
Abstract
Alzheimer's disease (AD) remains a significant global health challenge, characterized by its progressive neurodegeneration and cognitive decline. The urgent need for early diagnosis and effective treatment necessitates the identification of reliable biomarkers that can illuminate the underlying pathophysiology of AD. This review provides a comprehensive overview of the latest advancements in biomarker research, focusing on their applications in diagnosis, prognosis, and therapeutic development. We delve into the multifaceted landscape of AD biomarkers, encompassing molecular, imaging, and fluid-based markers. The integration of these biomarkers, including amyloid-β and tau proteins, neuroimaging modalities, cerebrospinal fluid analysis, and genetic risk factors, offers a more nuanced understanding of AD's complex etiology. By leveraging the power of precision medicine, biomarker-driven approaches can enable personalized treatment strategies and enhance diagnostic accuracy. Moreover, this review highlights the potential of biomarker research to accelerate drug discovery and development. By identifying novel therapeutic targets and monitoring disease progression, biomarkers can facilitate the evaluation of experimental treatments and ultimately improve patient outcomes. In conclusion, this review underscores the critical role of biomarkers in advancing our comprehension of AD and driving the development of effective interventions. By providing a comprehensive overview of the current state-of-the-art, this work aims to inspire future research and contribute to the goal of conquering AD.
This is a visual representation of the abstract.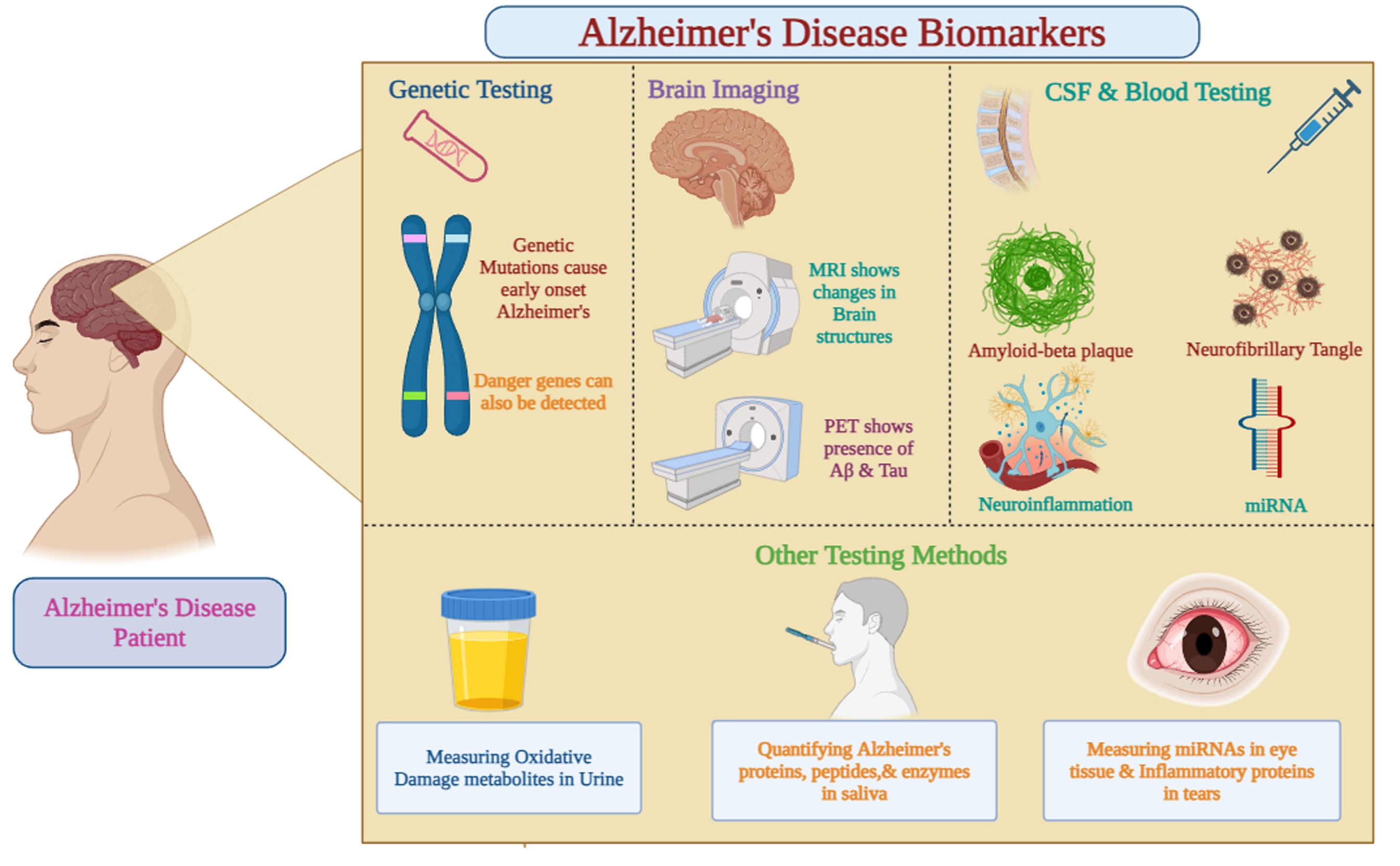
Introduction
Alzheimer's disease (AD) is a nervous system disorder that get worse with time and affect the cognitive, behavioral, memory, and personality of the diseased individual. AD is affecting millions of people worldwide and the most widespread cause of dementia, commonly old age individuals and sometimes adult under 65 also develop early symptoms of the disease. AD is identified by the abnormal protein deposition in the brain, firstly reported in 1906 by Dr Alois Alzheimer. 1 Two main pathological characteristics of AD are intracellularly accumulated hyperphosphorylated tau protein knows as tau tangles and extracellularly deposition of aggregated amyloid-β (Aβ) peptides called Aβ plaques. Loss of neurons and shrinkage of brain happens due to this abnormal deposition, which affects neuron functions and synaptic transmission, particularly in the cortex and hippocampus which are memory-related regions. 2 The development of AD takes place in different phases initially with cognitive deficits and minor memory loss and move forward to severe dementia and loss of autonomy. Personality changes and severe impairment in daily activities are seen in advance phases, while early signs include amnesia and problems with language and problem-solving abilities. Disease conditions impact the quality of life of patient and caretakers is negatively, ultimately increasing the socioeconomic and healthcare expenses. 3 Association of behavioral, environmental, and genetic variables with AD makes it complex. Hereditary AD is associated with genetic mutations in presenilin 1 (PSEN1), presenilin 2 (PSEN2), and amyloid-β protein precursor (AβPP) but APOE ε4 allele is the potential risk factor for late-onset AD. Environmental factors, i.e., diabetes, brain injury, and cardiovascular health influences disease risk and progression. 4 Early diagnosis and detections is getting easier due to recent advances in biomarker research, neuroimaging, and genetic knowledge of AD. Nowadays, by using biomarkers, AD pathology is detected and disease development is tracked such as blood-based tests, amyloid positron emission tomography (PET) imaging, and cerebrospinal fluid (CSF), tau proteins and Aβ levels. The aim of current research is altering the disease process and improving the patient outcomes.5,6
AD is the most common cause of dementia, accounting for an estimated 60% to 80% of cases. Most individuals also have the brain changes of one or more other causes of dementia. 7 Recent epidemiological studies have highlighted the alarming rise in AD cases globally. For example, a study published in The Lancet Neurology in 2019 estimated that the number of people living with dementia worldwide has nearly doubled in the past two decades, reaching 50 million in 2018. 8 This number is projected to triple by 2050, with the majority of cases occurring in low- and middle-income countries. The societal and economic burden of AD is immense. In the United States alone, the estimated cost of AD in 2020 was $355 billion, and this figure is expected to soar in the coming years. 7 AD not only impacts individuals with the disease but also places a significant strain on families, caregivers, and healthcare systems.
Role of biomarkers in Alzheimer's disease research
Biomarker plays crucial role as they provide information related to the disease etiology, course and therapy response to the condition. They provide valuable insights into the disease's underlying mechanisms, aid in early diagnosis, and help track disease progression and treatment response. AD-associated biomarkers are as follows in Figure 1.

Pathophysiology of Alzheimer's disease involves various factors contributing to its progression, with amyloid plaques and hyperphosphorylated tau playing central roles.
Cerebrospinal fluid markers
CSF is a clear fluid that surrounds the brain and spinal cord. By analyzing CSF samples, researchers can measure levels of proteins like Aβ and tau, which are associated with AD pathology. Elevated levels of tau and decreased levels of Aβ in CSF are indicative of AD.
Neuroimaging biomarkers
Neuroimaging techniques, such as PET and magnetic resonance imaging (MRI), allow for the visualization of brain changes associated with AD. Amyloid PET scans can detect the accumulation of amyloid plaques in the brain, while fluorodeoxyglucose (FDG)-PET scans can measure brain metabolism. MRI can assess brain atrophy and structural changes.
Blood-based biomarkers
Blood tests offer a non-invasive approach to biomarker detection. Researchers are actively investigating blood biomarkers, including Aβ and tau, as potential diagnostic tools for AD. While blood-based biomarkers are still under development, they hold promise for early disease detection and monitoring.
Genetic biomarkers
Genetic factors play a significant role in AD risk. The apolipoprotein E (APOE) ε4 allele is the most well-known genetic risk factor, increasing the likelihood of developing AD. Genetic testing can identify individuals at higher risk and inform personalized prevention and treatment strategies.
Amyloid-β protein
The amyloid hypothesis is a prominent theory in AD research, proposing that the accumulation of Aβ peptides in the brain is a primary driver of neurodegeneration and cognitive decline associated with the disease. According to this hypothesis, Aβ, which is derived from the cleavage of AβPP by enzymes such as β-secretase (BACE1), aggregates to form insoluble plaques and soluble oligomers. These aggregates disrupt neuronal function, leading to synaptic impairment and eventually neuronal death.9–11
Key features of the amyloid hypothesis
Aβ accumulation
The hypothesis posits that excessive accumulation of Aβ peptides leads to synaptic dysfunction and neuroinflammation, ultimately resulting in cognitive deficits characteristic of AD.10,12
Pathological characteristics
Amyloid plaques are primarily found in regions of the brain associated with memory and cognition, such as the neocortex and hippocampus.10,11
Mechanism of action
Aβ oligomers are believed to be particularly toxic, causing inflammation and neuronal death, while also impairing synaptic communication.10,11
Despite its widespread acceptance, the amyloid hypothesis has faced significant scrutiny and debate within the scientific community:
Correlation versus causation
Critics argue that while Aβ accumulation is observed in AD patients, it does not necessarily correlate with the degree of cognitive impairment. Some individuals exhibit substantial Aβ deposits without any signs of dementia, suggesting that other factors may contribute to disease progression.11,13
Alternative pathways
There is growing interest in exploring other potential mechanisms underlying AD, including tau pathology and neuroinflammation, which may play significant roles independent of Aβ accumulation.10,12
Therapeutic challenges
Many clinical trials targeting Aβ have failed to produce effective treatments for AD. This has led researchers to reconsider whether Aβ is a primary driver of the disease or merely a byproduct of more complex pathological processes.11,13,14
According to amyloid hypothesis, the abnormal Aβ accumulation affects neuronal function, synaptic impairment, and neurodegeneration, is depends on the Aβ protein. 2 BACE1 breaks AβPP, resulting in the formation of Aβ peptides. generally, moderate amounts of Aβ from the brain are removed by the microglial phagocytosis, blood-brain barrier, and enzymatic degradation. 13
Soluble Aβ (sAβ)
sAβ includes small, diffusible aggregates that are often referred to as oligomers. These forms of Aβ are thought to be the earliest and most toxic agents in AD pathology. Studies suggest that sAβ oligomers interfere with synaptic function, leading to neuronal damage. They can inhibit long-term potentiation, reduce dendritic spine density, and disrupt memory and learning processes in vivo. Elevated levels of sAβ have been observed in the white matter of AD patients, indicating that these peptides may independently contribute to white matter degeneration and overall cognitive decline. Furthermore, the composition of sAβ can influence its toxicity, with certain truncated forms being more harmful than full-length variants.15–17
Insoluble Aβ (iAβ)
iAβ primarily refers to larger aggregates that form amyloid plaques, a hallmark of AD pathology. While iAβ is associated with neurotoxicity, it is generally considered less directly harmful than sAβ oligomers; instead, iAβ may exacerbate the accumulation of soluble forms by promoting further aggregation. The presence of amyloid plaques correlates with certain pathological features of AD; however, it does not always align with cognitive impairment, suggesting a more complex relationship between iAβ and disease progression.16,17
Despite significant advancements in understanding the roles of soluble and insoluble Aβ, several limitations persist in biomarker research. Accurately measuring levels of sAβ and differentiating between various forms (e.g., oligomers versus monomers) remains challenging due to technical constraints in current assays. Additionally, there is ongoing debate regarding the relationship between Aβ levels and clinical symptoms; some studies suggest that elevated sAβ correlates more closely with cognitive decline than plaque burden, complicating the interpretation of biomarker data. Furthermore, the presence of Aβ in healthy individuals raises questions about its specificity as a biomarker for AD, necessitating further investigation into the biological context surrounding Aβ accumulation and its implications for different patient populations.10,11,18
Pathological role of Aβ in AD
On the other side of its direct neurotoxic effects, Aβ shows a pathogenic role in AD by initiating a series of downstream processes like tau hyperphosphorylation, oxidative stress, neuroinflammation, and impair synaptic function. The development of tau pathology and neurofibrillary tangles (NFTs) is caused by Aβ peptides (by activating kinases and suppressing phosphatases). 19 In addition, oxidative stress and Aβ-induced neuroinflammation intensify the neurodegeneration and neuronal loss in AD. 20
The evidence derived from animal models, human genetics, and clinical investigations shows crucial role of Aβ in AD development. AD conditions like cognitive impairments, synapse loss, amyloid deposition, and increased Aβ synthesis are detected in transgenic mice overexpressing mutant AβPP or presenilin. 2 Aβ's causative involvement in AD is further supported by the association between hereditary early-onset AD and genetic abnormalities in AβPP, PSEN1, and PSEN2, which affects Aβ synthesis or clearance. 21
Deposition of amyloid may be seen and quantify by using Aβ imaging and PET tracers such as [11C] Pittsburgh compound B (PiB) in clinical investigations, which benefits with early diagnosis and monitoring. 22 CSF biomarkers, such as Aβ42 and Aβ40 levels also indicates amyloid quantity; the ratio of Aβ42/Aβ40 is low in AD patients. 23 These indicators are essential for monitoring therapy, course, patient classification, and diagnostic evaluation in Aβ targeted clinical trials. 24
Detection methods: PET imaging and CSF analysis
PET imaging and CSF analysis are the two main techniques for identifying Aβ deposition in AD. 25 Radioligands such as florbetapir and [11C] PiB are used in PET imaging for the visualization and quantification of Aβ deposition in brain. These techniques are helpful in early detection and disease stage identification by giving comprehensive knowledge on the severity and location of amyloid. 22 PET is expensive, needs certain set of equipment, and not available everywhere. In CSF analysis process Aβ42, Aβ40, and other relevant biomarkers are measured using lumbar puncture-derived CSF fluid. The decreased Aβ42 levels and alterations in the Aβ42/Aβ40 ratio suggests amyloid deposition. 23 CSF analysis is less intruding and provides insightful diagnostic information compared to PET and may shows variations in biomarkers potential throughout laboratories.
Implications for diagnosis and treatment
Aβ deposition must be identified using PET imaging and CSF monitoring in order to diagnose and treat AD. Early stage diagnosis of Aβ is helpful in distinguishing AD from other dementias and authorize prompt interventions, such as lifestyle modifications and pharmaceutical therapies. 26 Biomarkers helps in patient classification, response tracking of Aβ targeted therapies and are integrated in clinical trials to evaluate the treatment efficiency and the disease progression. 27 Assay standardization and result interpretation continue to present difficulties despite its usefulness. 28 In general, AD diagnosis and therapy planning depend heavily on PET imaging and CSF analysis.
Tau protein
Important microtubule-associated protein tau is mostly expressed in neurons, where it promotes axonal transit and stabilizes microtubules. By binding to tubulin, tau promotes the formation of microtubules and plays a role in neuronal architecture, signaling, and synaptic plasticity.29,30 The tau hyperphosphorylation process is intricately connected to NFT formation and subsequent synaptic dysfunction in AD and other tauopathies.31,32 Tau is a crucial microtubule-associated protein predominantly expressed in neurons, where it stabilizes microtubules by binding to tubulin, thereby supporting axonal transport and maintaining neuronal architecture. 33 However, during the progression of AD, tau undergoes hyperphosphorylation, leading to its aggregation into NFTs, which consist of straight filaments (SFs) and paired helical filaments (PHFs). SFs are approximately 15 nanometers wide and are characterized by their relatively uniform structure. Unlike PHFs, SFs do not exhibit significant variations in width. They are considered a structural variant of PHFs and are formed from tau proteins that have undergone pathological changes, including hyperphosphorylation. PHFs, on the other hand, are formed by twisted double-helical ribbons of tau subunits. PHFs alternate in width between 8 and 20 nanometers and have a crossover spacing of approximately 80 nanometers. The term ‘paired helical filament’ was first introduced to describe the unique appearance of these filaments in electron microscopy studies of AD brain tissue. PHFs are more prevalent than SFs in NFTs, comprising about 90% of the total tau (t-tau) aggregates found in affected brain regions.33,34 These aggregates disrupt microtubule stability and impair neuronal function, contributing to synaptic dysfunction and cognitive decline. The accumulation of NFTs correlates with the severity of cognitive impairment, as tau pathology typically spreads from the entorhinal cortex and hippocampus to neocortical regions. The hyperphosphorylation of tau is influenced by several factors, including genetic mutations in the MAPT gene, environmental factors like traumatic brain injury, and neuroinflammation.34–37 This modification not only promotes tau aggregation but also leads to the loss of its normal microtubule-stabilizing function. As hyperphosphorylated tau disassembles microtubules and sequesters normal tau into tangles, it compromises axonal transport mechanisms essential for neuronal health. Consequently, this disruption contributes to synaptic dysfunction, which is a hallmark of cognitive decline in AD.38,39 Current research aims to develop targeted therapies that can halt or reverse tau aggregation through various approaches such as gene therapies, immunotherapies, and small molecule inhibitors. Additionally, biomarkers like tau PET imaging and CSF tau levels are critical for diagnosing and monitoring tauopathies. 39
Tau-based biomarkers, particularly phosphorylated tau (p-tau) species like p-tau181, p-tau217, and p-tau231, have shown promise as blood-based indicators for AD. Elevated p-tau levels correlate with abnormal Aβ status and predict progression to dementia, making them useful for early diagnosis and monitoring. Among p-tau assays, mass spectrometry-based p-tau217 performed best in detecting mild cognitive impairment (MCI) and predicting dementia progression. Tau biomarkers also reflect neurodegeneration better than Aβ biomarkers but are influenced by factors like age and comorbidities. However, p-tau levels may not directly represent tau aggregation or tangles seen in imaging.35,36
Aβ biomarkers include CSF and plasma Aβ42 levels and amyloid PET imaging, which detect amyloid plaque deposition. The Aβ42/Aβ40 ratio effectively differentiates AD from other dementias, and PET imaging confirms amyloid pathology. However, Aβ findings lack specificity as some cognitively normal individuals with positive results do not develop dementia. Moreover, Aβ biomarkers do not directly indicate neurodegeneration or cognitive decline.35,37
Integrating tau and Aβ biomarkers could improve diagnostic precision and provide a holistic understanding of the AD continuum.
Measurement in CSF and PET imaging
CSF and PET imaging can be incorporated to assess the tau protein levels, which gives crucial understanding and insights into tau pathology and AD-related tauopathies.40,41 t-tau and p-tau levels and the p-tau/Aβ42 ratio are measured by CSF analysis. High levels of t-tau and p-tau, along with reduced Aβ42, indicate amyloid accumulation and tau pathology, helping in diagnosis, treatment monitoring, and prediction of disease progression.42,43 In vivo visualization of tau accumulation is possible by using radiotracer like flortaucipir (AV-1451) and 18F-THK5351 which specifically binds to tau fibrils.44,45
Relationship to disease progression and cognitive decline
Tau pathology, which is analyzed by PET imaging and CSF biomarkers is intimately associated with the disease progression and cognitive decline. A greater likelihood of transitioning from MCI to AD dementia, increased hippocampal shrinkage, and rapid cognitive decline are all associated with elevated CSF tau biomarkers, notably p-tau. 46 These indicators have predictive significance for AD because they also indicate cognitive decline and conversion to dementia in cognitively normal persons. 47 Results from tau PET imaging correlate with cognitive impairment and the severity of the illness. Poorer cognitive function and a quicker rate of dementia progression are linked to increased tau PET uptake in brain areas that are more susceptible, such as the medial temporal lobe. 48 Tau PET imaging's function as a predictive biomarker for tau-related neurodegeneration is supported by the fact that it also predicts longitudinal cognitive decline and conversion to AD dementia. 49 By using CSF tau biomarkers with tau PET imaging together provide a comprehensive understanding of tau pathology. Various studies validated a relationship between CSF p-tau levels and tau PET tracer uptake, joint use for assessing tau pathology and predicting clinical outcomes. 50
Neuroimaging biomarkers
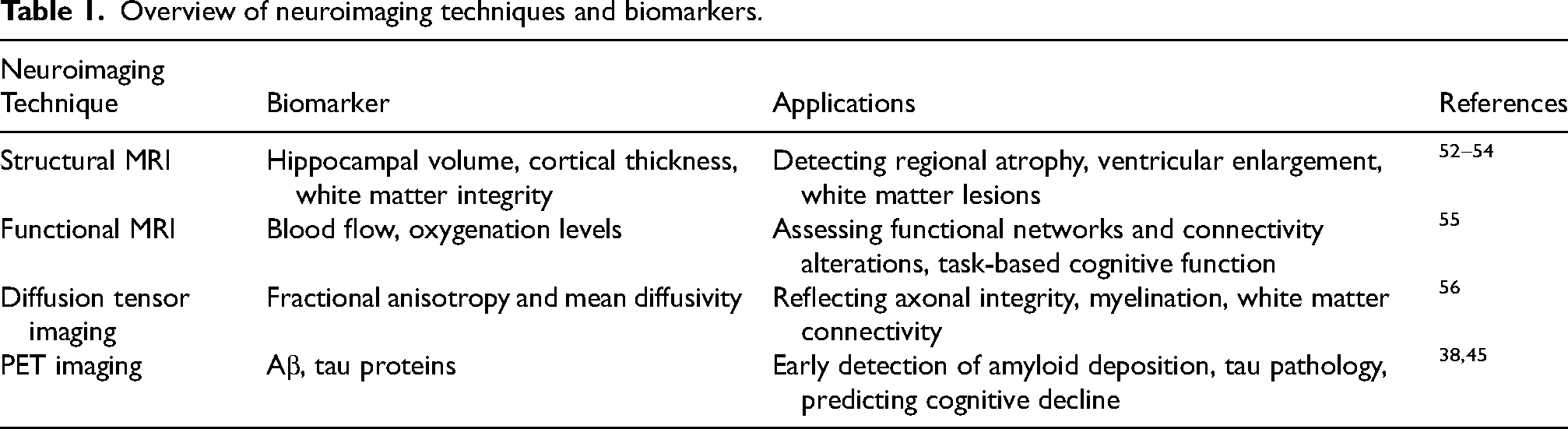
Over the past few decades, neuroimaging has opened up exciting non-invasive insights into the human brain. 51 Other non-invasive options for the study of various functions and aspects of the brain are advancing by the use of imaging models such as MRI and magnetoencephalography combined with regular methods such as electroencephalography. 51 Below are the details of neuroimaging techniques for biomarkers with applications in Table 1.
Overview of neuroimaging techniques and biomarkers.
PET imaging of Aβ and tau
Neuroimaging techniques, such as PET and functional MRI (fMRI), have revolutionized our understanding of brain function and pathology, particularly in the context of neurodegenerative diseases like AD. PET imaging allows for the visualization and measurement of key pathological markers, such as Aβ deposition and NFTs of tau. Specific ligands, including [18F] florbetapir, [18F] florbetaben, and [11C] PiB, target Aβ plaques in the brain, while [18F]AV-1451 (flortaucipir) and [18F]MK-6240 selectively bind to tau aggregates for in vivo visualization of NFTs. The advantages of PET include its high sensitivity for detecting metabolic changes at the cellular level, which can reveal disease processes before structural abnormalities become apparent. However, PET also has drawbacks, such as exposure to radiation from radioactive tracers and limitations in spatial resolution compared to other imaging modalities like MRI. Additionally, the high cost and limited availability of PET imaging can restrict its use in clinical practice.57,58 See Table 2.
PET imaging ligands for Alzheimer's disease.

Functional MRI and connectivity changes
fMRI quantifies brain activity through changes in blood oxygenation levels. Resting-state fMRI is particularly useful for studying functional connectivity alterations in AD. It has shown blocked connectivity within and between major brain networks, such as the default mode network, salience network, and executive control network, in AD patients compared to healthy controls.66–68 These disruptions may reflect neurodegenerative processes and serve as biomarkers for disease progression.
Task-based fMRI evaluates cognitive functions and neural activation patterns during specific tasks. In AD, task-based fMRI often reveals reduced activation in memory-related regions during memory tasks, reflecting impaired neural recruitment and network dysfunction.69,70
Longitudinal fMRI studies track changes in functional connectivity over time, demonstrating that these alterations often precede clinical symptoms and correlate with cognitive decline.71,72 This makes longitudinal fMRI valuable for predicting disease progression and identifying imaging biomarkers for future cognitive decline.
Advanced analytical techniques, such as graph theory and machine learning, are increasingly used to analyze fMRI data. Graph theoretical analyses indicate decreased network efficiency and increased path length in AD patients.73–75 Machine learning can greatly help to improve early diagnosis and prediction, models can be developed by using fMRI connection metrics. Integrating fMRI with neuroimaging models including as diffusion tensor imaging, PET, and structural MRI give thorough understanding of AD. 62 The utilization of imaging multi models may increase the sensitivity and specificity of AD biomarkers, which integrate structural and functional data for identification of changes in connectivity and the relationship with cognitive loss.76–78 Future directions may involve combining neuroimaging biomarkers with other biomarkers to enhance diagnostic accuracy and provide a more comprehensive understanding of AD pathology. Integrating structural MRI with functional imaging techniques like fMRI and PET could improve sensitivity and specificity for identifying changes associated with cognitive decline.
Cerebrospinal fluid biomarkers
Biomarkers of the CSF provide crucial insights on the biochemical changes happening in the brain, which helps in driving molecular mechanism of AD. The literature shows Aβ42, t-tau, and p-tau are the mostly researched biomarker in CSF. Several tau isoforms, like p-tau, exist and can be monitored in CSF (see Table 3). The elevated levels of CSF tau during the symptomatic phase of AD are responsible for the rise of p-tau isoforms. CSF p-tau measurement rarely adjusted from t-tau variance, The primary cause of high CSF p-tau level to only tau hyperphosphorylation as a result of aberrant brain metabolism and the presence of hyperphosphorylated tau aggregates.79–81
Summary of CSF biomarkers of Alzheimer's disease.
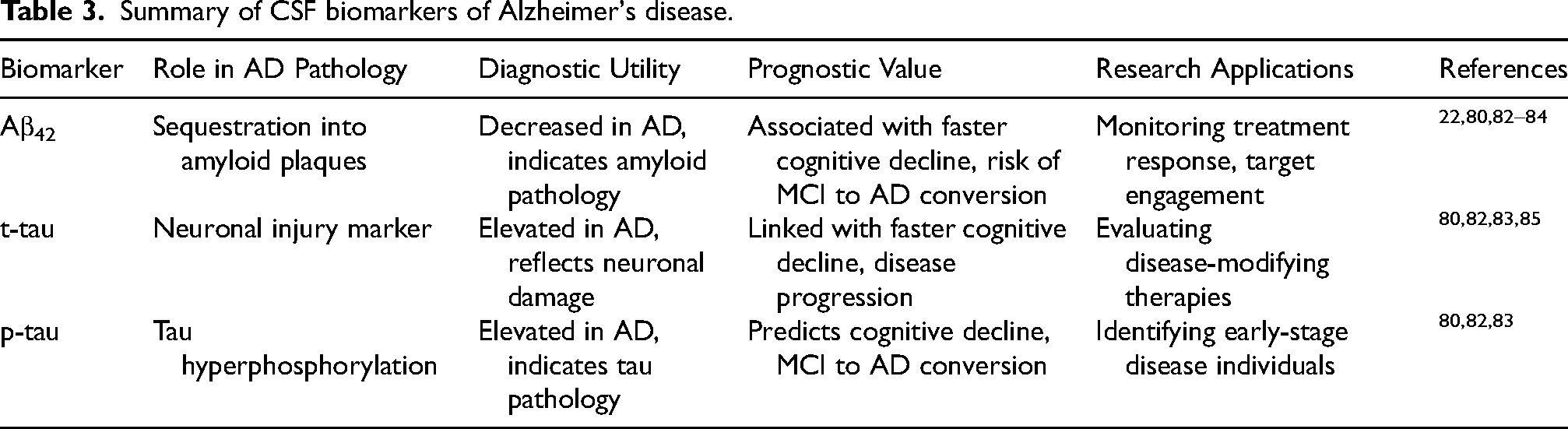
Recent advances in CSF biomarker detection, particularly through the development of ultrasensitive assays, have significantly enhanced our understanding of the biochemical changes occurring in the brain, which are crucial for elucidating the molecular mechanisms of AD. The most extensively researched CSF biomarkers include Aβ42, t-tau, and p-tau. Elevated levels of CSF tau during the symptomatic phase of AD are indicative of increased p-tau isoforms, which are associated with tau hyperphosphorylation and aberrant brain metabolism. The use of ultrasensitive assays has proven beneficial in quantifying trace amounts of biomarkers that are typically present at very low concentrations in CSF. For example, these assays have successfully detected visinin-like protein-1, which has been associated with clinical disease progression in AD. Furthermore, recent studies have demonstrated that using ratios of biomarkers, such as the Aβ42/Aβ40 ratio, can improve diagnostic accuracy compared to measuring Aβ42 alone. This highlights the importance of not only detecting individual biomarkers but also considering their interrelationships.83,86
Analysis of Aβ and tau levels
Immunoassays, like multiplexed bead-based assays and ELISAs are generally used for sensitive and precise quantification of tau and Aβ in CSF. The reliable and standard protocol gives guaranteed measurement which further helps in the accurate diagnosis and treatment plan of the AD. 87 People with AD mostly have lower levels of Aβ42 and higher concentration of t-tau and p-tau which distinguishes AD from other types of dementias. 88
Clinical utility and challenges in CSF testing
Decreased levels of Aβ42 and higher concentrations of t-tau and p-tau shows a rapid decline and a more chance of conversion from moderate cognitive impairment to AD. By analyzing CSF biomarkers, we can forecast disease progress and cognitive decline. 83 CSF biomarkers are integrated for the evaluation of treatment in clinical trials. 22 Data collection errors, processing techniques and individual variances affect the outcomes of CSF biomarkers. 89
Blood-based biomarkers
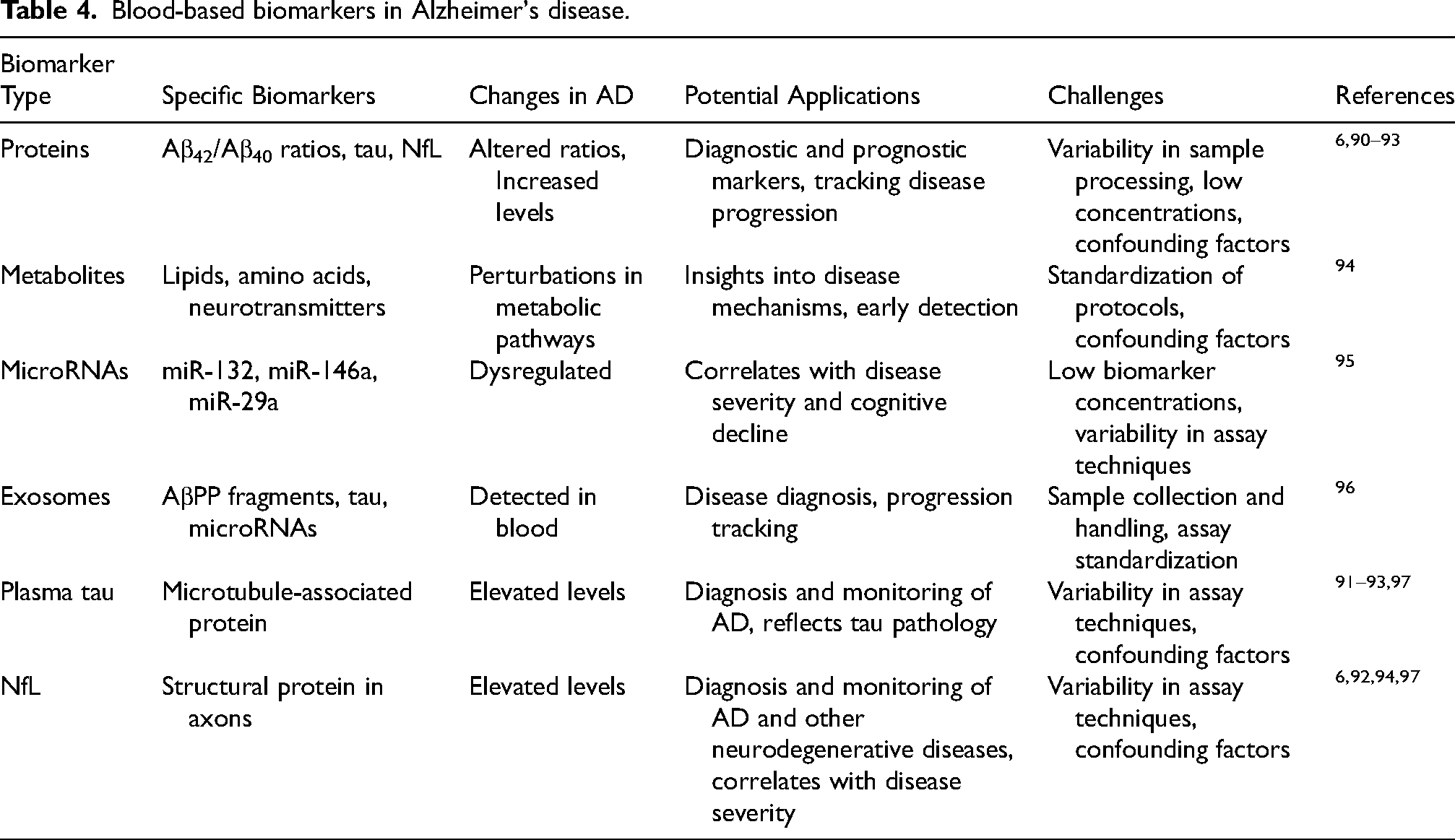
Plasma Aβ42/Aβ40, p-tau, neurofilament light chain (NfL), glial fibrillary acidic protein are the blood-based biomarkers for AD which can be combined with each other to ease and potentiate clinical studies. It is observed that plasma Aβ42/Aβ40 levels are already completely changed in the pre-symptomatic stages of the disease is a significant trait. Because of this reason, this biomarker, having similarity with CSF Aβ42/Aβ40, is capable to recognize Aβ pathology in cognitively unimpaired individuals with levels of precision comparable to those found in cognitively impaired individuals. As blood biomarkers for AD, many research groups have developed highly sensitive tests for p-tau, which includes assays for tau phosphorylated at amino acids 181 (p-tau181), 217 (p-tau217), or 231 (p-tau231). Protein biomarkers have demonstrated insight of interest in the plasma levels of tau protein isoforms, NfL, and Aβ peptides. Research has demonstrated that the plasma of AD patients differs from that of cognitively normal people in terms of Aβ42/Aβ40 ratios, tau, and NfL levels; these differences suggest that the plasma may serve as a diagnostic and prognostic marker. 90 See Table 4 for a list of some blood-based biomarkers.
Blood-based biomarkers in Alzheimer's disease.
Compared to CSF biomarkers, blood-based biomarkers have special benefits that help with important issues in the diagnosis and study of AD. Blood-based biomarkers are easier to obtain and more practical for normal clinical usage and large-scale population investigations than CSF biomarkers, which necessitate invasive lumbar puncture procedures. 98
Blood biomarkers show systemic changes linked to neurodegeneration, whereas CSF biomarkers, such as Aβ42, t-tau, and p-tau, offer direct insights into disease of the central nervous system (CNS). Because of this distinction, researchers can examine putative systemic factors that contribute to the advancement of AD as well as peripheral processes of AD pathogenesis. Additionally, blood biomarkers make it possible to regularly and continuously monitor the course of the disease, something that is sometimes not feasible with CSF because sample collection is so invasive.6,91
The sensitivity and specificity of blood biomarker readings have also been improved by sophisticated detection methods, such as single-molecule array (Simoa) and ultrasensitive immunoassays, which make them a good substitute for early detection and disease monitoring. Plasma biomarkers that bridge the gap between systemic physiological processes and CNS-specific alterations include tau, NfL, and Aβ42/Aβ40 ratios.92,93
Plasma tau and NfL
AD is becoming more widely recognized, and plasma biomarkers such as tau protein and NfL are being considered as viable diagnostic and tracking techniques. NfL, a structural protein in axons, and tau, a microtubule-associated protein, both show neurodegeneration and are hence useful for evaluating AD pathology. 98 Research has demonstrated that as compared to cognitively healthy people, AD patients had higher plasma tau and NfL levels. Increased NfL is correlated with disease severity, cognitive decline, and neuronal damage, whereas elevated plasma tau represents tau pathology.6,91 Measurement of biomarkers from the blood samples are more beneficial as compared to CSF as it is less invasive with wide range of therapeutic applications. Moreover, plasma biomarkers help to ease the tracking of disease progression and treatment response. Advanced assay techniques such as Simoa technology and ultrasensitive immunoassays improved the detection and measurement of these biomarkers in the clinical practices and AD research. 92 NfL and plasma tau also helps in diagnosis and treatment monitoring of neurodegenerative conditions other than AD such as amyotrophic lateral sclerosis, Parkinson's disease, and frontotemporal dementia. 93
Potential for non-invasive diagnosis and monitoring
Blood-based biomarkers NfL and plasma tau showed demonstrated potential for non-invasive monitoring and diagnosis of neurodegenerative disease, including AD. They provide less invasive options than invasive techniques such as CSF or neuroimaging, making them more patient-acceptable and easier to integrate into clinical practices. 92 After these encouraging outcomes also there are multiple issues such as process standardization, validation of biomarker cutoffs, and taking a count of age, sex, and comorbidities-related factors. that needs to be resolved before the frequent use of plasma biomarkers in clinical practices. 91 Additionally, a potential investigation is required to clarify the precise mechanisms behind alterations in NfL levels and plasma tau in neurodegenerative disorders.
Genetic biomarkers
Finding treatment targets and identifying at-risk individuals are made possible by the study of the genetics and genomes underpinning AD. The APOE gene is one of the most well-known genetic risk factors for AD; having the APOE ε4 allele is linked to a markedly increased risk of AD. Compared to non-carriers, carriers of this gene frequently show a faster pace of cognitive decline, increased amyloid deposition, and an earlier onset of disease.99–102
The diverse genetic makeup of AD has been highlighted by the discovery of new genetic loci connected to its risk by genome-wide association studies. Important genes that have been linked to AD vulnerability include clusterin (CLU), bridging integrator 1 (BIN1), and phosphatidylinositol-binding clathrin assembly protein (PICALM).103,104
These loci offer vital information about the molecular mechanisms underlying the pathophysiology of AD. Additionally, rare genetic mutations in AβPP, PSEN1, and PSEN2 are linked to familial forms of early-onset AD. These mutations either increase the production of Aβ or change its processing, which accelerates amyloid aggregation and neurodegeneration.105,106 Genetic counselling for impacted families is informed by genetic testing for these mutations, which also helps diagnose cases with an early onset.
In addition to determining risk, new research indicates that combining genetic markers with lifestyle risk variables including nutrition, exercise, and mental activity may improve precision medicine tactics’ prediction ability.
Combining data on modifiable risk factors with APOE genotype, for example, may assist stratify people according to their risk of developing AD and adjust preventative measures appropriately. Furthermore, genetic biomarkers could be used to create individualized treatment plans. For instance, tailored treatments that modify the tau or amyloid pathways may be beneficial for people with particular genetic backgrounds. Likewise, the existence of APOE ε4 may influence treatment strategies that target lipid metabolism. These genetic insights may also facilitate lifestyle changes, allowing for customized dietary and exercise advice to lower the risk or progression of AD.
Precision medicine techniques can maximize prevention, early detection, and treatment plans by utilizing genetic markers in combination with environmental and lifestyle data. These developments highlight the need for more investigation into the ways in which hereditary and non-genetic variables interact to affect the onset and course of AD.
APOE ε4 allele and AD risk
The APOE gene, located on chromosome 19, has three main isoforms: ε2, ε3, and ε4. Of these, the ε4 allele has been consistently associated with an increased risk of AD. Individuals who inherit one copy of the APOE ε4 allele have an elevated risk of developing AD, while those with two copies have an even higher risk compared to non-carriers.107,108
Various epidemiological research has shown a link between APOE ε4 and AD risk across diverse populations and ethnicities in Table 5. Meta-analyses have confirmed the robustness of this association, with APOE ε4 carriers exhibiting a significantly higher risk of developing AD compared to non-carriers. 109 The presence of the allele APOE ε4 is estimated to elevate the risk of developing AD by approximately three to fourfold in heterozygous individuals and up to fifteenfold in homozygous individuals. 110
Genetic biomarkers in Alzheimer's disease.

Despite the wealth of genetic discoveries in AD, the clinical utility of these genetic variants for risk prediction and therapeutic targeting remains limited. Polygenic risk scores, calculated based on multiple genetic variants associated with AD, may improve risk assessment and stratification in research settings. 107 However, the predictive power of genetic risk scores for AD remains modest, highlighting the complex interplay between genetic and environmental factors in disease development.
Inflammatory biomarkers
AD is mostly caused by inflammation, with astrocytes, microglia, and the release of pro-inflammatory mediators all contributing to chronic neuroinflammation. This inflammatory cascade is a crucial field of research for comprehending the course of disease and determining potential treatment targets since it leads to neuronal damage, synaptic dysfunction, and cognitive decline. 13 Inflammatory biomarkers have the ability to guide treatment measures, track the progression of disease, and identify patients early.
The brains and CSF of AD patients have higher levels of important pro-inflammatory cytokines, including interleukin-1β (IL-1β), interleukin-6 (IL-6), and tumor necrosis factor-alpha (TNF-α), which disrupt the blood-brain barrier and exacerbate neurodegeneration.114,115
These cytokines have two functions: they mediate immunological defense at first, but when they become dysregulated, they also contribute to chronic inflammation and neuronal damage.
Chemokines, such as macrophage inflammatory protein-1α (MIP-1α/CCL3) and monocyte chemoattractant protein-1 (MCP-1/CCL2), are markedly elevated in AD and are associated with both cognitive loss and the severity of the illness.116,117 By drawing peripheral immune cells to the CNS, these chemokines prolong inflammation. Acute-phase proteins that have been connected to an elevated risk and progression of AD include serum amyloid A and C-reactive protein, which further intensify the inflammatory response. 118 Furthermore, oxidative stress is exacerbated in AD by inflammatory mediators such as prostaglandins, reactive oxygen species, and nitric oxide. 119
Cytokines, chemokines, and microglial activation markers
Neuroinflammation is sustained when pro-inflammatory cytokines and chemokines are released as a result of microglia and astrocytes activating in response to neuronal injury. A key factor in this process is the promotion of neuronal damage and synaptic dysfunction by elevated levels of TNF-α, IL-6, and IL-1β. 120 MCP-1 and MIP-1α are examples of chemokines that draw in peripheral immune cells and increase CNS immune cell activation. 116
Neuroinflammation is characterized by microglial activation, which is signaled by markers like CD68, CD11b, and Iba1. Reactive oxygen species and pro-inflammatory cytokines are among the neurotoxic chemicals released by activated microglia, which accelerates neuronal degeneration.121,122 Immunomodulation and anti-inflammatory therapies are two therapeutic approaches that target these pathways and have the potential to reduce neuroinflammation and maintain cognitive abilities. 123
Notwithstanding their potential, there are obstacles to the therapeutic use of inflammatory biomarkers, such as the fluctuation of biomarker levels brought on by confounding variables like age, medication use, and concomitant illnesses. Cytokine levels, for example, can change in response to infections, metabolic diseases, or systemic inflammation, making it more difficult to interpret them in AD settings.
To reduce variability and increase repeatability, measurement methods must be standardized throughout research. Standardized sampling procedures for blood and CSF, the use of validated assays with reliable sensitivity and specificity, and the correction of statistical analysis for confounding variables are some strategies. Using a single strategy could improve these biomarkers’ accuracy in AD diagnosis and tracking.
Clinical applications and challenges
Diagnosis and prognosis
For the diagnosis of AD, a variety of biomarkers are being developed, including blood, urine, CSF, tau, p-tau, and Aβ. 124 Reduced levels of apoE4, a sign of neuronal degradation, are one example of a cargo protein seen in CSF that shows potential as an AD indication. Assessing apoE4 plasma levels offers a less intrusive diagnostic method with the ability to screen the entire population.
Neuroimaging methods, including as PET and structural MRI, are crucial for illustrating the pathogenesis of AD. As supplementary methods, blood-based tests are becoming more widely available and economical. By measuring biomarkers like p-tau and plasma Aβ42/Aβ40 ratios, these tests provide information about tau-mediated neurodegeneration and amyloid pathology.3,124
The AT(N) framework: a complete model for diagnosis
The National Institute on Aging-Alzheimer's Association (NIA-AA) created the AT(N) framework, which offers a systematic method for categorizing AD biomarkers according to three main pathophysiological processes:
A: Amyloid buildup, identified by CSF Aβ42/Aβ40 ratios or amyloid PET imaging. T: Tau pathology, as shown by tau PET imaging or CSF p-tau levels. (N): Neurodegeneration, as shown by increased CSF t-tau or structural MRI (e.g., hippocampus shrinkage).
Using this paradigm, researchers and physicians can classify people according to their biomarker profiles into preclinical, prodromal, or dementia stages. The AT(N) approach facilitates early diagnosis and customized therapies by providing a nuanced perspective of disease development through the integration of amyloid, tau, and neurodegeneration markers.125,126 The importance of multi-modal biomarker profiling in improving the early detection of AD is highlighted by emerging data. It has been demonstrated that combining genetic markers like APOE genotype with plasma biomarkers like Aβ42/Aβ40 ratios and p-tau increases diagnostic specificity and accuracy. By combining these fluid biomarkers with cutting-edge imaging methods like PET and MRI, a more thorough evaluation is produced, making it easier to identify at-risk patients before symptoms appear. Assay variability, high imaging costs, and confounding variables like age and comorbidities are still problems, though. Standardizing procedures, creating affordable blood-based assays, and using machine learning to adjust for confounders are all necessary to address these problems.
Challenges in standardization and interpretation
The application of AD biomarkers in clinical practice presents several challenges, including assay standardization, measurement variability, and result interpretation. Variability among platforms and labs is caused by a lack of reference materials and standardized techniques. 127 Assays are being harmonized for improved repeatability and dependability through initiatives such as the Alzheimer's Association Global Biomarkers Standardization Consortium or GBSC. 128 Age, sex, comorbidities, and genetics are among the characteristics that must be taken into account when interpreting biomarker results because they can affect levels and diagnostic accuracy. 129 The interpretation of anomaly cutoff values is complicated by the fact that they differ among research and populations. 130 Because biomarkers are dynamic, they must be validated and monitored over an extended period of time in a variety of cohorts in order to demonstrate their predictive and therapeutic relevance.
The potential for discrepancy or overlap in various disease stages or subtypes makes integrating several biomarkers into diagnostic algorithms difficult. 131 MCI and subjective cognitive decline, for example, may have different biomarker profiles, which represent a variety of underlying diseases. Increasing the precision of diagnosis and making better treatment decisions requires harmonizing biomarker data and considering individual variability.
Therapeutic implications
Targeting biomarkers in drug development
Biomarkers are essential to the development of treatments for AD because they help identify possible treatment targets and evaluate the effectiveness of those treatments. With tactics like BACE inhibitors and anti-Aβ antibodies targeted at lowering Aβ aggregation and plaque formation, key biomarkers like tau and Aβ proteins are at the center of current therapeutic research.132,133 Furthermore, early-stage clinical trials indicate potential for tau-targeted treatments, such as microtubule-stabilizing medicines and tau aggregation inhibitors. 103 Combining treatments that target tau and Aβ may increase the efficacy of treatment. 134 While MRI methods aid in tracking the course of the disease, neuroimaging biomarkers, such as tau-specific radiotracers and PET scans containing Aβ, provide important information about target engagement and therapy response. 135
Fluid-based biomarkers, such as the levels of tau and Aβ in CSF, are useful for evaluating the effectiveness of treatment and offer important insights into pathological processes, such as tau phosphorylation and Aβ clearance. 136
An important development in AD care is the use of personalized treatment plans that are based on each patient's genetic composition, disease pathology, and response to therapy. These biomarker-profile-based tactics seek to increase therapy efficacy while reducing adverse effects. For instance, more focused therapies can be informed by the discovery of genetic variants like APOE ε4 in conjunction with CSF levels of p-tau and Aβ. 137 Promising outcomes are observed with biomarker-guided therapy, such as amyloid-reducing medications for people with high Aβ levels. 131 Furthermore, patients with significant tau disease may benefit most from tau-targeted therapies. 138 Personalized therapy is crucial for the best results since genetic factors, like the APOE ε4 genotype, affect treatment choices in addition to illness risk. 135
Because genetic testing and personalized treatment create issues of privacy, informed consent, and potential discrimination based on genetic information, ethical considerations are essential. For personalized medicines to be successfully used in the treatment of AD, these ethical concerns must be addressed.52,139 Adaptive trial designs that incorporate biomarker-driven endpoints improve the detection of treatment effects, and the use of biomarkers in clinical trials also improves patient selection and trial design. 140 Tracking therapy responses, illness progression, and the appearance of biomarkers suggestive of treatment resistance or side effects is made easier with longitudinal monitoring of biomarker profiles.135,141
Future directions and research opportunities
As research on AD progresses, a number of intriguing areas for further study have surfaced, which could improve clinical treatment, uncover new therapeutic targets, and deepen our understanding of AD.
Early identification using innovative biomarkers
One of the main areas of research is creating biomarkers that identify AD pathology early, before clinical symptoms manifest. Digital biomarkers, blood-based biomarkers, and retinal imaging are examples of emerging technologies that provide non-invasive techniques for early detection, enhancing diagnosis and facilitating prompt action. 142 Furthermore, there is a great deal of promise for enhancing the sensitivity and specificity of early detection through the integration of artificial intelligence and machine learning for biomarker-based diagnostics, enabling more precise and customized evaluations. 143
Investigating non-amyloid and non-tau disorders
Non-amyloid and non-tau diseases in AD are receiving more and more attention in research. Disease development and heterogeneity may be influenced by vascular variables, neuroinflammation, synaptic dysfunction, and other proteinopathies.68,144 Finding biomarkers for these other pathways may result in new therapeutic approaches that go beyond treatments that target tau and amyloid. Additionally, investigating how neuroinflammation and synaptic loss contribute to the development of disease may be essential to creating treatments that target these pathophysiological pathways.
Environmental and lifestyle factors
Modifiable risk factors that impact AD risk and cognitive decline include social behavior, food, physical health, and cognitive pairing, according to epidemiological research.145,146 Promising paths for dementia prevention and public health initiatives are provided by comprehending these relationships and creating interventions to reduce risk factors. To verify the prediction ability of these lifestyle-related biomarkers and demonstrate their function in long-term illness prevention, longitudinal studies will be essential.
Genetic research and precision medicine
Personalized treatment strategies based on genetic, molecular, and clinical profiles are made possible by developments in precision medicine and genetics. Risk assessment, prognosis, and therapy selection are influenced by risk genes such as APOE, TREM2, and SORL1.23,98,147 Finding patient subgroups for targeted treatments may be possible by combining genetic data with biomarker and clinical phenotypic information. Furthermore, biomarker profiles and genetic studies may help direct therapeutic modifications, improving the applicability and effectiveness of treatments for people with certain genetic predispositions.
Novel approaches to research
Novel approaches that shed light on the intricate relationships between genetic, molecular, and environmental variables in AD pathogenesis include network neuroscience, machine learning, and multi-omics approaches.24,148 These techniques can identify therapy targets, uncover new pathways and develop models that predict the course of a disease and the effectiveness of a treatment. Validating these techniques’ long-term prediction potential as well as their capacity to monitor the course of the disease and its response to treatment requires longitudinal research.
Conclusion
The development of biomarker research has the potential to significantly change the diagnosis and treatment of AD, which is still a major global health concern. The most promising biomarkers, including as tau, Aβ, and neuroinflammatory markers, are already showing promise in the creation of tailored therapies, early identification, and tracking the course of disease. When combined, these biomarkers have the potential to produce a more comprehensive and reliable diagnostic profile for AD, which would enhance patient outcomes and allow for prompt therapies.
For improved diagnostic accuracy, future studies should concentrate on creating combinatory biomarker panels that combine fluid-based biomarkers, neuroimaging, and genetic data.
Additionally, investigating other pathophysiological pathways in addition to amyloid and tau, such as neuroinflammation and synaptic dysfunction, may result in new therapeutic approaches that focus on the various mechanisms driving AD. Validating the prediction ability of biomarkers, guaranteeing their efficacy in clinical settings, and facilitating the discovery of novel therapeutic targets will all depend on longitudinal research. As studies continue, a better knowledge of AD biomarkers will help to improve current therapies and open the door for novel ideas that may drastically change how the illness develops.
Footnotes
Acknowledgments
The authors gratefully acknowledge the funding of the Deanship of Graduate Studies and Scientific Research, Jazan University, Saudi Arabia, through project number: (RG24-L07).
ORCID iDs
Author contributions
Ruqaiya Jamal (Conceptualization; Methodology; Project administration; Visualization; Writing—original draft; Writing—review & editing); Mohammad Abuzar Shaikh (Conceptualization; Methodology; Project administration; Visualization; Writing—original draft; Writing—review & editing); Mohamad Taleuzzaman (Supervision; Visualization; Writing—original draft; Writing—review & editing); Ziyaul Haque (Writing—original draft; Writing—review & editing); Mohammed Albratty (Visualization; Writing—original draft; Writing—review & editing); Md Shamsher Alam (Visualization; Writing—original draft; Writing—review & editing); Hafiz A. Makeen (Funding acquisition; Writing—review & editing); Khalid Zoghebi (Visualization; Writing—original draft; Writing—review & editing); Safaa Fathy Saleh (Visualization; Writing—original draft; Writing—review & editing).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Deanship of Graduate Studies and Scientific Research, Jazan University, Saudi Arabia, through project number: (RG24-L07).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.