
Abstract
Background
Preclinical studies suggest β2-adrenergic receptor agonists may exert neuroprotective effects, but evidence in human populations is limited.
Objective
To examine the association between β2-adrenergic receptor agonist use and cognitive performance in older adults.
Methods
This retrospective cohort study linked Dutch pharmacy dispensing records (IADB.nl) with Lifelines cohort data. Participants aged ≥50 years with ≥1 prescription for β2-adrenergic receptor agonists or reference medications (COPD/cardiovascular) within 365 days prior to baseline cognitive testing were included. Cognitive function was assessed using the Cogstate Brief Battery. Linear mixed models adjusted for demographic, clinical, and lifestyle factors evaluated longitudinal changes.
Results
A total of 3179 participants were included (249 β2-adrenergic receptor agonist users, 2930 reference). The exposed group was younger (mean age 58.6 ± 7.4 years versus 63.7 ± 9 years) and included a higher proportion of females (68.2% versus 58.6%) compared with the referent group. At baseline, groups were similar in most cognitive domains, except for slightly higher attention (COG2) scores in the reference group (p = 0.010). Over time, psychomotor speed (COG1), attention (COG2), and visual learning (COG4) remained stable across groups. Working memory (COG3) declined significantly in both groups, with a steeper decline in the reference cohort (p = 0.048).
Conclusions
In this exploratory cohort study, β2-adrenergic receptor agonist use was not associated with broad cognitive benefits, though a modest attenuation of working memory decline was observed. These results highlight the need for larger, prospective studies to clarify whether specific subgroups or drug formulations may offer cognitive advantages.
Introduction
Dementia is a progressive neurodegenerative disorder characterized by a decline in cognitive abilities, including memory loss, impaired judgment, and behavioral disturbances.1,2 A diagnosis of dementia requires evidence of decline in at least two cognitive domains—such as memory, executive function, language, visuospatial abilities, or attention—that significantly interfere with daily activities.3,4 Dementia includes various etiologies, such as Alzheimer's disease (AD), vascular dementia, Lewy body dementia, and frontotemporal dementia, with AD being the most prevalent. 5 Globally, dementia's prevalence is rising due to aging populations, with an estimated 55 million affected in 2020, a number projected to reach 139 million by 2050. 6
In the Netherlands, around 290,000 individuals live with dementia, with the number expected to rise to 420,000 by 2030. 1 The personal, societal, and healthcare impact of dementia is substantial, with healthcare costs projected to increase from €6.6 billion in 2015 to €15.6 billion by 2040.1,7 Despite advances in understanding dementia's pathophysiology, effective disease-modifying treatments remain limited, underscoring the need for novel therapeutic strategies, including repurposing existing pharmacological agents. AD as the most common entity of dementia is pathophysiologically characterized by amyloid-β (Aβ) plaques and tau neurofibrillary tangles, leading to neuronal apoptosis and cholinergic dysfunction.8,9 Current treatments, such as cholinesterase inhibitors, offer limited symptomatic relief, but do not slow disease progression. 10 As a result, alternative therapeutic targets are being explored, including the role of β2-adrenergic receptors.
β2-adrenergic receptors are implicated in regulating neuroinflammation, cerebral blood flow, and synaptic plasticity—all of which are essential in the pathophysiology of dementia and AD. Dysregulation of β-adrenergic signaling has been linked to both neuroprotective and neurodegenerative effects, highlighting the complex role of β2-adrenergic receptors in cognitive decline. 11 Preclinical studies suggest that β2-adrenergic receptor agonists may exert neuroprotective effects by reducing neuroinflammation, enhancing vascular perfusion, and improving blood-brain barrier integrity.12–14
Additionally, β2-adrenergic receptor stimulation has been shown to promote hippocampal synaptic plasticity and memory consolidation, essential processes for learning and memory.15,16 Conversely, β2-adrenergic receptor antagonists show mixed effects in both preclinical and clinical settings.11,17–19 Some clinical studies indicate detrimental impacts on memory encoding or cognitive function, particularly with certain β-blockers, while others suggest protective roles through the modulation of cerebral blood flow and stress-related vascular effects.20,21 These conflicting findings highlight the complex relationship between β-adrenergic signaling and cognitive outcomes.
Despite promising preclinical evidence, clinical and epidemiological evidence regarding the cognitive and neuroprotective benefits of β2-adrenergic receptor agonists remains limited. Multiple epidemiological studies have demonstrated that β2-adrenergic receptor agonist use is associated with reduced dementia and AD risk in older populations.18,19 Centrally-acting β2-adrenergic receptor agonists like clenbuterol have demonstrated cognitive benefits in a recent Phase I study by penetrating the blood-brain barrier and increases cerebral perfusion in patients with mild cognitive impairment. 22 Critically, few studies have directly investigated domain-specific cognitive trajectories or cognitive outcomes in relation to β2-adrenergic receptor agonist exposure in respiratory disease populations, particularly in longitudinal cohort studies with validated cognitive testing.23–25 This represents a significant gap between the preclinical neuroprotective evidence and real-world clinical efficacy in cognitively at-risk populations.
Therefore, the present study aimed to investigate the association between selective β2-adrenergic receptor agonist use and cognitive trajectories in older adults using unique linkage of pharmacy dispensing data with population-based cohort information. By translating preclinical neuroprotective findings into a real-world observational setting, we sought to determine whether β2-adrenergic receptor agonists are associated with improved global or domain-specific cognitive performance. We hypothesized that β2-adrenergic receptor agonist users would demonstrate attenuated decline in cognitive function over time compared with individuals using chronic obstructive pulmonary disease (COPD) or cardiovascular reference medications.
Methods
Study design and setting
This retrospective cohort study utilized data from the IADB.nl pharmacy database and the Lifelines cohort database, with data collection extending up to 2023.
The longitudinal Dutch IADB.nl prescription database contains prescription records dating back to 1994 and undergoes continuous growth and updates over time. The database encompasses pharmaceutical dispensing records attained from approximately 125 community pharmacies in the northern region of the Netherlands. With an estimated population of 1.3 million patients, the source population is representative of the Dutch population, as inclusion in the database is independent of healthcare insurance status, age, or gender, ensuring representativeness across demographics. Each registered patient is assigned a distinct anonymous personal identifier code, enabling individual tracking throughout the database duration and facilitating the linkage of multiple prescriptions. Additionally, the patients’ gender and date of birth are recorded. Prescription records include details on the dispensing date, dosage regimen, dispensed quantity, prescription validity duration, prescribing physician's identity, and the Anatomical Therapeutic Chemical (ATC) code. 26 Due to the high commitment of patients to their pharmacy, most patients register with a single community pharmacy, resulting in comprehensive prescription records for the majority of individuals.
Lifelines is a multi-disciplinary prospective population-based cohort study examining in a unique three-generation design the health and health-related behaviors of 167,729 persons living in the North of the Netherlands. It employs a broad range of investigative procedures in assessing the biomedical, socio-demographic, behavioral, physical and psychological factors which contribute to the health and disease of the general population, with a special focus on multi-morbidity and complex genetics. Each participant is provided with a unique anonymized identifier, and the two databases can be linked to combine medication dispensing records (IADB.nl) with a wide range of patient characteristics (Lifelines). Notable patient characteristics in the Lifelines database include demographics (e.g., sex, education), diseases and symptoms (e.g., diabetes, depression, hypertension), lifestyle and environmental factors (e.g., alcohol use, home environment, physical activity), and subjective health (e.g., social functioning). Importantly, the Lifelines database also contains cognitive assessments, including the Cogstate Brief Battery (CBB) (Figure 1).
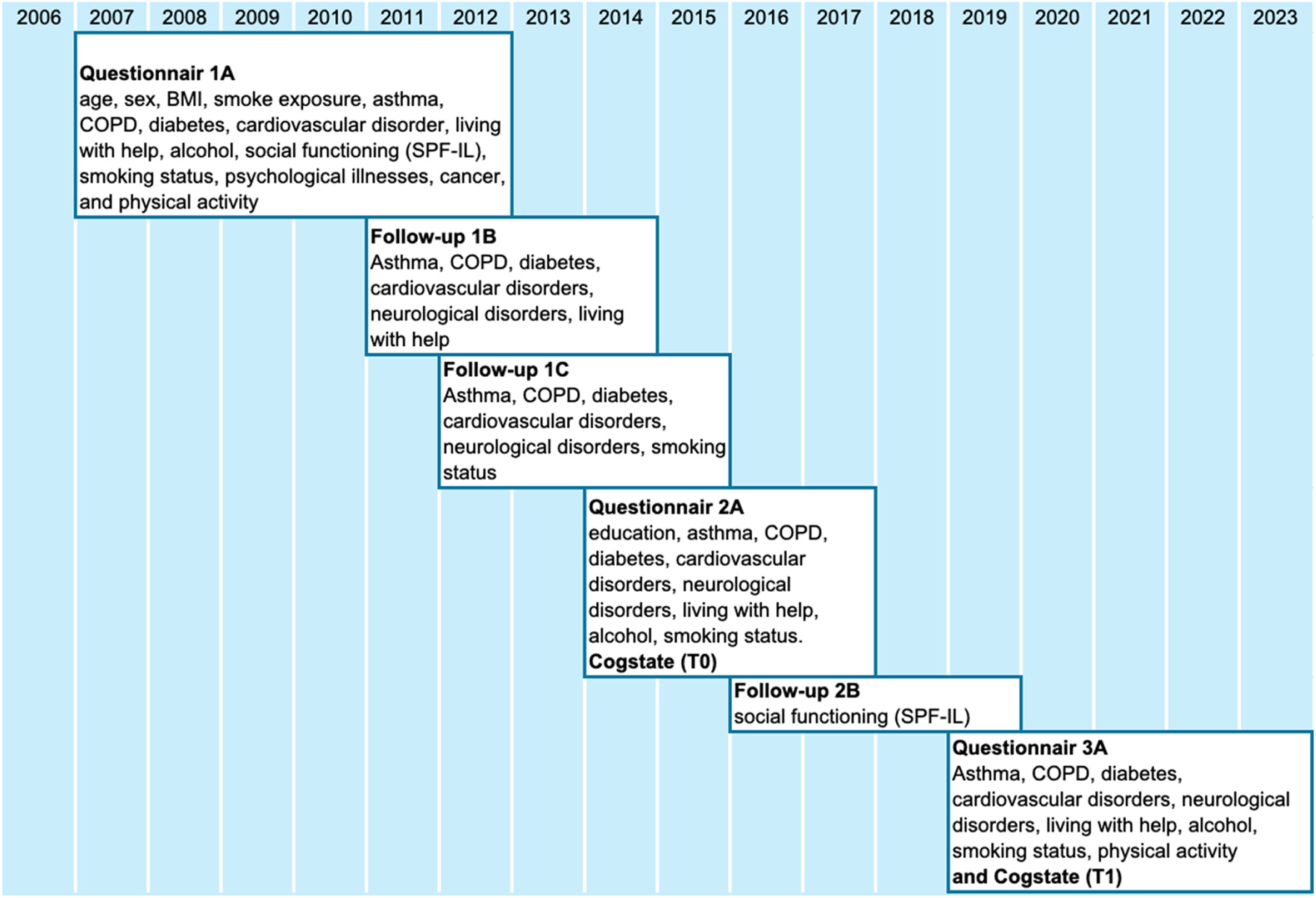
Data collection process and timeline of cognitive assessments.
Eligible participants
Study participants were defined as individuals exposed to any of the exposure (β2-adrenergic receptor agonists) or referent medications (medications for obstructive airway disease or medications for the cardiovascular system) (see section “Exposure”). Data was retrieved from the IADB.nl database for all participants with at least one prescription for one of these medications and this data was linked with that of the Lifelines database, with linkage facilitated via the Central Bureau of Statistics (CBS). The index date was defined as the date of the first available CBB during the 2A assessment (Figure 1). Notably, the index date was not the same date for all patients.
Inclusion and exclusion criteria
Individuals were included if they were present in both the IADB.nl and Lifelines databases for at least 365 days prior to and at least 365 days after their index date. Participants were required to be 50 years of age or older at the index date, with at least one prescription for either the exposure or reference medications within 365 days prior to their index date. Participants were required to be assigned to no more than one cohort. While the exposure window captures recent medication use, the study design allowed for assessment of longitudinal change over multiple years following baseline cognitive assessment. This approach captures the cumulative effects of sustained medication use rather than acute effects. Participants were required to have continuous pharmacy records for at least 365 days before and after the index date, ensuring that medication exposure reflects ongoing therapeutic use. The index date occurred between 2014–2017, with follow-up assessments in 2019, providing 2–5 years of longitudinal follow-up for cognitive trajectories.
Exposure definition
The exposure group was defined: B2-agonist (selective β2-adrenergic receptor agonists). Two reference groups in total were defined: 1) COPD (medications for obstructive airways diseases) not b-agonists, and 2) Cardio (medications for the cardiovascular system). Exposure was defined as at least one prescription for the relevant medication within 365 days prior to the index date (Table 1). Patients exposed to β2-adrenergic receptor antagonists or adrenergic medications (other than exposed ones) are excluded from the study.
Exposure and reference medications classified by Anatomical Therapeutic Chemical (ATC) codes.
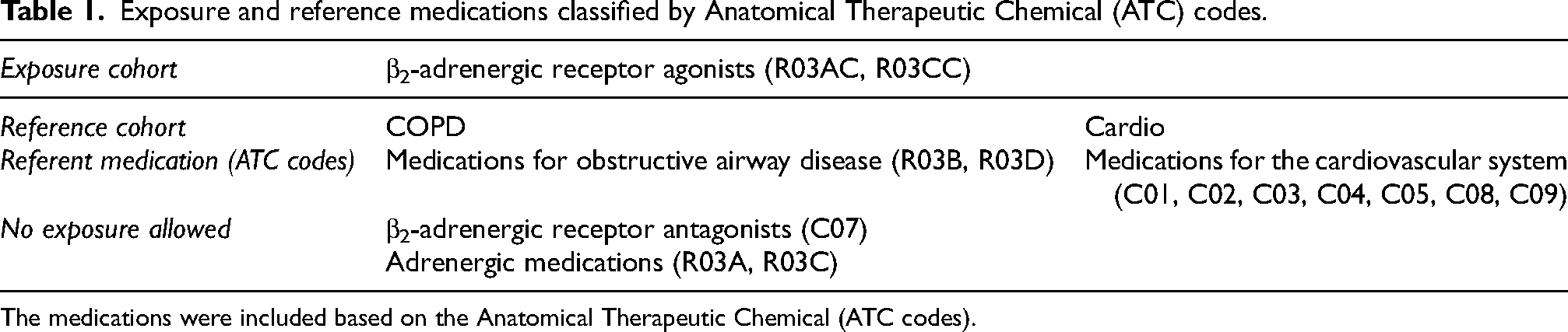
The medications were included based on the Anatomical Therapeutic Chemical (ATC codes).
Outcome measures
During the 2A and 3A Lifelines assessments (Figure 1), patients were invited to participate in the CBB examination. The CBB consists of computerized tasks (detection, identification, One Back, and One Card Learning), developed to measure various domains of cognition, including psychomotor functioning, speed of processing, attention, and working and visual memory. Although no gold standard currently exists in cognitive function testing, the Cogstate method has been validated in international peer-reviewed journals and has a reported sensitivity and specificity of 78 and 90%, respectively. 27 The cognitive outcomes were evaluated using four Cogstate tasks (Cogstate 1–4). Cogstate 1 (Detection task) and Cogstate 2 (Identification task) measured participants’ reaction time in milliseconds. These values were normalized using a log10 transformation, where faster reaction times indicated improved cognitive attention, psychomotor speed, and processing efficiency. In contrast, Cogstate 3 (One Card Learning task) and Cogstate 4 (One Back task) assessed the proportion of correct responses. These scores were normalized using the arcsine root transformation, with higher proportions of correct answers reflecting enhanced visual learning and working memory.
Covariates
Baseline characteristics were summarized to explore group differences and to inform the identification of potential confounders in the association between β2-adrenergic receptor agonist use and cognitive outcomes. Covariates were selected based on expert recommendations and the 2024 Livingston report on dementia risk factors. 5 Data on these covariates were obtained from the linked IADB.nl prescription database and the Lifelines cohort, with all baseline measurements derived from the Lifelines 2A assessment.
A total of 17 covariates were examined, covering a broad spectrum of demographic, clinical, and lifestyle domains. These included age, sex, body mass index (BMI), educational attainment, smoking status, exposure to second-hand smoke, and the presence of chronic conditions such as asthma, COPD, diabetes, cardiovascular diseases, and psychological disorders. Measures of social functioning and living situation were also assessed to capture broader contextual influences on cognitive health.
Histograms, boxplots, violin plots, and qq-plots were used to assess whether the various Cogstate scores fulfilled the normality assumption. For quantifying the association between the covariates and the outcome non-parametric Kruskal-Wallis tests were employed together with post hoc tests for pairwise comparisons where appropriate, while for assessing the association between the covariates and the exposure non-parametric Chi-squared tests were used.
Sensitivity analysis
Sensitivity analyses were performed to assess the robustness of the primary findings and to explore the potential impact of confounding by indication and exposure misclassification. First, analyses were repeated within restricted subsets of the non-exposed/reference cohort, separately including only participants receiving cardiovascular medications and only participants receiving COPD medications, thereby reducing heterogeneity related to comorbidity profiles. Second, to evaluate the influence of treatment continuity, the exposed cohort was restricted to individuals who remained exposed to β2-adrenergic receptor agonists for at least one year before the end of follow-up. In the primary analyses, participants initially classified as non-exposed who initiated β2-adrenergic receptor agonist therapy during follow-up retained their original classification. To examine the potential bias introduced by this approach, an additional sensitivity analysis excluded these participants.
Statistical analysis
Descriptive analysis
Descriptive statistics were used to assess the relationship between the covariates and the exposure as well as the outcome. Histograms, boxplots, violin plots, and qq-plots were used to assess whether the various Cogstate scores fulfilled the normality assumption. For quantifying the association between the covariates and the outcome non-parametric Kruskal-Wallis tests were employed together with post hoc tests for pairwise comparisons where appropriate, while for assessing the association between the covariates and the exposure non-parametric Chi-squared tests were used.
Primary analysis
To model cognitive outcomes, linear mixed model (LMM) with independent random intercepts to control for individual heterogeneity was used, to assess relationships between the use of B2-adrenergic receptor agonists and cognitive outcomes (CBB). The model included categorical variables for exposure and time together with their interaction and the selected covariates for each outcome. The p-values after applying Holm's correction for multiple testing and 95% confidence intervals (CIs) were reported to estimate the direction and strength of associations. The estimated regression coefficients together with their associated p-values were reported for assessing the effect size and its significance. Missing values were listwise deleted throughout the analysis.
The statistical analysis was performed in R (version 4.5.1) 28 using libraries therein. In particular, LMMs were fitted using the function lme from the R package nlme 29 and pairwise contrasts together with the adjusted p-values were calculated using the function emmeans from the R package emmeans. 30 For visualizing the results, the ggplot function from the ggplot2 package was employed. 31
Results
Study population
The final analysis included 3179 participants, comprising 249 individuals in the β2-adrenergic receptor agonist group and 2930 individuals in the COPD (228) /cardiovascular (2702) reference group (Table 2). At baseline, participants in the β2-adrenergic receptor agonist group were significantly younger (mean 58.6 years, SD 7.4) compared with those in the COPD/cardiovascular group (mean 63.7 years, SD 9.0) with p < 0.001. Female participants were higher in the β2-adrenergic receptor agonist group (68.2%) compared to reference group (58.6%). This age difference was accounted for in the statistical models by including age at index date as a covariate. In addition to age, all models were adjusted for education, sex, and other demographic, clinical, and lifestyle variables that showed significant associations with cognitive outcomes at baseline, including hypertension, high cholesterol, heart failure, smoking, alcohol intake›, social activity, and asthma (Table 3).
The distribution of β2-adrenergic receptor agonists based on the number of prescriptions dispensed.
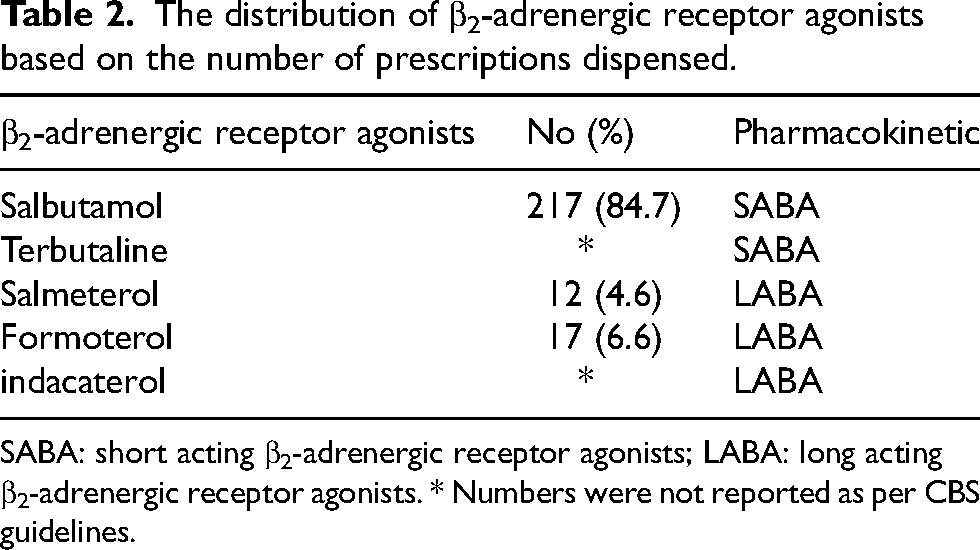
SABA: short acting β2-adrenergic receptor agonists; LABA: long acting β2-adrenergic receptor agonists. * Numbers were not reported as per CBS guidelines.
Baseline associations between demographic, clinical, and lifestyle covariates and cognitive test performance (COG1–COG4).
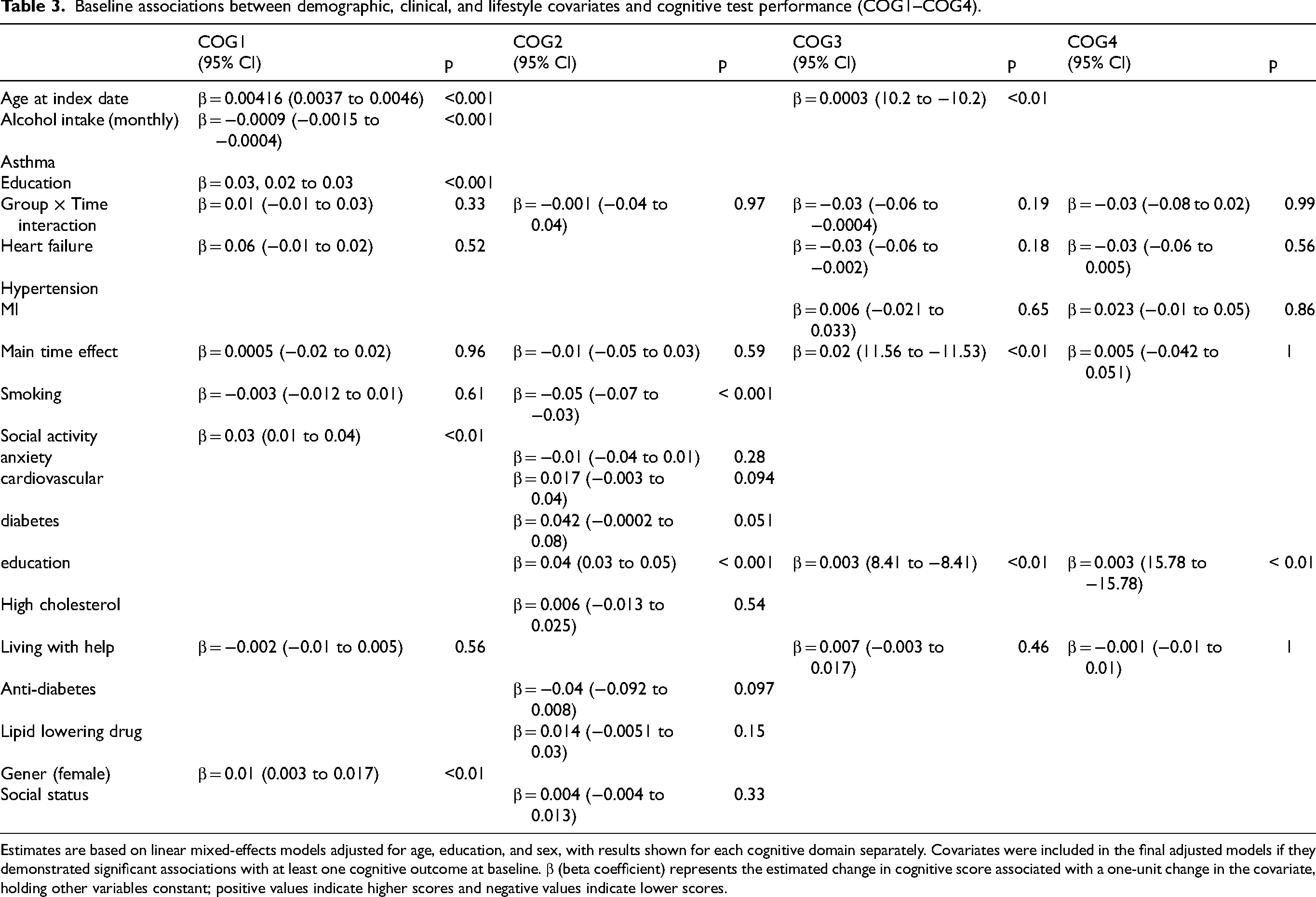
Estimates are based on linear mixed-effects models adjusted for age, education, and sex, with results shown for each cognitive domain separately. Covariates were included in the final adjusted models if they demonstrated significant associations with at least one cognitive outcome at baseline. β (beta coefficient) represents the estimated change in cognitive score associated with a one-unit change in the covariate, holding other variables constant; positive values indicate higher scores and negative values indicate lower scores.
The distribution of β2-adrenertic receptor agonists showed that most of the individuals included are using salbutamol with 217 prescriptions out of 256 followed by formoterol 17, salmeterol 12, and terbutaline and indacaterol <10 (Table 2).
Baseline cognitive performance
At baseline, adjusted differences in cognitive performance between exposed and non-exposed individuals were minimal and mostly non-significant across the cognitive domains. In COG1, no significant difference was observed between groups (β = –0.00193, 95% CI: −0.0152 to 0.0113, p = 0.78). Similarly, COG3 (β = 0.0125, 95% CI: −0.0083 to 0.0334, p = 0.48), COG4 (β = 0.0007, 95% CI: −0.0206 to 0.0220, p = 1) did not differ significantly between exposed and non-exposed groups. COG2 showed a statistically significant but modest difference (β = 0.0383, 95% CI: 0.0091 to 0.0674, p < 0.05), favoring the non-exposed group. These results suggest that baseline cognitive function was largely similar between groups after adjusting for confounders.
Visual inspection of the cognitive outcome plots further supports the statistical findings. At T0 (baseline), exposed and non-exposed groups had nearly identical mean scores across all domains. No visual group separation was evident in any figure, confirming that initial cognitive status did not substantially differ between groups.
Covariate effect
Several covariates showed significant associations with cognitive outcomes after adjustment. Older age was positively associated with COG1 (β = 0.00416, 95% CI: 0.0037 to 0.0046, p < 0.001) and COG3 (β = 0.0003, 95% CI: 10.2 to −10.2, p < 0.01), although the confidence interval for COG3 appears inconsistent.
Higher education was consistently associated with better cognitive scores across all domains. In COG1, education showed a strong positive effect (β = 0.03, 95% CI: 0.02 to 0.03, p < 0.001), and similar effects were found in COG3, COG4.
Alcohol intake was negatively associated with COG1 (β = –0.0009, 95% CI: −0.0015 to −0.0004, p < 0.001), while no significant associations were found in other domains. Social activity was positively associated with COG1 (β = 0.03, 95% CI: 0.01 to 0.04, p < 0.01), suggesting that higher social engagement supports better cognitive performance.
Smoking was significantly associated with lower COG2 scores (β = –0.05, 95% CI: −0.07 to −0.03, p < 0.001).
Heart failure showed weak, non-significant associations with COG3 (β = –0.03, 95% CI: −0.06 to −0.002, p = 0.18). Living with help was not associated with cognitive performance in COG1–COG4.
Female sex was associated with slightly higher COG1 scores (β = 0.01, 95% CI: 0.003 to 0.017, p < 0.01) but showed no consistent association in the other domains. Other covariates such as anxiety, cardiovascular disease, diabetes, and lipid-lowering agents did not show consistent significant effects, although diabetes was borderline significant in COG2 (β = 0.042, p = 0.051).
For the COG domains, interaction terms were non-significant, indicating parallel trajectories over time between exposed and non-exposed individuals. The main effect of time was significant only in COG3 (β = 0.02, 95% CI: 11.56 to −11.53, p < 0.01), but not in other domains.
Changes over time
These statistical findings were supported by the longitudinal trend figures (Figures 1–5). In COG1 (Figure 1), both exposure groups maintained nearly identical mean scores from T0 to T1, with no observable change over time. COG2 (Figure 2) and COG3 (Figure 3) showed similar patterns—mean cognitive scores remained flat, and the exposed and non-exposed trajectories were visually parallel. For COG4 (Figure 4), a stable pattern was also observed, with no change in slope or separation between groups across timepoints.
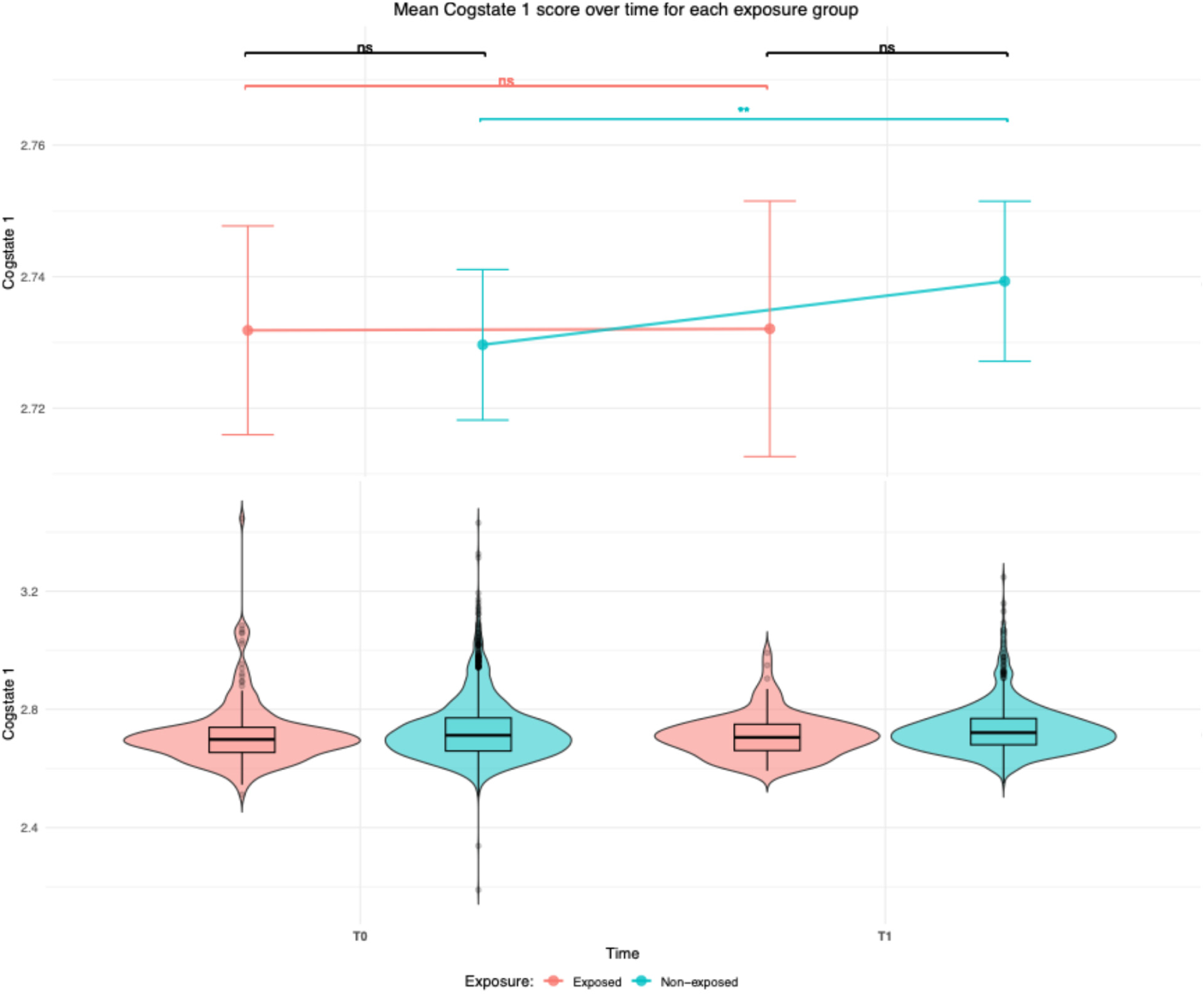
Mean psychomotor speed scores (COG1) at baseline (T0) and follow-up (T1) for the β2-adrenergic receptor agonist group (Exposed) and the COPD/cardiovascular group (non-exposed). ns: non-significant, *p < 0.05, **p < 0.01, ***p < 0.001.
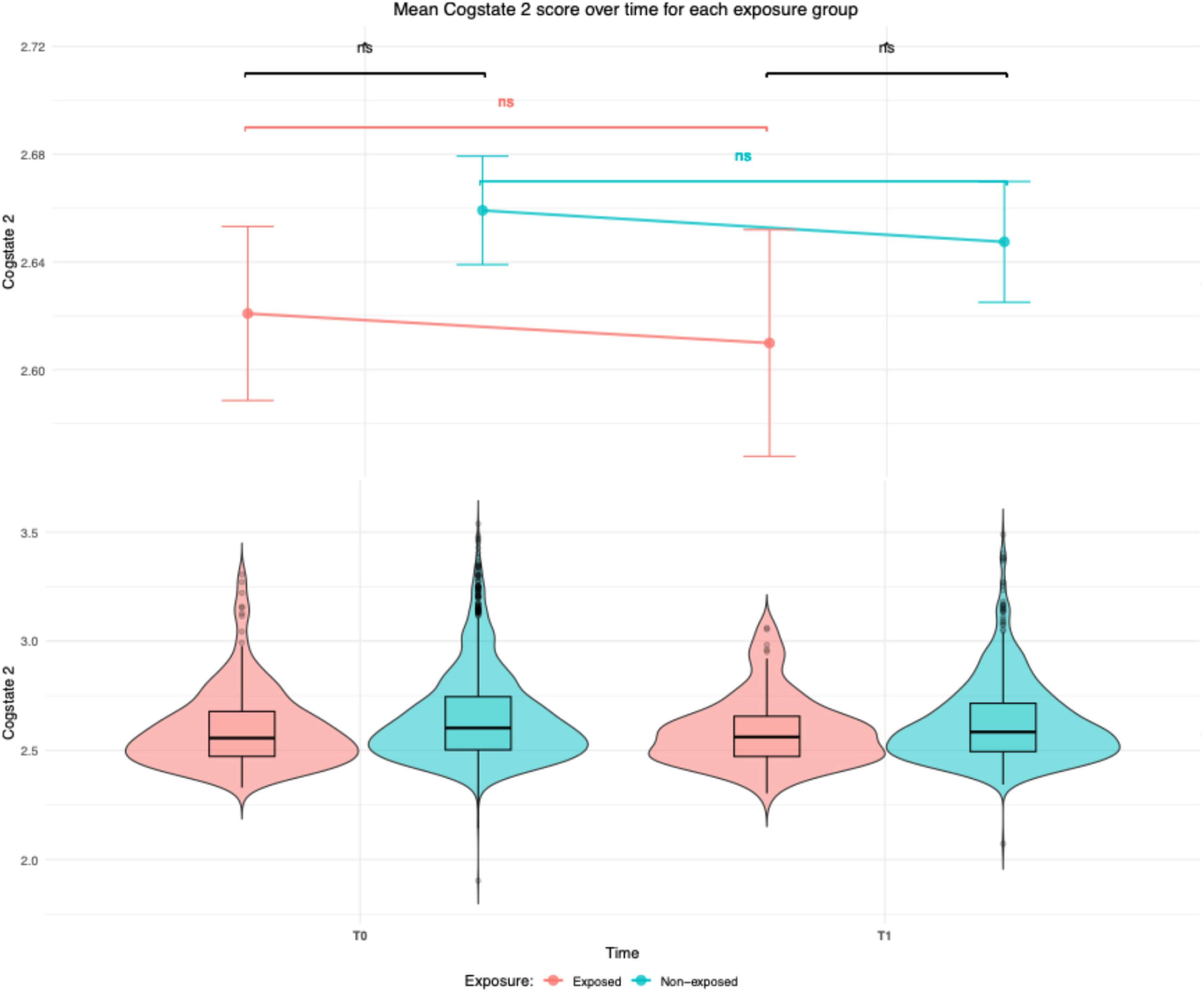
Mean attention scores (COG2) at baseline (T0) and follow-up (T1) for the β2- adrenergic receptor agonist group (Exposed) and the COPD/cardiovascular group (non-exposed). ns: non-significant, *p < 0.05, **p < 0.01, ***p < 0.001.
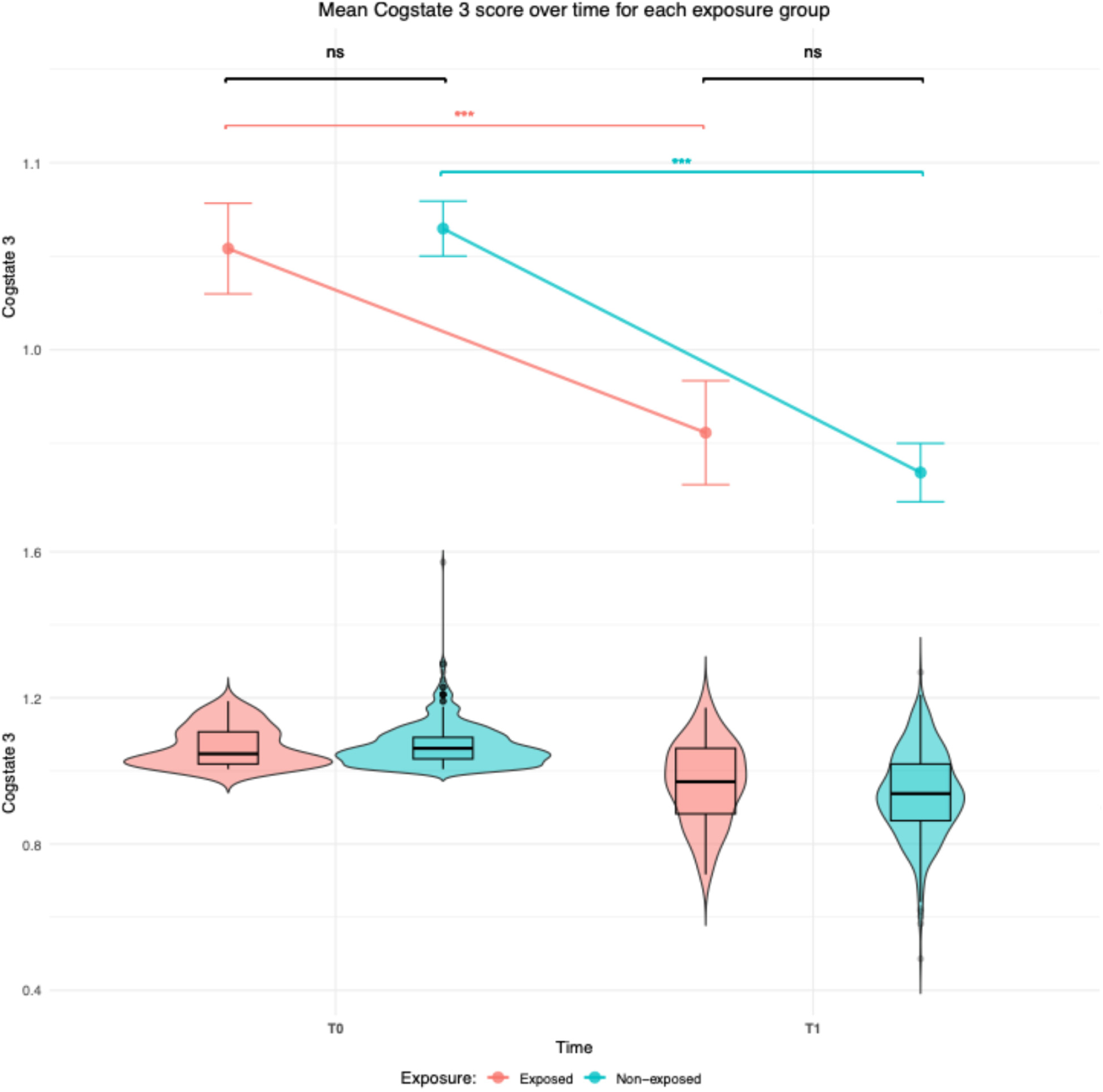
Mean working memory scores (COG3) at baseline (T0) and follow-up (T1) for the β2-adrenergic receptor agonist group (Exposed) and the COPD/cardiovascular group (Non-exposed). Ns: non-significant, *p < 0.05, **p < 0.01, ***p < 0.001.

Mean visual learning scores (COG4) at baseline (T0) and follow-up (T1) for the β2-adrenergic receptor agonist group (Exposed) and the COPD/cardiovascular group (Non-exposed). ns: non-significant, *p < 0.05, **p < 0.01, ***p < 0.001.
Sensitivity analysis showed similar outcome with few significant differences. In COG1 and COG4, cardiovascular group have statistically significant deterioration at T1 as compared to T0 while the exposed group showed stable non-significant cognitive outcome (Supplemental Figures 1–12).
Discussion
This retrospective cohort study investigated cognitive trajectories in adults aged ≥50 years exposed to β2-adrenergic receptor agonists (n = 249) compared to a COPD/cardiovascular medication reference group (n = 2930). At baseline, the β2-adrenergic receptor agonist cohort was significantly younger and more frequently female—characteristics consistent with demographic trends in asthma and COPD populations observed in European cohorts.32,33 As anticipated, the β2-adrenergic receptor agonist group exhibited higher prevalence of pulmonary conditions (e.g., asthma, COPD) and smoking history, while the reference group had a greater burden of cardiovascular comorbidities (e.g., hypertension, hypercholesterolemia), reflecting the medication profiles by indication. Baseline covariate analyses revealed that factors such as age, education, sex, hypertension, high cholesterol, heart failure, smoking, alcohol intake, social activity, and asthma significantly influenced at least one cognitive domain. These variables were retained in our models to reduce confounding, aligning with current recommendations for cognitive epidemiology.5,34
At baseline, cognitive performance in COG1 (psychomotor speed), COG3 (working memory), COG4 (visual learning), did not differ significantly between groups. The exception was COG2 (attention), where the reference group scored slightly higher—potentially reflecting disease- or treatment-related differences at baseline.
The decision to combine COPD and cardiovascular medication users into a single reference group warrants discussion. While both conditions are associated with cognitive risk, they differ in underlying mechanisms and medication profiles. Sensitivity analyses stratifying the reference group yielded similar findings with few differences. In COG1 and COG4, the cardiovascular referent group showed a significant decline at T1 compared to T0 suggesting worse psychomotor function and visual learning outcomes. While exposed group had steady yet not significant outcome. This suggests that BA users had better cognitive test outcomes as compared to referent group. The other results across all sensitivity analyses were consistent with the primary findings, indicating that the observed associations were not driven by differential medication use, comorbidity structure, or changes in exposure status over time. Nevertheless, future studies with larger β2-adrenergic receptor agonist cohorts should examine disease-specific reference groups separately.
Longitudinal analyses showed that COG1, COG2, and COG4 remained stable over time across both cohorts, evidenced by parallel trajectories. However, COG3 declined significantly in both groups, with a more pronounced decline in the reference cohort. This significant group-by-time interaction suggests that β2-adrenergic receptor agonist exposure may modestly attenuate working memory decline.
Although our findings did not provide strong evidence supporting the translation of preclinical neuroprotective effects of β2-adrenergic receptor agonism, such as reduction of neuroinflammation, improved cerebral perfusion, and enhanced synaptic plasticity, into clinically observable cognitive benefits in this population, attenuation of working memory decline was observed.12,35,36 The discrepancies between preclinical and observational epidemiological findings may reflect differences in experimental design, limited CNS bioavailability of systemic formulations, healthy user bias among individuals prescribed β2-adrenergic receptor agonists, and the relatively young age and short follow-up period of the cohort—insufficient to detect larger cognitive changes in a decades-long condition. These findings suggest that while preclinical evidence is biologically plausible, it may not translate to large cognitive preservation in all domains using current therapeutic formulations.
Most systemic β2-adrenergic receptor agonists have limited blood-brain barrier penetration and central nervous system bioavailability. 37 The pharmacokinetic characteristic may explain the observed absence of broad cognitive benefits. In contrast, preliminary evidence from phase I studies using centrally-acting β2-adrenergic receptor agonists (e.g., clenbuterol) has shown improvements in specific cognitive domains and our study confirmed some potential attenuation of working memory decline.19,38 Future research should investigate whether centrally-penetrating formulations or novel drug delivery systems might achieve more robust neuroprotective effects.
The elevated risk of cognitive impairment in COPD, documented in multiple studies, further contextualizes these findings. Cognitive impairment affects about 36% of individuals with COPD (versus ∼12% in the general population), and deficits are particularly pronounced in working memory, psychomotor speed, and executive function.39–41 The finding that the reference cohort (with greater cardiovascular burden) experienced steeper decline in working memory compared to β2-adrenergic receptor agonist users may align with COPD's known cognitive burden and suggest a slight protective effect, albeit small. In addition, it is well established that cardiovascular diseases, including coronary heart disease, heart failure, and atrial fibrillation, are independent risk factors for dementia. Large cohort studies and meta-analyses have demonstrated that individuals with cardiovascular disease have approximately 30–40% higher risk of developing dementia compared to those without.42–44 This may partly explain the observed steeper cognitive decline in the reference cohort, who carried a greater cardiovascular burden.
The instrumentation and CBB offered complementary sensitivity. The CBB has demonstrated robust sensitivity and specificity for mild impairments in attention and working memory. 27
An important consideration is whether the study population was optimally suited to address our research question. The average age at baseline was below 60 years, which is relatively young in the context of AD risk, as the likelihood of cognitive impairment increases sharply at older ages. Consequently, the follow-up period may not have been sufficient to capture the onset or progression of clinically relevant impairment. The Cogstate domains, baseline assessments (T0) occurred between 2014 and 2017, with follow-up from 2019 onwards, resulting in only about 2–5 years of follow-up. The relatively short Cogstate interval may be insufficient to observe domain-specific decline in a comparatively young population.
We observed attenuation of working memory decline, but not other cognitive effects possibly due to standard respiratory doses lack detectable broad cognitive benefits. Important caveats include: therapeutic doses are optimized for bronchodilation, not neuroprotection; most β2-adrenergic receptor agonists have poor blood-brain barrier penetration, whereas centrally-acting variants show promise; the study population was young without baseline cognitive impairment, whereas at-risk populations may benefit most; and β2-adrenergic receptor agonism may require combination with other neuroprotective interventions. These findings should thus guide future research toward optimized dosing, CNS-penetrating formulations, enriched patient populations, and combination approaches rather than curtail investigation into this target.
Strengths of this study include the use of robust linked prescription and cohort data from established Dutch databases, comprehensive covariate adjustment, and the application of linear mixed-effects models to assess within-person cognitive change. Limitations remain as a retrospective observational study, residual confounding and potential misclassification of medication exposure cannot be ruled out. The exclusion of individuals with overlapping exposures, while improving interpretability, reduced the β2-adrenergic receptor agonist sample size, which may have limited power to detect subtle cognitive effects.
A significant pharmacological consideration is the heterogeneity in CNS penetration across different β2-adrenergic receptor agonists molecules included in the exposure group. Salbutamol, the most frequently prescribed short-acting agent in this study (84.7%), exhibits limited blood-brain barrier penetration and may not achieve therapeutically relevant CNS concentrations. 45 In contrast, formoterol (6.6%) may be more likely to exert neuroprotective effects through central β2-adrenergic receptor stimulation. 46 The predominance of salbutamol within the pooled exposure group may therefore have affected detectable cognitive effects (Table 2).
To contextualize the impact of the relatively small β2-adrenergic receptor agonists sample, post hoc power analysis for independent samples t-tests indicated that the minimum detectable standardized effect size (Cohen's d) was 0.185, given our sample sizes and standard assumptions (power = 80%, α = 0.05). This corresponds to approximately 0.3 units in standardized CBB domains. Therefore, smaller differences in cognitive performance between exposure groups may have remained undetected, and findings should be interpreted with caution, particularly in the context of potential type II error. Because LMMs were used, which account for within-person variation and are more complex than t-tests, even subtler differences could have gone undetected, and findings should be interpreted with caution.
Conclusion
In conclusion, although β2-adrenergic receptor agonist use was not associated with significant changes in global cognitive function we observed attenuation of working memory decline in the reference group, but not so much in the β2-adrenergic receptor agonists group which deserves further study. Future prospective studies with longer follow-up periods, larger sample sizes, inclusion of centrally-acting β2-adrenergic receptor agonists, and biomarker-stratified analyses are warranted to clarify potential cognitive effects and underlying mechanisms of action.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261457957 - Supplemental material for Exploring the repurposing potential of β2-adrenergic receptor agonists for cognitive function: Evidence from the PharmLines Initiative Retrospective Cohort Study
Supplemental material, sj-docx-1-alz-10.1177_13872877261457957 for Exploring the repurposing potential of β2-adrenergic receptor agonists for cognitive function: Evidence from the PharmLines Initiative Retrospective Cohort Study by Ali Alghamdi, Elizabeth Combrtg, Spyros Balafas, Jens H.J. Bos, Barbara C. Van Munster, Martina Schmidt and Eelko Hak in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
The authors gratefully acknowledge the IADB.nl and Lifelines research teams for providing access to the linked pharmacy dispensing and cohort data used in this study. We also thank the Central Bureau of Statistics (CBS) for facilitating secure data linkage. Finally, we are indebted to the study participants whose contribution made this research possible.
Ethical considerations
Not applicable
Consent to participate
Not applicable
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Lifelines initiative has been made possible by subsidy from the Dutch Ministry of Health, Welfare and Sport, the Dutch Ministry of Economic Affairs, the University Medical Center Groningen (UMCG), Groningen University and the Provinces in the North of the Netherlands (Drenthe, Friesland, Groningen).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.