
Abstract
Background
Global cognitive performance is influenced by change in cerebral structure and educational background. However, little is known about how education moderates the impact of cerebral structural changes on different cognitive domains and other non-cognitive dysfunction across the clinical stages of Alzheimer's disease (AD).
Objective
To explore the moderating effect of education on relationship between cerebral structure and various clinical manifestations across the AD continuum, ranging from mild cognitive impairment (MCI) to AD.
Methods
This cross-sectional study included data of 570 patients diagnosed with MCI or AD. The total years of education were used as a moderating variable, and AD-related cerebral structure changes were assessed through visual ratings on magnetic resonance imaging (MRI). Multiple linear regressions were performed to examine whether education moderated the association between cerebral structure and clinical characteristics at different diagnostic stages of AD.
Results
Patients with higher levels of education demonstrated better cognitive ability, enhanced activities of daily living, and milder neuropsychiatric symptoms. The moderating effect of education was most prominent during the MCI or early AD stages, showing cognitive domain-specific effects. In these stage, education alleviated the negative impacts of neurostructural changes on immediate learning but exacerbated the detrimental effects of cerebral structural changes on speed/executive function, language, and episodic memory.
Conclusions
Education serve as a moderator in relationship between cerebral structure and various clinical characteristics. The moderating effect of education is domain-specific and most noticeable in the early stage of AD.
Keywords
Introduction
Alzheimer's disease (AD) is currently the most common cause of dementia. As a progressive neurodegenerative condition, core clinical manifestations include cognitive impairment, mental abnormalities, personality and behavioral changes, and a gradual decline in activities of daily living (ADLs).1,2 In AD patients, the prominent symptoms can be characterized a different cognitive or non-cognitive dysfunction. This heterogeneity may be related to different patterns of brain atrophy.3,4 The most typical pattern of atrophy in AD is medial temporal lobe atrophy (MTA), and some studies suggest that posterior atrophy (PA) predominates in specific subgroups, particularly among patients with early-onset AD who often present with non-amnestic initial symptoms.3,5,6 Additionally, an increasing body of studies indicates a causal relationship between white matter hyperintensities (WMH) volume and AD,7,8 with varying degrees of correlation to different clinical features of AD.9,10
Interestingly, brain regions exhibited comparable degree of structural changes can have varying clinical impact across individuals. Research has shown that education can attenuate the effect of MTA on global cognitive performance in AD patients.11–13 The variability in individual vulnerability to AD-related neuropathological changes is largely explained by the cognitive reserve (CR) hypothesis. According to this hypothesis, CR, accumulated through educational attainment and other lifetime exposures (such as occupational attainment), facilitates compensatory neural adaptations via neuroplasticity. This mechanism helps mitigate disease risk and clinical impact despite neuropathological burden. 11 Education, while not a direct or perfect measure of CR, is frequently used as a convenient proxy due to its standardized and easily quantifiable nature.
However, education does not always plays a benign moderating role between brain integrity and cognition, individuals with high reserve exhibit a greater neuropathological burden at equivalent clinical symptom severity. This suggests an extended preclinical resilience phase where compensatory mechanisms delay symptom onset. Once the pathology surpassess reserve capacity thresholds, the decline trajectory accelerates due to the depletion of neural compensation reserves. 11 Studies have shown that higher educational attainment correlates with better episodic memory at low levels of MTA, yet predicts poorer performance at more advanced MTA stages 14 ; in cases of mild cognitive impairment (MCI), education do not seem to moderate the effect of WMH on global cognition, immediate memory, or speed/executive function. 15 These findings highlight that the moderating role of education is context-dependent, varying across cognitive domains, stages of disease progression, and neurostructural biomarkers (e.g., MTA/PA/WMH patterns). However, there has been limited research on how the moderating effect of education evolves with disease progresses. Additionally, it remains unclear whether education similarly moderates the relationship between AD-related cerebral structure changes and key non-cognitive symptoms, such as neuropsychiatric symptoms (NPS) and ADLs.
Therefore, the current study investigates the relationship between diverse clinical manifestations and cerebral structural changes in AD, as assessed through magnetic resonance imaging (MRI). This include AD's primary cerebral structural change patterns: MTA, PA and WMH. We specifically focus on exploring the moderating effect of education on the associations between cerebral structure and clinical characteristic. Consistent with most previous research methodologies, our initial analysis encompassed the entire disease continuum, including patients with MCI—a stage in the AD pathophysiological continuum where there is no significant impairment in social or occupational function, and thus the criteria for dementia are not yet meet. 16 Building upon the evidence that educational effects are context-dependent, we further stratify our analyses by disease progression phases: MCI, mild AD, moderate AD, and severe AD.
Methods
Participants
All the patients were enrolled at the Memory Clinic of The First Affiliated Hospital of Chongqing Medical University between January 2015 and December 2023. This study was approved by the Ethics Committee of The First Affiliated Hospital of Chongqing Medical University (approved on 22 July 2014; approval no. 2014-15-2). Subjects with AD there has been limited research on how the moderating effect of education evolves with disease progresses, 1 while patients diagnosed with MCI met the clinical criteria for “MCI due to AD” according to the NIA/AA guidelines. 16 All participants completed basic information collection, neuropsychological assessment, and head MRI scans. Exclusion criteria included: (i) Subjects with other serious neurological diseases or psychiatric disorders; (ii) Patients with cognitive impairment due to other types of dementia (e.g., vascular dementia, frontotemporal dementia, Lewy body dementia, and Parkinson's disease17,18; (iii) Patients with conditions such as hypothyroidism, vitamin B12 or folic acid deficiency, neurosyphilis, HIV infection and other non-neurological diseases that may cause cognitive dysfunction; and (iv) patients with serious systemic diseases, such as advanced cardiac, pulmonary, hepatic, or renal failure.
A total of 776 participants underwent neuropsychological assessments and had available structural MRI data. Of these, 78 were excluded due to a confirmed diagnosis of cognitive impairment attributable to comorbid disorders (n = 45) or insufficient diagnostic information to confirm the etiology of cognitive impairment (n = 33). An additional 103 participants were excluded for incomplete neuropsychological assessment (n = 71) and/or missing covariates (n = 32), and 25 were excluded due to severe systemic diseases. 93 participants had CSF Aβ42/tau or amyloid-PET data, comfirming AD pathology (Aβ+). Ultimately, the final sample for analysis compsisted of 570 participants, including 408 with a diagnosis of AD and 162 with a diagnosis of MCI.
Neuropsychological assessment
Standardized tests were used to assess patients’ cognitive function, NPS, and ADLs, the severity of AD was graded by the global score of the Clinical Dementia Rating (CDR): CDR ≤1 indicates as mild AD, CDR = 2 indicates moderate AD, and CDR = 3 indicates severe AD. 19 The comprehensive neuropsychological battery assessed the following cognitive domains: episodic memory, immediate learning, speed/executive, attention, visuospatial abilities, and language. Composite scores were derived by converting neuropsychological scores into z-scores using the sample's mean and standard deviation (SD) of the raw scores, and averaging within corresponding domain. For example, the global cognition composite score incorporated standardized data from Chinese version of the Mini-Mental State Examination (MMSE) and the Alzheimer's Disease Assessment Scale–Cognitive Subscale (ADAS-Cog).20,21 The neuropsychological assessment scales for each domain are provided in Supplemental Table 1. The composite global cognition, composite ADLs, and NPS served as primary outcome variable, Secondary analyses examined individual cognitive domains. Higher cognitive scores indicated better performance, while higher scores in ADLs, NPS, and visual rating scales indicated worse performance in the corresponding aspects.
Structural MRI acquisition and image analysis
All participants underwent whole-brain MRI scans using a 3.0 T Phillps Ingenia scanner, high-resolution volumetric (3D) T1-weighted sequences were acquired, alongside a variable range of trans-axial T2-weighted or fluid-attenuated inversion recovery (FLAIR) images.
The complete MRI dataset of all participants was visually rated by three trained assessors who were blinded to any demographic information, neuropsychological assessments, and clinical diagnosis. MTA, PA and WMH were rated according to established scales from the literature: (i) MTA scoring was performed in T1-weighted coronal views, rating both hemispheres separately. A 5-point rating scale: 0 = no atrophy, 1 = minimal atrophy, 2 = mild atrophy, 3 = moderate atrophy, 4 = severe atrophy based on the height of hippocampal formation, choroidal fissure, and width of temporal horn 22 ; (ii) PA was rated using the scale by Koedam et al., 6 based on the anatomical regions including the parietooccipital sulcus, posterior cingulate sulcus, cortex of the parietal lobes, and the precuneus, on a 4-point scale (0 = no atrophy, 1 = mild sulcus enlargement and mild atrophy, 2 = substantial enlargement and substantial atrophy; and 3 = evident sulcus enlargement and knife-blade atrophy). (iii) WMH severity was assessed using the Fazekas scale, based on axial T2-weighted or FLAIR images, on a 4-point scale (0–3). 23 The ratings for MTA, PA and WMH were depicted in Figure 1.
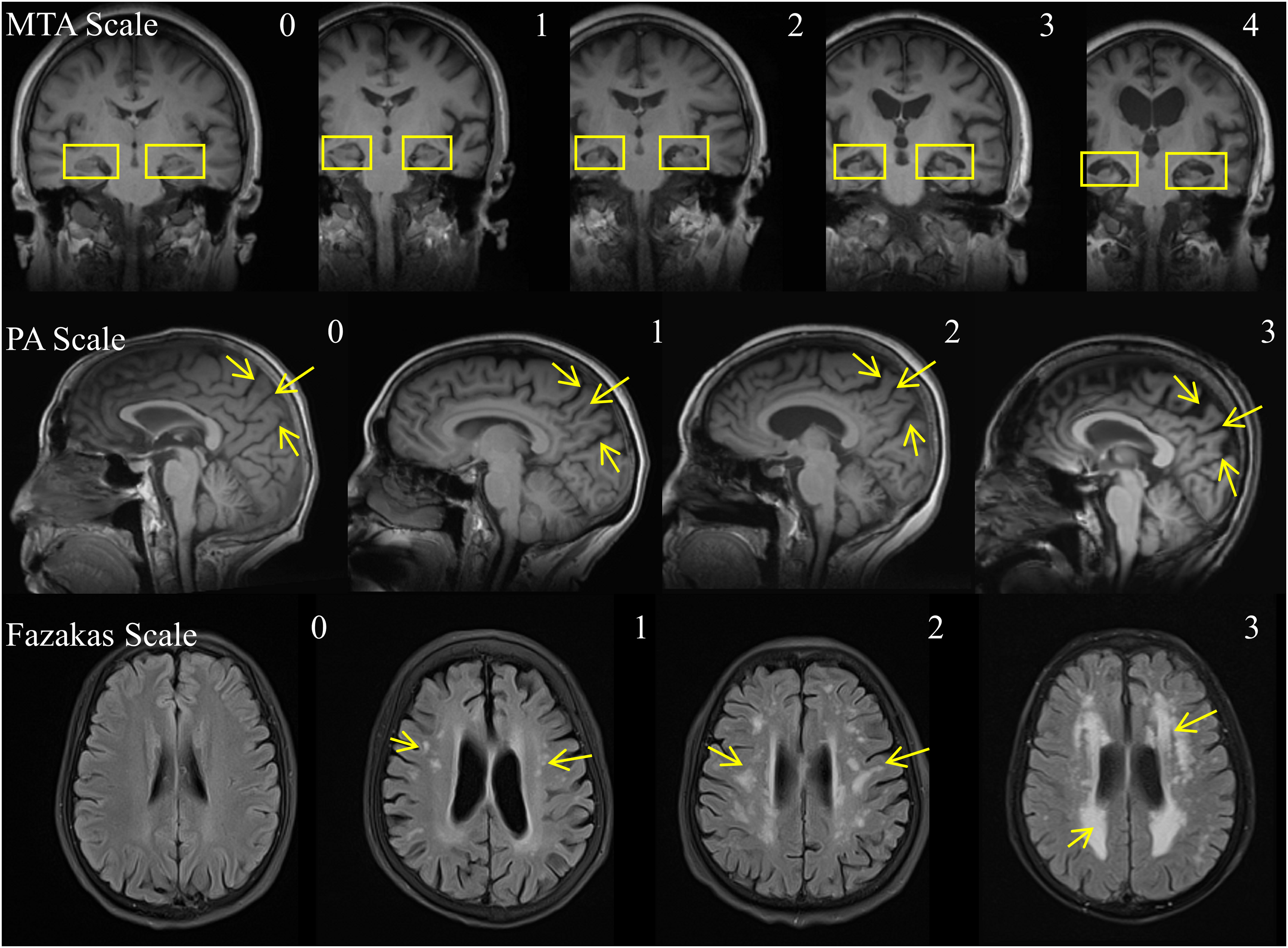
The scoring of visual rating scales for MTA, trans-axial PA, and WMH. Note. MTA, medial temporal atrophy; PA, posterior atrophy; WMH, white matter hyperintensities
Covariates
All analyses were controlled for age, gender, family history, and disease duration. Age was treated as a continuous variable, while gender was coded as a binary variable with females as the reference group. Family history was defined as the presence of at least one first-degree relative diagnosed with AD or another forms of dementia, and was represented by a binary variable with positive family history as the reference group. Disease duration was calculated as the time (in years) between the first reported occurrence of AD core symptoms (as recalled by the patient or caregiver) and the study enrollment evaluation. These covariates were retained based on prior evidence of their associations with both education and cerebral structural changes, as detailed in Supplemental Table 2, which all retained covariates demonstrated significant associations with at least one key variable.
Statistical analysis
Differences in the quantitative and ordinal variables (age, years of education, neuropsychological assessment scores, and visual rating scales scores) among four clinical groups (MCI, mild AD, moderate AD, severe AD) were compared using one-way ANOVA or Kruskal-Wallis H test. Nominal variables such as gender and family history were assessed between groups using the Chi-square test. Intraclass correlation coefficient (ICC) was used to assess the inter-rater reliability of each brain MRI visual rating scores, with a two-way random, single-measure absolute ICC used to determine the reliability for single rater.
Multiple linear regression was employed to examine the effects of AD-related cerebral structural changes (MTA, PA, WMH), years of education, and their interactions on cognitive ability, NPS, and ADLs. In the first step, analysis were conducted on the entire samples(570 patients with AD or MCI), with global cognitive composite score, NPS and ADLs composite score as dependent variables. Independent variables included the mean value of MTA (both hemispheres), PA, WMH and self-reported years of education, and covariates such as age, gender, family history and disease duration were controlled. Interaction terms were created by multiplying the centered visual rating scale scores by years of education. After the omnibus test of the main effect and interaction, separate regressions was carried out for each cognitive domains. And then, in the second step, the above analyzes were conducted separately for the MCI group and the three AD groups. The quantitative moderating effects of interactions were further explored through simple slope analysis. To visualize interaction effects, simple slope analyses were conducted by plotting conditional regression lines for the association between cerebral structure changes (X) and clinical manifestations (Y) at two discrete levels of the moderator (education years): + 1 SD above the mean (high education), and −1 SD below the mean (low education). These visualizations were generated unconditionallyfor the omnibus test of total sample but only for significant moderation effects in cognitive domain/disease-stage groups. Finally, multiple comparison correction for interaction effects were applied using the Benjamini-Hochberg procedure to control the false discovery rate (FDR) at 5%. All analyses were conducted in SPSS (Version 26), with two-tailed p-values, and statistically significant was set at p < 0.05.
Results
Demographic and clinical data
The demographic features, neuropsychological scores/composite scores and visual rating scores of the patients were summarized in Table 1. The distribution of gender and family history were no significant differences between four clinical groups (MCI, mild AD, moderate AD, severe AD). The years of education ranged from 0 to 19 years. Patients in more severe clinical stages have the following characteristics: older age, longer disease durations, shorter years of education, worse cognition, NPS and ADLs, as well as more pronounced MTA, PA, and WHM.
Demographic and clinical data.
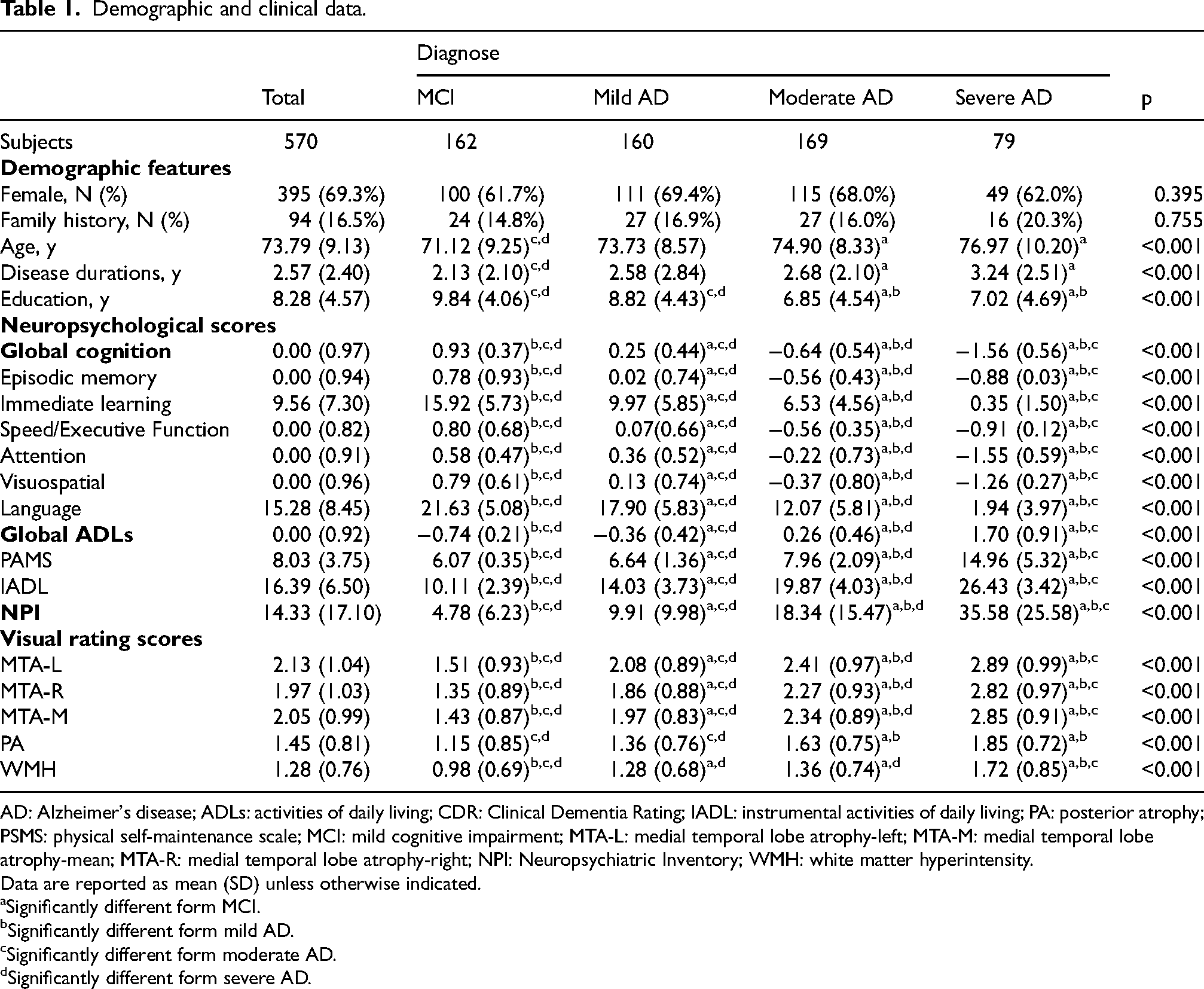
AD: Alzheimer's disease; ADLs: activities of daily living; CDR: Clinical Dementia Rating; IADL: instrumental activities of daily living; PA: posterior atrophy; PSMS: physical self-maintenance scale; MCI: mild cognitive impairment; MTA-L: medial temporal lobe atrophy-left; MTA-M: medial temporal lobe atrophy-mean; MTA-R: medial temporal lobe atrophy-right; NPI: Neuropsychiatric Inventory; WMH: white matter hyperintensity.
Data are reported as mean (SD) unless otherwise indicated.
Significantly different form MCI.
Significantly different form mild AD.
Significantly different form moderate AD.
Significantly different form severe AD.
In this study, 62.11% of participants demonstrated clinically significant MTA (MTA scores ≥2), 47.89% exhibited obvious PA (PA scores ≥2), and 29.82% showed WMH (WMH scores ≥2), meeting the threshold for pathological severity. After adjusting for age, gender, family history, and disease duration, years of education showed no significant association with MTA (β = −0.033, p = 0.478), PA (β = −0.050, p = 0.255), or WMH (β = 0.033, p = 0.490).
Inter-rater reliability of visual rating scores
The inter-rater reliability of the visual rating MTA, PA and WMH scores were reflected by single measure and average measure ICC values. Single-measure ICC values represent the reliability of individual rater, while average-measure ICC values reflect the reliability of the group as a whole. The inter-rater reliability was highest for the WMH scale [ICC (3, 1) = 0.913, 95%CI (0.882, 0.938)]. The PA scales also demonstrated good reliability [ICC (3, 1) = 0.714, 95%CI (0.624, 0.784)]. For MTA, the ICC values ranged from 0.716 to 0.844, with the reliability for right MTA scores [ICC (3, 1) = 0.631] being slightly lower than for left MTA[ICC (3, 1) = 0.780]. Reliability based on mean inter-rater scores was consistently high for all scales [ICC (3, k) ≥ 0.837].
Association between education, cerebral structure and clinical characteristics in total sample
Main effect and two-way interaction in global cognitive, ADLs and NPS
As shown in Table 2, after controlling for age, gender, family history and disease duration, individuals with higher MTA, PA and WMH scores had worse global cognition, ADLs, and NPS scores. Education was positively correlated with global cognition but negatively correlated with ADLs/NPS, suggesting that higher education level was associated with better outcomes in global cognition, ADLs and NPS. None of the interactions between MTA, PA, WMH and education were significant.
Regression coefficients for MTA, PA, WMH, education and their interaction on global cognition, global ADLs and NPS.

ADLs: activities of daily living; Edu: education; PA: posterior atrophy; MTA: medial temporal lobe atrophy; NPS: neuropsychiatric symptoms; WMH: white matter hyperintensity.
Main effect and two-way interaction in each cognitive domain
After general testing of main effects and interactions, we analyzed each cognitive domain separately, as shown in Table 3. For MTA, the strongest correlation was found in immediate learning (β = −0.371, p < 0.001), and the interaction between MTA and education was associated with speed/executive function (β = −0.076, p = −0.027). For PA, the strongest correlation was in visuospatial function (β = −0.240, p < 0.001), but no significant interaction with education was observed for any cognitive domain, although a nearly significant moderating effect on speed/executive function was noted (β = −0.058, p = 0.086). For WMH, the strongest correlation was in speed/executive function (β = −0.186, p < 0.001), and the interaction between WMH and education was also significant for speed/executive function also (β = −0.104, p = 0.002). Notably, speed/executive function was the only cognitive domain where education significant moderated the effects of cerebral structural changes.
Regression coefficients for MTA, PA, WMH, education and their interaction on different cognitive domains.
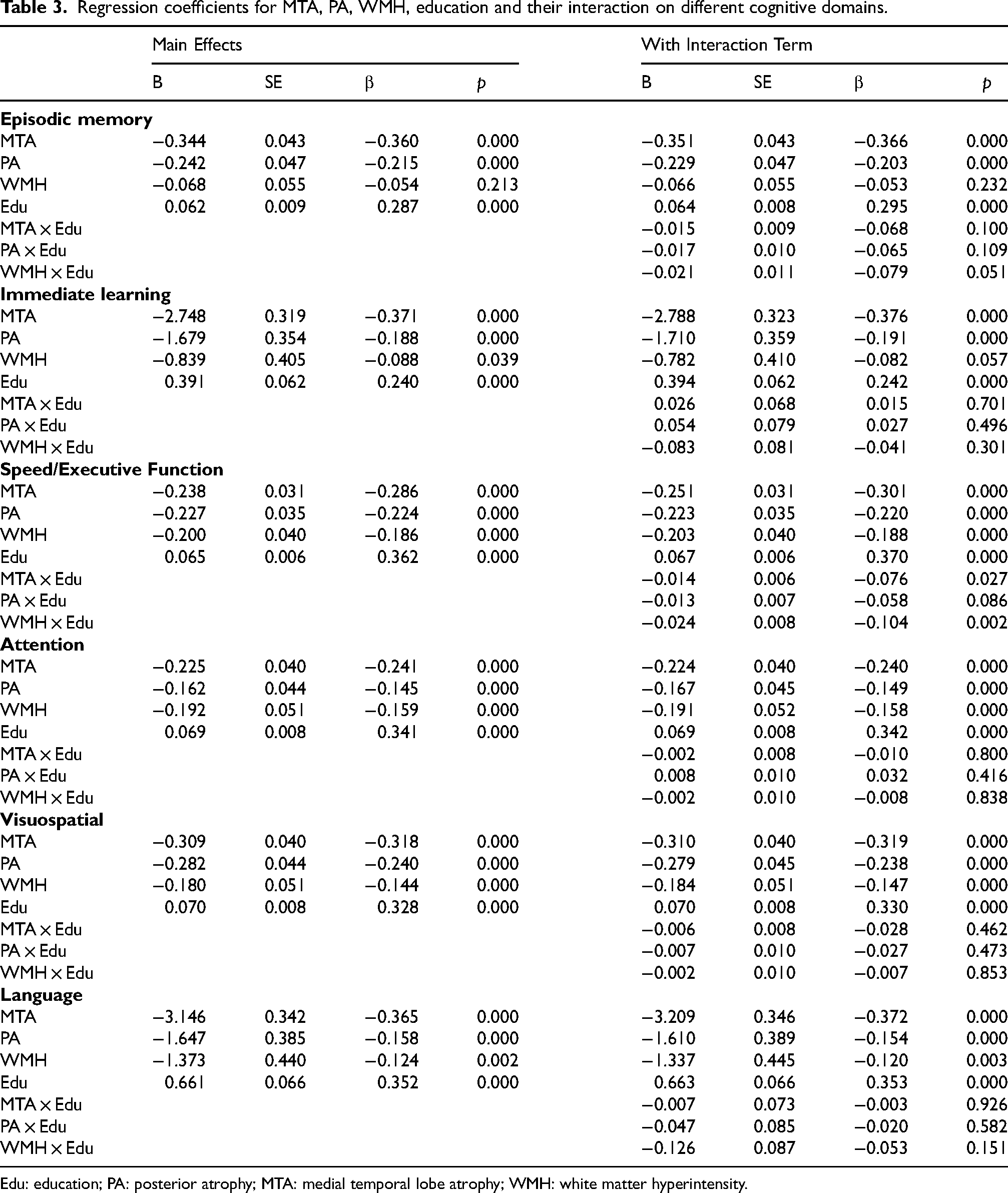
Edu: education; PA: posterior atrophy; MTA: medial temporal lobe atrophy; WMH: white matter hyperintensity.
Simple slope analysis
Firstly, simple slopes analyses in omnibus test of total sample were performed to facilitate comparison with previous studies and further explore the findings in ADLs and NPS (Figure 2). Simple slope analyses revealed significant associations between MTA, PA and WMH with global cognition, ADLs and NPS in individuals with higher education. However, for individuals with lower education, no significant association was found between PA and NPS (t = 1.505, p = 0.133) or between WMH and global cognition (t = −1.504, p = 0.133). Associations involving MTA and the remaining combinations (PA with global cognition/ADL; WMH with ADLs/NPS) remained significant in the low-education group.

Education years by AD-related cerebral structure interaction for global cognition, ADL and NPS. Figure 2 shows quantitative interaction dissected by a simple slope analysis plotting one SD above and below the mean of education years, in this sample, representing the effects of cerebral structure changes on clinical characteristics for those with less than 3.71 years of education and more than 12.85 years of education. No significant interactions between education and cerebral measures (MTA/PA/WMH) were observed for any outcome in the full sample across the illustrated slopes. Note. AD, Alzheimer's disease; ADL, activities of daily living; MTA, medial temporal atrophy; NPS, neuropsychiatric symptoms; PA, posterior atrophy; WMH, white matter hyperintensities.
Further analysis of the significant interactions in different cognitive domains (as shown in Figure 3) revealed that higher MTA severity was associated with poorer speed/executive function in both education groups. However, the negative association between MTA severity and executive ability was significantly stronger in individuals with higher education (high education: t = −7.516, p < 0.001; low education: t = −4.442, p < 0.001). Similarly, WMH had a significantly negative association with speed/executive function in individuals with higher educations (t = −6.058, p < 0.001), whereas no significant association was found in those with lower education (t = −1.724, p = 0.085).

Education years by AD-related cerebral structure interaction for speed/executive function. One standard deviation above and below the mean were used as points to plot for education and AD-related cerebral structure changes. No significant interaction between education and PA was observed for speed/executive function. Note. AD, Alzheimer's disease; MTA, medial temporal atrophy; PA, posterior atrophy; WMH, white matter hyperintensities.
Moderation analyses and simple slope analyses across diagnostic groups
Global cognitive, ADLs and NPS relationship
Supplemental Table 3 presented the standardized beta weights for AD-related core clinical symptoms regressed on education, visual rating scores, and their interaction terms within each diagnostic group, controlling for age, gender, family history, and disease duration. Education had a significant positive effect on global cognition in MCI, mild AD and moderate AD, but not in severe AD. A two-way interaction between MTA and education years was found for global cognition in the MCI group. Simple slope analyses revealed that for individuals with higher education, lighter MTA was associated with better global cognition (t = −7.868, p < 0.001), whereas no such association was found for those with lower education (t = −0.923, p = 0.357). In contrast, an opposite two-way interaction between WMH and education was found for NPS in the severe AD group. Among individuals with lower education, more pronounced WMH was associated with worse NPS (t = 2.180, p = 0.033), whereas no such association was found in those with higher education (t = −0.464, p = 0.644). Significant interaction effects across diagnostic groups were illustrated in Figure 4.
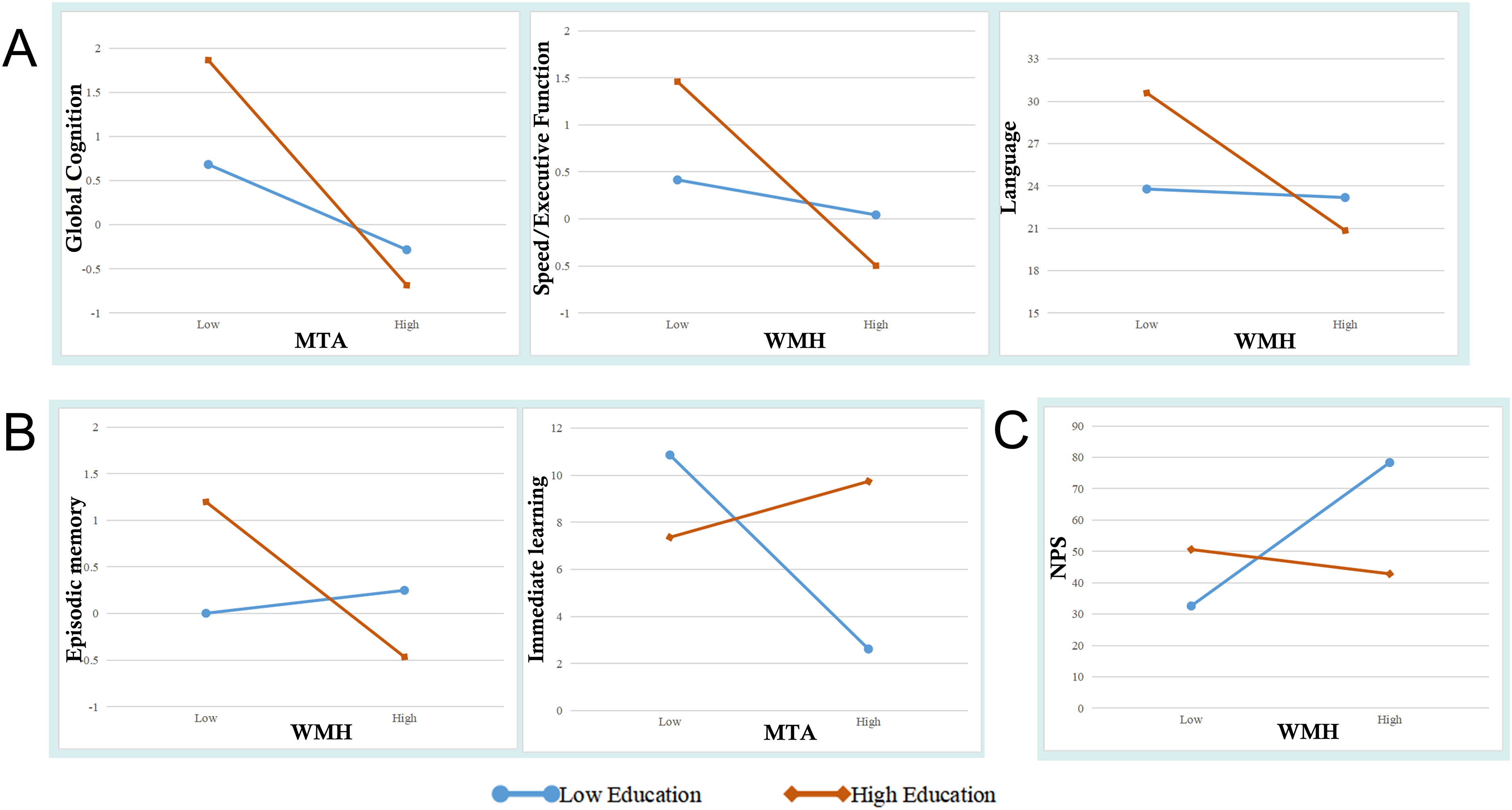
Moderating effects of education at different clinical stages. (A) Effects of MTA on global cognition, WMH on speed/executive function, and WMH on language (from left to right) in MCI patients with high education vs. low education; (B) Effects of WMH on episodic memory and MTA on immediate memory (from left to right) in mild AD patients with high education vs. low education; (C) Effects of WMH on NPS in severe AD patients with high education vs. with low education. Note. AD, Alzheimer's disease; MCI, mild cognitive impairment; MTA, medial temporal atrophy; PA, posterior atrophy; WMH, white matter hyperintensities.
Cognitive domain relationship
Further regression anlyses for each cognitive domain within each diagnostic group are presented in Supplemental Table 4. In MCI, a two-way interaction between WMH and education years was found for both speed/executive function and language, indicating that higher education strengthened the negative relationship between WMH and these cognitive abilities. In AD, the interactions between all cerebral structure changes and education were significantly associated with episodic memory. In mild AD, a two-way interaction between WMH and education years was found for episodic memory; a two-way interaction between MTA and education years was found for immediate learning, with attenuated negative correlations between MTA and immediate learning in individuals with higher education, while stronger negative associations between WMH and episodic memory. No significant interaction effects of cerebral structural changes and education were found for any cognitive domain in moderate AD and severe AD.
Finally, multivariable regression models were used to test three interaction terms (MTA × education, PA × education, WMH × education) as potential moderators of AD-related clinical manifestations. Benjamini-Hochberg FDR correction was applied to account for multiple comparisons. Key findings include: In the total sample, MTA × education (p = 0.027, q = 0.033) and WMH × education (p = 0.002, q = 0.017) remained significant for speed/executive function; In the MCI group, MTA × education (p = 0.013, q = 0.017) for global cognition and WMH × education (p = 0.005, q = 0.05) for speed/executive function survived correction; in the AD group: PA × education (p = 0.024, q = 0.033) for speed/executive function and WMH × education (p = 0.04, q = 0.05) for episodic memory retained significance. Other significant interaction did not survive the correction threshold. Notably, all education-moderated effects on speed/executive function remained robust across analyses, suggesting that education play a critical moderating role in the impact of cerebral structure on speed/executive function. Non-significant interactions may require replication with enhanced measurement precision or larger samples.
Discussion
This study demonstrates that MTA, PA, WMH and education are associated with global cognition, ADLs, and NPS; Specifically, MTA, PA and WMH are most strongly related to immediate learning, visuospatial abilities, and speed/executive functions, respectively. Education interacts significantly with MTA and WMH in the context of speed/executive function, with higher education correlating with stronger negative associations between MTA/WMH and speed/executive functions. The moderating effect of education differ across disease stages and particularly evident in the early stages of AD. In MCI or mild AD patients, higher education attenuates the negative associations between cerebral structural integrity and immediate learning, while also strengthening the inverse associations of cerebral structures with speed/executive function, language and episodic memory.
Clinical heterogeneity and cerebral structure variability
MTA and PA are commonly observed in patients with AD and MCI, and recent studies have highlighted that WMH is not only associated with aging and vascular factors but also contributed to AD pathogenesis through extravascular mechanism. 8 Consistant with previous studies, our study find that different cerebral structural changes are related to impairment in specific cognitive domains, and they are also significantly associated with non-cognitive symptoms. Among these, NPS and ADLs are most affected by MTA. Given the multitude of findings, the comparison between the present study and previous research findings is summarized in Supplemental Table 5. In addition, the correlation between a particular brain region and a cognitive domain varied disease stages. For instance, in MCI, MTA is most correlated with episodic memory whereas in AD, it is more correlated with language function. These stage-dependent changes may be due to the progressive involvement of multiple brain regions as the disease advances. These findings highlight how the specific pattern of brain structure changes, their differential relationships with cognitive and non-cognitive domains, and the stage-dependent shifts in these relationships contribute to the clinical heterogeneity observed in cognitive impairment.
Education's moderating effects and evidence for CR
In the total sample, education demongstrates a significant positive correlation with global cognition and most cognitive domains, as well as a significant negative correlation with NPS and ADLs. Although no significant interaction is observed between MTA, PA, WMH and years of education for global cognition, our analyses provide direct evidence supporting CR hypothesis: as illustrated in Figure 2, at equivalent global cognitive scores (Y-axis), individuals with higher education tend to have greater MTA, PA and WMH burden (X-axis). This discrepancy of pathological burden greater atrophy at equivalent cognitive performance in more educated individuals supports the CR hypothesis, independent of moderation effects.
However, in the total sample, only speed/executive function have shown a significant interaction effect between education and MTA/WMH, which contrasts with some previous findings.14,24 This discrepancy may be due to variations in educational status across populations in different studies. Gyllenhammar et al. 14 found that a steeper slope between MTA and episodic memory in higher-educated MCI and AD patients, whereas no such effect was found in our study. The mean years of education in their study (12.62 ± 3.67) was higher than in ours (8.28 ± 4.57). Similarly, the findings of Scarmeas et al. 25 (7.1 ± 4.5) align more closely with ours, showing a significant interaction only for speed/executive function. These differences highlight how the classification of education levels (e.g., dividing individuals based on one SD above or below the mean) can lead to varying results across studies. Future research should adopt a standardized method for classifying high and low education levels and explore how many years of education play a moderating role.
Heterogeneity in education's moderating effects across disease stages
Further validating Stern's CR model, 11 our analyses across diagnostic groups reveal that, at mild AD stage, individuals with high education show a non-significant positive slope in immediate learning, in contrast to a significant negative slope observed in the low-education group. Meanwhile, higher education is associated with steeper negative slopes in speed/executive function and language performance inthe MCI stage, as well as a steeper negative slope in episodic memory across all AD stages. This varying moderating effect of education across disease stages and the convergence of slopes in high and low education groups in specific clinical manifestations point to non-linear cognition-neuropathology relationships influenced by education. Although disease stage is not solely determined by atrophy severity, advancing clinical stages are generally linked with increased neurostructural degeneration (Table 1). Our study demonstrats that education has a significant positive effect on global cognition in MCI, mild AD and moderate AD, but not in severe AD, This suggest that the protective effects of education diminish as neurostructural degeneration progresses, culminating in the complete loss of moderation at advanced stages . These findings support the biphasic cognitive trajectory in CR theory,11,26 where highly educated individuals show prolonged cognitive maintenance during early neurodegeneration, followed by accelerated functional decline once reserve capacity is exceeded.
Despite general alignment with the biphasic CR trajectory, some domain-specific deviations warrant further exploration. Specifically, consistent with previous study, our high- education group do not exhibit an attenuated negative association between cerebral structures and global cognition, 15 executive function, 15 visuospatial 25 or language 25 in early AD. This domain-specific pattern may be due to the varying vulnerability of the neural substrates supporting different cognitive functions to AD pathology. Higher-order “fluid” functions like executive function and processing speed, which depend on prefrontal and fronto-striatal circuits, are often among the earliest and most severely affected in AD.27,28 Thus, the protective mechanisms of education may be less effective these particularly vulnerable networks during early AD stages. Additionally, the sample composition (fewer MCI, no SCD or cognitively normal individuals) may limit our ability to detect protective effects in the earliest phases across all domains.
It is important to note that CR, as a theoretical construct, cannot be directly evaluated. Instead, socio-behavioral proxies (such as education, intelligence quotient, occupational complexity, leisure and physical activities) are typically used in related research. In the context where CR proxy can elucidate individual differences in the relationship between brain states and functions, the results associated with the proxy and the CR model mutually interpret and reinforce each other.29,30 Thus, the present study contributes valuable evidence for CR.
Additionally, in severe AD, education plays a moderating role in the association between WMH and NPS. 31 However, due to the limited sample size in the severe AD group, the evidence supporting this finding is weak. Future studies with larger sample size may help verify the effect. As for ADLs, no significant moderating effect of education is observes in the overall sample or across different disease stage. This may reflect the domain-specific nature of CR proxies: while education enhances executive functions that support complex instrumental ADLs, such as financial management and meal preparation, it may not adequately buffer against motor/procedural impairments that predominantly affect basic ADLs in AD. Other CR proxies, such as physical activity and social engagement, may provide more direct support for preserving functional independence. 32
Strengths and limitations
The main strengths of this study include its comprehensive analysis across multiple cognitive domains, disease stages, AD-related cerebral structural changes, and the expanded focus of ADLs and NPS. Additionally, the study include a sample primarily from southwest China, which has been underrepresented in similar studies. Given that race can influence the association between education and cognition. These findings help bridge a gap in the literature and may facilitate generalization to other Asian and non-Asian populations.
However, several limitation exist. First, the cross-sectional design limits our ability to draw causal conclusions about the moderating effect of education. Longitudinal studies tracking clinical progression would help validate and extend these findings. Second, although years of education is a well-established proxy for CR, incorporating additional indicators–such as occupational complexity and engagement in leisure activities–could provide a more comprehensive insights into reserve mechanisms. Finally, while visual rating of MTA, PA and WMH have good inter-rater reliability, they may be less sensitive to neuroanatomical changes than machine learning-based methods. The possible future direction is to use machine learning algorithms to discover as many AD-related cerebral structural changes as possible and integrate them into a low-dimensional structure.
Conclusions
This study provide evidence that education moderates the relationship between cerebral structure and clinical features in AD. Education plays a moderating role mainly in MCI and mild AD stages, where immediate learning are less affected by cerebral structural changes in patients with high education, versus speed/executive function, language and episodic memory are more affected. The inconsistency in the moderating role of education across disease stages and cognition domains offer insights into the machanism underlying cognitive reserve and contribute to the ongoing exploration of AD prevention and therapeutic strategies.
Supplemental Material
sj-docx-1-alz-10.1177_13872877251379078 - Supplemental material for Education as a domain-specific moderator: Shaping the impact of cerebral structural changes on clinical manifestations in Alzheimer's disease
Supplemental material, sj-docx-1-alz-10.1177_13872877251379078 for Education as a domain-specific moderator: Shaping the impact of cerebral structural changes on clinical manifestations in Alzheimer's disease by Tianqing Deng, Jingxi Duan, Wuhan Yu, Zhangjing Deng, Qi Tian, Xintong Liu, Jianwei Shou, Ting Tang, Weihua Yu and Yang Lü in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
The authors express their gratitude to all persons who contributed to the realization of this work.
ORCID iDs
Ethical considerations
This study was approved by the Ethics Committee of The First Affiliated Hospital of Chongqing Medical University (approved on 22 July 2014; approval no. 2014-15-2).
Consent to participate
All the participants provided written informed consent to use their data.
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Chongqing Talent Plan (cstc2022ycjh-bgzxm0184), Key Project of Technological Innovation and Application Development of Chongqing Science & Technology Bureau (CSTC2021jscx-gksb-N0020), Science and Technology Innovation Guidance Project Led by the Academicians in Chongqing (2022YSZX-JSX0002CSTB), STI2030-Major Projects (No. 2021ZD0201802) and Program for Youth Innovation in Future Medicine, Chongqing Medical University (W0166).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data supporting the findings of this study are available from the corresponding author, upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.