
Abstract
Background
There is a growing interest in dementia prevention and scalable cognitive enhancement strategies for individuals at-risk, with or without Alzheimer's disease. Board games have shown potential cognitive and mood benefits, but randomized controlled evidence remains limited and heterogeneous.
Objective
We aimed at assessing whether chess and/or Go could improve cognition, mood, and quality of life in individuals with mild cognitive impairment (MCI) and subjective cognitive decline (SCD).
Methods
Individuals with MCI or SCD aged ≥55 years were randomized to one of three arms: chess, Go (each consisting of 12 weekly group sessions), or a waitlist control group. Montreal Cognitive Assessment, digit span, trail making test, categorical fluency, Geriatric Depression Scale, and the World Health Organization Quality of Life scale were administered at baseline and follow-up. We also updated our previously published meta-analysis including these new results.
Results
69 subjects completed the study. Categorical fluency improved significantly in the games groups (p < 0.05). No between-group differences were found in overall cognition. A significant group × diagnosis × time interaction showed improved quality of life in MCI participants in the games groups (p = 0.002). A group × gender × time interaction revealed reduced depression in females in the games groups (p = 0.013). The updated meta-analysis confirmed a significant effect on depression (standardized mean differences −0.48, p = 0.013), but not on cognition.
Conclusions
The improvements in mood and quality of life, particularly among females and MCI subjects, underscore the psychological value of board games interventions, possibly through their social component. These activities may foster emotional well-being in older adults at risk for Alzheimer's disease, even without cognitive benefits.
Introduction
Dementia has an enormous impact, both socially and economically. 1 Disease-modifying drugs seem to slow progression in Alzheimer's disease, but their large-scale adoption is hindered by the limited number of eligible patients, the side effects and costs.2–5 Therefore, it is imperative to find strategies to reduce the risk of dementia since the early phases of cognitive impairment, i.e., mild cognitive impairment (MCI) and subjective cognitive decline (SCD).
People living with MCI are usually evaluated in the memory clinics, while for people with SCD a new type of service has been envisioned, specifically dedicated to dementia risk assessment and reduction. These so-called Brain Health Services (BHS) are currently run across Europe with pilot experiences.6,7 A theoretical pillar of BHS is cognitive enhancement, for which new evidence needs to be gathered before being fully implemented. 8 Ideal cognitive interventions should increase the cognitive reserve of individuals, slow cognitive deterioration, improve quality of life, and be easily implementable, culturally acceptable and sustainable. 9 Among these, leisure activities (including reading, gardening, board games, crosswords, etc.) are especially interesting, since they are widespread and associated to a reduced incidence of dementia in population studies, 10 although reverse causality cannot be ruled out.
Humans have been playing board games for millennia. Historically, these use pieces or “men” to recreate battles, races or hunts. Board games may be broadly divided into games of skills and games of chance, with some falling in between these categories. 11 Games of skills may be very complicated; among these, chess is especially widespread in the Western world, while Go is more frequent in the Eastern society (i-Go in Japan, Weiqi in China, Baduk in South Korea). A number of works has elucidated neural correlates of board games skills, such as precuneus, a well-known epicenter of neurodegenerative disease in Alzheimer's disease.12–15 Moreover, board games typically entail a social component, which in a study on Go has been showed to contribute to the cognitive effect of the intervention. 16
We recently published a meta-analysis on board games and cognition in subject at-risk or affected by cognitive impairment, with benefits extending to quality of life and depression. 17 However, the included studies are small and heterogeneous in terms of inclusion criteria and outcomes and limited to just one game. It is therefore difficult to compare results. The interventions generally last 3–4 months and consist of weekly classes adapted to the cognitive level of the participants, who were usually not familiar with the rules.
In order to elucidate the role of different board games in cognitive enhancement, we performed the CogniChess study, specifically targeting subjects in the earliest phases of cognitive decline, i.e., MCI and SCD. The main aim of the study was to evaluate whether a board games intervention could result in cognitive benefits. Secondary aims included the effect of board games on quality of life and depression.
Methods
Subject selection and procedures
Following ethical committee approval, we planned to enroll 80 subjects affected by MCI or SCD. Subjects were selected among outpatients visiting our Center for Dementia and Cognitive Decline (CDCD) or BHS6,18 at Fondazione IRCCS San Gerardo dei Tintori, Monza.
The original protocol (Clinicaltrials.gov: NCT06281652) included four groups: controls, chess, Go, chess + Go. The chess group had to attend a total of 12 classes, once weekly, at Scacchi 2000, Lissone, Italy. The Go group attended the same number of classes at La Casa dei Giochi, Milan. The combined chess + Go group had to attend a total of 24 classes, with one weekly class of chess and one weekly class of Go, over 12 weeks. However, it became quickly clear at randomization that participants were not willing to attend the combined group due to various reasons. Therefore, the combined group was suppressed, and participants were again randomized to one of the three remaining groups. For each class, a maximum of 10 participants was allowed. Study partner participation was encouraged.
Inclusion criteria were the following: (a) Diagnosis of MCI 19 or SCD; 20 (b) CDR < 1; (c) Age > 55 years; (d) Interest for the proposed activities and willingness to participate in the study; (e) Driving license or availability of a study partner who could drive the participant to the study locations; (f) Living within 20 min by car from the study locations; (g) Signed informed consent.
Exclusion criteria were: (a) Significant sensory or linguistic deficits; (b) Significant behavioral or psychiatric disorders; (c) Significant medical condition that could make attendance difficult; (d) Impossibility to attend classes in the evening.
Participants could not be assigned to a game if they already knew how to play; however, in case they were familiar with one game, they could be randomized to the other game or to the control groups. If a participant lived within 20 min from a location, but more than 20 min from the other, they could be randomized to either the first intervention or controls.
Subjects were randomized with a minimization procedure considering three variables: age (>70 years), gender, diagnosis (MCI versus SCD). The raters were blinded to the randomization process and to the group allocation of the subjects. At baseline, participants were evaluated with the Montreal Cognitive Assessment (MoCA), digit span forward (DSF) and backward (DSB), 21 Trail making test (TMT-A and TMT-B), 22 and categorical fluency (CF). 23 They were also administered the Cognitive Reserve Index questionnaire (CRIq), 24 Geriatric Depression Scale (GDS), and World Health Organization Quality of Life (WHO-QoL) bref (https://www.who.int/tools/whoqol/whoqol-bref). A comprehensive neuropsychological evaluation was not performed; the specific tests and questionnaires were chosen based on what previously done to allow comparability with the published studies on the topic. All tests and scales except for CRIq were repeated at follow-up.
Sample size calculation and statistical analysis
Sample size was determined based on a t-test to compare MoCA scores between controls and the combined games groups, with alpha = 0.05 and 1 – beta = 0.90, estimating an effect size of 1.1, conservatively lowered from the effect size of 1.8 found in our meta-analysis, given the considerable heterogeneity across previous studies (albeit all were in the same direction). 17 A total of 36 subjects was computed with the software G-power. 25 Anticipating a drop-out rate of 10%, 40 subjects would be needed, i.e., 20 controls and 20 games. Since the study intended to elucidate differences between games, we extended the sample size to 20 per each group, for a planned total of 80 subjects. However, since a group was dropped, the subjects were redistributed among groups.
We computed a cognitive z-score across all cognitive tests (inverting the sign of trail making tests to allow comparability) at baseline and applied that scaling to cognitive tests at follow-up, to evaluate the longitudinal change. We also computed a total digit span score (digit span forward + digit span backwards, DS - total) and a trail making test score (TMT-B – TMT-A). WHO-QoL bref scores were scaled and averaged to obtain a composite WHO-QoL z-score (simply indicated as WHO-QoL).
Baseline differences and differences in variables changes among groups (controls versus games) were computed with t-test or Mann-Whitney test following Shapiro-Wilk test. Differences among the three groups (controls versus chess versus Go) were evaluated with ANOVA or Kruskal-Wallis test following normality check; if the test was significant, Tukey post-hoc test was run for pairwise comparisons. Intra-group pre-post intervention differences were computed with paired t-test or Wilcoxon test following Shapiro-Wilk test. p-values were adjusted with False Discovery Rate (FDR) correction. Two sets of linear mixed-effect models were run for each scaled variable with the interaction group*gender*timepoint and the interaction group*diagnosis*timepoint as predictors. Sensitivity analyses were run using the residuals corrected for age and education or CRIq.
Analyses were conducted exclusively on participants who completed the study, using a per-protocol approach, after verifying that there were no significant differences on baseline variables between participants who dropped out and those who completed the study by means of t-test or Mann-Whitney test following Shapiro-Wilk test. Finally, we updated our previous published meta-analyses on traditional board games and cognitive impairment, 17 using the same methodology. In brief, we conducted electronic searches for eligible studies within each of the following databases, since January 1, 2023, up to September 28, 2025: Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE (accessed via PubMed), Embase, Scopus, and Web of Science. Records were identified with tailored search strings for each database (the same used in our previous work), that can be found in the Supplemental Material. Citations identified from the literature searches were imported to Mendeley and duplicates were automatically removed by the software. Then, two reviewers (FEP and LT) independently screened the titles and abstracts of all the records to match the inclusion criteria. A consensus was reached through discussion in case of disagreements. The full texts of all eligible studies, reviews, and meta-analyses were retrieved, and their reference lists were checked.
The inclusion criteria included cohort studies and randomized and non-randomized controlled trials in English, on traditional abstract board games and cognitive impairment, enrolling at least 10 elderly patients (age >60 as per WHO standards), with or without cognitive impairment, or on patients with cognitive impairment irrespective of age, with at least one cognitive outcome.
Studies on newly developed ad hoc board games, cards, or other kinds of games, in which the effect of board games was not analyzed separately from other kinds of games, or without a control group were excluded.
As no new study satisfying inclusion criteria could be added to our previous work, we just added our own Cognichess trial results to the meta-analysis. We refer the reader to our previous publication for risk of bias assessment. 17
For each outcome, we calculated the distributions of changes for intervention and controls with the following formulas:

We computed standardized mean differences (SMD) with a random-effect model. τ2 and I2 were calculated as measures of heterogeneity. To check for publication bias, funnel plots were visually inspected, and the Egger test was performed.
The analyses were performed with the software R (https://www.r-project.org/).
Results
Baseline characteristics
Due to time constraints, we were able to recruit only 75 patients during the study period during the enrollment phase. Of these, 6 (8%) dropped out during the classes (i.e., did not attend beyond the first lesson, or were lost to follow-up due to personal issues). There were no significant differences between subjects who dropped out and subjects who completed the study. The complete flowchart of the study is presented in Figure 1.
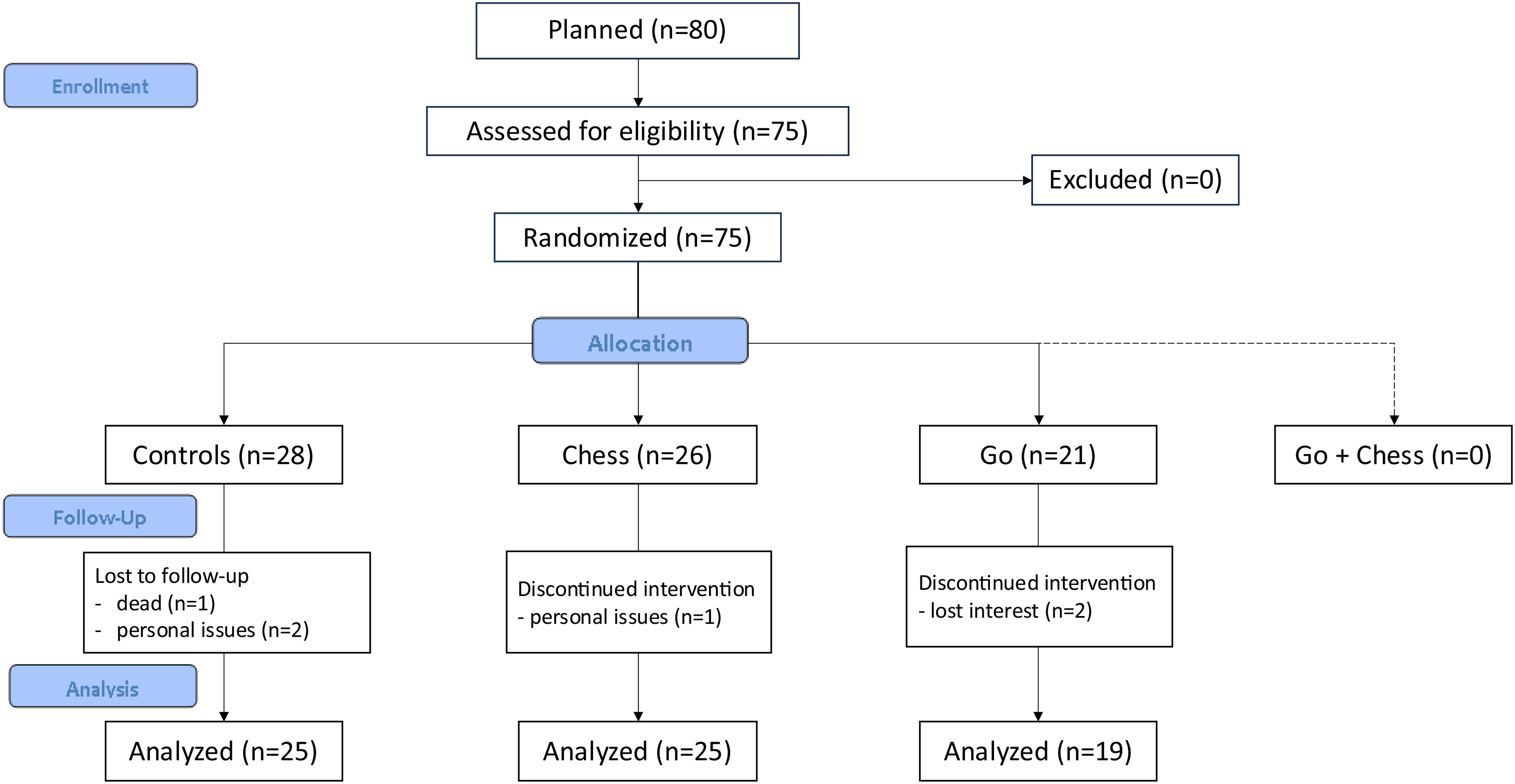
Flowchart of the study.
The mean age of the participants was 71.6 ± 6.5 years, with 32 females (46.3%). Mean education was 11.5 ± 4.5 years, and mean CRIq was 109.7 ± 19.7, corresponding to a medium level of cognitive reserve. A third of the participants were diagnosed with MCI (n = 22, 31.9%). Among those randomized to the games, mean attendance was 9.4 ± 3.8 classes, and a study partner was present in half of the cases (n = 22, 50%). No significant differences at baseline variables were noted between controls and games, or among groups. Baseline data are summarized in Supplemental Table 1.
Cognitive and affective measures
All three groups improved on the categorical fluency test from baseline to follow-up. The whole games group improved on TMT-A (the chess group in particular) and MoCA; the chess group also improved on the cognitive z score. A trend for an improvement in MoCA was noted for the Go group. After FDR correction, the only significant improvement was for the categorical fluency for the games group (p < 0.05). The differences from baseline to follow-up are shown in Table 1 and Supplemental Table 2.
Intra-group differences between at baseline and 3 months.
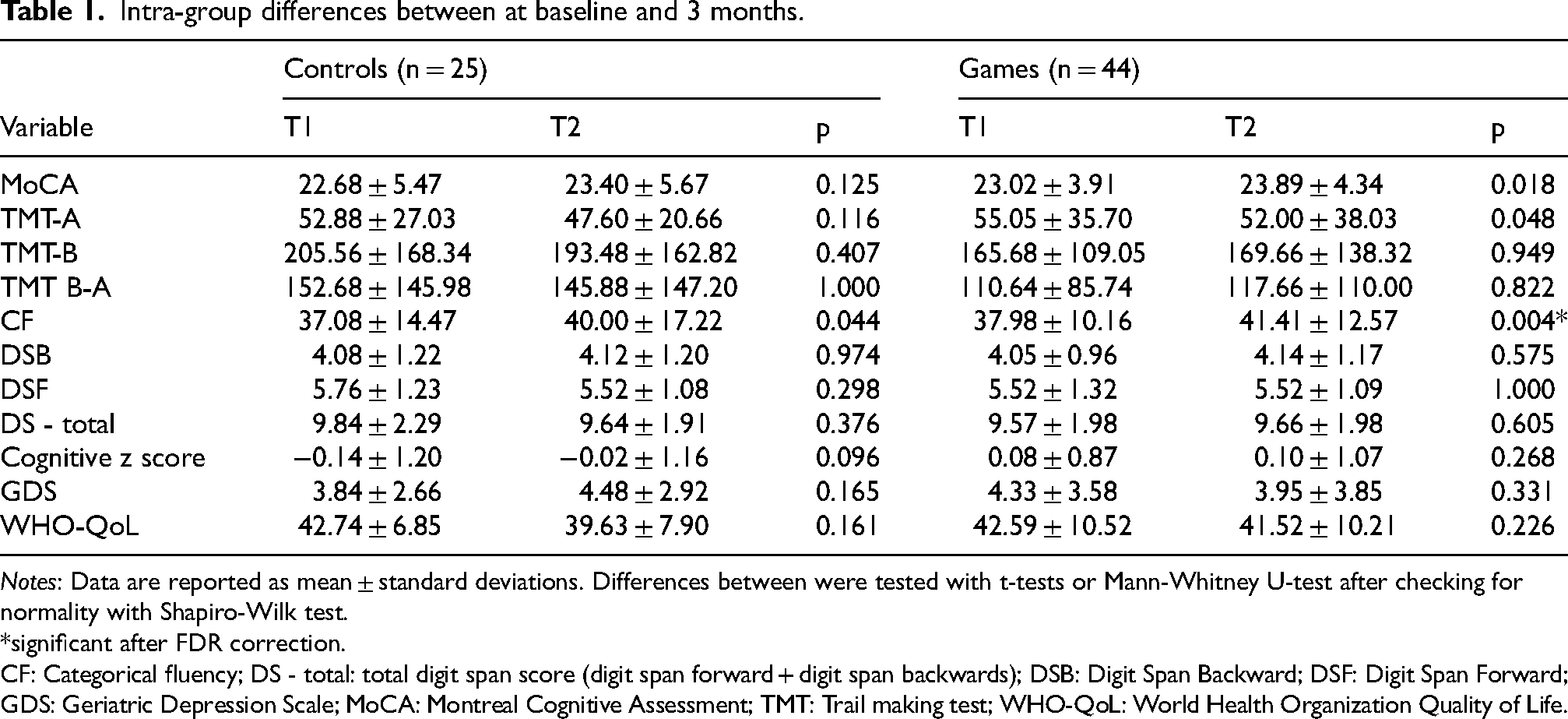
Notes: Data are reported as mean ± standard deviations. Differences between were tested with t-tests or Mann-Whitney U-test after checking for normality with Shapiro-Wilk test.
*significant after FDR correction.
CF: Categorical fluency; DS - total: total digit span score (digit span forward + digit span backwards); DSB: Digit Span Backward; DSF: Digit Span Forward; GDS: Geriatric Depression Scale; MoCA: Montreal Cognitive Assessment; TMT: Trail making test; WHO-QoL: World Health Organization Quality of Life.
Groups did not significantly differ in mean change from baseline to follow-up in any test or questionnaire. The data are shown in Supplemental Table 3. The cognitive z-score distributions at baseline and follow-up across the three groups are shown in Supplemental Figure 1.
Linear mixed-effect models
Linear mixed-effect models with diagnosis, time and group revealed a significant positive main effect of time on categorical fluency, and a significant negative main effect of time on DSF and DS – total. This main effect was not confirmed in the models with gender, time and group.
As expected, a significant negative effect of the diagnosis of MCI was noted for MoCA, DSF, DS – total, the cognitive z score, and a significant positive effect of MCI diagnosis was noted for TMT-B.
In the models with diagnosis, the interaction group×diagnosis was significant for the WHO-QoL (with a negative coefficient). The interaction time×diagnosis was significant for the WHO-QoL, categorical fluency (negative coefficients), DSB and DS – total (positive coefficients). The interaction group×diagnosis×time was significant for the WHO-QoL with a positive coefficient, with MCI patients assigned to the games group performing better over time compared to other subgroups.
In the models with gender, the interaction group×diagnosis was again significant for the WHO-QoL (but with a positive coefficient). The interaction time×gender was nearly significant for the WHO-QoL and categorical fluency (with a positive coefficient). Finally, the interaction group×gender×time was significant for GDS with a negative coefficient, with female subjects assigned to the games group showing less depression at follow-up. Marginal predictions revealed a drop of 1.25 points on GDS for females in the games group. A trend for a negative interaction was noted on CF and WHO-QoL, with an inverse trend for males×group over time (controls worsening, games stable). Sensitivity analyses correcting the cognitive tests for age and education or CRIq did not change these associations (data not shown).
The full models are shown in Supplemental Tables 4 and 5, while the spaghetti plots for GDS and WHO-QoL are shown in Figures 2 and 3. The marginal predictions according timepoint, gender, diagnosis and group for GDS and WHO-QoL are presented in Supplemental Tables 6–8.
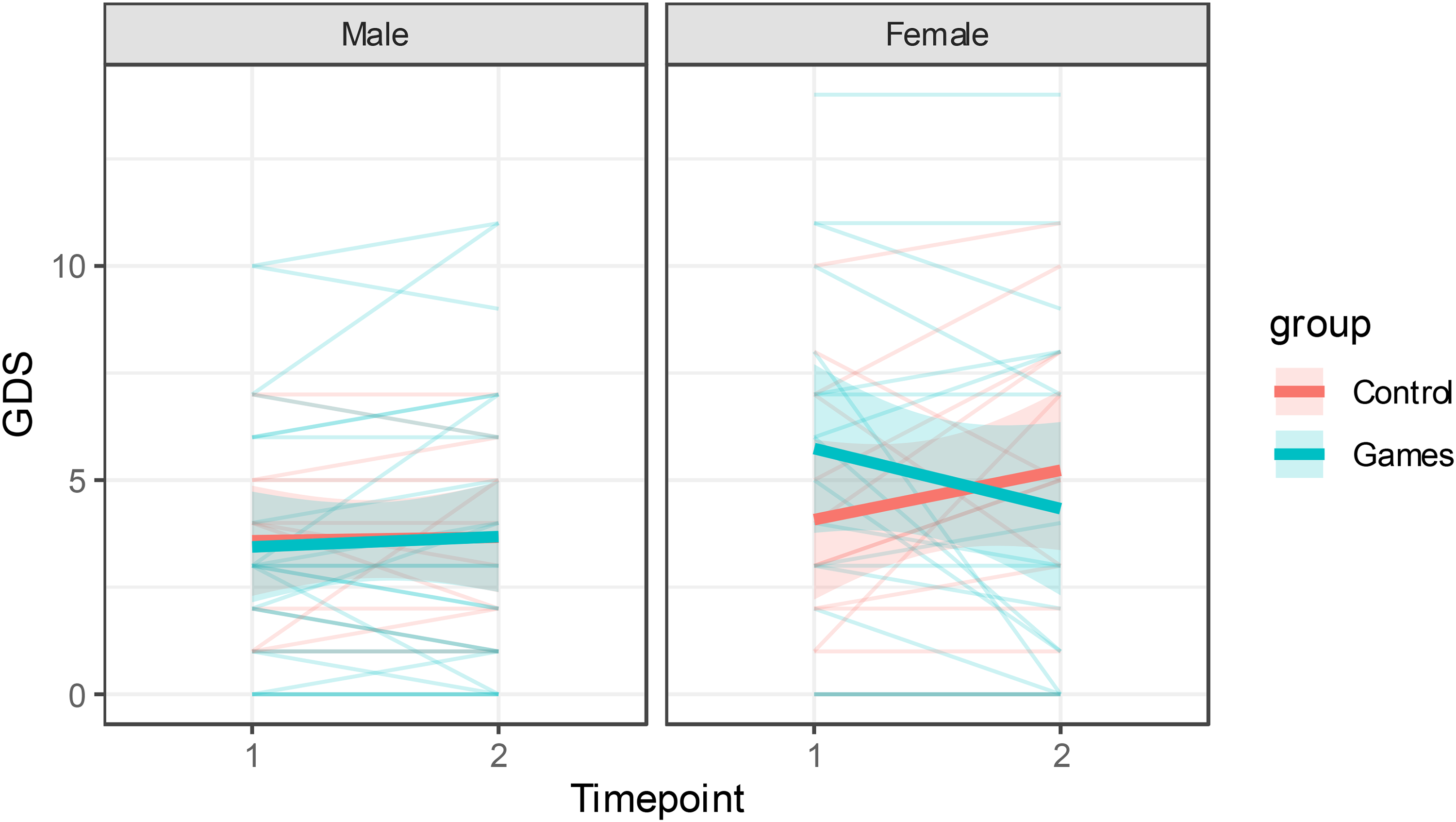
Effect of gender on change in GDS from baseline (timepoint 1) to follow-up (timepoint 2).
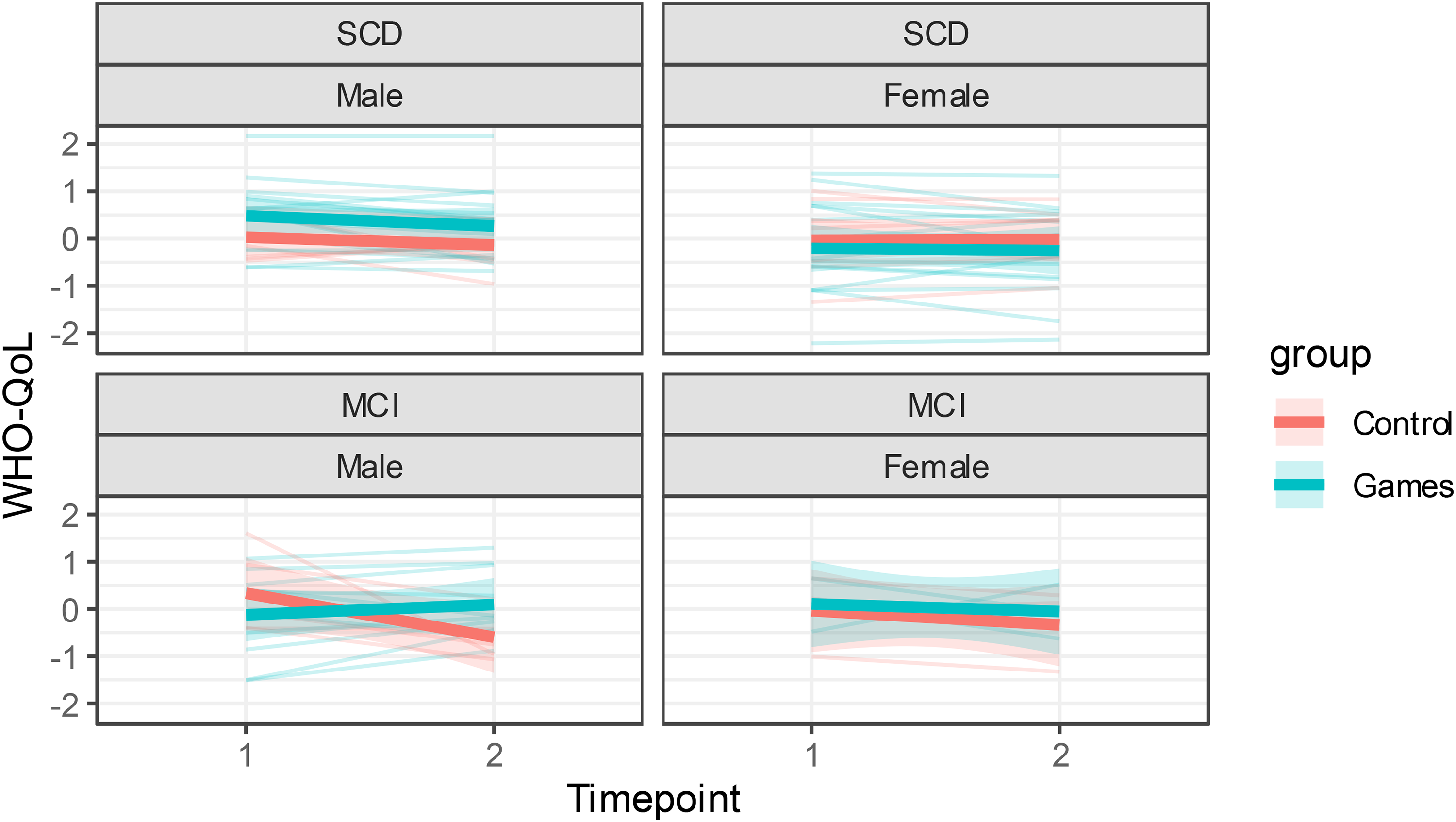
Effect of diagnosis and gender on change in WHO-QoL z-score from baseline (timepoint 1) to follow-up (timepoint 2).
Meta-analysis
We performed again the same meta-analyses in our previous work. 17 As no new study satisfying inclusion criteria could be found, we were only able to add the results of the Cognichess trial to our previous meta-analysis. The results are shown in Supplemental Table 9. In the context of a general trend favoring board games on all tests, the only significant result was noted for GDS (SMD −0.48, p = 0.013). Egger test excludes a publication bias, and the heterogeneity is null, with all three studies going in the same direction. Importantly, our updated meta-analysis does not confirm the cognitive benefits of the interventions found in our previous work. The forest plot for this meta-analysis is shown in Figure 4.
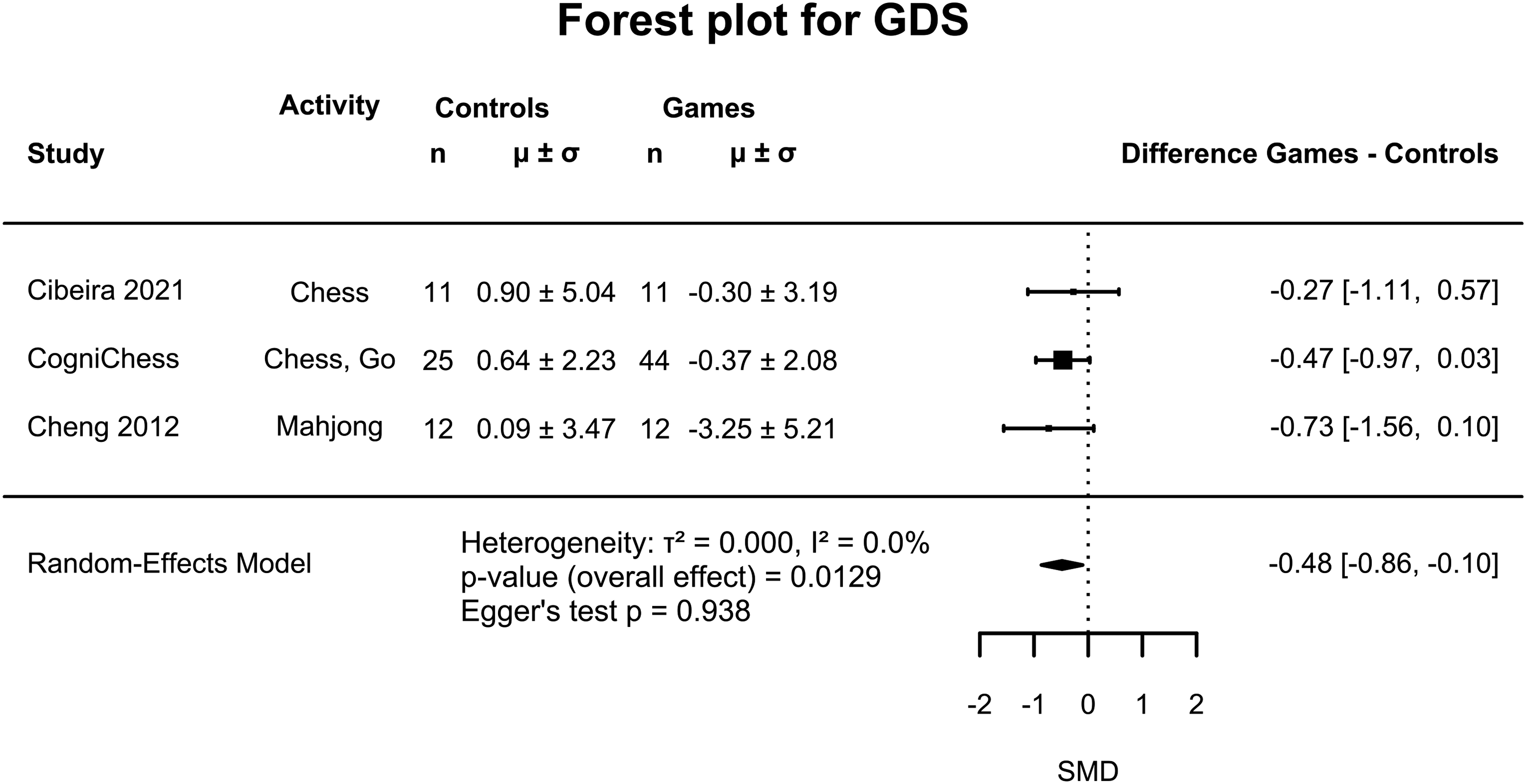
Forest plot for the meta-analysis of GDS differences from baseline to follow-up.
Discussion
Few randomized controlled trials have been performed on traditional board games for prevention of dementia or cognitive enhancement. In our previous meta-analysis, we found these studies to be small and heterogeneous; nevertheless, they showed an improvement in global cognition, attention, depression and quality of life. 17 Our trial is the first Italian study to investigate cognitive and affective effects of a 3-months intervention with weekly classes of chess and Go in subjects with SCD and MCI. A number of conclusions can be drawn from our results. First, the intervention is feasible and well accepted, with high attendance and few drop-outs. Second, no cognitive effect was noted, besides an improvement on verbal fluency in the games group. Third, exploratory analyses revealed that traditional board games might have complex positive effects on depression and quality of life, mediated by gender and cognitive status.
Only 6 subjects dropped out during the trial, half of them in the games groups, resulting in a drop-out rate of 6% in the active arms. This is substantially lower of the 10% anticipated from the literature, and markedly below the two studies on chess (25%).26,27 Go studies showed more variable drop-outs rates (0–30%).16,28,29 Attendance exceeded 75% on average and was higher in the Go group compared to the chess group, despite a lower presence of study partners, showing that even though this oriental game is less known in Italy, it was nevertheless appreciated. Notably, our study is the first randomized controlled trial on Go conducted in a Western country. However, we had to eliminate the combined chess + Go group due to the impossibility of participants to attend classes twice per week. Since the participants had to reach the places in which they had classes on their own, and these were relatively far from each other, this could reflect the specific challenges associated with the logistics of the study. Nevertheless, it could also be an indication that an intervention more intensive than once per week could be difficult to implement. Conversely, we offered the participants the possibility to attend the following cycle of classes of their liking at the end of each study, and many of them continued, suggesting that a longer, rather than more intensive intervention could be also feasible. However, our study is in line with the literature, in which board games classes went on for 3–4 months on average. 17
Contrary to our previous meta-analysis, 17 we could not find any significant between-group difference in terms of cognition. The games group significantly improved on categorical fluency from baseline to follow-up, but this was not different from the quite unexpected improvement in the control group. A few explanation could explain the discrepancy in the cognitive findings. First, studies reporting an effect on cognition were rather small; for MoCA, the total contribution of studies on Go and chess was of 20 subjects in the active group and 19 controls,27,29 fewer than our figures. The largest effect size (MD 4.80) was found in a non-randomized controlled trial, and both studies had a moderate risk of bias. 27 Second, the improvement in both groups on categorical fluency seen in our study suggest a practice effect, rather than a true result of the intervention. Third, our study dealt with a different population, comprising MCI and SCD subjects, while previous studies enrolled either cognitively unimpaired elderly subjects,16,26,30 or persons with dementia.27–29,31–34 Only one work included also MCI subjects, but the intervention was with mahjong. 34 It is possible that benefits on cognition vary depending on participants cognitive status. Nevertheless, our updated meta-analysis showed trends for better cognitive outcomes in the games group, although with high heterogeneity.
Our study showed a trend towards improvement on GDS in the games group compared to controls. By combining our results with those of Cibeira and Cheng27,32 the pooled effect became significant, with a moderate effect size (SMD −0.48). This shows that board games can indeed improve mood, possibly through their inherent social component. In our study, this effect was more pronounced in females, with a mean reduction of 1.3 points on GDS in the games group in an exploratory analysis. This is consistent with a recent meta-analysis showing a higher risk of depression in older women experiencing social isolation. 35 Depression is a recognized risk factor for dementia, included in the latest report of the Lancet Commission. 36 Socialization could also reduce the risk of dementia by increasing cognitive reserve and mitigating the impact of neuropathology in the brain. 37 Therefore, even in the absence of clear cognitive benefits, improving depressive symptoms through board games intervention could represent a valuable intervention in at-risk individuals.
Quality of life did not show significant improvement in the games group compared to controls, neither in the whole sample nor on the updated meta-analysis. Albeit exploratory, the three-way interaction on the linear mixed-effect model revealed a significant improvement in MCI subjects. This is in line with previous evidence, showing that cognitive intervention may improve quality of life in older adults with MCI, although with high heterogeneity.38,39 The underlying mechanisms or moderators remain unclear, but loneliness may mediate the relationship between depression and quality of life in older adults with MCI. 40 While our sample size precluded testing this hypothesis, it is plausible that the social engagement plays a role also in this case.
Our study has some limitations. First, we had to cancel the combined group, preventing assessment of potential synergistic effects. Second, a comprehensive neuropsychological evaluation was not performed; the tests were chosen based on what previously done to allow comparability with the published studies on the topic. This limits coverage of certain cognitive domains, such as visuo-spatial abilities, which are known to be enhanced in both chess and Go players.41–44 Third, the sample was heterogeneous, comprising both SCD and MCI subjects. While this offers the possibility to study differential effects based on cognitive status, complex interactions may have arisen from the intermingle of individuals with different baseline abilities in the context of the classes. One possibility is that the need to compromise could have resulted in a lower-than-effective stimulation for SCD subjects, and in an excessively difficult program for MCI individuals. A special attention was given to this topic, and in forming groups after randomization we tried to put people with the similar cognitive status together. Fourth, we lacked biomarker data. Response to the intervention could theoretically be different in subjects with early AD and no neurodegeneration. Indeed, biomarkers may have also partially explained differences between SCD and MCI subjects, as a higher prevalence of AD in the latter group is expected in clinical cohorts. 45 Fifth, although our sample was larger than most prior studies, it remains modest, reducing statistical power for detecting small or interaction effects (e.g., gender × diagnosis × time). Unfortunately, feasibility constraints prevented further recruitment. Lastly, our power analysis was based on a pooled effect size from a previous meta-analysis that showed considerable heterogeneity (I2 = 75%). Although all included studies pointed in the same direction, the magnitude of the effect varied substantially. To account for this uncertainty, we adopted a more conservative effect size assumption when calculating our sample size. All this considered, subgroup analyses should be interpreted as exploratory, given the limited number of observations per predictor and the reduced power to detect interaction effects.
Nevertheless, our study also has strengths. First, the rigorous design and conservative power analysis, grounded in our previous meta-analysis, supports the reliability of our findings. In contrast, other studies reporting positive outcomes with large effect sizes have often relied on extremely small samples. Second, we compared the effects of two different games and found no significant differences, suggesting that both can be considered as potential interventions. This finding broadens the range of options for enhancing well-being and reducing depression in older adults with SCD or MCI; unfortunately, it does not provide evidence that traditional board games may enhance cognition. Finally, the update of our meta-analysis contextualizes our results, providing robust conclusions that can guide future research and practice.
Conclusion
Traditional board games do not seem to improve cognition. Exploratory and meta-analysis revealed consistent improvements in mood and quality of life, particularly among females and MCI subjects, underscoring the psychological value of board games interventions, possibly influenced by their social component. High attendance and low dropout rates confirm the feasibility and acceptability of these interventions. These activities may foster emotional well-being in older adults at risk of dementia, even in the absence of cognitive benefits.
Supplemental Material
sj-docx-1-alz-10.1177_13872877251401481 - Supplemental material for Cognitive and social intervention with Go and chess in early and subjective cognitive decline: The COGniChESs study results, with an updated meta-analysis
Supplemental material, sj-docx-1-alz-10.1177_13872877251401481 for Cognitive and social intervention with Go and chess in early and subjective cognitive decline: The COGniChESs study results, with an updated meta-analysis by Federico Emanuele Pozzi, Alessandro Spanio, Francesco Gallo, Giovanni Isgrò, Giulia Remoli, Andrea Magi, Elena Moscatelli, Emilia Crisci, Giulia Negro, Ildebrando Appollonio, Carlo Ferrarese and Lucio Tremolizzo in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
The authors would like to thank the teaching team at ASD Scacchi2000 – Accademia Scacchi Lissone, Lissone (Mauro Palma, Andrea Lombardo, Matthieu Dambrain, Antonio Digiovinazzo, Giorgio Favarato, Giovanni Lo Pinto) and at La Casa dei Giochi, Milan (Gionata Soletti) for their dedication to the project.
Ethical considerations
Ethical approval was obtained by Comitato Etico Territoriale Lombardia 3 (protocol CogniChess) prior to the beginning of the study. All procedures have been conducted in compliance with the Declaration of Helsinki of 1964.
Consent to participate
All subjects signed informed consent before randomization.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was produced with the co-funding European Union – Next Generation EU, in the context of The National Recovery and Resilience Plan, Investment Partenariato Esteso PE8 “Conseguenze e sfide dell’invecchiamento”, Project Age-It (Ageing Well in an Ageing Society). Italian MUR Dipartimenti di Eccellenza 2023–2027 (l. 232/2016, art. 1, commi 314–337).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data of this manuscript are available upon request to the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.