
Abstract
Background:
Cognitive reserve (CR) and brain reserve (BR) could offer protective effects on cognition in the early stage of Alzheimer’s disease (AD). However, the effects of CR or BR on cognition in individuals with subjective cognitive decline (SCD) are not clear.
Objective:
To explore the effects of CR and BR on cognition in subjects with SCD.
Methods:
We included 149 subjects from the Sino Longitudinal Study on Cognitive Decline (SILCODE) study. Education was used as a proxy for CR, and head circumference was used as a proxy for BR. Multiple linear regression models were conducted to examine the effects of CR and BR on cognitive scores. Furthermore, we assessed differences in effects between APOE ɛ4 carriers with SCD (n = 35) and APOE ɛ4 non-carriers with SCD (n = 114) and linear trends among 4 reserve levels (low BR/CR, high BR/low CR, low BR/high CR, and high BR/high CR).
Results:
Both CR and BR had independent positive effects on multiple cognitive measures in SCD participants, and the effects of CR were greater than those of BR. CR has positive effects on cognitive measures in both APOE ɛ4 carriers and non-carriers with SCD. However, the positive effects of BR on cognitive measures were observed in APOE ɛ4 non-carriers with SCD but not in APOE ɛ4 carriers with SCD. Furthermore, there was a linear trend toward better cognitive performance on all cognitive measures in the BR+/CR+ group, followed by the BR–/CR+, BR+/CR–, and BR–/CR–groups.
Conclusion:
This study suggests that both CR and BR have the potential to delay or slow cognitive decline in individuals with SCD.
Keywords
INTRODUCTION
With an increasing aged population, Alzheimer’s disease (AD), the most common type of dementia, will pose a heavy burden on health-care systems worldwide [1]. AD is mainly characterized by memory loss, language problems, and other impairments of the cognitive domain and is pathologically characterized by amyloid-β (Aβ) plaques and neurofibrillary tangles [2, 3]. According to the amyloid cascade hypothesis of AD and the hypothetical model of dynamic AD biomarkers, Aβ deposition is a critical event and becomes abnormal first, then neurodegenerative pathological changes appear and finally lead to cognitive symptoms [4 –6].
Recently, it has been gradually recognized that 30–40% of elderly persons manage to remain cognitively normal despite sufficient AD neuropathologic changes meeting AD criteria littering their brain based on findings from neuropathologic and biomarker studies [7 –10]. To account for these individual disjunctions between severe degrees of brain pathology and normal cognitive outcomes, the concept of reserve has been proposed [11 –15]. As a theoretical construct, reserve generally refers to a capacity to fight aging and brain disease to maintain cognitive function [14]. Furthermore, reserve includes two aspects of cognitive reserve (CR) and brain reserve (BR) [11]. CR could be considered an active model and refers to the brain actively attempting to cope with brain pathology by utilizing the brain network more efficiently or calling up alternate brain networks, and is often measured by sociobehavioral indices such as educational attainment, IQ, occupational complexity, and leisure and physical activity [11, 14]. Previous studies have found that high CR is associated with a reduction in AD risk and can delay clinical progression in normal controls and mild cognitive impairment (MCI) patients, even those with AD pathology [16 –20]. BR could be envisioned as a passive model and represents neurobiological capital, including brain size and numbers of neurons and synapses and can be estimated by head circumference (HC) or directly by imaging techniques [11, 14]. Many studies have documented that lower BR was associated with an increased risk of developing AD, and greater BR had a protective effect on cognition in the predementia stages [21 –25].
Subjective cognitive decline (SCD) is defined as self-reported cognitive decline in the absence of objective neuropsychological dysfunction [26]. Mounting evidence suggests that older adults with SCD are viewed as at risk of developing MCI and AD and could serve as a potential target population for early intervention [27 –31]. Furthermore, apolipoprotein E (APOE) ɛ4 status, one of the SCD plus features proposed by the International Working Group on SCD (the Subjective Cognitive Decline Initiative [SCD-I]), increased the risk of dementia in individuals with SCD [26, 30]. Indeed, one of our recent studies has confirmed that compared with APOE ɛ4 non-carriers with SCD, APOE ɛ4 carriers with SCD showed additive reduction in the right cortical surface area [32]. However, whether there were effects of reserve on cognition and whether these effects were influenced by APOE ɛ4 status in individuals with SCD remain to be further investigated. Here, we aimed to examine the effects of CR and BR on memory, executive, language, and general cognitive functions in SCD subjects. Furthermore, we assessed differences in effects according to APOE ɛ4 status.
METHODS
Study population
In this study, we included 149 participants with SCD from the Sino Longitudinal Study on Cognitive Decline (SILCODE) (Fig. 1). The SILCODE study is a longitudinal study conducted to collect longitudinal multimodal neuroimaging data from the SCD population and aimed to construct a high-precision multimodal model for the ultra-early diagnosis of AD. Details of the design and data collection of the SILCODE study have been published elsewhere [33, 34]. In summary, SCD subjects were recruited through memory clinics or communities in April 2017, and each participant underwent an extensive assessment at the baseline visit, including a medical history interview, physical and neurological examinations, laboratory tests, neuropsychological tests, and brain magnetic resonance imaging (MRI) scanning as well as optional AV-45-positron and emission tomography (Aβ-PET) or 18F-fluorodeoxyglucose-positron emission tomography (FDG-PET). Individuals with SCD are interviewed every 15 months. Subjects were viewed as having SCD when they reported a decline in memory subjectively and failed to meet the criteria for MCI [35], dementia due to AD according to the guidelines of the National Institute on Aging Alzheimer’s Association workgroups (NIA-AA) [36], and any other diseases or conditions that can cause cognitive impairment. All subjects with SCD aged between 60 and 80 years old who were Mandarin-speaking, had at least 6 years of education and were right-handed were eligible for inclusion.
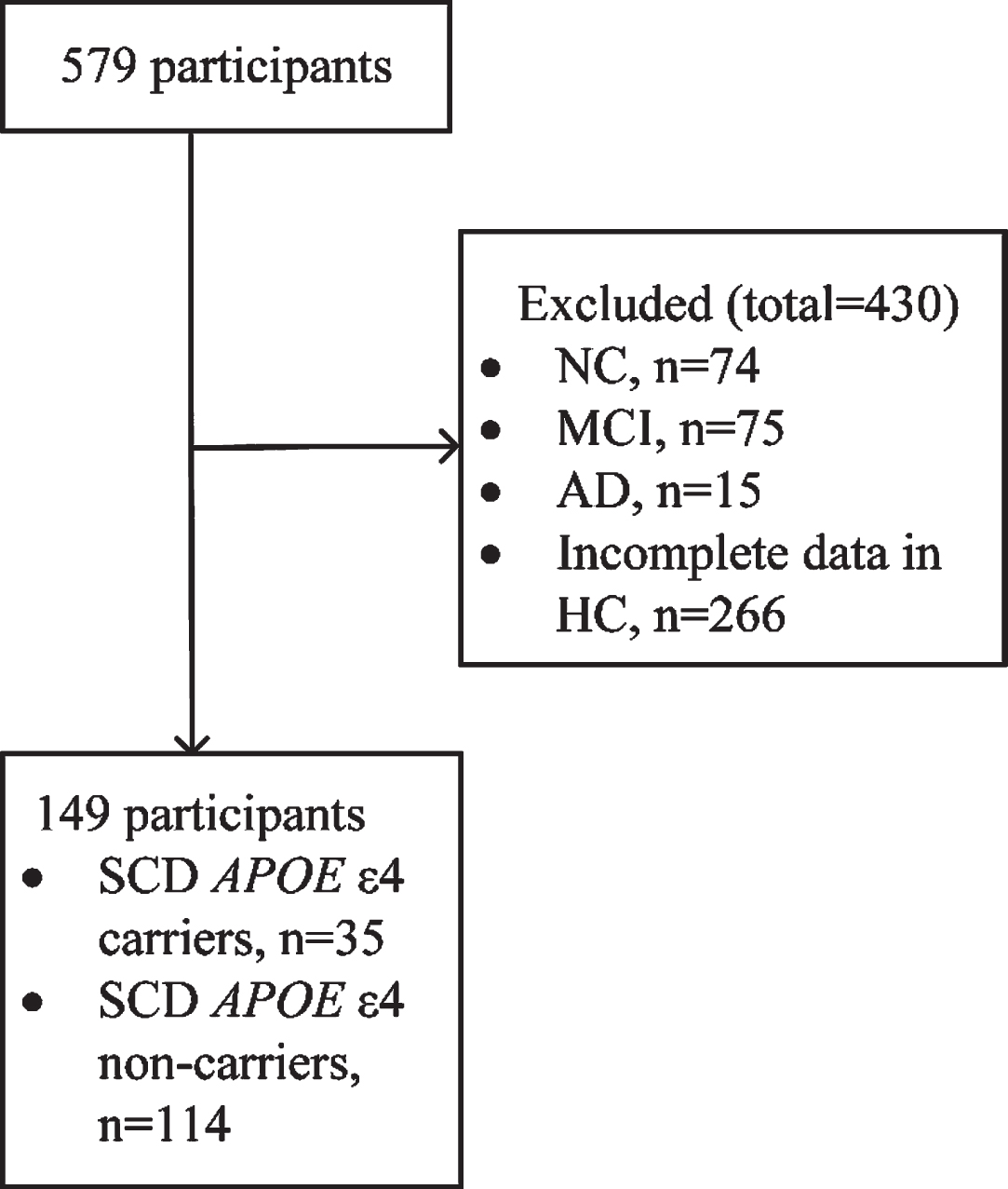
The flow charts of this study. NC, normal controls; MCI, mild cognitive decline; AD, Alzheimer’s disease; HC, head circumference; APOE, apolipoprotein E.
Neuropsychological tests
Details on neuropsychological tests were published previously [34]. In this study, we focus on 4 cognitive domains: memory (Auditory Verbal Learning Test-Huashan Version for long-delayed free recall [AVLT-H-N5] and recognition [AVLT-H-N7]), language (animal fluency test [AFT]; Boston Naming Test [BNT]), executive functioning (Shape Trailing Test A [STT-A] and B [STT-B]), and general cognitive function (Montreal Cognitive Assessment-Basic [MoCA-B]).
CR and BR
Years of education were used as a proxy measure of CR and were determined by asking participants the sum of years they spent in school and professional training. BR was estimated by HC. Subjects with SCD remained in a seated position, and HC was measured by placing a measuring tape over the eyebrows and passing it around the head to fit over the most posterior protuberance of the occiput [37, 38].
APOE genotyping
This work was completed by the staff of the clinical laboratory according to standard procedures. The details of APOE genotyping have been published elsewhere [33]. Blood samples were collected during the first visit, and then DNA was extracted from blood. The single nucleotide polymorphisms (SNPs) rs7412 and rs429358 form the ApoE ɛ2/ɛ3/ɛ4 haplotype. APOE was genotyped using the standard Sanger sequencing method (Sangon, Shanghai, China) with the following primers: 5′-ACGCGGGCACGGCTGTCCAAGG-3′ (forward) and 5′-GGCGCTCGCGGATGGCGCTGA-3′ (reverse). APOE was amplified using the following conditions: 1 cycle at 98°C for 10 s, 35 cycles at 72°C for 5 s, and 1 cycle at 72°C for 5 min. Polymerase chain reaction (PCR) was performed in a final volume of 30μl containing 10 pmol of forward and reverse primers, and 50 ng of genomic DNA template using PrimeSTAR HS DNA polymerase with GC Buffer (Takara Bio, Kusatsu Shiga, Japan). In this study, we categorized participants into two groups: subjects with SCD with at least one APOE ɛ4 allele (APOE ɛ4 carriers with SCD) and those without the APOE ɛ4 allele (APOE ɛ4 non-carriers with SCD).
Statistical analyses
All statistical analyses were performed with SAS (Version 9.2; SAS Institute Inc., Cary, North Carolina, USA) software. Statistical significance was set at p = 0.05 (2-sided). A Shapiro-Wilk test, Q-Q plot, and p-p plot were used to confirm normality for continuous variables. All normally distributed continuous variables are reported as the mean ± standard deviation, and non-normally distributed continuous variables are described with the median and interquartile ranges. First, linear correlation analyses (Spearman) were applied to analyze the relationships between CR, BR, and scores on neuropsychological tests, including AVLT-H-N5, AVLT-H-N7, STT-A, STT-B, AFT, BNT, and MoCA-B. Second, slopes in the two groups were compared to explore statistically significant differences in the APOE ɛ4 carriers with SCD and APOE ɛ4 non-carriers with SCD. Third, the predictive effects of CR and BR on cognitive functions were examined via a multiple linear regression analysis with the score of neuropsychological tests as the dependent variable and education and HC as independent variables assessed separately (unadjusted), followed by a model including HC or education (model 1) and a model including age, gender, HC or education, and body mass index (BMI, kg/m2) (model 2) to examine their independent effects in the total sample. Next, we examined whether the effects of CR and BR on cognition differed according to APOE ɛ4 status by performing the previously mentioned multiple linear regression analysis in APOE ɛ4 carriers with SCD and APOE ɛ4 non-carriers with SCD. For each regression model, we plotted and checked residuals. Residuals were normally distributed, heteroscedasticity was in conformance with test assumptions, and Durbin-Watson test statistics indicated independence of observations (results not shown). Then, we dichotomized the total sample into four groups in light of different total reserve levels: low BR and CR (BR–/CR–), high BR and low CR (BR+/CR–), low BR and high CR (BR–/CR+), and high BR and CR (BR+/CR+) according to the median of HC (55–56 = low BR, 57–62 = high BR) and education (6–12 = low CR, 13–22 = high CR). General linear models were used to assess the linear trend across these four levels. To examine the interactive effects of CR and BR on cognition in subjects with SCD, unbalanced ANOVA was performed with HC (quarter value: 55, 56 and 57 as cutoff) and education (6–12 = low CR, 13–22 = high CR). Furthermore, we fitted the trajectory of cognitive changes according to different levels of education and HC.
RESULTS
Demographic characteristics
Demographic and clinical characteristics and neuropsychological test results of the total sample and subgroup are summarized in Table 1. Of the 149 SCD participants, 35 (23.49%) SCD with APOE ɛ4, and 114 (76.51%) had SCD without APOE ɛ4. The mean age was 65 (63–68) years old, 68.46% of subjects were female, the mean years of education was 12 (11–15), and the mean HC was 56 cm in this study. There were no differences between APOE ɛ4 carriers with SCD and APOE ɛ4 non-carriers with SCD in demographic, clinical characteristics, and neuropsychological test results, with the exception of BMI. As shown in Table 1, BMI in APOE ɛ4 carriers with SCD was significantly higher than that in APOE ɛ4 non-carriers with SCD (p = 0.013).
Demographic and clinical characteristics of the total sample and according to APOE ɛ4 status
All normally distributed continuous variables in the table were described as mean±standard deviation and non-normally distributed continuous variables were described with the median (interquartile). APOE, Apolipoprotein E; HC, head circumference; BMI, body mass index; AVLT-H-N5, Auditory Verbal Learning Test-Huashan Version for long-delayed free recall (20 min); AVLT-H-N7, Auditory Verbal Learning Test-Huashan Version for long-delayed recognition (20 min); STT-A, Shape Trail Test A; STT-B, Shape Trail Test B; AFT, Verbal Fluency Test (animal); BNT, Boston Naming Test; MoCA-B, Montreal Cognitive Assessment-Basic. aThe p value was calculated using independent samples t tests. bThe p value was calculated using Mann-Whitney U. cThe p value was calculated using Chi-square.
Independent effects of CR and BR on neuropsychological tests
CR showed a significant correlation with each neuropsychological test (Supplementary Figure 1), and BR was merely correlated with AFT (Supplementary Figure 2). Multiple linear regression analysis revealed positive effects of CR on all neuropsychological tests for total SCD subjects in three models (all p < 0.05; Fig. 2a). However, there were no positive effects of BR on neuropsychological tests, except for the positive effect of BR on AFT (p < 0.05; Fig. 2b).
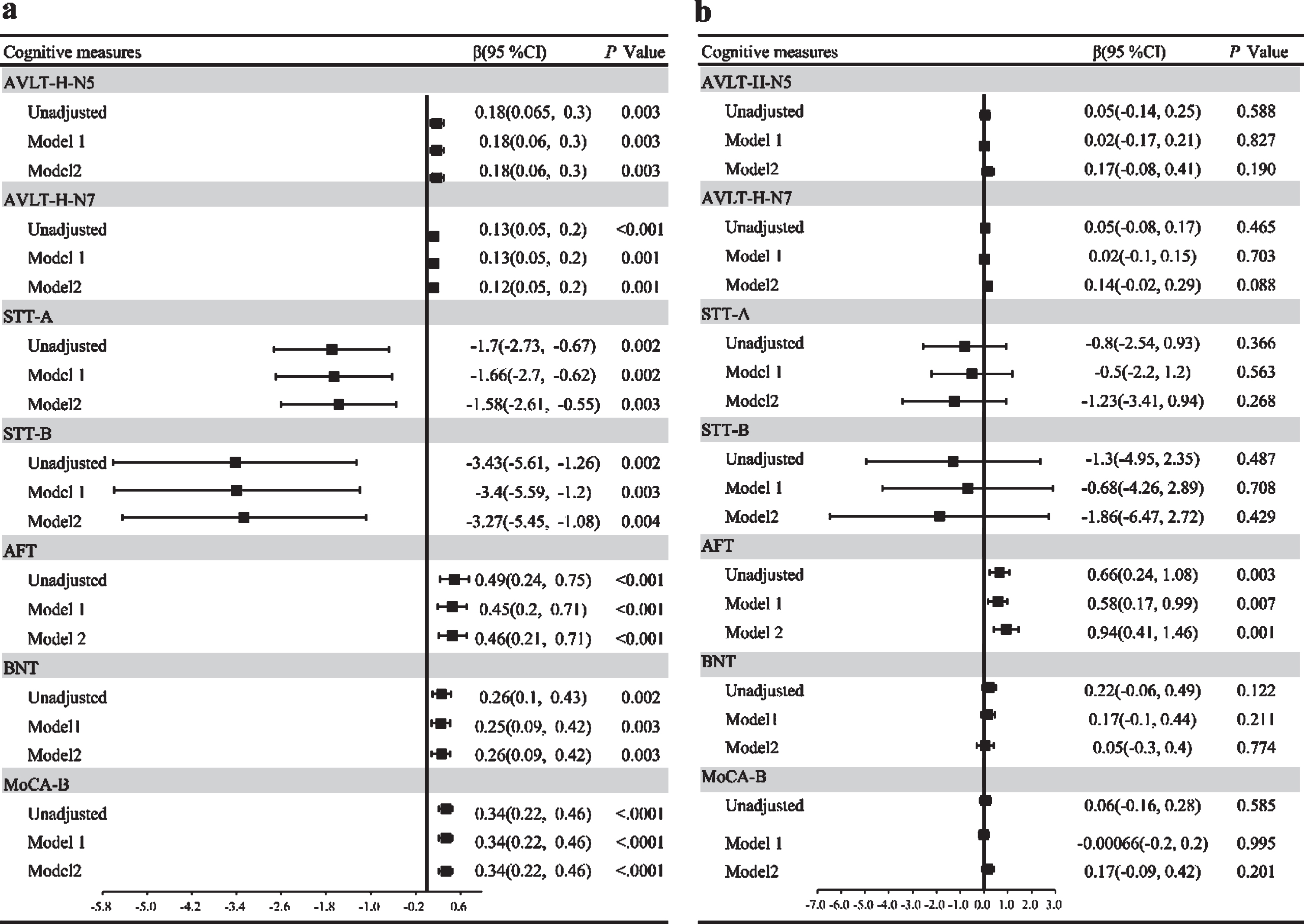
Effect sizes of education and HC on cognitive measures in the total subjects with SCD. a) Effect sizes of education. b) Effect sizes of HC. HC, head circumference; β, partial regression coefficients; CI, confidence interval; AVLT-H-N5, Auditory Verbal Learning Test-Huashan Version for long-delayed free recall (20 min); AVLT-H-N7, Auditory Verbal Learning Test-Huashan Version for long-delayed recognition (20 min); STT-A, Shape Trail Test A; STT-B, Shape Trail Test B; AFT, Verbal Fluency Test (animal); BNT, Boston Naming Test; MoCA-B, Montreal Cognitive Assessment-Basic. Model 1: adjusted for HC or education. Model 2: adjusted for age, gender, HC or education, BMI.
Independent effects of CR and BR on neuropsychological tests according to APOE ɛ4 status
The results show that all slopes in both the SCD APOE ɛ4 carrier and SCD APOE ɛ4 non-carrier groups were parallel (Supplementary Figures 3 and 4) and that carrying APOE ɛ4 had no effect on neuropsychological tests (all p > 0.05; Supplementary Tables 1 and 2). Subgroup analyses revealed that CR showed a positive effect on AVLT-H-N5, STT-A, STT-B, BNT, and MoCA-B, but not AVLT-H-N7 or AFT, for APOE ɛ4 carriers with SCD (Fig. 3a) and on all neuropsychological tests except for BNT for APOE ɛ4 non-carriers with SCD (Fig. 3b). Regarding BR, we found that there were no effects on any neuropsychological tests for APOE ɛ4 carriers with SCD (Fig. 4a). However, there were protective effects on STT-A and AFT in APOE ɛ4 non-carriers with SCD (Fig. 4b).
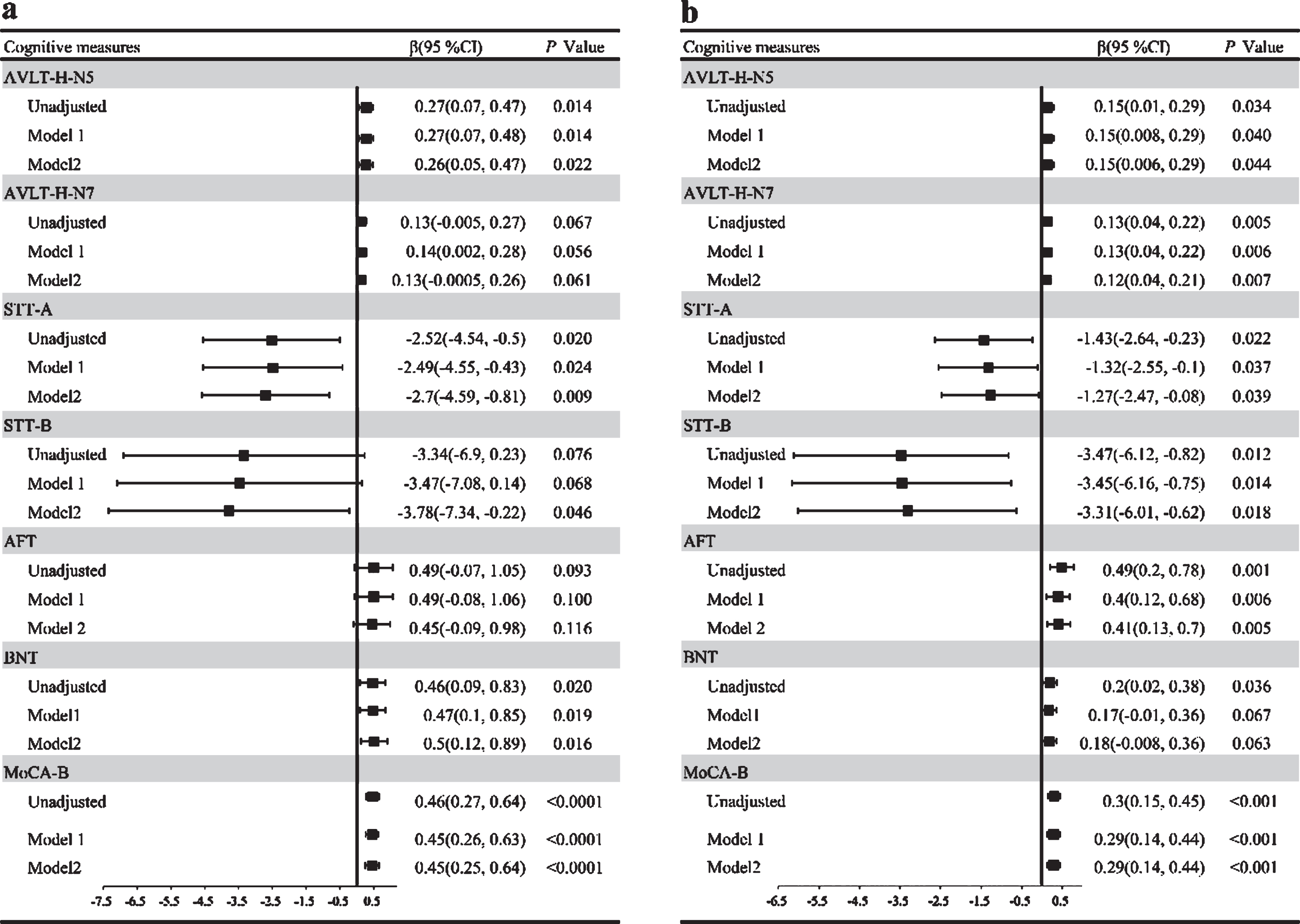
Effect sizes of education on cognitive measures according to APOE ɛ4 status. a) Effect sizes of education on cognitive measures in APOE ɛ4 carriers with SCD. b) Effect sizes of education on cognitive measures in APOE ɛ4 non-carriers with SCD. APOE, Apolipoprotein E; β, partial regression coefficients; CI, confidence interval; AVLT-H-N5, Auditory Verbal Learning Test-Huashan Version for long-delayed free recall (20 min); AVLT-H-N7, Auditory Verbal Learning Test-Huashan Version for long-delayed recognition (20 min); STT-A, Shape Trail Test A; STT-B, Shape Trail Test B; AFT, Verbal Fluency Test (animal); BNT, Boston Naming Test; MoCA-B, Montreal Cognitive Assessment-Basic. Model 1: adjusted for HC or education. Model 2: adjusted for age, gender, HC or education, BMI.
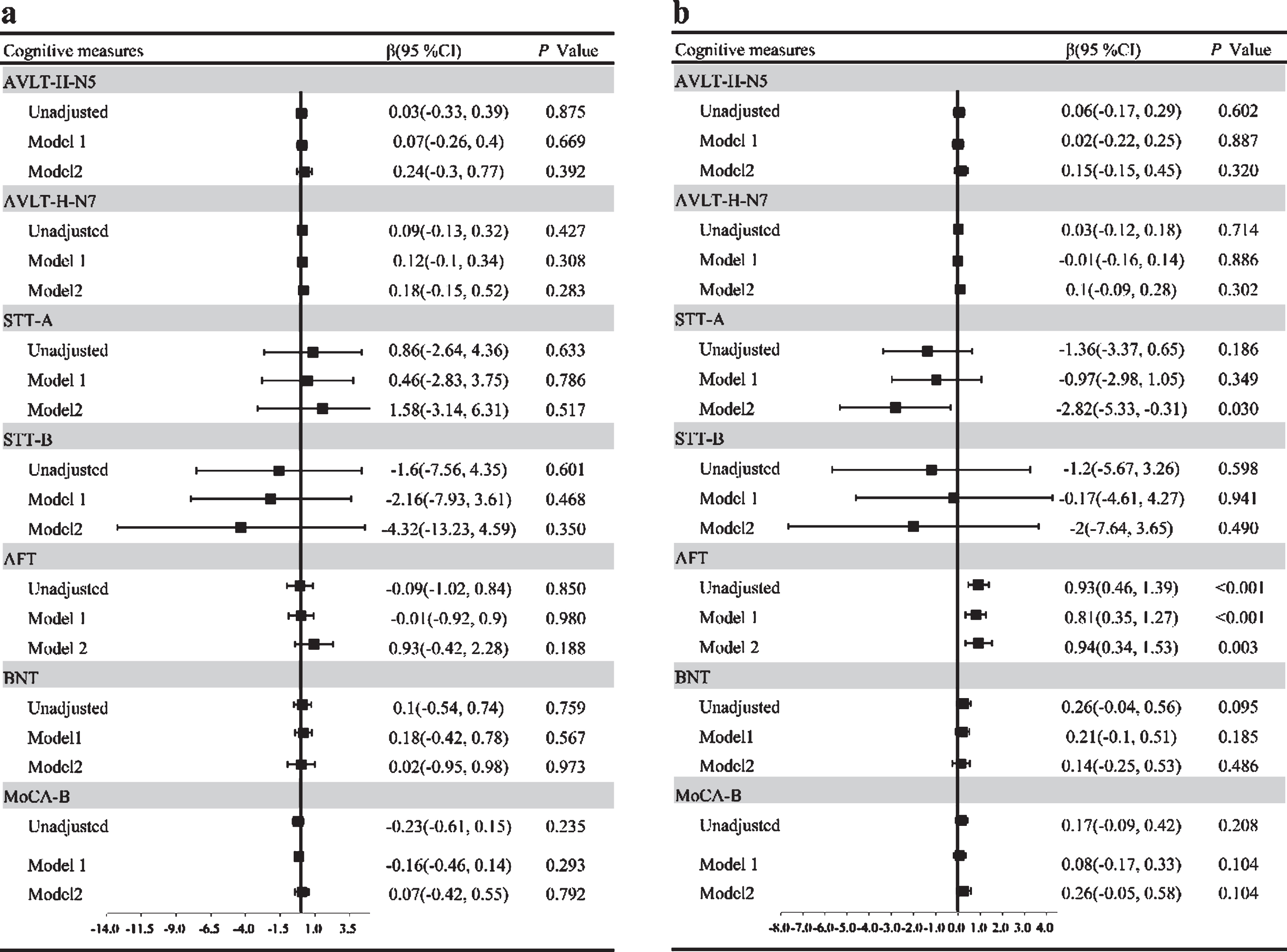
Effect sizes of HC on cognitive measures according to APOE ɛ4 status. a) Effect sizes of HC on cognitive measures in APOE ɛ4 carriers with SCD. b) Effect sizes of HC on cognitive measures in APOE ɛ4 non-carriers with SCD. APOE, Apolipoprotein E; β, partial regression coefficients; CI, confidence interval; AVLT-H-N5, Auditory Verbal Learning Test-Huashan Version for long-delayed free recall (20 min); AVLT-H-N7, Auditory Verbal Learning Test-Huashan Version for long-delayed recognition (20 min); STT-A, Shape Trail Test A; STT-B, Shape Trail Test B; AFT, Verbal Fluency Test (animal); BNT, Boston Naming Test; MoCA-B, Montreal Cognitive Assessment-Basic. Model 1: adjusted for HC or education. Model 2: adjusted for age, gender, HC or education, BMI.
Differences in neuropsychological tests across 4 levels of total reserve
There was a significant positive linear trend in AVLT-H-N5, AVLT-H-N7, AFT, BNT, and MoCA-B with the highest scores for BR+/CR+, followed by BR–/CR+, BR+/CR–, and BR–/CR–(all p for trend < 0.05; Fig. 5). Moreover, we found a negative linear trend in STT-A and STT-B with the highest score for BR–/CR–, followed by BR+/CR–, BR–/CR+, and BR+/CR+(all p for trend <0.05; Fig. 5). Furthermore, no statistical significance was observed in the results of the interaction of BR and CR with neuropsychological tests (all p > 0.05; Supplementary Figure 5 and Supplementary Table 3). However, overall, we observed that subjects with SCD had better cognitive performance with increasing BR and CR, but the contribution of CR was relatively greater (Supplementary Figure 6 and Supplementary Table 4).
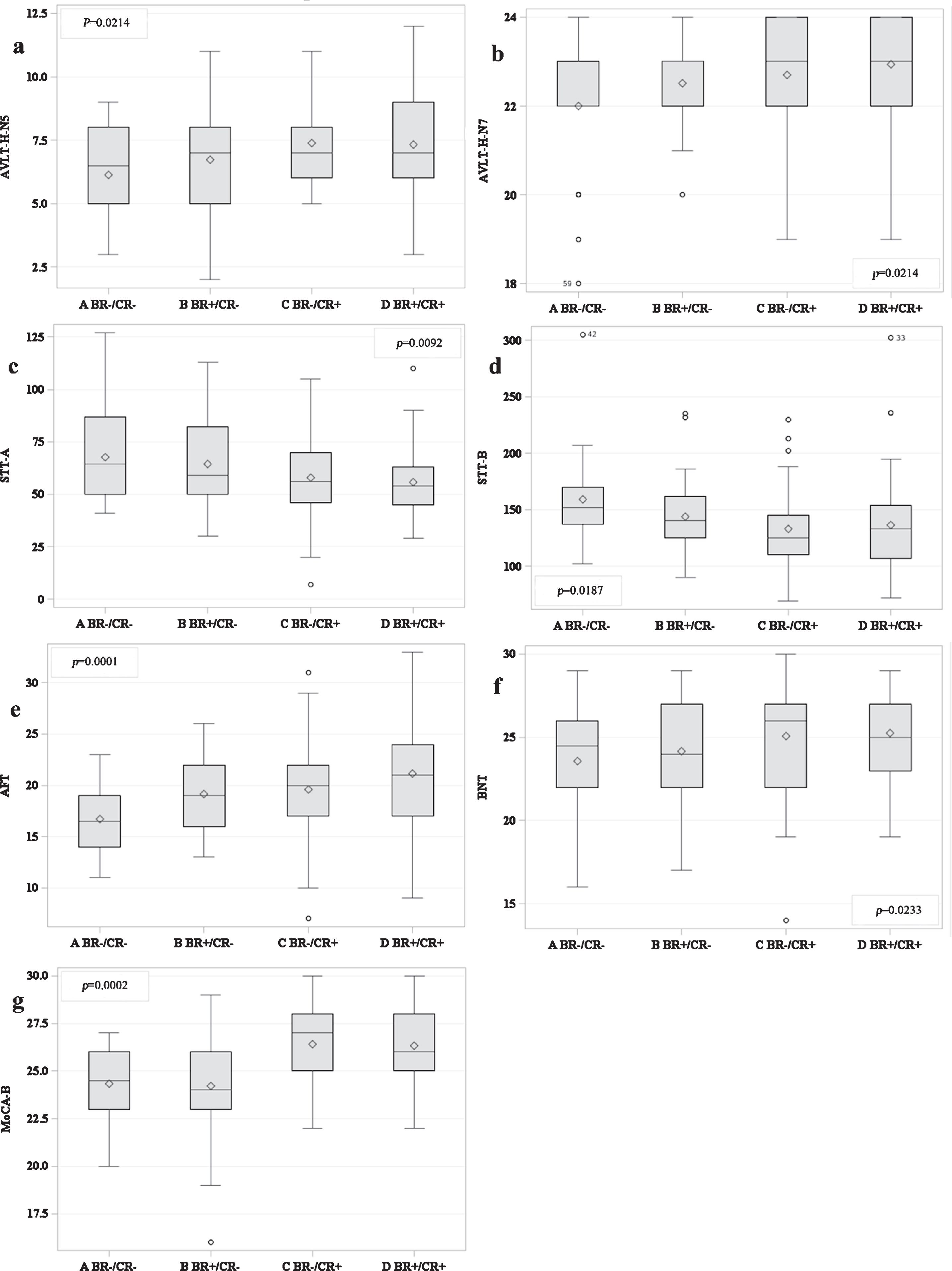
Cognitive performances in all cognitive measures across different levels of reserve. BR–/CR–, low BR and CR; BR+/CR–, high BR and low CR; BR–/CR+, low BR and high CR; BR+/CR+, high BR and CR; AVLT-H-N5, Auditory Verbal Learning Test-Huashan Version for long-delayed free recall (20 min); AVLT-H-N7, Auditory Verbal Learning Test-Huashan Version for long-delayed recognition (20 min); STT-A, Shape Trail Test A; STT-B, Shape Trail Test B; AFT, Verbal Fluency Test (animal); BNT, Boston Naming Test; MoCA-B, Montreal Cognitive Assessment-Basic.
DISCUSSION
In the present study, we investigated the effects of CR and BR on cognitive performance in SCD subjects, and whether there were differences in the effects according to APOE ɛ4 status. The main findings of our study are that 1) although CR and BR both have independent positive effects on cognition in participants with SCD, the effects of CR were generally greater than those of BR, 2) the positive effects of CR on cognition were greater in APOE ɛ4 non-carriers with SCD than in APOE ɛ4 carriers with SCD, 3) the positive effect of BR on cognition was found in APOE ɛ4 non-carriers with SCD but not in APOE ɛ4 carriers with SCD, and 4) subjects with SCD had better cognitive performance on all cognition tests in the BR+/CR+group, followed by in the BR–/CR+, BR+/CR–, and BR–/CR–.
Despite the fact that AD seems to be a very complex disease, increasing evidence has shown that dementia is more similar to cancer, heart disease and diabetes, and people have the potential to reduce their risk of dementia with early intervention [39]. Converging evidence has demonstrated that the prevalence and incidence of dementia have declined or stabilized over recent decades in Western societies, including Sweden, Spain, the UK, the Netherlands, France, and the USA [40]. Although the factors that can fully explain these observed trends have not been identified, some societal changes and improvements could be responsible for a reduced risk of dementia. According to a report issued by the Lancet Commission in 2017 [41], approximately 35% of dementia can be attributed to nine risk factors: less education, midlife hypertension, midlife obesity, hearing loss, late-life depression, diabetes, physical inactivity, smoking, and social isolation. In that report, less education, the second most important risk factor for dementia after hearing loss, was believed to be associated with a relative risk (RR) of dementia of 1.59 (95% CI 1.26–2.01) and was considered to result in less cognitive reserve. However, the available studies indicated that higher levels of CR (as measured by education, IQ, occupational attainment, bilingualism and so on) may reduce the risk of cognitive decline and incident dementia by delaying the onset of symptoms of MCI in healthy elderly individuals [42 –44]. On the other hand, a longitudinal study found that a larger BR (as measured by intracranial volume) offers protection against clinical deterioration in MCI patients [24]. Therefore, our findings are consistent with those of previous studies and expand upon these findings by demonstrating that both CR and BR have beneficial effects in subjects with SCD who are at risk for AD. In addition, we found that although CR seems to play a more important role than BR in SCD, the combination of CR and BR can produce additive effects, which was in line with the results of two previous studies [25, 45]. However, studies have suggested that CR and BR reduce dementia risk by weakening the association between AD pathology and cognition, rather than directly impacting the accumulation of AD pathology [46 –48]. However, the mechanism and neurobiological substrate underlying CR and BR in individuals with SCD is not clear, and we will explore these ideas in the future.
APOE ɛ4, the most prevalent genetic risk factor for AD, increases the risk of developing AD by Aβ-dependent and Aβ-independent mechanisms [49, 50]. Studies have demonstrated that APOE ɛ4 significantly increased the risk of progression to MCI and AD in individuals with SCD [51 –53]. A possible explanation could be that APOE ɛ4 carriers with SCD suffered greater abnormal AD pathology than APOE ɛ4 non-carriers with SCD [54]. According to the concept of reserve in which the protective effects occur in the early stage of AD and disappear beyond a certain threshold [12], APOE ɛ4 may affect the capacity of reserve by aggravating the pathological burden of AD. In this regard, it was reported that in the APOE ɛ4 non-carrier group, there was no difference in cognitive function between BR (as measured by HC) quintiles, while in the APOE ɛ4 carrier group, cognitive function between BR quintiles was significantly different, with the low BR quintile scoring lowest [55]. In addition, greater BR (as measured by HC) could attenuate the negative effect of the APOE ɛ4 on cognitive performance covering the spectrum from normal cognition to dementia [38]. Additionally, higher CR (as defined by bilingualism) can still play a strong protective factor in MCI patients with multiple risk factors such as APOE ɛ4, older age, and AD biomarkers [56]. The protective effects of CR on cognition are greater than those of BR in the early stage of AD [25]. Therefore, these findings may explain our results that CR has beneficial effects on cognition in both APOE ɛ4 carriers with SCD and APOE ɛ4 non-carriers with SCD, but the effect of BR on cognition was found in APOE ɛ4 non-carriers with SCD but not in APOE ɛ4 carriers with SCD. However, this requires molecular imaging research for further confirmation.
The advantages of this research are that we comprehensively investigated the effects of both CR and BR on cognition in subjects with SCD and examined differences in effects according to APOE ɛ4 status. Nonetheless, there are also some limitations in this study. First, this was a cross-sectional study and follow-up data are needed to verify whether CR and BR have a protective effect against the progression of cognitive decline in SCD populations. Second, insufficient sample size may affect the accuracy and repeatability of the results. Third, using HC to measure BR in this study may have been a relatively crude approach. It would be more appropriate to employ neuroimaging feature such as intracranial volume. Finally, exploring the mechanism and neurobiological substrate underlying CR and BR in subjects with SCD is critical for preventing AD. It is essential to include multimodal neuroimaging data such as MRI, Aβ-PET, and FDG-PET to capture the neural substrates of reserve in individuals with SCD.
Our results suggest that both CR and BR have the potential to delay or slow down cognitive decline in individuals with SCD, even for APOE ɛ4 carriers with SCD. Therefore, increasing educational opportunities and improving maternity and child health care could increase CR or BR in the population, which in turn may help protect against the effects of AD. It is of great significance to prevent AD due to the disappointing effects of anti-amyloid therapies in the last two decades.
Footnotes
ACKNOWLEDGMENTS
This article was supported by The National Key Research and Development Program of China (2016YFC1306300, 2018YFC1312001), National Natural Science Foundation of China (61633018, 81801052, 81601454), Beijing Municipal Commission of Health and Family Planning (PXM2020_026283_000002), and China Postdoctoral Science Foundation (2018M641414).