
Abstract
Background
Repetitive behaviors (RB) are purposeless movements, speech, or routines performed without self-awareness or conscious intent.
Objective
The present study aims to investigate the prevalence and longitudinal changes of RB and to assess these symptoms in a large cohort of patients with frontotemporal lobar degeneration (FTLD)-associated syndromes using a newly developed caregiver-based questionnaire.
Methods
This was a longitudinal cohort study conducted in tertiary frontotemporal dementia research clinics. A total of 210 FTLD patients were included, 68 of whom had follow-up evaluation. RB were assessed through structured caregiver interviews. Compulsive/impulsive behaviors, stereotypies, and ritualistic behaviors were recorded. Univariate and multiple generalized linear models and generalized linear mixed models were used to estimate predictors and longitudinal changes associated with RB.
Results
RB were reported in 71% of patients, showing a progressive increase from the prodromal to moderate dementia stages. Notably, 30% of patients presented RB since the disease onset phase, especially in the form of compulsive/impulsive behaviors. Predictors included male gender, the behavioral variant of frontotemporal dementia and the semantic variant of primary progressive aphasia phenotypes, and higher scores on Frontal Behavioral Inventory scale, part B. A significant increase in total RB was observed in patients reassessed at 8 to 22 months follow-up from baseline (p = 0.0001), especially in the form of stereotypies and ritualistic behaviors.
Conclusions
The questionnaire developed in this study effectively captures the prevalence and progression of RB. It could contribute to the standardization of the behavioral assessment in FTLD clinical trials and, consequently, to a deeper understanding of these syndromes.
Keywords
Introduction
Repetitive behaviors (RB) represent a hallmark of many clinical syndromes associated with frontotemporal lobar degeneration (FTLD), yet remain underexplored. 1 These include a spectrum of symptoms, including compulsive/impulsive behaviors, stereotypies, and ritualistic behaviors.1–2 RB may be present since the prodromal stages, leading the way to FTLD diagnosis.1–2 RB encompass movements, speech, or routines that are performed repetitively without clear purpose or self-awareness, typically arising automatically and independently of anxiety or conscious intent. The whole RB spectrum ranges from symptoms without a significant clinical impact in daily life to those which cause severe distress in patients and their families, and therefore requiring medications or other non-pharmacological interventions, including institutionalization.3–5
RB can emerge at various stages of the disease, typically intensifying rapidly during prodromal and intermediate phases before plateauing or diminishing in later stages.6–7 Previous studies reported that, in longitudinal cohorts of dementia patients, several factors may influence the emergence of neuropsychiatric symptoms. These include sex, age, dementia severity, clinical phenotype, disease duration and general medical health. 8 However, no previous studies have specifically investigated the clinical features or possible risk factors associated with RB, which therefore remain incompletely understood. 9
The classification into compulsive, impulsive, and stereotyped behaviors emerged from previous literature indicating that RB arises from an altered integration of emotion, cognition, and behavior within the cortical–striatal–thalamic–cortical (CSTC) loops. Compulsive behaviors have been associated with dysregulation of affective and fronto-limbic circuits, impulsive behaviors with dysfunction of orbitofrontal-ventral circuits, and stereotyped behaviors with alterations in sensorimotor CSTC pathways.1,2,5,10,11
RB are listed in the diagnostic criteria of the behavioral variant frontotemporal dementia (bvFTD), defined as “early perseverative, stereotyped or compulsive behaviors,” 12 and are estimated to occur in up to 80% of patients. 1 High prevalence has also been widely reported in the semantic variant of primary progressive aphasia (svPPA), with an estimated 60% affected during the early phases, that increase until 75% one year after the diagnosis.1,6,10,13 However, data remain limited for other syndromes associated with FTLD, including the non-fluent variant of PPA (nfvPPA), the corticobasal syndrome (CBS), and the progressive supranuclear palsy (PSP).
In this view, the prevalence and characteristics of RB in the spectrum of syndromes associated with FTLD have not been thoroughly investigated using structured assessment tools. Such a tool would enhance our understanding of the prevalence of RB at different disease stages and in different clinical phenotypes, allowing the assessment of predictors of RB development, and a framework for future evidence-based interventions.
These observations provided the rationale for the present study aimed to a) develop a questionnaire for comprehensively assessing RB in a large cohort of patients with FTLD associated syndromes, b) investigate the prevalence of RB across clinical phenotypes and disease stages, c) identify RB-associated variables, and d) assess longitudinal changes of RB over time.
Methods
Participants
This longitudinal study enrolled patients with FTLD associated syndromes from the Neurocognitive and Behavioral Unit, University of Brescia and from Neurology Unit, University of Padua, Italy. All patients fulfilled current clinical diagnostic criteria for bvFTD, svPPA, and nfvPPA, and CBS or PSP.12,14–16 Patients with the right temporal variant of PPA were not a priori excluded or specifically differentiated from the svPPA group.
All patients underwent a comprehensive clinical evaluation, including neuropsychological and behavioral assessments, and standard structural neuroimaging to support syndromic classification. In cases with atypical clinical presentation, AD pathology was ruled out using cerebrospinal fluid biomarkers (Aβ1-42, p-tau181, and total tau) or amyloid PET imaging (florbetapir or flutemetamol tracers). Genetic screening was not systematically performed. Cases of inherited FTLD were confirmed via genetic screening for known monogenic mutations.
Family history of dementia was classified according to the modified Goldman score. A positive family history was defined as a score of 1 (autosomal dominant inheritance pattern) or 2 (three or more affected relatives), while a negative history corresponded to scores of 3 (one additional affected relative) or 4 (no family history). 17
Disease severity was assessed using the CDR Dementia Staging Instrument plus National Alzheimer's Coordinating Center Behavior and Language Domains (CDR® plus NACC FTLD) global score. Scores were categorized as prodromal (score=0.5), mild (score=1), moderate (score=2), or severe (score=3). 18
A structured caregiver interview, the Frontal Behavioral Inventory (FBI), was used to assess behavioral symptoms. Scores were computed for the negative behavior subscale (FBI-A), the positive behavior subscale (FBI-B), and the total score (FBI-AB). 19
All participants or their legal representatives provided written informed consent in accordance with the Declaration of Helsinki, and the study protocol received approval from the local Ethics Committee (NP 2189).
Assessment of repetitive behaviors (RB)
Several instruments have been employed to assess the prevalence of RB in FTD, including the Neuropsychiatric Inventory, 20 the Cambridge Behavioral Inventory, 21 the Stereotypic and Ritualistic Behaviors subscale 22 of the Stereotypy Rating Inventory. 23 These tools are validated and widely used in clinical practice, enabling cross-study comparability. However, they only partially capture the complexity and heterogeneity of RB in FTLD, particularly in early stages or across different clinical variants. Due to the absence of comprehensive, validated instruments specifically designed for the FTLD spectrum, we developed a novel questionnaire aimed at exploring and assessing a broader range of repetitive and ritualistic behaviors in patients with FTLD. The presence of such behaviors was evaluated through structured interview with a primary caregiver or close family member.
The questionnaire items were derived from behavioral categories previously reported in the literature as common in patients affected by FTLD, 1 and covered a broad spectrum of symptomatology. For the purposes of this study we grouped RB into three main categories, each of which included targeted questions addressing: a) compulsive/impulsive behaviors, such as excessive cleaning or washing, compulsive ordering or symmetry, repetitive checking or repetitive numbering, excessive alcohol or drug use, gambling, compulsive spending or shopping, pathological stealing, hypersexuality, binge eating, and pathological joking; b) stereotypies, such as hand rubbing, body rocking, lip-smacking, finger tapping, humming, and skin picking; c) ritualistic behaviors, including clock-watching, rigid routines, hoarding or restricted interests.
A specific question was formulated for each item as reported in Supplemental Material 1. During the caregivers′ interviews, simple but explicit examples were provided to ensure consistent interpretation of each behavior. To differentiate between compulsions and impulsions the experimenters followed a standardized description: compulsions were defined as repetitive actions not aimed at a specific goal that are often accompanied by a feeling of compulsion to act; conversely, impulsions were described as repetitive behaviors characterized by poor impulse control and a reduced capacity to delay gratification. Each item included a practical example (e.g. Does the patient engage in excessive cleaning or washing? For example: repeatedly washes hands, constantly cleans the house, etc.), which facilitated consistent understanding and differentiation of behavioral subtypes by caregivers.
This version of the questionnaire was not submitted for external expert review due to the exploratory nature of the study and the early stage of development. At this point, the focus was on ensuring content coverage and assessing feasibility through clinical use by experienced neuropsychologists.
Statistical analyses
Group differences in demographic and clinical features were examined using the Kruskal-Wallis rank sum test for continuous variables, and the chi-square test for categorical variables.
RB were considered individually as the sum of each individual behavior (i.e., number of compulsive/impulsive behaviors, the number of stereotypies, etc.). We also considered the composite index (i.e., the sum of compulsive/impulsive behaviors, stereotypies and ritualistic behaviors). Poisson regression models were used to examine the relationship between behavioral subtypes (modelled as count data) and clinical phenotype or dementia severity. Dementia severity was stratified using scores obtained at CDR® plus NACC FTLD with 0.5 indicating prodromal, 1 mild, 2 moderate, and >2 severe. Pairwise comparisons were adjusted using the Benjamini-Hochberg correction for multiple testing.
In addition, we explored the association between RB subtypes and several clinical and demographic variables, including sex, age, years of education, age at onset, FBI-A, FBI-B, Goldman’s score, and CDR® plus NACC FTLD. Each predictor was first tested in a univariate Poisson regression model. Predictors that reached statistical significance (p ≤ 0.05) were then included in the multivariable model. Before the analyses, all models were tested for overdispersion. When equidispersion was violated, zero-inflated Poisson (ZIP) models were applied.
Retrospective information on the presence and prevalence of RB during the disease onset phase was obtained from caregiver responses to a specific item in the questionnaire.
To assess longitudinal changes in RB, ZIP Generalized Linear Mixed Models (GLMMs) were used. Disease duration was expressed in months since symptom onset and categorized into tertiles (0–24 months, 24–42 months, 42–66 months, 66-144 months), allowing us to model potential non-linear associations with behavioral outcomes.
Similarly, another time-dependent analysis modelled time in months since first evaluation (T0), as the interval between T0 and T1 varied across individuals. To account for non-linear trajectories, time was categorized into tertiles (<8 months, 8–22 months, 22–37 months). In both analyses, we used GLMMs in which a random intercept for subject was included to account for within-subject correlations.
Longitudinal analyses were conducted on the participants who had complete data at both baseline and follow-up. Participants without follow-up data were excluded from these analyses. All statistical analyses were conducted using R, version 4.3.2. (https://www.r-project.org/).
Results
Participants and frequency of RB
A total of 210 patients (mean age: 68.26 ± 8.5 years, males: 57%) were included in the study. Demographic and clinical characteristic by clinical phenotype are reported in Table 1. For the purpose of the present study, CBS and PSP patients were grouped together.
Demographic and clinical characteristics of the group.
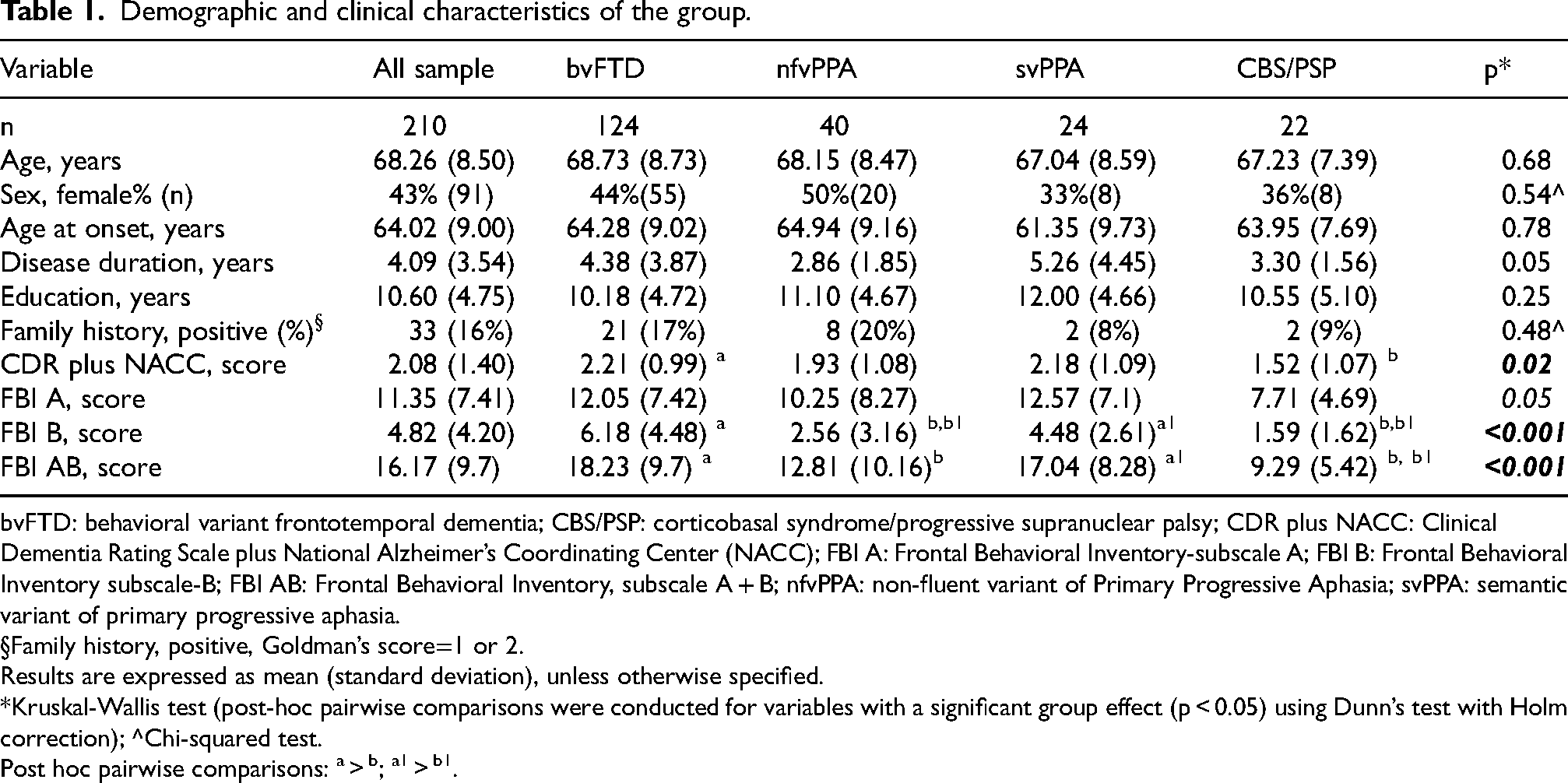
bvFTD: behavioral variant frontotemporal dementia; CBS/PSP: corticobasal syndrome/progressive supranuclear palsy; CDR plus NACC: Clinical Dementia Rating Scale plus National Alzheimer’s Coordinating Center (NACC); FBI A: Frontal Behavioral Inventory-subscale A; FBI B: Frontal Behavioral Inventory subscale-B; FBI AB: Frontal Behavioral Inventory, subscale A + B; nfvPPA: non-fluent variant of Primary Progressive Aphasia; svPPA: semantic variant of primary progressive aphasia.
Family history, positive, Goldman’s score=1 or 2.
Results are expressed as mean (standard deviation), unless otherwise specified.
*Kruskal-Wallis test (post-hoc pairwise comparisons were conducted for variables with a significant group effect (p < 0.05) using Dunn’s test with Holm correction); ^Chi-squared test.
Post hoc pairwise comparisons: a > b; a1 > b1.
Across the whole sample, 71% of FTLD patients reported at least one RB, with a mean of 1.83 RB per patient (SD = 1.87). Mean scores reflect the average number of behaviors per RB category, calculated across the entire sample. Specifically, 58% of patients exhibited at least one compulsive/impulsive behavior (1.00 ± 1.10), 25% showed stereotypies (0.31 ± 0.65), and 36% presented ritualistic behaviors (0.51 ± 0.80). These percentages refer to the presence of at least one behavior in each category and are not mutually exclusive, as many patients reported multiple RB types.
When stratified by dementia severity, overall RB were observed in 60% (mean scores: 1.50 ± 1.58) of patients tested that were in the prodromal stage at the evaluation (CDR=0.5), in 66% (1.43 ± 1.55) in the mild dementia stage (CDR=1), in 69% (2.21 ± 2.20) in the moderate stage (CDR=2) and in 78% (1.97 ± 1.86) in the severe stage (CDR=<2).
Overall RB were 62% more frequent in moderate stage compared to mild stage (ratio=1.62 [95% CI:1.05-2.48], p = 0.019). Among different RB, ritualistic behaviors were significantly different across dementia stages, being 93% more frequent in moderate dementia stage patients compared to mild stage patients (1.93 [0.96-3.86], p = 0.038), but also 90% more frequent in moderate stage patients compared to severe dementia stage (1.90 [0.99-3.67], p = 0.038) (see Figure 1).
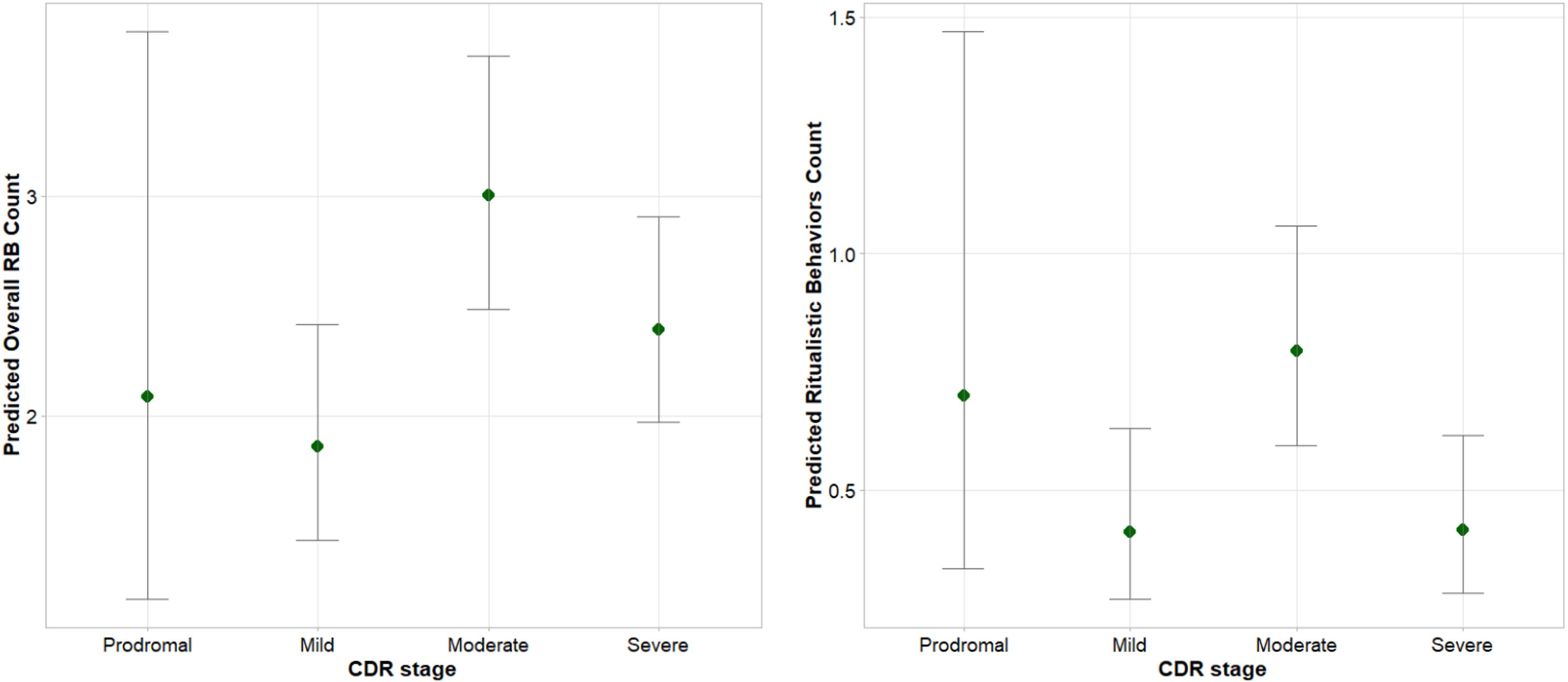
Prevalence of Repetitive Behaviors (RB) disaggregating by disease severity.
RB were reported in 80% (mean scores ± SD: 2.25 ± 1.96) of patients with bvFTD, 75% (2.25 ± 1.92) of patients with svPPA, 51% (0.75 ± 0.95) of patients with nfvPPA, and 48% (1.00 ± 1.48) of patients with CBS/PSP. Overall, RB were more frequent in bvFTD and svPPA than in nfvPPA (2.96 [1.72–5.12] and 3.07 [1.60–5.87], respectively, both p < 0.001) and CBS/PSP (2.03 [1.03–4.00], p < 0.001; 2.10 [0.98–4.51], p = 0.002). Compulsive/impulsive behaviors were more frequent in bvFTD and svPPA than in nfvPPA (3.64 [1.74–7.60], p < 0.001; 3.33 [1.41–7.91], p < 0.001), and were also more frequent in bvFTD and svPPA than in CBS/PSP (2.55 [1.12–5.80], p = 0.005; 2.33 [0.91–5.97], p = 0.02). Ritualistic behaviors were more frequent in bvFTD and in svPPA compared to nfvPPA (2.65 [1.05–6.73], p = 0.02; 3.52 [1.21–10.23], p = 0.01), and also more frequent in svPPA than in CBS/PSP (2.90 [0.84–9.99], p = 0.046) (see Figure 2).
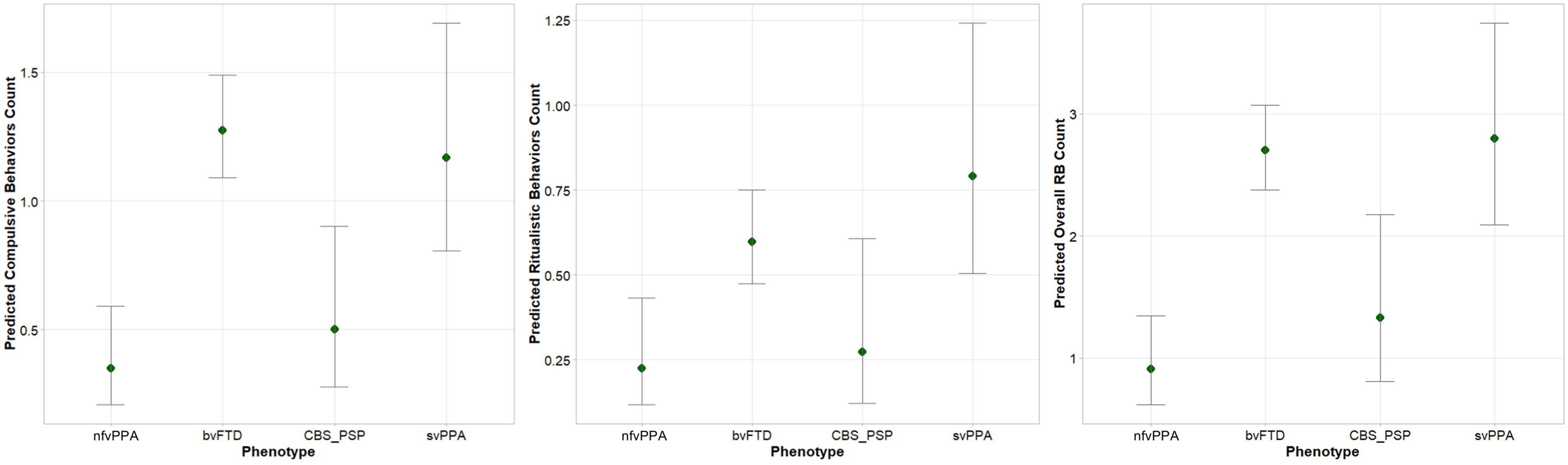
Prevalence of Repetitive Behaviors (RB) disaggregating by FTLD-associated syndrome.
Overall RB showed significant positive associations with other behavioral symptoms as measured by FBI scale. RB were associated, among others, with obsessions (τ=0.493, p = 3.90 × 10−13), impulsivity (τ=0.191, p = 0.010), and inappropriateness (τ=0.394, p = 3.41 × 10−8) of the FBI-B subscale, and with inflexibility (τ=0.239, p = 0.0009), inattention (τ=0.208, p = 0.004), and loss of insight (τ=0.158, p = 0.026) of the FBI-A subscale (see Supplemental Material 2).
RB at disease onset
In the overall sample, we also enquired about the presence of RB since the disease onset with a specific item in the questionnaire. RB were reported in 30% (62/206) of all patients. Specifically, 65% (40/62) had compulsive/impulsive behaviors, 10% (6/62) had stereotypies, and 26% (16/62) had ritualistic behaviors. Specifically, RB were observed in 74% (46/62) of patients with bvFTD, 11% (7/62) with nfvPPA, 10% (6/62) with svPPA, and 5% (3/62) with CBS/PSP.
Predictors of repetitive behaviors
Clinical phenotype (p = 2.82 × 10−6), male gender (1.35 [1.06-1.74], p = 0.004) and FBI-B (1.07 [1.04-1.10], p = 9.16 × 10−9) predicted the presence of RB in FTLD associated syndromes (see Table 2). When we considered clinical phenotype, bvFTD patients had significantly higher scores than nfvPPA (0.45 [0.25-0.80], p = 0.001) and CBS/PSP (3.10 [1.25-7.68], p = 0.001), and svPPA patients had significantly higher scores than nfvPPA (0.40 [0.20-0.77], p = 0.001) and CBS/PSP (0.28 [0.11-0.74], p = 0.001).
Demographic and clinical predictors associated with the presence of RB.
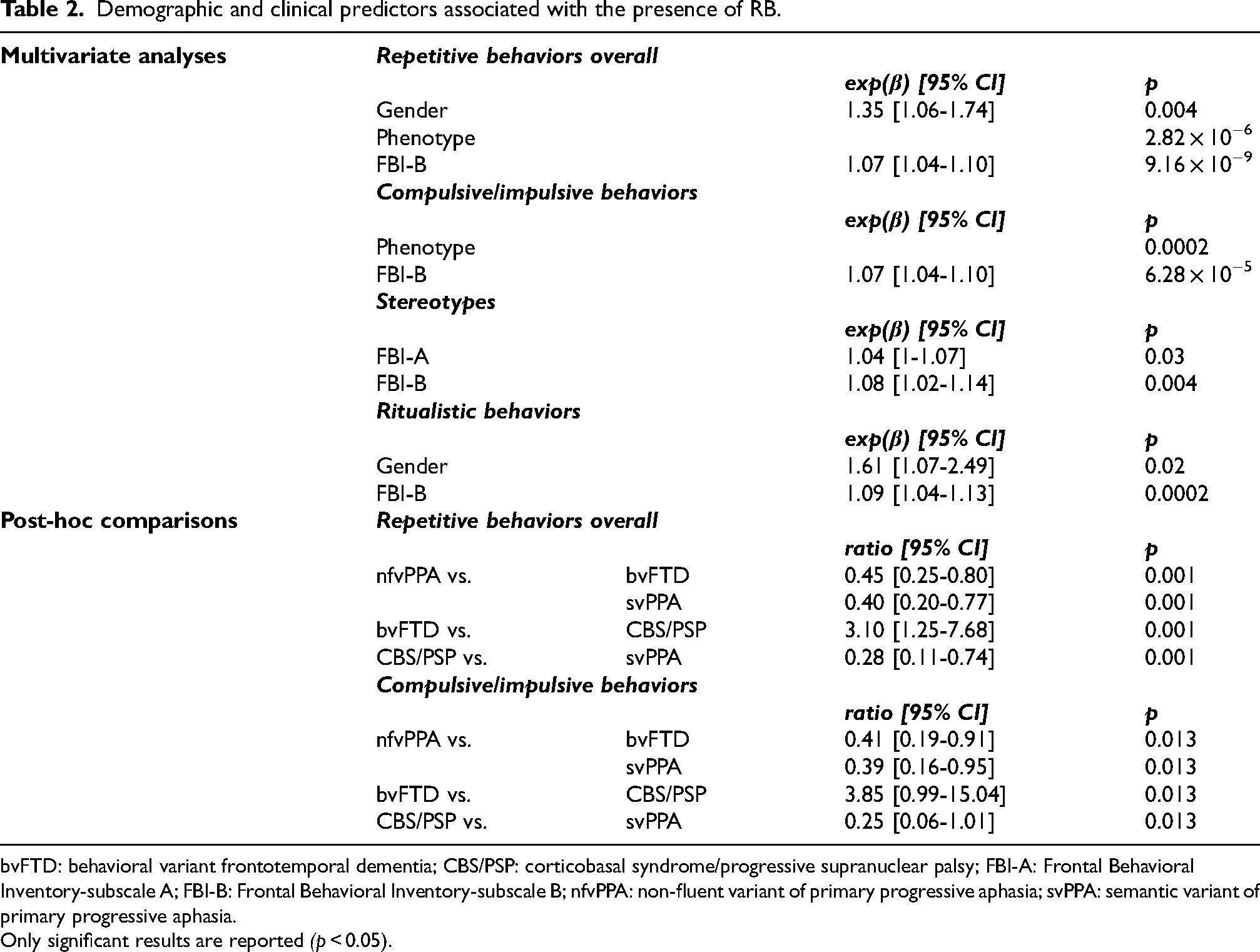
bvFTD: behavioral variant frontotemporal dementia; CBS/PSP: corticobasal syndrome/progressive supranuclear palsy; FBI-A: Frontal Behavioral Inventory-subscale A; FBI-B: Frontal Behavioral Inventory-subscale B; nfvPPA: non-fluent variant of primary progressive aphasia; svPPA: semantic variant of primary progressive aphasia.
Only significant results are reported (p < 0.05).
When we considered compulsive/impulsive behaviors, we observed a significant effect of clinical phenotype (p = 0.0002) and of FBI-B score (1.07 [1.04-1.10], p = 6.28 × 10−5). Post-hoc comparisons showed that bvFTD patients reported significantly increased scores than nfvPPA (0.41 [0.19-0.91], p = 0.013) and CBS/PSP (3.85 [0.99-15.04], p = 0.013), similarly to svPPA patients which scores were increased than nfvPPA (0.39 [0.16-0.95], p = 0.013) and CBS/PSP (0.25 [0.06-1.01], p = 0.013) (see Table 2).
Stereotypies were associated with FBI-A (1.04 [1-1.07], p = 0.03) and FBI-B (1.08 [1.02-1.14], p = 0.004). Ritualistic behaviors were significantly associated with male gender (1.61 [1.07-2.49], p = 0.02) and FBI-B (1.09 [1.04-1.13], p = 0.0002) (see Table 2).
RB in relation to disease duration
We next analyzed how the frequency of RB varied across the disease course. We observed a significant increase in overall RB (2.05 [1.27–3.31]; p = 0.009) between the early disease stage (0–24 months from onset) and the advanced stage (42–66 months from onset). Compulsive/impulsive behaviors also showed a significant increase during this time frame (2.07 [1.17–3.67]; p = 0.039), contributing to the overall increase in RB. From symptoms onset, the mean interval between baseline and follow-up assessments was of 48 (SD = 30.2) months (Figure 3). No significant differences were found between the other disease stages.
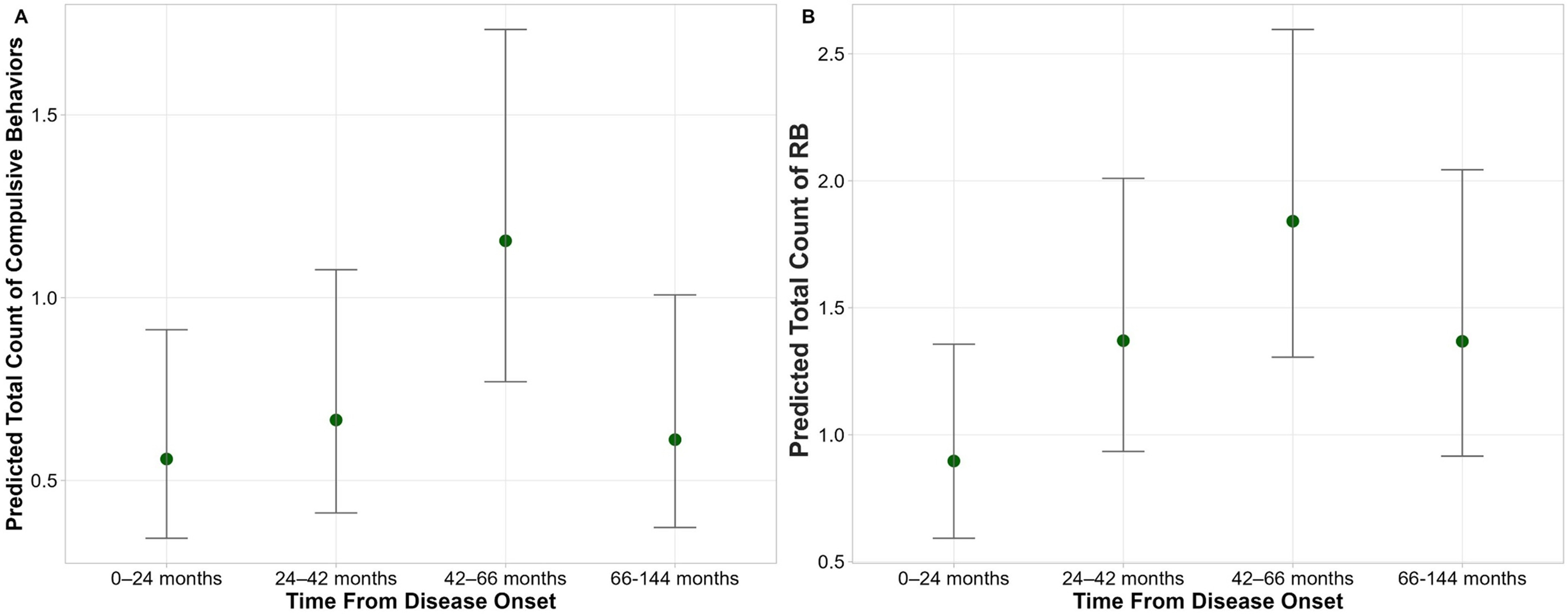
Changes in the prevalence of Repetitive Behaviors (RB) in relation to disease duration considering (A) compulsive/impulsive behaviors and (B) overall RB.
Longitudinal changes of RB
We examined whether the number of RB changed over time between the baseline and follow-up assessments. The only significant difference between the patients with and without follow-up concerned education (p = 0.034) (Supplemental Material 3). The mean interval between baseline and follow-up assessments was 16.1 (11.5) months. A significant increase in total RB was observed in patients reassessed at 8 to 22 months follow-up from baseline (2.07 [1.43-3.01], p = 0.0001). This increase mainly depended on stereotypies (3.19 [1.46-6.98], p = 0.004), and ritualistic behaviors (2.28 [1.16-4.48], p = 0.02) (Figure 4).
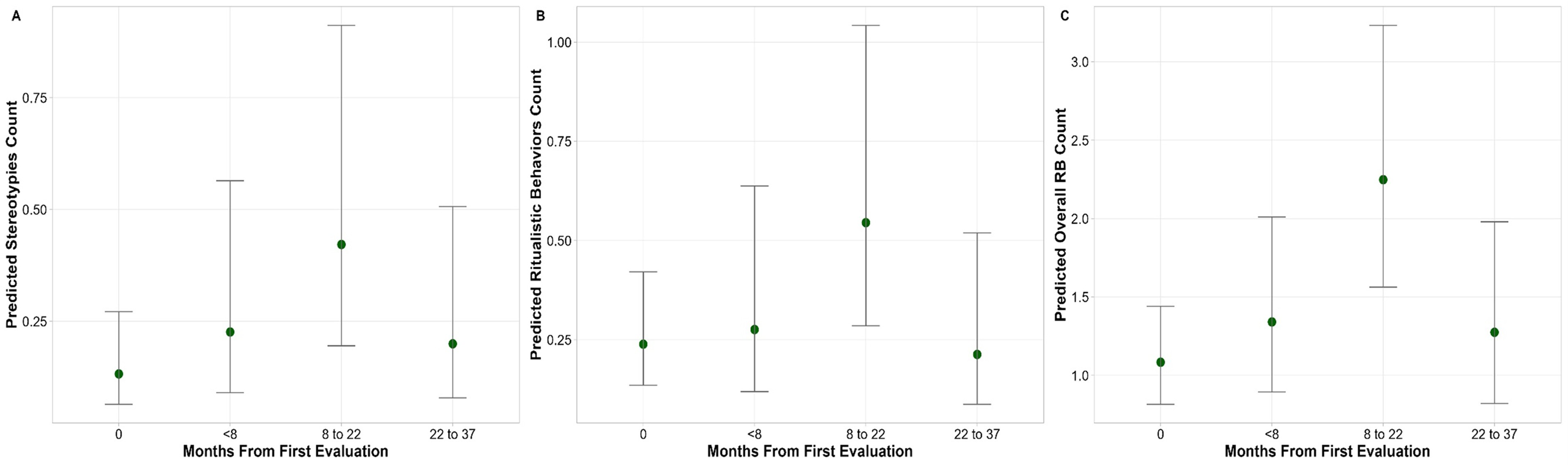
Changes in the number of Repetitive Behaviors (RB) between baseline and follow-up evaluations.
Discussion
In our cohort, 71% of patients exhibited at least one RB, particularly compulsive/impulsive behaviors. These behaviors were observed in 60% of patients during the prodromal stage (CDR = 0.5). The prevalence of RB increased progressively across dementia stages, reaching 78% in the severe stage. However, when analyzing frequency scores, RB were significantly more frequent in the moderate stage compared to both the mild and severe stages of the disease. This pattern is in line with previous literature describing a rise in RB until intermediate stages, followed by a decline in later phases.6–7 A hypothesis for explaining this phenomenon could be that, in the early stages of the disease, dysfunction within orbitofrontal and anterior cingulate cortices may promote disinhibition and impulsive–compulsive behaviors, while in later stages, widespread cortical and subcortical degeneration—also affecting premotor and supplementary motor areas—may limit the ability to initiate or sustain such behaviors. Notably, 30% of the caregivers reported RB since the disease onset, consistent with the high prevalence observed in the symptomatic disease and reinforcing their relevance as early diagnostic marker, in line with the ‘mild behavioral and/or/cognitive impairment in bvFTD’ (MBCI-FTD) framework. 2
Furthermore, RB were frequent not only in bvFTD, as expected, but also in svPPA. The significantly higher prevalence of RB in svPPA supports the hypothesis that these behaviors may be intrinsic to the clinical picture of svPPA and might be included in future revisions of the diagnostic criteria.1,6,10,13 Interestingly, nearly half of patients with nfvPPA and CBS/PSP exhibited at least one RB during disease, supporting this key feature across syndromes associated with FTLD.
Predictors of RB included clinical phenotype, scores on the FBI-B subscale, and male gender. The influence of clinical phenotype is consistent with the significant differences in RB prevalence observed across diagnostic groups, as confirmed by post-hoc comparisons. The association with FBI-B scores likely reflects the fact that this subscale partly captures positive behavioral symptoms, 19 as further supported by the association with specific FBI-B subitems, such as impulsivity and inappropriateness. 24 Gender also emerged as a relevant factor, with male patients showing a higher likelihood of exhibiting RB. This may partly be explained by the higher prevalence of bvFTD among men—a clinical phenotype typically associated with greater RB occurrence. 25 However, this association warrants further investigation to determine whether RB in women may appear in milder form or may even go under-recognized. 26 At the symptom subtype level, compulsive/impulsive and ritualistic behaviors were the main contributors to overall RB, with compulsive/impulsive behaviors specifically guiding the early increase observed from disease onset. In contrast, stereotypies were significantly associated with FBI-A scores, aligning with prior findings reporting increased simple motor stereotypies in apathetic FTD subtypes. 13
Even though RB play a central role in the FTLD syndromes, they remain relatively under-investigated, highlighting the need for a comprehensive and unique tool to consistently assess their prevalence. 1 RB can manifest as a wide spectrum of symptoms, including compulsive/impulsive behaviors, stereotypies, or ritualistic routines.1,3–5 Those behaviors have been shown to be associated with alterations in the CSTC loops that mediate motor and behavioral inhibition. Those neural alterations are hypothesized to disrupt the integration of emotion, cognition, and behavior, ultimately contributing to the emergence of RB.1,27–29
Finally, longitudinal data revealed an increase in RB between 8 and 22 months after the baseline, particularly in the form of stereotypies and ritualistic behaviors.
Given the heterogeneity of our sample and the study’s preliminary nature, analyses of internal consistency, item-level analysis, inter-rater reliability, or construct validity were not conducted. Cross-site reproducibility will be tested by replicating the questionnaire in independent FTLD cohorts from different clinical centers.
We acknowledge that this study entails limitations. First, the evaluation is based upon a caregiver-reported questionnaire which, although administered by expert neuropsychologists, may be subjected to misinterpretation or individual variability. Moreover, the binary present/absent structure may fail to capture the full range and nuance of RB symptoms. Second, longitudinal analyses were based on a subset of the cohort (n = 68), a factor that may have limited the statistical power to detect small-to-moderate within-group changes, particularly when stratified by clinical phenotype. Moreover, this reduced sample size may also have introduced a selection bias. Heterogeneity in disease duration and progression across clinical syndromes could have influenced the expression of RB, limiting the possibility of differentiating between syndrome-specific features and severity-related effects. Third, interventional therapies were not considered in the present study. Nonetheless, a key strength of this study is the use of a newly developed tool designed to systematically assess RB in a large cohort of patients, its focus on the whole FTLD spectrum rather than only on specific syndromes, and the large sample size.
In conclusion, this study expanded the current knowledge on RB across FTLD-associated syndromes. Our questionnaire appears to effectively capture the prevalence and progression of RB, and may serve as a valuable instrument for standardizing data collection in clinical and research settings. Future studies should further broaden the sample, explore the role of RB as early clinical markers across the FTLD spectrum, as well as their potential as targets of evidence-based effective interventional strategies. Finally, particular attention will have to be paid to potential gender-related differences in the expression of RB, considering that RB in women may be under-recognized due to sociocultural expectations or reporting biases.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261418302 - Supplemental material for Repetitive behaviors in syndromes associated with frontotemporal lobar degeneration
Supplemental material, sj-docx-1-alz-10.1177_13872877261418302 for Repetitive behaviors in syndromes associated with frontotemporal lobar degeneration by Maria Sofia Cotelli, Valeria Bracca, Davide Fasolato, Andrea Geviti, Alberici Antonella, Annachiara Cagnin and Barbara Borroni in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
The authors have no acknowledgments to report.
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki, and the study protocol received approval from the local Ethics Committee (NP 2189).
Consent to Participate
All participants or their legal representatives provided written informed consent in accordance with the Declaration of Helsinki.
Consent for Publication
Not applicable
Author Contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Italian Ministry of Health (Ricerca Corrente).
Declaration of Conflicting Interests
Barbara Borroni served as a medical advisor for Alector, Denali, Wave, AviadoBio, Lilly, and UCB.
The other authors report no conflicts with any product mentioned or concept discussed in this article.
Barbara Borroni is an Editorial Board Member of this journal but was not involved in the peer-review process of this article nor had access to any information regarding its peer-review.
Data Availability Statement
The data supporting the findings of this study might be available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.