36 However, with further Aβ aggregation, the pattern appears to reverse. Additionally, according to the findings of a murine model, higher diffusivity restriction could reflect a pattern during the early phase of disease where there is an FA increase prior to the onset of AD followed by an FA drop concurrent to plaque accumulation. 37 Another possible interpretation is that higher diffusivity restriction might reflect swelling due to vascular permeability and inflammation. 35 Taken together, the evidence emerging from the literature on Aβ accumulation suggests a bi-phasic trend of DTI changes accompanying different disease stages. Although methodologically distinct, the trend reported in our study of a significant difference uniquely found in the group of MCI might reflect similar mechanisms linked to different phases of pathology.
This pattern was not aligned with our original expectations (i.e., we had hypothesized no APOE status-based differences); however, when repeating the analysis without clinical diagnosis as a covariate (findings not shown), no effect of genotype was found for any of the diffusion indices, in line with Adluru et al. 38 who found no main effect of APOE genotype in a sample of cognitively unimpaired middle-aged participants at risk of dementia (either ε4 carrier or with parental family history) stratified by APOE genotype (carriers/non-carriers) and family history of AD (presence/absence). Another study that looked at both cross-sectional and longitudinal association of vascular burden and APOE ε4 carrier status found no significant baseline differences in FA or MD, except for the ε4 carriers having higher MD in the sagittal stratum, 21 a tract that includes the inferior longitudinal fasciculus and inferior fronto-occipital fasciculus. 29 One can speculate that the degeneration of these association fibers is salient in aging as they are highly vulnerable to AD pathology, and degeneration in these tracts may be a predictor of progression from MCI to dementia. 39
A significant main effect of vascular burden also emerged from our results. The group with high vascular burden had lower FA and higher AxD, MD, and RD values compared with the low-burden group. The largest cluster of altered FA included the left anterior corona radiata, corticospinal tract, inferior fronto-occipital fasciculus and forceps minor. These results are in line with those of previous studies that investigated healthy middle and old-age adults and found that aggregated vascular risk factors were associated with lower FA.20,21 Some of the tracts in which an effect was found in the present study overlap with the findings of Cox et al. 20 who confirmed that the aggregated influence of vascular risk factors on FA included all association, commissural and projection/thalamic tracts, whereas some tracts where a significant effect was found overlap with the cross-sectional results obtained by others 21 and were mostly association and projection fibers. On a similar note, Maillard et al. 18 found that having a higher number of vascular risk factors was associated with worse overall WM integrity, i.e., lower FA.
As for AxD, the strongest effect of vascular burden in the present study was seen mainly in the left projection and association tracts, as well as in commissural tracts. These findings are in line with those of Williams and co-workers 21 who found an increase in MD in the presence of high vascular burden in tracts largely comparable with those of our study (i.e., the anterior corona radiata and the posterior limb of the internal capsule). For RD, finally, the largest cluster of between-group differences was located in the left-sided projection and association fibers, with the exception of the right posterior thalamic radiations and inferior longitudinal fasciculus.
A significant interaction between APOE genotype and vascular burden was also found for all diffusion indices. For FA, this effect was widespread across multiple tracts, bilaterally. Similarly, Wang et al. 19 also found a significant interaction effect between APOE ε4 genotype and the number of vascular risk factors. Vice versa, Williams et al. 21 found no APOE-vascular burden interaction effect on FA, neither cross-sectionally, nor longitudinally.
A first set of post-hoc analyses revealed interesting findings between groups with different risk levels. The general trend from the post-hoc analyses was that there was a preference for leftward hemisphere tracts when comparing the low risk group versus the intermediate risk group (i.e., non-carriers low burden versus non-carriers high burden) or the low risk versus the high risk group (i.e., non-carriers low burden versus ɛ4 carriers high burden). When comparing the two intermediate risk groups (i.e., non-carriers high burden versus ɛ4 carriers low burden), bilateral WM tracts involvement was found. Similarly bilateral involvement was also observed for any comparisons between intermediate and high-risk groups (i.e., non-carriers high burden versus ɛ4 carriers high burden), but non-carriers with high burden had worse WM integrity than the ɛ4 carriers with high burden with a greater prevalence of right hemisphere tracts. Interestingly, no significant differences were found between non-carriers low burden versus ε4 carriers low burden and between ε4 carriers low burden versus ε4 carriers high burden after applying a threshold of p < 0.0125.
These results from the post-hoc analyses reveal a completely new finding for AxD as they suggest that there is a preferential vulnerability for the left association and projection tracts. Specifically, both high burden carriers and non-carriers seem to show greater AxD than the low burden carriers and non-carriers.
An early study found longitudinal gray matter atrophy rates in AD patients to show faster local loss, with greater severity in the left hemisphere. 40 Nevertheless, if we are to consider that the effects of APOE on WM microstructural alterations are likely to be subtle, we can conclude that this preferential leftward asymmetry for association and projection tracts might be a consequence of the greater impact of vascular burden on axonal changes, as indicated by AxD, along with disease severity. Previous findings have also demonstrated an association between vascular risk factors and higher AxD and RD indicative of an association between vascular risk and axonal degeneration and demyelination. 19 Similarly, Jang et al. 41 found higher AxD and RD in mixed dementia (amyloid positive with WM hyperintensities) relative to pure AD (amyloid positive without WM hyperintensities) and vascular dementia (amyloid negative with WM hyperintensities) patients. The authors attributed this increase in AxD and RD to ischemic conditions in the presence of amyloid burden.
A key signature of vascular pathology with respect to DTI indices is the increase in AxD and RD in the frontal and parietal WM areas compared with more temporal regions. 42 These variations in diffusivity indices have been highlighted by Burzynska et al. 43 as a pattern of chronic WM degeneration and is an indication that generally an increase in AxD reflects a more severe pattern of WM alteration that cannot be ascribed to Wallerian degeneration. It should also be noted that there are contradictory findings in the literature that have refuted the leftward asymmetry observed in AD. A meta-analysis did not find preferential vulnerability for the left hemisphere, rather a region-specific asymmetry in both healthy aging and neurodegeneration. 44 However, the authors failed to make a distinction between possible AD and probable AD along with stage specific severity in the meta-analysis. Despite these contradictions in asymmetry, these findings related to AxD suggests that these tracts in the left hemisphere are at a more severe stage of WM degeneration than those in the right hemisphere possibly due to a combination of both neurodegeneration and vascular risks.
For MD, a significant effect emerged primarily in the right hemisphere, across the anterior thalamic radiation, the posterior corona radiata, the cingulum and the splenium of the CC. These findings are similar to another study 19 that found a significant APOE-burden interaction influencing MD. In particular, high-burden non-carriers had greater MD than low-burden non-carriers, primarily in projection tracts, bilaterally, and in left-sided association tracts. High-burden non-carriers had greater MD than low-burden carriers mainly in the left projection tracts.
The results of the final post-hoc analysis diverged from the findings by Wang et al., 19 who found that being an APOE ε4 carrier with ≥ 2 vascular risk factors was associated with higher MD, whereas our results show that this is only true for non-carriers with high vascular burden. Although others found no significant interaction between APOE ε4 status, vascular burden and time, 21 they found that ε4 carriers with greater vascular burden had higher MD in the bilateral fornix (body). On the contrary, we found high-burden non-carriers to have higher MD than the ε4 carriers in the right fornix. These findings suggest that, generally, when high burden non-carriers are compared with the two least risky groups, i.e., the low burden carriers or non-carriers, the effect of vascular burden show a leftward asymmetry for association or projection tracts. However, this trend is reversed in the two risky groups, i.e., the high burden non-carriers and high burden carriers, who show a rightward asymmetry in association and projection tracts.
Finally, we also found an interaction between APOE ε4 status and vascular burden for RD, primarily in the body and splenium of the CC and in the right posterior corona radiata. These findings expand those by Adluru et al. 38 who observed an interaction effect for RD between age and APOE status, whereby ɛ4 carriers in the oldest group (i.e., ≥65 years) had higher RD in the genu compared with non-carriers, and suggest that the interactive effects of genetic susceptibility and vascular burden extends myelin damage beyond the genu to more mid and posterior regions of the CC. A similar interpretation that was mentioned for MD would also explain the observations for RD. Overall, the pattern of findings, emerged from published studies and from our research, suggests that the link between WM integrity and vascular burden is intricate and multi-dimensional. In all likelihood, this is also influenced by concurrent pre-existing neurostructural alterations, and by variability in the methodological tools used to quantify or define vascular burden.
APOE and WM microstructural integrity
We found higher FA values in high burden ε4 carriers compared with high-burden non-carriers, after controlling for clinical diagnosis. These results appear to be in line with those of Adluru et al. 38 in a sample of people with a family history of AD, who had higher FA in tracts such as the genu and superior longitudinal fasciculus. Higher FA values in high-burden carriers may be explained by the fact that generally ε4 carriers usually show more compromised WM microstructural integrity, i.e., lower FA values, than non-carriers. 45 This is also supported by findings from de Groot et al. 46 who reported that in localized areas ε4 carriers showed an increase of FA values over time and that this was due to them having lower FA values at baseline as compared with non-carriers who showed a much greater decline. However, these similar findings do not reveal much about the nature of the increase in FA. It is also important to note that we were unable to run additional analyses by accounting for Aβ levels as they were only available for a subset of the sample. However, when we ran the analyses for the main effect of APOE within each clinical group, this pattern was only observed in the MCI cohort (mean age = 69.51 years). This is similar to the findings by Collij et al. (2021). In this latter study, the effect was seen in a cohort of APOE ε4 carriers with an age range between 60–70 years and interpreted by the authors as possibly reflecting ongoing Aβ aggregation.
Vascular burden and widespread WM microstructural alterations
Vascular burden was associated with widespread disruption to the WM microstructural integrity. In particular, the analysis of both AxD and RD indicated that this extended to a range of different types of tracts, specifically to late-myelinating long-range association tracts, commissural and projection tracts. These findings are in line with those of a study that looked at the differences in diffusion indices between several dementia subtypes: Jang et al. 41 showed that only lower FA was relevant in pure AD cases, whereas in cases with either pure subcortical vascular dementia or mixed dementia, greater AxD and RD played an important role as they reflected chronic WM degeneration.
As high AxD values represent a more severe stage of compromised microstructural integrity, early-myelinating projection fibers were mostly implicated in the pattern of AxD. As for RD, on the other hand, the findings indicated an involvement of CC fibers (genu, body, and splenium). A longitudinal investigation by Williams et al. 21 found that a high baseline vascular burden was associated with lower FA in the cingulum (hippocampal part), fornix and splenium of the CC. Moreover, there was a longitudinal increase in MD in the splenium in this group. Consistently, a review found that limbic tracts, such as the fornix, cingulum, and tracts crossing through the hippocampus that are generally susceptible to the impact of AD were also the ones most vulnerable to vascular damage. 22
Moreover, previous evidence suggests that, when comparing patient groups with either mixed pathology (i.e., vascular and AD) or with AD only, those with mixed pathologies have less severe AD-related damage, despite having the same degree of cognitive impairment. 47 This is why Williams et al. 21 observed more widespread changes in cognitively normal participants at baseline rather than longitudinally, because pre-existing structural damage due to vascular burden was already present. Likewise, our study indicated that high-burden non-carriers had the most widespread white matter microstructural damage, even more than high-burden ɛ4 carriers. From a physiological perspective, ɛ4 carriers tend to go through a faster rate of hippocampal atrophy and cortical thinning. 48 Therefore, it may be argued that, in the presence of vascular burden, this group might have had an accelerated rate of gray matter atrophy as well as white matter degeneration and have already reached floor level in the curve of brain tissue loss, whereas high-burden non-carriers may still be undergoing structural changes.
A few studies found that when multiple vascular risk factors are present simultaneously, a reduction in WM microstructural integrity is observed, especially among APOE ε4 carriers.19,21,38 Aging-related findings show that the genu showed the strongest predisposition to chronic WM degeneration, Wallerian degeneration and demyelination, while the posterior areas of the CC showed no reduction in FA. 43 In general, published findings indicate that the effects on WM integrity of vascular diseases do not manifest with any specific topographical pattern. This heterogeneity may be due to the fact that different studies have focused only on a set of selective cardiovascular risk factors. Nevertheless, others have highlighted that alterations in WM due to vascular pathology are commonly seen in specific areas, such as the parietal WM, centrum semiovale, temporal/occipital areas, while ischemic damage is more typically found in the periventricular territory. 22 More importantly, our findings, in line with previous studies show that, aside from the late-myelinating association fibers, 49 vascular burden tends to have a detrimental effect on projection fibers and on the splenium of the CC. 50 The involvement of the splenium is important, given that there is some evidence to suggest that the CC may be one of the earliest tracts to degenerate in AD. 51 Different CC sub-regions show different levels of severity of degeneration in amnestic MCI patients. 52 However, the genu seems to be the most susceptible to AD pathology early on, as indicated by lower FA, higher MD and RD values and a negative correlation between MMSE and MD values in frontal tracts, to which fibers of the genu contribute to, due to anatomical proximity. 52 Previous studies looking at aging-related WM degeneration cross-sectionally and longitudinally have found myelin breakdown and reduced axonal density in late-myelinating tracts as compared with early myelinating tracts.53,54 Generally, the genu is considered to be late-myelinating compared with the posterior splenium, due to it being positioned anteriorly in the vicinity of the late-myelinating frontal areas. 51 Recent studies that have looked at properties of axonal metrics to study axonal diameter and density found that age-related alterations in axonal indices were spared in the splenium. 55 Based on this premise, it can be suggested that the effect of vascular pathology seems to be additive to the effects of neurodegeneration due to AD. These cumulative effects appear to be particularly evident in the regions that are already undergoing degeneration (leftward asymmetry) early in the AD disease course and progressively also spreading to those regions that are generally not susceptible to neurodegeneration until later stage (right asymmetry), given that these are observed in an early-myelinating region of the CC that is relatively spared during aging but affected by AD pathology. It needs to be pointed out, however, that when testing specifically for asymmetry of findings between the two hemispheres, no significant results were observed. This might be probably explained by subtle differences in WM integrity parameters between the two hemispheres that might be subthreshold. These did emerge in the individual comparisons that had very stringent statistical thresholds but were nullified when the two hemispheres were directly compared.
Limitations
A limitation of this study is its cross-sectional nature that prevents a deeper understanding of how individual differences in vascular measures (i.e., blood pressure, cholesterol) that change over time can affect diffusivity measures (first and foremost, FA and AxD) that are dependent on APOE status. Secondly, without histopathological data, a definitive conclusion cannot be drawn on whether higher RD values may be a sign of early inflammatory processes. Moreover, several of our dementia cases, although with a prevalence of neurodegenerative pathology consistent with AD, had some comorbid vascular conditions and, therefore, the duration of different vascular diseases (not adjusted for) may have played a role in determining more severe WM alterations.
These variegated findings suggest that diffusivity changes in WM are not as linear as once thought on the basis of findings from diffusion studies of ɛ4 carriers and Aβ+ participants. It is possible that being an ɛ4 carrier and having vascular as well as Aβ/tau pathology could contribute to early inflammation, prior to AD-related changes, resulting in increased FA and reduced AxD, MD, and RD values. However, as the disease progresses, when full-blown neurodegeneration succeeds this transient state, these diffusion parameters might show different trends, i.e., increased AxD, indicating axonal injury, and increased RD, suggesting demyelination, thereby reflecting a more severe phase of AD. It is still unclear whether the complex relationship between AD and vascular pathology generates either additive or synergistic effects on WM microstructural integrity decline. Previous findings have reported that vascular burden (as measured by WMHs) can influence cognitive impairment 56 and hippocampal atrophy 57 independently. Our results seem to indicate that, while some WM regions may be affected by both AD and vascular pathology, generally vascular pathology tends to exert an effect additive to that of AD, given that it affects early-myelinating tracts such as the splenium.
A similar principle would apply to AxD, whereby higher AxD might reflect a more serious stage depending on the severity of neurodegeneration and the presence of extraneous factors such as vascular comorbidities. To conclude, it is probable that the pathological processes such as amyloid and tau deposition prior to symptom onset and immediately post-onset might be dissociable in nature, but these processes might converge during the late disease stage reflecting a homogenous pattern. Given the non-monotonic nature of these changes in WM metrics, further research is warranted to understand whether having extraneous factors such as Aβ+/tau + status and vascular comorbidities results in multiple stages of WM damage. Future studies should validate whether it is possible to measure quantitatively the relationship between DTI WM metrics and histopathologic data to ascertain if WM microstructural changes may be due to early inflammatory processes. Additionally, a better characterization of the nature of WM damage might be achieved by running a complementary study that runs similar analyses using the normal-appearing white matter.
An important limitation that has not been discussed within the context of vascular burden but that needs to be highlighted is that the sample in this study was overwhelmingly Caucasian. Therefore, racial/ethnic background was not taken into account. This is important to note because in recent years there has been emerging evidence of racial/ethnic factors contributing to differences in AD biomarkers, highlighting the importance of race in disease trajectory. 58 There have also been other studies that have highlighted that vascular risk factors are more prevalent in certain racial groups such as Blacks compared with Whites and this greater prevalence in vascular risk factors contributes to the racial differences observed in WMH. 59 Another potential limitation of this study may be in the chosen index of vascular burden (i.e., the Framingham vascular risk score). For this index, anyone above the age of 75 years receives the same penalty points as those at 75 years. 26 However, there is evidence from a study by Pase et al. (2018) that, cross-sectionally, the strength of the association between vascular risk factor burden and brain volumes tends to show a progressive decline until it plateaus at age 75 years and over. 60 In their study, there were no significant differences in the strength of the association for those in the age ranges of 75–84 years and 85–94 years. Our sample had only 58 participants over the age of 75 years and based on these earlier findings we can conclude that it is highly unlikely that those over the age of 75 years might have had any significant differential profile in relation to the association between vascular burden and changes in WM integrity to a level that might have influenced the overall pattern of findings in our study. Our speculation is also supported by the essentially similar findings obtained when age was accounted for in our statistical models (main effects and interaction shown in Supplemental Table 10; additionally, effects of age on all white-matter diffusivity indices are reported in Supplemental Table 11).
To summarize, our findings from the interaction between APOE genotype and vascular burden show that the high-burden non-carriers followed by the high-burden ɛ4 carriers have the greatest risk of WM structural alterations, whereas the low burden ɛ4 carriers and non-carriers have a low risk. The impact of vascular pathology tends to show different asymmetry depending on the groups compared, such that when a high-risk group is compared with a low-risk group, a leftward asymmetry is observed, but this pattern is reversed when two high risk groups are compared and mostly rightward asymmetry is detected. This pattern of results is contrary to the findings by Minkova et al. 44 who found no asymmetries in AD. Overall the findings suggest that the preferential for the leftward asymmetry in the low-risk groups corresponds with the observations made by Thompson et al. 40 suggesting that vascular pathology tends to add on to the left hemisphere when vascular burden is low; however, a shift in pattern is underway from leftward to rightward asymmetry in the presence of high vascular burden. Direct testing for asymmetry, however, did not lead to any significant findings. This might reflect subthreshold differences in either hemispheres that do not emerge when they are directly compared. Given that these findings show a non-linear, non-monotonic pattern of diffusivity during disease progression, it appears that diffusivity indices such as FA and AxD change depending on the presence of biomarker positivity, APOE genotype and the influence of vascular comorbidity resulting in varying degree of chronic WM damage.
Supplemental Material
sj-docx-1-alz-10.1177_13872877251320660 - Supplemental material for Interactive effects of APOE ɛ4 status and vascular burden on white matter microstructural integrity in aging with and without neurocognitive decline
Supplemental material, sj-docx-1-alz-10.1177_13872877251320660 for Interactive effects of APOE ɛ4 status and vascular burden on white matter microstructural integrity in aging with and without neurocognitive decline by Srijan Konwar, Riccardo Manca, Matteo De Marco, Hilkka Soininen and Annalena Venneri in Journal of Alzheimer's Disease
Footnotes
Acknowledgments
The authors have no acknowledgments to report.
Author contributions
Srijan Konwar (Data curation; Formal analysis; Writing – original draft); Riccardo Manca (Formal analysis; Writing – review & editing); Matteo De Marco (Data curation; Writing – review & editing); Hilkka Soininen (Funding acquisition; Writing – review & editing); Annalena Venneri (Conceptualization; Data curation; Funding acquisition; Writing – review & editing).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The current study was supported through funds from the European Union Seventh Framework Programme (FP7/2007–2013) – under Grant Agreement no. 601055, to AV and HS. AV is supported by funding obtained under the National Recovery and Resilience Plan (NRRP), Mission 4 Component 2 Investment 1.3 - Call for tender No. 341 of 15/03/2022 of Italian Ministry of University and Research funded by the European Union – NextGenerationEU, Project code PE0000006, Concession Decree No. 1553 of 11/10/2022 adopted by the Italian Ministry of University and Research, CUP D93C22000930002, “A multiscale integrated approach to the study of the nervous system in health and disease” (MNESYS).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Data are available from the corresponding author on request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.