
Abstract
Midlife hypertension increases risk for dementia. Around one third of adults have diagnosed hypertension; however, many adults are undiagnosed, or remain hypertensive despite diagnosis or treatment. Since blood pressure (BP) follows a circadian rhythm, ambulatory BP monitoring allows for the assessment of BP over a 24-hour period and provides an important tool for improving the diagnosis and management of hypertension. The measurement of 24-hour BP profiles, especially nocturnal BP, demonstrate better predictive ability for cardiovascular disease and mortality than office measurement. However, few studies have examined 24-hour BP profiles with respect to dementia risk. This is an important topic since improvements in BP management could facilitate the primary prevention of vascular cognitive impairment and dementia. Therefore, this review discusses the evidence linking BP to dementia, with a focus on whether the implementation of 24-hour BP measurements can improve risk prediction and prevention strategies. Pathways linking nocturnal BP to dementia are also discussed as are risk reduction strategies. Overall, limited research suggests an association between 24-hour BP elevation and poorer cognition, cerebral small vessel disease, and dementia. However, most studies were cross-sectional. Further evidence is needed to substantiate 24-hour BP profiles, over and above office BP, as predictors of vascular cognitive impairment and incident dementia.
INTRODUCTION
Worldwide, an estimated 1.3 billion people aged 30–79 years (approximately one third) have diagnosed hypertension [1]. Hypertension remains an important public health concern for major cardiovascular disease and mortality [2]. Midlife hypertension is also a known dementia risk factor [3]. The number of individuals with dementia is expected to almost triple from 57.4 million in 2019 to 152.8 million by 2050 [4]. Management of hypertension in midlife represents a potential modifiable risk factor for dementia prevention. However, there remains a gap in both the detection and control of hypertension. Globally, 41–51% of adults remain undiagnosed and while 35–51% of hypertensive individuals receive treatment, less than half of those treated achieve hypertension control [1]. Considering global trends in population aging, better understanding of blood pressure (BP) management as a potential and meaningful protective factor in brain health is thereforecritical.
BP is most typically measured during the day, in a clinical setting using a brachial cuff. Measurement of BP in this manner is known as office BP. Basing clinical decisions on office BP assumes that the obtained BP reading is representative of a patient’s habitual BP levels. However, BP is not static, it is highly dynamic and can change rapidly in response to environmental and physiological demands. Moreover, BP exhibits a strong circadian (24 h) rhythm. Ambulatory BP monitoring allows the assessment of BP over the course of the day and night and provides an important tool for improving the diagnosis and management of hypertension [5]. Despite these advantages, the value of 24-h BP monitoring in the management of hypertension and risk prevention of dementia remains unclear. There is growing evidence that 24-h BP measures are associated with cognitive impairment and dementia [3] and are more strongly related to vascular brain injury compared to office BP [6–15]. Therefore, this review discusses the evidence linking BP to dementia, with a focus on whether the implementation of 24-h BP measurements can improve risk prediction and prevention strategies. For context, we first provide a brief review of the relationship between hypertension and risk of dementia, possible mechanisms involved and effect of treatment. With this background, we then outline the literature on circadian variation in BP and the links between 24-h BP and dementia risk. Finally, the review discusses the potential benefit of screening and targeted treatment of 24-h BP to improve brain health.
HYPERTENSION AND DEMENTIA
Incidence of dementia in hypertensive individuals
Dementia has a long preclinical phase, with Alzheimer’s disease (AD) patients exhibiting neuropathological changes decades prior to the onset of clinical impairment [16]. Similarly, hypertension can cause the insidious accumulation of cerebral small vessel disease [17]. Therefore, longitudinal and retrospective cohort studies are well suited to examining the relationship between BP and the incidence of dementia due to the likely length of time between occurrence of hypertension and onset of dementia. There is a consistent association between midlife hypertension and AD dementia or all-cause dementia reported in meta-analyses of longitudinal studies [18–21], where risk increased by 20-75% with history of midlife hypertension (Fig. 1). Studies differ in BP cut-offs used (i.e., systolic BP > 140 or > 160). There is evidence to suggest that risk of dementia increases linearly with systolic BP values over 130 [18]. Meta-analytic results with systolic cut-offs are noted in Fig. 1. Cohort studies considering multiple midlife vascular risk factors in addition to elevated BP, such as hypercholesterolemia and diabetes, demonstrate that the risk of dementia is greater for individuals with multiple vascular risk factors as compared to just hypertension [22–26].
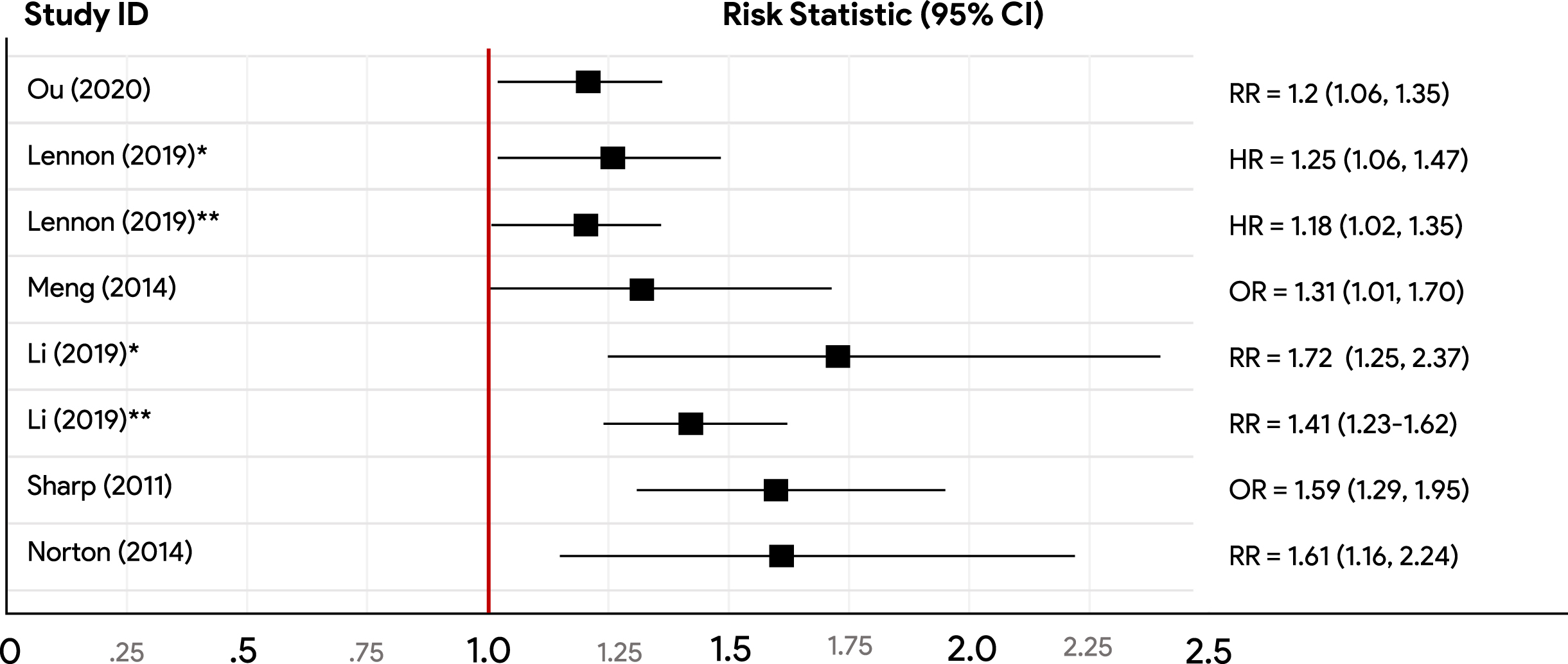
A summary of meta-analytic findings on midlife hypertension and dementia risk. Some studies appeared in multiple meta-analyses. Risk statistics reported include hazard ratio (HR), odds ratio (OR), or risk ratio (RR). *Systolic blood pressure≥160 mmHg, **systolic blood pressure = 140-160mmHg, all else systolic blood pressure≥140 mmHg. Lennon (2019) and Norton (2014), Alzheimer’s disease dementia; Sharp (2011), Vascular dementia; all else all cause dementia.
Trajectory of mid to late life hypertension
Whilst there is a demonstrated positive association between midlife hypertension and dementia incidence, the association between late-life hypertension and dementia has been mixed [18, 28]. It is possible that the trajectory of BP from mid to late life explains these mixed findings with two longitudinal studies demonstrating increased risk of dementia for participants with specific BP change patterns from mid to late life [29, 30]. Predominately, sustained hypertension from mid to late life and a steep decline in BP to late life hypotension were associated with increased risk of dementia compared to mid to late life normotensives [29, 30]. Sustained hypertension from mid to late life has also been associated with greater total brain and grey matter atrophy and subsequent impaired cognitive functioning [31], as well as smaller brain volumes in regions affected in early AD [32].
POTENTIAL MECHANISMS
There are many possible mechanisms that may explain the association between hypertension and dementia. An exhaustive consideration of all mechanisms is beyond the scope of this review. Here we focus on AD pathology, small vessel disease, impaired cerebral blood flow and promotion of oxidative stress and neuroinflammation (Fig. 2). These mechanisms commonly intersect through cerebral hypoperfusion, vascular brain injury (e.g., cerebral microbleeds), impaired autoregulation, blood-brain barrier disruption, and inflammatory pathways. Hypertension is often accompanied by several common comorbidities meaning that hypertension likely affects the development and progression of dementia in conjunction with other vascular risk factors. For example, hypertension increases risk of atrial fibrillation, heart failure, chronic kidney disease, diabetes, and carotid artery stenosis [33–35]. Further, repeated alcohol consumption, diabetes, and chronic kidney disease are also shown to promote hypertension [36–38]. Therefore, hypertension presents as one component of the relationship between cardiovascular health and dementia.
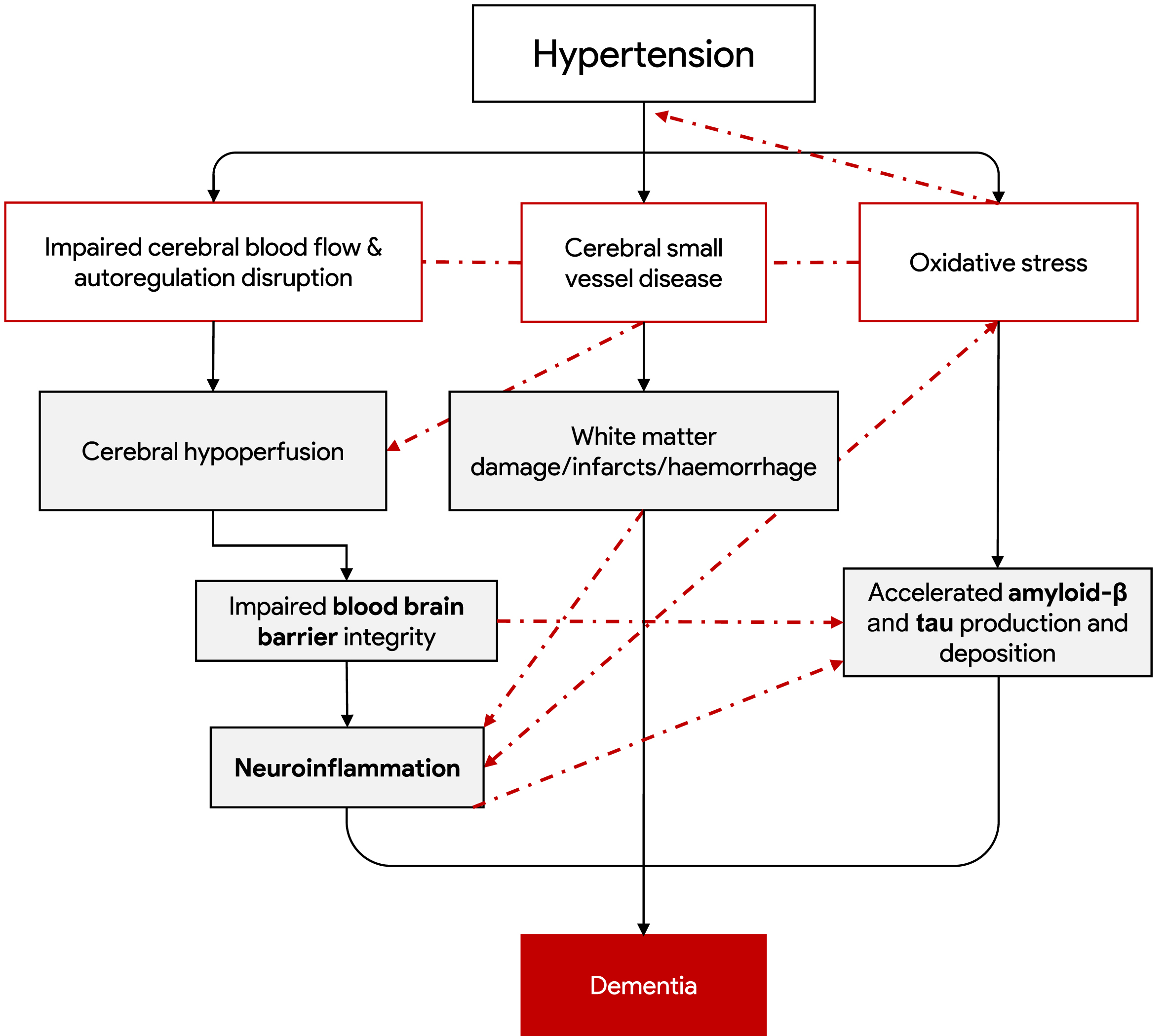
Key potential mechanisms of the hypertension to dementia relationship. Sustained hypertension can directly promote changes to cerebral blood flow, small vessel disease and oxidative stress (white boxes). These changes promote cerebral hypoperfusion and white matter damage, infarcts and haemorrhage (grey boxes). These elements promote key drivers of dementia (white boxes below hypertension) which have multiple causes in addition to factors induced by hypertension, not pictured. The dashed lines represent some of the interconnected relationships between factors that can further accelerate damage.
Alzheimer’s disease pathology
Midlife hypertension may contribute to the development of AD pathology. In mice models, induced hypertension associates with increases in cerebral vascular amyloid deposits, amyloid plaque load and phosphorylated tau levels [39–42] as well as dysregulated hippocampal gene expression involved in AD [43]. In humans, autopsy research demonstrated that the brains of individuals who had a history of midlife hypertension had increased AD pathology compared to normotensive individuals, including a higher number of neurofibrillary tangles [44] and amyloid plaques [44–46]. Emerging in vivo research indicates that midlife [47] and late life hypertension [48] are associated with higher CSF pTau181. However, there are conflicting findings for the relationship between BP andin vivo markers of amyloid-β measured with positron emission tomography (PET) [49–54].
Small vessel disease
Cerebral small vessel disease refers to chronic pathological conditions that damage arterioles and capillaries in the brain and result in microinfarcts, microhemorrhages, and white matter damage including axonal loss and demyelination [55]. Imaging markers include white matter hyperintensities, lacunes, microbleeds, and enlarged perivascular space. Cerebral small vessel disease is a well-established consequence of hypertension [56, 57] and is manifested by reduced cerebral blood flow, blood-brain barrier disruption, inflammation, secondary neurodegeneration, myelin damage, and brain injury itself [58, 59]. Small vessel disease increases risk of dementia [60–62]. For example, in hypertensive individuals demonstrating marked progression of periventricular white matter hyperintensities, risk of incident dementia was 6.2 times greater than those without white matter hyperintensity progression (95% CI 1.5–25.4) [62]. Small vessel disease may also relate to dementia through contributing to the pathogenesis of AD, where it has been demonstrated that white matter hyperintensities and cerebral microbleeds negatively correlate to CSF amyloid, and positively correlate to cortical amyloid, neurofibrillary tangles, and cortical atrophy in the majority of studies, although limited longitudinal research is available [59].
Cerebral blood flow
Due to the hemodynamic stress, chronic hypertension can lead to vascular wall remodeling and consequent stiffening and narrowing of arterioles [63–67]. These changes can result in reduced cerebral blood flow and cerebral hypoperfusion [68]. Cerebral blood flow autoregulation is a homeostatic mechanism that acts to maintain consistent perfusion pressure despite changes in arterial BP. In chronically elevated BP and subsequent vascular remodeling, the autoregulation curve is shifted to the right, meaning that the blood vessels require a higher BP to maintain the same level of blood flow to the brain [63]. Individuals with a history of hypertension therefore may also be more susceptible to hypoperfusion in periods of low or normal BP. Chronic hypoperfusion is also closely linked to impaired blood-brain barrier integrity [69] which subsequently promotes neuroinflammation processes and allows permeability of plasma proteins (including amyloid-β) [70–72]. Additionally, research utilizing mice models have also demonstrated cerebral hypoperfusion as accelerating amyloid-β production and accumulation [73–78].
Oxidative stress and inflammation
There is a large body of evidence that reports oxidative damage early in the course of AD [79]. Oxidative stress causes an alteration of BACE1, an enzyme involved in the β-secretase cleavage of the amyloid-β protein precursor, resulting in an accumulation of amyloid-β, which in turn promotes further oxidative stress [80]. Hypertension reduces antioxidant capacity and increases concentrations of reactive oxygen species [81], which results in both neuroinflammation and cell death [82, 83]. Neuroinflammation is a key pathological feature of AD and other neurodegenerative diseases [84, 85]. In animal models, hypertension can trigger adverse glial activation and neuroinflammation, followed by increased amyloid-β deposition and tau levels [39, 40]. Taken together, both oxidative stress and neuroinflammation arising from exposure to high pressure can have detrimental impact to brain tissue and formation of plaques. Oxidative stress may also exhibit a bidirectional relationship with hypertension as vascular oxidative stress is shown to also precede hypertension onset [86].
BLOOD PRESSURE LOWERING TO PREVENT DEMENTIA
There have been several meta-analyses that have demonstrated treatment of elevated office BP with anti-hypertensive medication as reducing dementia risk. In a meta-analysis of 14 randomized control trials (n = 96,158), individuals with lowered BP through anti-hypertensives, had a slightly lower risk of dementia or cognitive impairment (OR = 0.93, 95% CI 0.88-0.98) and cognitive decline (OR = 0.93, 95% CI, 0.88-0.99) compared to controls either receiving placebo (10 studies), an alternative antihypertensive agent (1 study), or higher BP targets (3 studies) [87]. Recent additional analyses of randomized controlled trials (RCTs) [88] and observational studies [89] demonstrate a 12-16% reduced risk of all cause dementia or AD dementia from anti-hypertensive use compared to non-use [89]. The effect sizes of anti-hypertensive treatment on dementia are small across studies and while there is good emerging evidence to support their use, most RCTs naturally have a short follow-up duration and therefore the efficacy of BP lowering specifically in midlife in reducing late life dementia or AD is not determined.
Alzheimer’s disease pathology
Lowering BP through anti-hypertensive medication may also limit AD neuropathology and slow progression of mild cognitive impairment. In a recent autopsy study, individuals with a history of anti-hypertensive medication use were compared to those with hypertension who were unmedicated [90]. While there was no difference in the number of amyloid-β and tau proteins, there was a reduction in spread of these proteins across the brain in those with a history of anti-hypertensive use. For example, medicated individuals had a 7.4 times greater chance of being in the less severe amyloid-β group as opposed to the most severe group than someone who was not medicated for hypertension. In an additional postmortem study, individuals who used anti-hypertensive medication had significantly lower mean neuritic plaques and neurofibrillary tangles, compared to unmedicated hypertensive individuals and even lower levels compared to those without history of hypertension [91]. Several studies suggest the possibility that anti-hypertensives that either act on the renin angiotensin system [92, 93] or reduce neuroinflammation [84] may serve neuroprotective effects [84, 93]. However, as meta-analytical results report no differences by class of medication in risk of dementia [89, 94], managing elevated BP may be more important than any specific anti-hypertensive medication use.
HYPERTENSION AND DEMENTIA CONCLUSIONS
There is strong epidemiological evidence to suggest hypertension in midlife relates to an increased risk of dementia. Therefore, management of hypertension is currently purported as a modifiable strategy for dementia prevention [3]. While there is good public awareness of hypertension as a major health risk factor, there are still a substantial number of individuals that remain undiagnosed, untreated, or with persistent hypertension despite treatment [1]. One potential opportunity for improvement in the way hypertension is detected, managed, and researched is 24-h BP monitoring.
BLOOD PRESSURE OVER 24 HOURS
Research on the relationship between BP and dementia largely ignores that BP follows a 24-h circadian rhythm (see Fig. 3) [95]. During the first half of nocturnal sleep, systolic BP (and to a lesser extent diastolic BP) falls 10-20% compared to daytime BP. This is followed by a slow rise during late sleep eventually leading to a morning surge where BP peaks upon awakening. BP falls mildly during the afternoon and rises mildly before sleep. 24-h BP changes are measured and quantified in a variety of ways including: dippers/non-dippers (i.e., nocturnal BP fall/non-fall), average day and night BP, BP variability ratio (24-h systolic BP standard deviation (SD) over diastolic SD), and coefficient of variation. There are four distinct patterns in nocturnal BP variation: an extreme dipper demonstrated a decline in BP by > 20%; a dipper, between 10 and 20% reduction; non-dipper < 10% reduction, and riser or reverse dipper, where BP increases during sleep [96]. However, these cut-off values are arbitrary [97].
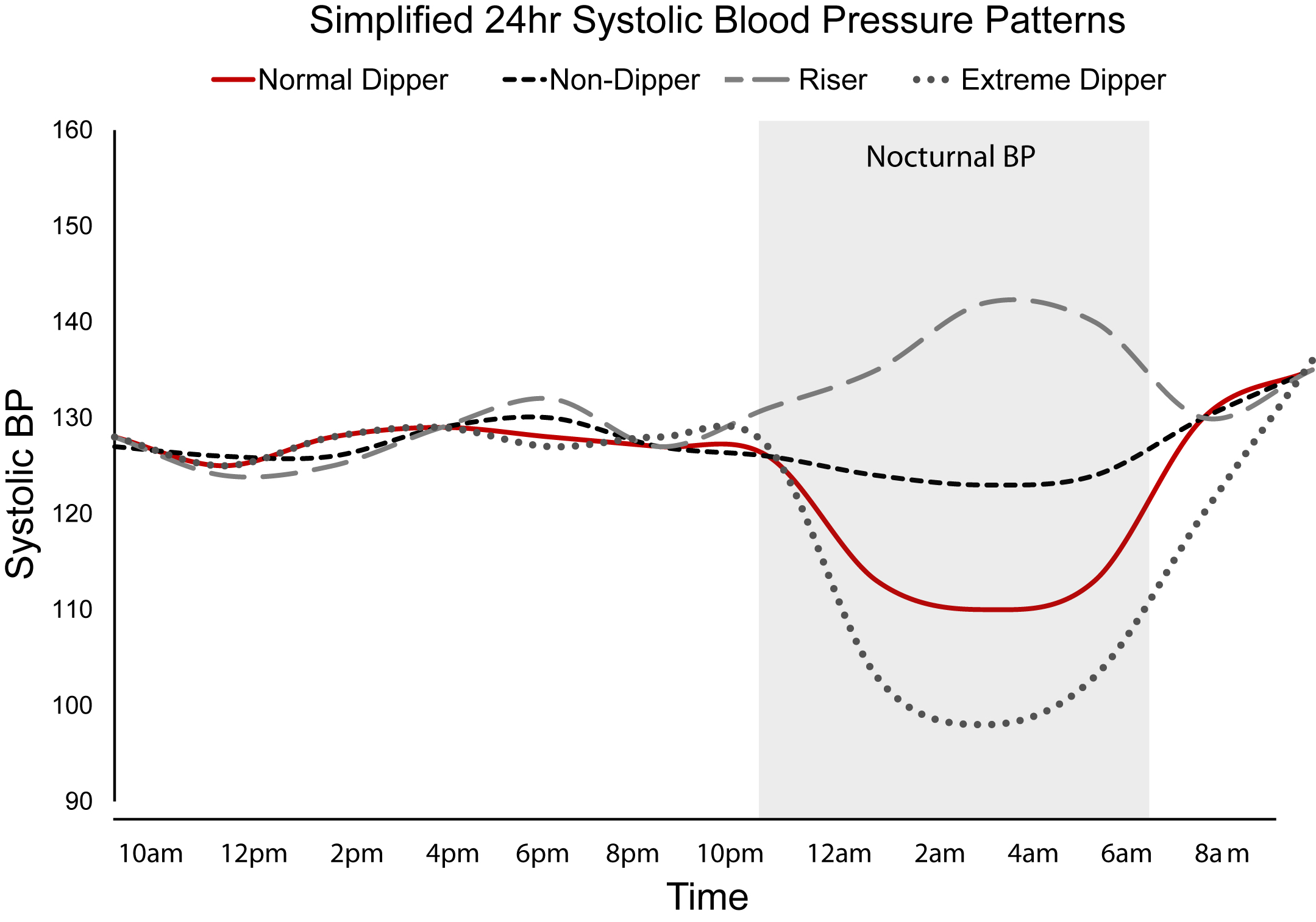
Simplified 24 h systolic blood pressure patterns. A simplified demonstration of four key systolic blood pressure patterns over a 24 h period. The duration of nocturnal BP (i.e., when the individual is asleep) is highlighted in the light grey box. From top to bottom, the lines within the grey box represent the following: rising blood pressure (grey dashed line), non-dipping blood pressure (black dashed line), normal dipping blood pressure (solid red line), and extreme differs (dark grey dashed line).
Measuring BP over 24 h can identify masked hypertension, where individuals present with a normal in office BP but an elevated out of office BP [98]. Individuals with masked hypertension may make up around 10% of the general population and are not identified by routine clinical examination yet still present with adverse lifetime effects of hypertension [98]. Of note, in a study of nearly 6,000 individuals not using anti-hypertensives, one in six had elevated office BP, yet one in three had elevated 24-h, daytime, or nocturnal average BP [99]. Further, in hypertensive individuals (n = 42,947), 41% of those untreated were found to have non-dipping BP and 53% who were treated with anti-hypertensive medication had non-dipping BP [100]. Measuring out of office 24-h BP can therefore identify hypertensive individuals unable to be detected during standard office BP assessments.
Why blood pressure changes over 24 hours
The circadian regulation of BP occurs through neurohormonal factors, vascular tone, the autonomic nervous system (ANS), and the renal system [95]. Vagal parasympathetic activity dominates during sleep and sympathetic nervous system activity dominates during wakefulness [95]. BP dipping occurs during the shift from sympathetic to parasympathetic activity. It is believed that autonomic dysfunction, via sympathetic overactivity primarily underlies non-dipping patterns [101–105]. Impaired ANS activity at age 65 (especially lower sympathetic tone) measured by 24-h heart rate variability, has also demonstrated to precede shifting to non-dipping status two years later [106]. Sleep disruption including obstructive sleep apnea (OSA), short sleep, insomnia, and poor sleep quality are associated with non-dipping BP patterns [107–110], as well as cognitive impairment and dementia [111–113]. These sleep pathologies are associated with increased sympathetic activity [114–117] which is known to be involved in the development of hypertension [118].
24-hour blood pressure, cerebrovascular and cardiovascular outcomes
24-h BP compared to office BP suggest better predictive ability for cardiovascular events, and all-cause, cardiovascular, and stroke mortality [6–15], and night-time BP as superior to daytime measures in predicting outcomes [6, 119]. Those who do not demonstrate nocturnal BP fall, non-dippers, risers, and also extreme dippers, experience greater cardiovascular risk and target organ damage compared to normal dippers [6, 121]. Specifically, non-dipping was related to a 1.5-3.3 times greater risk of developing cardiovascular disease [122]. Controlling nocturnal BP has also demonstrated to protect against stroke and cardiovascular events, with hypertensive individuals treated for nocturnal BP demonstrating significantly lower relative risk of total cardiovascular events than those treated for daytime hypertension (RR = 0.39, 95% CI 0.3–0.5; number of events 187 versus 68; p < 0.001) [122]. Much of the research to date on 24-h BP however has focused on cardiovascular disease outcomes rather than dementia.
24-HOUR BLOOD PRESSURE RELATIONSHIP TO DEMENTIA
While elevated 24-h BP profiles may be a stronger predictor of cardiovascular events than office BP, the literature on 24-h BP as predictive of dementia is less defined. However, there are several small community-based studies that have demonstrated links between elevated and abnormal 24-h BP profiles and dementia, AD, cognitive impairment, or small vessel disease (see Tables 1–3). This evidence is summarized below.
24-hour Blood Pressure, Dementia, and Alzheimer’s Disease
AD, Alzheimer’s disease; CU, Cognitive unimpaired; DU, dementia unspecified; MCI, mild cognitive impairment; PD, Parkinson’s disease; PDD, Parkinson’s disease dementia; SMI, subjective memory impairment; VaD, vascular dementia; y, years.
24-hour blood pressure and cognitive impairment
ISSYS project, Investigating Silent Strokes in hypersensitive individuals, a magnetic resonance imaging Study; INFINITY, INtensive versus Standard Ambulatory Blood Pressure Lowering to Prevent Functional DeclINe In The ElderlY; Stroop, Stroop Color Word Test; MCI, mild cognitive impairment; CU, cognitively unimpaired; y, years. *Completed a battery of 10 neuropsychological tests and neurological exam.
24-hour blood pressure and cerebral small vessel disease markers
MCI, mild cognitive impairment; CU, cognitively unimpaired; HTN, hypertension; WMH, white matter hyperintensities; SCI, silent cerebral infarct; y, years; INFINITY, INtensive versus Standard Ambulatory Blood Pressure Lowering to Prevent Functional DeclINe In The ElderlY.
24-hour blood pressure and risk of dementia
Cross-sectional research has indicated that dementia patients have higher BP during sleep, including significantly more incidences of non-dipping BP and rising BP profiles compared to healthy older adults across six studies of 845 individuals (see Table 1). In our literature search, no research to date has investigated the prospective association between midlife 24-h BP profiles and dementia risk. Limited longitudinal data available supports a relationship with late life 24-h BP profiles and development of dementia and AD [123, 124]. In a cohort of 1,283 men without dementia at baseline (aged 71 or 77 years) followed for up to 24 years, 286 later developed dementia [124]. Compared with normal BP dipping, those with reverse systolic BP dipping (i.e., rising but not reduced dipping) were more likely to be later diagnosed with all cause dementia (HR = 1.64, 95% CI 1.14–2.34, n = 286), AD dementia (HR = 1.67, 95% CI 1.01–2.76, n = 141), but not vascular dementia (HR = 1.29, 95% CI 0.55–3.06, n = 48), although the number of individuals with vascular dementia was considerably small. A similar study included 1,320 adults aged 57-85 years without dementia at baseline followed for an average of 5.3 years [123]. Those who were later clinically diagnosed with AD had significantly higher 24-h average BP and nocturnal systolic BP compared to those free from dementia, but only if they were also carrying the APOE4 allele. Additionally, in this study, individuals who were using anti-hypertensives had a reduced risk of AD dementia compared to untreated hypertensive individuals.
24-hour blood pressure, mild cognitive impairment, and cognitive functioning
Elevated nocturnal BP, non-dipping, elevated 24-h BP, and elevated nocturnal pulse pressure in adults is associated with mild cognitive impairment and worse cognitive functioning in mostly cross-sectional analyses (see Table 2). For example, in 144 older adults, mild cognitive impairment occurred more in extreme dippers (32%), non-dippers (30%), and risers (50%) than in normal dippers (13.2%, p = 0.018), even after adjusting for the APOE4 allele [125]. Moreover, in younger adults (mean age = 30 years), reduced nocturnal systolic dipping and higher diastolic BP levels were associated with worse executive functioning at follow-up 20 years later, independent of office BP [126]. Additionally, the relationship between abnormal 24-h BP profiles and poorer cognitive functioning also appeared to be mediated by MRI markers of small vessel disease [127–132].
24-hour blood pressure and cerebral small vessel disease
High 24-h BP and abnormal dipping are also associated with imaging markers of cerebral small vessel disease across multiple studies (see Table 3). 24-h BP measurement may also be a better predictor of WMH than office BP. That is, studies that include both office and 24-h BP measures, demonstrate significant associations with WMH for 24-h BP but not office BP [128, 134]. The effect of lowering 24-h BP on WMH outcomes has been conducted in a single clinical trial of older adults (the INFINITY trial; M = 80.5 years, n = 199) [135]. Mean 24-h BP lowering was achieved at either a standard (systolic BP≤145 mm Hg) or intensive (≤130 mm Hg) level. Followed for 3 years, participants with intensive BP lowering had greater reduction in WMH volumes (-0.48%) compared to standard BP lowering (-0.29%), p = 0.03) and less cardiovascular events (RR = 0.24, 95% CI, 0.08 – 0.68), although no significant changes in cognition.
Mechanisms linking 24-h blood pressure to dementia
The mechanisms previously discussed to explain the relationship between hypertension and dementia are still applicable for elevated 24-h BP. Monitoring 24-h BP provides a more complete picture of an individual’s BP profile and abnormal nocturnal BP patterns may cause further stress on the vasculature. In addition to the outlined mechanisms, elevated nocturnal BP offers a potential additional mechanism in promoting AD through disruption of the glymphatic transport system. The glymphatic system facilitates the clearance of amyloid and other toxic proteins primarily during sleep [136]. This system is shown to be impaired in early and advanced hypertension in rodents [137]. Inducing hypertension in mice resulted in a reduction in flow of cerebrospinal fluid through perivascular space [138]. It is possible the nocturnal BP dip may play an essential role in the glymphatic system’s efficacy, and when disrupted could result in amyloid-β accumulation and subsequent development of AD. In patients with amnestic mild cognitive impairment, reduced BP dipping was associated with increased amyloid-β burden (captured through PET imaging) in the posterior cingulate and altered cerebral blood flow (n = 35) [139]. Additionally, the majority of OSA patients (around 80%) experience non-dipping BP patterns [107, 140]. It has been demonstrated in longitudinal studies that OSA is associated with increases in amyloid burden [141–143] and in emerging evidence hypertension (as indicated by office measures) strengthened this relationship (n = 98, Mage = 69.6 years; B = 23.11; 95% CI: 23.71 - 22.51; p = 0.01) [144]. It is expected, but not yet identified, that nocturnal hypertension would exhibit similar or stronger effects. Though there appears to be a role of nocturnal BP dipping in glymphatic clearance of amyloid-β, alternatively, disturbed nocturnal BP may also be a sign of amyloid accumulation and an early indicator of AD progression. Several studies of mice have demonstrated that amyloid deposition in the brain can also lead to the disruption of normal sleep architecture, often prior to the appearance of amyloid plaques [145].
IMPROVING 24-HOUR BLOOD PRESSURE PROFILES
Despite advances in understanding the role of 24-h BP in cardiovascular and brain health, to date, research on BP lowering to prevent dementia is limited to office BP measures. Individuals who successfully lower office BP but remain with undetected nocturnal hypertension could attenuate the effect size of anti-hypertensive use on dementia risk. However, as trials using anti-hypertensive medications target office BP and not 24-h BP, this remains unclear. Research is needed to determine if targeting 24-h BP profiles has the potential to demonstrate similar or stronger effects to office BP lowering on risk of dementia. There are multiple successful treatment strategies for reducing BP across 24 h and restoring normal dipping patterns, including medication timing, lifestyle modification and sleep disorder treatment. Utilizing 24-h BP monitoring in treatment strategies has the capacity to better identify and treat hypertension and therefore could be an important avenue for research and clinical practice in the prevention of dementia. For example, chronotherapy, the administration of medication at times determined by circadian rhythms, is a treatment method to improve 24-h BP profiles. Taking at least one anti-hypertensive medication before bed (compared to morning) has shown to help restore normal BP dipping and/or reduce nocturnal systolic BP in the short term [146–148] and demonstrates reduced risk of major cardiovascular disease events in longitudinal studies [149].
Lifestyle modification
Treatment of hypertension additionally includes lifestyle modification, some of which has also shown to improve 24-h BP profiles. Many kinds of exercise programs have demonstrated as being effective in restoring normal dipping BP patterns and reducing 24-h BP [150–154]. Salt restriction and increased dietary potassium in salt-sensitive individuals has also shown to restore the dipping BP profile [155].
Treatment of sleep disorders
As sleep plays a key role in BP dipping, treatment of sleep disorders offers a potential method to improve BP profiles. Small clinical trials have repeatedly demonstrated that in hypertensive patients with OSA, treatment with continuous positive airway pressure (CPAP) led to a reduction in mean 24-h BP [156–161], 24-h pulse pressure [162], and restored normal dipping patterns [163]. Further, CPAP treatment was also lowered BP in patients with treatment resistant hypertension [164, 165]. There is a lack of research on whether restoring normal sleep amongst other sleep disorders demonstrates a similar effect to CPAP as it relates to reducing nocturnal BP.
FUTURE DIRECTIONS
Hypertension is one of the most established risk factors for dementia. Better screening and management of hypertension would likely prove to be beneficial in prevention of dementia. Ambulatory BP monitoring is one such strategy that is not only markedly more effective than office BP in determining masked hypertension, white coat hypertension and treatment resistant hypertension [99, 167], but also is the only way to identify blunted nocturnal BP dipping of which there is a high prevalence [99, 100]. Further, use of 24-h monitoring for medication timing strategies has the potential to help manage elevated nocturnal BP. Use of 24-h BP monitoring provides a stepping-stone towards improved screening and effective treatment of hypertension and therefore may have an important role in helping to curtail the rising burden of dementia.
Recommendations for use of ambulatory BP monitoring have emerged within the past decade. The latest international clinical guidelines across Europe, the US and Australia recommend ambulatory BP monitoring for better diagnosis of hypertension [168–170]. Data of ambulatory BP monitoring use in primary care settings suggests that uptake is limited [171–173]. More evidence is needed to support the use of 24-h BP monitoring in dementia prevention strategies.
This review has identified many research gaps in our knowledge of 24-h BP and dementia (see Fig. 4). Specifically, there is a dearth of longitudinal research that examines effects of elevated 24-h BP profiles over the life course and dementia outcomes. Cohort studies would also provide more detailed analysis of the mechanisms linking 24-h BP profiles to dementia through brain imaging and fluid biomarkers. Furthermore, for 24-h BP lowering to be used as a prevention strategy, intervention trials are much needed, including chronotherapy trials and anti-hypertensive use with nocturnal BP targets. Research is also needed to further understand the role of sleep disorders on nocturnal dipping and dementia risk, including sleep treatment intervention trials.

Summary of review findings including what is known and future research questions.
CONCLUSION
Persistent elevated BP harms the brain in a way that increases risk for dementia. Addressing the future public health burden of dementia means improving the way we identify, treat, and manage elevated BP, as there are major gaps in clinical practice and research. It is suggested that 24-h BP monitoring will help bridge some of these gaps. Elevated 24-h BP patterns are well researched as being better predictors of cardiovascular and mortality outcomes in comparison to office BP; similar studies are needed with dementia as an outcome. The limited research conducted to date with 24-h BP suggests that abnormal 24-h BP, especially blunted nocturnal dipping, is associated with higher dementia incidence, along with markers of brain injury. Although persistent knowledge gaps raise uncertainties in the relationship between 24-h BP and dementia, 24-h BP measurement has good clinical utility for identifying and treating the large number of individuals experiencing nocturnal hypertension and consequently could have a key role in risk reduction for dementia.
Footnotes
ACKNOWLEDGMENTS
The authors have no acknowledgments to report.
FUNDING
MPP is supported by a National Health and Medical Research Council of Australia Emerging Leader 2 Investigator Grant Fellowship (GTN2009264). SY is supported by an Alzheimer’s Association Research Grant – New to the Field (AARG-NTF-22-971405). MG is supported by an Australian Government Research Training Program (RTP) Scholarship.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.