
Abstract
Background
High blood pressure has been associated with dementia prevalence and incident. However, it is unclear the relationship of office and ambulatory BP monitoring with cognitive function and dementia and in particular, it remains unknown whether ambulatory BP variability relates to dementia.
Objective
To investigate the associations of office and 24-h blood pressure (BP) with cognitive function and dementia prevalence.
Methods
Cross-sectional population-based study of 1435 participants aged ≥40 years with office BP/24-h BP, and cognitive assessments (Mini-Mental State Examination [MMSE] and Selective Reminding Test [SRT]). Dementia was diagnosed with a clinical dementia rating ≥1.0. Statistics included logistic and linear regression models.
Results
The mean age was 63.8 ± 10.3 years old and 995 (69.3%) were women. Out of the 1435 participants, 46 (3.20%) had dementia at baseline. Office and 24-h BP levels were not associated with dementia but with one SRT. Increasing 24-h systolic BP variability was associated with lower MMSE (adjusted mean, −0.08; 95% confidence interval [CI], −0.13, −0.03), and SRT (adjusted means ranged from −0.13 to −0.06; 95% CI ranging from −0.19 to −0.01) scores and 1.48-fold greater odds of dementia (95% CI, 1.09–2.02) regardless of BP level.
Conclusions
Elevated 24-h BP variability, not the BP level, seems to have a stronger association with lower cognitive function and dementia prevalence. Prospective studies are needed to address whether 24-h BP variability relates to cognitive decline and dementia incidence.
Keywords
Introduction
Dementia is the second major cause of disability-adjusted life-years and deaths in older adults worldwide, 1 with the number of people living with dementia growing at alarming rates due to the rapid aging of the population. 2 Dementia is characterized by a marked cognitive decline that compromises the social and occupational functioning of individuals, to the point where they lose independence in everyday activities. 3 Public health and scientific efforts aim to prevent and slow cognitive decline and identify individuals at high risk of developing dementia by studying modifiable risk factors. 4 The 2024 Lancet Commission identified 14 potential modifiable risk factors for dementia including high blood pressure (BP). 5 Data from population-based studies, meta-analyses, and clinical trials support controlling BP level to prevent cognitive decline and dementia.6–8 It is, therefore, important to understand different methods and metrics of BP measurements and how they contribute to cognitive functioning and dementia. Most evidence is based on BP taken at the office. There are recent studies indicating that out-of-office BP might also play an important role when investigating cognitive function and dementia.
Ambulatory BP monitoring is an out-of-office BP method that measures BP over a 24-h (24-h), quantifying variability among consecutive BP readings (known as short-term variability) and evaluates nocturnal BP dipping. Numerous studies have related abnormal nocturnal BP dipping with cognition and dementia 9 but few reported on short-term BP variability.10–13 Despite BP variability being an emerging risk factor for cognitive decline and dementia,14–18 it is unclear whether high 24-h BP variability relates to cognitive functioning independently of the BP level, and evidence on dementia remains undocumented in population-based studies. Therefore, we investigated the relationships of office and 24-h ambulatory BP monitoring indices, and the contribution of BP level and variability to cognitive function and dementia in a cohort of Latinos/Hispanics from the ongoing Venezuela Maracaibo Aging Study.
Methods
The Institutional Review Boards of the Cardiovascular Institute at the University of Zulia, Maracaibo, and Columbia University, New York, approved the Maracaibo Aging Study, which complied with the Helsinki Declaration for investigations into human subjects. Informed consent was obtained from each participant. We followed the Oxford Equator Network STROBE guidelines (https://www.equator-network.org/).
Study participants
The Maracaibo Aging Study is an ongoing prospective population-based study of 2915 community-dwelling participants aged >40 years, were recruited from the Santa Lucia and Santa Rosa neighborhoods, in Maracaibo, Zulia, Venezuela. 19 The baseline assessments of participants were conducted between 1998 and 2001 (Santa Lucia) and 2010 and 2015 (Santa Rosa). The primary aim of the Maracaibo Aging Study was to investigate age related diseases including neurological, psychiatric, and cardiovascular diseases. We selected a subset of participants who underwent cognitive function testing within one week of measurement, 24-h ambulatory BP monitoring, and met the criteria of having (i) more than 48 valid BP readings over a 24-h period (minimum number needed to maintain the prognostic information of BP variability), 20 and (ii) at least three nocturnal BP readings. 21 A total of 1435 individuals were selected for this study.
Assessment of blood pressure
Nurses or physicians measured office BP readings with a validated oscillometric device (Dynamap®). Seated office BP was the average of two BP readings in the Santa Lucia cohort or five consecutive readings in the Santa Rosa cohort after participants rested five minutes in a sitting position. The 24-h ambulatory BP monitoring was recorded with validated oscillometric automated devices (validated oscillometric 90202 or 90207 Spacelabs monitors). Readings were programmed at 15-min intervals during the day (from 06:00 to 23:00) and at 30-min intervals at night (23:00 to 06:00, Supplemental Table 1). The raw ambulatory BP readings of the individuals were processed with the same SAS macro. The within-subject 24-h systolic BP was time-weighted, giving weights to each individual reading proportional to the preceding time interval, to generate weighted mean, standard deviation, and average real variability (ARV) 24-h systolic BP values. Our analysis focused on the ARV as it is the only metric that captures variability among consecutive BP readings.22,23 The ARV index was calculated as the average of the absolute changes between consecutive BP readings, as follows:

Cognitive function and dementia prevalence
The assessment of cognitive function and dementia diagnostic procedures used in the Maracaibo Aging Study are described elsewhere.19,25 Cognitive measures included a global cognition score based on the Mini-Mental State Examination (MMSE) (score range 0–30), and three memory domains obtained from the Selective Reminding Test (SRT) to evaluate memory impairment 26 which included total recall, long-term retrieval, and delayed recall. The SRT total recall domain involved recording the number of words recalled from a twelve-word list during six trials (score range 0–72) and the SRT long-term retrieval domain involved recording the number of words recalled in two consecutive trials without being reminded (score range 0–72). The SRT delayed recall domain involved recording the number of words recalled 15 min after completing the test (score range 0–12). In the Supplemental Methods, we described in detail how dementia diagnosis was. During a consensus with our multidisciplinary team, a definitive clinical dementia rating (CDR) score was adjudicated for each participant. A CDR equal to or greater than 1 were identified as having dementia 27 (cognitive impairment resulting in a functional decline in their social or occupational activities).
Statistical analysis
Continuous data are presented as the mean and standard deviation for normally distributed variables and as the median (Q1–Q3) for nonnormally distributed variables. Categorical data are shown as frequencies (%). Baseline characteristics, and office and ambulatory BP measurements were reported for the whole study sample and compared between participants without and with dementia at baseline using Student's t test for normally distributed data and the Mann Whitney U test for nonnormally distributed data, or chi-square tests.
Linear regression models were performed to examine the associations of office and ambulatory BP measures with cognitive tests (MMSE and SRT). For dementia, we used logistic regression models to calculate the odds ratios (OR) for dementia associated with office and ambulatory BP measures. Linear and logistic regression models accounted for age, sex, years of education, body mass index, previous or current smoking status, alcohol consumption, use of antihypertensive medication, serum total cholesterol, diabetes mellitus, and previous history of cardiovascular diseases. These covariables were selected based on their biological relevance to cognitive function and dementia. When examining BP variability, models additionally accounted for the mean BP level. Because both the BP level and variability are correlated, 28 we tested for collinearity effects by calculating the variance inflation factor obtained from linear regression models. 29 A variance inflation factor less than 1.0 indicates that there is no collinearity, < 5 indicates moderate collinearity, and ≥5 indicates strong collinearity. For office, 24-h, daytime, and nighttime systolic BP, the associations were expressed per 10 mm Hg increase in systolic BP as it is a standard unit of expression utilized for BP level. Whereas, for night-to-day ratio and BP variability, the associations were expressed per +1 standard deviation.
To examine the contribution of the 24-h BP level and ARV to cognitive function and dementia prevalence, we performed two sets of analyses. First, we divided the study sample into participants with normal 24-h systolic BP (mean 24-h systolic BP below 125 mm Hg) and those with 24-h systolic hypertension (mean 24-h systolic BP ≥125 mm Hg). We then standardized cognitive tests for the covariables to plot the association between 24-h systolic BP ARV and cognitive function while accounting for the effects of the covariable. Linear associations were plotted where the x-axis was the 24-h systolic BP ARV, and the y-axis was the cognitive scores. The β-coefficients and p values are included in the linear graphics. We constructed heatmaps to visualize the contribution of 24-h systolic BP level and the ARV to dementia and cognitive function. We used logistic (for dementia), and linear (for cognitive tests) regression modeling to derive the probability of dementia or estimated cognitive function scores standardized to the average of the distributions in the whole study population for covariables. The exploratory analysis included the comparisons of baseline characteristics between included and excluded participants. We used SAS software, version 9.4, and maintenance level 5. Statistical significance was indicated by a two-tailed α-level of 0.05 or less.
Results
Baseline characteristics
Of the 1435 participants included in our study, 995 (69.3%) were women and the overall mean age was 63.8 years (Table 1). The percentages of individuals with a history of smoking or alcohol consumption were 19.9% and 36.2%; respectively. A total of 13.0% of the participants had diabetes mellitus, 84.7% and 54.6% had office and 24-h hypertension, respectively, 33.5% were receiving antihypertensive treatment, and 11.9% had a previous history of cardiovascular disease. Supplemental Table 2 shows the comparison of baseline characteristics between included excluded participants.
Baseline characteristics of the study sample.
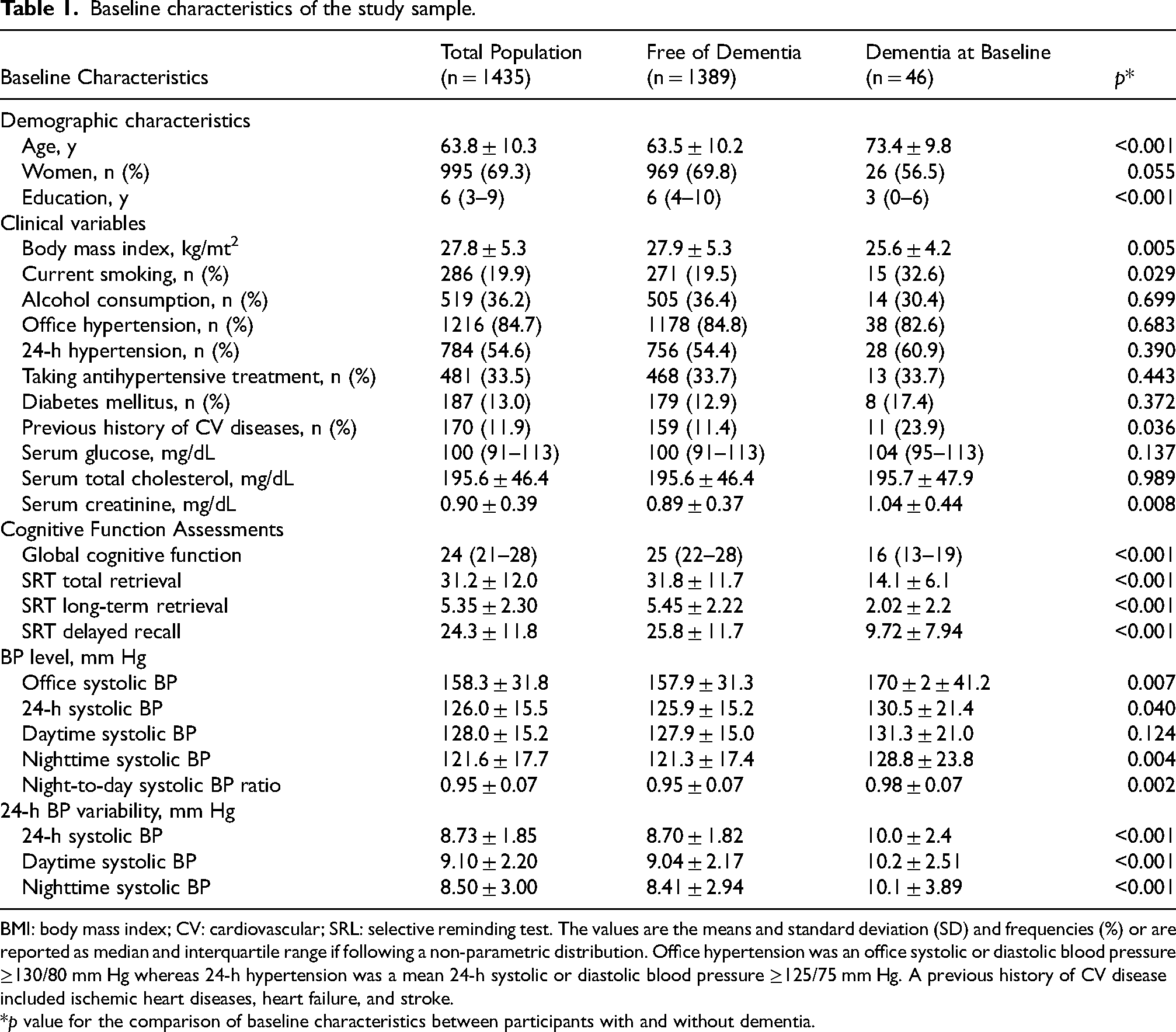
BMI: body mass index; CV: cardiovascular; SRL: selective reminding test. The values are the means and standard deviation (SD) and frequencies (%) or are reported as median and interquartile range if following a non-parametric distribution. Office hypertension was an office systolic or diastolic blood pressure ≥130/80 mm Hg whereas 24-h hypertension was a mean 24-h systolic or diastolic blood pressure ≥125/75 mm Hg. A previous history of CV disease included ischemic heart diseases, heart failure, and stroke.
*p value for the comparison of baseline characteristics between participants with and without dementia.
Associations of office and ambulatory BP with cognitive function
The median MMSE score (16 versus 25 points) and the mean SRT total retrieval (14.1 versus 31.8 points), long-term retrieval (2.02 versus 5.45 points), and delayed recall (9.72 versus 25.8 points) scores were lower in individuals with dementia at baseline than in those without dementia (Table 1). Each +10 mm Hg increase in office, 24-h, and daytime systolic BP level was associated with 0.07 (95% confidence interval [CI], 0.05 and 0.08; p < 0.001), 0.04 (95% CI, < 0.01 and 0.07; p = 0.027), and 0.05 (95% CI, 0.02–0.09; p = 0.005) higher SRT total retrieval scores, respectively (Table 2). A higher 24-h and daytime systolic BP ARV was related to lower scores in MMSE, SRT total retrieval, long-term retrieval, and delayed recall (Table 2); with estimates ranging from −0.13 (95% CI, −0.19 and −0.07; p < 0.001) to −0.06 (95% CI, −0.11 and −0.01; p = 0.041) per +1.85 mm Hg increase in 24-h systolic BP ARV, and from −0.10 (95% CI, −0.16 and −0.05; p < 0.001) to −0.06 (95% CI, −0.11 and −0.01; p = 0.045) per +2.19 mm Hg increase in daytime systolic BP ARV.
Adjusted linear regression analysis for the association of office and ambulatory blood pressure monitoring measures with cognitive function.
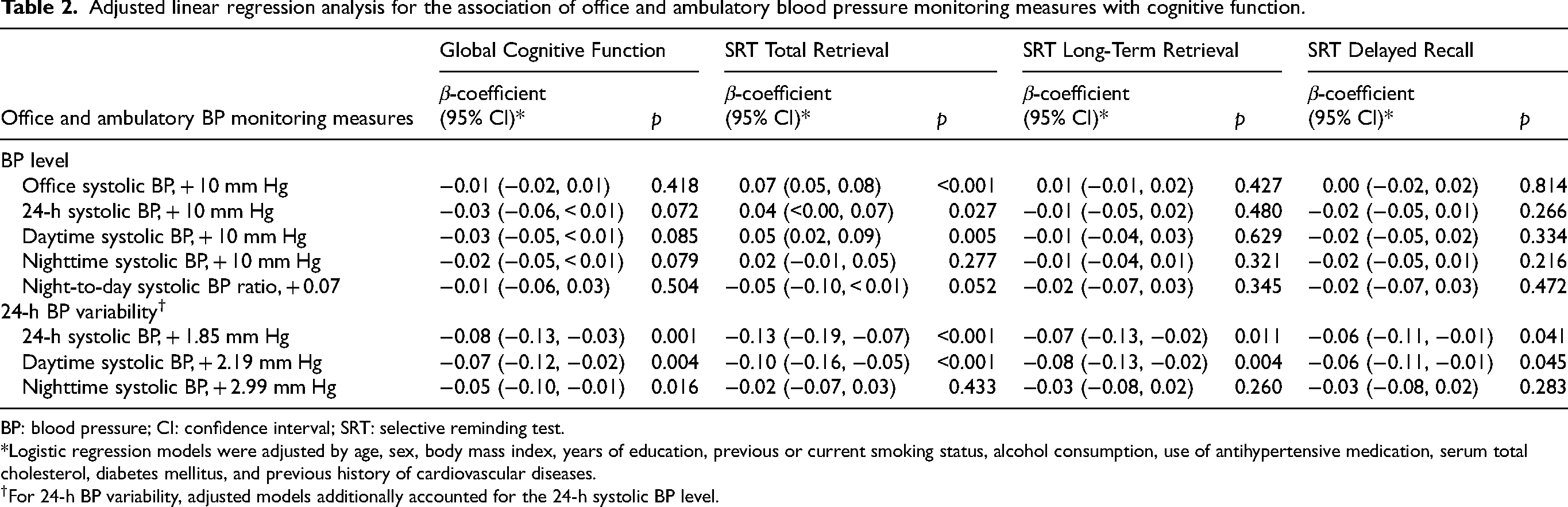
BP: blood pressure; CI: confidence interval; SRT: selective reminding test.
*Logistic regression models were adjusted by age, sex, body mass index, years of education, previous or current smoking status, alcohol consumption, use of antihypertensive medication, serum total cholesterol, diabetes mellitus, and previous history of cardiovascular diseases.
†For 24-h BP variability, adjusted models additionally accounted for the 24-h systolic BP level.
Associations of office and ambulatory BP with dementia
Participants with dementia at baseline had higher office BP, 24-h systolic BP and nighttime systolic BP level, night-to-day systolic BP, and 24-h, daytime, and nighttime systolic BP ARV than individuals without dementia (Table 1). According to the unadjusted analyses, except for the daytime systolic BP level, all office and ambulatory BP level measurements were associated with dementia at baseline (Table 3). Adjusted logistic regression models showed that measures of office and ambulatory BP levels were not related to dementia (P ≥ 0.076). A + 1.85 mm Hg increase in 24-h and a + 2.99 mm Hg increase in nighttime systolic BP ARV were associated with a 1.49-fold (95% CI, 1.10–2.03; p = 0.010) and 1.41-fold (95% CI, 1.07–1.90; p = 0.014) increase in dementia odds, respectively.
Logistic regression analysis of the association of office and ambulatory blood pressure monitoring measures with dementia at baseline.
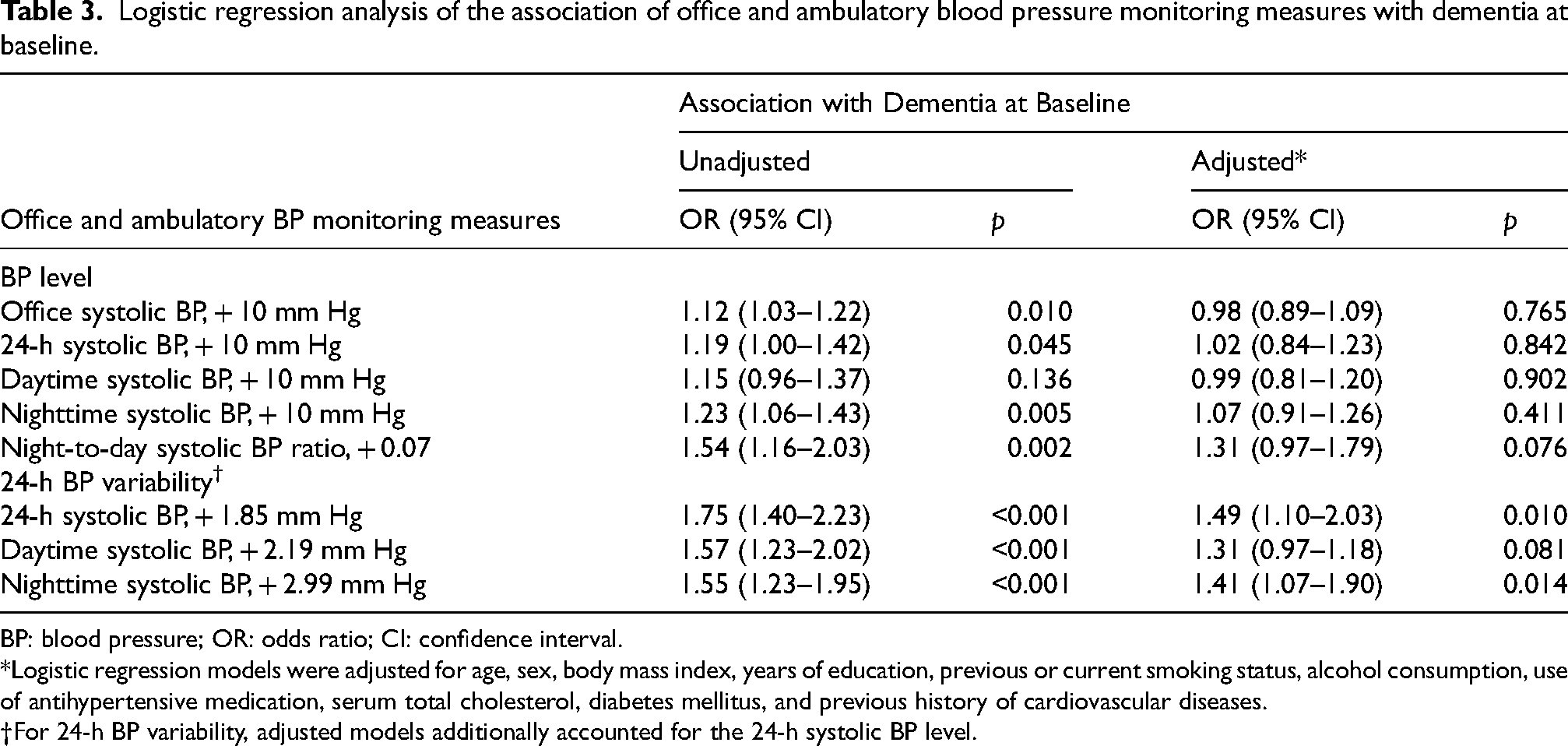
BP: blood pressure; OR: odds ratio; CI: confidence interval.
*Logistic regression models were adjusted for age, sex, body mass index, years of education, previous or current smoking status, alcohol consumption, use of antihypertensive medication, serum total cholesterol, diabetes mellitus, and previous history of cardiovascular diseases.
For 24-h BP variability, adjusted models additionally accounted for the 24-h systolic BP level.
Contribution of BP level and variability to cognition and dementia
In individuals with 24-h systolic normotension (n = 714; Figure 1), a higher 24-h systolic BP ARV was associated with lower scores in MMSE, SRT total retrieval, long-term retrieval, and delayed recall (p ≤ 0.025); the estimates per mm Hg increase in 24-h systolic BP ARV ranged from −0.611 to −0.178 points. Among individuals with 24-h systolic hypertension, each mm Hg increase in 24-h systolic BP ARV was associated with 0.712 lower points in the SRT total retrieval score. A higher 24-h systolic BP ARV was not associated with the MMSE, SRT long-term retrieval or delayed recall (p ≥ 0.070).
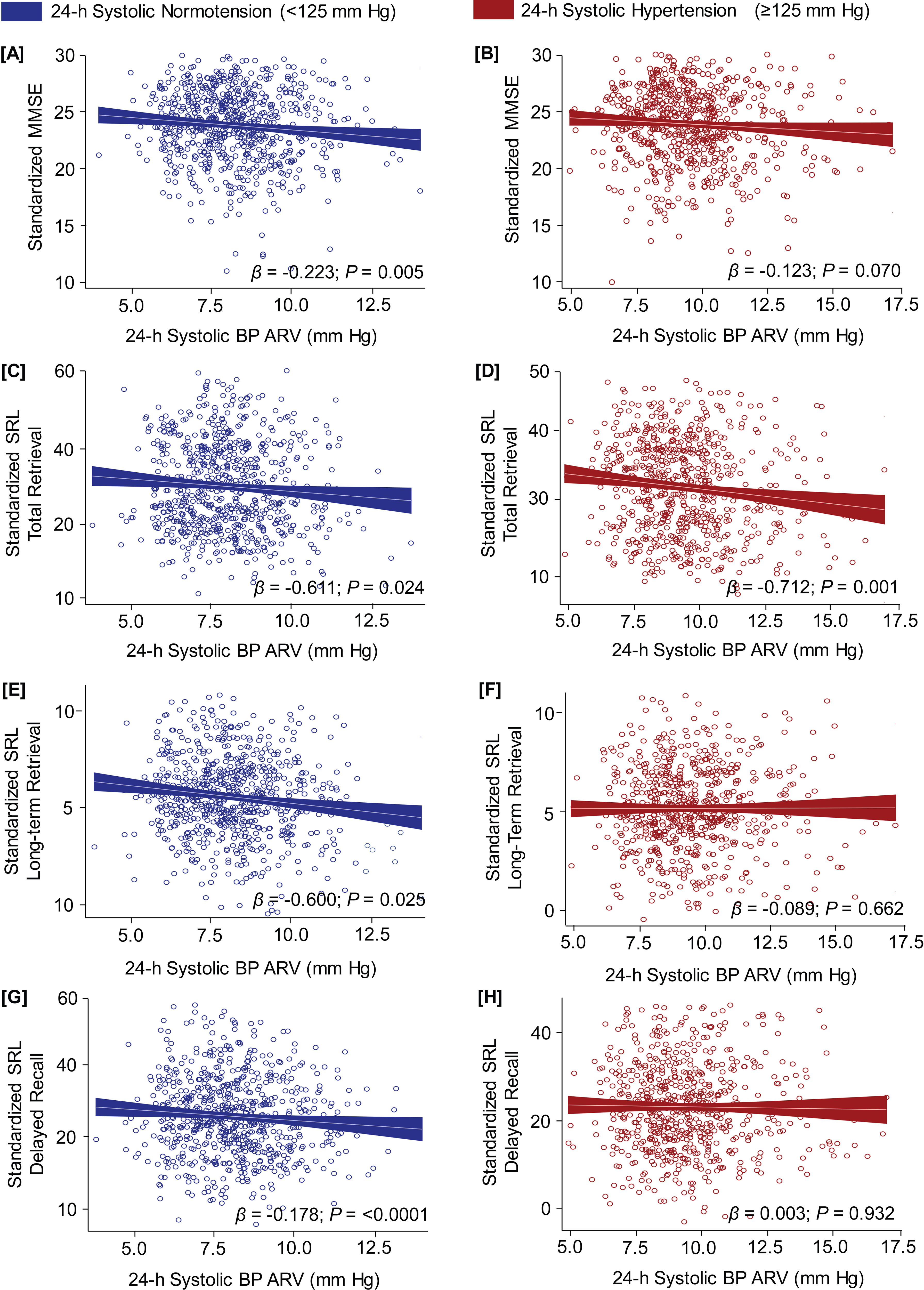
Associations of 24-h average real variability (ARV) systolic blood pressure with cognitive function. The cognitive scores were standardized for age, sex, body mass index, years of education, previous or current smoking status, alcohol consumption, use of antihypertensive medication, serum total cholesterol, diabetes mellitus, and previous history of cardiovascular diseases. Analyses were divided between individuals with 24-h systolic normotension (n = 741; A, C, E, and G) and those with hypertension (n = 694; B, D, F, and H).
The heatmaps in Figure 2 show the contributions of 24-h systolic BP ARV (y-axis) and level (x-axis) to dementia (Figure 2A) and cognition (Figure 2B-E). We observed that individuals with the lowest 24-h systolic BP level (110 mm Hg) and highest 24-h systolic BP ARV (12 mm Hg) had the highest probability of dementia (3.30% versus 0.45%) compared to individuals with the highest 24-h systolic BP (140 mm Hg) and lowest 24-h systolic BP ARV (6 mm Hg). MMSE and SRT delayed recall scores (Figure 2B, E) decreased with increasing 24-h systolic BP ARV (p < 0.001 and p = 0.027). A lower SRT total retrieval score was associated with higher 24-h systolic BP ARV (p < 0.001) and lower 24-h systolic BP level (p < 0.001, Figure 2C).
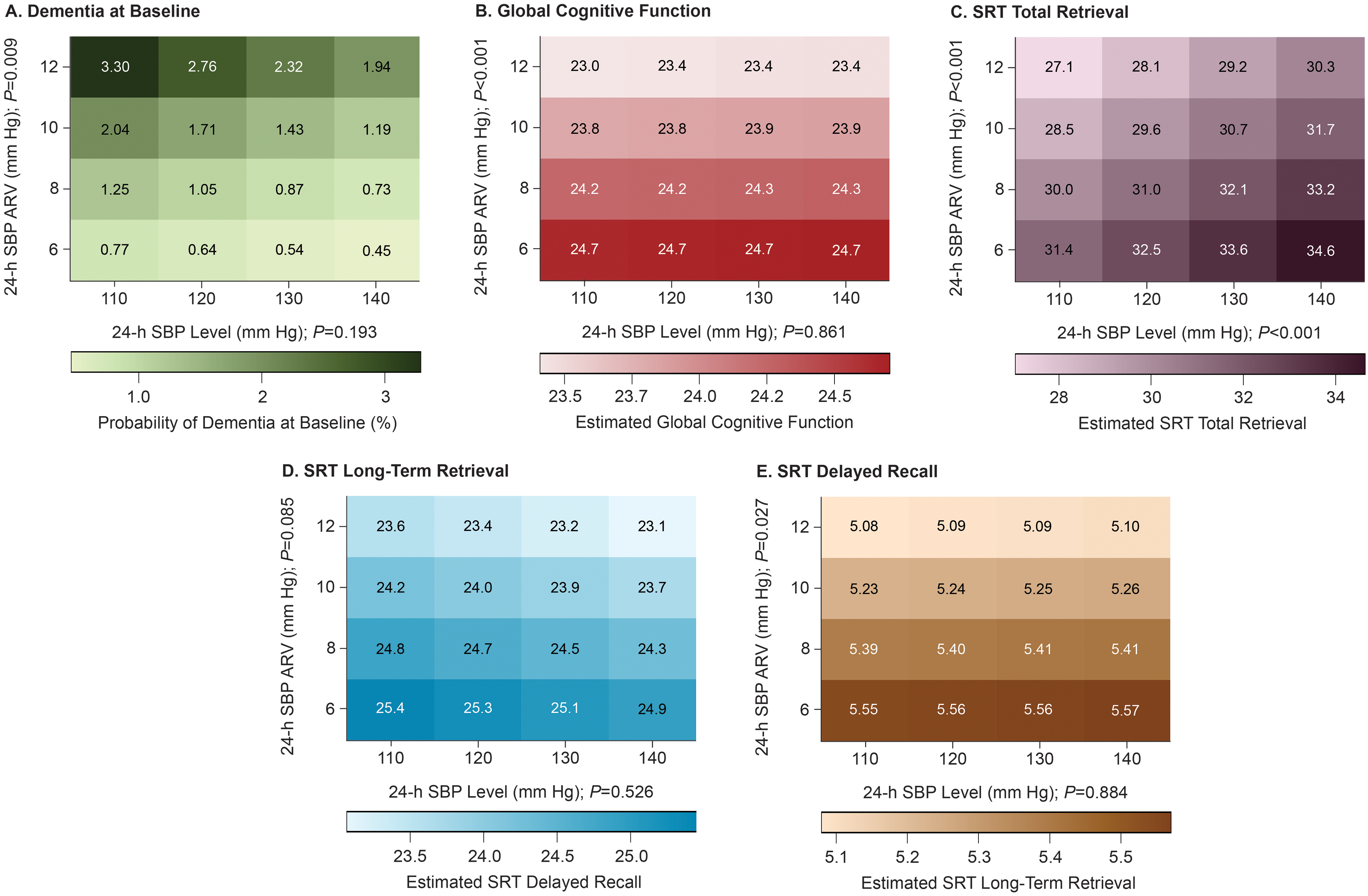
Contribution of 24-h systolic blood pressure (SBP) level and variability to cognitive function performance and probability of dementia at baseline. The numbers within the boxes indicate the probability of having dementia at baseline (A) or the estimated cognitive function scores (B-E). We used logistic (A) or linear (B-E) regression modeling to derive the probability of dementia or estimated cognitive function scores which were standardized to the average of the distributions in the whole study population for age, sex, body mass index, years of education, previous or current smoking status, alcohol consumption, use of antihypertensive medication, serum total cholesterol, diabetes mellitus, and previous history of cardiovascular diseases. The horizontal axis (24-h mean SBP level) is plotted against 24-h average real variability (ARV) in the vertical axis. SRT, selective reminding tests.
Discussion
In this population-based cohort of 1435 individuals aged ≥40 years old, we observed that high office or ambulatory BP levels were associated with one of the SRT domains and were not associated with dementia prevalence. In contrast, approximately every +2 mm Hg increase in ambulatory BP variability was associated with −0.13 to −0.06 lower scores on cognitive function tests and 1.48 and 1.35 higher odds for dementia at baseline. Heatmaps demonstrated that at baseline, individuals with the lowest 24-h systolic BP level, but with the highest variability had the lowest cognitive scores and highest probability of having dementia at baseline compared to individuals with the highest 24-h systolic BP level and lowest variability.
We observed that high office and ambulatory BP levels were associated with higher SRT total retrieval scores, which has also been reported in previous studies. The direction of this associations is not the only one as a systemic review of 68 studies revealed that the associations between BP and cognitive function has a negative (that is, a high BP level is related to lower cognitive function), positive (a high BP level is related to lower cognition), and U-shaped (both high and low BP levels are related to lower cognition). 30 Without solid evidence from clinical trials evaluating the benefits of high BP, especially in older adults, the association between high BP level and cognitive impairment should be interpreted with caution. Until then, treatment of BP should aim at office and ambulatory normotension to reduce the risk of the development of dementia or related disorders.31,32
BP variability is an emerging risk factor associated with cognitive decline and dementia, but most evidence is based on long-term BP variability.14,33 Our study provides novel findings showing that greater 24-h BP variability associates with cognitive function and dementia independently of the mean BP level. In light of the epidemiological data supporting BP variability as an emerging risk factor,14,15,17 there is enough evidence to highlight the importance of further investigating the associations of BP variability with cognitive and neurological outcomes. By using 24-h ambulatory BP monitoring, future studies could assess BP variability among consecutive BP readings (short-term variability) and abnormal circadian rhythms. To facilitate the interpretation of elevated BP variability, operative thresholds to define normal and high BP variability need to be established for guiding treating options to stabilize BP variability.
The relative contributions of both BP level and variability to cognitive function and dementia are not well understood. When we cross-referenced both metrics, lower 24-h BP levels with higher 24-h BP variability had the highest dementia prevalence and lowest cognitive function. This result suggested that individuals with normal 24-h BP level and with high systolic BP variability are more likely to have frequent and severe episodes of low BP, than are those with either low BP variability or with high BP level (Figure 2). These findings could help in understanding one of the two potential mechanisms linking high BP variability with cognitive decline and dementia, that is, cerebral hypoperfusion.16,33–35 Under physiological conditions, brain circulation ensures the maintenance of blood supply and flow to the brain tissue across a range of physiological BP levels. 36 However, excessive BP variability could result in extreme episodes of low BP, exposing cerebral autoregulation to operate outside a physiological BP level range. This can lead to hypotensive-related damage in the brain tissue and microcirculation, which might have a greater impact on individuals with cognitive impairment or dementia experiencing impaired cerebral autoregulation.16,37 The neurological clinical consequence of orthostatic hypotension supports such a mechanism. 38
Whether BP variability precedes or reflects the prodromal symptoms of dementia is still unclear. Studies have reported that high BP variability is related to cognitive decline and dementia incidence;6,17 however, reverse causation is also a potential hypothesis. 16 It has been reported that neurodegeneration in brain regions involved in autonomic control might correlate with changes in BP 39 and that baroreceptor sensitivity is reduced in Alzheimer's disease. 40 In both cases, current evidence indicates that BP dysregulation could reflect impairment of autonomic function. Therefore, 24-h BP data could help underlaying BP variability as a proxy for impaired autoregulation in individuals with cognitive impairment and dementia. This method allows the study of the circadian BP rhythms, which is a marker of autonomic function.41,42
Limitations and strengths
Our study should be interpreted within the context of its limitations. First, we did not include follow-up data on cognitive function or dementia incidence which limits the interpretation of 24-h BP variability as a risk factor for cognitive decline and dementia. Second, the number of BP readings necessary to maintain the prognostic value of 24-h BP variability should be at least 48 readings over 24-h. 20 Obtaining this number of readings and/or performing 24-h ambulatory BP monitoring is challenging among individuals with advanced dementia. Third, although 24-h BP variability was associated with cognitive function in our cohort, interpretation of the association of 24-h BP variability with dementia should be cautious due to the relatively low number of individuals with dementia at prevalence. Notwithstanding these limitations, our study has several strengths such as (i) the inclusion of Latinos/Hispanics, a population that is disproportionately affected by both high BP and dementia-related disorders; (ii) the extensive and in-depth assessment of cognitive function; and (iii) the multidisciplinary team of social workers, psychologists, and physicians who adjudicated dementia through consensus.
Conclusions
High BP seems to relate with better cognitive function whereas high 24-h BP variability associates with lower cognitive function and higher prevalence of dementia at baseline. Individuals with low BP level but high BP variability seem to have the poorest cognitive function and the greater odds for dementia prevalence. Our findings need further replication in prospective studies. Our results add novel data to the cumulative evidence supporting high BP variability as a potential emerging risk factor for cognitive decline and dementia.
Supplemental Material
sj-docx-1-alz-10.1177_13872877251322400 - Supplemental material for Baseline associations of office and ambulatory blood pressure monitoring with cognitive function and dementia prevalence
Supplemental material, sj-docx-1-alz-10.1177_13872877251322400 for Baseline associations of office and ambulatory blood pressure monitoring with cognitive function and dementia prevalence by Jesus D Melgarejo, Dhrumil Patil, Sokratis Charisis, Kristina P Vatcheva, Silvia Mejia-Arango, Luis J Mena, Claudia L Satizabal, Ciro Gaona, Egle Silva, Eron Manusov, Joseph H Lee, Joseph D Terwilliger, Jose Gutierrez, Sudha Seshadri and Gladys E Maestre in Journal of Alzheimer's Disease
Footnotes
Acknowledgments
The authors thank the participants and assessment team of the MAS in both Santa Lucía and Santa Rosa.
ORCID iDs
Ethical considerations
The Institutional Review Boards of the Cardiovascular Institute at the University of Zulia, Maracaibo, and Columbia University, New York, approved the Maracaibo Aging Study, which complied with the Helsinki Declaration for investigations into human subjects. We followed the Oxford Equator Network STROBE guidelines (![]() ).
).
Consent to participate
All human subjects provided informed consent and agreed to participate in the Maracaibo Aging Study.
Author contributions
Jesus David Melgarejo (Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Validation; Visualization; Writing—original draft; Writing—review & editing); Dhrumil Patil (Formal analysis; Investigation; Methodology; Writing—original draft; Writing—review & editing); Sokratis Charisis (Investigation; Writing—original draft; Writing—review & editing); Kristina Vatcheva (Data curation; Formal analysis; Investigation; Methodology; Validation; Writing—original draft); Silvia Mejia-Arango (Data curation; Formal analysis; Investigation; Methodology; Validation; Writing—original draft); Luis J Mena (Data curation; Formal analysis; Methodology; Supervision; Validation; Writing—original draft); Claudia Satizabal (Formal analysis; Investigation; Writing—original draft); Ciro Gaona (Conceptualization; Data curation; Resources; Supervision; Validation; Writing—original draft); Egle Silvia (Conceptualization; Data curation; Resources; Validation); Eron Manusov (Investigation; Resources; Supervision; Validation; Writing—original draft); Joseph Lee (Conceptualization; Formal analysis; Funding acquisition; Investigation; Methodology; Project administration; Resources; Supervision; Validation); Joseph Terwilliger (Conceptualization; Data curation; Funding acquisition; Investigation; Methodology; Project administration; Resources; Supervision; Validation); Jose Gutierrez (Data curation; Formal analysis; Investigation; Supervision; Writing—original draft); Sudha Seshadri (Formal analysis; Investigation; Methodology; Supervision; Validation; Writing—original draft); Gladys E Maestre (Conceptualization; Funding acquisition; Investigation; Methodology; Project administration; Resources; Software; Supervision; Validation; Writing—original draft; Writing—review & editing).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute on Aging of the National Institutes of Health under Awards Number R01AG036469, R03AG054186, DP1AG069870, P30AG059305, and P30AG066546. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Text from authors
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.