
Abstract
Background
Cholinesterase inhibitors (ChEIs) are cornerstones of the symptomatic treatment of Alzheimer's disease (AD) and dementia with Lewy bodies (DLB) and are also prescribed for vascular dementia (VaD). Despite their widespread use, patterns of ChEI prescribing are unclear.
Objective
Our objective was to examine the prevalence, timing, and types of ChEI prescriptions before and after dementia diagnosis.
Methods
We analyzed electronic health record and claims data for patients diagnosed with AD, DLB, or VaD between October 2015 and August 2022 from a large U.S. healthcare system. ChEI claims (donepezil, rivastigmine, galantamine) were identified in the ±3 years surrounding dementia diagnosis. Repeated measures logistic regression was used to estimate the likelihood of ChEI fills by time-period, dementia type, and time x dementia type interaction to determine if change in prescription patterns significantly differed by diagnosis.
Results
Among 3166 eligible patients, DLB had the highest prevalence of ChEIs both pre-and post-diagnosis compared to patients with AD and VaD. Post-diagnosis, donepezil was the most common, while galantamine use was sparse. After adjusting for demographics, patients with VaD had lower rates of ChEIs relative to AD (OR: 0.34, 95% CI 0.26–0.45). In the fully adjusted model, females (OR: 0.81, 95% CI: 0.71–0.91) and patients from ethnoracially minoritized populations (OR: 0.74, 95% CI: 0.62–0.88) were less likely to fill ChEI prescriptions.
Conclusions
Donepezil was the most frequently filled ChEI across dementias. Patients with DLB had the highest prevalence of ChEIs pre- and post-diagnosis. The potential disparities in treatment we identified should be investigated further.
Keywords
Introduction
Alzheimer's disease (AD), dementia with Lewy bodies (DLB), and vascular dementia (VaD) are the three most common causes of dementia. In the US, over 6 million individuals were estimated to have AD in 2020 and this number is expected to double by 2060 as the population ages. 1 The total cost of dementia care is estimated to exceed $600 billion in the US annually, 2 with both DLB and VaD having higher reported costs of care and increased caregiver burden compared to AD.3–5 Despite the recent availability of anti-amyloid therapies for the treatment of mild cognitive impairment and mild dementia due to AD,6,7 symptomatic management continues to play an important role in the treatment of AD, DLB, and VaD. 8
Cholinesterase inhibitors (ChEIs), including donepezil, rivastigmine, and galantamine, are used for the treatment of AD, DLB, and VaD. Donepezil was first approved by the Food and Drug Administration (FDA) in 1996 for the treatment of AD with additional approvals for different dosages, severity of AD symptoms, and delivery routes. 9 Rivastigmine was FDA-approved by the in 2000 to treat mild to moderate AD and Parkinson's disease dementia. 10 A transdermal patch was made available in 2007 and is indicated for severe AD. 11 Galantamine was FDA-approved in 2001 for the treatment of mild to moderate AD. 11
While these three ChEIs are FDA-approved to treat AD, multiple studies provide evidence for their off-label use to treat patients with DLB and VaD. 12 In fact, multiple systematic reviews have been published evaluating the efficacy and tolerability of ChEIs in AD, DLB and VaD.12–14 These studies demonstrated improvement in cognition and performance in activities of daily living using a range of standardized measures. Studies have also shown a reduction of psychotic symptoms with ChEIs in AD and DLB and improvement in neuropsychiatric inventory (NPI) scores.15–17 There is also evidence that patients with AD who are treated with rivastigmine are less likely to be placed in nursing homes than those not taking rivastigmine. 18 Although patients with DLB experience earlier nursing home placement relative to those with AD, ChEI use has been demonstrated to delay this transition in care. 19 Therefore, ChEI use can reduce the cost of care by reducing the risk of nursing home placement.18,20
A previous study evaluating ChEI prescription rates found that donepezil was the most commonly prescribed ChEI. 21 One international study found an increase in ChEI prescriptions for patients with dementia globally from 2008 to 2018. 22 Despite their widespread availability after 1996 and supporting evidence for use, little is known about contemporary patterns of ChEI prescribing, particularly in the early stages of dementia. The objective of this study was to examine patterns of ChEI prescriptions, including the prevalence, timing, and types, for individuals with AD, DLB, and VaD. We also sought to determine if any demographic factors were associated with differences in prescribing patterns of ChEI among patients with dementia.
Methods
Study population
Patient data used in this study were extracted from the electronic health record (EHR) and claims data from HealthPartners, a large integrated healthcare system across Minnesota and Western Wisconsin in the United States. that provides general medical and specialty care and insurance coverage to its members. We identified 3166 patients who received the following diagnoses between October 2015 and August 2022 based on International Classification of Diseases (ICD-10) codes: AD = G30.X, DLB = G31.83, and VaD = F01.50. In our analysis, patients with more than one diagnosis were categorized into one of the subgroups using methods described in Chen et al. 23 Patients with Parkinson's disease (PD) were not included, thus excluding those with PD and a dementia diagnosis. We utilized the Bynum-standard algorithm, 24 which requires more than one visit with a dementia diagnosis, to identify our cohort. The first instance of a documented AD, DLB, or VaD diagnosis was defined as the date of diagnosis and served as the index. Random chart audits (5%) were conducted to confirm diagnosis. Patients who did not consent to sharing their medical records were excluded. This study was approved by the Institutional Review Board at HealthPartners and was performed in accordance with the ethical standards as outlined in the 1964 Declaration of Helsinki.
Outcome measures
Insurance claims were extracted for up to three years pre- and post-index for a total of six years of observation per patient. Demographic data from the EHR, including age, sex, race, and ethnicity at the time of index, and the presence of claims for donepezil, galantamine, and/or rivastigmine and the date the prescription was filled, were collected for this study. Unfilled prescriptions were not included in our analysis as they did not generate an insurance claim.
Statistical analysis
Patient characteristics and ChEI fills were compared between diagnosis groups before and after diagnosis, and patterns of prescribing were described. Repeated measures logistic regression was used to estimate the likelihood of ChEI fills by time-period, dementia type, and time x dementia type interaction to determine if change in prescription fills significantly differed by diagnosis. The significance level was set at p < 0.05. Post-hoc testing employed Bonferroni correction to account for pairwise comparisons. All analyses were performed in R version 4.2.1.
Results
Study cohort demographics
We identified 2478 with AD, 175 patients with DLB, and 513 with VaD. Demographic characteristics are reported in Table 1. There were significant differences between the three groups for age, sex, race, and ethnicity (all p < 0.001). Compared to patients with DLB and VaD, patients with AD were more likely to be over the age of 84. A greater proportion of patients diagnosed with DLB were male compared to those with AD and VaD. Patients with VaD were more racially and ethnically diverse than patients with AD or DLB.
Characteristics of patients with dementia.
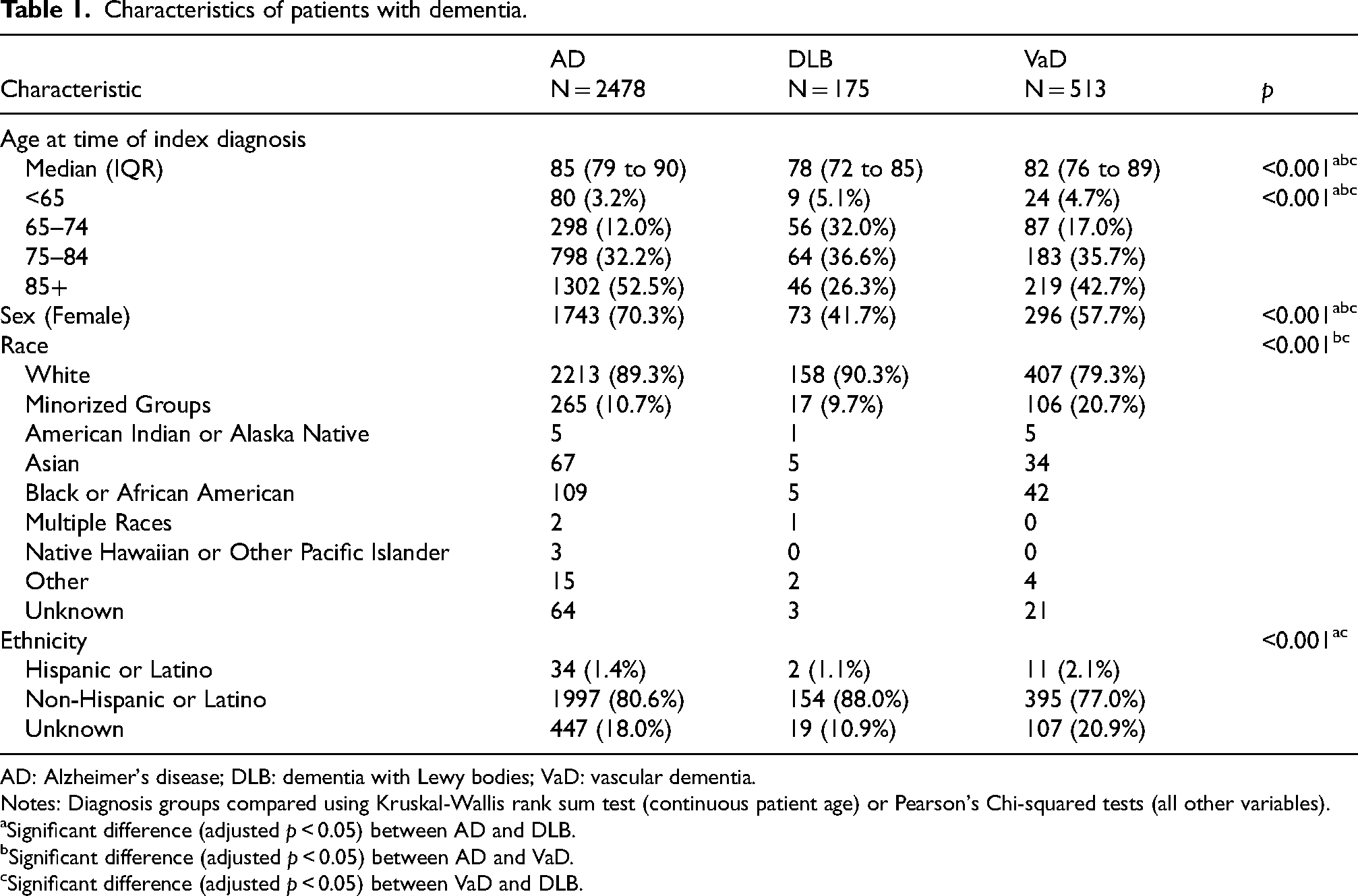
AD: Alzheimer's disease; DLB: dementia with Lewy bodies; VaD: vascular dementia.
Notes: Diagnosis groups compared using Kruskal-Wallis rank sum test (continuous patient age) or Pearson's Chi-squared tests (all other variables).
Significant difference (adjusted p < 0.05) between AD and DLB.
Significant difference (adjusted p < 0.05) between AD and VaD.
Significant difference (adjusted p < 0.05) between VaD and DLB.
Prevalence, type, and timing of ChEI prescriptions
Table 2 provides results regarding the prevalence, type, and timing of ChEI fills for patients with AD, DLB, and VaD. Pre-diagnosis, 26% of all patients with dementia filled prescriptions for ChEIs, and post-diagnosis 35% filled prescriptions for ChEIs, with 65% of patients not filling a ChEI after diagnosis. The prevalence of ChEI fills before and after diagnosis varied significantly among the groups. Patients with DLB had the highest prevalence of ChEI fills both before (39%) and after (59%) diagnosis, compared to those with AD (28% pre-diagnosis, 38% post-diagnosis) and VaD (13% pre-diagnosis, 14% post-diagnosis; Figure 1).
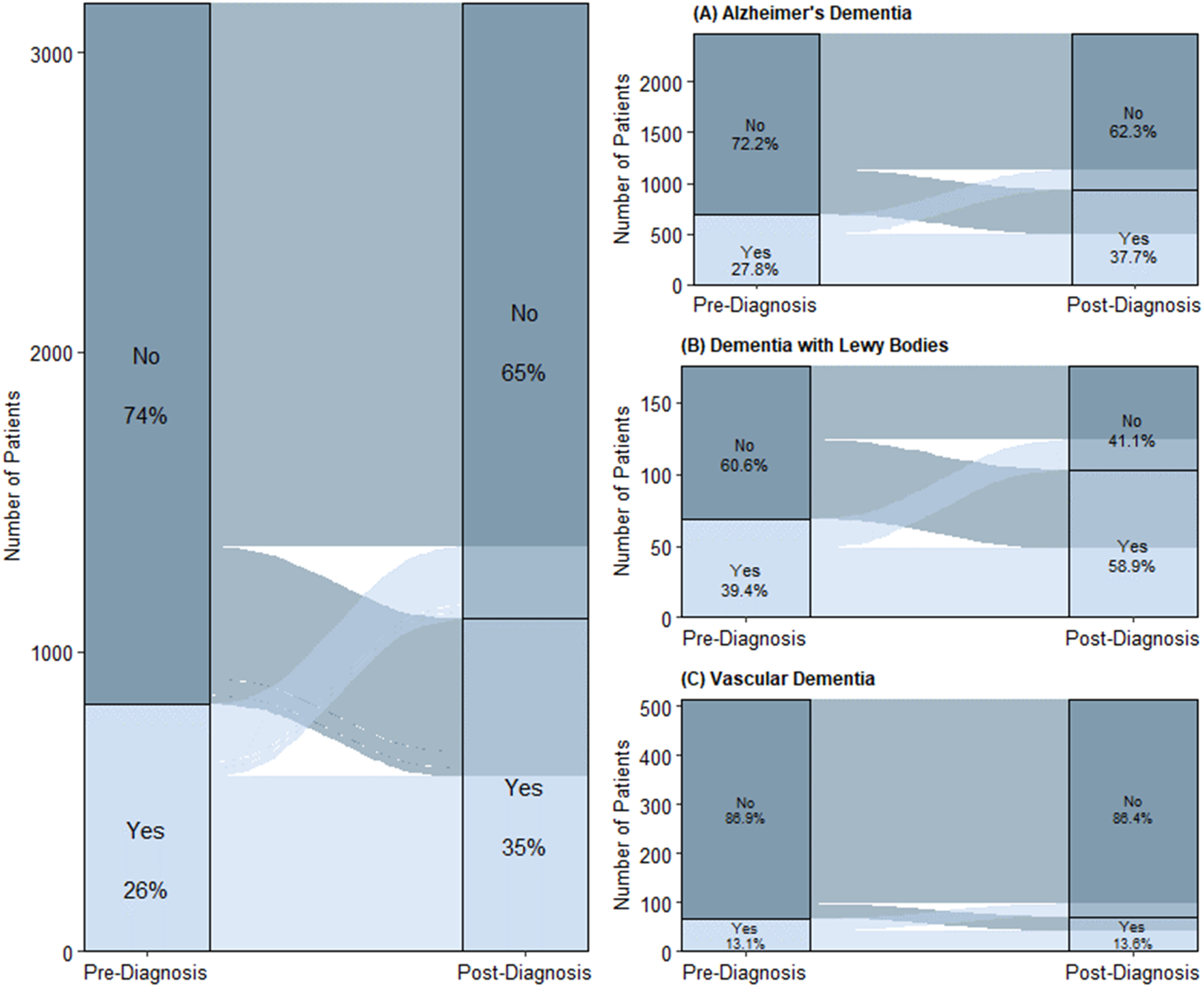
Sankey diagrams of ChEI prescriptions pre- and post-diagnosis by dementia diagnosis. The Sankey diagram on the left shows ChEI prescription status both pre- and post-diagnosis for all patients in the sample. 26% of patients had ChEI prescriptions pre-diagnosis compared to 35% post-diagnosis. The Sankey diagrams on the right show ChEI prescriptions for (A) Alzheimer's disease: 27.8% of patients with AD had ChEI prescriptions pre-diagnosis and 37.7% had prescriptions post-diagnosis; (B) Dementia with Lewy bodies: 39.4% of patients with DLB had ChEI prescriptions pre-diagnosis, while this number increased to 58.9 post-diagnosis; and (C) Vascular dementia: 13.1% of patients with VaD had ChEI prescriptions pre-diagnosis compared to 13.6% post-diagnosis.
Prevalence of ChEI prescriptions before and after dementia diagnosis.
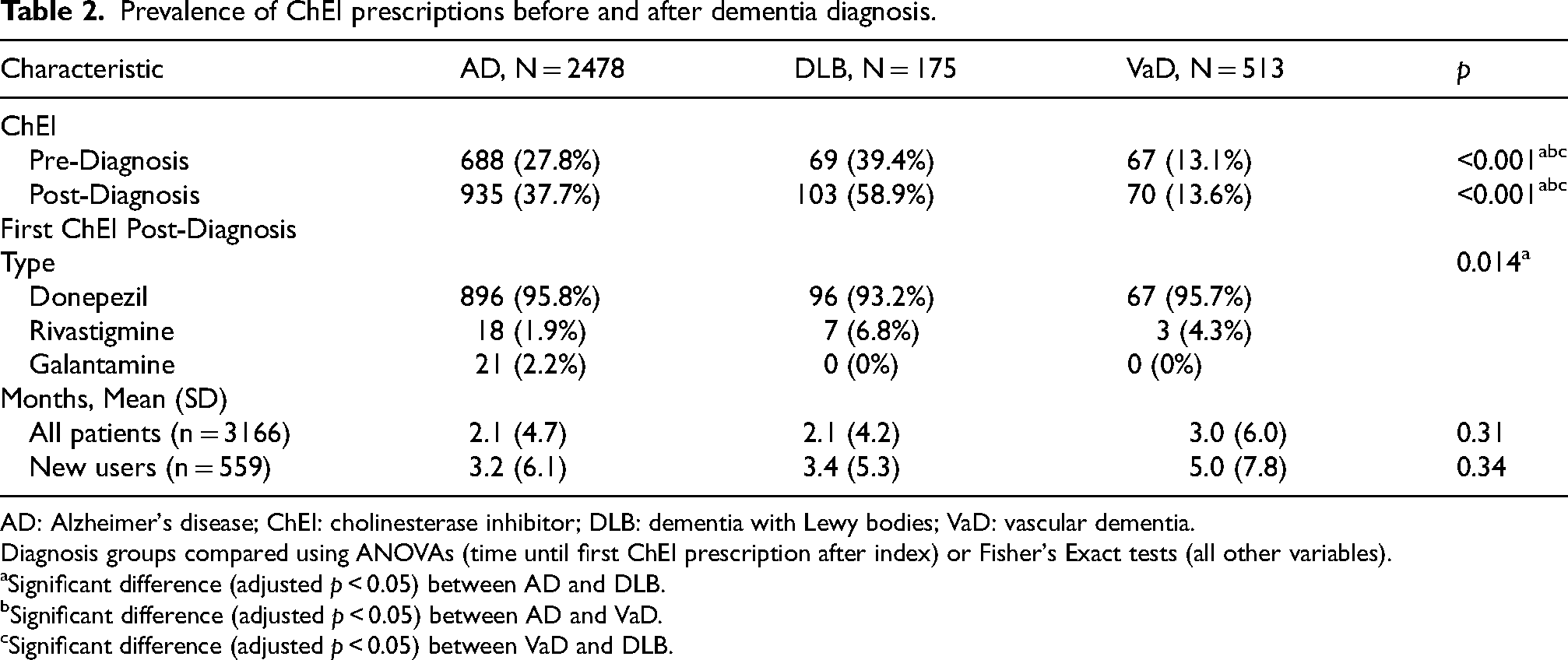
AD: Alzheimer's disease; ChEI: cholinesterase inhibitor; DLB: dementia with Lewy bodies; VaD: vascular dementia.
Diagnosis groups compared using ANOVAs (time until first ChEI prescription after index) or Fisher's Exact tests (all other variables).
Significant difference (adjusted p < 0.05) between AD and DLB.
Significant difference (adjusted p < 0.05) between AD and VaD.
Significant difference (adjusted p < 0.05) between VaD and DLB.
Donepezil was the most used first ChEI post-diagnosis, accounting for 96% of ChEI fills for patients with AD and VaD groups and 93% for patients with DLB. Rivastigmine was filled significantly more often for patients with DLB (6.8%) compared to those with AD or VaD (1.9% and 4.3%, respectively). Fills for galantamine were identified in only 2.2% of patients with AD, whereas no patients with DLB or VaD had fills for this medication. There was no difference between groups in terms of the amount of time between the diagnosis of dementia and their first ChEI fills.
Predictors of ChEI prescribing in AD, DLB, and VaD
The adjusted logistic regression model showed that patients with dementia were 1.6 times more likely to have a ChEI fill after diagnosis compared to the period before diagnosis. However, patients with VaD had significantly lower rates of ChEI use compared to those with AD at any time surrounding the initial diagnosis (OR: 0.34, 95% CI 0.26 to 0.45), with no significant differences observed between the DLB and AD groups. Females were less likely to fill ChEI prescriptions than males (OR: 0.81, 95% CI: 0.71 to 0.91), and patients from ethnic and racial minoritized populations had lower odds of filling ChEIs compared to patients from White populations (OR: 0.74, 95% CI: 0.62 to 0.88). Additionally, patient age at the index diagnosis was inversely associated with the likelihood of ChEI use (OR: 0.96, 95% CI: 0.95 to 0.97) (Table 3, Figure 2).
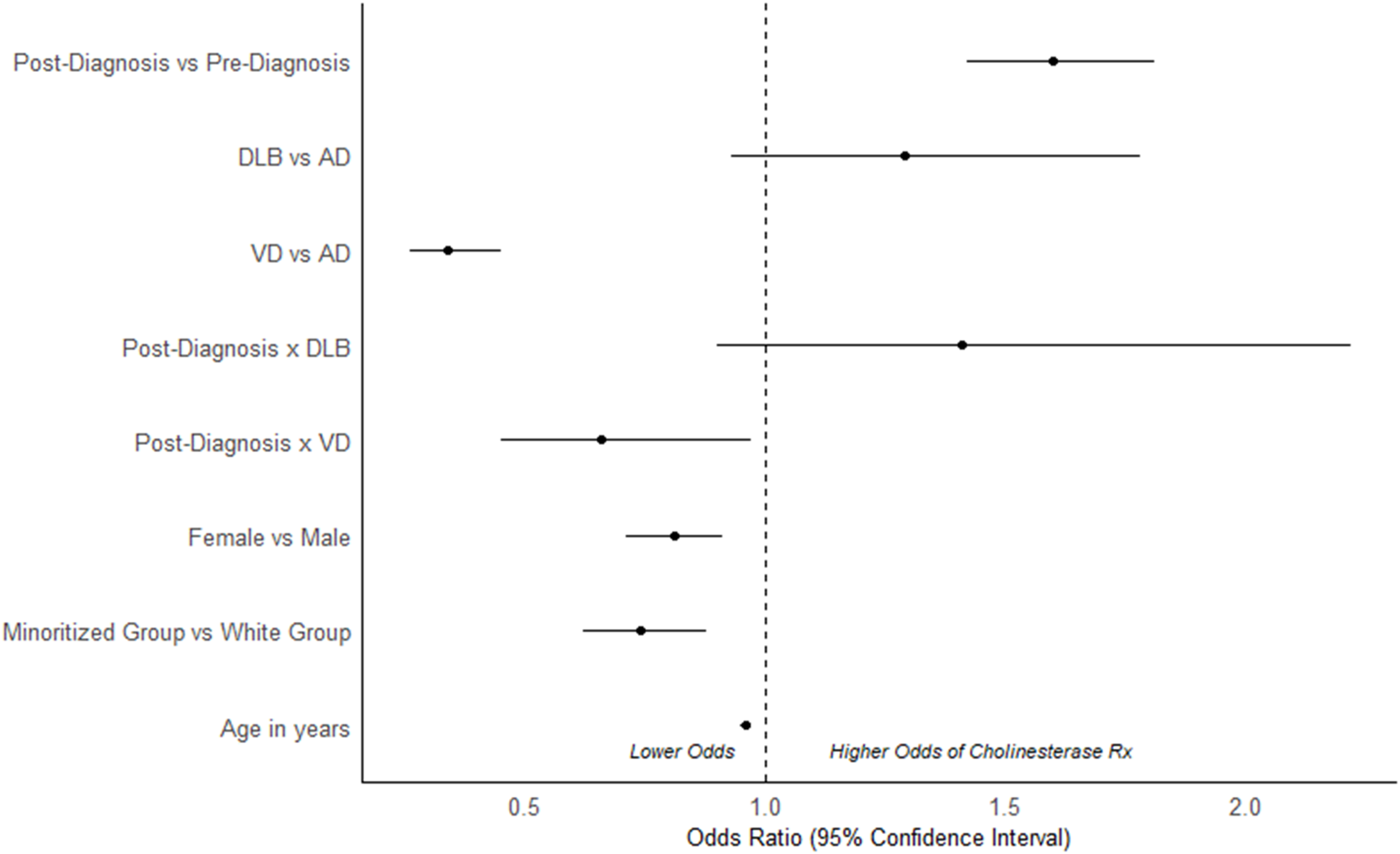
Odds ratios of ChEI prescription for each predictor variable. Forest plot of the OR and the corresponding 95% confidence intervals for the predictors of ChEI prescriptions, resulting from the regression analysis. AD: Alzheimer's disease; ChEI: cholinesterase inhibitor; DLB: dementia with Lewy bodies; VD: vascular dementia.
Odds of ChEI prescription for patients with dementia adjusted for sex, age, and race.
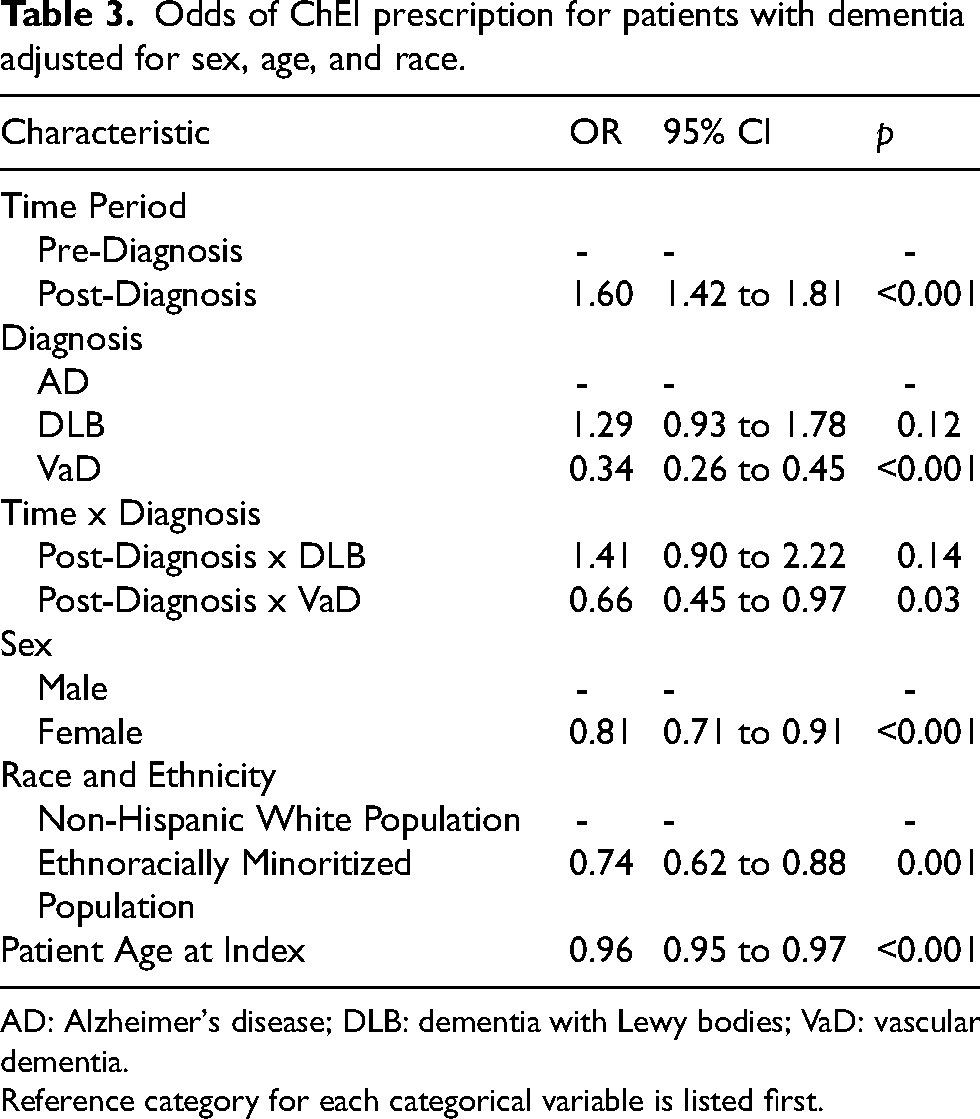
AD: Alzheimer's disease; DLB: dementia with Lewy bodies; VaD: vascular dementia.
Reference category for each categorical variable is listed first.
Discussion
In our cohort of patients diagnosed with AD, DLB or VaD, 65% of patients did not have a record of ChEI use, even after a diagnosis. Rates of ChEI fills increased the most after diagnoses of DLB followed by AD. ChEI fills increased only minimally after diagnoses of VaD (13% to 14%). The most common ChEI after dementia diagnosis was donepezil, followed by rivastigmine. Only a very small proportion of patients with AD filled orders for galantamine. Lastly, we found that patients who were older, female, and from ethnoracially minoritized groups were less likely to fill a ChEI prescription.
Fill rates of ChEIs for AD, DLB, and VaD were lower than expected considering the evidence supporting their use. Other studies have found ChEI therapy rates as high as 82% for patients with DLB and 74% for AD 25 as well as 42.6% for VaD. 26 Use of ChEIs in AD is supported by numerous clinical trials, and ChEIs are FDA-approved for mild, moderate, and severe AD.11,13 Although ChEIs are not approved in the US for the treatment of DLB, rivastigmine is FDA-approved for the treatment of Parkinson's disease dementia, and current evidence supports the use of ChEIs for DLB.14,27,28 Current evidence also supports the use of ChEIs in VaD 28 ; therefore, it is unexpected that prescription rates would be as low as 14% for patients with VaD following diagnosis. Possible reasons for low use of ChEIs include concerns about limited efficacy and tolerability. One review concluded that the use of ChEIs for individuals with mild to moderate AD leads to statistically significant, but clinically only marginal improvements for cognition and dementia severity. 29 A more recent review recognized the “modest but persistent cognitive benefits of [ChEIs]” and the evidence that they reduce caregiver burden. 30 Tolerability concerns could also lead to low prescribing: in one review, 80% of patients with DLB or Parkinson disease dementia experienced adverse events (AEs) related to ChEIs. 31 Additionally, 76% of individuals diagnosed with AD were found to have experienced at least one AE when using ChEIs with the most frequent AEs being nausea, vomiting, and diarrhea. 32 AEs were also found in higher frequencies among patients taking oral rivastigmine compared to the other ChEIs, resulting in 21% of participants withdrawing from studies. 32 While ChEI fill rates increased overall after diagnosis, a significant proportion of patients received ChEIs prior to their dementia diagnoses. Possible reasons for this include ChEI prescribing in the setting of uncharacterized cognitive changes, mild cognitive impairment, or an unspecified dementia diagnosis.
Our finding that donepezil was the most common ChEI across dementias is likely a result of its earlier approval, and efficacy and tolerability data among individuals with AD, DLB, and VaD support its use. Donepezil was the first ChEI approved in the US in 1996, four years before rivastigmine and five years before galantamine. Additionally, the safety and efficacy of donepezil have been investigated in the greatest number of studies.15,33 All three ChEIs are FDA-approved to treat patients with mild to moderate AD, but donepezil is the only ChEI approved to treat severe AD. While the majority of studies have been in AD, donepezil has been found to improve cognitive function, as measured by the MMSE, and behavioral and psychiatric symptoms in individuals diagnosed with DLB. 34 Donepezil also improved ADAS-Cog scores among patients with VaD. 35 Among ChEIs used to treat VaD, donepezil was found to be the most beneficial and least harmful while rivastigmine was the least beneficial and the most harmful. 12 Due to reduced gastrointestinal side effects over oral administration, 30 the rivastigmine transdermal patch, which entered the market in 2007, improved medication adherence.36–39 Caregivers also prefer the patch over an oral pill due to swallowing issues in older patients. 39 However, transdermal rivastigmine is associated with contact dermatitis unlike oral formulations. 40 Despite these potential advantages, we found relatively limited prescriptions for rivastigmine in our study cohort. Galantamine was not used among any patients with DLB or VaD in our cohort, which could be explained by its later approval and fewer clinical trials in these populations. Other factors influencing usage patterns among the ChEIs could be differences in cost and ease of administration.
We found disparities in ChEI prescriptions for patients with dementia who were older, female, and those who did not identify as White. A prior healthcare delivery study using Medicare beneficiary data similarly found that patients with dementia between the ages of 75 and 85 years or patients who identified as Black were less likely to be prescribed anti-dementia medications compared to patients identifying as Non-Hispanic White. 10 However, both Lu et al. and another study examining Medicare data found that female patients were more likely to be prescribed ChEIs.8,10 In contrast, we found that female patients were less likely to have fills for ChEIs. Other studies have also found that increased age is associated with lower ChEI prescribing rates, 41 but this effect is likely confounded by increasing comorbidities in older patients. 42 Because our sample was small and drawn from a healthcare system in the upper Midwest of the United States covering Minnesota and Western Wisconsin, with relatively little racial and ethnic diversity, individuals who did not identify as White were included together in one group for the purpose of statistical analysis. This less granular approach is a limitation and our results should be replicated in larger, more diverse samples. Reduced ChEI fills could be attributed to barriers to care43,44 or disparities in the accuracy of diagnosis 45 previously reported among minoritized populations. Cultural beliefs and attitudes may affect diagnosis and treatment due to variable perceptions of dementia and cultural caregiving patterns, 46 i.e., dementia is sometimes viewed as a natural progression of aging, which may discourage individuals from seeking medical help including for the treatment of dementia. 47
This study has several strengths. The analysis included a large sample size and spanned nearly seven years during which all three ChEIs were already approved by the FDA and available for prescribing. With the use of administrative claims data, we were able to ascertain prescription fill history rather than just prescriptions. However, unfilled prescriptions are not captured in the current analysis and there may be important differences between those who were prescribed a ChEI but did not fill prescriptions vs those who did. Further, we lacked information about the severity of dementia, tolerability of ChEIs, and long-term clinical outcomes.
Conclusions
Donepezil was the most frequently filled ChEI following a diagnosis of AD, DLB, or VaD. Patients with DLB had the highest prevalence of ChEI fills, even before a documented diagnosis of dementia. We found potential disparities in symptomatic treatment patterns. Older patients, females, and patients from ethnoracially minoritized groups were less likely to fill prescriptions for ChEI. This study expands the literature by providing new information about the patterns of ChEI fills for patients with dementia in the US. Our results highlight demographic groups that may benefit from interventions to improve access to care. Future studies should investigate larger, more diverse populations with respect to race, ethnicity, socioeconomic status, and geography to validate and expand our findings. If our findings are consistent in other healthcare settings, proposing and examining interventions is critical to reduce disparities in symptomatic treatment in clinical settings and improve care for patients with dementia.
Footnotes
Acknowledgements
The authors have no acknowledgments to report.
Ethical considerations
This study was approved by the Institutional Review Board at HealthPartners and was performed in accordance with the ethical standards as outlined in the 1964 Declaration of Helsinki.
Consent to participate
The HealthPartners Institutional Review Board approved waivers of consent for use of electronic medical records and claims data for patients who have not chosen to opt out of use of their data for research.
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Lewy Body Dementia Association and the NIH: R21AG074368 (K.W., A.W., R.R., M.B.), R01NS142622 (A.N., M.B.), 1R21AG077469 (A.N., M.B.), and R00AG073453 (E.B.). Other authors have no sources of funding to report.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data from this manuscript was obtained from HealthPartners and consists of electronic health records and claims data. Deidentified data may be accessed by contacting the primary author for a data-use agreement/provision, which requires the recipient to agree to use the data only for academic research. Custom code may be accessed by contacting the primary author.