
Abstract
Background:
Type 2 diabetes (T2D) and hypertension (HTN) are well-known modifiable risk factors for dementia, but their intricate attributes accounting for dementia development has not been clearly delineated.
Objective:
We conducted this study to investigate and compare the effects of T2D and HTN on dementia risk.
Methods:
We screened data of matched pairs of patients with T2D or HTN between January 1, 2000 and December 31, 2017 from Taiwan’s National Health Insurance Research Database. Fine and Gray’s subdistribution hazard models were used for calculating the risk of dementia.
Results:
Patients with T2D and subsequent HTN were associated with significantly higher risks of all-cause dementia (aHR 1.51, 95% CI 1.25–1.83) and vascular dementia (aHR 2.30, 95% CI 1.71–3.13) compared with those without subsequent HTN. Patients with HTN and subsequent T2D were associated with significantly higher risks of all-cause dementia (aHR 1.15, 95% CI 1.08–1.21), vascular dementia (aHR 1.25, 95% CI 1.62–1.34), and other dementia (aHR 1.31, 95% CI 1.03–1.66) compared with those without subsequent HTN. The subgroups of male and female patients, age of 50–69 and 70–90 years with subsequent comorbidity were associated with significantly higher risks of all-cause dementia and vascular dementia than those without subsequent comorbidity.
Conclusion:
This nationwide cohort study demonstrated that patients with T2D and subsequent HTN had association with higher risks of all-cause dementia and vascular dementia, and those with HTN and subsequent T2D were associated with higher risks of all-cause dementia, vascular dementia, and other dementia.
INTRODUCTION
Dementia is characterized by a decline in memory, language skills, attention, spatial orientation, and task execution [1]. This senescence-related disease imposes a significant burden on the families and caregivers [1, 2]. An increase in global population aging has increased the incidence of dementia from 19.7 million in 1990 to 51.6 million in 2019 [3]. Old patients with dementia often have many comorbidities, disability, frailty, and higher mortality; their cost of health care imposes a huge burden globally [4]. While research on curing dementia is not advanced yet, but if we can identify and improve the modifiable risk factors for dementia, we may then be able to reduce the associated healthcare burden.
Both diabetes mellitus (DM) and hypertension (HTN) are well-known modifiable risk factors for dementia [1]. Higher glucose levels are associated with a higher risk of dementia, even in persons without diabetes [5]. DM and dementia are closely related [6]. Chronic HTN can cause stiffness of large and small blood vessels, increasing the possibility of a stroke; therefore, it has been considered an important risk factor for dementia [2, 7]. Though the meta-analysis of randomized control studies has not revealed that intensive glucose control could reduce the risk of cognitive impairment or dementia [8], but several meta-analyses of randomized control trials have suggested that intensive blood pressure lowering does reduce the risk of cognitive decline and potentially dementia [9, 10]. Because there is no effective treatment for dementia, prevention is critical. Both DM and HTN are considered modifiable risk factors for dementia. It is important to know whether preventing HTN in people with DM, or preventing DM in people with HTN, can reduce the dementia risk. Therefore, we conducted this study to investigate whether 1) newly diagnosed type 2 diabetes (T2D) in hypertension patients, 2) newly diagnosed HTN in T2D patients, and 3) history of HTN versus history of T2D in patients with both conditions could influence the risk of dementia or not.
MATERIAL AND METHODS
Study population
We analyzed data of persons with newly diagnosed T2D or HTN from the National Health Insurance Research Database (NHIRD) [11] between January 1, 2000 and December 31, 2017. The NHIRD comprises medical records of the National Health Insurance (NHI) from 1995 to the present. It contains information on patient age, sex, residential area, medical management, and diagnosis according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) and ICD-10-CM codes. This study used the 2000 Longitudinal Generation Tracking Database (LGTD 2000) containing the sampled files of 2 million people from the NHIRD. Our study was approved by the Research Ethics Committee of China Medical University and Hospital (CMUH109-109-REC2-031). All methods used in this study were performed in accordance with the Declaration of Helsinki. Information related to patients or caregivers was enciphered before release to protect individual privacy. Therefore, the need for informed consent from patients was waived by the research ethics committee.
Study design
HTN and T2D were diagnosed by ICD-9-CM codes or ICD-10-CM codes (Supplementary Table 1), with at least two outpatient claims within 1 year or one hospitalization. This algorithm to define HTN and T2D using ICD codes has been validated by previous studies with acceptable accuracy [12, 13]. We excluded patients diagnosed with type 1 diabetes (ICD-9-CM code 250.1x, ICD-10-CM E10); those younger than 30 years or older than 90 years; those with missing age or sex information; and those diagnosed with cognitive impairment or memory loss, dementia, Parkinson’s disease, brain tumor, or hepatic failure. We also excluded patients who were followed up for less than 180 days after the index date.
Procedures
In this retrospective cohort study, we constructed three cohorts from 2000 to 2017 to compare the risks of all-cause dementia, Alzheimer’s disease, vascular dementia, and unspecified dementia in relation to T2D and HTN (Fig. 1 and Supplementary Table 2): (a) newly diagnosed T2D patients without preceding HTN, with and without subsequent HTN (DM cohort), (b) newly diagnosed HTN patients without preceding HTN, with and without subsequent T2D (HTN cohort), and (c) patients with HTN who subsequently developed T2D, and patients with T2D who subsequently developed HTN (comorbid DM and HTN cohort). Among 170,519 newly diagnosed T2D patients, after excluding ineligible patients (excluding patients with HTN before DM diagnosis), there were 80,556 patients with subsequent HTN and 551,166 patients without subsequent HTN. We defined the date of HTN diagnosis as the index date of this T2D cohort. Among 478,784 newly diagnosed HTN patients, after excluding ineligible patients (excluding patients with T2D before HTN diagnosis), there were 89,452 HTN patients with subsequent T2D and 193,923 patients without subsequent T2D. We defined the date of T2D diagnosis as the index date of this HTN cohort. Among 630,365 patients with coexisting T2D and HTN, after excluding ineligible patients, there were 350,618 patients with previous T2D and 180,756 patients with previous HTN. We defined the date of concurrent T2D and HTN diagnosis as the index date of this comorbid cohort. In the DM cohort, the index date for the exposure group was assigned to the date on which the HTN was diagnosed. Then, we assigned the same date as the index date for those who did not develop HTN. So, the matched pair shared the same duration between the study entry and the index date. Similarly, we defined the index date for the HTN cohort. The following variables were considered as potential confounders in this study: sex, age [because we wanted to investigate the different effects of diabetes and hypertension in midlife and late-life on the development of dementia, we selected people aged 30 to 90 years, and divided them into three age groups (30–49, 50–69, and 70–90 years) to do the subgroup analysis], overweight; obesity; severe obesity; smoking status; dyslipidemia; coronary artery disease; stroke; heart failure; atrial fibrillation; peripheral arterial occlusive disease; chronic kidney disease; retinopathy; chronic obstructive pulmonary disease; liver cirrhosis; head injury; Charlson Comorbidity Index (CCI) [14] and Diabetes Complication Severity Index (DCSI) scores [15]; number and type of oral antidiabetic medications and insulin (Supplementary Table 3); number and type of antihypertensive medications (Supplementary Table 4); statin; aspirin (Supplementary Tables 3–5); T2D duration (Supplementary Table 3); and HTN duration (Supplementary Table 4).

Flowchart of the study population.
Main outcomes
Approximately 50–70% of dementia can be categorized as Alzheimer’s disease [1], which is characterized by the accumulation of amyloid-β peptides and neurofibrillary tangles made up of hyperphosphorylated tau molecules. Cognitive enhancers such as cholinesterase inhibitors only produce moderate clinical benefits [16]. Approximately 20–30% of dementia cases are of vascular dementia, which is characterized by stroke-like features. Few patients may have other types of dementia, including Pick’s disease, senile degeneration of the brain, or dementia with Lewy bodies. Therefore, we defined our main outcomes [17] as: 1) Alzheimer’s disease (specifically identified by ICD-9-CM: 331.0, ICD-10-CM: G30; or by ICD-9-CM: 290.0, 290.1, 290.2, 290.3, 290.4, 294.1, 294.2; ICD-10-CM: F03.90, F05, F02.80, and F02.81 and medications for dementia [donepezil, rivastigmine, and galantamine]); 2) Vascular dementia (identified by ICD-9-CM: 290.4, ICD-10-CM: F01.50, F01.51); 3) Other dementia (identified by ICD-9-CM: 290.0, 290.1, 290.2, 290.3, 290.4, 294.1, 294.2; ICD-10-CM: F03.90, F05, F02.80, and F02.81 and without use of cholinesterase inhibitors), Pick’s disease, senile degeneration of the brain, or dementia with Lewy bodies; 4) All-cause dementia, which encompassed outcomes of Alzheimer’s disease, vascular dementia, and unspecified dementia. The incidence rates of all-cause dementia, Alzheimer’s disease, vascular dementia, and other dementia were calculated and compared between the study and control groups.
Statistical analysis
Propensity score matching was used to decrease the imbalance between the study and control groups in each investigated cohort [18]. The propensity score for every patient was estimated using non-parsimonious multivariable logistic regression. The control groups were matched without replacement; we performed optimal matching by the method of greedy nearest neighbor matching. Approximately 30 clinically related variables were used as independent variables (Supplementary Tables 2–4) to balance those with and without incident HTN (the DM cohort), those with and without incident DM (the HTN cohort) and people starting up with coexisting DM and HTN (the comorbid DM and HTN cohort). A standardized mean difference (SMD) algorithm was used to evaluate distinction for the matching pairs under the assumption that an SMD of 0.05 or less indicated a negligible difference.
For categorical variables, the chi square test was used to test the statistical difference between the study and control groups, and for continuous variables, the Student’s t-test was used to determine the statistical difference between the two groups. To assess the incidence rates of all-cause dementia, Alzheimer’s disease, vascular dementia, and other dementia, the respective events were divided by the person years in the observation period. Crude and multivariable adjusted analyses were performed to compare the risk of outcomes between the study and control groups. The results are presented as hazard ratios (HRs) and 95% confidence intervals (CIs) for the study versus control groups. We assured no violation of the proportional-hazards assumption using the Schoenfeld residuals test. To calculate risk of respective outcomes, we censored patients on the date of death, the date of respective outcomes, or end of follow-up on December 31, 2018, whichever came first. Taking death as a competing risk, subdistribution competing risk analysis was used to assess dementia risk to prevent death from interfering with the outcomes.
We adopted the Fine and Gray’s subdistribution hazard model to assess the competing risk of death and compared the cumulative incidences of dementia over time between the study and comparison groups. Subgroup analyses of female and male, age of 30–49, 50–69, and 70–90 years were performed to clarify whether there are inconsistent results among different sex or age groups. A two-tailed p value less than 0.05 was considered to indicate statistical significance. SAS v9.4 (SAS Institute, Inc., Cary, NC, USA) was used for the analysis.
RESULTS
Study population
In the DM cohort, after propensity score matching for age, sex, obesity, smoking status, comorbidities, CCI and DCSI scores, antidiabetic medications, number of oral antidiabetic medications, statin, and diabetes duration, 32,631 pairs of matched patients were selected (Supplementary Table 3). The mean follow-up time was 6.05 years for T2D patients with subsequent HTN and 6.00 years for patients without subsequent HTN. In the HTN cohort, after propensity score matching for sex, age, obesity, smoking status, comorbidities, type and number of antihypertensive medications, statin, aspirin, and HTN duration, 112,948 pairs of matched patients were identified (Supplementary Table 4). The mean follow-up duration was 8.12 years for HTN patients with subsequent T2D and 8.07 years for patients without subsequent T2D. In the cohort of comorbid DM and HTN, after propensity score matching for sex, age, obesity, smoking status, comorbidities, DCSI scores, item and number of antidiabetic medications and antihypertensive medications, statin, and aspirin, 172,463 pairs of matched patients were selected (Supplementary Table 5). The mean follow-up duration was 8.46 years for patients with previous T2D and 8.44 years for patients with previous HTN.
Main outcomes
In the matched DM cohort, 286 (0.88%) patients with subsequent HTN and 179 (0.55%) without subsequent HTN developed all-cause dementia during the follow-up period (incidence rate of 1.46 versus 0.93 per 1000 person-years). The multivariable-adjusted HR (95% CI) for patients with subsequent HTN to patients without HTN was 1.44 (1.20–1.74; Table 1) and 1.51 (1.25–1.83; death as a competing risk analysis). In the HTN cohort, 2699 (2.39%) patients with subsequent T2D and 2350 (2.08%) without subsequent T2D developed all-cause dementia during the follow-up period (incidence rate of 3.16 versus 2.72 per 1000 person-years). The adjusted HR (95% CI) for patients with subsequent T2D to patients without T2D was 1.17 (1.11–1.24; Table 1) and 1.15 (1.08–1.21; death competing risk analysis). In the comorbid DM and HTN cohort, 3,684 (2.14%) patients with previous HTN and 3,442 (2.00%) patients with previous T2D developed all-cause dementia during the follow-up period (incidence rate of 2.58 versus 2.39 per 1000 person-years). The adjusted HR (95% CI) for patients with previous HTN to patients with previous T2D was 0.94 (0.85–1.05; Table 1).
Hazard ratios (HRs) and 95% confidence intervals (CIs) for the outcomes of dementia
T2D, type 2 diabetes; HTN, hypertension; PY, person-years; IR, incidence rate, per 1000 person-years; cHR, crude hazard ratio; aHR, adjusted hazard ratio; CI, confidence interval. *p < 0.05, ***p < 0.001. aHR†, adjusted multivariable analysis of variables in Supplementary Tables 3–5, such as sex, age, obesity, smoking status, comorbidities, CCI, DCSI scores, medications, number of oral antidiabetic drugs, hypertension, and diabetes duration. aHR‡, taking death as a competing risk for sub-distribution competing risk analysis of outcomes.
The adjusted HR (95% CI) for vascular dementia in T2D patients with HTN versus those without HTN was 2.20 (1.63–2.98) and 2.30 (1.71–3.13; death competing risk analysis), in HTN patients with T2D versus those without T2D was 1.27 (1.19–1.37) and 1.25 (1.62–1.34; death competing risk analysis). The adjusted HR (95% CI) for other dementia in HTN patients with T2D vs. those without T2D was 1.33 (1.05–1.69) and 1.31 (1.03–1.66; death competing risk analysis). While the adjusted HRs (95% CI) for Alzheimer’s disease had no significant difference among the three cohorts (Table 1).
Figure 2 depicted that patients with T2D and subsequent HTN had significantly higher cumulative incidences of all-cause dementia (Fig. 2A; Log-rank test, p < 0.001) and vascular dementia (Fig. 2B; p < 0.001) compared with those without subsequent HTN. Figure 3 described that patients with HTN and subsequent T2D had significantly higher cumulative incidences of all-cause dementia (Fig. 3A; p < 0.001), vascular dementia (Fig. 3B; p < 0.001), and other dementia (Fig. 3C; p = 0.022) compared with those without subsequent T2D.
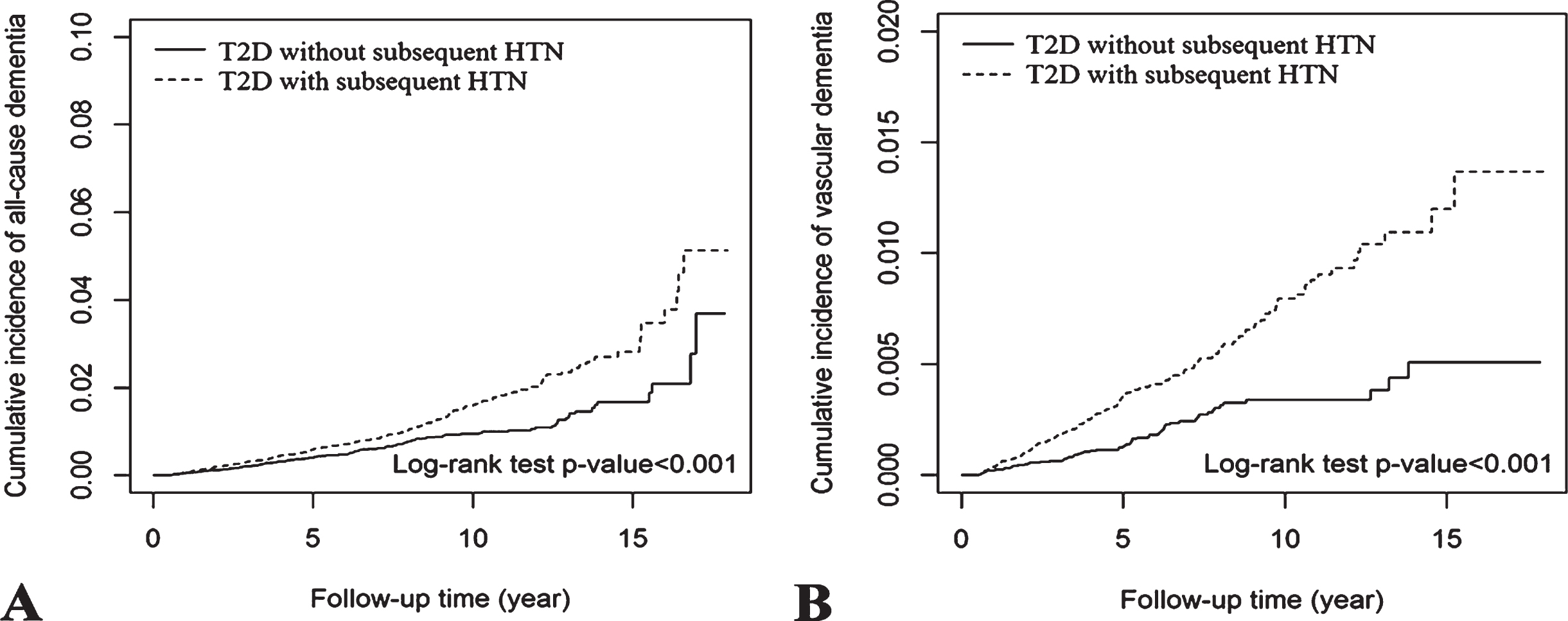
The cumulative incidence of all-cause dementia (A), and vascular dementia (B) over time between T2D with and without subsequent HTN.
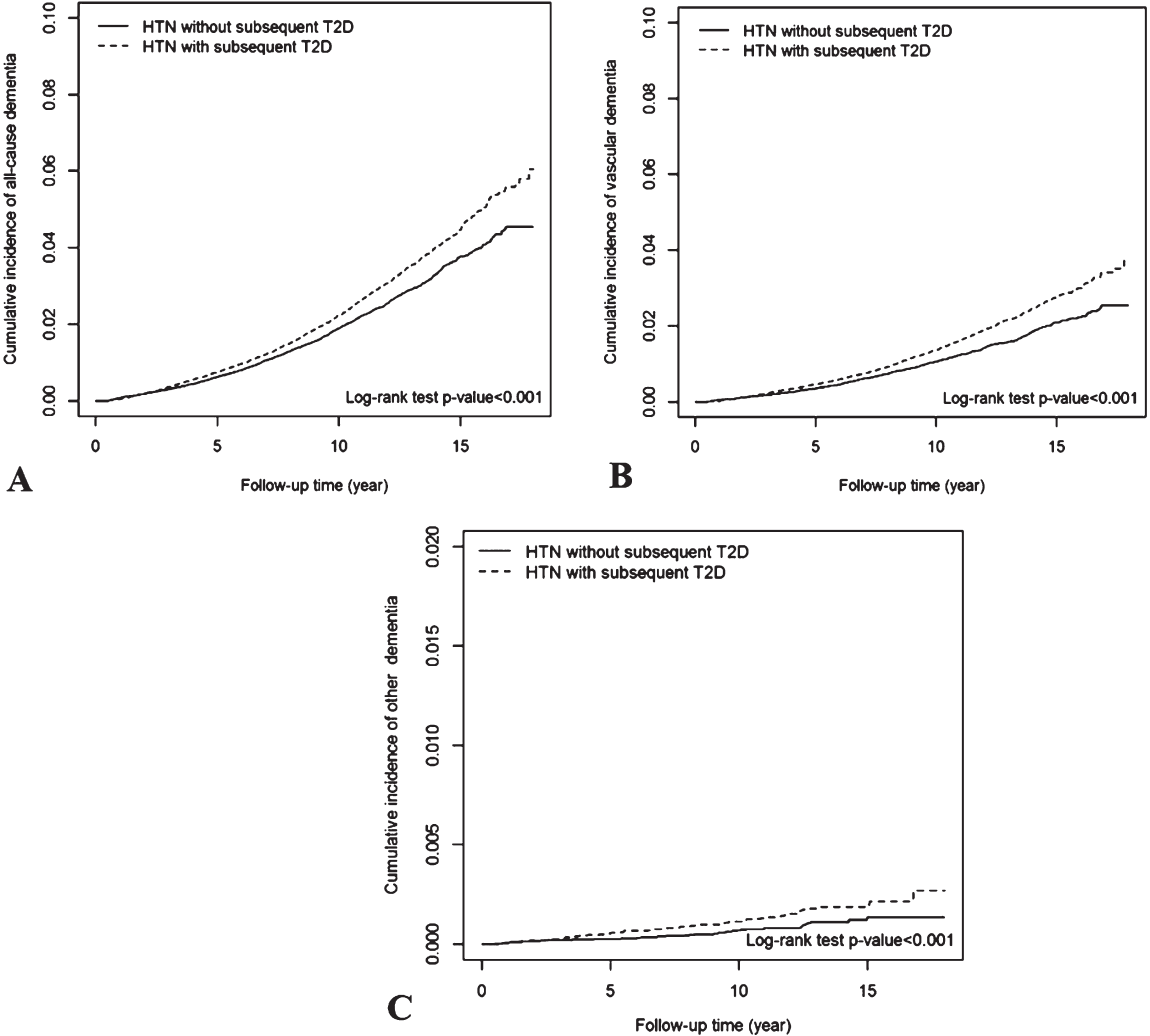
The cumulative incidence of all-cause dementia (A), vascular dementia (B), and other dementia (C) over time between HTN with and without subsequent T2D.
Subgroup analysis
The subgroup analysis disclosed that both male and female patients with T2D and subsequent HTN were associated with significantly higher risks of all-cause dementia and vascular dementia compared with those without HTN (Table 2); the male and female patients with HTN and subsequent T2D were associated with significantly higher risks of all-cause dementia and vascular dementia, and the male patients with HTN and subsequent T2D were associated with significantly higher risk of other dementia compared with those without T2D (Table 2).
Subgroup analysis of sex and age for the risks of dementia
T2D, type 2 diabetes; HTN, hypertension; PY, person-years; IR, incidence rate, per 1000 person-years; cHR, crude hazard ratio; aHR, adjusted hazard ratio; CI, confidence interval. *p < 0.05, **p < 0.01, ***p < 0.001. aHR†, adjusted multivariable analysis of variables in Supplementary Table 3–5, such as sex, age, obesity, smoking status, comorbidities, CCI, DCSI scores, medications, number of oral antidiabetic drugs, hypertension, and diabetes duration.
The subgroups of age 50–69, and 70–90 years in patients with T2D and subsequent HTN were associated with significantly higher risks of all-cause dementia and vascular dementia compared with those without HTN (Table 2); and the subgroups of age 50–69, and 70–90 years in patients with HTN and subsequent T2D were associated with significantly higher risks of all-cause dementia and vascular dementia compared with those without T2D (Table 2).
DISCUSSION
Our study demonstrated that patients with T2D and subsequent HTN have higher risks of all-cause dementia and vascular dementia than those without subsequent HTN, patients with HTN and subsequent T2D have higher risks of all-cause dementia, vascular dementia, and other dementia than those without subsequent T2D. The results suggest that patients with T2D or HTN should take utmost care to avoid developing HTN or T2D, to reduce their future risk of dementia.
Long-term exposure to pulsatile blood pressure and flow in HTN patients will cause atherosclerosis of large blood vessels and arteriosclerosis of small vessels, which can lead to cerebrovascular insufficiency, micro-infarcts, white matter lesions, and stroke with ensuing vascular dementia [2, 20]. HTN with chronic inflammation and excessive oxidative stress may reduce cerebral blood flow and disrupt the blood-brain barrier, which could decrease amyloid-β clearance and lead to Alzheimer’s disease [19]. Observational studies have consistently reported that midlife HTN may lead to dementia [20, 21], and that HTN has a higher impact on vascular dementia and with moderate influence on Alzheimer’s disease [22]. Recent meta-analyses of randomized control trials have shown that intensive blood pressure lowering can reduce the risks of cognitive decline and dementia [9, 10]. Our study disclosed that patients with T2D and subsequent HTN were associated with a higher risk of all-cause dementia and vascular dementia. Adding HTN to patients with T2D may increase their risk of dementia, and this increased risk existed in both sexes and in midlife and elderly patients.
Advanced glycation end-products and oxidative stress in patients with diabetes may lead to macrovascular and microvascular complications, stroke, and vascular dementia [1, 6]. The toxic effect of hyperglycemia with excessive oxidative stress and microvascular pathology is referred to as glucose-mediated “accelerated brain aging” [23]. Glucose-mediated toxicity may also interfere with the metabolism of amyloid-β and tau in the brain, increasing the risk of Alzheimer’s disease [1, 24]. Insulin resistance may lower regional cerebral glucose metabolism [1]. Severe hypoglycemia can also cause neuronal loss through neuroglycopenia [25].
Systemic reviews of observational studies have shown that patients with T2D have approximately 50–60% increased risk of incident dementia compared with those without T2D [6, 26]. Patients with higher glucose levels [5] or longer duration of diabetes also have a higher risk of dementia [25]. A recent study of patients with type 1 diabetes, who were followed up for 32 years, demonstrated that exposure to higher HbA1c levels, more episodes of severe hypoglycemia, and higher blood pressure are associated with a greater decline in psychomotor and mental function [27]. Our study shown that patients with HTN and subsequent T2D were associated with a higher risk of all-cause dementia, vascular dementia, and other dementia. The risk of death for these patients is very high, but we get the same results as we use death as a competing risk to analyze. Our results suggest that combined with the pathological changes caused by diabetes, HTN facilitates glucose-mediated “accelerated brain aging” [23], which is likely to lead to dementia, especially vascular dementia. Our results are similar to those of a long-term follow-up study of patients with type 1 diabetes [21]. Most youths with type 1 diabetes do not have baseline HTN, and it is not until microvascular complications develop that HTN will gradually occur [27]. This 32-year follow-up study found that in patients with type 1 diabetes, higher systolic blood pressure is associated with a higher risk of cognitive impairment. These results suggest that patients with diabetes should be strictly advocated a low-salt and low-fat diet, abstinence from smoking or alcohol drinking, and more physical activity to decrease the risk of HTN, thereby reducing the future risk of dementia [7].
This study compared the dementia risk between comorbid patients with T2D and HTN history and found no significant difference between the effect of these two previous comorbidities. It may be because the impact of T2D and HTN history in the two groups was similar, and their durations may be not long enough to cause a significant difference in dementia risk. Among our patients with HTN or T2D, the subsequent development of T2D or HTN did not have a higher risk of Alzheimer’s disease dementia. The reasons for this are not clear. It is possible that this additional disease is not strong or long enough to increase the risk of Alzheimer’s disease dementia. Potentially, a longer period of observation may lead to different results.
There are some limitations in this study. First, some misclassification using the ICD codes to identify patients with dementia is possible. Our NHI Administration regularly monitors diagnostic codes and the medical management of clinical units to ensure the diagnostic accuracy and adequate disposal of the NHI system. We added the criterion of use of cholinesterase inhibitors, which under the NHI regulation, has to be pre-censored before prescription, to define Alzheimer’s disease to decrease the possibility of misclassification. However, milder cases of dementia or cognitive impairment may not be identified by this method. Second, the 17-year (2000–2017) panel of claims data used in this study may not be sufficient to compare the risk of dementia between the study and control patients. Third, the administrative database lacks information on family history, alcohol drinking, and physical activity. We tried to include as many critical variables as possible, such as age, sex, obesity, smoking status, comorbidity, diabetes complication scores, and medications, and performed propensity score matching to decrease the imbalance between the study and control groups. Fourth, this dataset also lacks information on blood pressure, glucose, hemoglobin A1C, renal function, mental tests, and CT or MRI scans of the brain to diagnose and discriminate the severity of HTN, T2D, and dementia. We tried to match the numbers of antihypertensive drugs and antidiabetic drugs, as well as the scores of CCI and DCSI, to balance the severity and management of HTN and DM. However, the unmeasured and unknown confounding factors could have influenced our results. Fifth, the people in this nationwide population-based study were mainly Taiwanese; therefore, the results may not be generalizable to other ethnicities. Finally, this study is a retrospective cohort study with some inevitable bias, and more prospective studies are needed to verify our results.
In conclusion, this study demonstrated that T2D patients with subsequent HTN, and HTN patients with subsequent T2D were associated with higher risks of all-cause dementia and vascular dementia. We shall design further experiments to investigate how hypertension affects patients with T2D and how T2D causes dementia in patients with HTN, to observe whether hypertension and diabetes have different impacts on various subtypes of dementia. The caregivers need to put much effort to attenuate the development of T2D or HTN in patients with HTN or T2D to reduce their future risk of dementia.
Footnotes
ACKNOWLEDGMENTS
We are grateful to the Health Data Science Center, China Medical University Hospital, for providing administrative, technical, and funding support. This study is supported in part by the Taiwan Ministry of Health and Welfare Clinical Trial Center (MOHW109-TDU-B-212-114004), MOST Clinical Trial Consortium for Stroke (MOST 109-2321-B-039-002), China Medical University Hospital (DMR-110-222), Tseng-Lien Lin Foundation, Taichung, Taiwan; and Taipei Veterans General Hospital (V105C-204, V110C-175, V109C-189, V108C-172, VN107-07), Taiwan. These funding agencies had no role in the study design, data collection and analysis, decision to publish, or manuscript preparation. No organization provided funds to assist with the preparation of this paper, and data analysis was not performed by employees of funders or any author who received funding. The funders did not offer writing support. The corresponding authors had complete access to all data in the study and the final responsibility of the decision to publish.