
Abstract
This article synthesizes key themes emerging from the CTAD 2025 meeting, highlighting significant advances in Alzheimer's disease (AD) research and clinical practice. New disease-modifying approaches—ranging from next-generation anti-amyloid-β and anti-tau antibodies to small-molecule aggregation inhibitors and gene-based strategies—underscore a growing shift toward multi-target therapeutic frameworks. Blood-based biomarkers, such as p-tau217, p-tau181, glial fibrillary acidic protein, and neurofilament light, are nearing clinical readiness, while digital biomarkers and wearable technologies are enabling remote, continuous assessment of cognitive and physiological functions. Clinical trial design is increasingly oriented toward earlier disease stages and genetically or biomarker-defined high-risk groups, incorporating adaptive methodologies and real-world data to enhance efficiency and generalizability. Collectively, these developments signal an impending transition over the next two to three years from a centralized, cognitive scale–driven model of AD care to a more decentralized, biomarker-guided precision paradigm. CTAD 2025 thus marks a pivotal inflection point in the evolving structure of AD diagnosis and treatment.
Keywords
Introduction
The Clinical Trials on Alzheimer's Disease (CTAD) meeting has become one of the most influential annual forums worldwide for advances in Alzheimer's disease (AD) therapeutics and clinical research. 1 It convenes leading groups from neuroscience, clinical trial methodology, drug development, and digital medicine. 2 The data released, ranging from novel therapeutics to innovative trial designs and translational tools, often shape global AD clinical programs and regulatory thinking in subsequent years. 3 As such, CTAD is increasingly viewed as a barometer for emerging research directions and technological shifts in the field. 4
The 2025 meeting is particularly notable, occurring at a moment when several significant developments are reaching pivotal inflection points. Disease-modifying therapies (DMTs), particularly anti-amyloid-β (anti-Aβ) antibodies, have entered the post-approval real-world evidence phase, prompting a reevaluation of their positioning, safety profiles, and implementation strategies. 1 At the same time, the rapid maturation of blood-based biomarkers has brought early diagnosis and trial stratification to the threshold of routine clinical adoption. 5 In parallel, artificial intelligence–assisted imaging, wearable devices, and multimodal digital phenotyping have been increasingly integrated into mainstream clinical trial infrastructures, reshaping approaches to disease monitoring, endpoint quantification, and participant management.6,7 Collectively, these developments are expanding the technical and conceptual boundaries of AD research.
Against this backdrop, the present review synthesizes overarching trends emerging from CTAD 2025, including the evolution of therapeutic strategies, the restructuring of biomarker frameworks, and the expanding role of digital methodologies in clinical trials. Rather than cataloguing individual datasets, we highlight the broader patterns and forward-looking signals embedded within the meeting's content. We aim to provide researchers and clinicians with a concise overview of the key directions identified at CTAD 2025 and to serve as a reference point for future investigations.
Overview of conference highlights
Progress in new disease-modifying treatments
CTAD 2025 highlighted an apparent broadening of the therapeutic landscape for DMTs. Research efforts are expanding beyond traditional Aβ targets to encompass tau-directed strategies, immune modulation, and gene-level interventions, reflecting a more multidimensional and mechanistically diverse approach to AD therapy. 8
A prominent focus of the meeting was the advancement of next-generation anti-Aβ monoclonal antibodies. 9 Compared to earlier agents, these antibodies are engineered to bind selectively to pathogenic conformations, such as oligomers and protofibrils, while enhancing peripheral clearance and central target engagement. A recurring theme was the shift away from pursuing maximal Aβ removal toward balancing efficacy with a lower risk of amyloid-related imaging abnormalities, thereby broadening suitability for early-stage populations.1,2 Several groups also discussed reduced dosing or more flexible administration strategies to support long-term adherence in real-world settings.
Tau-targeted therapeutics showed a notable transition toward “network-level modulation”. 10 Rather than focusing solely on inhibiting aggregation of a specific tau species, emerging approaches aim to impede transneuronal spread, enhance axonal transport, or stabilize microtubule dynamics. Although most programs remain in critical developmental stages, accumulating evidence suggests a potential role for tau therapies in early intervention, particularly when combined with anti-Aβ antibodies, thereby strengthening discussions on multi-mechanism combination strategies. 11
Small-molecule approaches, targeting protein misfolding, toxic oligomer formation, or mitochondrial stress, also gained visibility. Their advantages include oral administration, lower cost, and scalability in diverse clinical environments. Several speakers suggested that small molecules may ultimately serve as key components of future combination regimens that integrate antibodies and oral agents.
Immune and microglial targets represented another area of emphasis. Work involving TREM2, CSF1R, and related pathways is shifting from simple up- or downregulation toward functional reprogramming of microglia. 12 Strategies aimed at enhancing metabolic capacity, modulating activation states, or improving neuron–glia interactions indicate that “immune microenvironment rebalancing” is emerging as an increasingly important direction in AD DMT development.
Gene-level interventions also showed more pragmatic momentum. Updates included vector-based expression systems, gene-regulatory enhancers, and RNA-targeted approaches related to APOE2. Investigators emphasized that these strategies may demonstrate clinical relevance first in genetically defined or ultra-early populations. Although still in early development, they underscore the potential to address AD risk at its biological roots.
Taken together, the DMT landscape presented at CTAD 2025 reflects a shift away from single-target breakthroughs toward a more precise, earlier-stage, and mechanistically integrated therapeutic framework. This evolution represents an important step toward transitioning AD treatment from isolated interventions to coordinated, multi-strategy management. 13
Blood biomarkers as “quasi-clinical standards”
Blood biomarkers have rapidly advanced in recent years and further solidified their role as core tools for stratification and diagnosis in AD at CTAD 2025. Large, multi-center cohorts from North America and Europe consistently demonstrate that p-tau217, p-tau181, glial fibrillary acidic protein (GFAP), and neurofilament light (NfL) are highly stable and reproducible across platforms and disease stages. Notably, p-tau217 has achieved performance closest to that of positron emission tomography (PET) imaging as a surrogate marker. 14 Multiple summary analyses emphasized that these blood-based measures can not only differentiate AD from non-AD dementias with high accuracy but also predict disease progression, supporting their gradual emergence as “quasi-clinical standards”.
A key trend highlighted at the meeting was the increasing regulatory readiness of blood biomarkers. Specific assay platforms have entered the FDA pre-submission stage and are already being employed for high-risk screening, trial subject stratification, and longitudinal risk monitoring in real-world studies. 15 Reflecting this shift, an increasing number of early intervention trials have incorporated blood p-tau and NfL as inclusion criteria or secondary endpoints, indicating that conditions for reducing or replacing PET dependency are steadily advancing.
Despite these advances, significant gaps remain between laboratory development and routine clinical implementation. Challenges such as cross-platform standardization, batch variability, threshold harmonization, and population applicability persist, and performance data in Asian, Hispanic, and other ethnic groups remain limited. Furthermore, real-world confounders, including comorbidities, renal function, and inflammatory status, require long-term evaluation to understand their impact on biomarker reliability fully.
Overall, CTAD 2025 marks a pivotal moment in the evolution of AD blood biomarkers from research tools to potential clinical standards, while underscoring the need for further regulatory validation and global harmonization before their broad clinical adoption. 13
Innovation in diagnostic technology: AI, digital biomarkers, and wearable devices
A prominent theme at CTAD 2025 was the rapid evolution of diagnostic technology from traditional laboratory-based models toward continuous monitoring, remote collection, and AI-driven prediction. The findings presented highlight a clear shift in AD diagnosis and risk stratification—from single, point-in-time assessments to highly personalized, dynamic disease-monitoring systems.
First, AI models for predicting cognitive decline have reached a substantial level of maturity. Several teams reported using machine learning algorithms trained on large-scale clinical cohorts that integrate blood biomarkers, demographic variables, longitudinal cognitive scores, and wearable device data to estimate the probability of cognitive decline over 2–5 years. 16 Compared with conventional statistical approaches, these models demonstrate enhanced sensitivity in early-stage populations, particularly for identifying the fastest-progressing subgroups in preclinical AD. Such models are increasingly used to stratify enrollment in early intervention trials, becoming a central component of precision medicine strategies.
Second, smartphone-based cognitive assessment tools emerged as a key highlight. Multiple studies presented at CTAD 2025 demonstrated that brief, daily self-administered tests, such as numerical memory, reaction time, and verbal fluency tasks, can capture subtle cognitive changes at high frequency, often outperforming traditional in-person assessments in terms of sensitivity. 17 The ecological validity of mobile cognitive tasks continues to improve, supporting their potential use as endpoints in clinical research and as remote preliminary screening tools for large populations.
Wearable devices also showed significant promise, particularly in monitoring sleep architecture, gait parameters, and heart rate variability. Reports from the meeting underscored growing correlations between these digital biomarkers and AD pathology, including Aβ and tau deposition and NfL levels: (1) sleep disturbances reflect early cortical amyloid accumulation; (2) micro-changes in gait correlate with parietal-basal ganglia network degeneration; (3) reductions in heart rate variability may indicate early autonomic dysfunction. As sampling frequency, algorithm accuracy, and long-term compliance improve, these wearable-derived signals are moving from exploratory markers toward regulatory evaluation readiness.
Additionally, remote biological sample collection has progressed from laboratory validation to large-scale feasibility. Multi-center consistency for dried blood spot assays of p-tau and GFAP has markedly improved, enabling a “home collection plus mail-in analysis” model. Integrated with digital data streams, this approach enhances accessibility for longitudinal studies and reduces trial costs.
Collectively, CTAD 2025 illustrates the emergence of a “new diagnostic ecosystem” for AD: AI supports prediction and stratification, mobile devices capture high-frequency behavioral indicators, wearables provide continuous physiological monitoring, and remote sampling complements molecular-level data. The integration of these technologies promises an earlier, more sensitive, and real-world–aligned approach to AD diagnosis. 13
New trends in clinical trial design
CTAD 2025 clearly highlighted that clinical trial design in AD is undergoing a structural transformation, with study populations, endpoints, enrollment strategies, and research frameworks all moving toward earlier, more precise, and real-world–aligned approaches. Several key trends presented at the conference are likely to define global AD clinical research over the next 3–5 years.
First, trials targeting early populations (preclinical AD, Stage 1–2) have expanded significantly. As blood biomarkers such as p-tau217 and GFAP, along with digital endpoints, mature, more interventions are being moved to the pre-symptomatic stage. Multiple presentations emphasized that pathological progression in preclinical populations is highly predictable, allowing small, short-term trials to detect subtle pathological and functional changes. 18 This trend translates “ultra-early intervention” from a theoretical concept into a feasible trial paradigm, potentially informing regulatory pathways for even earlier patient inclusion.
Second, precise enrollment of high-risk populations has become a hallmark of trial design in 2025. APOE4 carriers, blood biomarker–positive individuals, and digital biomarker subgroups signaling rapid progression are increasingly targeted. Several studies demonstrated the use of composite risk algorithms, combining blood biomarkers, genetic risk, and digital behavioral data, to identify the 10–20% of participants most likely to progress quickly, thereby reducing sample size and improving efficiency. Such strategies not only enhance trial success rates but also enable analysis of individualized treatment effects.
Third, run-in periods and adaptive trial designs have gained prominence. Run-in phases are widely used in early- and mid-stage trials to stabilize baseline variability, assess compliance, and evaluate the reliability of digital endpoints, ensuring robust data before randomization. Adaptive designs demonstrated at CTAD 2025 included dose adjustments, subgroup enrichment, and early futility analyses, enabling trials to optimize their approaches based on interim results dynamically. 19 These approaches are particularly valuable in next-generation antibody and small-molecule trials, where disease-modifying therapies are costly, and response variability is high.
Finally, real-world data and pragmatic trials are emerging as complementary strategies. US and European teams showcased approaches that leverage health system databases, routine clinical blood markers, high-frequency wearable data, and home sample collection to construct “trial-like” cohorts in real-world settings. Compared with conventional randomized clinical trials, these studies emphasize generalizability, cost-effectiveness, and practical effectiveness. As DMTs enter clinical practice and reimbursement systems, pragmatic trials will play an increasingly important role in assessing long-term efficacy, safety, and treatment adherence. 13
Overall, CTAD 2025 demonstrates that AD trials are evolving from a traditional pathology-centered model to a comprehensive framework that integrates pathology, physiology, behavior, and digital biomarkers. Designs that are earlier, more precise, flexible, and real-world–aligned will fundamentally shape the evidence generation pathways for future AD treatment strategies.
Comorbidities, accessibility, and clinical translation challenges
CTAD 2025 highlighted that as DMTs gradually enter routine clinical practice, the AD treatment system faces multiple challenges, including the management of comorbidities, access to treatment, reimbursement structures, and ethical considerations. Addressing these challenges is crucial to ensure that new therapies benefit the broadest patient population.
First, differences in treatment response among older adults and individuals with multiple comorbidities received significant attention. Real-world evidence indicates that the risk–benefit profiles for patients with cardiovascular disease, chronic kidney disease, diabetes, or those on anticoagulants may diverge substantially from those observed in clinical trials of anti-Aβ and other DMTs. 20 Presenters emphasized that future treatment strategies will require refined risk-stratification models to assess the risk of intracerebral hemorrhage, inflammatory responses, drug clearance, and cognitive outcomes across comorbidity subgroups. Moreover, comorbidities should be considered “biological interacting factors” that influence disease progression, rather than merely exclusion criteria, thereby enhancing the translational relevance of clinical trials.
Second, racial and socioeconomic disparities remain core barriers to equitable treatment. Multi-center international data presented at CTAD 2025 revealed systematic differences among ethnic groups in baseline biomarker levels, PET positivity thresholds, APOE4 distribution, and risks of DMT-related adverse events. 21 At the same time, economic burdens, frequent infusion requirements, and uneven access to imaging and laboratory infrastructure contribute to a persistent “treatment gap.” The conference emphasized the importance of incorporating health equity measures into future trials and regulatory pathways, including multi-ethnic, calibrated biomarker reference ranges, cost-effective testing platforms, and community-level engagement strategies.
Third, integration of DMTs into healthcare and reimbursement systems remains a critical bottleneck. Several teams highlighted that, despite proven efficacy, the high costs, intensive monitoring (e.g., MRI, safety labs), and frequent follow-up requirements could strain healthcare resources. 22 Simulations in US and European health systems suggested that without optimized workflows and resource allocation, drugs may be approved yet remain inaccessible to patients. Proposed solutions include low-cost monitoring pathways, hybrid care models, and AI-assisted risk stratification using blood biomarkers to improve efficiency and resource utilization.
Finally, ethical considerations are increasingly prominent in the era of early DMT and widespread screening. Blood biomarkers can identify AD risk in asymptomatic individuals, raising concerns about overdiagnosis, psychological burden, and unnecessary interventions. 23 CTAD 2025 emphasized that future ethical frameworks should define appropriate screening populations, establish informed communication standards, provide risk–benefit explanation models, and ensure privacy protections for high-risk individuals. Scientific progress should not compromise mental health or equity.
In summary, CTAD 2025 demonstrates that scientific breakthroughs in AD must be pursued alongside robust comorbidity management, equitable access, streamlined reimbursement, and ethical governance. Only through the concurrent advancement of innovation and system-level reform can DMTs be translated into broadly accessible clinical benefits.
Summary: forward-looking trends of CTAD 2025
The advances presented at CTAD 2025 not only continue the scientific progression of AD research but also clarify key directions for future clinical and research development, reflected in the following trends:
① Treatment strategies: A shift from single-target therapies (e.g., Aβ or tau) toward multi-pathway, multi-target combination approaches is evident, aiming to address the complex pathology and heterogeneity of AD. ② Diagnostic methods: Traditional PET imaging is gradually being complemented or replaced by blood biomarkers, enhancing the accessibility of early diagnosis while reducing costs and invasiveness. ③ Clinical trial design: Trials are transitioning from institution-centered models to decentralized, remote frameworks, incorporating smart devices and home sampling to facilitate broader, more efficient participant coverage. ④ Endpoints: The focus is expanding from single cognitive scales to include digital cognitive assessments and biomarker-based endpoints, improving sensitivity and the detection of early signals. ⑤ Research strategies: There is a clear move toward precision medicine for subgroups, leveraging multidimensional data, including genotype, blood biomarkers, and lifestyle factors, for precise enrollment and personalized interventions in high-risk populations. ⑥ Overall trend: Treatment, diagnosis, trial design, and research strategies are converging into an integrated, refined paradigm that supports early intervention and accelerates the clinical translation of AD therapies.
CTAD 2025 thus underscores a critical inflection point in AD research and care, laying a strong foundation for the next generation of clinical and translational advancements. The key developments and forward-looking trends highlighted at CTAD 2025 are summarized in Table 1 and Figure 1, providing a concise overview of how current research is translating into clinical and trial innovations in AD. All trends were summarized from CTAD 2025 presentations and official abstracts.
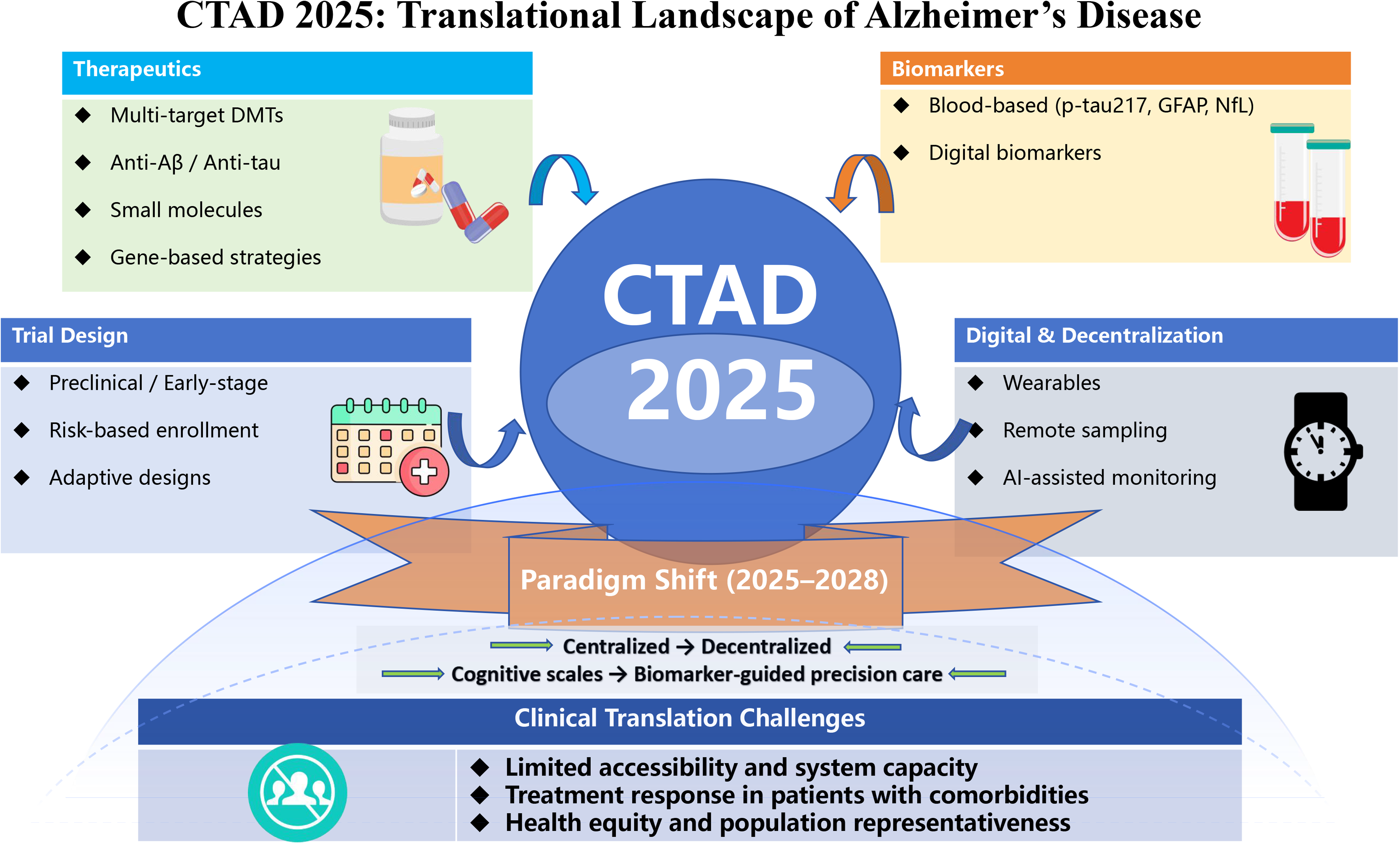
Schematic overview of the major translational themes highlighted at CTAD 2025, spanning therapeutic development, biomarker innovation, clinical trial design, and challenges in clinical translation.
Key trends from CTAD 2025: translating AD research into clinical and trial innovations.
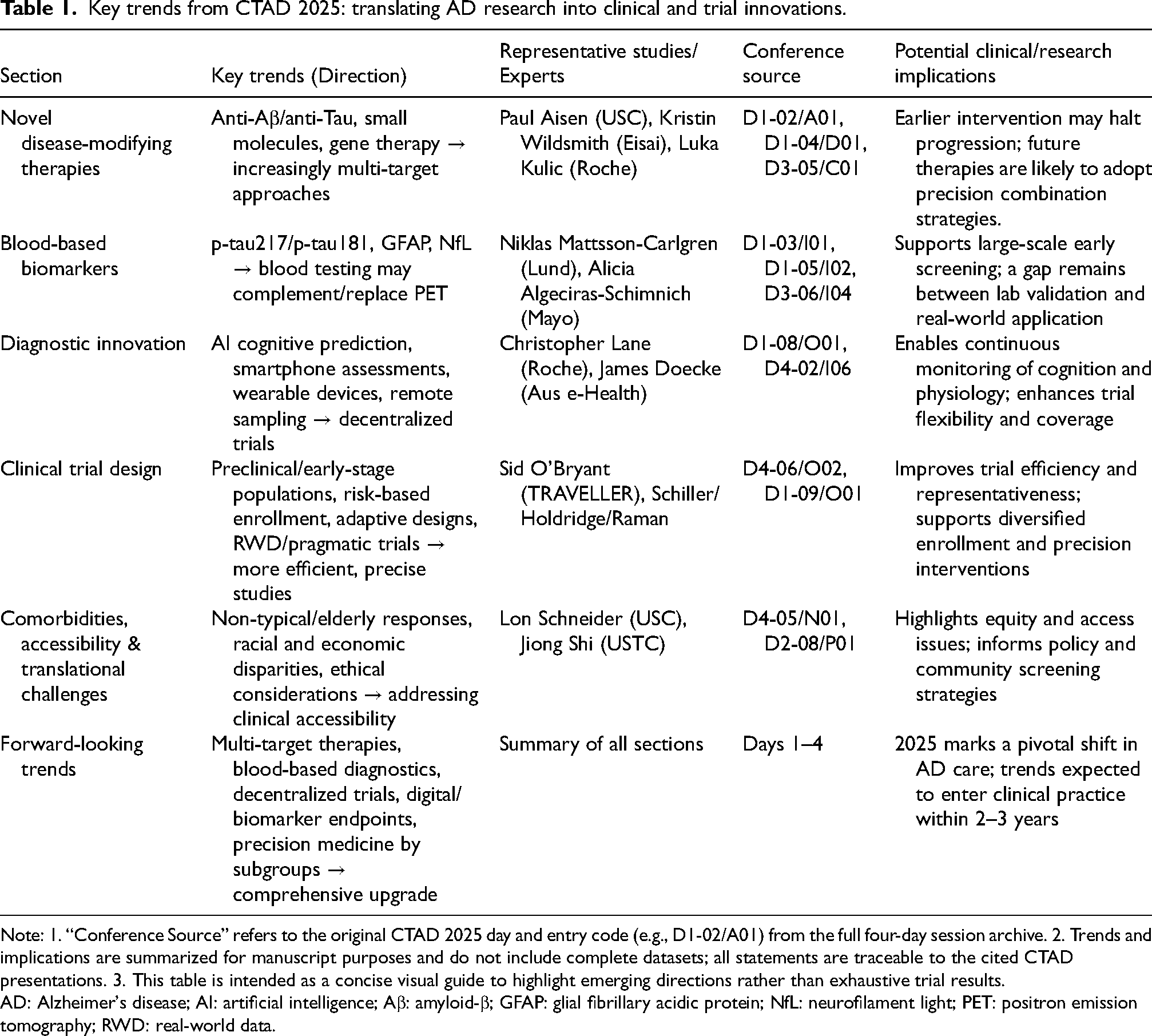
Note: 1. “Conference Source” refers to the original CTAD 2025 day and entry code (e.g., D1-02/A01) from the full four-day session archive. 2. Trends and implications are summarized for manuscript purposes and do not include complete datasets; all statements are traceable to the cited CTAD presentations. 3. This table is intended as a concise visual guide to highlight emerging directions rather than exhaustive trial results.
AD: Alzheimer's disease; AI: artificial intelligence; Aβ: amyloid-β; GFAP: glial fibrillary acidic protein; NfL: neurofilament light; PET: positron emission tomography; RWD: real-world data.
Conclusion
CTAD 2025 represents a pivotal moment in the structural transformation of the AD diagnostic and therapeutic landscape. The trends highlighted at the conference, including multi-pathway disease-modifying therapies, the clinical accessibility of blood biomarkers, the integration of AI and wearable technologies, and decentralized, precision-focused clinical trial designs, are poised to enter clinical practice within the next two to three years. These advances are expected to enhance the feasibility of early intervention and personalized treatment, while also providing clear guidance for drug development, diagnostic strategy optimization, and clinical translation. Collectively, the insights from CTAD 2025 underscore the importance of addressing AD heterogeneity and establish a foundation for a more efficient, precise, and sustainable AD diagnosis and treatment system in the years ahead.
Footnotes
Acknowledgements
Min Yuan is currently a Visiting Scholar at Boston Children's Hospital, Harvard Medical School, Boston, MA, USA. The authors thank the organizers and participants of the 18th Clinical Trials on Alzheimer's Disease (CTAD 2025) meeting for the scientific discussions that informed this review.
The authors declare that artificial intelligence tools (e.g., ChatGPT) were used solely for limited language refinement and minor grammatical corrections in a small number of sentences. All intellectual content, literature interpretation, and critical analysis were independently developed, reviewed, and verified by the authors, who take full responsibility for the accuracy and integrity of the manuscript.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by Jiangxi Provincial Health Technology Project (202610008) and the Jiangxi Province Key Laboratory of Neurology (2024SSY06081).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.