
Abstract
Background
Donanemab, a monoclonal antibody targeting amyloid-β (Aβ) plaques, has shown the ability to reduce cerebral amyloid burden in early Alzheimer's disease (AD). However, uncertainties remain regarding its clinical relevance, particularly in relation to tau pathology, APOE ε4 genotype, and methodological limitations in existing trials.
Objective
To conduct a systematic review and exploratory meta-analysis to evaluate the efficacy, safety, and tolerability of donanemab in patients with mild to moderate AD.
Methods
We conducted a systematic review and exploratory meta-analysis following PRISMA guidelines. Randomized controlled trials comparing donanemab to placebo in individuals aged ≥65 years with biomarker-confirmed mild to moderate AD were included. Outcomes included cognitive measures (ADAS-Cog13, MMSE, CDR-SB, iADRS, ADCS-iADL) and adverse events (ARIA-E, ARIA-H, infusion reactions, discontinuations). Random-effects models were used to estimate pooled mean difference (MD) or risk ratio (RR) with 95% confidence intervals. Subgroup analyses were performed by baseline tau burden and APOE ε4 genotype.
Results
Three trials (n = 2054) were included. Donanemab modestly reduced cognitive decline compared to placebo: ADAS-Cog13 (MD, −1.86), CDR-SB (MD, −0.36), MMSE (MD, 0.64), and iADRS (MD, 3.19), with similar effects across tau subgroups. The risk of ARIA-E was markedly increased (RR, 12.39), especially among APOE ε4 homozygotes. Infusion reactions (RR, 11.90) and discontinuations (RR, 3.22) were also more frequent.
Conclusions
Donanemab demonstrated modest cognitive benefits, the clinical significance of which remains uncertain. Independent, longer-term trials with rigorous methodology and active comparators are warranted to more clearly define its therapeutic value in the treatment of AD.
Keywords
Introduction
Alzheimer's disease (AD) is the leading cause of dementia worldwide, affecting more than 50 million individuals, with projections indicating a twofold increase every two decades.1–3 Cognitive decline is the central clinical feature of AD, progressing gradually and impairing memory, executive function, and independence in activities of daily living.4,5 Despite advances in research, currently available pharmacological therapies have a limited impact on disease progression.6,7
In recent years, disease-modifying strategies targeting beta-amyloid deposition have gained prominence. 8 Donanemab is a monoclonal antibody directed against N-terminal pyroglutamate-modified amyloid-β (Aβ) plaques, developed to facilitate amyloid clearance in the early stages of AD.9–13 Preliminary randomized clinical trials (RCTs) have demonstrated cognitive stabilization in selected subgroups, particularly in individuals with high amyloid burden and low tau pathology.9,10,13 However, its safety profile remains a clinical concern, especially regarding the risk of amyloid-related imaging abnormalities (ARIA) and infusion-related reactions.14–16
Among the known genetic risk factors for AD, the apolipoprotein E (APOE) ε4 allele stands out as the strongest predictor of late-onset AD. 17 Individuals carrying one (heterozygotes) or two (homozygotes) copies of the ε4 allele have an increased risk of developing AD and tend to exhibit earlier disease onset and greater amyloid deposition.4,18
Recent evidence suggests that APOE ε4 status may also modulate both the efficacy and safety profile of anti-amyloid therapies.17,19 Donanemab, in particular, may exhibit variable outcomes depending on the APOE genotype. 20 Homozygous carriers of the ε4 allele are more susceptible to ARIA, especially vasogenic edema and microhemorrhages, which may limit treatment tolerability and require close monitoring.13,20,21 Additionally, some studies suggest that the clinical response to donanemab may differ across APOE genotypes, though further investigation is needed to establish genotype-specific efficacy. 22
Emerging data from a network meta-analysis compared Terao and Kodama 23 donanemab with lecanemab, aducanumab, and lithium in patients with mild cognitive impairment or Alzheimer's disease, assessing cognitive efficacy, tolerability, and acceptability in 6547 participants across eight RCTs. 23 The results showed that all active agents outperformed placebo on the Alzheimer's Disease Assessment Scale–Cognitive Subscale (ADAS-Cog), while both donanemab and lecanemab also showed superiority over placebo on the Clinical Dementia Rating–Sum of Boxes (CDR-SB).24,25 However, donanemab, along with the other anti-amyloid monoclonal antibodies, was associated with lower tolerability and acceptability compared to placebo.16,26
Although individual trials and indirect comparisons suggest a potential therapeutic role for donanemab, important uncertainties remain regarding the clinical relevance of its effects, particularly in relation to tau pathology and the APOE ε4 genotype. Moreover, discrepancies in methodological rigor and the generalizability of findings across studies justify an independent synthesis of the available evidence.14,27 Therefore, we conducted a systematic review and exploratory meta-analysis of the available evidence to estimate the efficacy and tolerability of donanemab for the treatment of cognitive impairment in patients with AD.
Methods
This systematic review and meta-analysis was conducted based on the Cochrane Handbook and the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) statement.28,29 The protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO) registration number: CRD 420251023460.
Eligibility criteria
This meta-analysis included RCTs that compared donanemab with placebo in elderly individuals (≥65 years) with a clinical diagnosis of AD in mild to moderate stages.16,30 Eligible studies were required to report at least one predefined outcome of interest related to efficacy or safety/tolerability. Efficacy outcomes included changes in cognitive performance measured by validated scales, such as the ADAS-Cog13, Mini-Mental State Examination (MMSE), CDR-SB and Alzheimer's Disease Cooperative Study–Instrumental Activities of Daily Living (ADCS-iADL).24,25,31 Safety and tolerability outcomes included treatment-emergent adverse events (TEAEs), discontinuation due to adverse events, amyloid-related imaging abnormalities (ARIA-E and ARIA-H), infusion-related reactions, amyloid-negative population. 15 We excluded case reports, reviews, editorials, letters to the editor, conference abstracts, and studies that did not include a placebo control group or failed to report outcome-specific data relevant to efficacy or tolerability. Non-English language publications were also excluded.
Search strategy, study selection, and quality assessment
A comprehensive literature search was conducted across four electronic databases: PubMed, Embase, Cochrane Central Register of Controlled Trials (CENTRAL), and SCOPUS from inception to March 2025, using the following search strategy: (“donanemab”) AND (“Alzheimer's disease” OR “mild cognitive impairment”) AND (“cognition” OR “ADAS-Cog” OR “MMSE” OR “CDR-SB”). A Cochrane Highly Sensitive Search Strategy was applied in the MEDLINE, Embase and SCOPUS databases to ensure the search was restricted to RCTs. 29 The entire search string is available in the Supplemental Material. Additionally, the reference lists of the included studies were manually screened for additional relevant studies. All retrieved citations were imported into the Rayyan® platform for systematic screening. 32
The risk of bias for RCTs was assessed using Version 2 of the Cochrane risk-of-bias tool (RoB 2). 33 Two authors independently assessed the studies for data extraction and quality assessment (AMPS & ESF), and any conflict was resolved by a third author (MBSM).
Data extraction
The following data were extracted from each included study: first author, year of publication, study location, study design, sample size, mean age of participants, diagnostic criteria for AD, and baseline cognitive status. Detailed information regarding the intervention (donanemab: dosage, administration route, treatment duration), comparator (placebo), and follow-up period was collected. Primary outcomes included measures of cognitive efficacy (changes in ADAS-Cog13, MMSE, CDR-SB) and safety/tolerability outcomes, such as TEAEs, discontinuation rates due to TEAEs, ARIA-E/H, infusion-related reactions.
Outcomes, definitions, and subgroup analyses
The outcomes analyzed in this review encompassed both efficacy and safety/tolerability domains. Efficacy endpoints included changes in cognitive performance and functional capacity, evaluated through the 13-item version; ADAS-Cog13 34 which quantifies cognitive decline in AD; the MMSE, a widely adopted tool for assessing global cognitive function 35 ; the CDR-SB, which integrates cognitive and functional metrics 36 ; the Integrated iADRS, a composite index of cognitive-functional status 37 ; and the ADCS-iADL 38 ; which captures patient capacity in performing routine instrumental tasks.
Safety and tolerability outcomes included the incidence of TEAEs, defined as any undesirable clinical event occurring after the administration of donanemab or placebo, regardless of causality. These outcomes also included adverse events and safety events (deaths, treatment discontinuations and infusion reactions); discontinuations attributed to TEAEs; and ARIA, encompassing both vasogenic edema (ARIA-E) and hemorrhagic manifestations such as microhemorrhages and superficial siderosis (ARIA-H), as detected by magnetic resonance imaging and defined according to radiological criteria. 39 All outcomes were evaluated at the 76-week follow-up. Predefined subgroup analyses were conducted to explore potential effect modifiers.
For efficacy endpoints including: ADAS-Cog13, MMSE, CDR-SB, iADRS, and ADCS-iADL stratification was based on baseline tau burden, categorized as low/medium tau versus combined tau groups. For safety outcomes related to ARIA events, subgroup analyses were performed according to APOE ε4 genotype, including homozygous carriers, heterozygous carriers, and noncarriers.
Statistical analysis
The present systematic review and meta-analysis adhered to the updated PRISMA guidelines. 29 We calculated pooled effect sizes using mean difference (MD) for continuous outcomes, and risk ratio (RR) with 95% confidence intervals (CI) for dichotomous outcomes. 29 All analyses were performed under a random-effects model, accounting for expected clinical and methodological heterogeneity across studies. A p-value < 0.05 was considered statistically significant. Heterogeneity was assessed using the Cochran Q test and quantified with the I² statistic, interpreted as follows: < 40% (low), 40–60% (moderate), and >60% (substantial heterogeneity). 29 All statistical analyses were conducted using R software version 4.4.2 (R Foundation for Statistical Computing, Vienna, Austria) with the meta packages. 40 The DerSimonian and Laird method was employed for estimating between-study variance (τ²) under the inverse variance framework. 41
Results
Study selection
A total of 380 records were identified through database searches from PubMed (31), Scopus (229), Embase (75), and Cochrane Library (45). After removing 197 duplicates, 183 records were screened by title and abstract, resulting in the exclusion of 177 studies. The remaining 6 full-text articles were assessed for eligibility, of which 3 were excluded for being conference abstracts. Ultimately, 39,10,13 studies met the inclusion criteria and were included in the final analysis.28,42 This search process is illustrated in Figure 1.

PRISMA flow diagram.
Baseline characteristics
The three randomized, multicenter, placebo-controlled trials included in this meta-analysis, conducted between 2015 and 2020 across sites in North America, Europe, Asia, and Australia enrolled a total of 2054 participants, with 1037 (50.5%) allocated to donanemab and 1017 (49.5%) to placebo. Mean age ranged from 66.8 to 78.3 years in the donanemab arms and from 73.0 to 75.4 years in the placebo arms. The proportion of male participants ranged from 42% to 60% across study groups. Baseline MMSE scores ranged from 18.86 (SD 2.41) to 23.6 (SD 3.1) in the donanemab groups, and from 21.67 (SD 4.81) to 23.7 (SD 2.9) in the placebo groups, consistent with mild to moderate cognitive impairment at study entry. All trials required biomarker confirmed AD, with mandatory amyloid PET positivity and, when applicable, tau PET stratification. The prevalence of APOE ε4 carriers in the donanemab groups ranged from 66.7% to 100%. Discontinuation rates were high, reaching up to 37.4% in the donanemab group, primarily due to adverse events, consent withdrawal, or protocol violations. Concomitant use of acetylcholinesterase inhibitors or memantine was permitted and reported in approximately 60% of participants. Strict eligibility criteria, substantial screening failure rates, and high discontinuation frequencies, particularly in the donanemab arm were observed. Baseline characteristics of the included studies and participants are presented in Table 1.
Baseline characteristics of included studies.
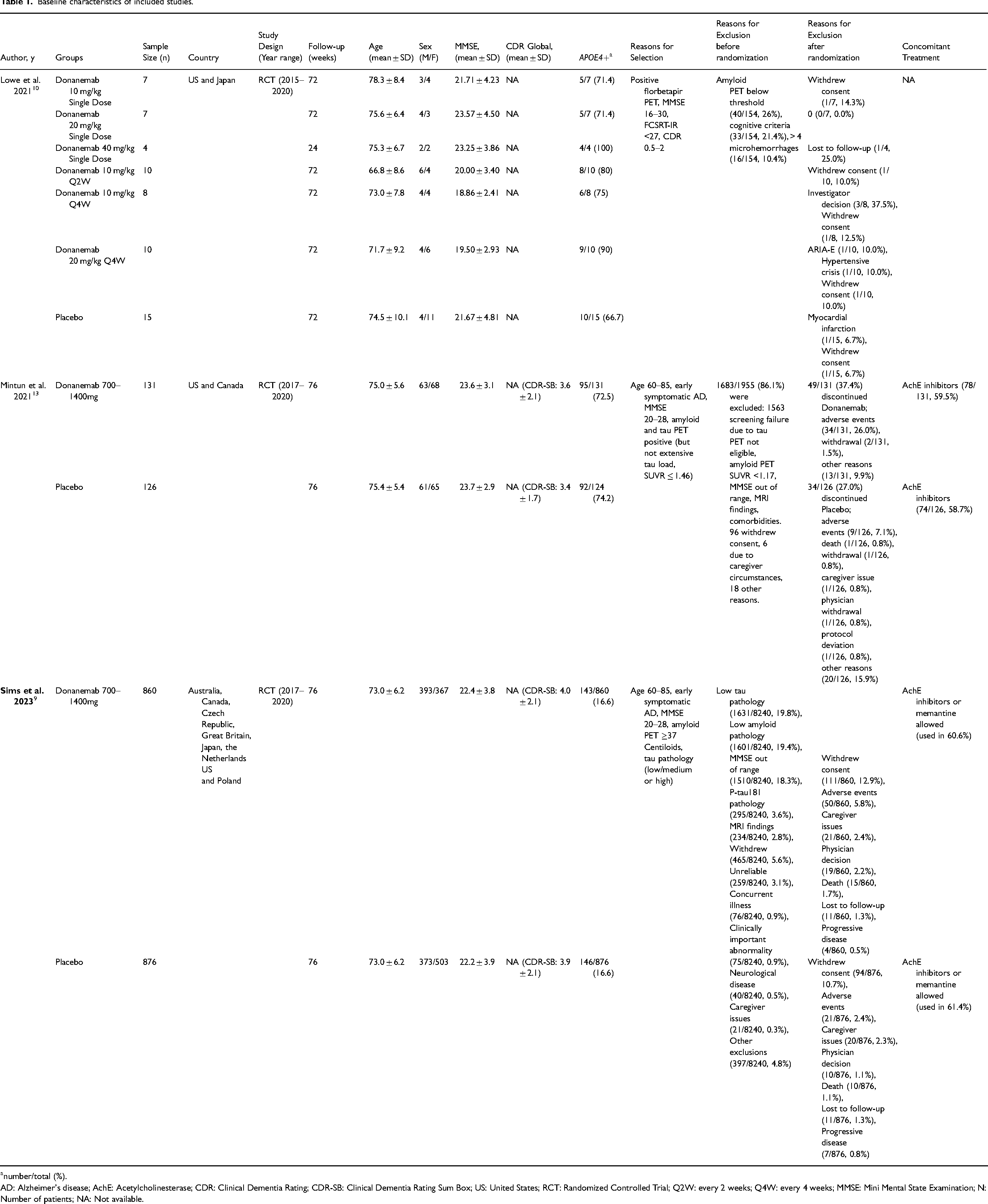
number/total (%).
AD: Alzheimer's disease; AchE: Acetylcholinesterase; CDR: Clinical Dementia Rating; CDR-SB: Clinical Dementia Rating Sum Box; US: United States; RCT: Randomized Controlled Trial; Q2W: every 2 weeks; Q4W: every 4 weeks; MMSE: Mini Mental State Examination; N: Number of patients; NA: Not available.
Pooled analysis of included studies
Cognitive and functional outcomes
ADAS-Cog13 by tau subgroup
At 76 weeks, donanemab was associated with reduced cognitive decline on the ADAS-Cog13 scale compared to placebo (MD, −1.86; 95% CI, −1.99 to −1.72; I² = 0%; Figure 2). Stratification by baseline tau pathology revealed comparable treatment effects in participants with combined tau (MD, −1.86; 95% CI, −2.05 to −1.67) and those with low/medium tau burden (MD, −1.85; 95% CI, −2.04 to −1.66), with no indication of subgroup interaction (p = 0.96).

Forest plot of ADAS-Cog13 change at 76 weeks comparing donanemab and placebo, stratified by baseline tau burden (low/medium versus combined).
ADCS-iADL
Donanemab led to a modest but statistically significant preservation of instrumental activities of daily living at 76 weeks relative to placebo (MD, 6.82; 95% CI, 0.16 to 13.48; p = 0.04; I² = 99%; Figure 3). Despite substantial heterogeneity across studies, stratified analyses showed similar effect estimates for both low/medium tau (MD, 8.07; 95% CI, −5.39 to 21.52) and combined tau groups (MD, 5.59; 95% CI, −3.02 to 14.19), without evidence of differential treatment response (p = 0.76).

Forest plot of change in ADCS-iADL scores at 76 weeks comparing donanemab and placebo, stratified by tau pathology.
CDR-SB
Global cognitive-functional decline was attenuated in the donanemab group compared with placebo at 76 weeks (MD, −0.36; 95% CI, −0.40 to −0.33; p < 0.001; I² = 0%; Figure 4). This benefit was consistent across both trials and tau subgroups. Participants with low/medium tau burden exhibited a pooled effect of −0.36 (95% CI, −0.41 to −0.31), closely mirroring the estimate in the combined tau group (MD, −0.37; 95% CI, −0.46 to −0.28). There was no evidence of effect modification by tau burden (p = 0.87).

Forest plot of CDR-SB change from baseline to 76 weeks comparing donanemab and placebo across tau subgroups.
iADR
At week 76, donanemab was associated with a significantly reduced rate of decline on the iADRS compared to placebo (MD, 3.19; 95% CI, 2.96 to 3.42; P < 0.001; I² = 0%; Figure 5). Treatment effects were consistent across tau strata, with similar estimates observed in the combined tau group (MD, 3.20; 95% CI, 2.87 to 3.52) and low/medium tau group (MD, 3.19; 95% CI, 2.86 to 3.51). Subgroup interaction was not detected (p = 0.96).

Forest plot of iADRS scores at 76 weeks comparing donanemab and placebo, stratified by tau status (low/medium versus combined).
MMSE
At 76 weeks, donanemab was associated with a smaller decline in global cognitive function compared to placebo, with a MD of 0.64 points on the MMSE score (95% CI, 0.56–0.71; p < 0.001; I² = 0%; Figure 6). The absence of heterogeneity across studies reinforces the consistency of this observed effect. In stratified analyses by baseline tau burden, results remained stable. Among participants with combined tau, the MD was 0.64 (95% CI, 0.53–0.75), while in the low/medium tau subgroup, the effect estimate was similar (MD, 0.63; 95% CI, 0.52–0.74). No evidence of subgroup interaction was detected (p = 0.92), indicating that the cognitive efficacy of donanemab on MMSE performance is independent of baseline tau pathology.
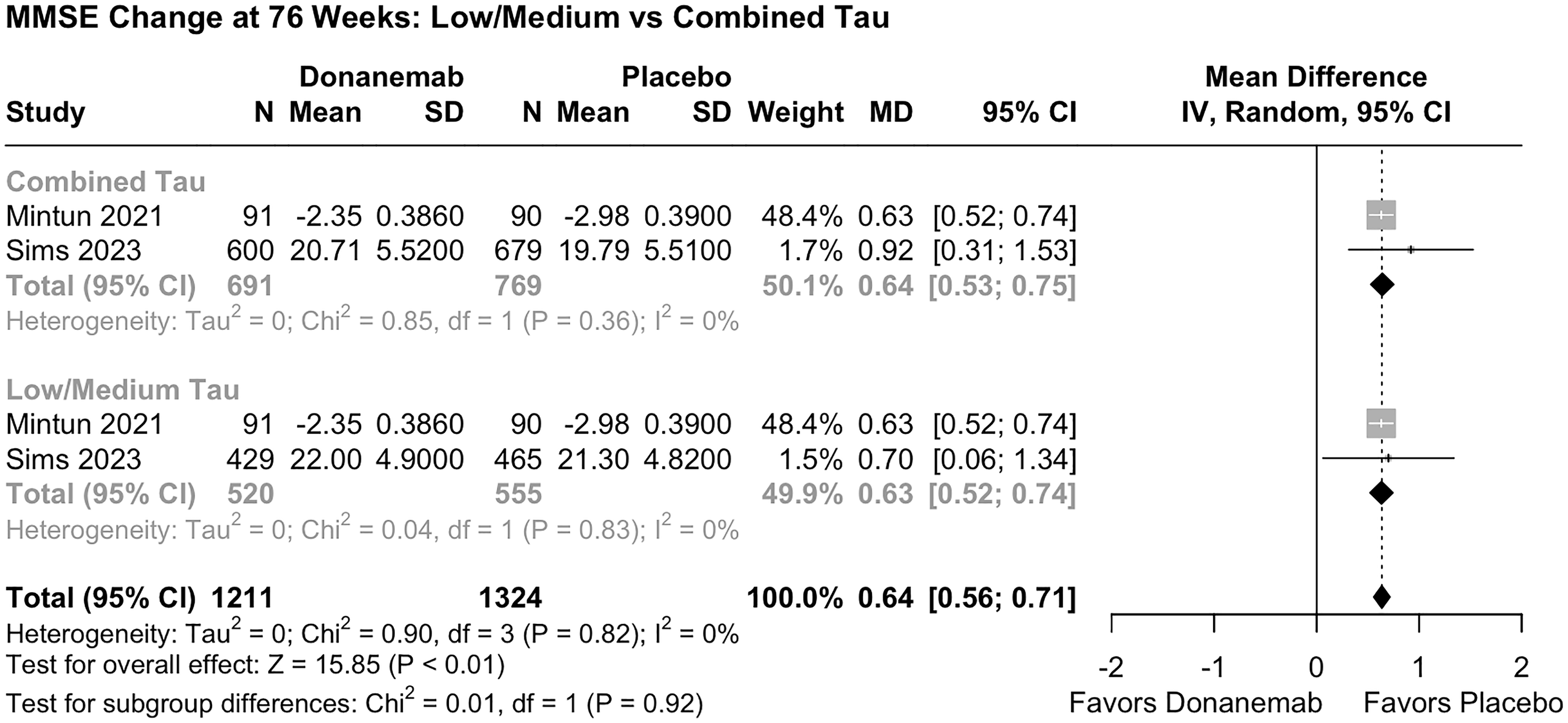
Forest plot of MMSE score change at 76 weeks comparing donanemab and placebo, stratified by tau pathology.
Amyloid-related imaging abnormalities
ARIA-E by APOE status
Donanemab was associated with an increased risk of ARIA-E events across all APOE subgroups (Figure 7). Relative risks were elevated among heterozygous ε4 carriers (RR, 12.80; 95% CI, 6.68 to 24.54), homozygous ε4 carriers (RR, 11.92; 95% CI, 5.32 to 26.71), and noncarriers (RR, 16.49; 95% CI, 4.65 to 58.48). The overall pooled estimate indicated a 12.39-fold increased risk of ARIA-E with donanemab (95% CI, 8.92 to 17.21; I² = 0%), with no significant subgroup interaction by genotype (p = 0.96). In individuals with confirmed APOE ε4 positivity, the risk of ARIA-E was increased 9.81-fold (95% CI 5.04–19·08; I² = 0%), with no heterogeneity across studies (p = 0.81), supporting the consistency of the effect in this genetic subgroup (Supplemental Figure 2). In the total population, the pooled RR for ARIA-E favored placebo (RR, 12.87; 95% CI, 8.09–20.49; I² = 0%) (Supplemental Figure 2). The consistency across studies supports the robust association between donanemab and vasogenic edema events. The absolute incidence of ARIA-E also varied by genotype (Supplemental Figure 1), reaching 41.08 (95% CI, 33.89 to 48.67) in homozygous carriers, 25.33 (95% CI, 18.77 to 33.25) in heterozygotes, and 15.23 (95% CI, 11.53 to 19.85) in noncarriers. Subgroup interaction was significant (p < 0.001), indicating differential risk by APOE genotype.
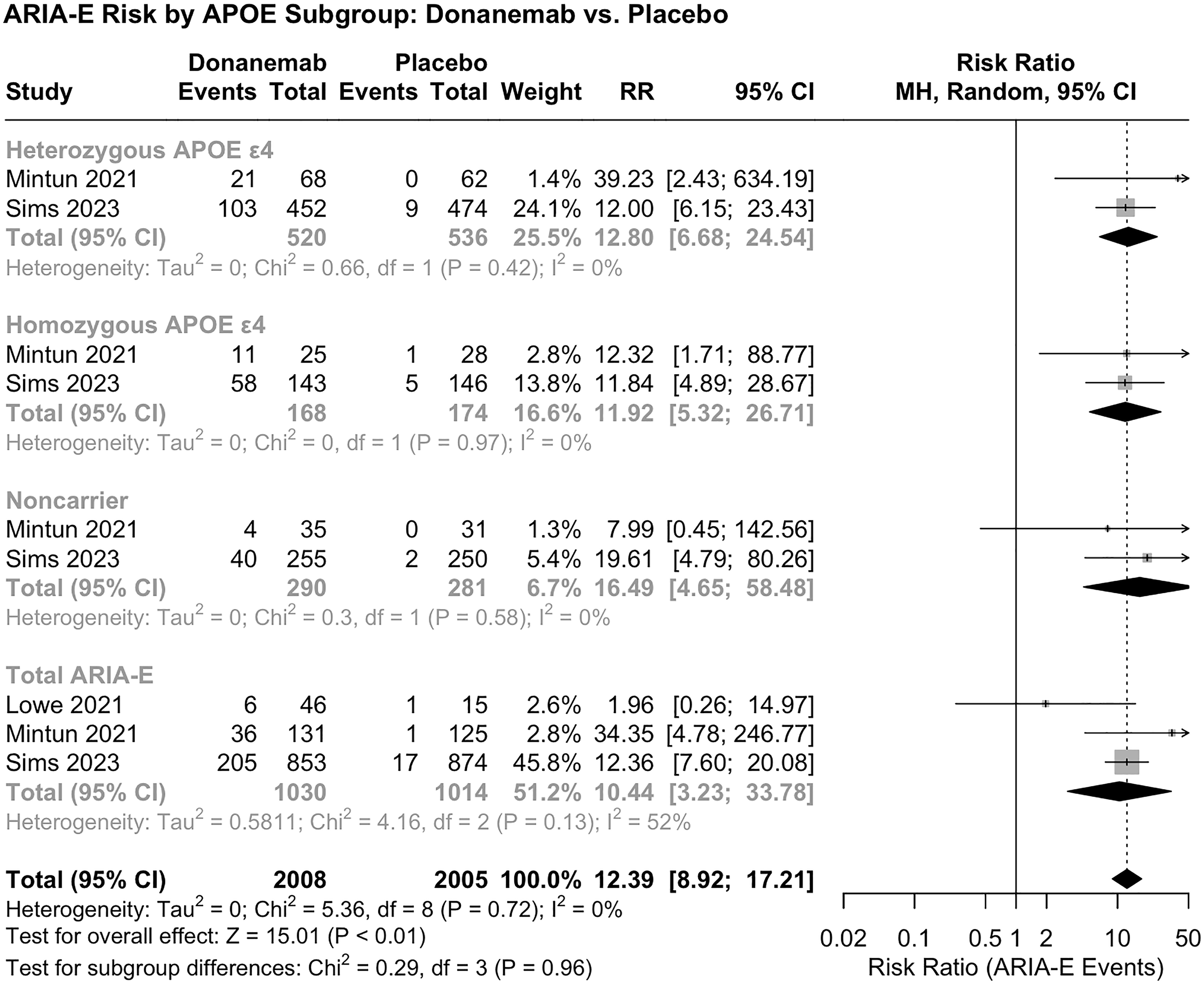
Forest plot of ARIA-E risk associated with donanemab, stratified by APOE ε4 genotype (noncarrier, heterozygous, homozygous).
The pooled safety analysis revealed a consistently elevated risk of ARIA stratified by APOE Genotype and Amyloid-PET among participants treated with donanemab when compared to placebo (RR, 6.06; 95% CI, 2.83–13.00; I² = 96%) (Supplemental Figure 2). Subgroup-specific patterns further clarified the stratified risk profiles.
ARIA-H events
Donanemab was also associated with an elevated risk of ARIA-H (RR, 3.32; 95% CI, 2.35 to 4.69; I² = 66%; Figure 8). The increased incidence was primarily driven by microhemorrhages (RR, 2.60; 95% CI, 1.46 to 4.65) and superficial siderosis (RR, 5.47; 95% CI, 3.72 to 8.05). Large intracerebral hemorrhages (ICH > 1 cm) were infrequent and not significantly different between groups. In a complementary analysis encompassing ARIA-H subtypes, the pooled effect confirmed the increased incidence of these events with donanemab (RR, 2.91; 95% CI, 2.06–4.11; I² = 0%), with low statistical heterogeneity (p = 0.42) (Supplemental Figure 2).

Forest plot of ARIA-H risk (including microhemorrhage, siderosis, and ICH > 1 cm) associated with donanemab versus placebo.
Adverse events and safety
There was no significant difference in deaths during follow-up between treatment groups (RR, 0.78; 95% CI, 0.18 to 3.34; I² = 40%; Figure 9). However, discontinuations due to TEAEs occurred more frequently in the donanemab group (RR, 3.22; 95% CI, 2.36 to 4.41; I² = 0%; Figure 8). Infusion reactions were substantially more common with donanemab (RR, 11.90; 95% CI, 2.97 to 47.69; I² = 35%; Figure 8). The overall adverse event risk favored placebo (RR, 2.83; 95% CI, 1.18 to 6.81; p = 0.02; I² = 68%), with moderate between-subgroup heterogeneity (p = 0.03).

Forest plots of safety outcomes: deaths during follow-up, discontinuations due to treatment-emergent adverse events (TEAEs), and infusion-related reactions.
Amyloid-negative population
In participants with negative amyloid PET imaging, the estimated risk associated with donanemab was highly uncertain (RR 7.42; 95% CI 0·42–130·35; I² = 86%) (Supplemental Figure 2).
Sensitivity analysis
To assess the robustness of findings related to ARIA events and amyloid-PET–defined subgroups, leave-one-out sensitivity analyses were conducted. For amyloid-negative conversion (Supplemental Figure 3), omission of the Sims et al. 9 study resulted in the highest risk estimate (RR, 30.91; 95% CI, 2.02–474.25), whereas excluding Mintun et al. 13 yielded the lowest estimate (RR, 1.67; 95% CI, 0.27–10.40). Heterogeneity ranged from 49% to 92%, indicating that results were sensitive to the inclusion of individual studies and that interstudy variability significantly influenced the pooled effect. For the proportion of ARIA-E events (Supplemental Figure 4), omitting Lowe et al. 10 produced a stable estimate (0.25; 95% CI, 0.22–0.27) with no observed heterogeneity (I² = 0%). However, exclusion of Mintun et al. 13 or Sims et al. 9 increased heterogeneity to 64% and 73%, respectively, with only minor changes in effect size.
Quality assessment
The risk of bias assessment is summarized in Figure 10 and detailed in Supplemental Table 1. Two trials Mintun et al. 13 and Sims et al. 9 were classified as having a high overall risk of bias. Both studies raised concerns in Domain 2 (deviations from intended interventions) and Domain 4 (missing outcome data). Mintun et al. 13 also showed potential bias in Domain 5 (selection of reported outcomes), while Sims et al. presented additional concerns in Domain 3 (measurement of outcomes) and again in Domain 5. Lowe et al. 10 was assessed as having a lower overall risk; however, it did not report on random sequence generation or allocation concealment (Domain 1). In all trials, protocol modifications related to the occurrence of ARIA were implemented without clearly defined procedures for maintaining blinding. None of the trials explicitly reported the use of intention-to-treat analyses, and strategies for handling missing data were limited or unspecified. Selective reporting of safety outcomes was also noted, including underreporting of ARIA-related complications and mortality.
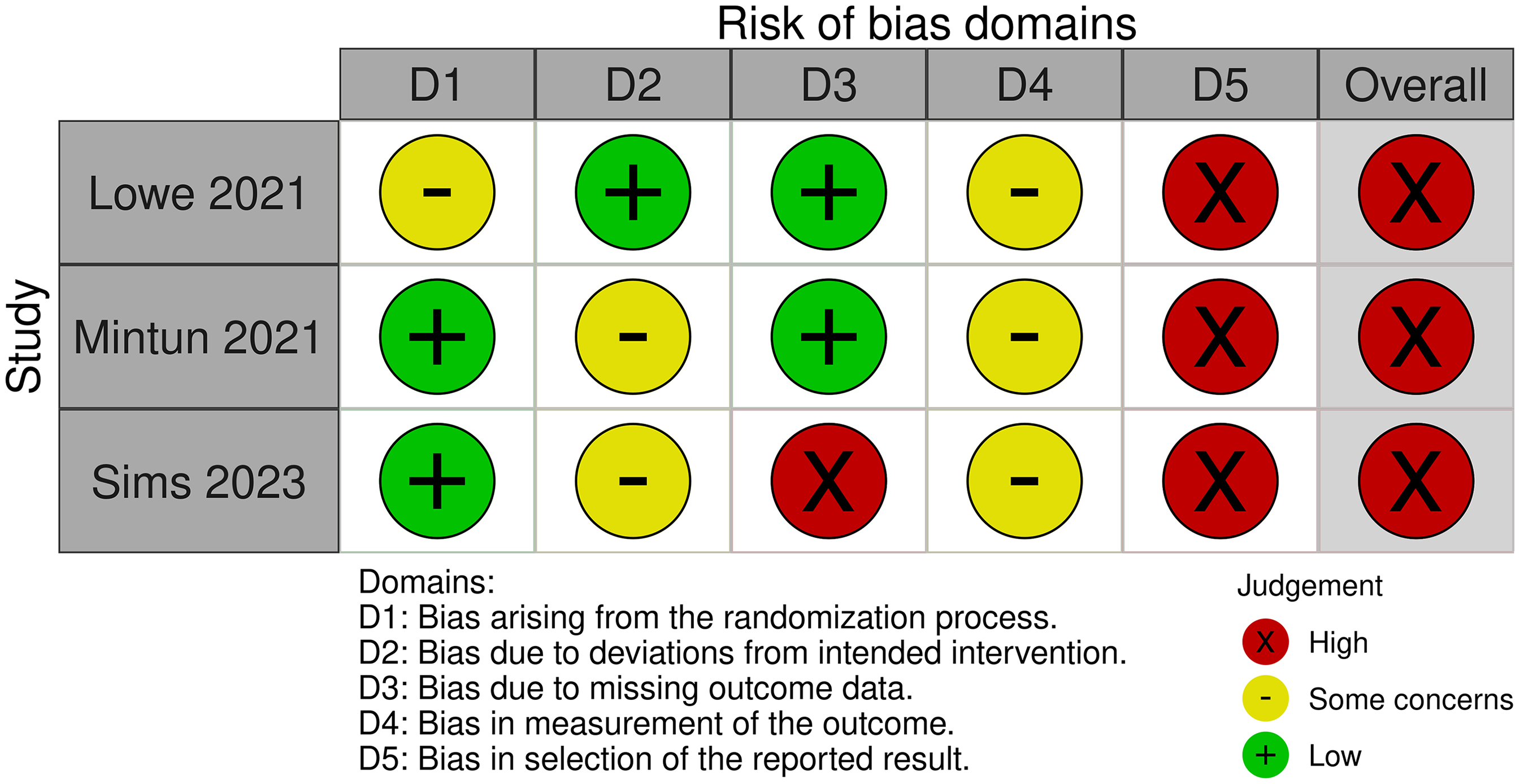
Risk of bias assessment of the included studies was conducted using version 2 of the Cochrane risk-of-bias tool for randomized trials (RoB2).
Discussion
In this meta-analysis, we provide the first comprehensive synthesis of the efficacy and tolerability of donanemab for the treatment of cognitive impairment in patients with AD. Given the increasing momentum behind disease-modifying therapies in AD, our primary objective was to consolidate available clinical evidence and deliver a quantitative assessment of donanemab's therapeutic profile, with particular emphasis on stratification by baseline tau burden and APOE genotype.
Consistent with previous research on anti-amyloid monoclonal antibodies such as gantenerumab, lecanemab, and aducanumab,14,43–46 dose-escalation studies have demonstrated that donanemab induces a rapid and dose-dependent reduction in cerebral amyloid plaques. 10 However, the interpretation of amyloid-PET findings remains a subject of ongoing debate. Experts have raised concerns regarding the anatomical specificity and clinical relevance of PET-detected amyloid reduction, noting that published imaging data frequently demonstrate tracer retention in white matter regions where amyloid deposition is minimal or absent in the early stages of AD. Confirming amyloid clearance in gray matter, where the pathological burden is most relevant, remains technically challenging and subject to methodological limitations. 47 Moreover, the degree of amyloid reduction attributed to donanemab has not been consistently paralleled by a proportional slowing of cognitive or functional decline, raising questions about the direct clinical utility of anti-amyloid interventions.
Our meta-analysis corroborates these biochemical effects, showing statistically significant improvements in cognitive and functional outcomes, including ADAS-Cog13 (MD, −1.86), CDR-SB (MD, −0.36), MMSE (MD, 0.64), and iADRS (MD, 3.19), compared to placebo. However, the magnitude of these changes, although statistically robust, remains modest and falls below established thresholds for minimal clinically important differences, suggesting that these effects are unlikely to be perceived by patients in their daily functioning. Thus, while donanemab may modestly slow the progression of cognitive decline, this does not appear to translate into perceptible clinical benefit. Moreover, responder rates were not reported in the included trials, preventing the calculation of the number needed to treat. Conversely, the number needed to harm was estimated to be approximately 3, indicating that one in every three patients exposed to donanemab develops ARIA-related adverse events. These findings should be interpreted with caution, particularly in light of ongoing debates regarding the clinical relevance of amyloid-targeted therapies. It is noteworthy that treatment effects were observed regardless of baseline tau burden, suggesting that donanemab's efficacy is not strictly dependent on tau stratification.
Based on these cognitive endpoints, it is essential to contextualize the interpretability of the instruments used. Among them, the iADRS warrants particular consideration. Although it was developed to jointly capture cognitive and functional decline and is increasingly used in anti-amyloid therapy trials the iADRS has yet to be widely adopted in routine clinical practice.37,48,49 In contrast, more established scales such as the MMSE and CDR-SB are widely validated and integrated into both clinical practice and regulatory frameworks.35,36 While the iADRS provides valuable complementary information, particularly in research contexts, its limited external validation underscores the importance of relying on globally recognized and routinely applied instruments for primary interpretation and cross-drug comparisons.
However, the efficacy profile of donanemab is tempered by its safety considerations. Treatment was associated with a markedly increased risk of ARIA-E and ARIA-H, particularly among APOE ε4 carriers. The incidence of ARIA-E varied by genotype, with homozygous ε4 carriers exhibiting the highest rates. ARIA-H was similarly elevated, primarily driven by cerebral microhemorrhages and superficial siderosis. These findings were consistent across included trials, strengthening the evidence for a genotype-dependent safety signal.
The safety profile of donanemab aligns with prior findings. In the study by Lowe et al., the drug was generally well tolerated, with ARIA-E being the most commonly reported adverse event, which resolved upon discontinuation of treatment. 50 The observed rates of ARIA-E fall within the expected range reported for other amyloid-targeting monoclonal antibodies. However, several studies have also documented reductions in brain volume and/or increases in ventricular size among patients treated with anti-amyloid antibodies, including donanemab.16,46,51–53 While these morphological changes are often attributed to amyloid plaque removal, their clinical significance remains uncertain. Emerging evidence suggests that such structural alterations may reflect accelerated neurodegeneration or compensatory shifts in brain tissue, with potential adverse functional consequences. 54
In addition to ARIA, adverse events such as infusion-related reactions and treatment discontinuations were more frequently reported in the donanemab group. Although the pooled mortality rate did not reach statistical significance, several deaths occurred in the context of ARIA-related complications, raising concerns about a potential underestimation of treatment-associated risk. Moreover, the incidence of ARIA-H, particularly cerebral microhemorrhages and superficial siderosis was consistently higher among participants receiving donanemab, reinforcing the need for rigorous safety monitoring. 55 In amyloid-negative individuals, the safety profile remains uncertain due to limited and heterogeneous data, preventing definitive conclusions and highlighting the need for further investigation in this subgroup.56,57
Taken together, our findings suggest that donanemab may provide clinical benefits in mitigating cognitive and functional decline in patients with AD, as demonstrated across multiple validated outcome measures.58,59 While these results are encouraging given the limited therapeutic options for early symptomatic stages of the disease, the observed effect sizes should be interpreted with caution, particularly regarding their clinical relevance. Subgroup analyses stratified by baseline tau burden and APOE ε4 genotype, though informative, are exploratory in nature and should not be used to guide clinical decisions. Their primary value lies in hypothesis generation and in identifying patterns that warrant further investigation in future trials. Larger-scale studies, conducted independently and with extended follow-up, are needed to clarify the clinical value of donanemab, establish its long-term risk–benefit profile, and define its role within an evolving therapeutic landscape. Importantly, the safety profile of donanemab most notably the increased risk of ARIA in genetically predisposed individuals, underscores the need for careful patient selection and rigorous safety monitoring. Further research is warranted to elucidate the long-term impact of donanemab, refine its risk–benefit assessment, and define its role in broader and more diverse patient populations.
It is also essential to consider the methodological quality of the included trials when interpreting donanemab's therapeutic profile. In our meta-analysis, two of the three trials exhibited a high overall risk of bias, primarily due to protocol deviations, incomplete outcome data, absence of intention-to-treat analyses, and selective reporting of outcomes. The occurrence of ARIA led to treatment modifications without clearly defined safeguards to maintain blinding, raising the possibility of functional unblinding and potential inflation of subjective cognitive outcomes. These limitations are consistent with the critical appraisal by Høilund-Carlsen et al., 14 who reported that the absolute gains on the CDR-SB (0.45 points) and iADRS (3.2 points) represented only 3.7% and 2.3% of their respective scale ranges well below accepted thresholds for clinical relevance and inferior to the benefits observed with conventional therapies such as cholinesterase inhibitors and memantine.49,60–63 In line with our findings, the Bayesian reanalysis conducted by Høilund-Carlsen et al. 14 indicated a lack of efficacy of donanemab even in the subgroup with low to medium tau burden. 14 Moreover, cumulative safety concerns including treatment-related brain volume loss of up to 6–7 cm³ underscore the need for independent, long-term trials using functional imaging endpoints and standardized adverse event reporting to determine the true clinical value of anti-amyloid therapies.
Limitation
Despite the strengths of this meta-analysis, several limitations should be acknowledged. First, the number of included studies was limited to three RCTs, with most quantitative comparisons based on only two studies.9,13 While meta-analyses with two studies are methodologically acceptable in emerging research areas, the restricted evidence base reduces statistical power and limits the generalizability of findings. This limitation is particularly relevant for subgroup analyses stratified by tau burden and APOE genotype, requiring cautious interpretation of the results. Second, heterogeneity in study design, inclusion criteria, and outcome reporting across trials may introduce bias and limit the comparability of results. Third, the relatively short follow-up period (maximum of 76 weeks) restricts insights into the long-term efficacy and safety of donanemab, especially regarding sustained cognitive benefits and delayed adverse events. Additionally, the available data on amyloid-negative individuals and underrepresented demographic groups were insufficient, constraining conclusions about donanemab's broader applicability. Fourth, the exclusion of patients who developed symptomatic ARIA during the clinical trials may have resulted in an underestimation of the incidence and clinical severity of these adverse events in real-world practice. The exclusion of patients who experienced early adverse events, such as symptomatic ARIA, may have introduced selection bias and led to an overestimation of the intervention's tolerability and efficacy. 64 Additionally, the scarcity or absence of robust data on treatment-related structural brain changes, such as volumetric atrophy and ventricular enlargement limits a comprehensive assessment of donanemab's safety profile, particularly regarding its functional and prognostic implications. Fifth, an important limitation is the absence of active comparator groups in the included trials. None of the studies evaluated donanemab against optimized conventional therapies, such as acetylcholinesterase inhibitors or memantine, which limits the contextualization of its efficacy relative to established treatment options. Given that these conventional agents remain widely accessible, cost-effective, and have demonstrated cognitive benefits in early AD, future RCTs should prioritize active comparator arms to more accurately define the therapeutic value of donanemab beyond placebo-controlled settings. Finally, publication bias cannot be entirely ruled out, as negative or inconclusive results may be underreported. An additional potential source of bias relates to unblinding. Since ARIA events occurred exclusively in the donanemab-treated group and often required protocol modifications, there is a risk that both participants and investigators became aware of treatment allocation. This unintentional unblinding may have influenced subjective cognitive assessments, potentially inflating the perceived treatment effect. Future trials should implement rigorous strategies to minimize unblinding-related bias, including the use of blinded outcome assessors and centralized, standardized evaluation protocols.
Conclusion
Donanemab provides questionable cognitive and functional benefits in patients with mild to moderate AD, regardless of baseline tau burden. While these effects are statistically consistent across trials, their magnitude appears modest and may not surpass those achievable with optimized conventional therapies, which remain safer and more cost-effective alternatives. Furthermore, treatment is associated with a significantly increased risk of ARIA and other adverse events, particularly in APOE ε4 carriers, underscoring the importance of careful patient selection and rigorous safety monitoring. In light of these considerations, larger-scale studies, conducted independently and with longer follow-up periods, are essential to clarify the true clinical value of donanemab, establish its long-term benefit-risk profile, and define its role within the therapeutic landscape of AD.
Supplemental Material
sj-docx-1-alz-10.1177_13872877251361044 - Supplemental material for Efficacy and APOE ε4-stratified risk of donanemab in Alzheimer's disease: A systematic review and meta-analysis of randomized clinical trials
Supplemental material, sj-docx-1-alz-10.1177_13872877251361044 for Efficacy and APOE ε4-stratified risk of donanemab in Alzheimer's disease: A systematic review and meta-analysis of randomized clinical trials by Anderson Matheus Pereira da Silva, Luciano Falcão, Filipe Virgilio, Isabelle Rodrigues Menezes, Marianna Leite, Elizabeth Farias, Maria Nascimento, Mariana Lee Han, João Paulo Mota Telles, Eryvelton de Souza Franco and Maria Bernadete de Sousa Maia in Journal of Alzheimer's Disease
Footnotes
Acknowledgments
We thank the Coordination for the Improvement of Higher Education Personnel (CAPES) for the financial support provided through its postgraduate scholarship program.
ORCID iDs
Author contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.