
Abstract
Background
Growing evidence suggests that dementia risk is influenced not only by genetic factors but also by social and environmental determinants. Understanding these modifiable factors is critical for informing prevention strategies.
Objective
To synthesize existing evidence from systematic reviews on the associations between social and environmental determinants and the risk of dementia, including Alzheimer's disease, vascular dementia, and frontotemporal dementia.
Methods
An umbrella review was conducted by systematically searching five major databases for systematic reviews published between 2004 and 2024. Eligible reviews examined the relationship between at least one social or environmental determinant and dementia outcomes.
Results
The review found strong associations between environmental exposures and increased dementia risk. Exposure to fine particulate matter (PM2.5) was consistently linked to elevated dementia risk, with estimates ranging from 3% to 226% per 10 μg/m3 increase. Occupational exposures to toxic metals, pesticides, and electromagnetic fields were also associated with higher neurodegeneration risk. Conversely, protective environmental factors included residential greenness and walkable neighborhoods. Among social determinants, higher education, socioeconomic status, and social engagement were found to promote cognitive resilience. In contrast, social disadvantage and limited access to healthcare contributed to increased dementia risk, likely through cumulative psychosocial stress.
Conclusions
This umbrella review underscores the significant role of social and environmental determinants in dementia risk. Targeted public health policies aimed at reducing environmental hazards and addressing social inequalities are essential for mitigating dementia risk and promoting cognitive health at the population level.
Keywords
Introduction
Dementia is a growing global health challenge, affecting millions of individuals worldwide and placing an increasing burden on healthcare systems, caregivers, and economies. 1 As average life expectancy increases, the prevalence of dementia is expected to rise significantly, 2 necessitating a greater understanding of risk factors and potential avenues for prevention.
Genetic and biological mechanisms contribute to dementia onset. Yet, a growing body of evidence underscores the importance of social and environmental determinants in shaping cognitive health trajectories. 3 Understanding the impact of these modifiable risk factors offers critical insights for public health interventions aimed at mitigating dementia risk and promoting brain health across the lifespan.1,4
Environmental exposures have emerged as significant contributors to dementia risk, with air pollution, occupational hazards, and urban design factors playing a crucial role in cognitive decline. 5 Long-term exposure to fine particulate matter (PM2.5), nitrogen oxides (NO2 and NOx), and other airborne pollutants has been associated with increased inflammation, oxidative stress, and cerebrovascular damage, all of which are implicated in neurodegeneration.6,7 Notably, individuals residing in highly polluted urban areas, particularly those in low-income communities with limited access to healthcare, face disproportionately higher risks.8–10 Occupational exposures to toxic metals, pesticides, and electromagnetic fields have also been linked to an elevated risk of Alzheimer's disease (AD) and related dementias, highlighting the potential for workplace interventions to reduce harmful exposures.11–13 In contrast, aspects of the built environment, such as green spaces and neighborhood walkability, may offer protective effects by promoting physical activity, reducing stress, and enhancing social engagement.14,15
Social determinants, including education, socioeconomic status (SES), and social engagement, also play a fundamental role in dementia risk. 16 Education, a key factor in delaying dementia onset, has been consistently shown to protect against cognitive decline, with each additional year of schooling associated with a reduced likelihood of developing dementia.17,18 This protective effect is thought to result from enhanced neural plasticity, greater cognitive stimulation, and improved health literacy, leading to better overall brain health.19–21 Similarly, social networks and engagement contribute to cognitive resilience by providing mental stimulation, reducing stress, and promoting emotional well-being. Conversely, social isolation and loneliness have been linked to an increased risk of dementia, underscoring the importance of maintaining strong social connections throughout life. 4 Socioeconomic disparities further compound dementia risk, as individuals from lower SES backgrounds often experience multiple disadvantages, including limited educational opportunities, financial insecurity, and restricted access to healthcare services.22,23
Given the multifaceted and interrelated nature of social and environmental risk factors, it is essential to synthesize evidence regarding their collective impact on dementia risk. This umbrella review aims to comprehensively evaluate and synthesize findings from available systematic reviews and meta-analyses, providing an overview of current evidence regarding the social and environmental determinants of dementia. By identifying key modifiable risk factors, this review seeks to inform public health policies, urban planning initiatives, and social interventions that can mitigate dementia risk and promote cognitive health on a population level.
Methods
Registration
This review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 24 The protocol for this review has been registered on PROSPERO International prospective register for systematic reviews under registration ID of CRD42024591097.
Definitions and conceptualization of social and environmental determinants of dementia risk
The social and environmental determinants were defined and operationalized during the study process through iterative review of the existing literature. Initial conceptual boundaries were informed by established public health frameworks and following discussion among authors, definitional criteria and coding rules were refined to ensure clarity and reproducibility. The final operational definitions and full codebook are available in the Supplemental Material (Supplemental Text 2).
Literature search strategy
Our primary interest was to identify reviews on social and environmental determinants of dementia risk, and the search terms were developed in consultation with a librarian. The three main domains of interest were searched utilizing keywords and pre-defined subject headings: Dementia (e.g., dementia, AD), social determinants (e.g., social capital, social environment, social fragmentation), environmental determinants (e.g., air pollution, built environment) and systematic review (e.g., systematic review, meta-analysis). Search terms used were constructed as follows: ((“Dementia” OR “Alzheimer*” OR “Frontotemporal dementia” OR “Vascular dementia”) AND ((“Social determinants” OR “Social factors” OR “Socio*economic status” OR “Social environment” OR “Education level” OR “Social Fragmentation” OR “Social Isolation” OR “Social Cohesion” OR “Social integration” OR “Social Vulnerability” OR “Social contact” OR “Social relation” OR “Social Network”) OR (“Environmental determinants” OR “Environmental factors” OR “Environmental exposure” OR “Air pollution” OR “Built environment”)) AND (“Systematic Review” OR “Meta analysis” OR “Meta-analysis”))). The detailed search strategy has been outlined in the Supplemental Material (Supplemental Text 1). Five databases most relevant to the scope of this review were selected to conduct a series of systematic literature searches including CINAHL, PsychINFO, PubMed, Scopus, and Web of Science. In these searches papers published between January 2004 to September 2024 were considered. The initial database search was conducted in September 2024 and repeated in November 2025 to ensure that the results were reproducible and up to date. Search strategies and databases of interest were identical across both searches, with the repeat search extending the time frame to capture systematic reviews published between September 2024 and November 2025.
Eligibility criteria
The following inclusion criteria were considered when screening the studies:
If the articles were on social and/or environmental determinants of all cause dementia, AD, vascular dementia (VaD), frontotemporal dementia (FTD) but not on cognitive decline or mild cognitive impairment (MCI). Articles that were in English. Systematic reviews and/or meta-analysis.
The following exclusion criteria were considered as well.
If articles were assessing biomedical or lifestyle determinants. Articles that were focusing on MCI. Correspondence, opinion piece or original study. Animal model studies were also excluded.
Study selection
The retrieved citations were imported into Covidence (Veritas Health Innovation, Melbourne, Australia 2024), a standard online platform for Cochrane reviews. 25 Duplicates are automatically removed by Covidence. The title and abstract screening were performed by two reviewers (S.G. and G.T.) and the full-text assessment, based on the eligibility criteria, was performed independently. Covidence automatically flags studies that two reviewers did not agree upon their exclusion/inclusion. Reviewers (S.G. and G.T.) discussed these inconsistencies and reached an agreement. When consensus could not be reached, senior author (N.B.) was consulted to make a final decision. Covidence was applied using the same procedures as the initial database search. in the repeat round of study selection. The title and abstract screening and full-text assessment of retrieved articles was performed by the first author (S.G.).
Data extraction
A template for data extraction was developed to systematically extract data from each study, which included: first author, publication year, publication region, study type, intervention/exposure, outcome, number of studies included in the publication, sample size and age range (if available), effect sizes (if available), and risk of bias assessment tool. Data extraction was completed by two authors (S.G and G.T) and inconsistencies were resolved through a third reviewer joining the process.
Quality appraisal
The AMSTAR-2 tool was utilized to assess the quality of studies; its outcomes are represented in the Supplemental Material (Supplemental Table 1). The AMSTAR 2 Tool (A Measurement Tool to Assess Systematic Reviews, version 2) is a critical appraisal tool. It is particularly suited for systematic reviews that include randomized or non-randomized studies of healthcare interventions. The key aspects that are assessed by this tool include, but are not limited to: comprehensive literature search, risk of bias in included studies, statistical methods and meta-analysis, quality of included studies data synthesis, and funding resources.
AMSTAR 2 does not provide an overall score but instead categorizes the confidence in the results of the review based on critical domains. Reviews can be rated as “High confidence”: Few or no concerns regarding methodological quality; “Moderate confidence”: Some concerns that might affect the validity; “Low confidence”: Major concerns about the review's reliability; or “Critically low confidence”: Significant methodological flaws undermine trust in the review's findings.
Results
Identification of studies
The search yielded 818 results of which 310 were duplicates. After removal of duplicates, the abstracts from 508 studies were screened from which 63 were deemed eligible for full-text screening. Subsequently, 29 articles that fit the selection criteria were included (see Figure 1). A repeat search was conducted in November 2025 to confirm the completeness of the original retrieval. This search returned 1243 records, including 385 duplicates. No new studies meeting the inclusion criteria were identified following title/abstract and full-text screening. Of these chosen articles, 11 were on social determinants and 18 were on environmental determinants.
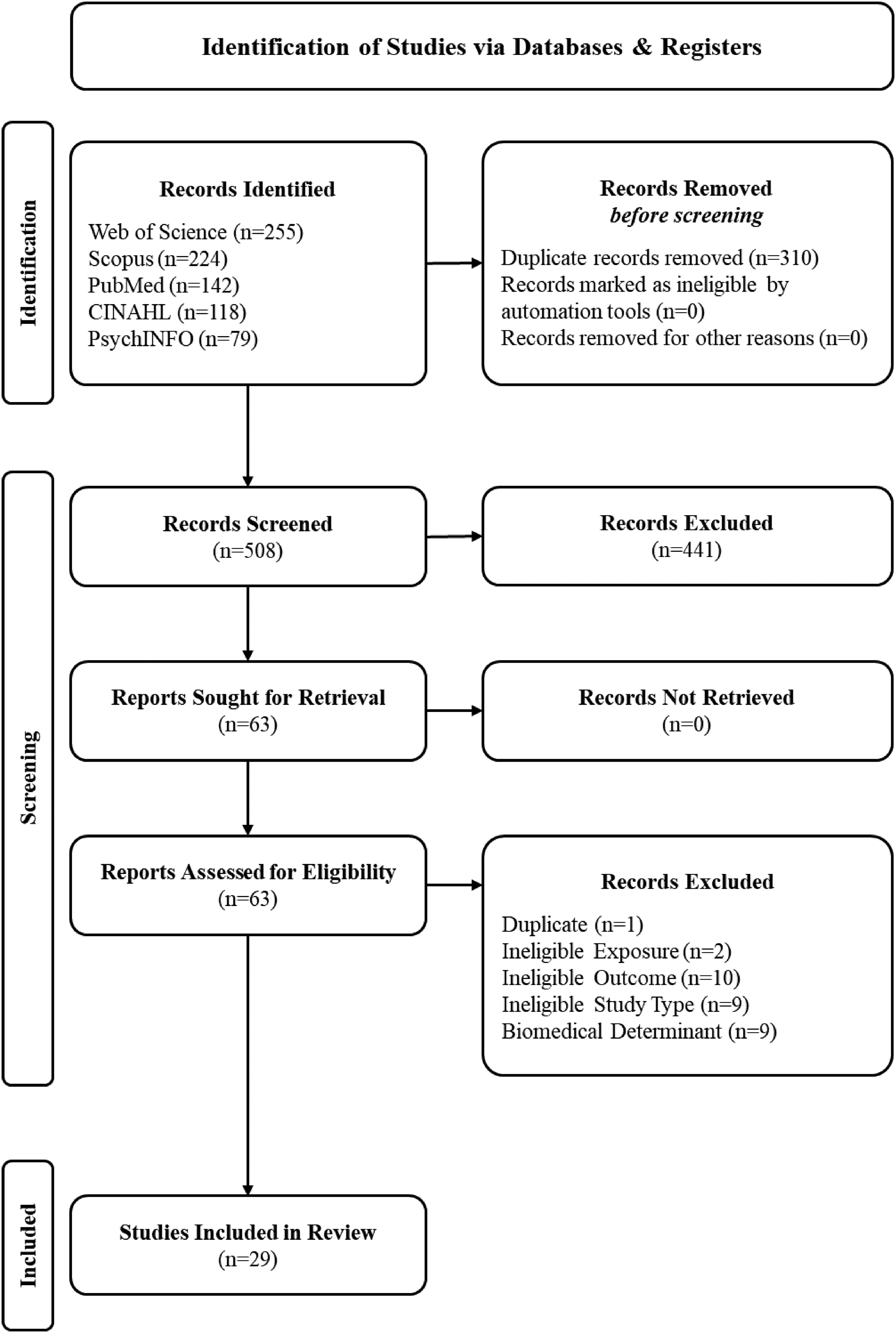
Flow diagram of study selection process.
Among potential determinants of dementia, the most studied have been air pollution (n = 9) followed by education (n = 4) and environmental risk factors (n = 4). Due to the lack of a sufficient number of systematic reviews, it was not feasible to conduct a meta-meta-analysis.
The included reviews were conducted in various regions, with majority of publications from the USA (n = 8) and China (n = 7) followed by Australia (n = 3), UK (n = 3), and Canada (n = 3) and others distributed across the globe (see Figure 2).

Distribution of systematic reviews and/or meta-analysis by country.
Environmental determinants
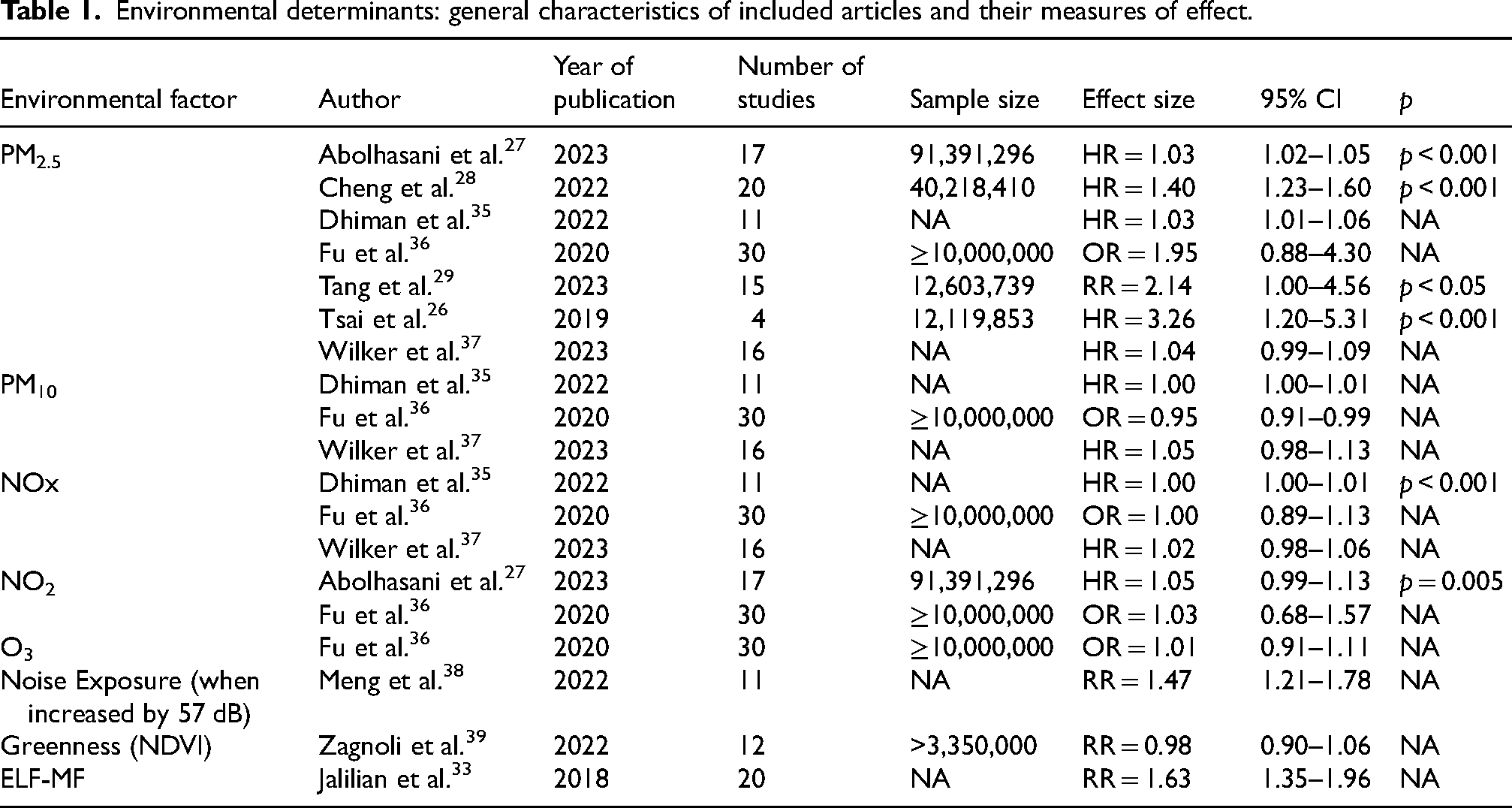
PM2.5 is the air pollutant with the strongest link to dementia risk, with its effects on dementia risk ranging from 3%–47% for each 10 unit increase in PM2.5 levels, and highly polluted areas can see an increase of up to 226%.26–28 Long-term PM2.5 exposure is associated with all-cause dementia (40% higher risk, hazard ratio (HR) = 1.40; 95% CI: 1.23–1.60), 28 AD (HR = 1.47; 95% CI: 1.22–1.78), 28 and VaD (HR = 2.0; 95% CI: 1.30–3.08). 28 In contrast, particulate matter (PM10) has a weaker association, primarily with VaD. NO2 and NOx exhibit modest associations (approximately 3%–5% estimated higher risk), 27 while the role of ozone (O3) in dementia risk remains uncertain due to inconsistent findings.
Dementia risk was found to be higher in heavily polluted urban areas, particularly in China, and among vulnerable populations such as older adults and low-income communities.10,29
One systematic review identified air pollutants, toxic metals, occupational exposures, and trace elements as significant environmental risk factors for dementia risk, with a strong dose-response relationship observed for air pollution. 30 Occupational exposure to aluminium, 31 pesticides, 32 electromagnetic fields, 33 and solvents 34 is linked to an elevated risk of AD.
Conversely, low-dose lithium in drinking water appears protective, reducing dementia incidence even at micro-dose levels. Residential greenness and social engagement have also been observed to offer protective effects, although further research is needed to confirm these associations.
Various physical waves including radiation and sound have been associated with dementia. For example, a meta-analysis by Jalilian et al. (2018) found that occupational exposure to extremely low-frequency magnetic fields (ELF-MF) increases AD risk (relative risk (RR) = 1.63; 95% CI: 1.35–1.96), with train drivers exhibiting the highest risk (RR = 2.94; 95% CI: 1.15–7.51).Female workers appear more vulnerable (RR = 2.39; 95% CI: 1.29–4.40), and geographic differences influence risk estimates. 33
Similarly, a meta-analysis of 18 studies found a slight increase in dementia risk with radiation exposure (RR = 1.11 per 100 mSv; 95% CI: 1.04–1.18), with a stronger association observed for Parkinson's disease (RR = 1.12; 95% CI: 1.07–1.17). 49 Findings for AD were inconclusive due to limited data as studies primarily focused on occupational exposure, limiting generalizability.
Also associated with dementia risk is chronic noise exposure. A 57 dB increase in noise exposure was associated with increased dementia risk (RR = 1.47; 95% CI: 1.21–1.78). 38 A nonlinear relationship suggests that even moderate noise increments contribute to risk, with effects plateauing at higher exposure levels. While consistent associations were found across dementia subtypes, study heterogeneity and methodological differences warrant further investigation. A systematic review and meta-analysis of 12 studies focused on greenness, found no strong association between residential greenness and dementia risk (RR = 0.98 for Normalised Difference Vegetation Index [NDVI]; (RR = 0.99 for land use /land cover). 39 However, a U-shaped relationship suggests that moderate greenness exposure may be protective, whereas excessive exposure offers no additional benefit. Limited evidence links greenness to cognitive impairment, and methodological challenges—such as exposure misclassification and unaccounted confounders (e.g., air pollution and social isolation)—necessitate further research. An overview of the key characteristics and findings of the included systematic reviews investigating environmental determinants is provided in Table 1.
Environmental determinants: general characteristics of included articles and their measures of effect.
Social determinants
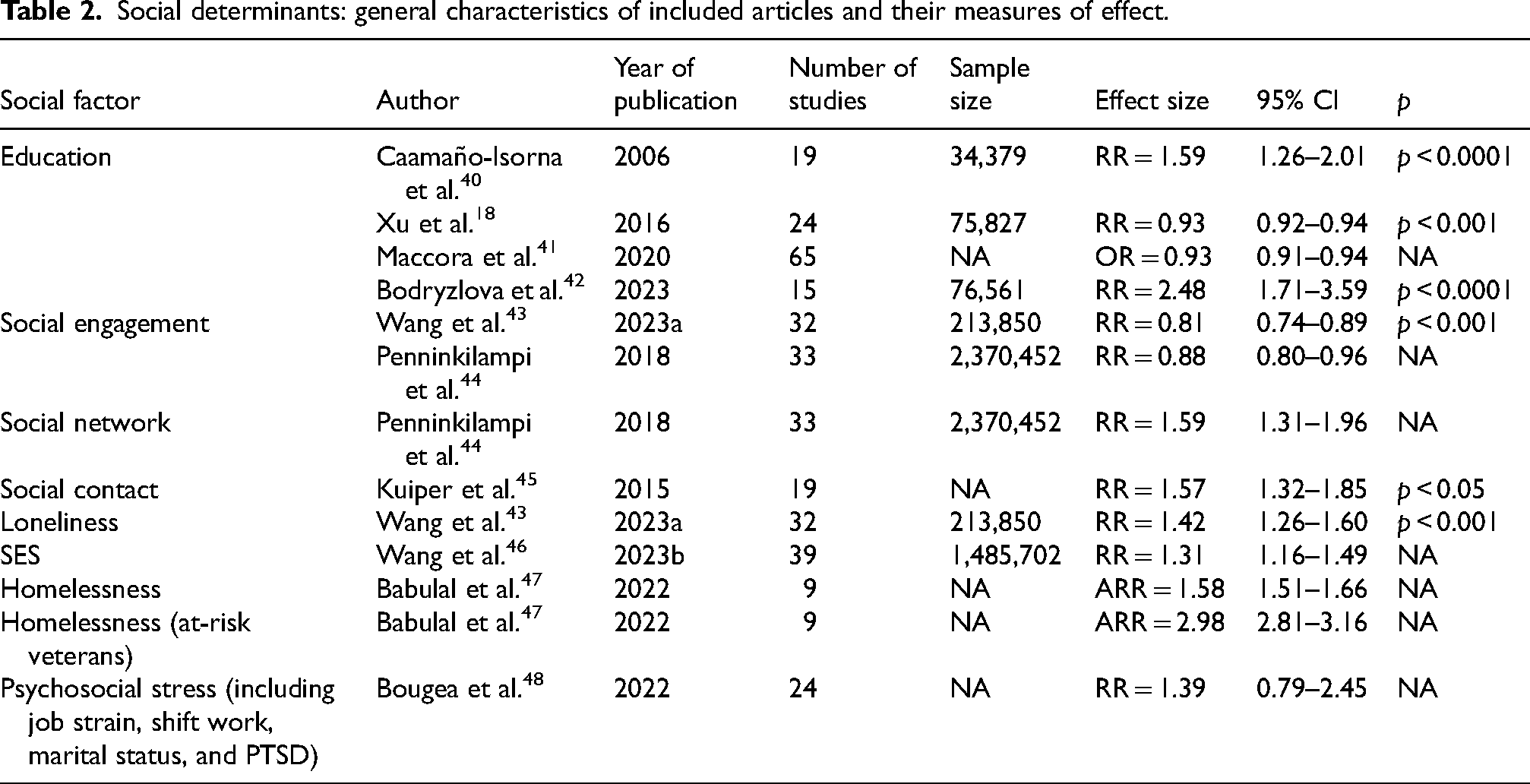
The reviewed studies consistently demonstrate a significant relationship between education level and dementia risk, supporting the hypothesis that higher education acts as a protective factor against cognitive decline. The meta-analysis by Caamaño-Isorna et al. (2006), synthesizing data from 19 studies (13 cohort and six case-control), reported a RR of 1.80 (95% CI: 1.43–2.27) for AD among individuals with lower education levels. The risk for non-AD dementias was slightly lower (RR = 1.32; 95% CI: 0.92–1.88), with an overall dementia risk of 1.59 (95% CI: 1.26–2.01). 40 Xu et al. (2016) reported a dose-response relationship, where each additional year of education corresponded to a 7% reduction in dementia risk (RR = 0.93; 95% CI: 0.92–0.94, p < 0.0001). 18 Similarly, Maccora et al. (2020) found that each additional year of education, up to grade 12, reduced AD risk by 8% (95% CI: 5%–12%) and overall dementia risk by 7% (95% CI: 0.91–0.94). The impact of education was particularly pronounced in studies using a dichotomous classification, with lower-educated individuals exhibiting an 85% increased risk for AD (95% CI: 56%–118%).
The relationship between social engagement and dementia risk underscores the protective effects of strong social networks. Wang et al. (2023a) found that high social engagement and frequent social contact were associated with lower dementia risk (RRs: 0.81 and 0.86, respectively). 43 Conversely, loneliness was identified as a significant risk factor (RR = 1.42; 95% CI: 1.26–1.60). 43 Kuiper et al. (2015) corroborated these findings, linking poor social participation (RR = 1.41; 95% CI: 1.13–1.75) and infrequent social contact (RR = 1.57; 95% CI: 1.32–1.85) to increased dementia risk. Comparably, Penninkilampi et al. (2018) reported that long-term social engagement (≥10 years) reduced dementia risk (RR = 0.88; 95% CI: 0.79–0.98), whereas less extensive social networks with low frequency of interaction increased it (RR = 1.59; 95% CI: 1.31–1.94).44,45 These results emphasize the importance of social interaction as a modifiable factor in dementia prevention strategies.
SES also emerged as a key determinant of dementia risk, with lower SES being associated with greater vulnerability. Bodryzlova et al. (2023) reported that lower education levels correlated with a dementia RR of 2.48, while low occupational status was associated with an RR of 2.09. 42 Wang et al. (2023b) found that low SES individuals had a 31% higher combined risk of cognitive impairment and dementia (RR = 1.31; 95% CI: 1.16–1.49), compared to those with higher SES, with education being the most consistent SES predictor (RR = 1.66; 95% CI: 1.20–2.32). 46
A risk factor often overlapping with low SES and an extreme form of deprivation is homelessness. A systematic review by Babulal et al. (2022) revealed that homelessness is both a risk factor for, and a consequence of dementia. Studies focusing on homeless veterans reported an increased dementia risk, with adjusted RRs ranging from 1.14 (95% CI: 1.04–1.25) to 1.58 (95% CI: 1.51–1.66) compared to stably housed individuals.47,50,51 Comorbid conditions, such as substance use disorders and psychiatric illnesses, were prevalent among homeless individuals with dementia.
Psychosocial stressors have also been implicated in dementia risk, though findings remain inconclusive. Bougea et al. (2022) reported inconsistent associations between SES markers and dementia risk, with only two of four studies finding significant correlations. 48 Work-related stress, including high job strain and shift work, was linked to increased dementia risk in three of six studies. Post-traumatic stress disorder (PTSD) was consistently associated with higher risk of dementia across three studies, reinforcing the long-term cognitive effects of severe psychological trauma. For a concise overview of the findings of included systematic reviews investigating social determinants see Table 2.
Social determinants: general characteristics of included articles and their measures of effect.
Discussion
This umbrella review provides a comprehensive synthesis of the social and environmental determinants of dementia and highlights the potential gaps in the socio-environmental drivers of dementia risk. The findings highlight the significant role of modifiable factors, such as air pollution, education, occupational exposures, psychosocial stress, and built environment characteristics, in shaping cognitive health trajectories. Whilst strong associations between these determinants and dementia risk were identified, methodological inconsistencies such as variations in exposure assessments, and the absence of uniform study designs present challenges in establishing causality. Notably, air pollution, particularly PM2.5 exposure, emerged as a key environmental risk factor. Higher educational attainment was consistently associated with reduced dementia risk. Additionally, effects of social engagement and socioeconomic status played crucial roles, which reinforces the importance of structural and policy-driven interventions to mitigate dementia risk.
The findings of this review align with previous research indicating that air pollution, particularly PM2.5, is a significant contributor to neurodegeneration.45,49,52,53 The reported HRs across studies varied considerably due to differences in exposure assessment methodologies, study designs, and population demographics. Similar to prior epidemiological findings, chronic exposure to airborne pollutants was associated with increased dementia risk, likely through mechanisms involving systemic inflammation, oxidative stress, and cerebrovascular damage.54,55 However, regional disparities in pollution levels and study methodologies complicate direct comparisons, necessitating more geographically diverse and uniform research.
Education was consistently identified as a protective factor, reinforcing the cognitive reserve hypothesis. 56 The estimated 7% reduction in dementia risk per additional year of education is consistent with prior meta-analyses, suggesting that cognitive enrichment plays a key role in mitigating neurodegeneration.57,58 However, variability in how education is defined and measured across studies complicates cross-study comparisons, highlighting the need for standardized approaches. 41
The role of occupational exposures, particularly to ELF-MF and ionizing radiation, remains an area of debate. While the findings suggest an increased dementia risk among high-exposure occupations, (such as train drivers and welders), differences in study methodologies and potential confounding of other workplace hazards limit definitive conclusions. This contrasts with some previous studies that failed to detect a strong association, emphasizing the need for more precise exposure assessments and longitudinal investigations.
Findings regarding social engagement and socioeconomic status also align with existing literature, which suggests that strong social networks enhance cognitive reserve and reduce dementia risk. 59 However, inconsistent definitions and measures of social engagement across studies present a challenge in quantifying its impact. Similarly, the observed association between lower SES and dementia risk is well-established, though variations in the strength of this relationship across studies underscore the complex interplay of economic, educational, and health-related factors.
The findings of this review have important implications for public health, clinical practice, and policy. Mechanistically, air pollution appears to contribute to dementia risk through pathways involving neuroinflammation, oxidative stress, and vascular damage.60–62 Given the consistent evidence linking PM2.5 exposure to cognitive decline, policymakers should prioritize air quality improvements and urban planning strategies to mitigate this risk.63,64 Efforts to reduce pollution levels in highly affected regions may be key to lowering dementia incidence.
The protective effect of education underscores the importance of early-life cognitive enrichment and lifelong learning. Educational investments, particularly in underserved communities, could serve as a long-term strategy to reduce dementia burden. 65 Furthermore, initiatives promoting cognitive engagement in mid-to-late life, such as occupational training and social programs, may help reinforce cognitive resilience. 66 The association between occupational exposures and dementia risk suggests the need for workplace safety regulations and enhanced monitoring of environmental hazards. Future policies should aim to reduce exposure to neurotoxic agents in high-risk occupations and develop guidelines to protect workers from potential long-term cognitive effects.
From a clinical perspective, these findings highlight the importance of assessing social and environmental factors in dementia risk evaluations. Clinicians should consider incorporating social determinants, such as loneliness, occupational history, and SES, into dementia risk assessments and prevention strategies. Social prescribing interventions, aimed at increasing social engagement among older adults, may serve as an effective approach to mitigating dementia risk.
Despite the valuable insights gained from this review, several unanswered questions remain. The precise mechanisms underlying the association between air pollution and dementia require further investigation, particularly regarding the differential effects of specific pollutants and potential gene-environment interactions. Future studies should employ consistent exposure assessment methodologies and longitudinal designs to refine risk estimates and improve comparability.
The role of ELF-MF in neurodegeneration remains inconclusive due to heterogeneity in exposure assessments and study methodologies. High-quality longitudinal studies with standardized diagnostic criteria and exposure measurements are needed to clarify ELF-MF's contribution to dementia risk. Similarly, research on trace lithium levels in drinking water as a potential protective factor is in its early stages, necessitating further investigation into its neuroprotective properties and feasibility as a public health intervention.
The relationship between homelessness and dementia also warrants further exploration. While this review highlights a bidirectional association, the predominance of studies focusing on veteran populations limits the generalizability of findings. Future research should examine non-veteran homeless populations and assess the impact of targeted interventions in this high-risk group.
Measures to ensure consistency in assessing social engagement and SES in dementia research are critical for future investigation. Understanding the complex interactions between these factors and other determinants of cognitive health will be essential for designing effective interventions.
A key strength of this umbrella review is its comprehensive and systematic evaluation of a wide range of social and environmental risk factors, providing valuable insights into their collective impact on dementia. 67 The inclusion of multiple determinants allows for a holistic perspective on how various exposures interact to influence dementia risk. Furthermore, this study highlights gaps in the literature, underscoring the need for improved exposure assessment methodologies and standardized diagnostic criteria.
However, several limitations must be acknowledged. First, due to the nature of this project being embedded within a doctoral research program, the full-text screening and review were conducted by a single author (S.G.). While this approach ensured consistency in decision-making, it also introduces the possibility of selection bias and may limit the robustness typically associated with multi-reviewer processes. The involvement of additional reviewers was constrained by limited availability and/or lack of specialized expertise among co-authors. Second, a formal pilot test was not conducted prior to conducting the full strategic search. As a result, the sensitivity and precision of the overall search might have been impacted. The methodological heterogeneity across studies, including variations in exposure assessments and inconsistent definitions of key variables, hinders direct comparisons and meta-analytic synthesis. Lastly, the absence of a meta-meta-analysis due to data limitations precludes a quantitative synthesis of effect sizes, limiting the ability to derive precise risk estimates. Additionally, the predominance of observational studies introduces potential biases, including residual confounding and reverse causation, which may affect causal inferences.
Conclusion
This umbrella review underscores the significant role of social and environmental determinants in shaping dementia risk. Air pollution, education, occupational exposures, social relationships, and built environment characteristics all contribute to cognitive health outcomes. However, methodological inconsistencies and exposure assessment challenges highlight the need for further research. Policymakers should consider integrating these findings into public health strategies, emphasizing air quality improvements, educational investments, and social engagement initiatives to mitigate dementia risk. Future studies should focus on refining exposure assessment methods, elucidating causal mechanisms, and identifying targeted interventions to reduce the global dementia burden.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261456777 - Supplemental material for Social and environmental determinants of dementia risk: An umbrella review
Supplemental material, sj-docx-1-alz-10.1177_13872877261456777 for Social and environmental determinants of dementia risk: An umbrella review by Saba Ghiasvand, Gobezie T. Tegegne, Hossein Tabatabaei-Jafari, Soumya Mazumdar, Ananthan Ambikairajah and Nasser Bagheri in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
The authors have no acknowledgments to report.
ORCID iDs
Ethical considerations
Not applicable
Consent to participate
Not applicable
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was supported by an Australian Government Research Training Program (RTP) Scholarship, which contributed to the publication costs.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Nasser Bagheri is an Editorial Board Member of this journal but was not involved in the peer-review process of this article nor had access to any information regarding its peer-review.
Data availability statement
The data supporting the findings of this study are available within the article and/or its supplemental material.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.