
Abstract
Background
Predementia, encompassing subjective cognitive decline (SCD) and mild cognitive impairment (MCI), represents an early phase of neurodegeneration with a heightened risk of progression to dementia. This stage offers a critical window for intervention. Virtual reality (VR) enhances neuroplasticity in predementia via multisensory stimulation, addressing research gaps.
Objective
To assess the impact of VR-based interventions on cognitive abilities, emotional well-being, and instrumental activities of daily living (IADL) in individuals with predementia conditions.
Methods
A search of seven databases identified studies involving seniors aged ≥65 with SCD or MCI. Eligible studies compared conventional cognitive training or usual care as controls. Quality was assessed using the Cochrane Risk of Bias Tool, and evidence certainty was graded using the GRADE framework.
Results
Twelve randomized controlled trials were included. The meta-analysis revealed that, in comparison to control groups, VR-based cognitive interventions had superior effects on subjective cognitive complaints (SMD = −4.06, 95% CI [−4.86, −3.25]), learning and memory (SMD = 0.41, 95% CI [0.02, 0.80]), working memory (SMD = −0.06, 95% CI [−0.08, −0.03]), verbal fluency (SMD = 0.49, 95% CI [0.03, 0.94]), spatial cognition (SMD = 1.43, 95% CI [0.77, 2.10]), and IADL (SMD = 0.77, 95% CI [0.14, 1.40]).
Conclusions
VR-based cognitive interventions could improve objective cognitive performance, subjective cognitive complaints, and IADL in predementia. Future research should prioritize optimizing the intervention protocols and enhancing the geriatric-specific VR-based cognitive intervention.
Keywords
Introduction
As a chronic neurodegenerative syndrome, dementia manifests through the progressive decline in multiple domains of mental capacity, impacting an estimated 57 million individuals globally. 1 This neurodegenerative spectrum comprises multiple etiological categories, such as Alzheimer's disease (AD), cognitive decline associated with Lewy bodies, 2 cerebrovascular dementia, frontotemporal lobar degeneration, and Parkinson's disease. 3 These clinically defined entities demonstrate heterogeneous neuropathological signatures, ranging from amyloid plaque deposition to α-synuclein aggregation and cerebrovascular lesions. Within this nosological framework, AD emerges as the predominant subtype, constituting an estimated 60–80% of clinically diagnosed dementia instances based on contemporary epidemiological data. 4 Prodromal dementia, also known as the predementia phase, refers to the transitional stage characterized by subtle but measurable cognitive decline that does not yet meet the full diagnostic criteria for dementia. This stage encompasses clinical entities such as subjective cognitive decline (SCD) and mild cognitive impairment (MCI), which are increasingly recognized as the earliest measurable symptomatic manifestations of neurodegeneration. Although diagnostically distinct, SCD and MCI are increasingly regarded as stages along the prodromal continuum of AD, supported by longitudinal evidence demonstrating elevated risks of progression to dementia in both populations.5,6 Specifically, MCI is regarded as a state of high risk, with annual progression rates to dementia ranging from approximately 10% to 15% among individuals diagnosed with this condition. 7 Previous studies have demonstrated that these transitional phases represent a critical therapeutic window.8,9
While substantial progress has been made in elucidating the neurodegenerative cascade and developing targeted pharmacotherapeutics for AD, therapeutic outcomes remain suboptimal for comprehensive disease management. Current treatment modalities primarily focus on symptom palliation, with efficacy progressively decreasing as synaptic integrity declines. This underscores the critical importance of early intervention, particularly during the predementia stages of AD.10,11 Therapeutic efforts, including cognitive training, physical exercise, and both pharmacological and non-pharmacological therapies, have shown significant potential in attenuating cognitive decline have shown significant potential in attenuating cognitive decline and improving learning and memory, executive function, or daily functioning in individuals at the prodromal stage and may even contribute to reversing certain impairments.12–14 Consequently, the predementia phase has emerged as a pivotal focus for early therapeutic strategies aimed at preserving cognitive function and delaying or preventing the onset of full-blown dementia. The opportunity to mitigate disease progression during this critical stage emphasizes the imperative for timely diagnosis and targeted interventions that could substantially alter the disease trajectory.
Virtual reality (VR) technology has emerged as a novel adjunctive tool in neurorehabilitation due to its ability to deliver immersive, interactive, and ecologically valid therapeutic experiences.14,15 In clinical practice, VR-based interventions have been implemented through two primary modalities: head-mounted display systems, which fully immerse users in computer-generated 3D environments via goggles or helmets equipped with motion sensors, and screen-based VR, which presents interactive simulations on monitors, utilizing motion sensors, controllers, or touch interfaces for user interaction (Figure 1).16–18 These systems are commonly adapted to accommodate the sensory and cognitive profiles of older adults, ensuring usability and safety. Despite its growing popularity, the clinical utility of VR in early-stage neurocognitive disorders remains inadequately characterized, necessitating a systematic synthesis of current evidence.
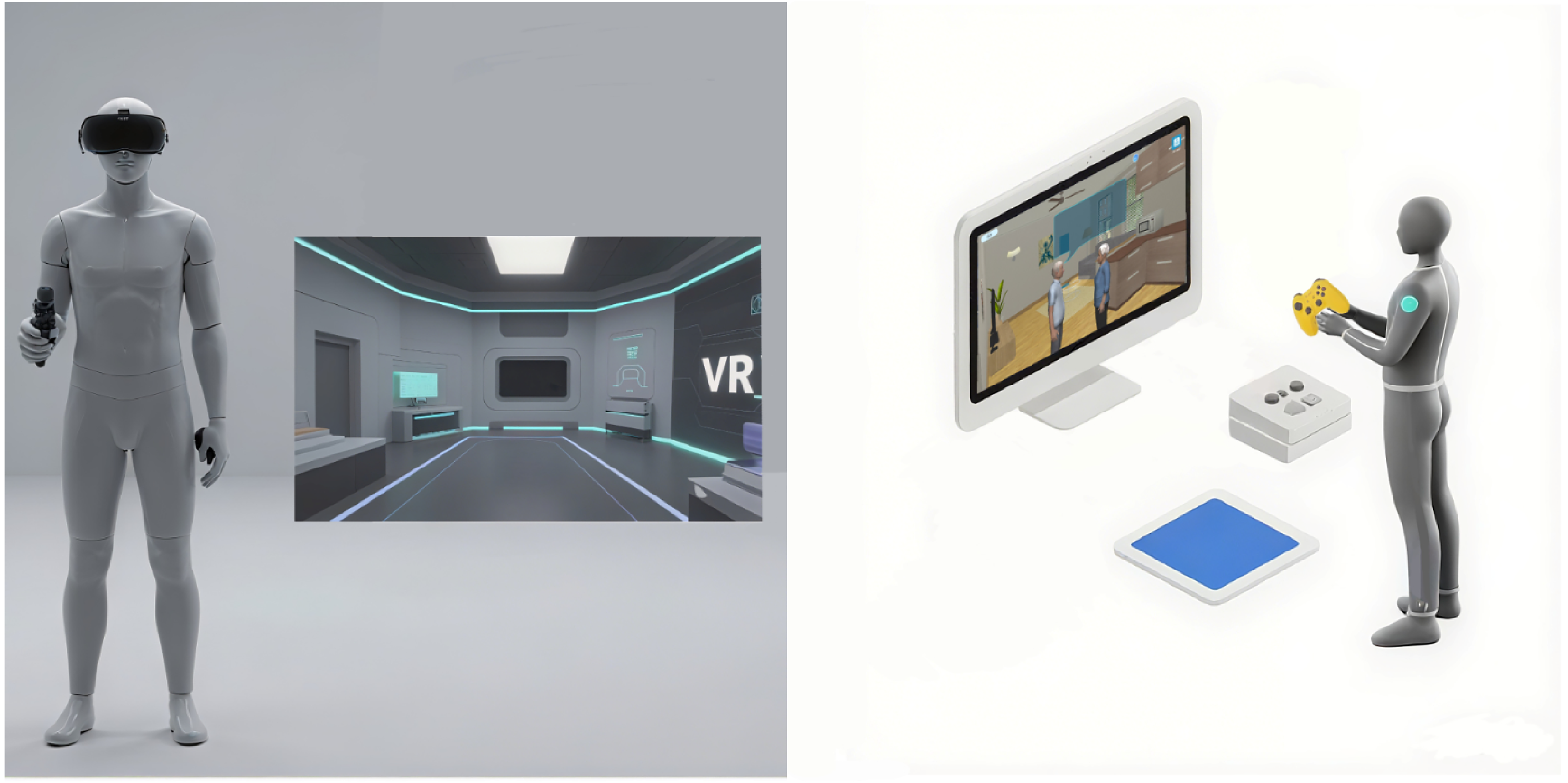
Comparative schematic of VR cognitive training modalities: head-mounted display (immersive, left) versus screen-based system (non-immersive, right).
VR-based cognitive interventions targeting cognitive rehabilitation typically involve structured, domain-specific tasks embedded in virtual environments that replicate real-world settings. For instance, supermarket navigation tasks are used to stimulate episodic memory, a key component of the broader domain of learning and memory; sequence-following games for working memory enhancement; and problem-solving simulations to engage executive function. Such programs allow for real-time adjustment of difficulty based on performance, facilitating individualized and adaptive training.19–21 In contrast to conventional cognitive therapies—which are often paper-based, abstract, and delivered in static clinical environments—VR offers dynamic, contextualized, and highly engaging training that fosters better transfer of skills to daily life.20,21
VR-based cognitive interventions complement traditional rehabilitation by enhancing engagement and enabling precise performance quantification. Crucially, the reviewed interventions constitute targeted cognitive training for predementia, primarily enhancing learning and memory, working memory, and executive functions through adaptive tasks in simulated environments (e.g., virtual navigation, problem-solving scenarios). 22 While VR inherently leverages multisensory inputs (visual/auditory cues, occasional tactile feedback) to heighten immersion and ecological validity, these elements serve a subsidiary role—distinguishing them from passive multisensory stimulation (e.g., Snoezelen rooms) focused on sensory exposure or mood regulation. Although most VR programs are designed to improve cognitive functions, some also incorporate modules aimed at emotional regulation (e.g., stress reduction scenarios) or functional training (e.g., virtual kitchen tasks to support instrumental activities of daily living).23,24 Therefore, in this review, we define VR-based cognitive intervention as any structured VR protocol designed to enhance cognitive function, regardless of delivery format, with or without adjunctive psychological or functional components.
However, the existing literature is limited by several methodological deficiencies, including small sample sizes, a predominant focus on AD populations, and a lack of research involving individuals in the predementia stages. 25 While VR-based cognitive interventions show promise in cognitive rehabilitation for individuals with MCI, existing evidence remains inconsistent. For instance, Liao et al. reported significant post-intervention improvements in Montreal Cognitive Assessment (MoCA) scores within VR-trained groups, 26 whereas Kang et al. found only marginal, non-significant enhancements in Mini-Mental State Examination (MMSE) metrics following immersive VR or computerized cognitive training. 27 Similarly, VR's effects on learning and memory are contested: improvements in delayed recall were observed after 8-week interventions, yet Park revealed no superiority of semi-immersive VR exercise training over conventional computer-based programs for MCI patients. 28 In the attention domain, while Torpil et al. documented significantly greater gains in VR groups using the LOTCA-G assessment, 29 Liu et al. found no measurable advantage of immersive VR over traditional methods in post-stroke cognitive impairment cohorts. 30 These discrepancies underscore the need for systematic analysis of VR's efficacy across cognitive domains.
The application of VR technology in cognitive training has garnered considerable interest in recent years, yet existing research has yielded inconsistent findings. To address this, the current study employs a rigorous evidence synthesis framework to systematically assess the therapeutic effectiveness of VR-based cognitive training interventions on specific neurocognitive functions and functional independence in daily living among individuals with SCD or MCI. Our preliminary analysis suggests that VR interventions may offer superior benefits compared to traditional approaches, a finding that warrants further in-depth exploration.
Moving forward, we advocate for the conduct of more robustly designed, well-powered studies with meticulously characterized participant groups and a careful selection of appropriate cognitive and instrumental activities of daily living (IADL) measures. Such efforts will facilitate more precise comparisons between VR and traditional interventions, thereby providing a stronger evidence base for the integration of VR technology in cognitive rehabilitation.
Methods
The present quantitative evidence synthesis was conducted in strict alignment with the methodological standards established by the Cochrane Collaboration, while reporting procedures conformed to the PRISMA 2020 statement for transparent research dissemination. 31 The methodological protocol for this systematic evidence synthesis was prospectively documented in the International Prospective Register of Systematic Reviews (PROSPERO) with the assigned identifier CRD 42024614616. During the data extraction process, we expanded the outcome measures to include additional domains of cognition. The assessment framework included psychometrically validated constructs across multiple cognitive domains: general neurocognitive capacity, mnemonic processing, attentional control, visuospatial processing accuracy, self-perceived cognitive deficits, and executive regulation.
Search strategy
To ensure both comprehensiveness and methodological rigor, we systematically searched seven major biomedical and psychological databases—MEDLINE, EMBASE, APA PsycINFO, PubMed, Web of Science, CINAHL, and Cochrane Library—from January 1, 2004, to November 1, 2024. These databases were selected based on their broad disciplinary coverage, use of controlled indexing systems (e.g., MeSH, Emtree), and inclusion of peer-reviewed, high-impact journals, thereby maximizing retrieval of relevant and methodologically sound random controlled trials (RCTs). The search strategy was designed in accordance with PRISMA 2020 guidelines and a pre-registered protocol in PROSPERO (CRD42024614616). It combined free-text terms and controlled vocabulary tailored to each database, using the following core structure: (virtual reality OR augmented reality OR exergame OR virtual task* OR virtual environment* OR virtual world OR serious game* OR virtual game* OR video game* OR computer game* OR exergame* OR VR OR computer OR digital*) AND (dementia OR Alzheimer disease OR cognitive dysfunction OR cognition OR MCI OR predementia OR neurocognitive disorders) AND (random*), in the database which has its mesh terms, we use their mesh terms and maximized sensitivity while ensuring that indexed studies met baseline quality criteria (random*: the truncated term ‘random’ expands to encompass all suffix derivatives critical for identifying RCTs) (Supplemental Material 1). To further ensure the inclusion of unpublished or non-indexed data, we conducted systematic citation tracking of key reviews and searched the ProQuest Dissertation & Theses Global database for gray literature. Inclusion was restricted to English-language RCTs evaluating VR-based cognitive interventions in individuals with predementia. Non-English studies were excluded due to limitations in translation resources and quality control.
Inclusion and exclusion criteria
Inclusion in the meta-analysis was determined based on the fulfillment of the prespecified PICOS-based eligibility criteria:
Population: We included studies involving participants with a clinician-based diagnosis of a predementia state (SCD or MCI). Details of the specific inclusion criteria, including the diagnostic standard and quantitative cognitive cut-off scores used by each study. It is important to note that the included studies did not consistently report detailed baseline neuropsychological data, which precluded a direct statistical comparison of cognitive status between intervention and control groups across all studies. While the reliance on a formal clinical diagnosis ensures a standard for inclusion, we acknowledge that this approach does not account for the well-documented clinical heterogeneity within these populations, particularly MCI. This is recognized as a primary limitation of this review. Intervention: VR-based cognitive intervention refers to structured therapeutic protocols delivered through immersive or non-immersive virtual reality technology, explicitly designed to target and enhance specific cognitive domains via adaptive, interactive tasks requiring active cognitive processing. Any VR-based cognitive intervention designed to promote neuroplastic adaptation through structured virtual tasks. Comparator: The study employed two distinct comparator groups: (1) Cognitive rehabilitation received conventional cognitive interventions through alternative modalities, including paper-and-pencil training protocols, computerized cognitive training programs, or therapist-administered sessions, all matched to the VR-based cognitive intervention in duration and frequency to ensure comparable treatment intensity; (2) Usual therapy/non-cognitive training (routine care) underwent standard clinical monitoring involving periodic neuropsychological assessments and general health advice but were explicitly excluded from structured cognitive training components, thereby serving as a true non-intervention baseline. This dual-comparator design allowed for simultaneous evaluation of VR's absolute effects (versus usual therapy/non-cognitive training) and relative efficacy against established cognitive interventions (versus cognitive rehabilitation). Outcomes: Studies were required to report quantitative outcomes in at least one of the following domains: neurocognitive performance, psychological well-being, or functional independence in IADL. Study design: Only RCTs with either a comprehensive outcome assessment protocol or a targeted cognitive component analysis were included.
Exclusion from the meta-analysis was determined based on the fulfillment of the prespecified methodological disqualifier:
Focused on evaluating the effectiveness of VR equipment or algorithm, rather than the outcomes related to improvements in cognition, psychological health, or IADL. Classified as secondary literature (including systematic reviews, clinical practice recommendations, non-peer-reviewed conference proceedings, expert position papers, and editorial commentaries) were excluded from the analysis. Diagnosed neurocognitive disorders (e.g., AD), neurodegenerative conditions (Parkinsonism), cerebrovascular pathology, immune-mediated demyelinating diseases (multiple sclerosis), seizure disorders, primary psychiatric comorbidities, or chronic systemic illnesses were excluded to mitigate confounding effects. The control group received VR-based interventions during the study. VR-based cognitive interventions primarily targeting non-cognitive therapies (e.g., cognitive behavior therapy, physiotherapy, motor rehabilitation) were excluded.
Data extraction
Dual independent data abstraction was performed by paired researchers utilizing standardized protocols, with subsequent cross-verification to ensure accuracy (by Jiaping Wang and Hanbo Li). We designed and piloted a structured data collection tool to maintain methodological rigor and systematically capture key variables from eligible studies while minimizing inter-rater variability. The curated datasets were systematically structured in tabular format and processed through RevMan 5.4 for analytical preparation. Documented elements encompassed essential bibliographic descriptors (investigator names, publication chronology), methodological specifications comprising experimental contrasts (interventional modalities, control groups), cohort profiles (population metrics, age distributions), and treatment protocol dimensions (virtual reality immersion depth, session intensity, frequency, therapeutic timeline). For studies provided only in graphical format without accessible numerical data, we initiated standardized multilingual communication with authors per ICMJE guidelines. If no response was received, data were extracted from high-resolution figures using GetData Graph Digitizer, following a standardized protocol: axis calibration, pixel-level digitization, and dual independent extraction with cross-validation. This process ensures that the graphical data, such as bar charts used in the studies, is accurately and reliably converted into numerical data for analysis. All extracted data underwent dual independent extraction with cross-validation. This software-assisted methodology demonstrates superior accuracy compared to manual estimation techniques, with subsequent statistical conversions executed in accordance with Cochrane Handbook guidelines. 32 Disputes concerning study eligibility or data extraction were resolved by a third investigator, Yi Zhu, who served as the final decision maker.
Risk of bias
Methodological rigor assessment of included trials was conducted using the Cochrane risk of bias tool 2 (Cochrane RoB 2 tool), 33 with a structured assessment in six key areas: 1) concealment of randomization sequence generation and allocation, 2) implementation of participant/person blinding protocol, 3) completeness of outcome data reporting, 4) objectivity of outcome measurement procedures, 5) transparency of selective outcome reporting, and 6) identification of external confounders (whether or not mentioning the conflict of interest statement). Given the interactive and immersive nature of VR-based interventions, full blinding of participants and personnel was generally not feasible. This limitation is inherent to the modality and has been observed in other technology-assisted behavioral interventions. 34 Nonetheless, we systematically evaluated the risk of performance bias associated with a lack of blinding and explicitly documented such risks under the relevant RoB 2 domains. In most trials, control groups received either conventional cognitive training, standard rehabilitation, or routine care without additional digital tools. To address heterogeneity in outcome measurement across studies, we used SMD for meta-analyses. Although different tools (e.g., MMSE, MoCA) were used to assess global cognitive function, these instruments are validated for similar cognitive domains and are frequently treated as interchangeable. 35 Furthermore, study-level characteristics—such as intervention duration, frequency, and type—were included in subgroup and meta-regression analyses. While participant-level variables (e.g., baseline cognitive impairment severity) were not consistently reported across studies, subgroup analyses stratified by clinical diagnosis were performed where data permitted. Assessment of evidence certainty followed the GRADE framework,36,37 with independent dual-review using the GRADEpro Guideline Development Tool (GRADEpro GDT; https://www.gradepro.org),38,39 followed by consensus reconciliation.
Data synthesis and statistical analysis
Statistical computations were conducted within the Cochrane Review Manager (RevMan) 5.4 platform and the R programming suite 4.4.1 environment, with dedicated modules employed for meta-analytical procedures and sensitivity analyses respectively. The analytical strategy prioritized clinical heterogeneity assessment through a two-phase protocol:
In phase 1, all studies underwent systematic scrutiny to identify clinically meaningful differences across three key areas: population characteristics (e.g., age and the reported criteria for defining cognitive impairment), intervention protocols (e.g., total intervention number and duration), and outcome measurement methods (e.g., domains of cognitive function).
A primary characteristic of interest was the participants’ baseline degree of cognitive impairment. However, a formal subgroup analysis based on cognitive severity was precluded by the significant heterogeneity in assessment tools used across the included studies (e.g., MMSE, MoCA, MMQ). These instruments differ in their structure, scoring, cut-off values, and clinical interpretation. Furthermore, most studies did not report severity distributions in a standardized format that would permit pooling. Therefore, in accordance with Cochrane guidance to avoid bias from non-standardized stratification criteria, we did not perform a subgroup analysis based on baseline cognitive severity. Instead of a subgroup analysis, we addressed potential baseline differences by extracting available group-level data, such as age, education, and the originally reported cognitive scores (e.g., mean MMSE or MoCA). This information was then used to inform our study-level Risk of Bias assessment. Any notable imbalances were documented and incorporated into the risk of bias assessment via the Cochrane RoB 2 tool framework.
Subsequently, phase 2 employed heterogeneity across studies, which was assessed using the χ² test and I² statistic, with a significance level set at α = 0.1. Fixed-effects models were prioritized when clinical homogeneity was confirmed (p > 0.1 and I² < 50%), while random effects models were selectively applied. The significance level for the meta-analysis was set at α = 0.05. In cases of significant clinical heterogeneity, additional analyses, such as subgroup analysis, sensitivity analysis, meta-regression, or descriptive methods, were conducted to explore and explain the variability across studies.
Measure consistency mean deviation (MD) when trial instruments demonstrated measure consistency, while SMD addressed scale heterogeneity across studies. All estimates were precisely quantified with 95% probability intervals to delineate parameter uncertainty boundaries. Analytic procedures implemented random-effects assumptions to accommodate between-study variance, while heterogeneity quantification was conducted through dual computational verification processes utilizing RevMan 5.4 and R 4.4.1 statistical platforms. The findings of the meta-analysis were displayed through forest plots and tables, offering a visual depiction of the effect sizes.
Subgroup analysis and meta-regression
Subgroup analyses were performed to examine potential moderators of intervention effectiveness. Grouping variables were based on intervention characteristics and predefined participant stratifications. These included:
Intervention duration (≤30 min, > 30 min per session) Frequency (sessions < 3 per week, ≥ 3 per week) Total intervention duration (< 2 months, ≥ 2 months) Total number of sessions (< 20 sessions, ≥ 20 sessions) Degree of immersion (head-worn VR, screen-based VR) Involvement of motor activities (with motor intervention, without motor intervention)
All subgroup divisions were based on a binary categorization, with cutoff values determined by the median of each variable calculated across the 12 included studies for each respective outcome measure. This approach ensured a data-driven and balanced stratification while maintaining sufficient sample size within subgroups.
These categories were used in RevMan 5.4 to perform subgroup analyses, where effect sizes for each subgroup were calculated separately. Statistical comparisons were conducted to assess significant differences in effect sizes between the subgroups (Table 1).
Subgroup types.

The absence of reported intervention durations in Park (2) et al. precluded the classification of these interventions.
The baseline unit of frequency is established as per week.
Control group: Active: Cognitive training, Participants who received the primary intervention, such as traditional cognitive training; Passive: Non-cognitive training, Participants who were given a less interactive intervention, like general health education.
For meta-regression, the same grouping factors were used as covariates to explore their relationships with overall effect sizes. Meta-regression was performed using R 4.4.1 to examine how each covariate, such as age, intervention type, and duration, influenced the intervention's effects on neuropsychological outcomes. Given the limited number of included studies (4–5 per outcome), multivariate meta-regression was preemptively excluded based on established methodological standards. Current guidelines explicitly prohibit complex adjustments with fewer than 10 studies per covariate to prevent overfitting and spurious associations (Cochrane Handbook §10.11 32 ; JAMA Statistical Guidance 2023 40 ). We therefore prioritized univariate meta-regression supplemented by subgroup analyses. This conservative approach balances analytical rigor with clinical interpretability while adhering to contemporary reporting standards for evidence synthesis.
Sensitivity analysis
Methodological consistency was verified through leave-one-out cross-validation during sensitivity assessments of the outcomes. In this approach, each study was sequentially excluded, and the meta-analysis was rerun to examine the impact of each study on the overall outcome. This analysis helps evaluate the stability of the results and the potential influence of individual studies on the conclusions. In RevMan 5.4, this can be done by sequentially removing studies and recording the changes in the pooled effect size.
Results
Literature search and study selection
A PRISMA flowchart (Figure 2) tracked evidence selection from 19,980 initial records to 12 included studies. After deduplication (n = 15,953), three-stage screening (automated title filtering, ML-assisted abstract review, full-text appraisal) excluded 15,569 irrelevant works. Full-text assessment of 424 articles applied PICOS criteria, excluding mismatched designs/populations. The final evidence synthesis incorporated 12 methodologically qualified studies meeting predefined PICOS criteria, constituting the analytical foundation for both qualitative review and quantitative pooled estimation.
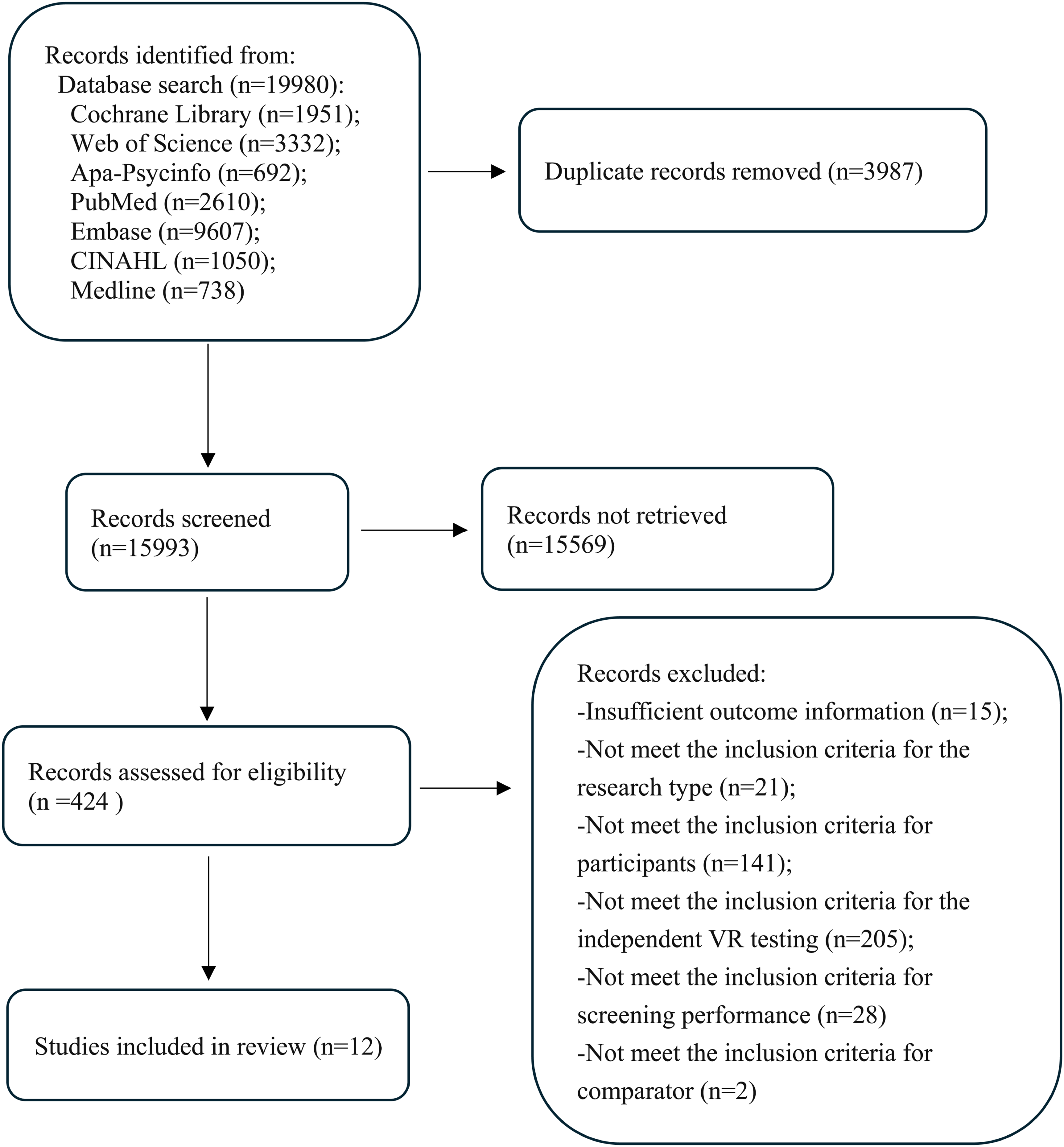
Literature screening flowchart.
Assessment of the credibility of the evidence
Methodological rigor assessment through the Cochrane Risk of Bias framework (Figure 3; Supplemental Material 2) identified the assessment of risk across the analyzed trials. Principal methodological deficiencies involved intervention protocol adherence, incomplete outcome disclosure, and participant withdrawal management.
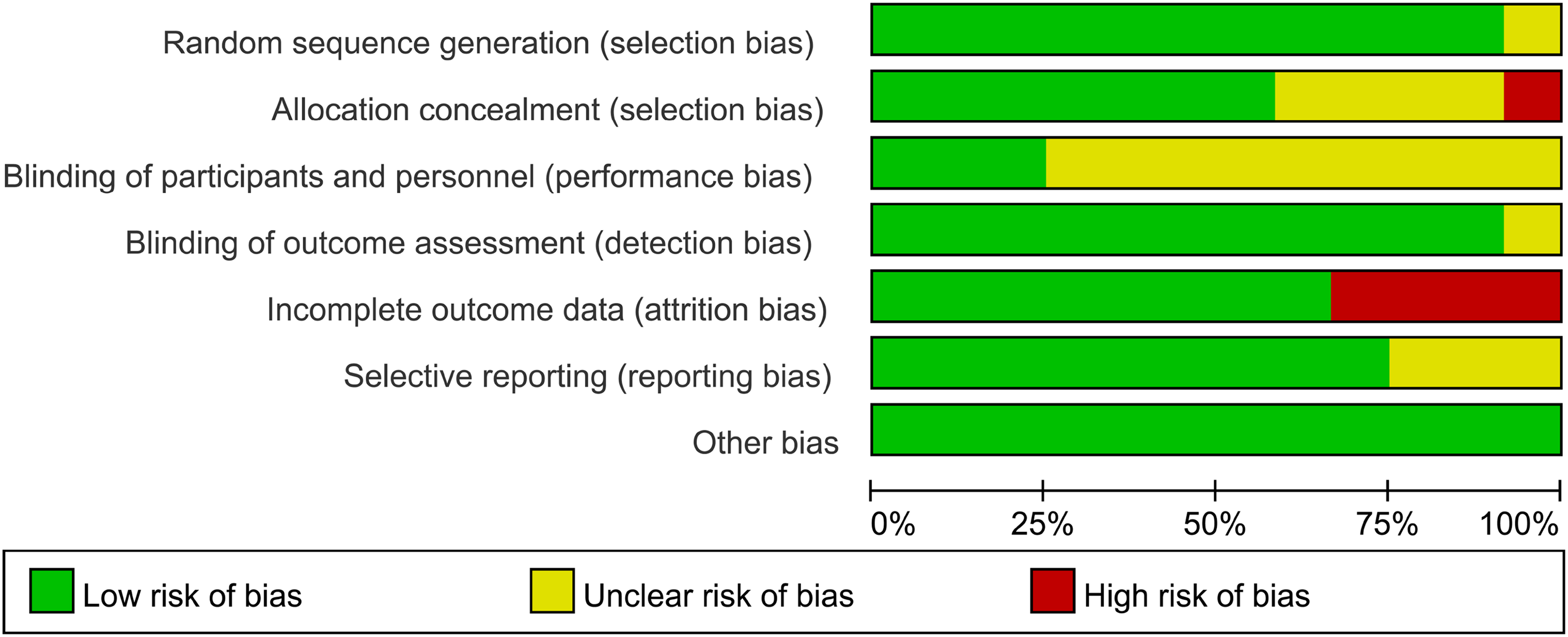
Risk of bias graph.
Notably, a single trial demonstrated elevated methodological risk in group assignment procedures, suggesting inadequacies in random sequence generation protocols. Four studies reported participant dropout, which could affect outcome validity due to incomplete data. Additionally, one study was flagged for reporting bias due to incomplete initial reporting, raising concerns about the transparency of its outcome reporting. Collectively, the majority of investigations exhibited satisfactory methodological control, particularly in terms of randomization sequence construction and allocation blinding mechanisms, reflecting rigorous design implementation on these critical dimensions.
Using the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) framework, we assessed five primary outcomes. 50 Subjective cognitive complaints demonstrated high-certainty evidence, supported by minimal bias and high precision. IADL outcomes were rated as moderate certainty, with limitations in study heterogeneity. Evidence for working memory and executive function outcomes was classified as low certainty due to the significant risk of bias and inconsistency. Episodic memory and global cognitive function were deemed very low certainty, primarily due to attrition-related bias in included studies. A detailed summary of evidence certainty, including the rationale for downgrading or upgrading (Supplemental Material 3).
Study characteristics
To account for variability in assessment tools and participant inclusion criteria, we adopted a domain-based framework for analyzing cognitive outcomes. The methodological attributes of the analyzed investigations are systematically cataloged in Table 2. While the included studies did not utilize a single unified standard to define cognitive impairment, each study applied validated instruments, such as the MMSE or MoCA, to determine participant eligibility and classify baseline cognitive status. The methodological attributes of the analyzed investigations are systematically cataloged in Table 2. During outcome synthesis, we grouped cognitive tests into predefined domains based on their primary functional target, including global cognition, learning and memory, working memory, executive function, verbal fluency, and visuospatial abilities. This domain-based classification was informed by prior literature and neuropsychological consensus frameworks.
The synthesized evidence incorporates a comprehensive characterization.
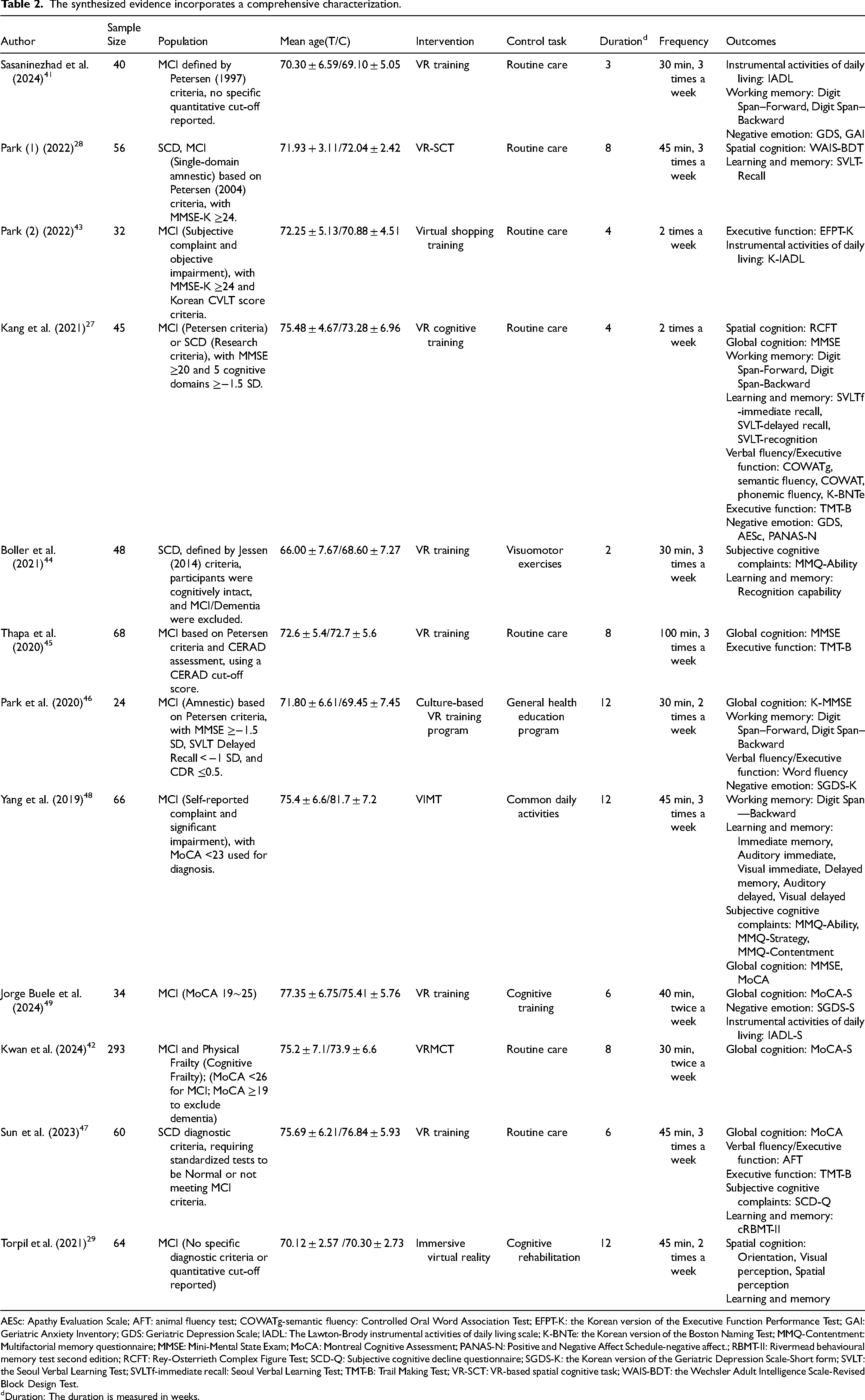
AESc: Apathy Evaluation Scale; AFT: animal fluency test; COWATg-semantic fluency: Controlled Oral Word Association Test; EFPT-K: the Korean version of the Executive Function Performance Test; GAI: Geriatric Anxiety Inventory; GDS: Geriatric Depression Scale; IADL: The Lawton-Brody instrumental activities of daily living scale; K-BNTe: the Korean version of the Boston Naming Test; MMQ-Contentment: Multifactorial memory questionnaire; MMSE: Mini-Mental State Exam; MoCA: Montreal Cognitive Assessment; PANAS-N: Positive and Negative Affect Schedule-negative affect.; RBMT-II: Rivermead behavioural memory test second edition; RCFT: Rey-Osterrieth Complex Figure Test; SCD-Q: Subjective cognitive decline questionnaire; SGDS-K: the Korean version of the Geriatric Depression Scale-Short form; SVLT: the Seoul Verbal Learning Test; SVLTf-immediate recall: Seoul Verbal Learning Test; TMT-B: Trail Making Test; VR-SCT: VR-based spatial cognitive task; WAIS-BDT: the Wechsler Adult Intelligence Scale-Revised Block Design Test.
Duration: The duration is measured in weeks.
Narrative integration of the endpoint evaluations
Among the 12 included randomized controlled trials, 9 focused on patients with MCI,27–29,41,43,45,46,48,51 while 4 enrolled individuals with SCD.27,28,44,47 The demographic distribution of the study population encompassed that the average age ranges from 60 to 90 years, with male representation fluctuating between 20% and 65%. These trials assessed the diagnostic performance of VR-based tests for individuals with predementia across six different countries. Detailed information on each study, including author details, intervention types, control tasks, outcomes, duration, frequency, and other relevant aspects, is summarized in Table 2.
In this review, cognitive performance was not treated as a unified construct due to the heterogeneity in assessment domains and tools. Instead, we categorized outcomes into distinct domains—global cognition, learning and memory, working memory, executive function, verbal fluency, and spatial cognition—based on the theoretical construct each measurement aimed to capture. This approach improves conceptual clarity and prevents inappropriate aggregation of dissimilar outcomes. Each domain was analyzed separately, and the number of studies contributing to each analysis was reported to ensure transparency and methodological rigor.
Regarding the cognitive outcomes, six studies assessed global cognition,27,45–48,51 four examined executive function,27,45–47 three examined subjective cognitive complaints,44,47,48 six focused on learning and memory,27–29,44,47,48 four evaluated working memory,27,41,46,48 two assessed verbal fluency,46,47 three measured visuospatial abilities.27–29 Additionally, three studies evaluated IADL.41,43,51 Furthermore, four studies explored negative emotional states,27,45,46,51 such as depression, anxiety, apathy, and positive emotional processing. Cognitive performance was assessed using a range of standardized instruments. Working memory was evaluated using the digit span test. Assessment of executive function employed the Trail Making Test's task-switching paradigm (TMT-B) and verbal fluency tasks, evaluating mental flexibility and processing speed. 52 Learning and memory performance, verbal fluency, and spatial cognition were evaluated using tools specified in the individual studies. Functional independence was evaluated using the IADL scale; gains in IADL scores signify improved capacity for self-care, household management, and medication adherence, thereby indicating reduced dependence on caregivers and enhanced personal autonomy, while psychoemotional status evaluation incorporated the validated Geriatric Depression Scale (GDS) psychometric protocol. Collectively, the selected assessment battery provides critical insights not only into core cognitive functions and emotional states per se, but also into their clinical relevance, offering valuable indicators of an individual's potential for maintaining real-world functional performance and independent living. However, it is important to note that some cognitive domains were evaluated in only a limited number of studies—for example, verbal fluency (2 studies) and visuospatial function (3 studies). It must be acknowledged that the small number of contributing studies in these subgroups may reduce the robustness of pooled estimates and limit the interpretability of domain-specific findings.
Subgroup analysis and meta-regression
Given the substantial methodological variability across included studies—particularly in intervention duration, frequency, session length, and the use of motor components—we performed both subgroup and meta-regression analyses to explore potential sources of heterogeneity. Subgroup analyses stratified studies based on clinically relevant thresholds (e.g., intervention duration <2 versus ≥2 months; frequency <3 versus ≥3 sessions/week; session length <20 versus ≥20 min). These analyses often revealed more consistent effects in specific subgroups and notably reduced heterogeneity, indicating that intervention dosage and structure may moderate cognitive outcomes. Complementarily, meta-regression provided a quantitative evaluation of linear relationships between these continuous moderators and effect sizes. For instance, shorter session durations and lower intervention frequency were significantly associated with greater improvements in working memory and psychological symptoms, respectively. These analytical strategies improved the interpretability of domain-specific effects and clarified sources of outcome variability, thus reinforcing the validity of pooled conclusions. Subgroup analyses were conducted based on pretreatment biopsychosocial characteristics, with results reported separately by cognitive domain and summarized using forest plots. For each meta-analysis, I² values and heterogeneity p-values were reported. Where high heterogeneity remained, potential sources were qualitatively discussed and conclusions appropriately qualified.
Meta-analysis results
Cognition function
Global cognition in people with predementia. A pooled analysis of 6 clinical trials involving 276 subjects evaluated the therapeutic efficacy of VR-based cognitive training protocols on neurocognitive trajectories among prodromal dementia. Non-significant divergence in global cognitive function was found between the VR and intervention modalities (SMD = 0.28, 95% CI [−0.13, 0.69], I² = 63%, p = 0.17). Subgroup analyses were conducted, but we found no subgroup showing significant results.
The outcome measures were further disaggregated into the MoCA and MMSE scales, both used to assess global cognition. For MoCA, a significant effect was observed (MD = 0.96, I² = 65%). In contrast, the results for MMSE indicated that VR showed an effect similar to that of traditional cognitive interventions on global cognition in predementia participants (Table 3).
Heterogeneity of articles with subgroup analysis tables.
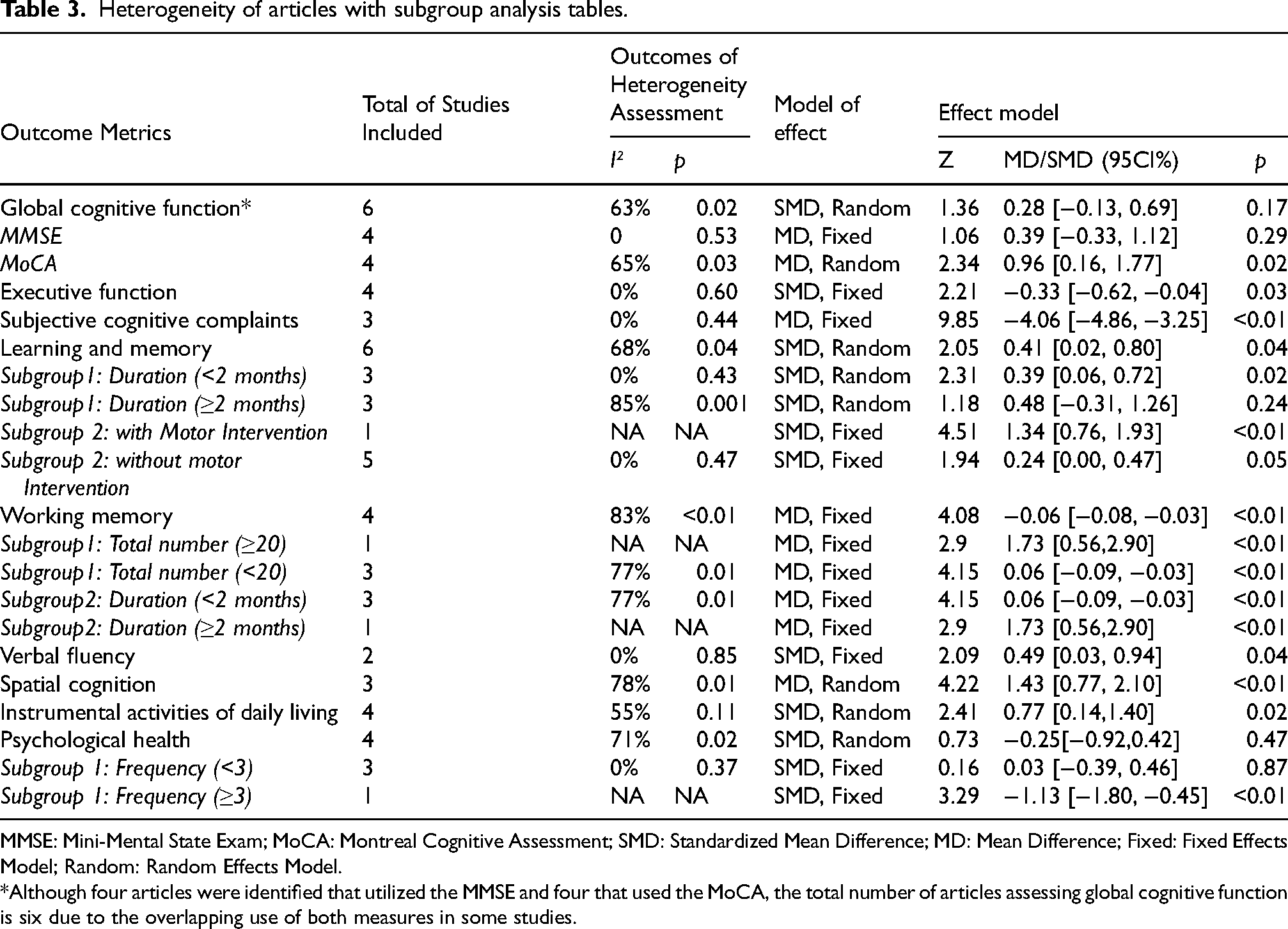
MMSE: Mini-Mental State Exam; MoCA: Montreal Cognitive Assessment; SMD: Standardized Mean Difference; MD: Mean Difference; Fixed: Fixed Effects Model; Random: Random Effects Model.
*Although four articles were identified that utilized the MMSE and four that used the MoCA, the total number of articles assessing global cognitive function is six due to the overlapping use of both measures in some studies.
Global cognitive function was assigned very low certainty evidence. Despite originating from high-certainty RCTs, two critical concerns necessitated downgrading: 1) unmasked outcome assessment introducing performance bias, 2) substantial unexplained heterogeneity (I² = 63%, p<0.05). Full adjudication criteria are documented in Supplemental Material 2.
Executive function in people with predementia. Four studies (188 participants) assessed the effects of executive function. The pooled results indicated that VR was significantly less effective than cognitive intervention or usual care, with a small but statistically significant standardized mean difference favoring the control group (SMD −0.33, 95% CI [−0.62, −0.04], I² = 0, p = 0.03) (Figure 4 and Table 3). For this analysis, the effect size was standardized so that a negative value indicates a more favorable outcome for the control group. However, the small effect size suggests that the practical difference between the groups is modest. This result should therefore be interpreted cautiously as indicating no substantial difference between VR and control conditions in the executive function domain.

Forest plot of the effects of VR compared to control on executive function in patients with predementia.
Evidence on executive function interventions is low-quality, with moderate RCTs downgraded twice for methodological limitations (primarily reporting biases per ROB 2.0). These biases introduced uncertainty, critically undermining the credibility and generalizability of the findings.
Subjective cognitive complaints in people with predementia. Self-perceived cognitive complaints were primarily assessed in patients with SCD. Three studies compared changes in subjective cognitive complaints before and after VR-based cognitive intervention. Quantitative synthesis demonstrated significant improvements in patient-perceived cognitive functioning post-intervention, with fewer subjective cognitive complaints in those with VR-based intervention than with traditional intervention. Fixed-effects meta-analysis revealed a clinically meaningful between-group divergence (SMD = −4.06, 95% CI [−4.86, −3.25]) (Figure 5). Notably, the absence of between-study heterogeneity (I²=0%, p < 0.01) corroborates methodological congruence across outcome measurement frameworks.

Forest plot of the effects of VR compared to control on subjective cognitive complaints in patients with predementia.
High-quality assessment of subjective cognitive complaints has methodological rigor, validated tools, and comprehensive contextualization. Studies use standardized criteria with psychometric integrity to capture self-perceived cognitive decline. Integration with objective testing improves diagnostic specificity. High-quality evidence emphasizes reproducibility, aligns with established frameworks, and informs targeted interventions.
Comprehensive assessment of learning and memory in the predementia cohort. The effects of VR on learning and memory performance were significant (SMD = 0.41, 95CI [0.02, 0.80], I² = 68%, p < 0.05). Subgroup analysis revealed temporal dependency in therapeutic outcomes, with short-duration protocols (under 2 months) demonstrating clinically meaningful enhancements (I² = 0%, p < 0.05). Conversely, extended implementation periods exceeding 2 months failed to demonstrate statistical significance (I² = 85%, p = 0.24). Regarding motor involvement, VR without motor activities elicited marginal yet statistically detectable treatment effects (SMD = 0.24, 95% CI [0.00, 0.47], I² = 0%, p < 0.01), while VR with motor activities demonstrated a more pronounced effect, suggesting that incorporating motor elements may enhance learning and memory (Table 3). Meta-regression analysis revealed an inverse temporal efficacy association between intervention duration and memory improvement (β = −1.6883, p = 0.0035), indicating that interventions lasting sub-20 min were more effective (Table 4). Sensitivity analysis showed that excluding the study by Sun reduced heterogeneity from I² = 95% to 0, with the pooled effect size ranging from −0.80 to 0.10, likely due to the lower quality of this study.
Meta-Regression analyses on linear relationships between moderators and outcome measures.

ΔZr: Fisher's r-to-z correlation difference.
The quality of the learning and memory outcome is very low. This is mainly due to the inconsistency in the results and the high risk of bias in the original articles, which leads to a downgrade in the quality of this outcome.
Working memory in people with predementia. The meta-analytic synthesis of 4 RCTs demonstrated superior working memory enhancement through VR-based cognitive interventions compared to conventional protocols (SMD = −0.06 [−0.08, −0.03], I² = 83%, p < 0.001). In the subgroup analysis, the effect size of the intervention duration less than 2 months was statistically significant (I² = 77%, p < 0.01). In contrast, longitudinal comparative analysis revealed non-significant effect trajectories in extended-duration experimental arms. The total number of interventions was identified as another influencing factor. The subgroup with fewer than 20 interventions showed a significant improvement in working memory with VR (SMD = 0.06 [−0.09, −0.03], I² = 77%, p < 0.05) (Table 3). Meta-regression analysis further confirmed that shorter intervention durations (less than 20 min each) led to more pronounced VR effects on working memory (β = −0.717, p = 0.01) (Table 4). Leave-One-Out influence diagnostics demonstrated critical outlier sensitivity profiles, where iterative exclusion of outlier clusters, Kwan et al., substantially attenuated between-study variance components (I² = 49%) and increased the standardized mean difference from −0.06 to 0.96. The observed growth might be explained by the limited efficacy of Kwan's experimental protocol, wherein a three-month VR-based cognitive intervention focusing on cultural immersion showed no significant improvement in working memory or sustained attention.
Verbal fluency in people with predementia. Two studies evaluated the effects of VR on verbal fluency.46,47 The statistical findings demonstrated that participants undergoing VR-based training protocol exhibited markedly superior performance in linguistic fluency metrics relative to the cohort without the VR-based cognitive intervention (SMD = 0.49, 95% CI [0.03, 0.94], I² = 0%, p < 0.05) (Figure 6). Specifically, Park's randomized controlled trial documented modest enhancement in verbal fluency within MCI populations, 46 whereas Jong-Hwansun demonstrated that VR enhanced verbal fluency in patients with SCD to a similar extent as in the controls. 47

Forest plot of the effects of VR compared to control on verbal fluency in patients with predementia.
Spatial cognition in people with predementia. For spatial cognition, the VR-based rehabilitation group demonstrated superior outcomes compared to those receiving conventional therapeutic approaches (MD = 1.43, 95% CI [0.77, 2.10], I² = 78%, p < 0.01) (Figure 7). However, the high heterogeneity warranted further exploration of potential contributing factors.

Forest plot of the effects of VR compared to controls on spatial cognition in patients with predementia.
Excluding Park, Jin-Hyuck reduced heterogeneity, with the I² value dropping from 78% to 0. 28 Additionally, the effect size shifted from 1.43 to 1.11. This systematic shift in effect estimates indicates that the divergent neurocognitive assessment framework employed in this particular study, specifically, the implementation of WAIS-BDT for evaluating visuospatial constructional reasoning–introduces critical measurement variance when compared to navigation-based spatial orientation paradigms (e.g., virtual Morris water maze) measuring allocentric mapping capacity in other included trials.
IADL
The comparative assessment of IADL showed that the VR-based cognitive intervention showed a statistically significant difference in instrumental activities of daily living level indicators compared with conventional care participants (SMD = 0.77, 95% CI [0.14,1.40], I² = 55%, p = 0.02). This between-group variance suggests the therapeutic benefits of VR training in functional independence domains (Figure 8). Sensitivity analysis showed that excluding Sasaninezhad, 41 Mahdieh caused the effect size to fluctuate between 0.77 and 0.52, with heterogeneity decreasing from 55% to 6%. In the present investigation, the medium risk of bias assessed in this study may plausibly account for these observed outcome variations.

Forest plot of IADL.
The quality assessment of IADL is rated as moderate. This is primarily due to the bias introduced by the inclusion of high-risk articles. The scores obtained, are higher, indicating a greater need for external care or support. The assessment also considers various determinants such as demographic factors, psychosocial characteristics, and functional status. These determinants are important for understanding the factors that affect the quality of life in older adults and can help in developing targeted prevention and rehabilitation schemes.
Psychological health
Four studies have shown a close relationship between cognitive impairment and emotional disorders, particularly negative emotions. In our study, the GDS was used to assess depressive mood. VR-based cognitive interventions were found to be as effective as usual care regarding depressive symptom alleviation, with quantitative synthesis revealing substantial statistical heterogeneity that may reflect implementation variability across trials (SMD = −0.25, 95% CI [−0.92,0.42], I² = 71%, p = 0.47).27,41,46 Subgroup analysis suggested that intervention frequency may moderate the effect on emotional symptoms. Meta-regression analysis demonstrated a notable linear correlation between the frequency of interventions and emotional outcomes (β = −4.1191, p < 0.01). This finding suggests that as the frequency of interventions increases, there is a marked decline in GDS scores, indicating a reduction in the severity of depression. Kang's study evaluated, 27 among other factors, negative effects, and found that VR not only enhanced apathy but also positively impacted both positive and negative emotional states, as well as quality of life. These findings provide further evidence of VR's capacity to address emotional disturbances in the older population (Table 3).
Additionally, the Geriatric Anxiety Inventory (GAI) assessed anxiety symptoms. 41 VR led to significant improvements within both the intervention (p < 0.001) and control groups (p < 0.001). However, no significant between-group differences were observed at baseline or follow-up (p > 0.05), suggesting that VR may improve anxiety within groups but does not show a clear advantage over traditional interventions.
Discussion
Principal results
This systematic review and meta-analysis explored the impacts of VR-based cognitive interventions across diverse cognitive domains, emotional and psychological aspects, and IADL in older individuals with predementia. Our findings suggest that VR-based cognitive interventions may offer improvements in specific areas such as learning and memory, working memory, verbal fluency, spatial cognition, and IADL compared to control groups, with p-values indicating statistical significance (p < 0.05). However, it is important to interpret these results with caution due to the substantial heterogeneity observed and the variability in baseline cognitive levels across the studies included. No statistically significant variations were observed in other outcomes, including global cognitive performance, self-perceived cognitive deficits, and affective symptom profiles. This indicates that while there are promising trends in certain cognitive areas, the overall impact of VR-based interventions requires further investigation to account for the diverse methodological approaches and participant characteristics in existing literature.
The therapeutic benefits of VR-based cognitive interventions on visuospatial cognition in cognitive decline populations have been substantiated, 53 aligning with our spatial navigation enhancement findings. Enhanced verbal fluency and IADL performance observed in VR-based cognitive interventions mirror our experimental outcomes,26,54 particularly regarding lexical retrieval and instrumental IADL. A synthesis of current evidence supports VR's noninferiority compared to conventional protocols, 55 with longitudinal data suggesting its potential to decelerate cognitive deterioration trajectories through personalized adaptive training paradigms.
Prior research has established that early VR-based cognitive interventions are efficacious in recognizing and managing mood disorders, 56 exhibiting their potential as a valuable therapeutic modality. 57 The limited improvements observed across various domains of negative emotion in our study, compared to prior research, could stem from participant-specific factors inherent to our sample. The study cohort predominantly comprised patients presenting with SCD and MCI based on established diagnostic criteria. Notably, these individuals exhibited relatively low baseline levels of negative emotions compared to other populations reported. As a result, the observed improvement following intervention may not have been sufficient to bridge the gap between our findings and those reported in prior studies that focused on groups with higher baseline negative affectivity, such as those with AD. This may explain why the observed changes following intervention were not more pronounced.
Methodological rigor was ensured through the application of the ROB 2.0 for systematic evaluation of trial design integrity. Four studies by Jorge Buele, Torpil Kang, Jae Myeong Park, and Jong-hwan, which were assessed as high risk, included low-quality evidence across nearly all outcome measures. This may account for the observed substantial variability in our findings.
Sensitivity analysis showed that excluding Sun reduced heterogeneity from moderate to low for global cognition, learning, and memory function, 47 and this investigation used the Rivermead Behavioral Memory Test, highlighting significant learning and memory improvements with VR. In the case of working memory, we excluded Kwan, 42 which reduced the heterogeneity and increased the effect size, which is likely due to the shorter duration (12 weeks) of VR training in their study. Analysis of IADL outcomes revealed that omitting the dataset from Sasaninezhad Mahdieh substantially decreased between-study variability. 41 This methodological adjustment aligns with the moderate risk identified in the aforementioned assessment, which nevertheless demonstrated the greater therapeutic efficacy of VR-based cognitive interventions in IADL enhancement relative to conventional rehabilitation approaches documented in this literature.
Subgroup analysis and meta-regression were used to examine how intervention characteristics may influence the efficacy of immersive digital therapies. Specifically, shorter intervention durations (<2 months) and session lengths (<20 min) were associated with greater improvements in working memory. This aligns with prior evidence on cognitive load dynamics in VR training; for example, a previous study reported diminished adherence and increased cybersickness in prolonged VR sessions among older adults, suggesting that excessive cognitive demands and adverse side effects may undermine user engagement and limit therapeutic efficacy. 58 While the meta-regression identified a statistically significant association between shorter session duration and working memory gains, this result should be interpreted cautiously, as baseline cognitive status was not standardized across studies. It remains possible that the observed pattern reflects uncontrolled group differences rather than a true dose-response relationship. Nevertheless, the findings tentatively support the use of streamlined VR-based cognitive interventions—particularly in older populations—to balance cognitive stimulation with tolerability. In addition, learning and memory outcomes were more favorable in studies that incorporated motor elements into the VR tasks, suggesting that sensorimotor integration may facilitate learning and memory encoding. Conversely, longer interventions (≥2 months) appeared to benefit learning and memory consolidation, indicating that the optimal duration of VR-based training may depend on the targeted cognitive domain. This distinction—shorter regimens for working memory, and longer ones for episodic memory—has not been systematically addressed in previous VR literature.
To further explore potential factors influencing global cognitive function, we performed a broader meta-regression analysis. This analysis indicated near-significant negative associations for both immersion (p = 0.064) and intervention frequency (p = 0.055) with overall cognitive outcomes, collectively explaining 51.3% of the heterogeneity. These findings tentatively suggest that excessive technological immersion or high-frequency sessions may diminish cognitive benefits, potentially due to cognitive fatigue or habituation effects. Such patterns reflect the “diminishing returns” phenomenon, wherein neuroplastic adaptations may plateau or decline with overexposure to repetitive cognitive stimuli. 59
From a clinical perspective, our findings support a stratified design approach, where intervention length and complexity are tailored to specific cognitive outcomes. For example, memory-focused protocols may benefit from longer durations with progressive difficulty to support consolidation, while working-memory-focused protocols may favor brief, high-frequency sessions to avoid cognitive overload. Regarding emotional outcomes, higher intervention frequency was associated with greater reductions in depressive symptoms, consistent with behavioral activation theory, which suggests that structured engagement in rewarding activities can counteract avoidance behaviors in depression. 60 In VR-based interventions, frequent immersive sessions may facilitate cognitive stimulation, goal-directed action, and emotionally salient interactions, thereby promoting positive reinforcement and mood regulation through dopaminergic pathway activation. Collectively, these findings highlight modifiable design parameters—session length, duration, motor integration, and dosing frequency—as potential targets for optimizing VR-based interventions. Future trials should prioritize factorial and adaptive designs to validate and refine these parameters, especially in diverse and clinically vulnerable populations. 60 It is hypothesized that emotional disturbances may exacerbate cognitive decline through alterations in neurochemistry or by influencing functional connectivity within the brain's cortical networks. 61 Consequently, early detection and therapeutic intervention for affective disorders in cognitively compromised populations emerge as critical clinical priorities. 62 Early VR-based cognitive interventions, particularly in managing emotional symptoms, show promise as an effective therapeutic tool. 56
Future directions
Subsequent investigations necessitate focused attention on three principal methodological constraints in current VR rehabilitation research: compromised immersive fidelity, absence of subject-specific ergonomic modifications, and inadequate integration of gerontologically compatible design parameters. Enhancing the immersion of VR-based cognitive interventions through full-body tracking, 360-degree environments, and more interactive scenarios could improve user engagement and replicate real-world cognitive and emotional challenges, thereby addressing the significant heterogeneity attributable to differences in VR task design. Additionally, the personalization of VR-based cognitive interventions to accommodate the specific cognitive and emotional profiles of patients should be explored.
The impact of intervention duration also warrants further investigation. As noted, shorter intervention durations may yield more pronounced effects on certain cognitive domains, possibly due to reduced adverse reactions and better participant engagement. Future studies could explore the potential benefits of intermittent short-duration VR-based cognitive interventions, which might lead to different outcomes compared to longer, continuous sessions. However, there is a lack of empirical evidence to indicate that reducing intervention frequency adversely affects results.
Lastly, our findings highlight a critical need for methodological standardization and rigor across the field. Specifically, the field requires larger, well-powered RCTs that directly compare VR-based interventions with traditional therapy, addressing the current variability in methodological quality and limited sample sizes. Establishing a standardized methodological framework across investigations is essential to allow for evidence-based parameter setting for clinical VR applications.
Limitations
First, despite conducting subgroup analyses and meta-regressions to explore potential sources of between-study variance—including baseline cognitive profiles, intervention duration, and VR device specifications—substantial heterogeneity persisted across key outcome measures, particularly in attention and memory. A considerable proportion of this variance could not be explained by measured moderators, which may reflect unmeasured factors such as differences in VR task design (e.g., scenario complexity, feedback mechanisms) or participant-level neuropsychological profiles.
Second, the analyses for specific cognitive domains were based on a relatively small number of studies (typically two to six per domain), and the overall sample sizes of individual trials were limited. These constraints not only increase the likelihood of statistical noise and bias but also reduce the power of subgroup and meta-regression analyses, making domain-specific results preliminary and subject to influence by a few studies.
Third, the included studies exhibited significant variability in methodological quality and participant retention rates. Deficiencies in these areas could introduce potential biases into the pooled estimates and limit the overall strength and certainty of our conclusions.
Fourth, interpreting the findings related to intervention duration is challenging. While shorter intervention durations appeared more effective in some trials, this may not necessarily reflect the superiority of brief interventions but rather the influence of progressive cognitive decline during longer trials. Further research is needed to clarify how intervention duration interacts with disease progression and participant engagement.
Finally, the lack of standardized methodological frameworks across investigations hinders the establishment of evidence-based parameters for VR applications. To advance this field, future studies should adopt more rigorous and harmonized designs, rather than being limited by current methodological inconsistencies.
Conclusions
This meta-analysis suggests that VR-based cognitive interventions may be associated with improvements in select cognitive domains—such as global cognition, working memory, and daily functioning—in individuals with predementia. However, the number of available studies for each domain was limited, and substantial heterogeneity, along with the inclusion of several high-risk-of-bias trials, restricts the strength and generalizability of the conclusions. In particular, subgroup analyses in this review often relied on lower-quality evidence, which may have introduced bias and contributed to variability in observed effects.
While individual studies and theoretical frameworks support the neuroplastic potential of VR through multisensory stimulation and adaptive cognitive engagement, robust longitudinal evidence confirming structural or functional neural changes remains scarce. Therefore, conclusions regarding the disease-modifying potential of VR should be drawn cautiously. VR-based interventions are thought to enhance neuroplasticity primarily through repetitive, goal-directed cognitive engagement in enriched, ecologically valid virtual settings that simultaneously stimulate multiple sensory modalities (e.g., visual, auditory, and proprioceptive).15,63 This multimodal stimulation, combined with real-time feedback and adaptive task difficulty, may facilitate synaptic strengthening and functional reorganization of neural networks associated with working memory, learning and memory, and executive control.64,65 However, despite these theoretical underpinnings, robust and longitudinal evidence for sustained structural or functional brain changes—and their translation into clinically meaningful outcomes—remains limited. Consequently, while VR holds promise as a tool for cognitive rehabilitation, current claims regarding its ability to slow neurodegenerative progression should be interpreted cautiously until validated by high-quality, long-term trials with appropriate neurobiological endpoints.
With regard to psychological outcomes, preliminary associations between higher intervention frequency and reduced depressive symptoms may reflect underlying mechanisms described by behavioral activation theory—which posits that increased engagement with rewarding and structured activities can mitigate depressive effects. However, this hypothesis was not directly tested in the included studies and should be further explored in future research.
In summary, VR-based interventions represent a promising and increasingly studied modality for cognitive rehabilitation in predementia populations. Nevertheless, current evidence remains preliminary, and definitive conclusions about clinical efficacy cannot yet be made. Future studies should aim to reduce bias, increase sample sizes, explore longitudinal outcomes, and clarify mechanisms of action to better establish the role of VR in clinical cognitive care.
Supplemental Material
sj-docx-1-alz-10.1177_13872877251404046 - Supplemental material for Effects of virtual reality-based therapy on cognitive and psychological outcomes in older adults with predementia: A systematic review and meta-analysis
Supplemental material, sj-docx-1-alz-10.1177_13872877251404046 for Effects of virtual reality-based therapy on cognitive and psychological outcomes in older adults with predementia: A systematic review and meta-analysis by Jiaping Wang, Hanbo Li, Yizhen Wang, Fanfan Meng, Zheyuan Liu, Tingting Zhao, Ping Xu, Chuan Guo and Yi Zhu in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
Declaration of Generative AI: The initial image for Figure 1 was generated using Doubao (ByteDance). The authors reviewed, refined, and finalized the content and take full responsibility for the accuracy and integrity of the figure.
Ethical considerations
Not applicable
Consent to participate
Not applicable
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research initiative received funding support through the National Key R&D Program of China [Grant No. 2023YFC3603605, Grant No. 2023YFC3603604]; in conjunction with the Science & Technology Department of Jiangsu Province [Grant No. BE2023778]; Jiangsu Provincial Medical Innovation Center [Grant No. Rehabilitation Medical Innovation Center (CXZX202222)].
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data sharing is not applicable to this article as no datasets were generated or analyzed during this study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.