
Abstract
Background
Arterial stiffness is an emerging risk factor for Alzheimer's disease (AD) and related dementias (ADRD) and is assessed by measuring pulse wave velocity (PWV). Recent mathematical modeling has allowed for the delineation of arterial stiffness caused by structural remodeling (S) and blood pressure, termed “load-dependent” stiffening (LD). While we recently demonstrated that S-PWV and LD-PWV are differentially associated with risk for cognitive decline and AD/ADRD brain imaging biomarkers, the associations between paired measures of S-PWV and LD-PWV with cognitive function, AD/ADRD brain imaging biomarkers, and plasma AD biomarkers have not been assessed.
Objective
To conduct a comprehensive analysis combining cross-sectional data from the Wake Forest Alzheimer's Disease Research Center. We hypothesized that higher S-PWV would be associated with worse cognitive function. We also hypothesized that S-PWV and LD-PWV would be differentially associated with brain imaging biomarkers of ADRD and plasma AD biomarkers.
Methods
Multivariable linear regression models were used to relate S-PWV and LD-PWV to all outcomes.
Results
As hypothesized, higher S-PWV, but not LD-PWV, was associated with lower global cognitive function. Higher S-PWV and LD-PWV were differentially associated with AD/ADRD brain MRI biomarkers. We did not observe any significant associations with plasma or PET AD biomarkers in this cohort.
Conclusions
S-PWV was associated with lower cognition, while S-PWV and LD-PWV were differentially associated with brain MRI biomarkers. Interventions specifically targeting arterial stiffness may preserve cognition and brain health in AD/ADRD.
Introduction
The majority of patients with ‘probable Alzheimer's disease (AD)’ present with co-occurring vascular cerebral small vessel disease in addition to AD pathology.1–5 Accordingly, vascular contributions to cognitive Impairment and dementia have been increasingly linked to risk for AD and AD and related dementias (ADRD); yet, the pathways underlying these relationships remain unclear. Arterial stiffness has emerged as an age-related subclinical risk factor for the development of abnormalities in cerebral perfusion, cerebral small vessel disease, AD pathology, and cognitive decline or dysfunction.6–19 Recently, the Alzheimer's Association Workgroup revised their AD and ADRD biomarker criteria to include “Vascular Brain Injury” (e.g., white matter hyperintensities or infarction) as part of the revised “AT(N)” framework (Amyloid and Tau, with Neurodegeneration) as a measure of “non-AD co-pathology”. 20 Thus, vascular brain injury may be a downstream consequence of elevated arterial stiffness that ultimately results in cognitive dysfunction and ADRD development.
Arterial stiffness is caused by two mechanisms: (1) elevated blood pressure increasing the load-dependent or “functional” stiffness of the arterial wall (LD); and (2) morphological changes to the structure of the arterial wall (S).21–25 These mechanisms are often reported as a combined measurement, here called total pulse-wave velocity (T-PWV). T-PWV has recently been delineated into its LD-PWV and S-PWV subcomponents using mathematical modeling21–24; allowing for the non-invasive assessment of stiffness centrally, using the gold-standard carotid-femoral PWV, 26 or in specific arteries such as the carotid artery, using B-mode ultrasound. The delineation of S-PWV and LD-PWV provides a more accurate understanding as to how stiffness is related to cognitive deficits and worse brain health in ADRD. For instance, in the Multi-Ethnic Study of Atherosclerosis (MESA) higher carotid artery S-PWV, but not LD-PWV, like drove the observed association between T-PWV and dementia risk. 22 Our group also expanded on these findings in the MESA to demonstrate differential associations between S-PWV and LD-PWV with cognitive decline and magnetic resonance imaging (MRI) imaging biomarkers. Specifically, carotid artery T-PWV and S-PWV were associated with cognitive decline over 12 years and total gray matter volume and white matter hyperintensities, while LD-PWV was only associated with white matter fractional anisotropy. 27 Further, another study observed that higher central S-PWV, but not LD-PWV, was associated with higher white matter hyperintensities and lower cortical thickness. 25 These results suggest that S-PWV is associated with risk for cognitive decline, gray matter atrophy, and white matter disease, while LD-PWV is associated with aspects of poorer white matter microstructure.
Association studies examining the relationships between arterial stiffness and positron emission tomography (PET) and plasma AD biomarkers have been inconsistent. In prior studies we observed that central T-PWV was positively associated with amyloid-β (Aβ) deposition and its accumulation over time,8,14,15 while others did not.28,29 Another study observed that that measures of carotid stiffness, but not central T-PWV, were associated with brain Aβ-PET. 30 Moreover, central T-PWV was associated with tau-PET and cerebrospinal fluid measures of neuroinflammation and tau pathology; with the strength of these associations increasing with age across cohorts evaluated.28,29
We previously published on the relationships between central T-PWV, cognition, and brain MRI biomarkers in the Wake Forest Alzheimer's Disease Research Center (ADRC) Healthy Brain Study. 16 However, to date, no study has investigated the associations of central S-PWV and LD-PWV with cognition, MRI and PET imaging biomarkers, or plasma AD biomarkers in the same cohort of participants. Here, we provide a comprehensive analysis expanding on our prior findings by examining these cross-sectional associations in the same cohort. Based on the prior literature, we hypothesized that only higher S-PWV would be associated with lower cognitive function; yet, both central LD-PWV and S-PWV would be associated with worse brain MRI and plasma and PET biomarkers of AD/ADRD.
Methods
Participants
The Healthy Brain Study of Wake Forest ADRC Clinical Core began enrolling participants in 2016 with the goal of identifying vascular and metabolic risk factors for AD/ADRD. Existing data from adults between 55 and 85 years of age (N = 516) enrolled in the Wake Forest ADRC Clinical Core were leveraged for this study. All Clinical Core participants were invited to participate in a combined oral glucose tolerance test and central arterial stiffness measurement between study initiation and March 2020. Enrollment was stopped in March 2020 due to COVID-19. Participants were excluded if they had a history of large vessel stroke; non-AD neurological diseases; evidence of organ failure, active cancer treatment, uncontrolled clinical depression, or psychiatric illness; current use of insulin; or history of substance abuse or heavy alcohol consumption within the previous 10 years. All study procedures were approved by the Wake Forest Institutional Review Board and are consistent with the ethical standards described by the 1964 Declaration of Helsinki. All participants and/or their legally authorized representative provided written informed consent.
Medications
Prescription and over-the-counter medications were self-reported by participants. To control the influence of anti-hypertensive medication use, we adjusted for an indicator of any anti-hypertensive medication use as a covariate in our models.
Blood pressure and arterial stiffness measurement
Participants were asked to fast for a minimum of 6 h prior to clinic visits including vascular assessments and blood draw. A single seated brachial blood pressure measurement was taken using a DINAMAP automated blood pressure device (GE Healthcare). Participants were seated quietly for 5 min in a dark room prior to the blood pressure measurement. Blood pressure was categorized as previously described by the American College of Cardiology/American Heart Association guidelines. 31 Participants also rested supine for 5 min prior to the measurement of supine brachial blood pressure and carotid-femoral PWV (SphygmoCor Xcel, CONNEQT Health), as previously described. 16 Carotid-femoral PWV was measured twice and averaged. Carotid-femoral PWV is considered a measure of central T-PWV for this analysis,32,33 and is expressed in units of meters per second (m/s).
LD-PWV and S-PWV calculations
LD-PWV and S-PWV were calculated using participant-specific exponential models, the methodology for which has been documented elsewhere.21–25 Briefly, T-PWV was normalized to each participant's blood pressure, and then S-PWV was calculated using a nonlinear stiffness parameter at a reference blood pressure of 120/80 mmHg. LD-PWV was calculated as the difference between T-PWV and S-PWV.
Magnetic resonance imaging
Participants were scanned using a 3-Tesla Siemens Skyra MRI equipped with a 32-channel head coil to acquire T1, T2 fluid-attenuated inversion recovery, neurite orientation dispersion and density imaging, diffusion tensor imaging, and arterial spin labeling scans. 16 The imaging acquisition parameters have been published elsewhere in more detail.16,34–40 T1 normalization and tissue segmentation was performed using SPM12 (www.fil.ion.ucl.ac.uk/spm) CAT12, and cortical thickness and total intracranial volume were calculated from T1 using FreeSurfer v7.2 (https://surfer.nmr.mgh.harvard.edu).16,41 White matter hyperintensity volume (WMHv) segmentation was performed using the lesion growth algorithm in the LST toolbox using SPM12 from T2 fluid-attenuated inversion recovery and T1.16,42 Diffusion tensor imaging, neurite orientation dispersion and density imaging, and arterial spin labeling processing details have previously been published.16,43 Free water (FW) metrics were calculated from neurite orientation dispersion and density imaging. MRI metrics include FreeSurfer temporal cortical thickness and total gray matter volume (GMv), whole-brain WMHv, white matter (WM) and GM FW, WM fractional anisotropy (FA), GM and WM cerebral blood flow (CBF), and GM CBF spatial coefficient of variation (sCOV). Mean WM FW, FA, and CBF were calculated from supratentorial JHU WM tracts. 37 Mean GM FW, CBF, and sCOV were calculated from supratentorial automated anatomical labeling GM ROIs. 44 A log transformation was applied to WMHv to account for its skewed distribution. MRI brain volumes and WMHv were adjusted for total intracranial volume to account for head size.
Cognitive testing
Participants underwent extensive cognitive testing using the Uniform Data Set Version 3 (UDSv3). 16 The UDSv3 battery includes the Montreal Cognitive Assessment (MoCA), Craft Story, Benson Figure, Number Span, Phone-mic Fluency (letters C, F, and L), Category Fluency (Animals and Vegetables), Trail Making Test A and B, and the Multilingual Naming Test.16,45 Z-scores for each test were based on the expanded UDSv3 cognitive test normative data.16,45 UDSv3 scores were normalized for age, sex, race, and education, thus the statistical models that include UDSv3 scores were not adjusted for those variables. Executive function, memory, language, attention, and visuospatial cognitive domain scores were created as the mean of normed Z-scores.16,46
Participants also underwent additional supplemental cognitive tests to aid in the cognitive adjudication (Mini-Mental State Examination and American Adult Reading Test), and to measure executive function and processing speed (Digit Symbol Coding Test) and memory (Rey Auditory Verbal Learning Test and Free and Cued Selective Reminding Test). 16 Five cognitive tests were used to calculate the modified Preclinical Alzheimer's Cognitive Composite (PACC5).16,47 PACC5 data were normalized to the cognitively normal group.16,48
Cognitive adjudication
All available cognitive, functional, and behavioral data were used in the adjudication process to determine cognitive status according to the National Institute on Aging-Alzheimer's Association guidelines for diagnosing mild-cognitive impairment and dementia16,49,50 by an expert panel consensus review. 16
Aβ-PET imaging
Fibrillary Aβ deposition was measured using PET imaging with [11C]-Pittsburgh compound B ([11C]PiB), 51 as previously described.52,53 Participants were injected with ∼10mCi (approximately 370 MBq) [11C]PiB bolus, intravenously. 53 Attenuation correction was performed using computed tomography, following which participants were scanned using a 64-slice GE Discovery MI DR PET/CT scanner for 40 to 70 min. 53 [11C]PiB uptake was used to measure Aβ deposition and was quantified using voxel wise standardized uptake volume ratio (SUVR). 53 Aβ was analyzed both as a continuous variable (Pittsburgh compound B PET SUVR, PiB PET SUVR) and as a binary, categorical variable indicating amyloid positivity (Aβ- or Aβ+) utilizing SUVR cut-point ≥1.21.53,54
Tau-PET imaging
Tau-PET deposition was assessed using [18F]Flortaucipir.55,56 Approximately 10mCi (370 MBq) (+/-10%) [18F] Flortaucipir bolus was injected intravenously, after which participants rested for 75-min. Following rest, continuous emission images were acquired using a 64-slice GE Discovery MI DR PET/CT scanner (6 × 5-min frames). The tau-PET image was corrected for attenuation using the participant's CT scan. Rigid registration aligned motion corrected PET frames to their MRI scan (PMOD, v.4.1). The inferior cerebellar grey region was referenced to generate a voxel wise tau SUVr image. FreeSurfer segmented anatomical regions (Desikan-Killiany atlas) were used to create a temporal meta-region mask.57–59 The mask was then applied to the SUVR image that served as a biomarker of tau deposition.
Plasma AD biomarkers
Blood was drawn in the fasting state and processed within 30 min, as previously described. 53 Plasma samples were analyzed using Quanterix Simoa Neurology 4-Plex E and phosphorylated tau (p-tau)181 version 2 Advantage Kits on a Quanterix Simoa HD-X. 53 Plasma neurofilament light (NfL), glial fibrillary acidic protein (GFAP), Aβ42, Aβ40, and p-tau181 were measured in batch by the National Centralized Repository for ADRD Biomarker Assay Laboratory. 53 Plasma p-tau217 was measured in duplicate using the ALZpath Simoa p-tau217 assay on a Simoa HD-X at Neurocode (Bellingham, WA).53,60 The Aβ42/40 ratio was calculated.53,61,62 The concentration of each plasma AD biomarker is reported in picograms per milliliter (pg/mL).
Statistical analysis
Our study included 516 participants with central PWV and at least one measure of cognitive function, cognitive status, or MRI, PET, or plasma AD/ADRD biomarkers. Differences in demographic data among cognitive states were assessed using chi-square tests and ANOVA. Associations between central PWV measures (T-PWV, S-PWV, and LD-PWV) and normed cognitive domain scores were assessed using multivariable linear regression. Two models were employed to assess the association with cognitive function. Model one did not adjust for co-variates and model two adjusted for BMI, and anti-hypertensive medications.
Multivariable linear regressions were used to assess the associations between central PWV measures and MRI, amyloid and tau PET SUVR, and plasma AD biomarkers. Logistic regressions were performed to assess the association between central PWV measures and amyloid PET positivity (Aβ- or Aβ+). Like cognitive function, two models were employed. Model one adjusted for age, sex, race/ethnicity, education, BMI, and anti-hypertensive medication use, and Model two adjusted for model one co-variates and cognitive status. In these models, central PWV, imaging, and plasma AD biomarkers were standardized by subtracting the mean and dividing by the standard deviation.
To control for potential sampling bias, we also investigated whether sex, race, age, education, and cognitive status were associated with missing amyloid and tau PET SUVR. We observed race/ethnicity and cognitive status were associated with missing tau PET SUVR, while only race/ethnicity was associated with missing amyloid PET SUVR. As such, we developed sampling weights that were applied to all linear regression analyses on amyloid and tau PET SUVR. Amyloid PET SUVR weights were equal to the total number of participants in the racial category divided by the number of participants in the racial category that had amyloid PET SUVR data. For tau PET SUVR models, weights were equal to the total number of participants in the racial/ethnicity x cognitive status category divided by the number of participants in the racial/ethnicity x cognitive status category that had tau PET SUVR data. Diversity, equity, and inclusion were considered in our study design. Sex and self-reported race/ethnicity were included as co-variates in our models. We systematically explored the interaction effect of age, cognitive status, self-reported race/ethnicity, and sex on our outcomes and performed stratified analyses.
Statistical significance was defined as a false discovery rate (FDR) < 0.05. FDR was calculated by sorting and ranking nominal p-values from smallest to largest and multiplying the nominal p-value by the number of models and dividing by the rank. A 0.05 nominal significance level was used if the FDR p-value was not significant and for all interaction effects and stratified analyses. As we did not have a priori hypotheses, the findings from the interaction effect and stratified analyses should be considered exploratory and interpreted cautiously.
Lastly, after completing all analyses, we evaluated the influential data points by calculating the Cook's Distance. If an observation had a Cooks Distance >4/n, then it was considered an outlier, and the analyses we re-performed. Only the results from analyses excluding outliers are presented.
Results
Participant characteristics
The overall cohort had a mean age of 70.4 (SD = 8.1) years and was composed of a greater proportion of females (56%) than males (Table 1). Cognitive adjudication determined that 287 participants had normal cognition, 176 had MCI, and 53 had dementia (Table 1). Participant characteristics were then stratified by cognitive status, and several demographic differences were observed between groups (i.e., age, sex, education, and race/ethnicity). Participants with dementia exhibited the lowest cognitive function, brain volume, and cerebral blood flow and the highest indices of WM injury, Aβ-PET and tau-PET, and plasma AD biomarkers (Table 1). There were no significant cognitive group differences in mean T-PWV, S-PWV, or LD-PWV. However, there was a nominally significant association for T-PWV (P = 0.041), such that it was highest in the MCI and dementia groups compared to those with normal cognition. The correlations between age and measures of PWV and blood pressure are shown in Figure 1.
Demographics and participant characteristics by cognitive status.

Participant demographics are presented in the full cohort and stratified by cognitive status. Hypertension was defined as being on anti-hypertension medications or Stage 1 or Stage 2 hypertension based on measured blood pressure. MPACC5 version FCSRT96 is reported. Raw (non-standardized) cognitive data are reported. Our analysis was restricted to participants with all three central arterial stiffness measures. WMHv data were adjusted for intracranial volume and log transformed. GMv was scaled to intracranial volume. NC: normal cognition; MCI: mild cognitive impairment; BMI: body mass index; MoCA: Montreal Cognitive Assessment; mPACC5: modified preclinical Alzheimer cognitive composite 5; SBP: systolic blood pressure; DBP: diastolic blood pressure; T-PWV: total pulse-wave velocity; S-PWV: structural pulse-wave velocity; LD-PWV: load-dependent pulse-wave velocity; GMv: gray matter cortical volume; GM FW: gray matter free water; a.u.: arbitrary units; WMHv: white matter hyperintensity volume; WM FA: white matter fractional anisotropy; WM FW: white matter free water; GM CBF: gray matter cerebral blood flow; WM CBF: white matter cerebral blood flow; GM CBF sCOV: gray matter cerebral blood flow spatial coefficient of variation; Aβ: amyloid-β; PET: positron emission tomography; PiB PET SUVR: Pittsburgh compound B PET standardized uptake value ratio; p-tau: phosphorylated tau; NfL: neurofilament light; GFAP: glial fibrillary acidic protein. p-values for categorical variables were obtained using chi-square tests. Pairwise tests use a Bonferroni correction [alpha (0.0167) = 0.05/3] to adjust for multiple comparisons. * < 0.05/3 MCI versus NC, +<0.05/3 dementia versus NC, and # < 0.05/3 MCI versus dementia. p-values for continuous variables were obtained using one way ANOVA models. Pairwise tests use Tukey's method for multiple comparisons. * < 0.05 MCI versus NC, +<0.05 dementia versus NC, and # < 0.05 MCI versus dementia.
Associations between central PWV and cognitive function
We next assessed the association between central T-PWV, S-PWV, and LD-PWV with measures of global cognition and five cognitive domains. In unadjusted models, higher T-PWV was significantly associated with lower global cognition (MoCA and mPACC5) and appeared to be due to higher S-PWV, but not LD-PWV (Table 2). Furthermore, a significant association was observed between higher T-PWV and lower executive function (FDR P = 0.042) in Model 2, which may be more closely related to S-PWV (Nominal p = 0.051) than LD-PWV (Nominal p = 0.73). The associations between T-PWV and S-PWV with global cognition (MoCA and mPACC5) were only slightly attenuated after adjusting BMI and anti-hypertensive medications in Model 2. There were no significant or nominally significant associations between our measures of central PWV and the remaining cognitive domains, including memory, language, attention, and visuospatial.
Standardized cognitive test performance associated with arterial stiffness measures.

The estimate, SE, and p-values for the association between central arterial stiffness (PWV) and cognitive measures are presented. Model 1 was not adjusted because cognitive scores are normed for age, sex, race/ethnicity, and education. Model 2 was adjusted for BMI and anti-hypertensive medications. Regression coefficients correspond to a decrease (where negative) in cognitive test performance corresponding to a one unit increase in central stiffness. Our analysis was restricted to participants with all three arterial stiffness measures. The MoCa data and three central stiffness measures were standardized. T-PWV: total pulse-wave velocity; S-PWV: structural pulse-wave velocity; LD-PWV: load-dependent pulse-wave velocity; SE: standard error; BMI: body mass index; SBP: systolic blood pressure; MoCA: Montreal Cognitive Assessment; mPACC5: modified preclinical Alzheimer cognitive composite 5. Cook's Distance was calculated for each observation, and models were refit with observation where Cook's Distance > 4/n was removed. Statistical significance was set at false discovery rate <0.05* and displayed in bold text. Nominal significance was set at p < 0.05# and displayed in bold text.
Associations between central PWV and MRI ADRD biomarkers
We observed that higher central T-PWV and S-PWV were significantly associated with higher GM and WM FW, which is indicative of lower integrity (Table 3). Further, higher LD-PWV was significantly associated with higher GM FW. T-PWV was inversely associated with WM FA, likely driven by higher LD-PWV. Only a nominally significant association was observed between T-PWV and WMHv in Model 2. Lastly, higher LD-PWV was associated with lower CBF metrics, including GM CBF, WM CBF, and GM CBF sCOV (Table 3).
Linear regression coefficients of arterial stiffness and MRI ADRD biomarkers.

The estimate, SE, and p-values for the association between arterial stiffness and MRI biomarkers of ADRD are presented. The three central arterial stiffness measures and all outcomes were standardized. Model 1 was adjusted for age, sex, race/ethnicity, education, BMI, and anti-hypertension medications and Model 2 was adjusted for Model 1 co-variates and cognitive status. WMHv data were adjusted for intracranial volume and log transformed. GMv was scaled to intracranial volume. ADRD: Alzheimer's disease and related dementias; MRI: magnetic resonance imaging; SE: standard error; T-PWV: total pulse-wave velocity; S-PWV: structural pulse-wave velocity; LD-PWV: load-dependent pulse-wave velocity; BMI: body mass index; a.u.: arbitrary units; GMv: gray matter cortical volume; GM FW: gray matter free water; WMHv: white matter hyperintensity volume; WM FA: white matter fractional anisotropy; WM FW: white matter free water; GM CBF: gray matter cerebral blood flow; WM CBF: white matter cerebral blood flow; GM CBF sCOV: gray matter cerebral blood flow spatial coefficient of variation. Cook's Distance was calculated for each observation, and models were refit with observation where Cook's Distance > 4/n was removed. Statistical significance was set at false discovery rate <0.05* and displayed in bold text. Nominal significance was set at p < 0.05# and displayed in bold text.
Associations between central PWV and PET imaging and plasma AD/ADRD biomarkers
We did not observe any significant or nominally significant associations between measures of central arterial stiffness and continuous Aβ-PET or tau-PET (Table 4) or with amyloid positivity (Supplemental Table 1). There were also no significant associations between the three measures of arterial stiffness and any plasma AD biomarker (Table 4). However, we observed a nominally significant association between higher T-PWV and S-PWV with a lower Aβ42/40 ratio in Model 2 that was not statistically significant after FDR adjustment.
Linear regression coefficients of arterial stiffness and PET and plasma AD/ADRD biomarkers.

The estimate, SE, and p-values for the association between arterial stiffness and plasma AD biomarkers are presented. The three central arterial stiffness measures and all outcomes were standardized. PET and tau outcomes were weighted to control for sampling bias. Model 1 was adjusted for age, sex, race/ethnicity, education, BMI, and anti-hypertensive medications and Model 2 was adjusted for Model 1 co-variates and cognitive status. AD: Alzheimer's disease; PET: positron emission tomography; PiB PET SUVR: Pittsburgh compound B PET standardized uptake value ratio; T-PWV: total pulse-wave velocity; S-PWV: structural pulse-wave velocity; LD-PWV: load-dependent pulse-wave velocity; Aβ: amyloid-β; p-tau: phosphorylated tau; NfL: neurofilament light; GFAP: glial fibrillary acidic protein; BMI: body mass index. Cook's Distance was calculated for each observation, and models were refit with observation where Cook's Distance > 4/n was removed. Statistical significance was set at false discovery rate <0.05* and displayed in bold text. Nominal significance was set at p < 0.05# and displayed in bold text.
Interaction effects
To explore potential effect modification by age, sex, race/ethnicity, or cognitive status with the three arterial stiffness exposures on all outcomes, we tested the characteristic x stiffness interaction effects and then stratified by participant characteristic (Supplemental File 2). A nominally significant age x LD-PWV interaction effect was observed for tau PET and age x S-PWV interaction effect was observed for plasma Aβ40. However, stratified analyses did not reveal any nominally significant associations (55–64, 65–74, and 75 + years).
Multiple nominally significant sex x arterial stiffness interaction effects were observed, and stratified analyses revealed many of these associations were driven by males, but not females. For example, a sex x T-PWV and S-PWV interaction effect was observed, such that higher T-PWV and S-PWV were associated with higher WMHv in males, but not females. Similarly for WM FA and WM FW, sex x S-PWV interaction effects were observed, where higher S-PWV was associated with lower WM FA and higher WM FW only in males. A sex by LD-PWV association was also observed with plasma NFL, which was only observed in males. However, a sex x LD-PWV interaction effect revealed a negative nominal association between LD-PWV and plasma Aβ42 only in females. Lastly, we observed and sex x LD-PWV interaction effect, such that, LD-PWV was positively associated with plasma p-tau181 in males, but not females. The interaction effects and sex-stratified analyses also revealed several counterintuitive associations in males, such as a positive association between T-PWV and WM CBF and a negative association between S-PWV and plasma p-tau181.
Only one race/ethnicity x arterial stiffness interaction effect was observed, such that higher S-PWV was nominally associated with lower total GMv in self-identified Black participants. We also observed multiple cognitive status x arterial stiffness interaction effects. With regards to MRI ADRD biomarkers, we observed that higher T-PWV and S-PWV were nominally associated with higher WM and GM FW in adults with NC and MCI. Additionally, S-PWV was nominally associated with higher WMHv in adults with MCI, and higher T-PWV was nominally associated with lower temporal cortical thickness in adults with MCI. With regards to plasma AD/ADRD biomarkers, we observed higher S-PWV was nominally associated with a lower Aβ42/40 ratio in adults with MCI, higher T-PWV and S-PWV were nominally associated with higher Aβ40 in adults with MCI, and higher LD-PWV was nominally associated with lower Aβ40 in adults with DEM. Higher LD-PWV was nominally associated with higher plasma p-tau 217 and higher S-PWV was nominally associated with higher GFAP in adults with NC. Lastly, higher T-PWV and S-PWV were nominally associated with higher plasma NFL in adults with DEM, and we observed a counterintuitive negative nominally association between higher LD-PWV and lower plasma NFL in adults with dementia.
In many of the stratified analyses, associations between the arterial stiffness metrics and outcomes were nominally significant when the respective interaction effects were not. For this reason, and because we tested over 200 interaction effects, the stratified analyses should be interpreted with extreme caution and require future replication.
Discussion
Using the Wake Forest ADRC Healthy Brain Study, we cross-sectionally examined associations between central total, structural, and load-dependent stiffness with existing cognitive measures, MRI and PET imaging ADRD biomarkers, and plasma AD biomarkers. Structural arterial stiffness was associated with lower global cognitive function and MRI biomarkers, while blood pressure-related or load-dependent stiffness was only associated with MRI biomarkers. Specifically, structural stiffness was most closely associated with GM and WM integrity, while load dependent stiffness was associated with lower cerebral blood flow metrics, WM neuronal integrity (Free Water) and WM microstructure (fractional anisotropy). Consistent with prior literature cognitive status and sex may modify the associations between arterial stiffness and MRI or plasma AD/ADRD biomarkers; supporting the proposition that relationships between arterial stiffness and AD/ADRD risk are more pronounced in individuals with different cognitive statuses and in males or females. However, the results from the interaction effect and stratified analyses are exploratory and should be interpreted cautiously.
In our present study, higher total and structural stiffness were significantly associated with lower global cognitive function and total stiffness was associated with lower executive function. These findings are consistent with our prior observations between central total stiffness 16 and carotid artery total and structural stiffness with cognitive function. 22 Other studies have also observed associations between central stiffness and cognition 17 or risk of MCI, vascular dementia, or AD.6,12 Moreover, a meta-analysis observed that higher total stiffness was associated with lower executive function and memory. 17 Collectively, these observations suggest that central total and structural stiffness may be associated with risk for cognitive decline and dementia. Prospective, longitudinal studies comparing the risk that higher central and carotid stiffness pose for dementia phenotypes are warranted to understand the temporal relationships between these stiffness measures and ADRD risk. Interventions aimed at reducing structural stiffness should also be considered or developed to preserve global cognitive function.
We also observed positive associations between central total and structural stiffness with GM and WM free water and between higher LD-PWV and WM perfusion, integrity, and free water. These free water metrics are markers of neuronal integrity (i.e., higher free water is indicative of lower integrity). Previously, free water was able to distinguish between adults with normal cognition versus MCI or AD,63,64 and the associations between the PWV metrics with free water persisted even after adjusting for cognitive status in this study. Thus, differences in arterial stiffness phenotype may be contributing to the association between neuronal integrity and cognition. In contrast to structural stiffness, higher load-dependent stiffness was significantly associated with lower WM fractional anisotropy, which is indicative of worse WM microstructure. 65 Thus, load-dependent stiffness may be driving the previously observed association between central total stiffness and WM fractional anisotropy. 65 Lastly, higher central total stiffness was nominally associated with higher WM hyperintensity volumes after adjusting for cognitive status. Thus, total stiffness may increase WM hyperintensity burden, independent of cognitive status.
We further observed that higher load-dependent stiffness was associated with lower mean GM and WM perfusion and GM blood flow variability. Blood flow variability quantifies the degree of variability in blood flow across different regions of the brain, and has been previously associated with dementia and cognitive decline.66–68 In the past, we demonstrated blood pressure was to be associated with cerebral blood flow. 16 Thus, blood pressure may increase load-dependent stiffness and reduce cerebral perfusion to ultimately increase the risk of cognitive dysfunction. Taken together, our findings suggest that higher load-dependent stiffness is related to greater spatial variability in GM cerebral blood flow that may be driven by cumulative pulsatile damage over the lifespan.
There are key differences in these results compared to prior studies that include MRI biomarkers. For example, we did not replicate the prior associations between arterial stiffness and GM volume. 27 This could be due to differences in the artery in which stiffness was measured (e.g., predominantly aorta versus carotid). Additionally, our data are inconsistent with observations from a recent study in which higher large-artery structural stiffness was associated with higher WM hyperintensity volume and lower cortical thickness irrespective of sex. 25 However, in accordance with the prior study, 25 we found higher central structural stiffness to be nominally associated with higher WM hyperintensity volume in males, but not females. Our stratified analyses also revealed a nominal effect of sex on our associations between central stiffness and WM fractional anisotropy and WM free water. Our findings suggest stronger relations among WM fractional anisotropy and WM free water with structural stiffness in males and WM free water with load-dependent stiffness in females.
In this analytic sample, we did not observe any significant associations between our three central stiffness metrics with PET or plasma Aβ or tau biomarkers. However, we found that higher T-PWV and S-PWV were nominally associated with a lower Aβ42/40 ratio, consistent with the hypothesis that arterial stiffness promotes AD pathology; yet this was not supported by other biomarker profiles and the lack of amyloid PET results. The broader lack of significant associations are not consistent with what we initially hypothesized but could be due to the smaller sample size of these analytic subsamples, the younger age of our analytic sample, the different methods used to measure PWV, or the vascular bed in which PWV was measured. In the past, using various methods to measure PWV observed no associations between PWV and amyloid PET deposition or status in cross-sectional analyses across several populations.8,14,29,30,69 Contrary to this, prior studies have demonstrated PWV to be associated with amyloid PET or cerebrospinal fluid tau and Aβ42 ratios in cross-sectional analyses,14,30,70,71 while carotid-femoral PWV was associated with change in amyloid PET deposition over 2-years in older adults 80 years and older. 8 This segment of the population was under represented in this analysis. These data suggest that cumulative exposure to arterial stiffness may promote AD pathology. Interestingly, sex may also modify the association between central stiffness and plasma AD biomarkers. Specifically, we observed a negative nominal association between higher central load-dependent stiffness and lower plasma Aβ42 in females, but not males. Additionally, LD-PWV was positive associated with plasma p-tau181 in males, but not females. These findings are somewhat consistent with several prior studies demonstrating arterial stiffness or surrogate measures, such as carotid-femoral PWV, pressure pulsatility, and pulse pressure were associated with PET 29 or plasma28,71 tau biomarkers in cross-sectional analyses. It is important to note these associations may also be influenced by the oldest participants, which we were underpowered to detect in this study.28,29 Future research is needed to continue to assess the effect of age and sex on the association between arterial stiffness measured in different vessels with plasma and PET AD biomarkers.
Sex also modified the association between central load-dependent stiffness with plasma NfL, such that load-dependent stiffness was nominally associated with higher plasma NfL in males. In addition to sex and plasma NFL, we observed a significant interaction effect of cognitive status on the associations between structural stiffness with plasma GFAP and NFL, where higher stiffness was nominally associated with higher plasma GFAP in adults with normal cognition and higher plasma NFL in adults with dementia. We hypothesize the association between structural arterial stiffness and GFAP represents pre-clinical inflammation that contributes to neuronal injury (represented by plasma NFL) in adults with dementia. In other words, adults with dementia are more vulnerable to astrocytic injury from pulsatile pressure, whereas in cognitively normal patients, astrocytic damage may not be detectable and only comes as a result of cumulative exposure to neuroinflammation. However, this hypothesis requires additional research.
Our study has several strengths and limitations that should be considered. This was the first study to assess the association between central stiffness caused by structural remodeling and elevated blood pressure with a wide array of cognitive measures and imaging and plasma biomarkers of AD/ADRD in the same cohort of adults. This was also among the first studies to deconstruct arterial stiffness into its structural and load-dependent components to determine how they relate to brain structure and function. This deconstruction enables a better understanding of the structural and blood pressure dependent mechanisms linking upstream arterial stiffness to AD/ADRD biomarkers underlying potential targets for dementia prevention. However, causality cannot be confirmed from a single, cross-sectional study. We also only assessed the associations between arterial stiffness and global brain imaging measures, and different associations may be observed regional imaging measures. Because the WF ADRC's Healthy Brain study is focused on a cohort of individuals at risk for developing cognitive impairment, it has a limited number of individuals with dementia at baseline. Therefore, we were not adequately powered to fully examine biomarker relationships in the dementia subgroup. Lastly, because we rigorously tested multiple interaction effects, indicating the need for stratified analyses, these results should be considered exploratory, interpreted cautiously, and replicated in the future.
Conclusions
In summary, higher central stiffness due to structural remodeling was cross-sectionally associated with lower global cognitive function. While stiffness due to structural arterial remodeling and elevated blood pressure were differentially related to MRI AD/ADRD biomarkers. We also observed interaction effects of sex, race/ethnicity, and cognitive status that require confirmation in future studies. Collectively, our data suggests that arterial stiffness components of structural and load-dependent stiffness may represent complimentary mechanisms underlying vascular contributions to dementia, rather a marker specific to AD pathology. Functionally, because adults with cognitive impairment often present with mixed vascular co-pathology,1–5 preventing vascular or mixed dementia by targeting arterial stiffness may reduce AD risk or symptom severity. Prospective, longitudinal studies and clinical trials targeting structural and load-dependent stiffness are warranted to further elucidate the relation between arterial stiffness and dementia risk and prevent or delay cognitive decline.
Arterial stiffness and BP plotted against age. (A) T-PWV, (B) S-PWV, (C) LD-PWV, (D) SBP, and (E) DBP are plotted against participant age in the Wake Forest University School of Medicine ADRC. BP: blood pressure; SBP: systolic blood pressure; DBP: diastolic blood pressure; ADRC: Alzheimer's Disease Research Center; cfPWV: carotid-femoral pulse-wave velocity; T-PWV: total pulse-wave velocity; S-PWV: structural pulse-wave velocity; LD-PWV: load-dependent pulse-wave velocity.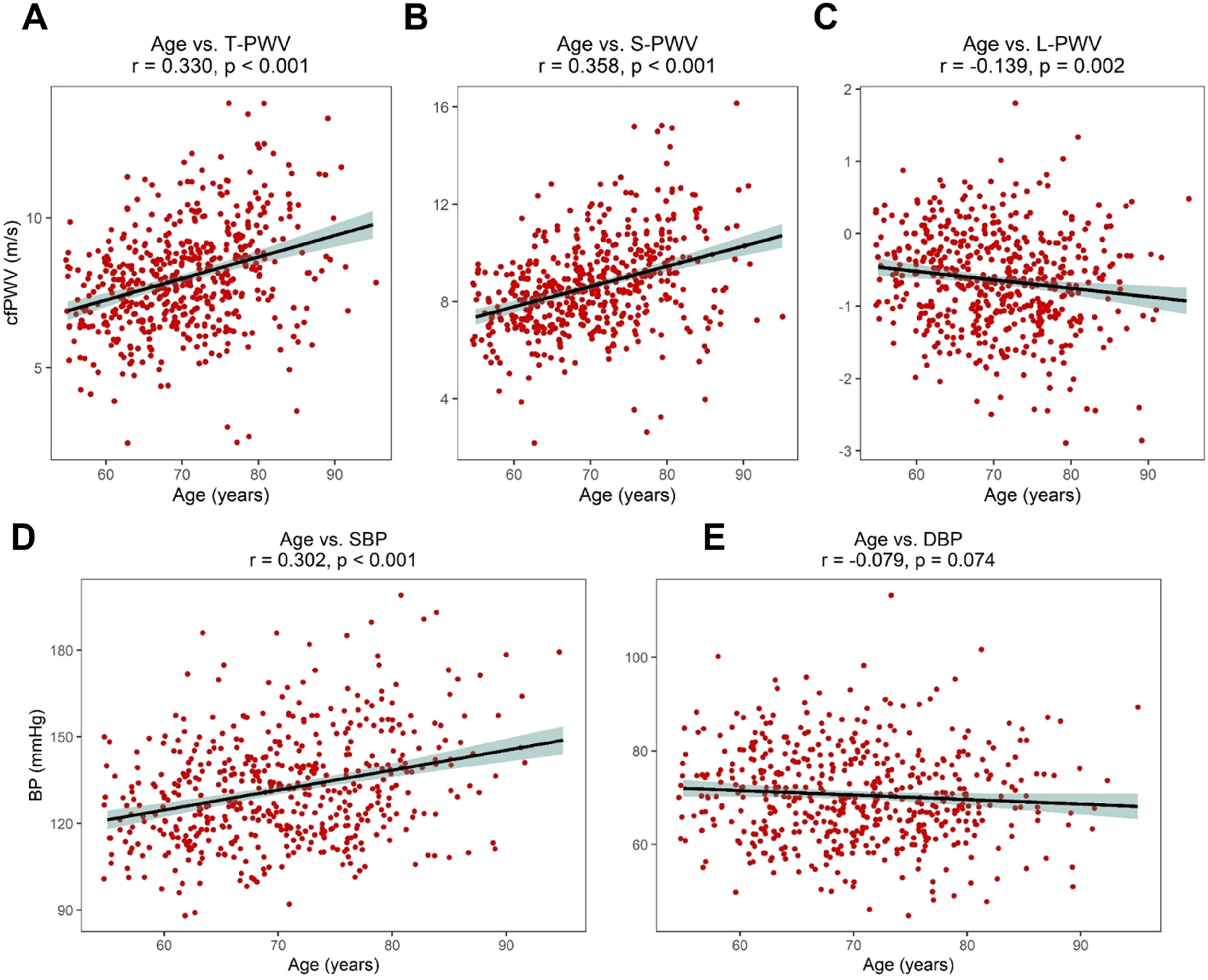
Supplemental Material
sj-docx-1-alz-10.1177_13872877261458779 - Supplemental material for Structural and load-dependent arterial stiffness are differentially associated with cognition or biomarkers of Alzheimer's disease and related dementias: The healthy brain study
Supplemental material, sj-docx-1-alz-10.1177_13872877261458779 for Structural and load-dependent arterial stiffness are differentially associated with cognition or biomarkers of Alzheimer's disease and related dementias: The healthy brain study by Theodore M. Deconne, Cynthia K. Suerken, Megan E. Lipford, Samuel N. Lockhart, James R. Bateman, Mark Espeland, Marc D. Rudolph, Melissa M. Rundle, Courtney Sutphen, Thomas C. Register, Michelle M. Mielke, Ryan Pewowaruk, Adam D. Gepner, Laura D. Baker, Suzanne Craft and Timothy M. Hughes in Journal of Alzheimer's Disease
Supplemental Material
sj-xlsx-2-alz-10.1177_13872877261458779 - Supplemental material for Structural and load-dependent arterial stiffness are differentially associated with cognition or biomarkers of Alzheimer's disease and related dementias: The healthy brain study
Supplemental material, sj-xlsx-2-alz-10.1177_13872877261458779 for Structural and load-dependent arterial stiffness are differentially associated with cognition or biomarkers of Alzheimer's disease and related dementias: The healthy brain study by Theodore M. Deconne, Cynthia K. Suerken, Megan E. Lipford, Samuel N. Lockhart, James R. Bateman, Mark Espeland, Marc D. Rudolph, Melissa M. Rundle, Courtney Sutphen, Thomas C. Register, Michelle M. Mielke, Ryan Pewowaruk, Adam D. Gepner, Laura D. Baker, Suzanne Craft and Timothy M. Hughes in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
The authors have no acknowledgments to report.
Ethical considerations
All study procedures were approved by the Wake Forest Institutional Review Board and are consistent with the ethical standards described by the 1964 Declaration of Helsinki.
Consent to participate
All participants and/or their legally authorized representative provided written informed consent to participate in the study.
Consent for publication
All participants and/or their legally authorized representative provided written informed consent for their data to be published.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research in this article was supported by the Translational Training in Aging and Alzheimer's Disease Related Disorders (T32AG033534) from the National Institute on Aging and the NIH-funded P30 ADRC (P30AG072947).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.