
Abstract
Background
Few studies have examined the inverse relationship between dementia and falls, i.e., whether falls before dementia are a herald of dementia.
Objective
We aimed to explore the relationship between fall experiences and risk of dementia, assessing how factors like APOE ε4 allele, family history of dementia, comorbidities, traumatic brain injury (TBI), and frailty modify this association.
Methods
We used data from the UK Biobank. We used Cox proportional hazards models to estimate the HRs and 95% CIs for the association between falls and all-cause dementia, Alzheimer's disease (AD), vascular dementia (VaD), and non-Alzheimer/non-vascular dementia (NAVD). The synergistic effects of fall experiences and APOE, dementia family history, cardiovascular disease (CVD), diabetes, TBI, frailty on dementia were also investigated.
Results
Totally, 403,502 participants were included. 99,832 people experienced at least one fall, and 4143 dementia cases were observed. People who experienced falls had a higher risk of all-cause dementia, AD, VaD, and NAVD, with HRs (95% CIs) of 1.71(1.61, 1.83), 1.33 (1.20, 1.47), 2.00 (1.74, 2.29), and 2.03 (1.84, 2.24), respectively. The risk of dementia increased with the number of falls and with falls occurring later in life (after age 60). Fall experiences had a synergistic effect with dementia risk factors (APOE ε4 allele, family history of dementia and comorbidities), TBI, and frailty, collectively increasing the risk of dementia.
Conclusions
Falls before dementia were linked to a higher risk of dementia. The risk escalated with more falls and falls after age 60. Combining falls with risk factors further amplified dementia risk.
Introduction
Dementia has become a huge global public health challenge, affecting an estimated 150 million people worldwide by 2050. 1 Dementia is also the leading cause of disability for people over 65 years of age worldwide in the 21st century.2–4 Given that there is currently no cure for dementia, identifying modifiable risk factors remains critical to advancing prevention and management strategies.
Globally, falls are a major public health problem. According to the World Health Organization (WHO), a fall is defined as an event that results in a person resting inadvertently on the ground, the floor, or other lower levels. 5 It is estimated that 684,000 fatal falls occur each year, which is the leading cause of accidental or unintentional injury deaths among older adults.6,7 Therefore, reducing and preventing the occurrence of falls plays a crucial part among older adults.
In older adults, falls and dementia often coexist and can affect each other. However, most research in this area has focused on how dementia is linked to an increased risk of falls.8–10 One longitudinal study has shown that dementia participants experienced nearly eight times more incident falls than controls. 11 Meanwhile, another major study has found that people with cognitive impairment have a twice higher risk of falls than those with normal cognition. 12 Few studies have examined the inverse relationship between dementia and falls, i.e., whether falls before dementia are a predictor of dementia. Using data from Hispanic population, Padubidri et al. examined whether falls were associated with subsequent cognitive decline, measured by Mini-Mental State Examination (MMSE) scores over six years. 13 They found two or more falls were independently associated with a steeper decline in cognition. 13 In addition, some studies have suggested that falls are also associated with the risk of developing motoric cognitive risk syndrome,14–16 a pre-dementia syndrome. 17 However, few studies have examined the relationship between falls and subsequent dementia.
We aimed to evaluate the association between falls and the onset of various forms of dementia, including all-cause dementia, Alzheimer's disease (AD), vascular dementia (VaD), and non-Alzheimer/non-vascular dementia (NAVD). Additionally, we also explored how various covariates may shape this relationship, including APOE ε4 allele carrier status, family history of dementia, comorbidity condition, traumatic brain injury (TBI), and frailty status.
Methods
Study design and participants
The UK Biobank is a prospective population-based cohort, recruited over 500,000 volunteers aged 40–69 years between 2006 and 2010. Individuals were invited to attend one of the 22 centers across England, Scotland, and Wales for baseline assessment. Written informed consent was obtained for collection of questionnaire and biological data. UK Biobank has approval from the North West Multicenter Research Ethics Committee (https://www.ukbiobank.ac.uk/learn-more-about-uk-biobank/about-us/ethics). This research was conducted under UK Biobank application number 227947. By utilizing the UKB baseline data along with subsequent health outcome follow-up data (until 2022), we have access to a wide range of demographic, lifestyle, and health-related variables essential for our analysis. A prospective analysis was adopted based on participants with no dementia at baseline, and if a participant had dementia during follow-up and also experienced falls, his/her falls must occur before dementia. We excluded participants with missing data on key covariates, including age, sex, ethnicity, education, income, cigarette smoking, alcohol drinking, leisure activities, physical activities, body mass index (BMI), diabetes status, hypertension status, cardiovascular disease (CVD) status, dementia family history, and APOE ε4 allele carrier status at baseline, leading to a final cohort with 403,502 participants included for analysis (Figure 1).
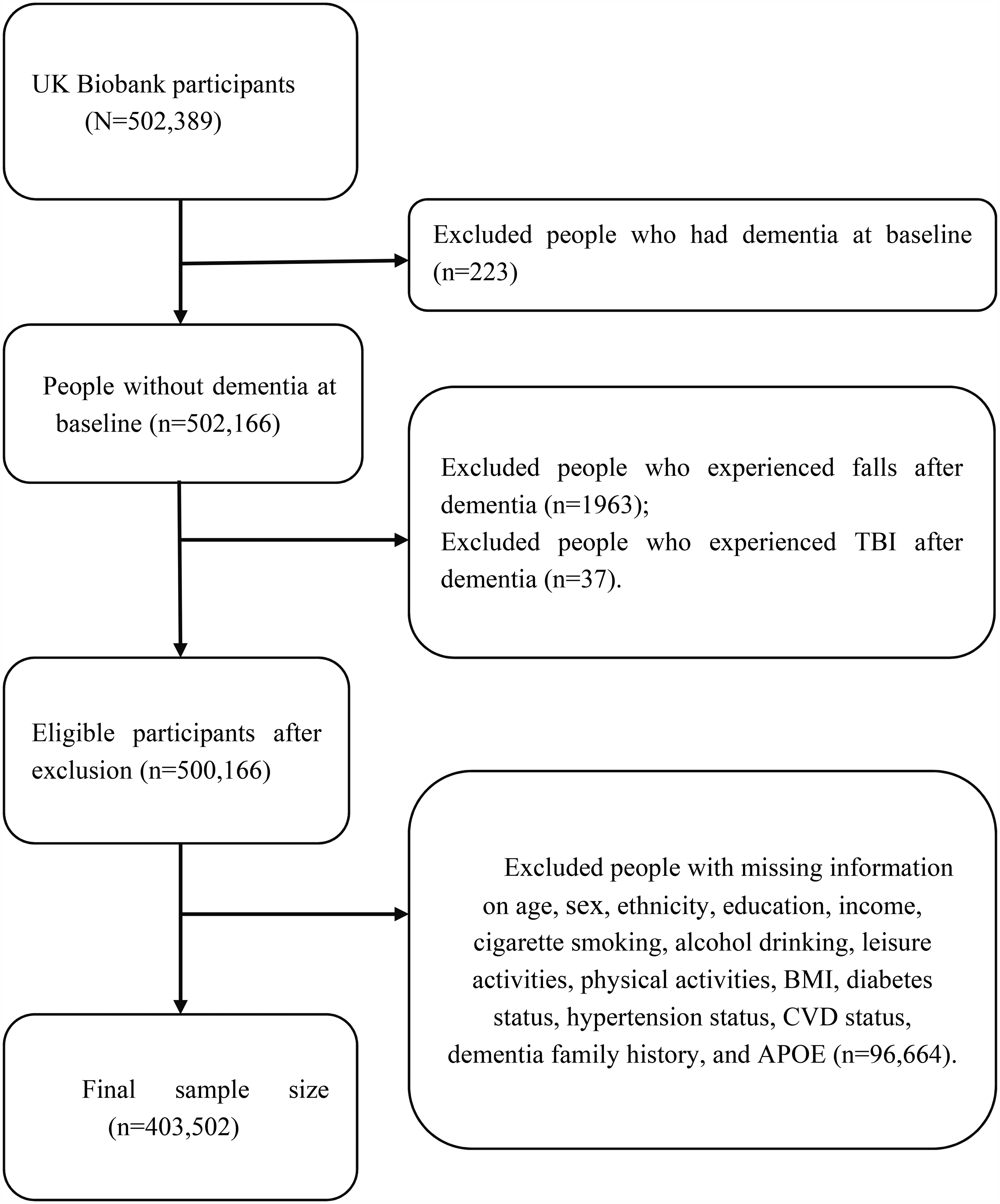
Flow diagram of study participant selection.
Exposure and outcome variables
The exposure variable was the occurrence of falls. Data on falls came from two sources, one was from hospital medical records and the other from self-reported records. The first occurrence of inpatient fall was defined by the International Classification of Diseases 10th Edition (ICD-10) codes W00-W19, or defined by ICD-9 codes E880-E888. The self-reported data was obtained by asking the participants “In the last year have you had any falls?” The possible answers were “no falls” “only one fall” and “more than one fall”.
The outcome variable was incident all-cause dementia, including dementia subtypes of AD, VaD, and NAVD. The ICD-10 codes F00, F01, F02, F03, G30, G31.0, G31.1, G31.8, and ICD-9 code 290.1 were used to identify participants with all-cause dementia if one or more of these codes were recorded as a primary or secondary diagnosis. Incident AD was defined by ICD-10 codes F00, G30, and ICD-9 code 290.1. Incident VaD was defined by ICD-10 code F01. Incident NAVD was defined by ICD-10 code F02, F03, G31.0, G31.1, G31.8. Outcome adjudication for incident dementia was conducted by the UK Biobank Outcome Adjudication team.
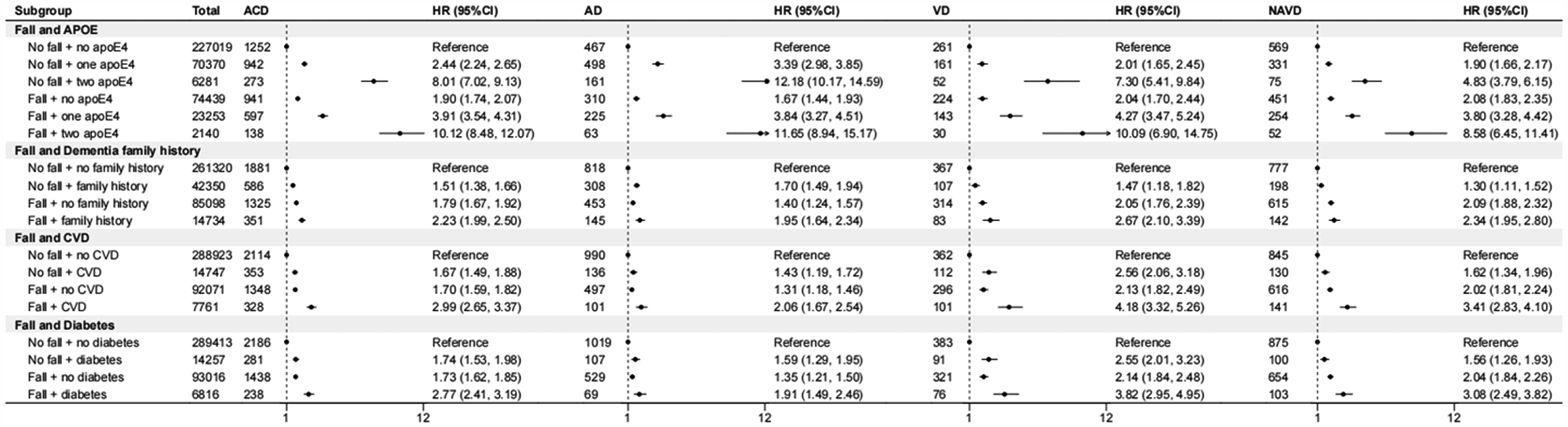
The synergistic effect of fall experiences and APOE, dementia family history, CVD, diabetes on dementia. ACD: all-cause dementia; AD: Alzheimer's disease; VD: vascular dementia; NAVD: non-Alzheimer disease/non-vascular disease.
Covariates
We included the following factors in the analyses as covariates according to evidence from previous studies: age at baseline, sex, ethnicity, years of education, income level, smoking status, alcohol status, physical activity level, leisure activity, BMI, hypertension status, diabetes status, CVD status, dementia family history, and APOE ε4 allele carrier status. 13 Sex was divided into male and female. Ethnicity was categorized as white and non-white. Years of education was categorized as ≤10, 11–12, and >12 years. Income level was categorized into four groups: level 1 (i.e., low income, less than £18,000), level 2 (£18,000 to £30,999), level 3 (£31,000 to £51,999), and level 4 (more than £52,000). 18 Smoking status was categorized as current, former, or never smokers. Alcohol status was categorized as current, former, or never drinkers. Physical activity level was categorized as light (<600 metabolic equivalent (MET)-min/week), moderate (600 to <3000 MET-min/week) and high (≥3000 MET-min/week) based on standard scoring criteria. Leisure activity was categorized as yes or no. BMI was categorized according to the WHO criteria as underweight (<18.5 kg/m2), normal (18.5 to 24.9 kg/m2), overweight (25.0 to 29.9 kg/m2), and obese (≥30 kg/m2). Hypertension, diabetes, and CVD status was dichotomized as present or absent based on self-report at baseline. Dementia family history was classified into yes or no. APOE ε4 allele carrier status was based on two single nucleotide polymorphisms (SNPs): rs7412 and rs429358. Participants with APOE ε4 allele (ε3/ε4, ε4/ε4, and occasionally ε2/ε4 genotypes) were compared with those with the ε2/ε2, ε2/ε3, or ε3/ε3 genotype. Detailed definitions of covariates were listed in Supplemental Table 1.

The synergistic effect of fall experiences and TBI, frailty on dementia. ACD: all-cause dementia; AD: Alzheimer's disease; VaD: vascular dementia; NAVD: non-Alzheimer disease/non-vascular disease.
Traumatic brain injury and frailty
TBI is defined as an alteration in brain function, or other evidence of brain pathology, caused by an external force. 19 In this study, TBI was identified using ICD-10 code S06 and corresponding ICD-9 codes 801, 802, and 850–854.
Frailty was evaluated based on the Fried frailty phenotype (FP), a framework initially proposed by Fried et al. in the Cardiovascular Health Study and subsequently confirmed for validity using data from the UK Biobank. 20 The FP model incorporates five clinical indicators: unintended weight loss, fatigue, diminished physical activity, reduced walking speed, and decreased grip strength (indicative of weakness). Individuals exhibiting three or more of these characteristics were categorized as with frailty, those with one or two features were classified as in pre-frailty, and individuals showing none of the criteria were considered robust. The detailed definitions of each clinical feature of FP were shown in Supplemental Table 2.
Statistical analyses
Baseline characteristics were presented as means and standard deviation (SD) for continuous variables and as percentages (%) for categorical variables. Hazard ratios (HRs) and corresponding 95% CIs for the risk of dementia were estimated for people with a history of falls and compared with people with no history of falls using Cox proportional hazards regression models. We also considered age when the fall occurred and number of falls occurred. For participants who experienced dementia, follow-up time was calculated as their age at the time of dementia diagnosis minus baseline age; for participants who did not experience dementia, follow-up time was defined as their age at last follow-up (censored date) minus baseline age. All models were adjusted for age at baseline, sex, ethnicity, years of education, income level, smoking status, alcohol status, physical activities, leisure activities, BMI, hypertension status, diabetes status, CVD status, dementia family history, and APOE ε4 allele carrier status. Furthermore, we did several joint effect analyses. We combined falls with APOE ε4 allele status, family history of dementia, CVD, diabetes, TBI, and frailty to analyze their joint effects on dementia. Further, we analyzed the mediating role of frailty between falls and dementia, based on the methods of Baron and Kenny. 21 The relationship between falls and dementia may be bidirectional, with cognitive impairment contributing to increased risk of falls. 22 To minimize the potential for reverse causation, a sensitivity analysis was conducted, including only dementia cases that occurred at least three years after the fall. Considering the two data sources—hospital-recorded and self-reported—we performed separate analyses to assess the consistency of findings.
Ethics approval and consent to participate
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. As part of the UK Biobank recruitment process, written informed consent was obtained from all individual participants included in the study.
Results
Characteristics of participants
The baseline characteristics of the cohort were described in Table 1. Overall, 403,502 participants were included in the analysis, with a mean (SD) age at baseline of 56.4 (8.1) years, and 54.1% were females. The majority of them were white (95.3%). During the study period, 99,832 (24.7%) people experienced at least one fall, and 4143 (1.03%) dementia cases were observed. Compared to those who did not experience a fall, individuals who did were more likely to be female, have lower education and income levels, and suffer from obesity and hypertension. Compared to those who had no dementia, those who had dementia were more likely to be older, have lower education and income levels, carry APOE ε4 alleles and have family history of dementia.
Characteristics of participants by fall and dementia experienced or not, n (%).
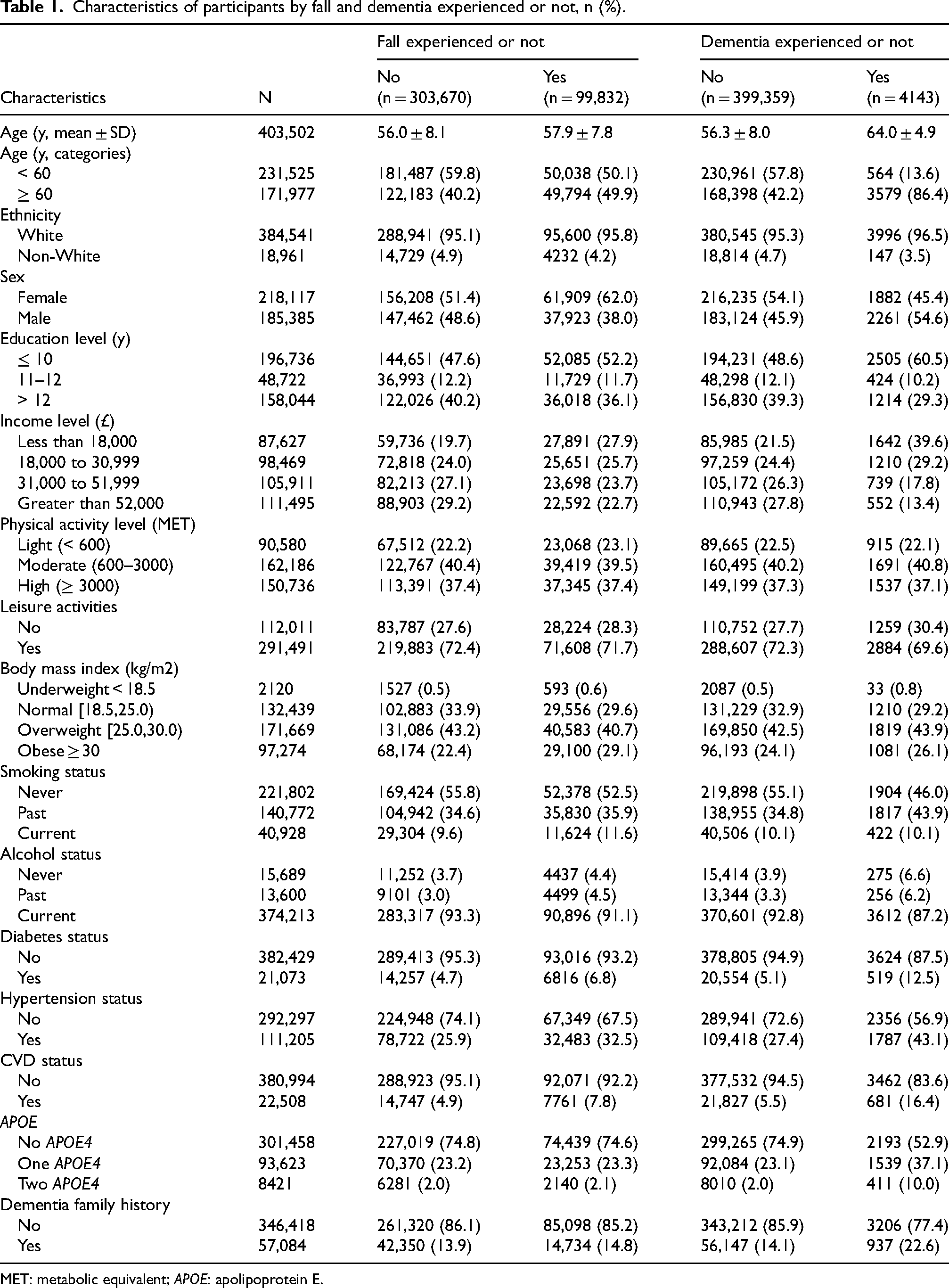
MET: metabolic equivalent; APOE: apolipoprotein E.
Association between fall experiences and dementia
Compared to people who did not experience any falls, people who experienced falls had a higher risk of all-cause dementia, AD, VaD, and NAVD, with HRs (95% CIs) of 1.71 (1.61, 1.83), 1.33 (1.20, 1.47), 2.00 (1.74, 2.29), and 2.03 (1.84, 2.24), respectively. The risk of dementia increased with number of falls, from 1.28 (1.17, 1.39) in people with one fall to 1.89 (1.72, 2.08) in people with two falls or more. After stratifying by the age at which falls occurred, we found that individuals who experienced a fall after the age 60 had a higher risk of dementia compared to those who had a fall before age 60 years (1.94, 1.61–2.34). Similar results were observed in relation to subtypes of dementia (Table 2). In a sensitivity analysis, when only fall events that occurred at least three years before dementia were included, we found similar findings with the main analyses, although the magnitude of the effect size was slightly reduced (Table 3). Separate analyses based on data sources (hospital records and self-reported data) revealed a significant association between falls and subsequent dementia in both groups, aligning with our main findings (Supplemental Tables 3 and 4).
Hazard ratios (HRs) and 95%CIs between fall experiences and dementia.
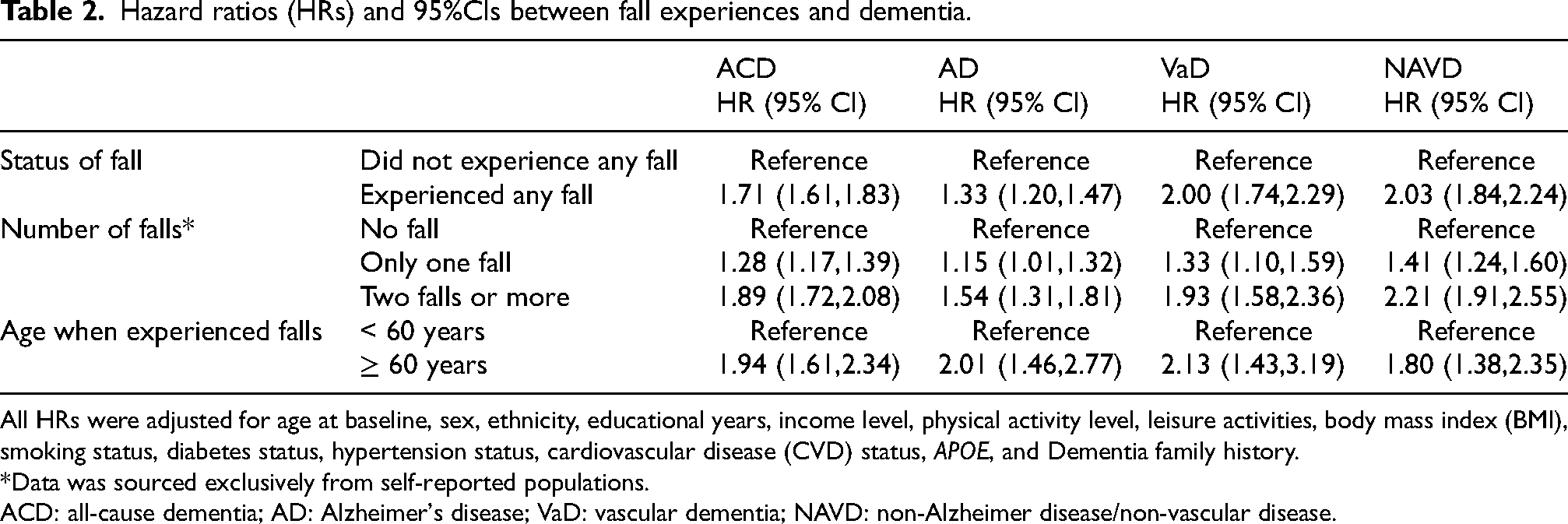
All HRs were adjusted for age at baseline, sex, ethnicity, educational years, income level, physical activity level, leisure activities, body mass index (BMI), smoking status, diabetes status, hypertension status, cardiovascular disease (CVD) status, APOE, and Dementia family history.
Data was sourced exclusively from self-reported populations.
ACD: all-cause dementia; AD: Alzheimer's disease; VaD: vascular dementia; NAVD: non-Alzheimer disease/non-vascular disease.
Association between fall experiences and dementia when falls occurred at least three years before dementia: sensitivity analysis.
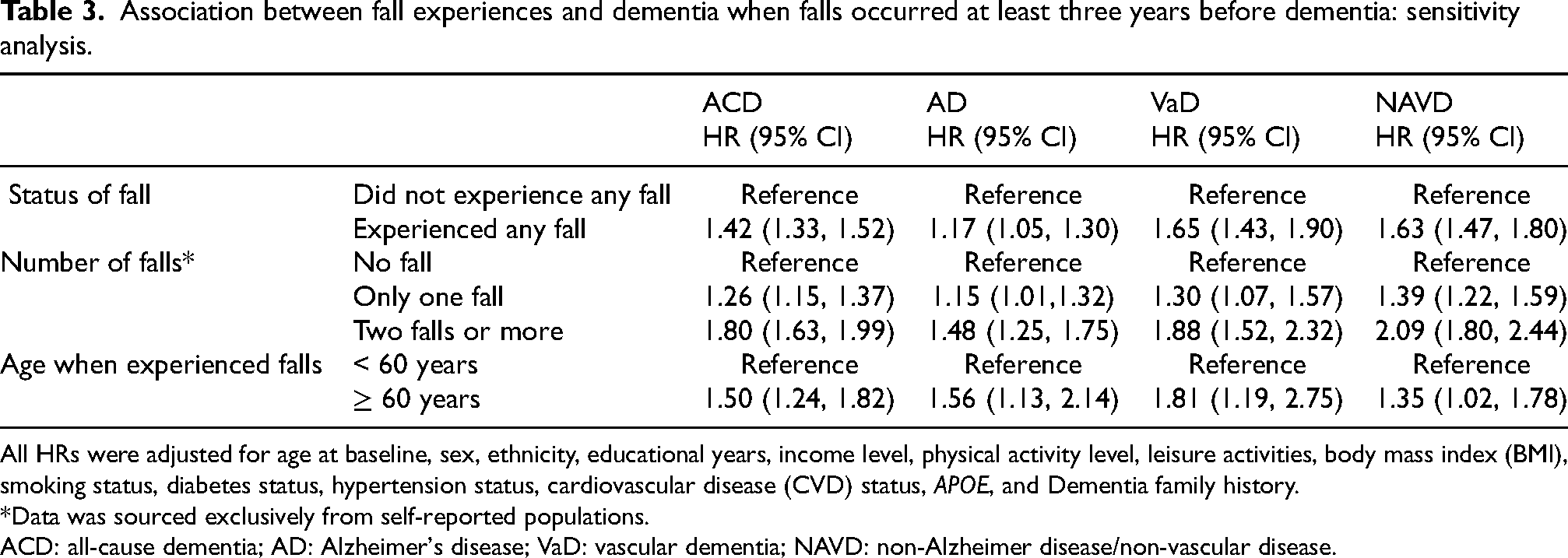
All HRs were adjusted for age at baseline, sex, ethnicity, educational years, income level, physical activity level, leisure activities, body mass index (BMI), smoking status, diabetes status, hypertension status, cardiovascular disease (CVD) status, APOE, and Dementia family history.
Data was sourced exclusively from self-reported populations.
ACD: all-cause dementia; AD: Alzheimer's disease; VaD: vascular dementia; NAVD: non-Alzheimer disease/non-vascular disease.
Synergistic effect of fall experiences and dementia risk factors on dementia
When fall experiences combined with APOE ε4 alleles status, family history of dementia, CVD and diabetes status, we observed that these risk factors synergistically increased the risk of dementia with falls, with HRs (95% CIs) of 10.12 (8.48, 12.07), 2.23 (1.99, 2.50), 2.99 (2.65, 3.37) and 2.77 (2.41, 3.19), respectively (Figure 2).
Synergistic effect of fall experiences and TBI, frailty on dementia
When fall experiences combined with TBI status and frailty status, we found a joint effect on dementia. The joint effect of falls and TBI on dementia was 3.37 (2.67, 4.25). The joint effect was mainly manifested in the association with VaD. The joint effect of falls and pre-frailty, frailty were 1.96 (1.79, 2.15) and 3.07 (2.67, 3.54), respectively (Figure 3). The mediation analysis showed that the relationship between fall experiences and dementia was 14% mediated by frailty (Figure 4).
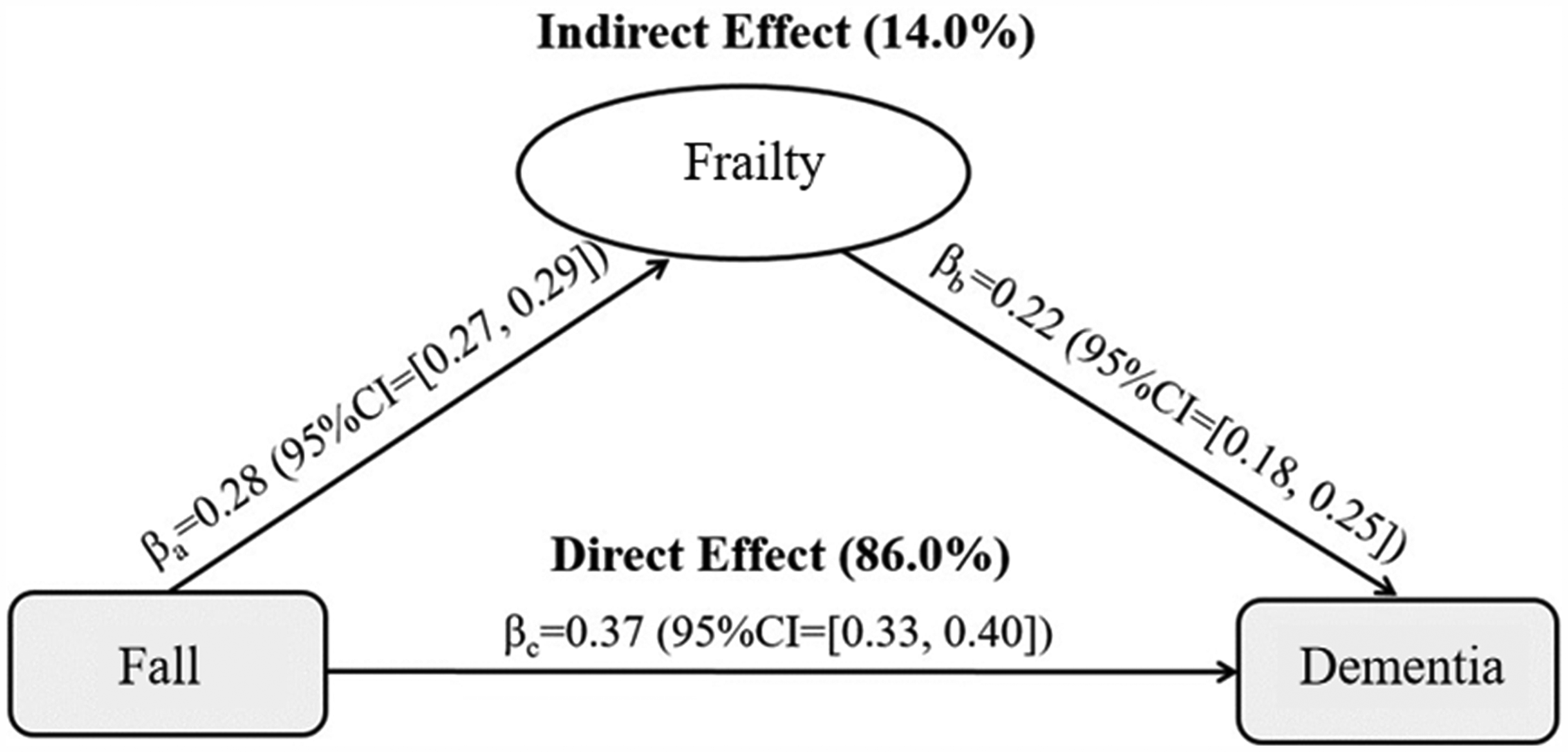
The mediated effects of frailty on the pathway between falls and dementia.
Discussion
Summary of findings
In this population-based cohort study, a history of falls was associated with an increased risk of all-cause dementia, AD, VaD, and NAVD compared with those without experiencing falls. The risk of dementia increased with the number of falls and with falls occurring later in life (after age 60). Falls combined with dementia risk factors (such as APOE genotype, family history of dementia, comorbidities), TBI, and frailty synergistically increased the risk of dementia.
It has been proposed that the association between falls and cognitive decline appeared to be driven mainly by the occurrence of at least two falls. 13 Our results also support this hypothesis. Having experienced more than one fall during the survey period was associated with a greater risk of dementia. Single fall may be caused by fainting, environmental hazards, and high-risk activities,23,24 while multiple falls are more likely to be the result of intrinsic impairments such as poorer sensorimotor and poorer cognitive functions.23,25 Both our research and previous studies have indicated that falls, especially multiple falls, may be a marker of declining cognitive abilities in older adults. Although falls may be a common event at any age, our study showed that the older group (≥60 years) had a higher risk of developing dementia after a fall compared to the younger group (<60 years). This suggests that falls occurring at an older age have a stronger association with the risk of future dementia. This conclusion may reflect the effects of age on various systems in the body. Aging is companied by a decrease in bone density, muscle strength, and balance ability, all of which elevate the risk of falls. After a fall, older adults often have a more limited capacity for physical recovery compared to younger individuals, potentially leading to more severe consequences such as head injuries or intracranial hemorrhages, thereby increasing the risk of dementia.
Falls, TBI, and dementia
Previous studies mainly focused on the link between fall-related brain injury and subsequent dementia, i.e., TBI and dementia.26–28 It has been well established that TBI is associated with an increased risk of dementia, and the ORs ranged from 1.25 to 1.63.29–31 Similar with previous studies, we observed people with TBI had an increased risk of all-cause dementia, AD, VaD, and NAVD compared with those without TBI. Also, there was a synergistic effect of them on dementia, especially to VaD, with a HR (95%CI) of 4.29 (2.77, 6.66). More than 60% of TBI in older adults results from falls. 32 Additionally, the prevalence of fall-related TBI has increased in recent decades. 33 Preventing falls and managing their consequences is pivotal in mitigating the risk of TBI and subsequent dementia.
Falls, frailty, and dementia
There is growing evidence showing that frailty is independently associated with an increased risk of poor health outcomes in older adults, including subsequent falls 34 and cognitive impairment. 35 The relationship between frailty and falls was closely linked. On one hand, frailty led to various physical and cognitive declines, including muscle weakness, reduced mobility, slower walking speed, and diminished cognitive abilities. These factors collectively increased the risk of falls. On the other hand, falls were not only a direct consequence of frailty but also a significant factor leading to further frailty. The interrelationship between frailty and falls underscored the importance of preventive measures. It warrants taking measures such as enhancing muscle strength, improving balance abilities, and increasing home safety, which not only lower the risk of falls but also alleviate the severity of frailty.
Potential mechanisms
The mechanisms linking falls to dementia are unclear, though several possibilities have been suggested. First, some risk factors associated with dementia are also risk factors for falls, such as older age, frailty, obesity, cardiovascular disease, diabetes, and higher burden of white matter hyperintensities in the brain. 36 Therefore, shared risk factors may be antecedent or causal pathways between falls and dementia. Second, falls may lead to behavioral changes that indirectly lead to cognitive decline. For example, older people choose to reduce their physical activities due to fear of falling, which causes certain social isolation and leads to depression. 37 Depression is thought to increase the risk of dementia. Research has found that depressive symptoms preceded memory decline in later life, and higher depressive symptoms were associated with accelerated memory decline. 38 It has been documented that depression plays a mediating role in the association between falls and cognitive decline. 13 Finally, TBI from falls can ultimately lead to cognitive decline in older adults, especially if there is damage to the frontal lobes. There has been substantial research undertaken on the potential mechanisms for dementia linked to TBI, including tau and amyloid-βpathology, chronic neuroinflammation, vascular damage, and white matter degeneration.39–41 Notably, females are more prone to falls than males, likely due to lower muscle strength, 42 balance, 42 and postmenopausal hormonal changes 43 that increase the risk of osteoporosis and fractures.
Strengths and limitations
One of the strengths of our study was the large sample size, which enabled us to conduct some joint analyses to further explore the synergistic effect of falls and risk factors, TBI, frailty on dementia. Second, both dementia outcomes and the vast majority of fall exposures were ascertained from hospital-associated medical records to avoid self-reported bias. Despite these strengths, several limitations should be noted. First, the generalizability of our findings to other populations is limited because 95.4% of the involved population was white. Second, UK Biobank participants were relatively healthy compared to the general population, such as with lower smoking rates and higher educational attainment, which may also limit the extrapolation of our results. Third, some of the fall events might have been due to accidents rather than health status, which we had no way to exclude from the analysis, possibly leading to some bias. Fourth, while we adjusted for a wide range of potential confounders and excluded subjects whose dementia events occurred less than three years after the fall to avoid reverse causation, other unadjusted factors, such as depression and visual impairment, could have influenced our conclusions. Finally, the use of linkages to electronic health records may have higher specificity but lower sensitivity.
Conclusions
Falls, especially in later life may serve as a predictive factor for the onset of dementia, acting as a harbinger for future cognitive decline. Experiencing falls, particularly those resulting in TBI and frailty, could be intricately linked to the early stages of neurodegenerative processes that culminate in dementia. This connection underscores the importance of closely monitoring and addressing fall incidents among older adults, not only to prevent immediate physical harm but also as a potential strategy for early identification and intervention in the progression towards dementia. From a primary care perspective, inquiring about falls allowed for quick dementia assessments. Clinically, repeated falls signaled a high future dementia risk, highlighting the importance of early detection and prevention to reduce dementia's healthcare burden. Public health efforts focused on fall prevention can significantly reduce the risk factors for dementia caused by falls.
Supplemental Material
sj-docx-1-alz-10.1177_13872877251333799 - Supplemental material for The fall-dementia connection: Synergistic effects of falls with genetic and health risk factors
Supplemental material, sj-docx-1-alz-10.1177_13872877251333799 for The fall-dementia connection: Synergistic effects of falls with genetic and health risk factors by Zhongxuan Wang, Qi Wang, Chunying Fu, Xiang Li, Luyi Zhang, Xiaoyu Zhang and Dongshan Zhu in Journal of Alzheimer's Disease
Footnotes
Acknowledgments
The authors would like to express their sincere gratitude to all participants in this study.
Ethical considerations
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Consent to participate
As part of the UK Biobank recruitment process, written informed consent was obtained from all individual participants included in the study.
Consent for publication
All participants agree to publish.
Author contributions
Zhongxuan Wang: Writing - original draft.
Qi Wang: Data curation.
Chunying Fu: Conceptualization.
Xiang Li: Formal analysis.
Luyi Zhang: Methodology.
Xiaoyu Zhang: Investigation.
Dongshan Zhu: Writing - review & editing.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the National Natural Science Foundation of China (82273702), the National Key Research and Development Program of China (2022YFC2703804), Science Fund Program for Excellent Young Scholars of Shandong Provence (Overseas) (2022HWYQ-030), Taishan Scholars Project Special Fund (tsqnz20221103), and the Shandong University Distinguished Young Scholar program (202099000066).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.