
Abstract
Background
Alcohol use disorder (AUD), epilepsy, hemorrhagic stroke (HS), and traumatic brain injury (TBI) are all linked to neuroinflammation and associated with an increased risk of Alzheimer's disease (AD). Drug responses in cognitive health remain largely unknown in patients with neuroinflammation-related conditions.
Objective
To investigate the associations between drug exposure and AD incidence in patients with neuroinflammation-related conditions.
Methods
We derived covariate matched cohorts for individuals with and without neuroinflammation-related conditions (e.g., AUD, epilepsy, HS and TBI) from a US nationwide insurance claim data. We used covariate-adjusted Cox models to estimate the hazard ratios (HRs) of drug exposure on AD. We identified neuroinflammation-specific drug responses by comparing HRs between individuals with and without neuroinflammation-related conditions.
Results
We identified 0.4 million matched pairs of individuals with and without neuroinflammation-related conditions. We identified three drugs (levothyroxine [HR = 0.89], mirabegron [HR = 0.69], and ropinirole [HR = 0.81]) had a lower HR and two drugs (levetiracetam [HR = 1.19], and quetiapine [HR = 1.83]) had a higher HR in individuals with neuroinflammation-related conditions compared to without (false discovery rate <0.05).
Conclusions
In patients with neuroinflammation-related conditions, we identified drugs associated with lower risks (levothyroxine, mirabegron and ropinirole) and higher risks (levetiracetam and quetiapine) of AD incidence.
Introduction
Alcohol use disorder (AUD), epilepsy, hemorrhagic stroke (HS), and traumatic brain injury (TBI) can induce neuroinflammation,1–4 which can further affect cognitive health.5,6 In fact, patients with these conditions have a higher incidence of developing Alzheimer's disease (AD).7–13
Real-world data-based (RWD-based) pharmacoepidemiologic studies have identified drugs that may have potential beneficial or adverse effects in AD.14,15 For instance, US Medicare data-based studies identify exenatide (a type 2 diabetes drug) is associated with a reduced risk of AD, 16 and exposure of anticholinergic drugs is associated with an increased risk of AD. 15 Furthermore, leveraging the diversity of RWD can reveal precise drug responses in AD in subpopulations, especially for certain underrepresented subpopulations in AD clinical trials. In a recent study, telmisartan is associated with a reduced risk of AD in African Americans, but has a neutral association with AD in non-Hispanic White Americans. 17 Currently, drug responses in cognitive health and/or AD remain largely unknown for patients with neuroinflammation-related conditions.
In this study, we compared drug responses in AD between individuals with and without neuroinflammation-related conditions (e.g., AUD, epilepsy, HS, and TBI) in a quasi-difference-in-difference setting. We used a large-scale US nationwide health insurance claim data and covariate-adjusted Cox model to investigate frequent drugs. We identified drugs that might have potentially differential effects in AD in patients with neuroinflammation-related conditions compared to without.
Methods
Data source and preprocessing
We used Optum's de-identified Clinformatics® Data Mart Database (2007–2021). Optum's Clinformatics® Data Mart (Clinformatics) is derived from a database of administrative health claims for members of large commercial and Medicare Advantage health plans. The data included demographics variables (e.g., sex, birth year, and race), enrollment records, diagnoses, and pharmacy claims. The Indiana University Institutional Review Board (IRB) designated this study as exempt.
We used ICD-9 and ICD-10 codes to identify phenotypes. We used established algorithms to identify alcohol use disorder (AUD; e.g., ICD-9: 291*, 303*, and ICD-10: F10*, etc.), 18 epilepsy (e.g., ICD-9: 345*, and ICD-10: G40*), 19 hemorrhagic stroke (HS; e.g., ICD-9: 430, 431, 432*, and ICD-10: I60*, I61*, I62*), 20 and traumatic brain injury (TBI; e.g., ICD-9: 850*, 851*, and ICD-10: S06*). 21 We used a validated algorithm to identify Alzheimer's disease (AD; e.g., ICD-9: 331.0, ICD-10: F00*, G30*). 22 We used the R package comorbidity to identify AIDS, cancer, cerebrovascular disease, congestive heart failure, chronic pulmonary disease, diabetes, dementia, depression, hemiplegia or paraplegia, liver disease, myocardial infarction, peptic ulcer disease, peripheral vascular disease, other neurological disorder, psychoses, renal disease, and rheumatoid arthritis. 23 We used the drug name look up table from the data source and RxNorm to assess drug exposure. 24
As described in our previous work, 11 we derived covariate matched cohorts for AUD, epilepsy, HS and TBI (i.e., neuroinflammation-related conditions) (Figure 1(a)). We included individuals with ≥60 years of age and ≥2 years of enrollment. First, we identified patients with neuroinflammation-related conditions. Specifically, we identified patients that had their earliest known neuroinflammation-related diagnosis after 365 days of the enrollment start date. We defined the index date as the first diagnosis date for patients with neuroinflammation-related conditions. We excluded patients with AD, AIDS, cancer, dementia, and/or hemiplegia/paraplegia prior to the index date. Second, we matched patients with neuroinflammation-related conditions to individuals without the corresponding conditions on index date, age, gender, race, and comorbidities (e.g., cerebrovascular disease, congestive heart failure, chronic pulmonary disease, diabetes, depression, liver disease, myocardial infarction, peptic ulcer disease, peripheral vascular disease, other neurological disorder, psychoses, renal disease, and rheumatoid arthritis). Specifically, for each and every patient, we randomly selected a matched individual from all individuals met the following criteria: (i) without the corresponding neuroinflammation-related condition, (ii) without AD, AIDS, cancer, dementia, and/or hemiplegia/paraplegia prior to the corresponding patient's index date, and (iii) with same gender, race, birth year, and comorbidities on the corresponding patient's index date. In other words, a matched pair had no AD, AIDS, cancer, dementia, and/or hemiplegia/paraplegia prior to the index date, and the matched pair had same age, race, gender, and comorbidities on the index date.
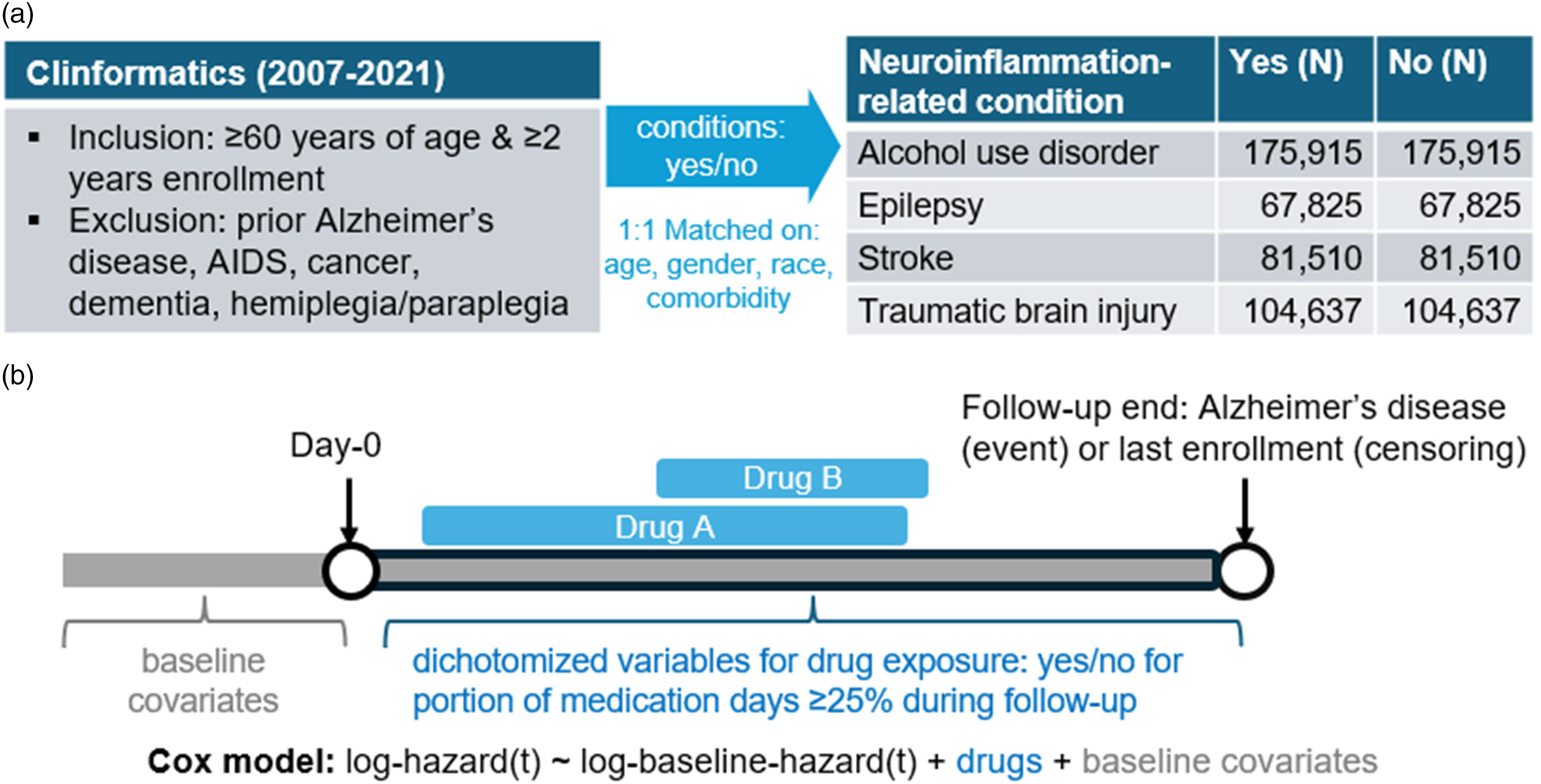
Illustration of study design and analytical model. (a) Derivation of analytical datasets; (b) Illustration of analytical model.
We derived eight cohorts for individuals with and without a neuroinflammation-related condition for all four neuroinflammation-related conditions. We defined the outcome as time from index date (i.e., day-0) to the first diagnosis date of AD. We censored Individuals without any outcome at the last date of enrollment. We assessed data on drug exposure during follow-up periods. We defined binary drug exposure covariates (i.e., yes/no for percent of medication days ≥25% during the follow-up period) for frequent drugs in all cohorts (Figure 1(b)). We used 25% as the threshold based on a recent pharmacoepidemiologic study of AD. 17
Statistical analyses
We fitted covariate-adjusted Cox models to the eight cohorts (Figure 1(b)). The outcome was time to AD. The covariates included gender, race, age, comorbidity status (i.e., yes/no) at index date; as well as drug exposure covariates. We estimated the coefficients and standard errors for all drug exposure covariates.
We conducted meta-analysis on coefficients (e.g., log-hazard ratios [log-HRs]) by setting weights as the inverse of the variance across the four cohorts with neuroinflammation-related conditions, and across the four cohorts without neuroinflammation-related conditions. First, we estimated the HRs, and the false discovery rates (FDRs) by using the Benjamini-Hochberg procedure in patients with neuroinflammation-related conditions for all drugs. 25 Second, we used z-test to compare the log-HRs between individuals with and without neuroinflammation-related conditions in a quasi-difference-in-difference setting. For a HR < 1 (or >1) in individuals with neuroinflammation-related conditions, the null hypothesis was that the HR was lower (or higher) in individuals with neuroinflammation-related conditions compared to without. We used 0.05 as the threshold for one-sided p-value. We selected drugs that had: (1) FDR < 0.05 for testing HR = 1 in metanalysis of neuroinflammation-related cohorts; and (2) p-value <0.05 for comparing HRs between individuals with and without neuroinflammation-related conditions. All analyses were conducted in R.
Results
We derived eight cohorts. The four neuroinflammation-related cohorts included 175,915 patients with alcohol use disorder (AUD), 67,825 patients with epilepsy, 81,510 patients with hemorrhagic stroke (HS), and 104,637 patients with traumatic brain injury (TBI). The four matched cohorts included the same numbers of individuals as the corresponding neuroinflammation-related cohorts. The demographics of the cohorts were presented in Table 1. In the rest sections, false discovery rate (FDR) was adjusted for multiple comparisons, and all p-values were not adjusted for multiple comparisons.
Demographics of the analytical datasets.
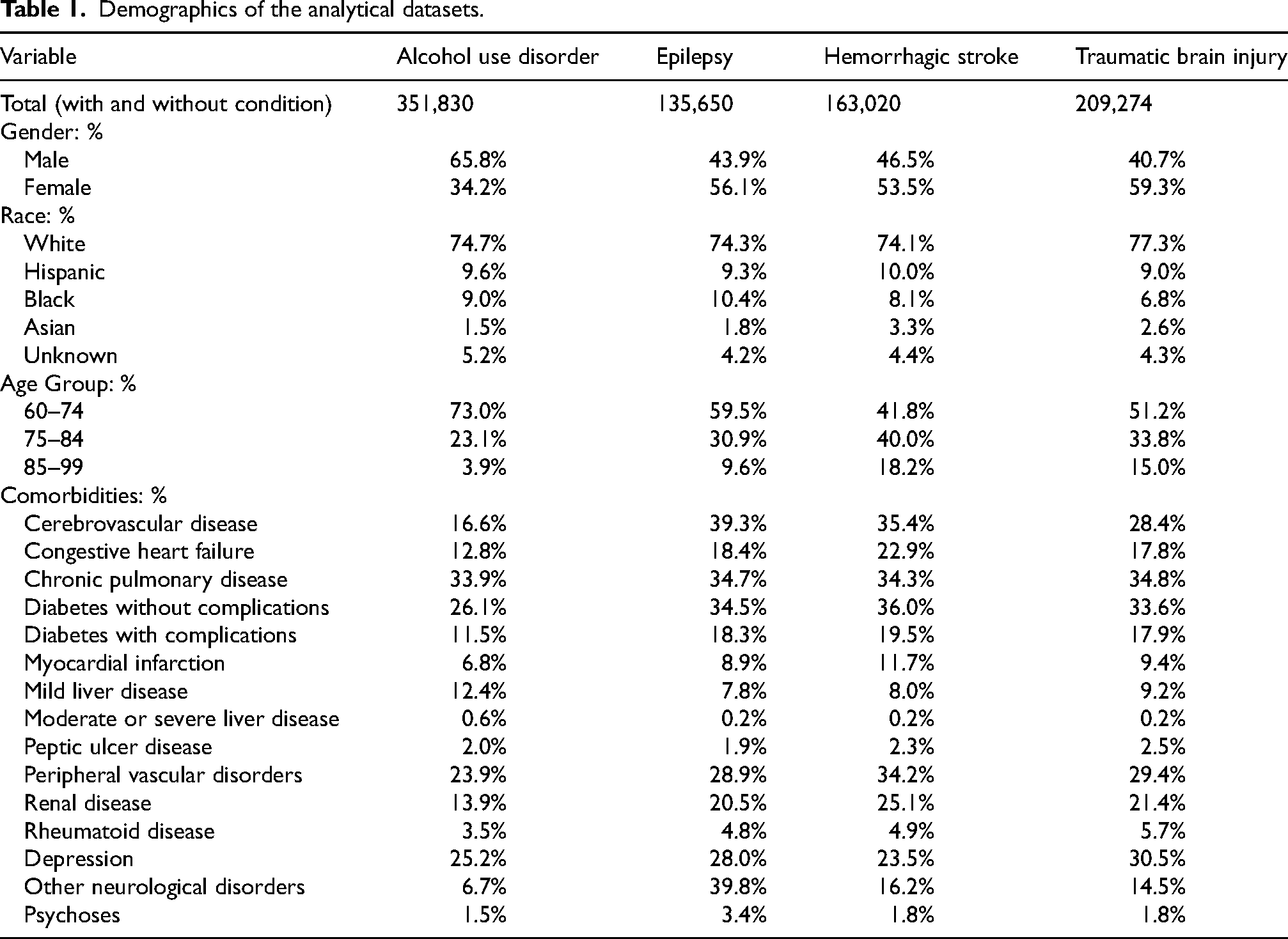
Figure 2 shown the hazard ratios (HRs) of all tested drugs on AD in individuals with and without neuroinflammation-related conditions. We identified 5 drugs (levothyroxine, mirabegron, ropinirole, levetiracetam and quetiapine) were associated with AD (FDR < 0.05) in patients with neuroinflammation-related conditions and had differential HRs between individuals with and without neuroinflammation-related conditions (p < 0.05). For these 5 drugs, Figure 3 shows their HRs in individual cohorts and meta-analyses.
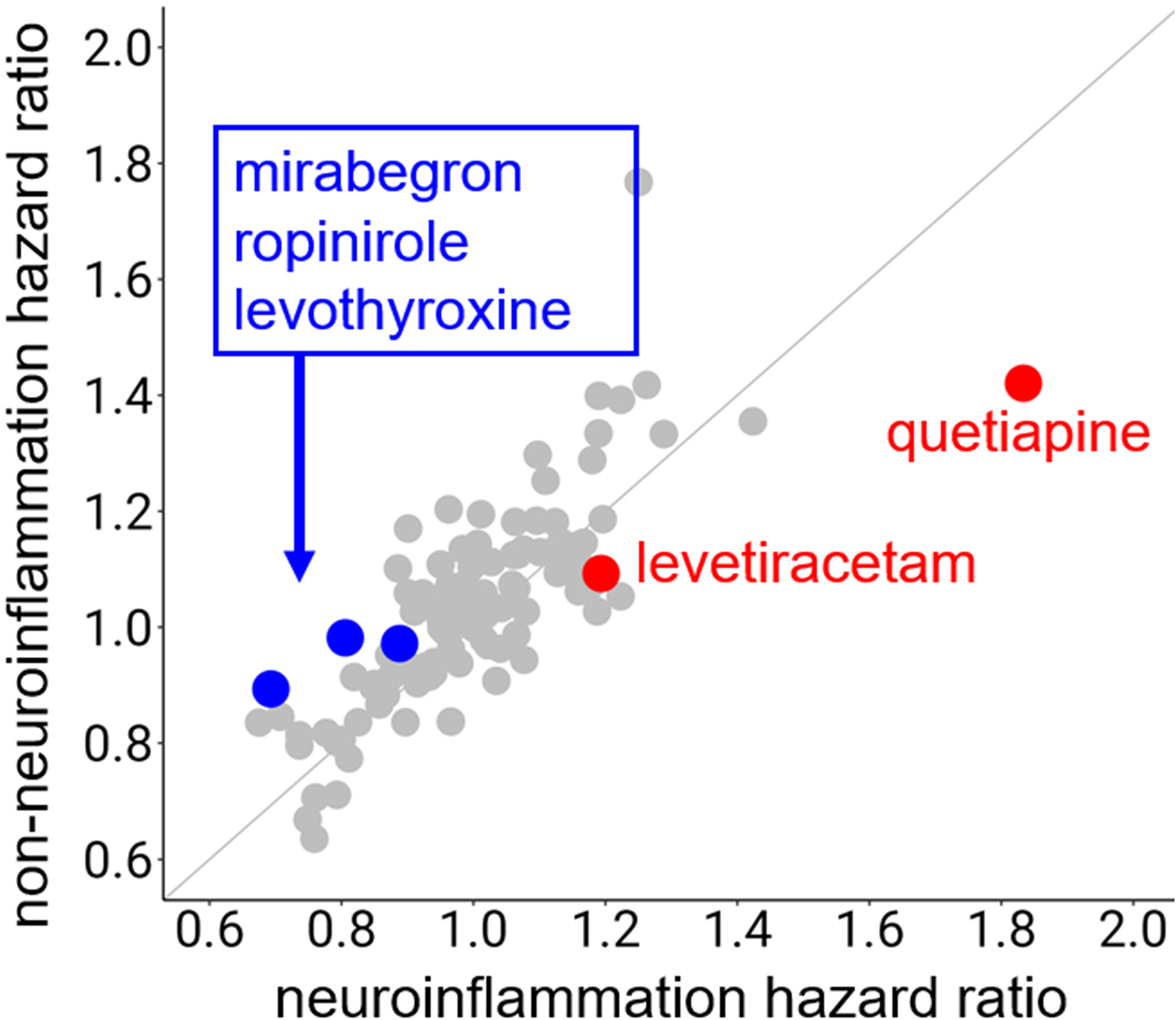
Associations between tested drugs and Alzheimer's disease in individuals with and without neuroinflammation-related conditions.
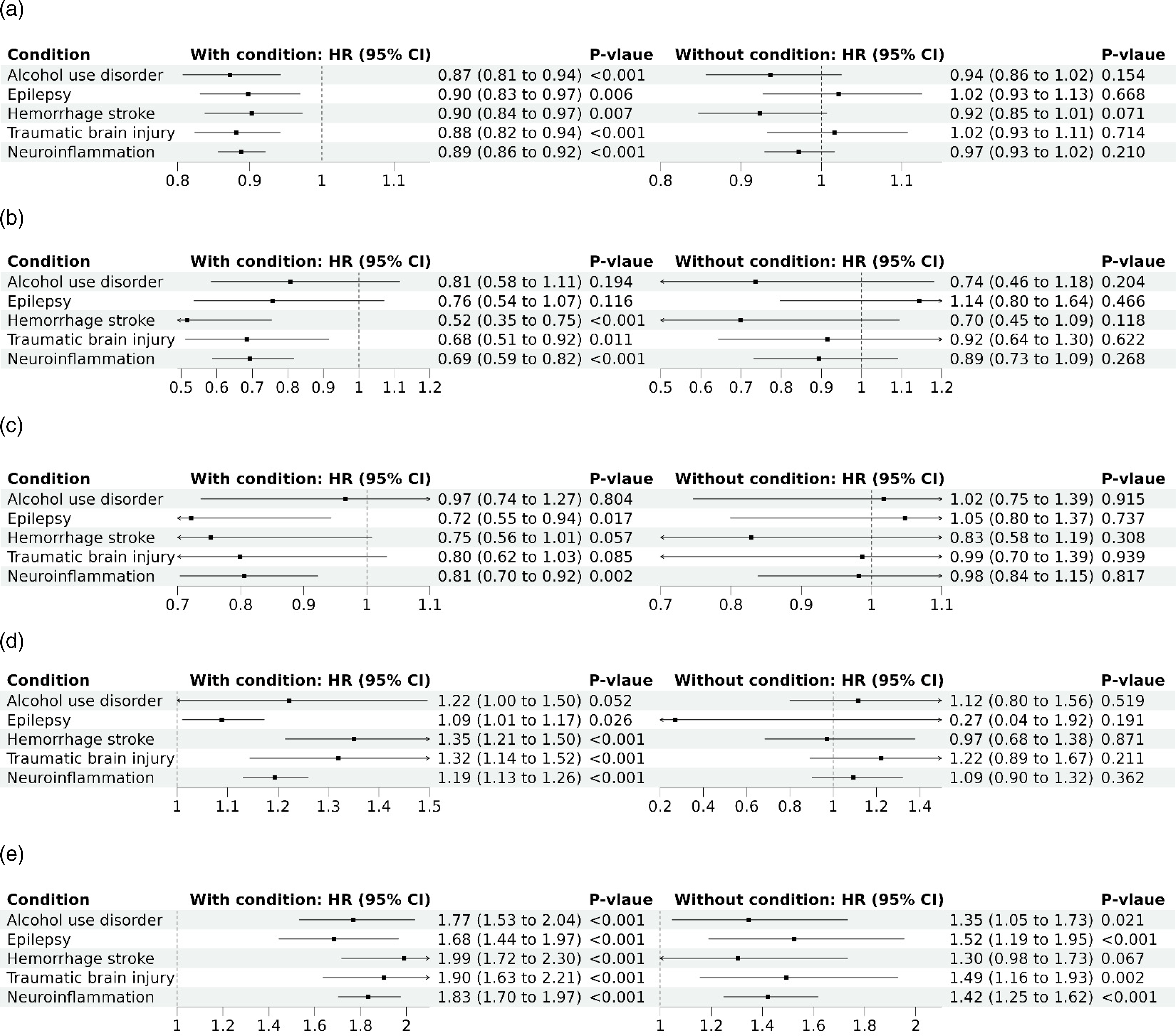
Associations with Alzheimer's disease. (a) Levothyroxine; (b) Mirabegron; (c) Ropinirole; (d) Levetiracetam; (e) Quetiapine.
Levothyroxine exposure was associated with a decreased risk of AD in all neuroinflammation-related cohorts and the all individuals with neuroinflammation-related conditions (Figure 3(a); hazard ratios [HRs] ≤ 0.90 and p < 0.01). Mirabegron exposure was associated with a decreased risk of AD in HS cohort, TBI cohort, and all patients with neuroinflammation-related conditions (Figure 3(b); HRs ≤ 0.69 and p ≤ 0.01). Ropinirole exposure was associated with a decreased risk of AD in epilepsy cohort and all patients with neuroinflammation-related conditions (Figure 3(c); HRs ≤ 0.81 and p ≤ 0.02). All of levothyroxine exposure, mirabegron exposure, and ropinirole exposure were not associated with AD in individuals without neuroinflammation-related conditions (Figure 3(a)–(c)).
Levetiracetam exposure was associated with an increased risk of AD in patients with neuroinflammation-related conditions (Figure 3(d); HR = 1.19 and p < 0.01); but was not associated with AD in individuals without neuroinflammation-related conditions (Figure 3(d)). Quetiapine exposure was associated with an increased risk of AD in most cohorts (Figure 3(e)), and the pooled HR was higher in patients with neuroinflammation-related conditions compared to without (HR = 1.83 versus HR = 1.42 [p < 0.01 for comparing 1.83 to 1.42]; Figure 3(e)).
Discussion
Our real-world data-based study identifies drugs that might have a potential beneficial effect (levothyroxine, mirabegron and ropinirole) and a potential adverse effect (levetiracetam and quetiapine) in AD in patients with neuroinflammation-related conditions such as AUD, epilepsy, HS, and TBI.
Levothyroxine (a drug for hypothyroidism) is associated with a decreased risk of AD in patients with neuroinflammation-related conditions but have a neutral association with AD in matched individuals without the corresponding conditions (Figure 3(a)). Levothyroxine demonstrates potential anti-inflammatory effect in clinical studies and AD mouse models.26,27 Hypothyroidism can be treated by levothyroxine. Additionally hypothyroidism is related to the development of AD and AUD,28,29 and the progression of HS and TBI.30,31 However, drug responses of levothyroxine in AD in patients with neuroinflammation-related conditions are largely unknown. We find consistent results between levothyroxine and AD in all neuroinflammation-related cohorts and all non-neuroinflammation-related cohorts (Figure 3(a)), which suggesting a potential beneficial drug-host (i.e., levothyroxine-neuroinflammation) interaction effect in AD.
Mirabegron (a drug for overactive bladder) exposure is associated with a decreased risk of AD in HS and TBI cohorts, and all individuals with neuroinflammation-related conditions (Figure 3(b)). Mirabegron is not associated with cognitive function in a randomized clinical trial with wet overactive bladder patients. 32 However, mirabegron has potential neuroprotective effect, 33 especially for patients with stroke. 34 Ropinirole (a drug for Parkinson's disease and restless legs syndrome) exposure is associated with a decreased risk of AD in epilepsy cohort and all individuals with neuroinflammation-related conditions (Figure 3(c)). Ropinirole has been identified as a candidate repurposable drug for AD,35,36 while its relationship with epilepsy remains unclear. In our analyses, mirabegron and ropinirole are significantly associated with a reduced risk of AD only in certain neuroinflammation-related cohorts, and all individuals with neuroinflammation-related conditions. Thus, further studies are warranted to validate and/or explain the mechanism of our findings.
Levetiracetam exposure is associated with an increased risk of AD in in patients with neuroinflammation-related conditions but is not associated with AD in individuals without neuroinflammation-related conditions (Figure 3(d)). Levetiracetam could be used to treat seizures related to AUD, epilepsy, HS and/or TBI. In our study, levetiracetam exposure has HR = 1.09 (p = 0.03) in patients with epilepsy. The relationship between levetiracetam and cognitive health remains inconclusive. In a phase 2 randomized clinical trial, levetiracetam is not associated with cognition change in all participants, but improves performance on spatial memory and executive function tasks in patients with AD and epileptiform activity. 37 Other studies suggest levetiracetam might adversely affect cognition.38,39 Quetiapine exposure was associated with an increased risk of AD in most cohorts with higher pooled HR in individuals with neuroinflammation-related conditions compared to without (Figure 3(e)). Quetiapine is considered to have a strong anticholinergic cognitive burden scale, 40 but might be used to manage neuropsychiatric symptoms due to AD. 41 Our results suggest more considerations on levetiracetam and quetiapine shall be given to patients with neuroinflammation-related conditions. However, as levetiracetam and quetiapine are related to risk factors of AD, despite covariate-adjustment, we cannot rule out the potential of confounding by indication. Specifically, levetiracetam exposure in individuals with AUD, HS and TBI indicate the presence of seizure, which reflects a higher severity of the diseases. As higher severity of these diseases could increase the risk of AD,42,43 the association between levetiracetam and AD could be confounded by the severity of AUD, HS and TBI. Likewise, the association between levetiracetam and AD in patients with epilepsy could also be confounded by the severity of epilepsy. We find quetiapine is associated with an increased risk of AD in both patients with neuroinflammation-related conditions and individuals without neuroinflammation-related conditions. As quetiapine can be used to manage neuropsychiatric symptoms related to AD, 44 the association between quetiapine and AD could be confounded by neuropsychiatric symptoms related to prodromal/undiagnosed AD. For ropinirole, the drug can be used to treat Parkinson's disease, and patients with Parkinson's disease may have a lower risk of AD. 45 Thus, the association between ropinirole and AD could be confounded by Parkinson's disease. Again, further studies are warranted to validate and/or explain the mechanism of our findings.
Our study also has additional limitations. First, our analytical datasets are derived from individuals with commercial and/or Medicare supplemental health insurance plans. Our findings cannot be generalized to individuals without the corresponding health insurance plans. Second, we used specific algorithms to define phenotypes including neuroinflammation-related conditions (AUD, epilepsy, HS, and TBI), AD, and comorbidities. Despite the algorithms are derived by subject matter experts, the phenotypes could be misclassified. Additionally, patients with the aforementioned neuroinflammation-related conditions may have heterogeneous severity of neuroinflammation both within and between the neuroinflammation-related conditions. For instance, patients with TBI may range from mild to severe TBI, and patients with AUD may range from recovery (i.e., in remission) to alcoholism, both of which may left heterogeneous severity of neuroinflammation. We assume patients with neuroinflammation-related conditions have a higher severity of neuroinflammation than the matched individuals in general. However, the presence of neuroinflammation could be misclassified, and the severity of neuroinflammation is not adjusted. Third, we use pharmacy claims data to define drug exposure, while we cannot confirm drug adherence and/or cumulative exposure. We largely assume pharmacy claims data are consistent to drug exposure in the overall population, but this assumption may not be hold for all study individuals. Fourth, our findings are subject to unmeasured confounding. The potential confounders include genetic risk factors, social determinants of health, cognitive status. Fifth, our findings are subject to potential model violations such as the proportional hazard assumption in Cox model, while the associations are consistent between covariate-stratified log-rank tests and Cox models (Supplemental Table 1). Despite these limitations, we believe our findings deserve further investigations, especially for the differential drug responses in AD in a quasi-difference-in-difference setting.
We identified drugs that might have a potential beneficial effect (levothyroxine, mirabegron and ropinirole) and a potential adverse effect (levetiracetam and quetiapine) in AD in patients with neuroinflammation-related conditions.
Supplemental Material
sj-docx-1-alz-10.1177_13872877251376291 - Supplemental material for Real-world observations on neuroinflammation-related drug responses in Alzheimer's disease
Supplemental material, sj-docx-1-alz-10.1177_13872877251376291 for Real-world observations on neuroinflammation-related drug responses in Alzheimer's disease by Jing Xu, Anna Sun, Yuedi Yang, Yi Shi, Dongbing Lai, Jing Su, Lang Li, Donglin Zeng, Andrew J Saykin, Feixiong Cheng, Yunlong Liu and Pengyue Zhang in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
The authors have no acknowledgments to report.
Ethical considerations
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the NIH (R01LM013771, R01AG092591, 3R01DA053722-03S1 and 01U10AA008401).
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Saykin receives support from multiple NIH grants (P30 AG010133, P30 AG072976, R01 AG019771, R01 AG057739, U19 AG024904, R01 LM013463, R01 AG068193, R01 AG092591, T32 AG071444, U01 AG068057, U01 AG072177, U19 AG074879, as well as U24 AG074855). Dr Saykin has also received in-kind support from Avid Radiopharmaceuticals, a subsidiary of Eli Lilly (PET tracer precursor) and Gates Ventures, LLC and Sanofi (Proteomics panel assays on IADRC and KBASE participants as part of the Global Neurodegeneration Proteomics Consortium), and has participated in Scientific Advisory Boards (Bayer Oncology, Eisai, Novo Nordisk, and Siemens Medical Solutions USA, Inc) and an Observational Study Monitoring Board (MESA, NIH NHLBI), as well as External Advisory Committees for multiple NIA grants. He also serves as Editor-in-Chief of Brain Imaging and Behavior, a Springer-Nature Journal. The remaining authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Optum's de-identified Clinformatics® Data Mart Database is available from Optum, Inc. Summary statistics generated in this study are available in tables, figures and supplemental material.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.