
Abstract
Background
Alzheimer's disease (AD) is a progressive neurodegenerative disorder frequently associated with dysphagia, leading to malnutrition, dehydration, and aspiration pneumonia. The Eating Assessment Tool-10 (EAT-10) is widely used for dysphagia screening; however, its reliability in advanced AD, where cognitive impairments hinder self-reporting, remains uncertain.
Objective
This study aimed to evaluate the diagnostic accuracy of EAT-10 in detecting dysphagia and aspiration across different AD stages.
Methods
The study included 30 AD patients classified into mild, moderate, and advanced stages based on Clinical Dementia Rating (CDR) scores. Dysphagia was assessed using EAT-10 and validated through Videofluoroscopic Swallowing Study (VFSS) and the Penetration-Aspiration Scale (PAS). Statistical analyses included the Mann-Whitney U test, Spearman correlation, and receiver operating characteristic (ROC) curve analysis (p < 0.05).
Results
EAT-10 scores significantly differed across AD stages (p = 0.001), with mean scores of 3.11 ± 1.17 (mild), 11.70 ± 4.64 (moderate), and 18.00 ± 6.90 (advanced). Unsafe swallowing and aspiration were observed in 43.3% and 23.3% of patients, respectively, with higher prevalence in advanced AD. ROC analysis determined an EAT-10 cut-off score of 15 for unsafe swallowing (AUC: 0.96, sensitivity: 88%, specificity: 77%) and 18 for aspiration (AUC: 0.81, sensitivity: 81.2%, specificity: 75%). Strong correlations were found between EAT-10 and PAS scores (r = 0.812, p < 0.001).
Conclusions
EAT-10 is an effective screening tool for dysphagia and aspiration risk in early and moderate AD stages. However, in advanced AD, objective assessments like VFSS remain essential to complement EAT-10 results. Integrating EAT-10 into routine evaluations may enhance early detection, enabling timely interventions and improved clinical outcomes.
Introduction
Alzheimer's disease (AD) is one of the most common types of dementia worldwide and is a progressive neurodegenerative disorder that affects memory, orientation, judgment, language, and activities of daily living.1,2 With the progression of the disease, severe impairments in sensorimotor and motor functions also occur. This may cause dysphagia by affecting swallowing functions. Dysphagia refers to impairment at any stage of the swallowing act and is frequently observed in patients with AD. 3
Dysphagia leads to serious complications such as aspiration pneumonia, malnutrition, dehydration and weight loss in AD patients, significantly decreasing quality of life and increasing mortality rates.4,5 Especially aspiration pneumonia is one of the most common causes of mortality associated with dysphagia in AD patients. 1 Therefore, early diagnosis and treatment of dysphagia symptoms are critical in terms of preventing these complications and improving quality of life. 6
Swallowing-specific objective assessment tools are needed to determine dysphagia. Swallow-specific tools such as videofluoroscopic swallow study (VFSS) and fiberoptic endoscopic swallow study (FEES) are necessary to assess swallowing adequacy, airway protection and food escape into the airway. These methods are the gold standards for swallowing evaluation7–9; however, the fact that the majority of AD patients are elderly, have comorbid diseases, and require specialized instrumentation and experienced personnel for objective evaluations constitute limitations for the use of objective methods in clinics. Therefore, it is not possible to apply these methods to detect potential aspiration risks for every dysphagia patient. For this purpose, it may be appropriate to use a valid, reliable screening tool that can be applied in patients before objective swallowing assessments. Especially in underdeveloped countries that lack sufficient resources and equipment for instrumental dysphagia assessment, it is important to use a screening tool with high predictive ability to distinguish between swallowing safety and aspiration.
Eating Assessment Tool-10 (EAT-10), one of the screening tools that can be used for this purpose, is a rapid and reliable tool that measures dysphagia symptoms. 3 EAT-10 is a screening tool that has been translated into many languages and its validity and safety have been proven in different countries with its feature of being a rapid and easy-to-administer tool in identifying individuals at risk who need a more comprehensive instrumental evaluation of swallowing function. The EAT-10 is widely preferred especially in the identification and severity of dysphagia symptoms in patients with AD. 10 The number of individuals with AD is increasing with the increase in risk factors and the aging population. This may be due to the patient's sensory and motor impairments as well as being older. 11 Research reports show that 90% of hospitalized individuals with dementia and 84–93% of individuals with moderate to severe AD experience dysphagia. 12 Although studies indicate that dysphagia is more common in advanced stages of AD, the time of onset of dysphagia during the disease process is unknown and dysphagia symptoms can be seen even in mild stages of AD. 13 Therefore, recent studies with individuals with dementia emphasize that these individuals should be evaluated for dysphagia from an early stage. 14
Dysphagia in patients with AD usually affects all stages of the swallowing process starting from oral preparation and oral phase. While symptoms such as decreased taste and odor perception, decreased saliva production and delayed swallowing reflex may be observed in the oral phase, complications such as decreased hyolaryngeal elevation, decreased upper esophageal sphincter patency and increased oral residues occur in the later stages.4,5 Especially in the advanced stages of the disease, aspiration pneumonia is among the leading causes of death in AD patients. 2
Cognitive level is a critical factor in the evaluation of dysphagia in patients with AD, as individuals in advanced stages may have difficulty understanding subjective assessment tools like the EAT-10, potentially compromising the reliability of self-reported outcomes. Previous studies examining the relationship between EAT-10 scores and objective measures of swallowing across different patient populations have produced inconsistent findings,5,15–17 emphasizing the importance of accounting for cognitive decline in such evaluations. In this study, AD stages were categorized based on clinical dementia ratings and functional status: the mild stage included individuals with early cognitive impairment and preserved independence; the moderate stage comprised patients with more pronounced memory and communication deficits and partial dependence in daily activities; and the severe stage reflected profound cognitive deterioration, impaired communication, and complete daily dependence. These classifications provided a framework for investigating the effectiveness of the EAT-10 in distinguishing the severity of dysphagia and aspiration across AD stages. Accordingly, this study aimed to determine the discrimination ability of EAT-10 in detecting dysphagia and aspiration according to AD stage.
Methods
Participants
This study was conducted between January and November 2024 at the Neurology Clinic of Atlas University Hospital with 30 AD patients over the age of 60 who were admitted to the clinic and diagnosed with AD according to the DSM-V (Diagnostic and Statistical Manual of Mental Disorders) 18 and the National Institute on Aging and Alzheimer's Association (NIA-AA) diagnostic criteria. 19 Patients were included in the study if (i) they were not allergic to barium, (ii) they had a dementia stage determined using the Clinical Dementia Rating (CDR), (iii) they had only Alzheimer's-type dementia, and (iv) they did not have any additional neurological disease (e.g., Parkinson's disease, multiple sclerosis, and stroke). Patients with other disorders that may affect swallowing function (e.g., head and neck cancer), those with a history of dysphagia before the diagnosis of AD, and patients with hearing loss that may affect the scale results were excluded. The CDR scale, 20 which includes 6 categories (memory, orientation, reasoning and problem solving, community work, home and hobbies, and personal care), and the Turkish version of the Mini-Mental State Examination (MMSE) test 21 were used to assess cognitive status. According to the CDR scores, patients were categorized as mild AD (CDR 1), moderate AD (CDR 2) and severe AD (CDR 3). Informed written consent was obtained from all patient and/or caregiver during the study and all met the specified inclusion criteria. The study was approved by the Ethics Committee and Commissions of Istanbul Atlas University (Date: 30.10.2023, No: 34026) and was conducted in accordance with the Declaration of Helsinki.
Assessment procedure
Clinical swallowing assessment
Clinical assessment of patients for dysphagia was determined by the EAT-10. The EAT-10 is a validated, self-administered, symptom-specific dysphagia outcome tool that has been implemented in clinics worldwide and validated in Turkish. 22 The EAT-10 consists of 10 questions with a 5-point Likert scale to assess dysphagia severity and its clinical and social impact, and questions are scored from 0 to 4 (0 = no problem, 4 = serious problem). The total EAT-10 score is calculated by summing the scores of each question. A total score of 3 or more indicates a risk of swallowing disorder and higher scores indicate a perception of a high level of dysphagia severity.
The EAT-10 scale was administered to each patient on a single occasion in an examination room by a speech-language pathologist (SLP) blinded to the patient's medical history. Information was collected from each participant and/or their primary caregiver, who was familiar with the participant's eating behavior. In patients with advanced-stage AD, data were specifically obtained from the primary caregiver, who could provide reliable details about the patient's functional status and spent at least 20 h per week caring for them. It was emphasized that a “symptom” should represent a significant change from the participant's pre-disease condition rather than a long-standing characteristic. The EAT-10 questions and answer choices were read aloud to the patient and/or caregiver by a SLP to minimize the potential impact of low educational attainment and reduced visual acuity, thus trying to facilitate correct understanding of the questionnaire and minimize misleading answers due to lack of understanding of the questionnaire. To avoid possible bias, the same procedure was followed for all participants.
Instrumental swallowing assessment
Patients were objectively evaluated using VFSS on the same day they answered the EAT-10. VFSS is widely used in the evaluation of swallowing disorders and is considered the gold standard among swallowing assessment methods. 8 General Electric Precision RXi fluoroscopy device was used for VFSS evaluation. Patients were positioned upright at a 90° angle, 1.5 meters away from the X-ray tube, and their heads were fixed laterally. VFSS sequences were recorded continuously at 30 frames per second at full resolution and digitally captured. Patient positioning ensured that certain boundaries were visible in the images, including the anterior lips, posterior pharyngeal wall, lower cervical esophagus and upper nasopharynx.
All subjects underwent a standardized modified barium swallow study and each patient completed three swallow trials for both liquid and semi-solid consistencies. The consistencies used during testing were prepared according to the International Dysphagia Diet Standardization Initiative (IDDSI) criteria. 23 Initially, liquid consistencies were administered using controlled volumes (3 x teaspoons of 5 ml), followed by sips self-modulated by patients in a free volume environment. Semi-solid consistencies were administered in three portions, each consisting of a controlled single teaspoon containing 5 ml per mouthful. Finally, the patient was given a piece of bread and instructed to take a single bite. For statistical analysis, 5 ml for liquids. IDDSI-0 for liquids, 5 ml for semi-solid consistencies. IDDSI-4 for semi-solid and IDDSI-7 for solid.
The clinical swallowing assessment was conducted by a SLP, while the instrumental assessment was performed by a second SLP with a minimum of 15 years of experience in VFSS. The SLP conducting the instrumental evaluation completed the assessment in a blinded manner, without knowledge of the patient's disease stage or the results of the clinical swallowing assessment. VFSS-recorded images were analyzed using the Functional Oral Intake Scale (FOIS) and the Penetration-Aspiration Scale (PAS). For each consistency, the highest PAS score among all bolus trials was considered for analysis.
The FOIS is a 7-point scale that evaluates the level of oral intake in patients with dysphagia, ranging from complete reliance on tube feeding to full oral intake without restrictions. Levels 1–3 represent varying degrees of non-oral feeding or minimal oral intake, while levels 4–7 indicate increasing levels of oral intake, with level 7 indicating a full oral diet without restrictions. 24
The PAS is used to describe the severity of penetration and aspiration. It is an 8-point clinical scale used to grade penetration and aspiration and to determine whether material entering the airway is expelled. 25 A PAS score of 1–2 indicates normal airway protection without penetration and aspiration during swallowing. Scores between 3–5 are considered penetration, which means that food enters the larynx but does not pass below the vocal cords, and scores between 6–8 are considered aspiration. 26
In the study, swallowing trials at each consistency were considered “safe swallowing” if the PAS score was PAS ≤ 2 (penetration/aspiration -) and “unsafe swallowing” if the PAS score was ≥3 (penetration/aspiration +).
It is important to note that transient penetration may occasionally occur even in healthy geriatric individuals. In this study, we adopted a conservative approach in our PAS-based classification. Any PAS score ≥3, including transient or isolated penetration episodes, was categorized under the “unsafe swallowing” group. This classification was made to ensure consistency and to reduce the risk of underestimating swallowing impairment in a cognitively vulnerable population such as those with AD.
Data analysis
Data were analyzed with IBM SPSS 26.0 program (IBM SPSS Inc., Chicago, IL). The study investigated the relationship between disease duration, disease stage and dysphagia in AD patients. Descriptive statistics were presented as frequency and percentage for categorical variables, and as mean and standard deviation for continuous variables. The Shapiro-Wilk test was used to assess the normality of the distribution of scores across all scales. The test indicated that none of the scale scores followed a normal distribution; therefore, Spearman's rank-order correlation analysis was employed to examine the relationships between variables. Correlation coefficients were interpreted as low correlation between 0.05–0.30, moderate correlation between 0.30–0.60, high correlation between 0.60–0.75 and very high correlation between 0.75–1.00. 27 Kruskal-Wallis test was used to evaluate the differences between groups for more than 2 groups and Mann-Whitney U test was used for comparisons between two groups.
To determine the diagnostic accuracy of EAT-10, a receiver operating characteristic (ROC) curve was constructed by calculating area under the curve (AUC) with 95% confidence intervals (CI), sensitivity, specificity, optimal cut-off point, positive predictive value (PPV), negative predictive value (NPV) and likelihood ratios (LR). The optimal cut-off point was determined using Youden's J statistic. All statistical analyses were evaluated and significance was evaluated at the p < 0.05 level.
Results
Of the AD patients who participated in the study, 14 (47.7%) were male and 16 (53.3%) were female. The mean age of the participants was 75.23 ± 7.19 years, the youngest participant was 64 years old and the oldest was 90 years old. According to the CDR scores, the patients were categorized as mild, moderate and advanced AD. Of the patients, 9 (30%) were mild, 10 (33.3%) moderate and 11 (36.7%) advanced. There was no statistically significant difference between the groups in terms of age, gender and educational level. There was a statistically significant difference between the groups in terms of disease duration, FOIS, MMSE and EAT-10 scores. Demographic and clinical characteristics of the participants are shown in Table 1.
Demographic and clinical characteristics of AD patients.

CDR: Clinical Dementia Rating; MMSE: Mini-Mental State Examination; EAT-10: Eating Assessment Tools; x̄: Mean; SD: standard deviation. Results with significant p-value are shown in bold *p < 0.05, **p < 0.01 is considered statistically significant.
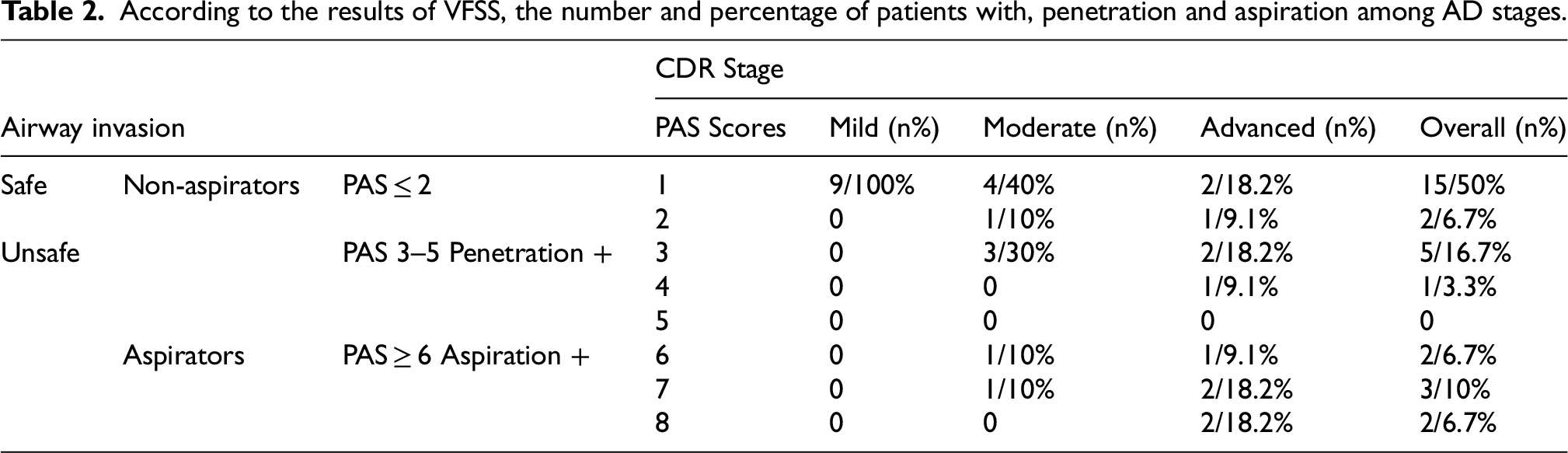
Of the AD patients included in the study, 6 (20%) had penetration and 7 (21%) had aspiration. While 17 (56.7%) of all patients swallowed safely, 13 (43.3%) did not. Of the patients with penetration, 3 were moderate and 3 were advanced AD patients. Of the patients with aspiration, 2 (20%) were moderate and 5 (45.5%) were advanced AD patients. Of the 11 patients with advanced AD, 3 (27.3%) swallowed safely and 8 (72.7%) swallowed unsafely. Of the 10 patients with moderate AD, 5 (50%) swallowed safely and 5 (50%) swallowed unsafely. None of the patients with mild AD showed signs of penetration and aspiration and all of them were safe to swallow (Table 2). In addition, there was a statistically significant, positive, high-level (r:0.657; p:0.0001) correlation between AD stages and PAS scores. The higher the AD grade of the participants, the higher their score on the PAS scale and the probability of penetration/aspiration increased significantly towards the advanced stage.
According to the results of VFSS, the number and percentage of patients with, penetration and aspiration among AD stages.
The mean EAT-10 score of the patient included in the study was 11.43 ± 7.83. The mean EAT-10 scores of patients with safe swallowing during VFSS were 9.22 ± 6.86 and 6.18 ± 4.08 in IDSSI 4 and IDSSI 0 consistency, respectively, while the mean EAT-10 scores of patients with unsafe swallowing were 19.5 ± 6.86 and 18.3 ± 5.97. A statistically significant difference was found between patients with safe and unsafe swallowing in both consistencies (p = 0.010, p = 0.001). The mean EAT-10 scores of patients without aspiration during VFSS were 9.96 ± 6.81 and 9.39 ± 6.78 at IDSSI 4 and IDSSI 0 consistency, respectively, while the mean EAT-10 scores of patients with aspiration were 21.00 ± 8.08 and 18.14 ± 7.69. A statistically significant difference was found between patients with and without aspiration in both consistencies (p = 0.025, p = 0.014) (Table 3).
Comparison of EAT-10 scores among Alzheimer's disease patients with safe versus unsafe swallowing and aspirators versus non-aspirators, by IDDSI level.

In addition, there was a statistically significant difference in EAT-10 scores between AD stages (p = 0.001). The EAT-10 scores of patients with mild, moderate and advanced AD were 3.11 ± 1.17, 11.70 ± 4.64 and 18.00 ± 6.90, respectively (Table 1). According to the EAT-10 results, 80% of all patients, 30% of patients with mild AD, and 100% of patients with moderate and severe AD had dysphagia. In addition, there was a statistically significant, positive, very high correlation (r:0.822; p:0.0001) between AD stages and EAT-10 scores.
The relationship between PAS scores and EAT-10 scores in AD patients was analyzed and the results are presented in Table 4.
Correlation analysis results between PAS and EAT-10 total scores by IDDSI level.

*p < 0.05, **p < 0.01 is considered statistically significant.
A linear correlation was found between EAT-10 and PAS scores in both consistencies. There was a statistically significant, positive, very high correlation between PAS IDDSI 0 consistency scores and EAT-10 scores (r:0.812; p:0.0001), and a statistically significant, positive, moderate correlation between PAS IDDSI 4 consistency and EAT-10 scores (r:0.504; p:0.004) (Table 4).
ROC analysis was performed to determine the discriminative ability of EAT-10 in detecting swallowing safety and aspiration in patients with AD and the results are given in Table 5 and Figure 1.

ROC curve analysis results for the ability of the EAT-10 to identify AD patients who swallow safe versus unsafe and non-aspirators versus aspirators. Safe versus Unsafe. Non-aspirators versus Aspirators.
ROC curve analysis results for between safe (PAS ≤ 2) versus unsafe (PAS ≥ 3) swallowers and non-aspirators (PAS ≤5) versus aspirators (PAS ≥ 6).

*p < 0.05, **p < 0.01 is considered statistically significant. PPV: positive predictive value; NPV: negative predictive value; +LHR: positive likelihood ratio; -LHR: negative likelihood ratio; AUC: area under curve.
ROC analysis results showed that EAT-10 significantly discriminated both swallowing safety and aspiration in AD patients (AUC: 0.96, p < 0.001; AUC: 0.81, p = 0.014). The cut-off value for discrimination of swallowing safety was 15 and the cut-off value for predictive assessment of aspiration was 18. Furthermore, the EAT-10 showed a sensitivity of 81.2% (95% CI: 65.0–97.0), specificity of 75.0% (95% CI: 62.2–89.1), PPV of 80.0% (95% CI: 69.0–91.0) and NPV of 76.0% (95% CI: 64.0–88.0) for predicting aspiration. In addition, the positive odds ratio was calculated as 3.24 (95% CI: 3.03–3.45) and the negative odds ratio as 0.25 (95% CI: 0.04–0.46).
Comparisons based on ROC analysis were also made for patients with safe swallowing versus unsafe swallowing. The EAT-10 demonstrated a sensitivity of 88.0% (95% CI: 79.0–95.0), a specificity of 77.0% (95% CI: 65.1–89.3), a PPV of 85.0% (95% CI: 75.0–95.0) and a NPV of 78.0% (95% CI: 67.0–89.0) in predicting swallowing safety. In addition, the positive likelihood ratio was 3.83 (95% CI: 3.65–4.01) and the negative likelihood ratio was 0.16 (95% CI: 0.00–0.34).
Discussion
Dysphagia findings are observed starting from the early stages of AD. As the degree of AD increases, swallowing function decreases and the risk of aspiration increases. As in all neurogenic dysphagia problems, early detection of dysphagia symptoms in AD is of great importance. 4 Early evaluation of dysphagia is crucial to prevent complications such as malnutrition, dehydration, weight loss, inadequate oral intake, decreased quality of life, depression and aspiration pneumonia.28,29
Instrumental assessment methods such as VFSS and FEES are considered the gold standard for evaluating swallowing efficiency, airway protection, and aspiration in patients with dysphagia, although they may not always be accessible in clinical settings. 30 These methods require specialized equipment, trained personnel, dedicated space, and time, which may limit their application for every patient to identify aspiration risks. Therefore, there is a need for a valid, reliable and easily applicable screening tool that offers high discrimination in detecting dysphagia and aspiration risk in patients with AD. 10
The aim of this study was to determine the discriminative ability of the EAT-10 to detect dysphagia and aspiration according to AD stage. The results of our study showed that the EAT-10 has the discriminative ability to identify patients with swallowing insecurity and aspiration. EAT-10 scores were approximately 3 times higher in AD patients with aspiration than in those with safe swallowing. This value indicated that it correctly identified 88.0% of AD patients with unsafe swallowing and 81.2% of AD patients with aspiration. In our study, the cut-off score to determine swallowing safety was 15 and the cut-off score to determine aspiration risk was 18. These values were derived from ROC curve analyses conducted on the overall pooled sample, rather than separately for each stage of AD.
In the literature, the relationship between the EAT-10 score and both swallowing efficiency and safety has been investigated in various studies, including patients with different diagnoses. In some studies to date, it has been reported that EAT-10 has a high discrimination power in patients with aspiration.3,5,10,15,31,32 However, in these studies, different cut-off points were suggested for the detection of safe swallowing and aspiration. The cut-off points recommended in other studies vary between 2 and 16. 26 For example, both Plowman et al. and Printza et al. reported a cut-off score of 8 for individuals with amyotrophic lateral sclerosis,15,31 while Cheney et al. reported a cut-off score of 15 and Arslan et al. reported a cut-off score of 16 for a group of patients with different etiologies of dysphagia.3,10 These differences between cut-off scores may be due to methodological differences in the studies and the etiology of dysphagia in the studied populations. Another reason that may explain the heterogeneity in cut-off scores for aspiration in other studies may be cultural differences. Notably, among the various language adaptations of the EAT-10, the highest mean scores have been reported in the Turkish version, 33 which may partly account for the higher cutoff values identified in our study compared to others. However, it is important to note that no formal cross-linguistic analysis has been conducted to confirm the impact of these factors. Therefore, the cutoff values identified in this study may not be directly generalizable to other linguistic or cultural contexts, and caution is advised when applying these thresholds in different clinical settings. While some of the studies conducted to determine the discrimination ability of the EAT-10 in detecting dysphagia and aspiration reported the relationship between the EAT-10 score and aspiration only,3,10,15 others examined this relationship for both aspiration and residue after swallowing.4–6,16,17 Apart from this, there are also differences between the instrumental assessment methods used. While FEES was used in some studies, VFSS was used in others. In contrast to these findings, some studies in the literature failed to obtain a cut-off point for detecting aspiration and reported that the EAT-10 failed to detect aspiration.4,6,17 One of the questions that this study seeks to answer is the ability of the EAT-10 to predict objective findings as an information source in different stages of AD where cognitive effects change. According to the results of our study, as the AD stage progressed, the swallowing safety of the patients deteriorated and the rate of penetration and aspiration increased. The scores of the AD patients who participated in our study on both the EAT-10 and PAS scales increased significantly as the AD grade increased. These findings are similar to other studies in the literature.14,34,35 This may be due to the fact that cellular destruction caused by neurodegeneration, together with cognitive impairment, involves the primary sensory and motor cortices, leading to an increase in the severity of dysphagic symptoms.
In the literature, the number of studies on the instrumental assessment of swallowing and swallowing in patients with AD is limited.36,37 Leder et al., 38 in a study of patients with altered cognitive status as a result of different etiologies including dementia, asked patients orientation questions in an acute care setting and reported that they were able to predict the presence of aspiration before FEES by following simple verbal commands. In our study, a high correlation was observed between the EAT-10 scores, which include the subjective reports of the patients, and the PAS scores obtained with the VFSS, which is an objective assessment tool. In addition, a significant difference was found between EAT-10 scores in both IDDSI-4 and IDDSI-0 consistency when safe swallowers and non-safe swallowers and aspirators and non-aspirators were compared according to PAS scores.
In our study, EAT-10 scores indicated that patients presented with signs of dysphagia starting from the mild severity level. According to the EAT-10 results, the number of patients with dysphagia increased towards the advanced stage. When we ignored the cut-off score we found in our study and accepted the EAT-10 score as ≥ 3, 80% of all patients in our study, 30% of patients with mild AD, and 100% of patients with moderate and advanced AD had dysphagia. However, when the PAS scores obtained as a result of the evaluation with VFSS were analyzed, aspiration was not detected in any of the patients with mild AD. Aspiration was detected in only 20% of moderate patients and 45.5% of severe patients. One reason for this finding may be that the accuracy of completing the EAT-10 worsens with the progression of the disease and the patient may not be able to accurately identify complaints of dysphagia. It may be misleading in patients with dementia due to cognitive impairment, deficits in verbal communication and loss of insight. Although dysphagia is commonly seen in patients with AD, it has been shown that their level of awareness of swallowing difficulties is often low. 1 Possible causes include cognitive decline affecting the integration of sensory and motor functions related to swallowing. 5 Furthermore, structural and functional impairments in the oral, pharyngeal and laryngeal regions are thought to further reduce patients’ awareness of dysphagia by reducing somatosensory feedback. 17 The discrepancy observed between EAT-10 scores and aspiration findings across AD stages suggests that the EAT-10 may be sensitive in detecting potential swallowing difficulties, particularly in the early stages. However, it also underscores the limitation of self-report-based assessment tools, which may be influenced by cognitive impairments and may not always align with objective clinical findings. Progressive cognitive decline in AD compromises individuals’ ability to monitor, assess, and communicate their symptoms, contributing to the ongoing debate in the literature regarding whether patients or caregivers provide more reliable information.14,39,40 Accordingly, in this study, EAT-10 responses for patients in advanced stages were collected from primary caregivers who closely observed the patients’ eating behaviors. Nonetheless, due to the limited sample size, patient and caregiver responses could not be statistically analyzed as separate groups, which constitutes a limitation of the study.
This study aimed to assess the discriminatory capacity of EAT-10 in individuals at various stages of AD; however, several methodological limitations need to be considered. Most importantly, the relatively small sample size from a single center and the lack of a healthy control group limit the statistical power of the analyses and limit the ability to distinguish the effects of AD from those attributable to normal aging. These factors collectively compromise the external validity of the findings. In addition, although ROC curve analyses were performed on a pooled sample and yielded general cutoff values, this approach prevents the identification of stage-specific differences that may be of clinical importance. To increase the robustness and generalizability of future studies, we recommend the application of a priori power analyses, the inclusion of larger and more heterogeneous cohorts through multicenter participation, the inclusion of appropriate control groups, and the use of stage-specific ROC analyses to derive clinically actionable thresholds tailored to AD severity
Conclusion
In conclusion, our study demonstrated that the EAT-10 has a discriminative ability to identify patients with AD who lack swallowing safety and are at risk of aspiration. As the severity of AD increases, patients experience a decline in swallowing safety and a higher likelihood of aspiration. While we report that the EAT-10 offers significant clinical utility and discriminative power in detecting aspiration risk in the AD patient group, it is important to emphasize a crucial caveat regarding our findings. It should be noted that such a screening tool cannot and should not replace the need for a comprehensive clinical evaluation. Therefore, it is recommended that the EAT-10 be integrated into comprehensive clinical assessments to provide additional information to support clinical decision-making and to refer patients for further swallowing evaluations. Specifically, it can serve as a screening tool for identifying the presence of dysphagia in AD patients at risk of airway compromise.
Footnotes
Acknowledgments
The authors have no acknowledgments to report.
Ethical considerations
This study was conducted in accordance with the Declaration of Helsinki and was approved by the by the Ethics Committee and Commissions of Istanbul Atlas University (Date: 30.10.2023, No: 34026)
Consent to participate
Written informed consent to participate in the study was obtained from all patients and/or their caregiver.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data used to support the findings of this study are included within the article.