
Abstract
Background
Semaglutide is a glucagon-like peptide-1 analog that is on the market to treat type 2 diabetes and weight loss (Ozempic, Wegovy). Two phase 3 clinical trials have been conducted, Evoke and Evoke+, testing the drug in patients with Alzheimer's disease. The trial management presented results of the intermediate readout at week 104 of the CDR-SB scores, which were negative. On the basis of that, the management decided to declare the trials a failure. However, data from week 130 and 156 had not been statistically analyzed.
Objective
When evaluating time points 130 and 156, several results show a separation between drug group and placebo group with semaglutide showing better results.
Methods
Using the means, converting the SEMs to SDs and numbers of patients per group, I analyzed the results using the Welch T-test (two-tailed), which does not assume equal SD.
Results
The ADCS-ADL-MCI test, Evoke trial, week 130, did show a significant difference, p = 0.0039. Other test such as the ADAS-cog-13 results show trends towards improvement by semaglutide at week 156. Cerebrospinal fluid biomarker analyses showed significant differences in some AD markers, too.
Conclusions
The results did show some limited drug effects at later time points of the trials. However, Semaglutide has been designed to stay in the blood for a long time and therefore does not cross the blood-brain barrier readily. Novel GLP-1 type drugs that can cross the blood-brain barrier easily may show superior protective effects in AD patients.
Introduction
Alzheimer's disease (AD) is a progressive neurodegenerative disorder for which there is no cure. Current treatments only marginally affect disease progression, and there is a great need for novel treatments that do not have serious side effects and are easy to apply. Glucagon-like peptide-1 (GLP-1) is a peptide hormone that serves many roles in the body. GLP-1 receptor agonists have been developed to treat type 2 diabetes and weight loss. 1 In addition to normalizing blood glucose levels and reducing appetite, GLP-1 receptor agonists have shown neuroprotective effects in animal models of AD, Parkinson's disease, stroke, and others. 2 A recent phase 2 trial testing the GLP-1 analog Liraglutide (Victoza, Saxenda) 3 in patients with AD showed a reduction of cognitive deterioration as well as a reduction in the shrinkage of brain areas that are affected by the disease. 4 In addition, analyses of patient databases who took semaglutide to treat diabetes show a reduction in the risk of developing AD over time when compared to patients who took other diabetes drugs.5,6 Based on considerable evidence that GLP-1 receptor agonists have neuroprotective properties, the company Novo Nordisk conducted two large Phase 3 trials, testing their drug semaglutide 3 in the oral formulation in patients with mild cognitive impairment (MCI)/AD: Evoke (1855 patients at starting point) and Evoke + (1953 patients at starting point). The trial was supposed to go on for 3 years with a follow-up of 4 months. 7 On 3 December 2025, the intermediate results at week 104 had been presented at the Clinical Trials on Alzheimer's Disease (CTAD) conference in San Diego. The primary endpoint was the result in the CDR-SB test scores at week 104. As this had been defined as the primary endpoint in the trial design, the trial was declared a failure, and the trial had been stopped. No further data had been statistically analyzed. The results have been published. 8 However, some of the patient cohort had already completed the week 130 assessments (around 450 patients per group), and around 250 patients per group had finished the trials at week 156. These data had not been analyzed in post-hoc evaluations. Such analyses can provide important information on the effects of semaglutide and can be helpful for planning new trials with drugs may show better effects in the clinic than semaglutide.
Methods
In order to analyze data sets statistically, the means, standard deviations (SDs), and number of patients are required. In the presentation given at the CTAD conference, these parameters had been published. The data shown were means and standard errors of the means (SEMs), and the patient numbers were given on the slides. I therefore extracted the information from the presentation graphs using graphical methods and used a Welch T-test, which does not assume equal SDs. The SDs of groups were not equal in the data sets. The graphs showed SEMs which were converted to SDs using the formula SEM times the square root of the sample size (n). The T-test was two-tailed. The statistical program used is available for free online: https://www.statskingdom.com/150MeanT2uneq.html.
Results
When analyzing the time point 130 weeks, there was a significant difference between drug group and placebo group in the Change in the 24-item Alzheimer's Disease Cooperative Study Activities of Daily Living Scale for Mild Cognitive Impairment (ADCS-ADL-MCI) test in the Evoke + group. Placebo group: mean 9.9; SEM 6.6; n = 433. Drug group: mean 11.25; SEM 7.5; n = 448 (DF = 879; t = 2.89; p = 0.0039). In addition, the time points at week 156 showed a non-significant improvement in Evoke and Evoke + trials (Figure 1). Similarly, there were trends for improvements by semaglutide in the ADAS-cog-13 results at week 156 for Evoke and Evoke + (Figure 2). In addition, there was a trend for improvement in the Montreal Cognitive Assessment (MoCA) scores in the Evoke + data at week 156 (Figure 3). Furthermore, there was a trend for improvement in the Mini-Mental State Examination (MMSE) scores (Figure 4).
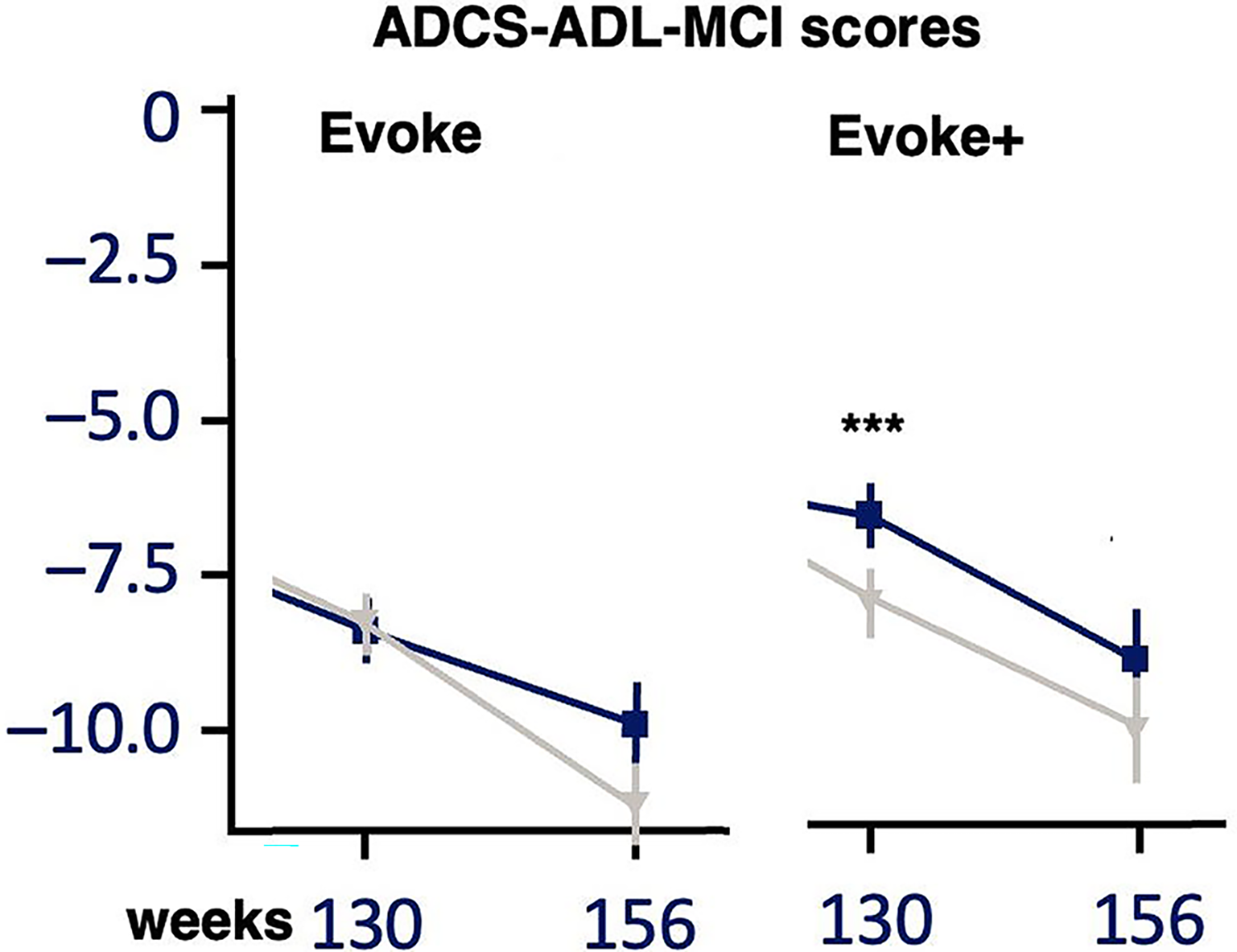
Scores in the ADCS-ADL-MCI tests, weeks 130 and 156 (lower scores are worse). Means and SEMs are shown. ***p = 0.0039.
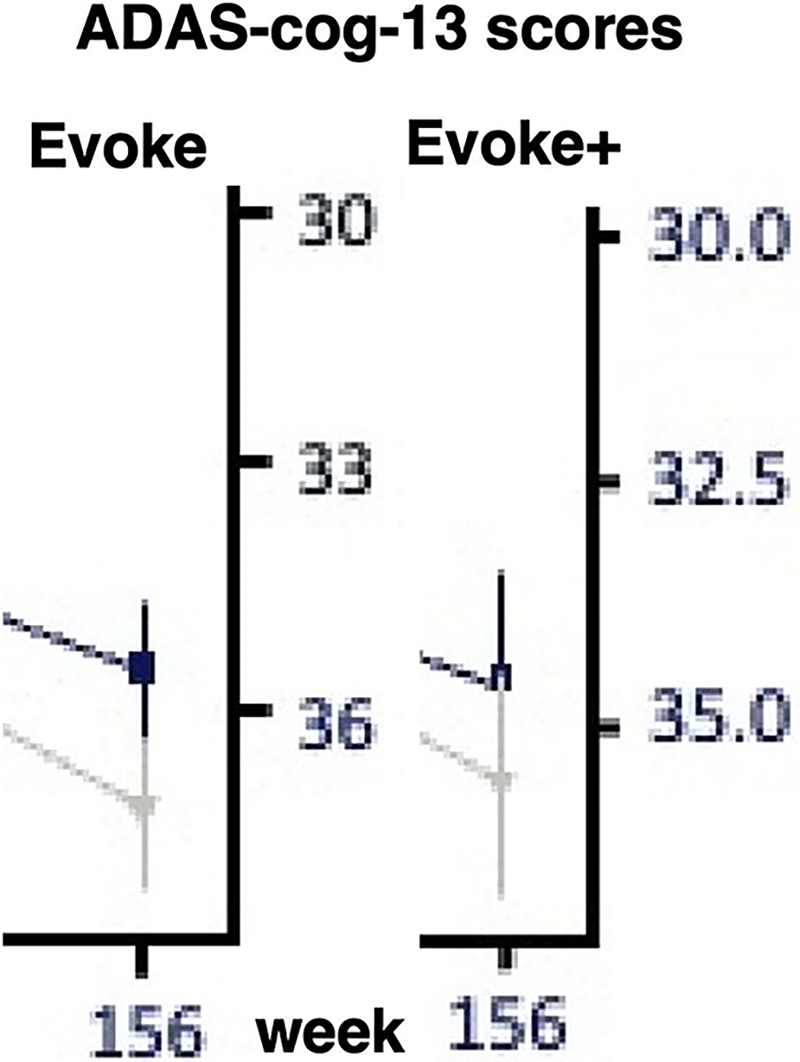
ADAS-cog-13 scores. (Higher scores are worse). Means and SEMs are shown.
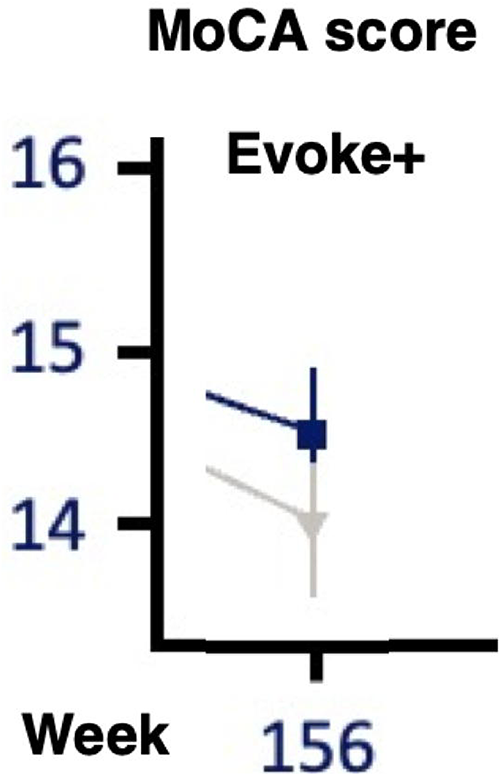
The Montreal Cognitive Assessment (MoCA) scores (lower scores are worse). Means and SEMs are shown.
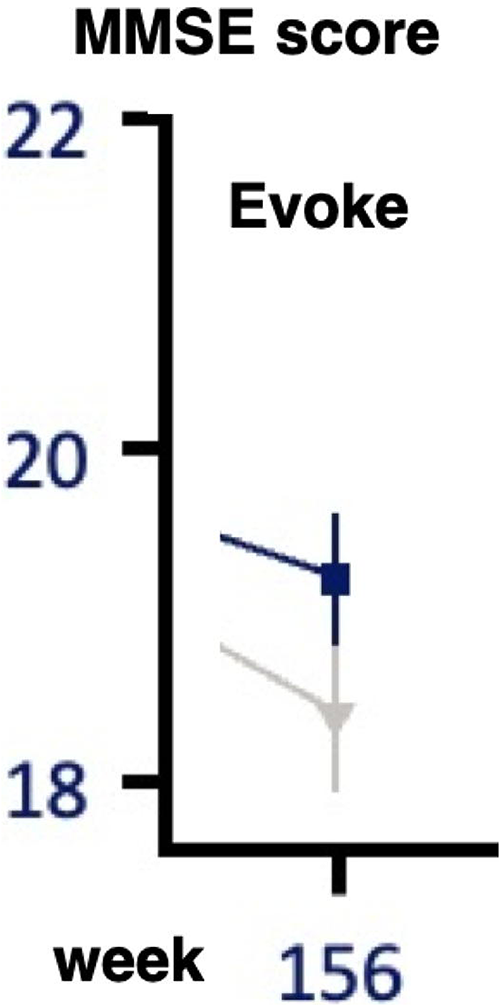
Mini-Mental State Examination (MMSE) scores (lower scores are worse). Means and SEMs are shown.
It is noteworthy that biomarkers that are associated with AD were improved by semaglutide treatment, too. Cerebrospinal fluid (CSF) samples had been collected at week 78, and several phosphorylated tau species were found to be reduced in the drug group (p-tau181; np-tau205; p-tau217; np-tau181; total tau levels) The biomarker YKL-40 which is associated with neuroinflammation was reduced, too. In addition, the biomarker neurogranin that is associated with neurodegeneration was reduced by drug treatment, too. For details, please refer to. 8 No CSF samples had been taken at the end of the trials at week 156, which may well have shown stronger reductions of AD-related biomarkers. In addition, the conversion rate of patients progressing from the MCI status to the AD status was different, with the drug group converting at 75% and the placebo group at 100%. In this study, all patients from both trials had been pooled and the numbers of patients that had been diagnosed with AD had been plotted over time. 8
Discussion
In conclusion, the results show that the drug effect of semaglutide was limited but not zero as claimed by the clinical trials management and in the publication of the trial results. 8 At week 130, there was a significant result in the ADCS-ADL-MCI test, and there were several trends towards improvement by Semaglutide treatment at week 156. However, there were only around 200–250 patients per group at that time point. A continuation of the clinical trial would have increased the number of patients at that time point and most likely resulted in more significant differences between drug and placebo groups at week 130 and 156. As there were two trials, the results of both trials could be pooled to enhance patient numbers per group and statistical power. It is important to fully analyze the trial results and to publish the full results of the trials. The fact that semaglutide did show some limited effects supports the concept that GLP-1 receptor agonists show promise in treating diseases such as AD, in particular if these drugs can cross the blood-brain barrier (BBB) easier than semaglutide. A study that measured semaglutide in CSF only showed a 0.1% influx into the brain. 9
A previous phase 2 study showed an improvement in the ADAS-exec test battery when testing the GLP-1 analogue Liraglutide in patients with AD. 4 The difference to semaglutide is that Liraglutide has a short half-life in the blood of about 10–14 h. 10 In contrast, Semaglutide has a half-life in the blood of about 7 days,11,12 which is ideal for treating diabetes, but because of that, the drug does not enter the brain readily,9,13,14 and is therefore not ideally suited for treating CNS diseases. Clearly, a GLP-1 receptor that can readily cross the BBB is required to show superior target engagement. We and others have shown that drugs of this class that can enter the brain more easily showed superior neuroprotective effects in the brain in several animal studies.15–19 Other GLP-1 receptor agonists that can cross the BBB better (exenatide, lixisenatide) have shown better efficacy in clinical trials in patients with Parkinson's disease. Drugs that can enter the brain readily showed good effects in phase 2 clinical trials,20,21 while a GLP-1 receptor agonist that does not enter the brain well did not show effects in a phase 2 trial. 22 We have developed novel dual GLP-1/GIP receptor agonists that have a CPP amino acid sequence added which can cross the BBB at an accelerated rate13,14 and that show superior protection in animal models of AD or Parkinson's disease.16–19,23–25 These findings bring hope to patients and carers and should spur new drug discovery programs that are likely to lead to novel treatments that will make a difference.
Limitations
This study is not an exhaustive post-hoc analysis of the Evoke and Evoke + trials, but rather a first exploratory evaluation to demonstrate that semaglutide did show some limited effects in several assessments that have not been analyzed in post-hoc tests up to now. As there is a great need for novel treatments for AD, and since the data sets generated in the two trials of a very large number of patients that took the drug or placebo, attended the different tests and gave blood samples, it is of great importance to make full use of these unique data sets and learn from the outcomes in order to be able to design future clinical trials testing GLP-1 type drugs that perhaps have an increased ability to cross the BBB.
Footnotes
Acknowledgements
The author has no acknowledgments to report.
Ethical considerations
Not applicable
Consent to participate
Not applicable
Consent for publication
Not applicable
Author contribution(s)
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CH is a named inventor on patents that cover GLP-1, GIP or dual GLP-1/GIP receptor agonists as treatments for AD and PD. He is the CSO of the biotech company Kariya Pharmaceuticals Ltd, Denmark.