
Abstract
Background
Determinants of reported parental history of dementia among older adult research volunteers, and its relation to participation in brain aging studies, are incompletely understood.
Objective
We aimed to characterize older adults enrolled in Alzheimer's Disease Research Center (ADRC) cohorts by reported history of parental dementia according to age, APOE ε4 dose, sex, race, Hispanic ethnicity, education, and baseline cognitive status.
Methods
Data were drawn from the National Alzheimer's Coordinating Center Uniform Data Set (NACC UDS). We included all participants who were age ≥ 65 at their most recent visit (N = 34,154). Participants were classified according to reported parental history of dementia (neither parent, mother only, father only, both parents, and unknown). Multinomial regression was used to estimate the adjusted odds ratios for reported parental history of dementia.
Results
Dementia in at least one parent was reported by 40% of participants (n = 13,596), 52% (n = 17,881) reported that neither parent had dementia, and 8% (n = 2677) did not know. Participants reporting neither parent had dementia, or reported unknown history, were older, less educated, more likely to be minoritized, and were also most likely to be missing APOE genotype (28% and 37%, respectively) and to be diagnosed with cognitive impairment at baseline (62% and 75%, respectively).
Conclusions
ADRC participants who report no parental dementia history may represent a meaningfully different group of volunteers, and within this group there is also substantial heterogeneity among all of the characteristics of interest investigated, especially by race. These differences need to be carefully considered during secondary analyses of NACC UDS data.
Introduction
Alzheimer's disease (AD) is estimated to contribute to 60% to 80% of all dementia cases, the majority of which are attributable to a combination of AD neuropathologic changes as well as one or more other pathologies, such as cerebrovascular disease or Lewy body disease. 1 Globally, approximately 11% of people over age 65 years have AD-type dementia, and due to the aging of the population, prevalence is expected to triple by 2050. 2 Late onset AD (LOAD) is the most frequently diagnosed form of AD, comprising an estimated 90–95% of all diagnosed AD cases.3,4 LOAD prevalence increases rapidly after age 65: an estimated 3% of the population age 65–74, 17% between age 75–84, and 32% of those over the age of 85 have LOAD-type dementia.1,5
Major non-modifiable risk factors for LOAD are advanced age, genetics, sex,1,6 and having a parent or sibling with AD (“family history”). 7 The complex interplay between genetic and environmental factors makes estimating attributable genetic risk difficult. 4 Dozens of AD-associated risk genes have been identified using genome wide association (GWAS), but much of the genetic risk associated with AD remains unexplained.8,9 Despite the magnitude of association with APOE ε4 allele dosage, it has been suggested that ε4 accounts for roughly 10–27% of the estimated overall LOAD risk attributed to genetic factors (60–80%).4,6,10 Having inherited a single APOE ε4 allele increases the risk of developing AD-type dementia by approximately 2- to 4-fold on average, and having two APOE ε4 alleles increases the risk by 8- to 12-fold compared to those with two copies of APOE ε3.1,11,12 Those with two copies of the APOE ε4 allele have a significantly earlier age of onset of dementia compared to those with one or no copies of the allele, 66.4 years of age versus 72.0 years of age respectively.12–14
Family history of dementia encompasses both known and unknown genetic risk factors, as well as environmental and behavioral risk factors.7,10,15 First-degree family history of dementia is associated with an estimated 4- to 10-fold higher LOAD risk. 7 Additionally, a maternal history of dementia (versus a paternal history) is associated with increased LOAD risk and a higher likelihood of abnormal levels of AD fluid biomarkers when compared to those without a parental history.7,10,15
The concept of family history of dementia is also methodologically challenging. For example, family history of dementia could motivate people to join AD research, 16 resulting in study samples with greater average LOAD risk than reference populations. A recent study found people with a family history of dementia were more likely to show interest in dementia testing. 17 Moreover, accuracy of reported family history of dementia may depend on the sex of the parent. Devi et al. found 76% of female relatives with dementia were correctly identified compared to only 21% of males. 18 Women tend to live longer than men and advanced age is a leading risk factor for the diagnosis of LOAD. 19 The death of a parent and cognitive impairment are both associated with sociodemographic factors, higher socioeconomic status (SES) is associated with a lower risk of cognitive impairment as well as a more advanced age at the time of parental death when compared to those with a lower SES. 20 Among those with a higher SES, women's increased longevity may increase the likelihood of AD research participants reporting a maternal history of dementia. Similarly, knowledge and meaning of family history of dementia may differ across ethnoracial groups 21 due to factors including structural racism limiting access to health care (e.g., probability of early and accurate diagnosis).1,22,23 In a recent study of recruitment factors among Black and White Alzheimer's Disease Research Center (ADRC) participants, Gleason et al. point out that given known barriers to accessing timely dementia diagnosis, reports of family history of dementia among marginalized groups may be indicative of protective factors like better health literacy and a higher socioeconomic status.21,22,24
In recent GWAS studies based on large cohorts of adults in midlife, parent or first-degree family history of dementia was used as a proxy phenotype for participant AD or dementia.9,25,26 Researchers have raised concerns that such methods may yield misleading results, due to biases inherent in reported family history of dementia.27,28 Additional studies of the relation between reported family history of dementia and genetic risk factors in different cohorts are needed, as even the relation between APOE genotype and parental family history of dementia is not well understood, at least in part because self-reporting of parental family history most likely results in misclassification. 18
APOE is involved in lipid metabolism in the peripheral blood and central nervous system (CNS) and is a major risk factor for cardiovascular disease, stroke, and other neurodegenerative diseases in addition to LOAD.12,29 Studies are mixed on whether or not there is a difference in age of onset between those with no copies and one copy.12–14 The APOE ε2 and the rare APOE ε3 CM (Christchurch mutation) alleles appear to have a protective effect against cognitive decline and dementia relative to the APOE ε3 allele. 30
Perfect concordance between genetic risk factors and family history of dementia is unlikely. For example, the presence of APOE ε4 is not necessary or sufficient to cause AD-type dementia as only 40% of people with LOAD carry an APOE ε4 allele, 31 and not everyone who carries an APOE ε4 develops dementia. In a prospective observational cohort study of centenarians, for example, only 5.6% carried an APOE ε4 allele among the group with declining cognitive performance during the study, compared to 18.6% of the group that maintained relatively high cognitive performance throughout the study. 30 Another study of cognitively stable people older than 80 years found 20% were carriers of the APOE ε4 allele. 32
In the current study we used data from the National Alzheimer's Coordinating Center (NACC), which aggregates and distributes standard data elements collected by all federally-funded ADRCs, to examine associations between reported parental family history of dementia and participant characteristics, including demographics, APOE genotype, and cognitive status. Over 1400 studies utilizing NACC data have been published. 33 Previous research has established that participants enrolled in ADRC cohorts differ from the general population of older adults in important ways. 34 While participants with family history of dementia and APOE ε4 carriers are both expected to be overrepresented among ADRC cohorts, the ways that different patterns of family history may influence participation among different populations is not well understood.
Methods
Participants
Data were drawn from participant visits, occurring approximately annually from September 2005 through June 2019, at the National Institute on Aging-funded ADRCs. ADRCs capture participant visit data using the Uniform Data Set (UDS) protocol, and de-identified participant data is maintained and shared with researchers by the NACC. All participants who were age 65 or older at the most recent visit and who had available parental dementia history were included in the current study. We excluded participants who were younger than 65, due to concerns that their reporting of parental dementia history may be qualitatively different than older participants (e.g., younger participants are more likely to have a living parent, and public awareness and diagnosis procedures have changed over time). ADRC research activities are overseen by local Institutional Review Boards (IRB), and all participants provided written informed consent for ADRC participation. No IRB approval was required for this secondary analysis of the de-identified data.
Study design
We conducted a secondary data analysis to evaluate the association between parental dementia history and selected participant characteristics: age, sex, race, ethnicity, APOE ε4 allele dose, diagnosis of cognitive impairment, and age of onset of cognitive impairment. Study data were drawn from each participant's initial and most recent visit, reflecting their most current diagnosis and parental history as of June 2019.
Family history of dementia
We focused on parental history of dementia, rather than first-degree family history more broadly, due to our specific interest in the association of reported family history and APOE ε4 carriership. Parental history of dementia was reported by participants or their study partners, and collected by trained interviewers at the participant's ADRC, using the NACC UDS Family History Form (Form A3). Determinations of parental dementia were made by ADRC clinicians based on set criteria and follow up questions. 35 Parental history of dementia was operationalized in the current study as a four-level categorical variable: neither parent, maternal only, paternal only, and both parents.
APOE genotype
APOE genotype data are provided to NACC from the National Centralized Repository for Alzheimer's Disease (NCRAD) and coded into the NACC database. Genotyping is performed on participant blood samples provided to NCRAD from the ADRCs. APOE genotype for this study was operationalized as dose: zero, one, or two ε4 alleles. 36 APOE results were not disclosed to participants by ADRCs during the study period.
Cognitive status and age of onset
Syndromic cognitive status was assessed at each UDS visit and recorded as normal, impaired but not mild cognitive impairment (MCI), MCI, or dementia for all participants. Diagnosis is based on objective cognitive testing, neurological examination, physical examination, medical history, and information provided by study partners. For the current study, a binary variable for cognitive status was created based on the ADRC clinical assessment: MCI and dementia were operationalized as “cognitively impaired” (i.e., MCI or dementia), and normal and impaired not MCI were coded as “without significant cognitive impairment” (i.e., normal/impaired not MCI). The age of onset of cognitive impairment is based on clinician assessment of when the participant's decline began, which is derived from UDS Form B9.
Statistical analysis
Included participants were classified according to reported parental history (neither parent, maternal only, paternal only, and both parents) and described by characteristics of interest: age at visit, APOE ε4 dose (0, 1, 2, or unknown), sex, race, Hispanic ethnicity, years of education, diagnosis of cognitive impairment, and average age of onset of cognitive impairment.
Multinomial regression analysis was used to estimate mutually adjusted odds ratios for parental history of dementia (neither parent as reference category) and the characteristics of interest: age, APOE ε4 dose (0, 1, 2, or unknown), sex, race (coded as White, Black, and All Others due to sparse cells), Hispanic ethnicity, years of education, and baseline diagnosis of cognitive impairment. Among those with diagnosed cognitive impairment, we used multiple linear regression to test the hypothesis that parental history of dementia is associated with age at onset, adjusting for APOE ε4 dose, years of education, race, ethnicity, and sex. All statistical analyses were performed using SAS 9.4®.
Results
A total of 34,154 participants were age 65 or older. Table 1 presents descriptive characteristics of included participants (N = 34,154, representing 39 unique ADRCs) by parental history of dementia and overall. Parental history of dementia was commonly reported, though 52% (n = 17,881) of participants reported that neither parent had dementia, and 8% (N = 2677) were unable to report on their parental history. Among participants who reported any history of parental dementia (N = 13,596), maternal only was most common (64%, n = 8726), followed by paternal (24%, n = 3225), and both parents (12%, n = 1645). Participants who reported neither parent with dementia had the lowest frequency of ≥1 ε4 alleles (25%, p < 0.0001), compared to participants reporting maternal only (36%), paternal only (37%), or both parents (40%). Participants with unknown parent history also had low frequency of ≥1 ε4 alleles (26.6). However, participants reporting neither parent had dementia or unknown history were also most likely to be missing APOE genotype (28% and 37%, respectively), while participants reporting mother only, father only, or both parents had between 21–23% missing genotype data (p < 0.0001). Patterns of reported parental history of dementia and probability of APOE missingness were both associated with ADRC cohort (p < 0.0001 for both comparisons; Supplemental Table 1).
Alzheimer's disease research center participant characteristics (2005–2019) by reported parental history of dementia.
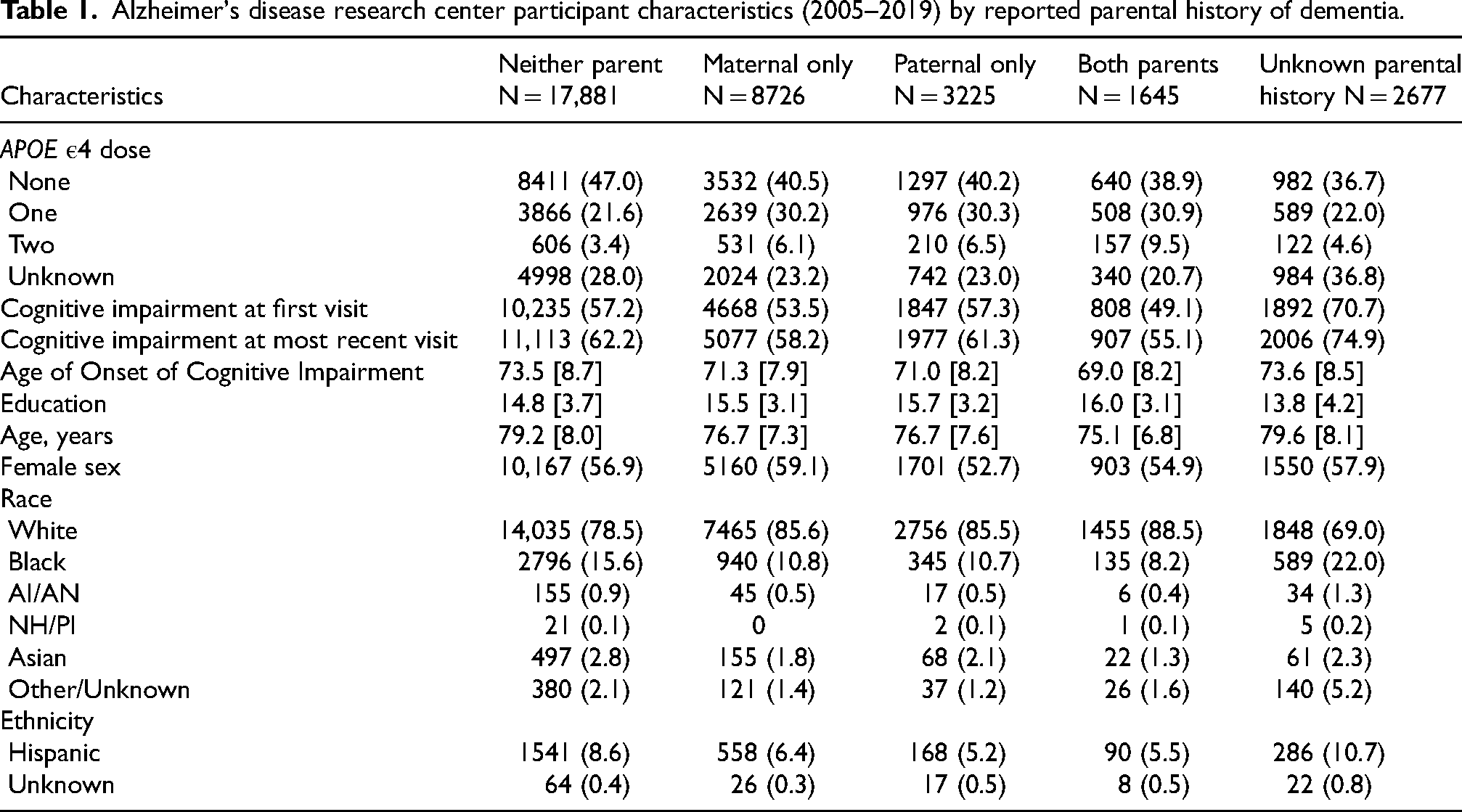
Participants reporting neither parent with history of dementia and those with unknown parent history were significantly older (∼79 versus ∼76 years, p < 0.0001) and had educational attainment about 1–2 years lower (p < 0.0001) compared to the other parental history groups. Frequency of cognitive impairment diagnosis at the initial UDS visit was significantly different across groups (p < 0.0001), with the highest proportion observed among participants who reported unknown history (71%), followed paternal only and neither parent (57% each), while the lowest was among participants who reported both parents (49%). Similarly, the highest frequency of cognitive impairment diagnosis at the most recent UDS visit was observed among those reporting unknown history (75%), followed by those reporting neither parent had dementia (62%), while the lowest frequency was among those who reported both parents (55%). Participants reporting unknown history or neither parent also tended to be older at cognitive impairment onset (∼74 years) compared to participants reporting maternal only (71), paternal only (71), or both parents (69) (p < 0.0001).
As in the total sample, reported history of both parents with dementia corresponded to the lowest proportion of diagnosed cognitive impairment at either initial or most recent UDS visit for both male and female participants (Supplemental Tables 2 and 3). However, the association in the total sample was driven primarily by female participants. Among male participants, for example, those reporting a history of both parents were the least likely to be diagnosed with cognitive impairment at the initial UDS visit (61%), but proportions ranged only between 61–73% by history type (Supplemental Table 3). More variation was observed for female participants, where proportion diagnosed with cognitive impairment at the initial UDS ranged more widely from 39% for those reporting dementia history for both parents to 53% among those reporting neither parent had dementia and 73% reporting unknown history (Supplemental Table 2).
Participants reporting neither parent, maternal history only, or unknown history were slightly more likely to be female (57%, 59%, and 58% respectively) relative to participants reporting paternal only (53%) or both parents (55%). Participants reporting unknown history or neither parent had dementia, were relatively less likely to be White compared to participants who reported at least one parent (69% and 79%, respectively versus 86%), but were more likely to be Black (22% and 16% versus 10%), American Indian/Alaska Native (1.3% and 0.9% versus 0.5%), or Hispanic (11% and 9% versus 6%). Similar patterns were observed within strata of sex (Supplemental Tables 2 and 3), but these differences were most pronounced among female participants.
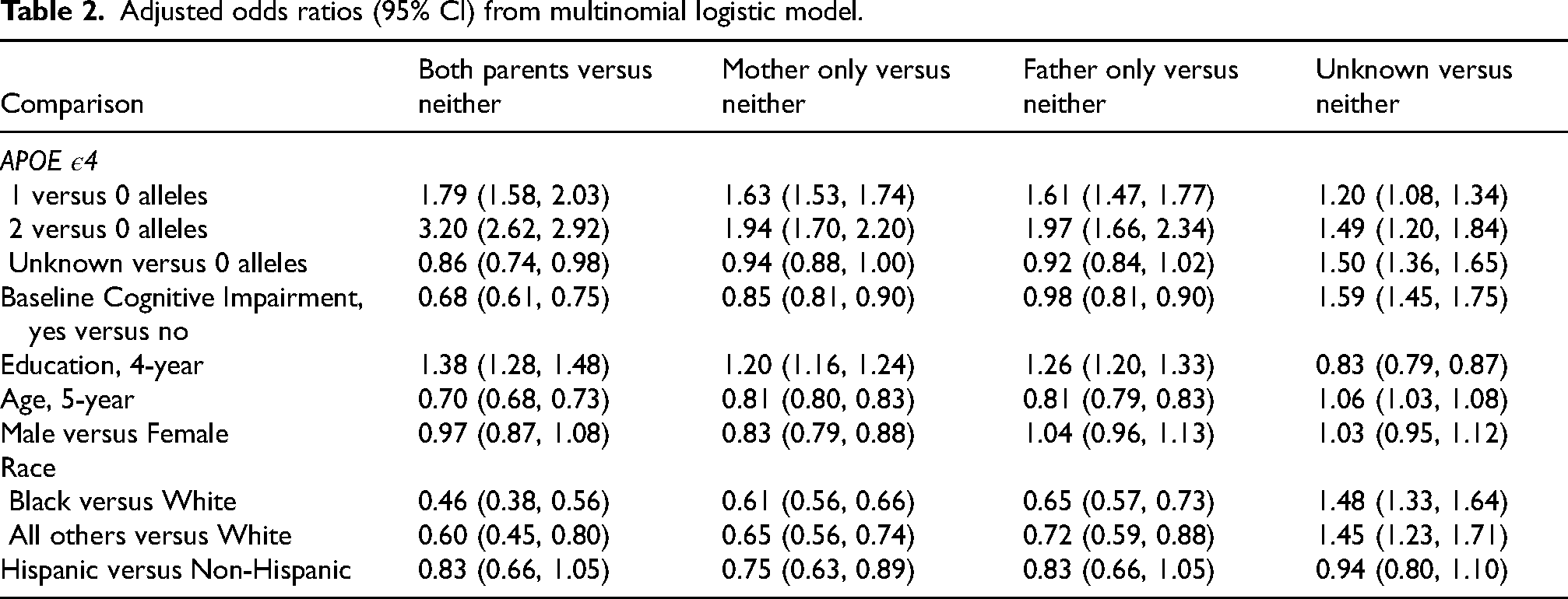
In the multinomial regression analysis (Table 2), ε4 allele dose was strongly and significantly associated with reported parental history of dementia; carrying two ε4 alleles was most strongly associated with history of both parents with dementia (OR = 3.21; 95% CI: 2.62–3.92) but was associated with increased odds of all reported history types versus neither parent. Participants with unknown APOE genotype were significantly less likely to report both parents vs neither parent, and significantly more likely to report unknown history, but no other differences were observed. Participant sex was not strongly associated with type of reported parental history, and while male participants were less likely to report maternal history relative to reporting neither parent (OR = 0.83; 0.79–0.88), no other differences were observed. A diagnosis of cognitive impairment at baseline was associated with reduced odds of reporting both parents, maternal only, and paternal only, but was most strongly associated with increased odds of reporting unknown history (OR = 1.59; 1.45–1.75). Increased educational attainment was associated with higher odds of reporting all types of parental history versus neither parent, while increased age was associated with reduced odds of reporting parental history across all types, with exception of unknown history, where increased age was associated with higher odds of reporting unknown history and higher education was associated with reduced odds of reporting unknown history. Minoritized racial identity was associated with reduced odds of reporting any type of parental history of dementia relative to reporting neither parent, again with the exception of unknown history. Relative to White participants, Black participants were more likely to report unknown history (OR = 1.48; 1.33–1.64), as were participants in the aggregated racial group (OR = 1.45; 1.23–1.71). Hispanic ethnicity was not strongly associated with parental history reporting, and was only significantly associated with reporting maternal only versus neither parent (OR = 0.75; 0.63–0.89).
Adjusted odds ratios (95% CI) from multinomial logistic model.
Results from the linear regression analysis of mean age of onset for participant cognitive impairment were similar to the unadjusted results. Overall, conditional on the other covariates, adjusted mean age of onset was lowest for participants reporting both parents had dementia (67.4 years (95% CI: 66.5–68.3)—and highest among those reporting neither parent had dementia (71.4 years [70.7–72.2]) and unknown history (71.4. [70.7, 72.2]).
Discussion
We studied the association between reported parental history of dementia and selected participant characteristics among the ADRC cohorts. Our results suggest substantial heterogeneity between ADRC participants with and without any reported parental history of dementia, as well as among participants whose reported parental history was unknown, and our results indicated differential reporting of parental history of dementia by APOE status, age, education, sex and especially by race.
Overall, Black and other minoritized participants were less likely than White participants to report any type of parental history, supporting earlier findings.21,27 Although population-based epidemiological studies in the US consistently report that Black and Hispanic Americans are at substantially increased risk of dementia,37–39 differences in life expectancy 40 and more limited access to specialized neurological care may help explain this apparent discrepancy. This interpretation is supported by the results for the unknown parental history group, where Black participants especially were overrepresented.
APOE ε4 allele dose was strongly associated with likelihood of reporting a parent had dementia, suggesting reported family history is capturing some genetic risk information. However, we observed that participants who reported neither parent had dementia had the lowest burden of ε4 alleles, but were diagnosed more frequently with cognitive impairment. This also may be explained in part by differences in survival, if parents did not live long enough to develop dementia, but did harbor non-APOE genetic risk.
Additionally, selection processes at least partially explain these results. People who have a higher level of education and a parental history of dementia are more likely to participate in this type of research. 16 They may also be more likely to join a dementia-related research study when they are younger and before signs and symptoms begin to manifest, particularly when both parents had dementia. However, this potential motivation may vary by sex: women who reported both parents were much less likely to be diagnosed with cognitive impairment at baseline compared to women who reported neither parent or men who reported both parents. Overall, men in this sample appeared more motivated to participate due to the presence of cognitive problems, such that 64% had diagnosed impairment at baseline compared 52% of women.
Alternatively, information bias and ascertainment bias may also partially explain our observed results. For example, it is possible that less frequent reporting of either parent with dementia by those with cognitive impairment may reflect information bias, where the participant or their co-participant may not report a parent had dementia, when they actually did. This may also partially explain why those participants who reported neither parent had dementia tended to be a few years older; older participants may have had one or both parents with dementia, but they were not diagnosed due to decreased awareness. For example, research on the validity of family history reporting conducted during the 1990s suggests that specificity was high (84–98%) while sensitivity was much lower (21–64%).18,41 The more frequent reporting of maternal only versus paternal only dementia history that we observed among both male and female participants likely reflects both the increased prevalence of dementia among women relative to men 42 as well as sociocultural factors. 43
This study conducted among a large sample of well characterized research volunteers has some limitations. Within ADRCs, volunteers tend to be highly educated, with higher socioeconomic status, more likely to be White non-Hispanic, and less likely to be male relative to the general population of older adults. 34 As such, our results on the relation of these factors with family history reporting are not readily generalizable outside the ADRC program data. Moreover, measurement of participant-reported parental history of dementia among older adults is subject to many biases. While we have attempted to elucidate many of them in relation to our study results, it is likely that unidentified biases remain.
Conclusion
Reported parental history of dementia in ADRC cohorts may capture unmeasured genetic risk as well as other behavioral and environmental risk factors associated with the risk of LOAD. The accuracy of the reported information likely depends on many factors in addition to the true history. Given the similarities in the groups reporting neither parent and unknown parental history, participants in ADRC cohorts who report no parental dementia history may represent a meaningfully different group of volunteers, and within this group there is also substantial heterogeneity. Differences in recruitment, enrollment, and selection factors need to be carefully considered when designing secondary analyses of NACC UDS data.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261450630 - Supplemental material for Potential biases associated with reported parental history of dementia in the Alzheimer's Disease Research Center cohorts: Implications for secondary data analyses
Supplemental material, sj-docx-1-alz-10.1177_13872877261450630 for Potential biases associated with reported parental history of dementia in the Alzheimer's Disease Research Center cohorts: Implications for secondary data analyses by Chad Guilliams and Erin Abner in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
The NACC database is funded by NIA/NIH Grant U24 AG072122. NACC data are contributed by the NIA-funded ADRCs: P30 AG062429 (PI James Brewer, MD, PhD), P30 AG066468 (PI Oscar Lopez, MD), P30 AG062421 (PI Teresa Gomez-Isla, MD), P30 AG066509 (PI Thomas Grabowski, MD), P30 AG066514 (PI Mary Sano, PhD), P30 AG066530 (PI Helena Chui, MD, Arthur Toga, PhD), P30 AG066507 (PI Marilyn Albert, PhD), P30 AG066444 (PI David Holtzman, MD), P30 AG066518 (PIs Lisa Silbert, MD, Miranda Lim, MD, PhD), P30 AG066512 (PI Thomas Wisniewski, MD), P30 AG066462 (PI Scott Small, MD), P30 AG072979 (PI David Wolk, MD), P30 AG072972 (PIs Charles DeCarli, MD, Rachel Whitmer, PhD), P30 AG072976 (PI Andrew Saykin, PsyD), P30 AG072975 (PI Julie Schneider, MD, MS), P30 AG072978 (PI Ann McKee, MD), P30 AG072977 (PI Robert Vassar, PhD), P30 AG066519 (PI Joshua Grill, PhD), P30 AG062677 (PIs Brad Boeve, MD, Ronald Petersen, MD, PhD), P30 AG079280 (PI Jessica Langbaum, PhD), P30 AG062422 (PI Gil Rabinovici, MD), P30 AG066511 (PI Allan Levey, MD, PhD), P30 AG072946 (PI Linda Van Eldik, PhD), P30 AG062715 (PI Sanjay Asthana, MD, FRCP), P30 AG072973 (PI Russell Swerdlow, MD), P30 AG066506 (PIs Glenn Smith, PhD, ABPP, David Lowenstein, PhD, Ranjan Duara, MD), P30 AG066508 (PIs Stephen Strittmatter, MD, PhD, Christopher Van Dyck, MD), P30 AG066515 (PI Victor Henderson, MD, MS), P30 AG072947 (PI Suzanne Craft, PhD), P30 AG072931 (PI Henry Paulson, MD, PhD), P30 AG066546 (PIs Sudha Seshadri, MD, Gladys Maestre, MD, PhD), P30 AG086401 (PI Erik Roberson, MD, PhD), P30 AG086404 (PI Gary Rosenberg, MD), P30 AG086403 (PI Angela Jefferson, PhD), P30 AG072958 (PIs Heather Whitson, MD, Gwenn Garden, MD, PhD), P30 AG072959 (PI Jagan Pillai, MD, PhD), P30 AG092752 (Ihab Hajjar, MD, MS).
Ethical considerations
Not applicable.
Consent to participate
ADRC research activities are overseen by local Institutional Review Boards (IRB), and all participants provided written informed consent for ADRC participation. No IRB approval was required for this secondary analysis of the de-identified data.
Consent for publication
Not applicable.
Author contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.