
Abstract
Background
The burden of early-onset Alzheimer's disease and other dementias (EOAD) in BRICS nations (Brazil, Russia, India, China, South Africa, Egypt, Ethiopia, Iran, Saudi Arabia, the United Arab Emirates, and Indonesia) is poorly characterized.
Objective
Our aims are to characterize national trends, identify high-burden populations, quantify sex- and risk factor-specific burdens, and inform targeted prevention and age-inclusive healthcare strategies in these key nations.
Methods
Using data from the Global Burden of Disease Study (GBD) 2023, we analyzed EOAD (ages 40–64) across BRICS countries from 1990–2023, employing decomposition, Joinpoint regression, and Bayesian Age-Period-Cohort modeling to project trends to 2035.
Results
Prevalent cases increased in all nations, led by China. Age-standardized incidence rose in China (average annual percentage change 0.461%) but declined in India and Iran. Females consistently bore a higher burden. Ambient particulate matter drove substantial disability-adjusted life years in Iran (74.43/100,000) and Saudi Arabia, while household air pollution was key in Ethiopia and India. Projections indicate divergence by 2035, with Russia's incidence rising to 56.22 and Saudi Arabia's prevalence falling to 160.10 per 100,000.
Conclusions
EOAD burden in BRICS is heterogeneous, driven by aging, sex, and modifiable risks, necessitating tailored public health strategies.
Keywords
Introduction
Alzheimer's disease (AD) and other dementia represent a defining public health crisis of the twenty-first century, with global prevalence projected to triple by 2050, primarily due to population aging.1–6 Historically, research has concentrated on high-income countries and late-onset cases; however, this narrow focus obscures two critical shifts in the trajectory of the epidemic: the increasing burden in low- and middle-income regions and the often-overlooked impact of early-onset (ages 40–64) forms of the disease.7–9
The BRICS grouping, comprising eleven diverse economies (Brazil, Russia, India, China, South Africa, Egypt, Ethiopia, Iran, Saudi Arabia, the United Arab Emirates (UAE), and Indonesia), epitomizes the first shift and serves as a natural laboratory for studying dementia drivers across developmental stages. These nations are experiencing rapid demographic aging, often at a faster pace and with a lower level of socioeconomic readiness than has historically been observed in the West. This discordant transition indicates that the future burden of dementia will not merely replicate past patterns but will evolve in distinct ways, influenced by local risk factors and varying healthcare capacities. Understanding these national trajectories and their underlying drivers is therefore essential for effective global health planning.
Concurrently, the challenge of early-onset Alzheimer's disease (EOAD) and other dementias, which occur in individuals aged 40 to 64, demands specific attention.10–14 Although less common than late-onset dementia, its societal and economic impact is profound and disproportionate.15,16 Affecting individuals during their peak productive and family-building years, it results in significant losses in workforce productivity, imposes catastrophic long-term care costs on households, and creates unique burdens for caregivers. Despite this, population-level analyses of its burden, particularly those elucidating sex-specific patterns and risk factor drivers, in rapidly changing contexts, such as the BRICS nations, remain scarce.
Current global estimates often obscure significant sub-regional variations, resulting in a notable knowledge gap. There is an urgent need for a comparative, longitudinal study that not only quantifies and projects the burden but also disentangles the relative contributions of population growth, aging, and epidemiological changes. Such an analysis is critical to move beyond a one-size-fits-all approach and to inform nationally tailored, precision public health policies.
To address this gap, this study utilizes data from the Global Burden of Disease Study (GBD) 2023 to analyze the incidence, prevalence, deaths, and disability-adjusted life years (DALYs) associated with EOAD and other dementias across the BRICS countries from 1990 to 2023. Furthermore, we project the future burden up to 2035. Our aims are to delineate diverging national trajectories, identify high-burden populations, uncover the sex-specific and risk-factor-attributable burdens, and provide a robust evidence base to guide targeted prevention strategies and the development of age-inclusive healthcare systems in these pivotal nations.
Methods
Data source and framework
This comparative study utilized datasets generated by the GBD 2023, which are publicly accessible through the GBD Results Tool (https://vizhub.healthdata.org/gbd-results/). Recognized as the most extensive initiative to measure population health loss, GBD 2023 provides consistent and standardized metrics, including incidence, prevalence, mortality, and DALYs, for 375 diseases and injuries across 204 countries and territories. For this study, we extracted data specific to AD and other dementias from the 11 BRICS countries. In line with the research focus on early-onset disease, the analysis was limited to the 40–64 years age group to assess the burden within this demographic.
Statistical analysis
Decomposition analysis
Decomposition analysis was employed to identify the underlying factors contributing to the temporal changes in incidence, prevalence, deaths, and DALYs from 1990 to 2023. This method quantifies the extent to which the total change in each metric can be attributed to population growth, shifts in age structure (population aging), and changes in age-specific rates (epidemiological change). This approach is crucial for determining whether trends in the burden of EOAD and other dementias are driven by demographic forces or by underlying changes in disease risk and outcomes, thereby providing essential insights for public health planning.
Joinpoint regression analysis
To analyze temporal patterns in the burden of early-onset dementias across the BRICS countries, we utilized Joinpoint Regression software (Version 5.1.0.0 from the National Cancer Institute). This analytical technique employs segmented log-linear models to analyze longitudinal data, effectively identifying years in which significant changes occur in the trajectory of age-standardized rates. The model selection process optimizes parsimony and minimizes residual variance. For each resulting segment, we calculated the annual percentage change (APC) along with its 95% confidence interval (CI) for age-standardized incidence, prevalence, deaths, and DALY rates. The average annual percentage change (AAPC), which serves as a time-weighted summary of APC trends over the entire period (1990–2023), was computed to characterize the magnitude of long-term trends. Furthermore, to provide a single overall estimate of the trend for each metric and country, we applied generalized linear models with Poisson distribution assumptions, and the results are expressed as the estimated annual percentage change (EAPC). The uncertainty associated with all trend estimates is characterized by the 95% uncertainty intervals (UIs) included in the GBD 2023 data.
BAPC analysis
Our projections for the burden of EOAD and other dementias across the BRICS countries from 2024 to 2035 utilized a Bayesian Age-Period-Cohort (BAPC) model implemented in R, with the GBD 2023 data serving as the baseline. The model treated incidence, prevalence, deaths, and DALYs as Poisson-distributed outcomes. We specified second-order random walk (RW2) priors for age, period, and cohort effects to ensure appropriate smoothing, and employed recommended weakly informative priors for precision parameters and the intercept. Inference was conducted using Integrated Nested Laplace Approximation (INLA). This robust modeling framework provides a computationally efficient and accurate approach for generating validated and reliable forecasts of all four core burden metrics, facilitating a comprehensive comparative assessment of the future disease trajectory across the eleven countries.
All statistical analyses and data visualizations were performed using R (version 4.4.2) and JD_GBDR (V2.76, Jingding Medical Technology Co., Ltd). Descriptive statistics were generated for all key variables, with results presented as means and 95% UIs or 95% CIs.
Results
The burden of early-onset Alzheimer's disease and other dementias in the 40–64-year population of BRICS countries
Table 1 presents the prevalence cases and age-standardized rates (ASR) of EOAD and other dementias among individuals aged 40–64 years in BRICS countries for the years 1990 and 2023. Between 1990 and 2023, the number of prevalent cases increased in all studied countries. China recorded the largest absolute increase, from 1,000,163.19 cases (95% UI: 753,124.59–1,278,723.43) in 1990 to 2,547,037.02 cases (95% UI: 1,936,955.43–3,229,958.70) in 2023. India also demonstrated a substantial increase, rising from 349,732.21 cases (95% UI: 257,181.22–459,918.54) to 840,447.75 cases (95% UI: 617,610.65–1,100,373.00). Brazil more than doubled its case count, increasing from 117,077.70 to 317,250.13 cases. In contrast, the age-standardized rates (ASR per 100,000 population) remained relatively stable across the study period in most countries. For example, Brazil's ASR changed from 473.49 to 467.38, while China's ASR increased from 416.69 to 441.88. Russia's ASR was 302.22 in 1990 and 304.44 in 2023, whereas India's ASR was 246.56 and 245.09, respectively. Similar patterns of stable ASRs alongside increasing case numbers were observed in South Africa, Egypt, Ethiopia, Indonesia, Iran, Saudi Arabia, and the UAE.
The prevalence cases and age-standardized prevalence rates of early-onset Alzheimer's disease and other dementias in the 40–64-year age group across BRICS countries in 1990 and 2023.
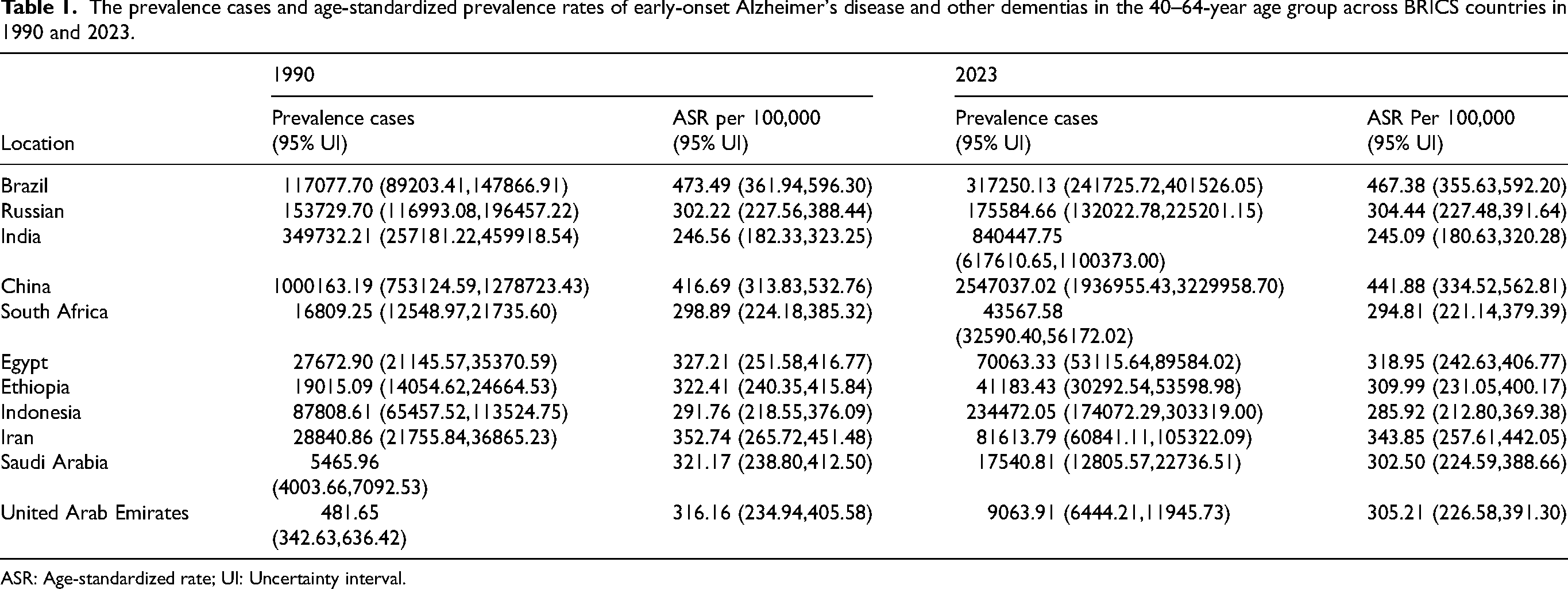
ASR: Age-standardized rate; UI: Uncertainty interval.
The analysis of geographical variation in the burden of EOAD and other dementias in 2023 revealed distinct patterns across incidence, mortality, and disability metrics (Figure 1). For age-standardized incidence rates (ASIR), the highest burdens were observed in the Federative Republic of Brazil (84.13; 95% UI: 57.20–116.87), the People's Republic of China (79.65; 95% UI: 53.52–111.96), and the Islamic Republic of Iran (60.34; 95% UI: 39.75–86.39) (Figure 1A). The profile for age-standardized death rates (ASDR) differed, with the highest rates found in Brazil (5.10; 95% UI: 1.06–14.76), Iran (4.23; 95% UI: 0.86–12.64), and Saudi Arabia (4.02; 95% UI: 0.81–12.22) (Figure 1B). Finally, the distribution of DALY rate, which encapsulates the overall disease burden, indicated that Brazil (245.79; 95% UI: 111.28–554.25), China (199.43; 95% UI: 95.65–410.77), and Iran (196.03; 95% UI: 83.00–461.60) experienced the greatest loss of healthy life years (Figure 1C).
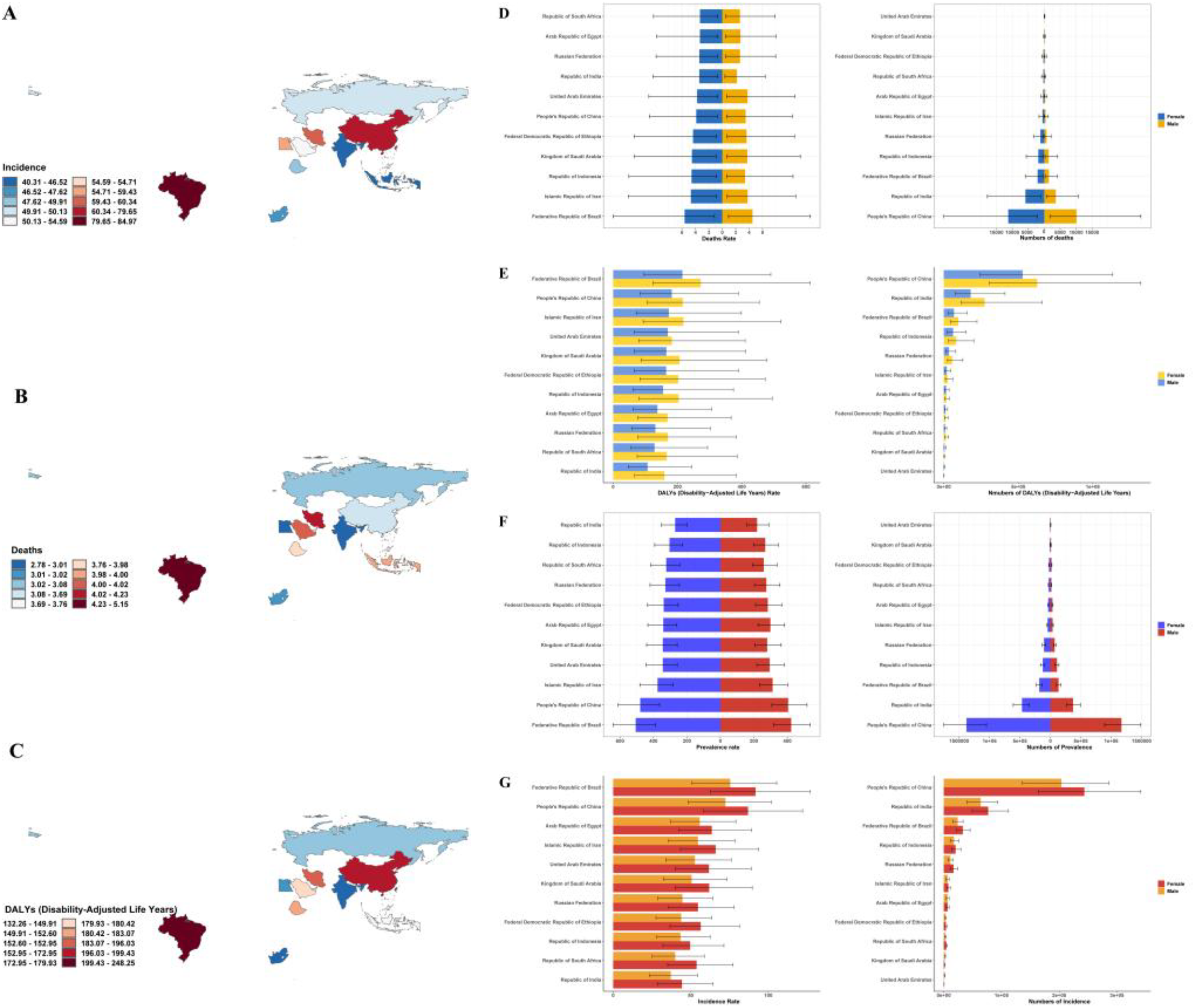
Geographic and sex-specific patterns in the burden of early-onset Alzheimer's disease and other dementias among adults aged 40–64-years across BRICS countries, 2023. (A) Age-standardized incidence rate (ASIR) per 100,000 population. (B) Age-standardized death rate (ASDR) per 100,000 population. (C) Age-standardized disability-adjusted life years (DALYs) rate per 100,000 population. (D) Sex disparities in mortality rate and number. (E) Sex disparities in DALYs rate and number. (F) Sex disparities in prevalence rate and number. (G) Sex disparities in incidence rate and number.
In 2023, significant sex disparities in mortality from AD and other dementias were documented across BRICS countries, as evidenced by both age-standardized rates and absolute death counts. Females generally experienced a higher mortality burden. In China, the age-standardized mortality rate was 3.88 per 100,000 for females, compared to 3.49 for males. Similarly, in Brazil, the rate among females reached 5.62 per 100,000, while the male rate was 4.51 per 100,000. India exhibited the largest relative sex disparity, with a female rate of 3.43 per 100,000—58.5% higher than the male rate of 2.16. An exception was the UAE, where the rates were nearly identical (females: 3.75; males: 3.76 per 100,000). A comparable pattern was observed in absolute death counts. In China, female deaths numbered 11,285.15, exceeding the 10,106.40 deaths among males. India recorded 5898.63 female deaths, substantially higher than the 3617.57 male deaths. Higher female fatalities were also noted in Brazil, Russia, Indonesia, and Iran. In contrast, Saudi Arabia (males: 124.50; females: 85.94) and the UAE (males: 66.17; females: 18.95) reported more male deaths. Egypt and Ethiopia showed minimal differences, although female counts remained slightly higher. South Africa also reported elevated female deaths (272.66) relative to males (170.91) (Figure 1D). Regarding age-standardized DALY rates, females consistently exhibited higher values across all countries. The gap was widest in Brazil, where female rates reached 272.49 per 100,000 compared to 215.36 for males, and in India, where the female rate of 159.35 per 100,000 exceeded the male rate of 107.12 by 48.7%. The UAE displayed the smallest gap, with female rates at 182.52 and male rates at 170.08. The highest female DALY rates were recorded in Brazil (272.49), Iran (218.76), and China (216.43). A similar trend was observed for absolute DALYs: female counts surpassed male counts in China (females: 627,764.95; males: 529,082.85), India (females: 274,394.72; males: 180,552.15), Indonesia, Russia, Brazil, Egypt, Iran, Ethiopia, and South Africa. Conversely, Saudi Arabia (males: 5832.18; females: 4051.54) and the UAE (males: 3401.40; females: 1026.46) reported higher DALYs for males (Figure 1E). In 2023, age-standardized prevalence rates of EOAD and other dementias were consistently higher among females in all BRICS nations. In China, the female rate was 478.84 per 100,000, which is 18.2% above the male rate of 405.00. Brazil exhibited a female rate of 506.05 per 100,000, 19.5% higher than the male rate of 423.45. India displayed the largest relative disparity, with a female prevalence of 270.28 per 100,000—23.1% greater than the male rate of 219.53. Saudi Arabia also demonstrated a significant difference (females: 344.21; males: 279.39, a 23.2% gap). This pattern was reflected in absolute prevalent cases: female cases exceeded male cases in China (females: 1,378,610; males: 1,168,427), India (females: 466,956; males: 373,492), Brazil (females: 182,493; males: 134,757), Russia, Indonesia, Iran, Ethiopia, and South Africa. In contrast, Saudi Arabia (males: 10,532; females: 7009) and the UAE (males: 6892; females: 2172) reported higher male case numbers, while Egypt exhibited minimal sex differences (females: 35,409; males: 34,654) (Figure 1F). Analysis of the 2023 incidence data for EOAD and other dementias revealed consistently higher age-standardized incidence rates among females across BRICS countries. In China, the female incidence rate was 86.94 per 100,000, substantially exceeding the male rate of 72.38. Brazil reported a female rate of 91.80 per 100,000 compared to 75.44 for males. Ethiopia exhibited the most pronounced relative disparity: the female incidence of 56.46 per 100,000 was 28.9% higher than the male rate of 43.81. This trend was also evident in Indonesia, Russia, and Saudi Arabia. In terms of absolute incident cases, females outnumbered males in China (females: 243,630; males: 203,778), India (females: 77,023; males: 63,865), Brazil (females: 32,960; males: 23,995), Russia (females: 17,083; males: 11,457), as well as in Indonesia, Iran, Ethiopia, and South Africa. In contrast, Saudi Arabia (males: 2013; females: 1306) and the UAE (males: 1349; females: 432) reported more male incident cases, while Egypt exhibited minimal sex differences (Figure 1G).
Based on the GBD data from 1990 to 2023, age-standardized rates for incidence, prevalence, DALYs, and mortality from AD and other dementias exhibited diverse temporal trends across the eleven studied countries, yet consistently demonstrated higher rates among females. In terms of incidence, China experienced a 13.4% increase to 79.65 (95% UI 53.52–111.96) per 100,000 in 2023, while Brazil peaked in 2015 before declining to 84.13 (95% UI 57.20–116.87); most other countries showed relative stability (Figure 2A). A similar pattern was observed for prevalence, with China gradually increasing to 441.88 (95% UI 334.52–562.81) and Brazil exhibiting a non-linear trend, whereas other nations remained stable or experienced minor declines (Figure 2B). The rates of DALYs varied substantially, with China showing a decline for females to 216.43 (95% UI 106.10–454.66), India reflecting a slight increase for females to 159.35 (95% UI 67.12–383.63), and the UAE demonstrating the most pronounced decline for males to 170.08 (95% UI 66.26–389.04) (Figure 2C). Mortality trends also differed, featuring a notable decline in the UAE for males to 3.76 (95% UI 0.70–10.82), a gradual decrease in China, while Indonesia exhibited an upward trend and Brazil maintained persistently high rates (Figure 2D). A universal and consistent finding across all metrics, countries, and the entire study period was the significantly higher burden borne by females compared to males.
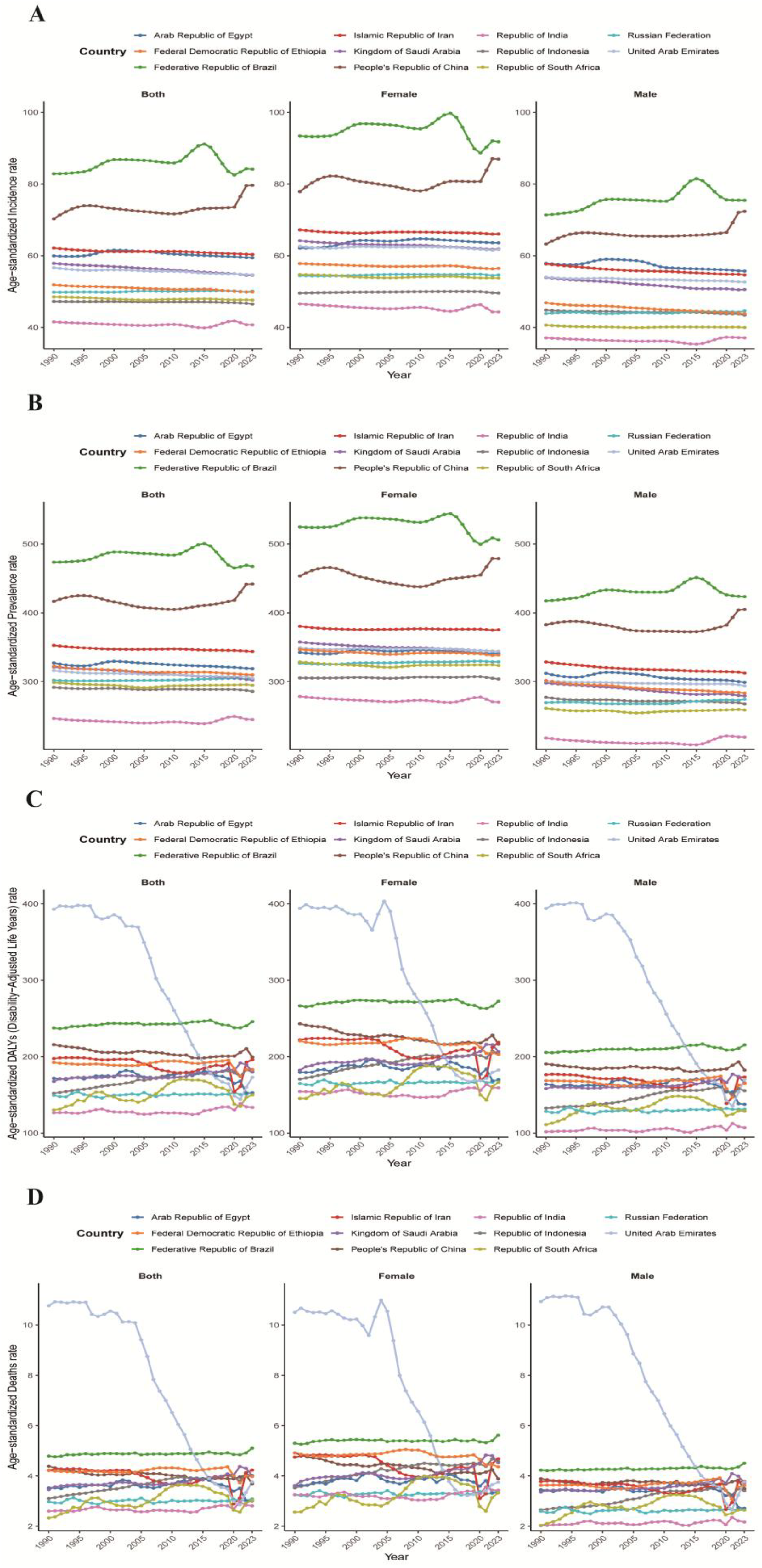
Temporal trends and sex differences in the burden of early-onset Alzheimer's disease and other dementias across BRICS countries, 1990–2023. (A) Incidence rate. (B) Prevalence rate. (C) Disability-Adjusted Life Years (DALYs) rate. (D) Mortality rate.
Based on the GBD 2023 data, the burden of AD and other dementias in adults aged 40–64 years exhibited a consistent and marked exponential increase with advancing age across all eleven countries. This trend was observed across all metrics, with mortality rates in the 60–64 age group being approximately 300 to 600 times higher than those in the 40–44 age group (Figure 3A). China, India, and Brazil consistently carried the highest absolute burdens. For instance, China recorded the highest death counts (men: 5670.41, 95% UI 1083.16–16,496.48; women: 6492.16, 95% UI 1324.06–17,624.41) (Figure 3B), prevalent cases (men: 485,389.99, 95% UI 382,101.52–607,499.28; women: 584,872.84, 95% UI 457,007.12–725,926.01) (Figure 3F), and incident cases (women: 105,148.79, 95% UI 73,814.47–146,117.15; men: 83,820.62, 95% UI 59,456.72–116,736.23) (Figure 3H) in the 60–64 year age group. A consistent female preponderance was observed across mortality, DALYs (both rates and counts), prevalence, and incidence in the vast majority of country and age group combinations. For example, females exhibited higher DALYs rates in all countries, with the disparity widening with age, as seen in China (female: 747.75, 95% UI 373.31–1577.89; male: 623.63, 95% UI 286.28–1348.25) (Figure 3C) and in absolute DALYs, where the female burden was 21.0% higher in China and 56.2% higher in India (Figure 3D). Similarly, prevalence rates were consistently higher in females, such as in China's 60–64 age group (female: 1430.04, 95% UI 1117.40–1774.92; male: 1197.63, 95% UI 942.78–1498.92) (Figure 3E), and incidence rates were highest in females in Brazil (265.19, 95% UI 189.46–364.17) compared to males (214.20, 95% UI 149.85–295.81) (Figure 3G). Notable exceptions to this pattern were observed in Saudi Arabia and the UAE, where males had higher death counts (Figure 3B) and incidence numbers (Figure 3H) across several age groups.
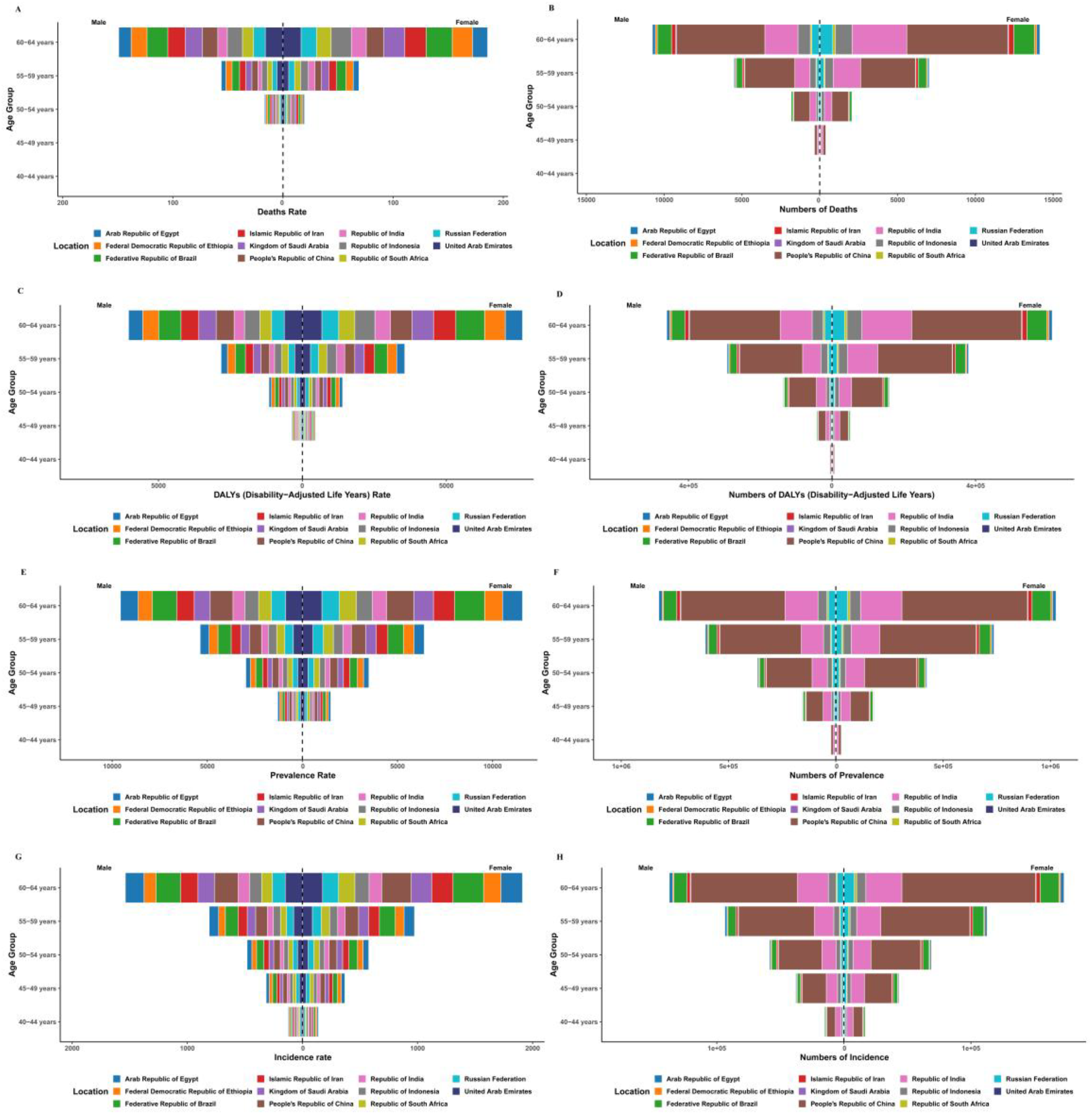
The burden of Alzheimer's disease and other dementias in adults aged 40–64-years across BRICS countries, 2023. (A) Deaths Rate. (B) Deaths number. (C) DALYs rate. (D) DALYs number. (E) Prevalence rate. (F) Prevalence number. (G) Incidence rate. (H) Incidence number.
Attributable burden of key risk factors by country
Based on the GBD 2023 data, this analysis focuses on EOAD and other dementias in BRICS countries, revealing distinct geographical patterns in risk factor-attributable burden. For mortality rates (per 100,000 population), ambient particulate matter pollution exhibited the highest attributable rates in Iran (1.60), Saudi Arabia (1.59), and the UAE (1.45). In contrast, household air pollution from solid fuels demonstrated a substantial burden in Ethiopia (1.46) and India (0.50), while its impact was minimal in Russia, Egypt, and Saudi Arabia (<0.01). Metabolic risk factors also showed significant contributions: high fasting plasma glucose accounted for elevated mortality in Brazil (1.03), Saudi Arabia (1.08), and the UAE (1.02), whereas high body mass index had notable impacts in Russia (0.44), Egypt (0.61), and Saudi Arabia (0.74) (Figure 4A). Furthermore, the analysis of DALY rates (per 100,000 population) indicated that ambient particulate matter pollution contributed significantly in Iran (74.43, 95% UI 12.58–215.91), China (64.90, 95% UI 12.08–164.35), and Saudi Arabia (71.56, 95% UI 12.10–212.74). Household air pollution from solid fuels revealed markedly higher burdens in Ethiopia (67.37, 95% UI 11.79–199.76) and India (23.60, 95% UI 4.11–70.53) compared to Russia (0.38, 95% UI 0–1.83) and the UAE (0.01, 95% UI 0–0.11). Metabolic risk factors had a considerable impact, with Brazil showing high DALY rates attributable to high fasting plasma glucose (48.98, 95% UI 19.26–113.31) and Saudi Arabia exhibiting high DALY rates due to high body mass index (33.38, 95% UI −14.84–113.53) (Figure 4B).
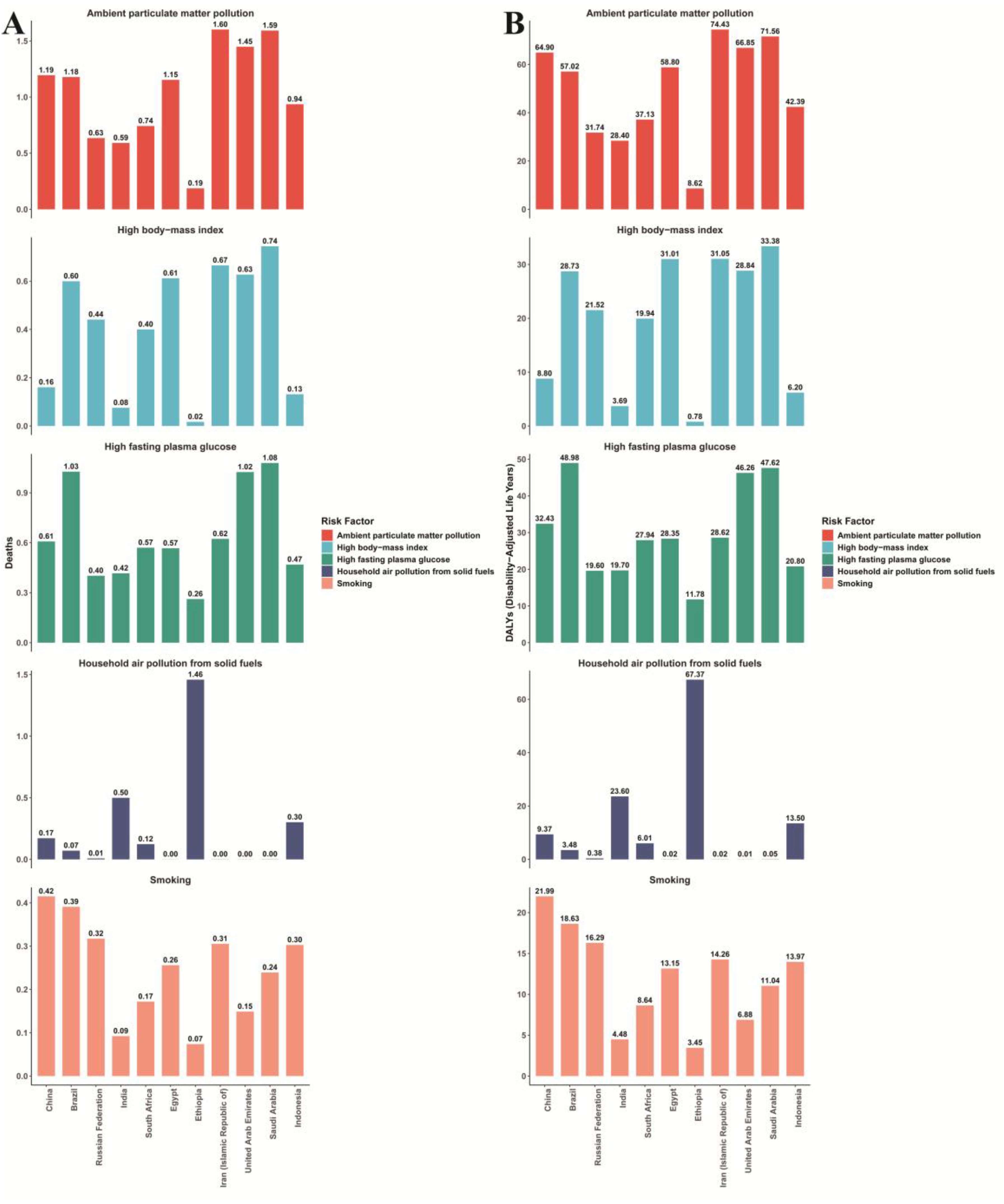
Geographic variation in risk factor attributable burden of early-onset Alzheimer's disease and other dementias in BRICS countries, 2023. (A) Mortality rates attributable to key risk factors. (B) DALY rates attributable to key risk factors.
Analysis of the average annual percent change in incidence across BRICS nations
Based on the GBD data from 1990 to 2023, the temporal trends in age-standardized incidence rates of EOAD and other dementias across BRICS countries revealed distinct national patterns. China demonstrated a significant overall increase (AAPC 0.461%, 95% CI 0.389–0.534) with accelerating growth in recent years (Phase 4 APC 2.811%, 95% CI 2.398–3.225) (Figure 5A). In contrast, most other countries exhibited declining trends: India (AAPC −0.064%, 95% CI −0.099 to −0.030), South Africa (AAPC −0.058%, 95% CI −0.069 to −0.047), Egypt (AAPC −0.027%, 95% CI −0.037 to −0.017), Ethiopia (AAPC −0.120%, 95% CI −0.132 to −0.107), Iran (AAPC −0.086%, 95% CI −0.090 to −0.083), and Indonesia (AAPC −0.052%, 95% CI −0.057 to −0.047) all exhibited statistically significant decreases (Figure 5D-H, K). Brazil and Russia showed overall stability with non-significant AAPC trends of 0.015% and 0.007%, respectively, although both demonstrated significant phase-specific fluctuations (Figure 5B, C). All reported trends were statistically significant (p < 0.001) except for Brazil's overall AAPC (p = 0.873).
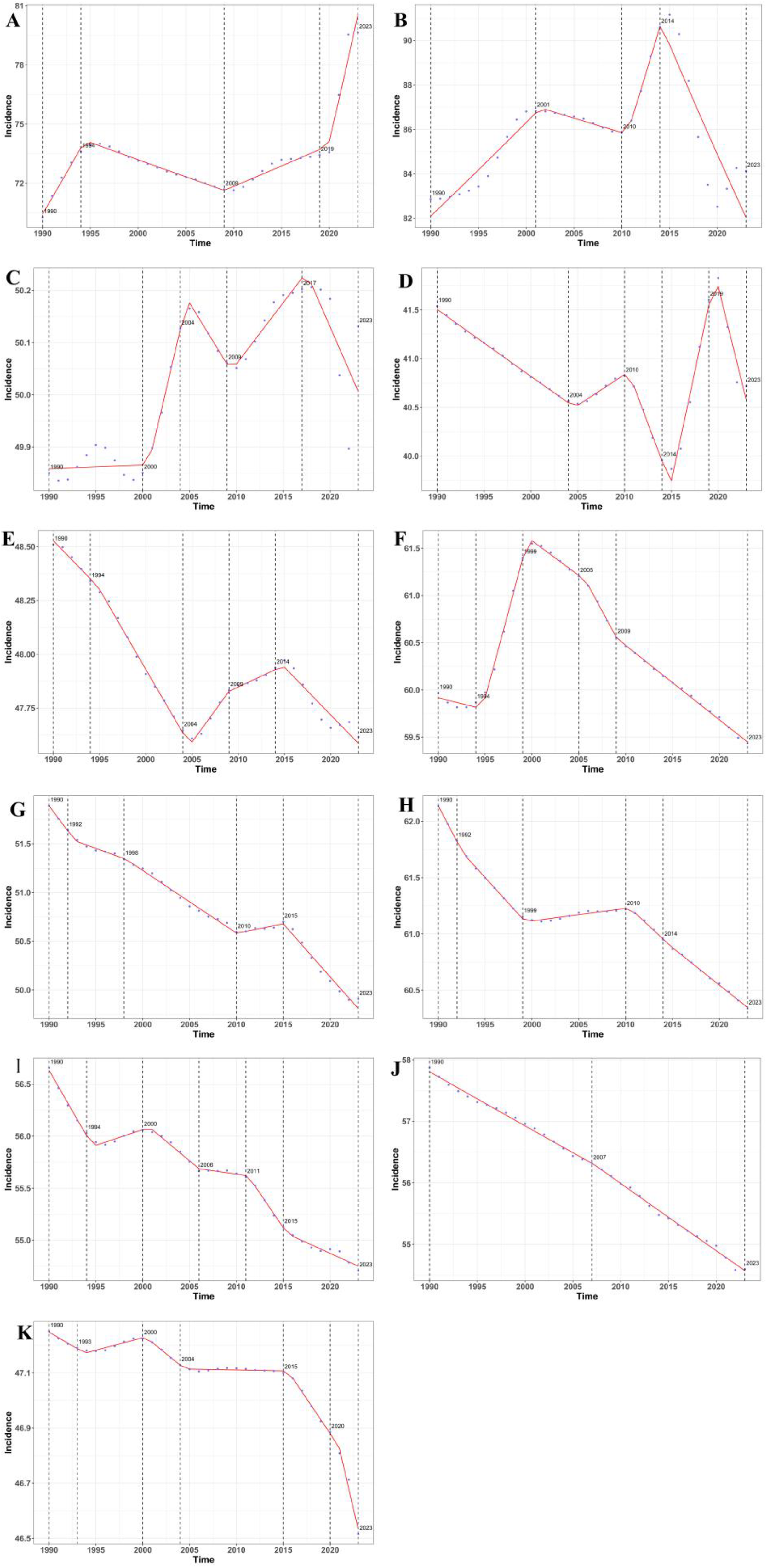
National trends in the incidence of early-onset Alzheimer's disease and other dementias across BRICS countries, 1990–2023. (A) China. (B) Brazil. (C) Russia. (D) India. (E) South Africa. (F) Egypt. (G) Ethiopia. (H) Iran. (I) Arab Emirates. (J) Saudi Arabia. (K) Indonesia.
Decomposition of changes
Based on decomposition analysis from 1990 to 2023, population growth has consistently emerged as the predominant driver behind the increased burden of EOAD and other dementias across BRICS countries (Figure 6). It accounts for 57.3%-97.9% of incidence increases, over 70% of prevalence rises, 58%-91.9% of the growth in DALYs, and more than 50% of mortality increases (Figure 6A-D).
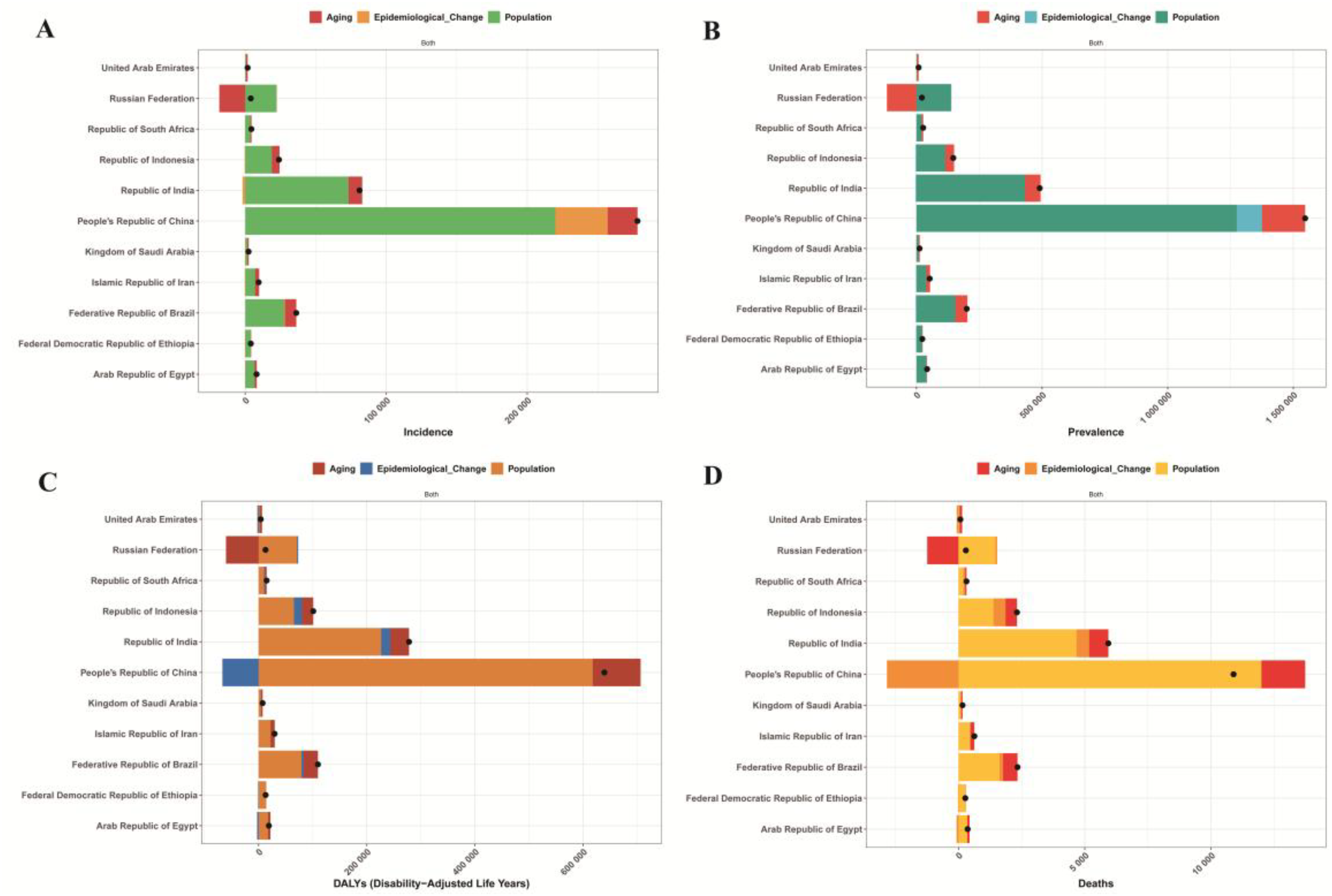
Decomposition analysis of early-onset Alzheimer's disease and other dementias burden in BRICS countries, 1990–2023: the dominant role of population growth and heterogeneous aging impacts. (A) Incidence. (B) Prevalence. (C) DALYs. (D) Mortality.
The contribution of population aging exhibited substantial geographical polarization, ranging from minimal effects in Ethiopia (7.3% for incidence) and India (11.9%) to accelerated impacts in the UAE (69.3% for incidence, 110.88% for DALYs) and Saudi Arabia (40.5% for incidence). Notably, Russia demonstrated exceptional negative contributions from aging across prevalence (−541.91%), DALYs (−473.26%), and mortality (−424.98%) metrics. Epidemiological changes exhibited bidirectional patterns, with protective effects observed in China (−10.48% for DALYs, −26.03% for mortality) and Egypt (−14.81% for DALYs, −21.07% for mortality), contrasting with unfavorable trends in Brazil (+1.6% for incidence), India (6.07% for DALYs), and Indonesia (14.8% for DALYs, 20.73% for mortality).
Incidence, prevalence, DALYs, and mortality trends with projections to 2035
Based on the Bayesian Age-Period-Cohort modeling analysis from 1990 to 2035, the burden of EOAD and other dementias across BRICS countries reveals complex and divergent epidemiological trajectories. In terms of incidence rates, China demonstrates a notable pattern of resurgence, increasing to 78.02 per 100,000 (95% CI 77.79–78.24) in 2023 after previous fluctuations; however, projections indicate a declining trend toward 71.71 (95% CI 66.81–76.61) by 2035. The Russian Federation exhibits sustained growth, rising from 50.02 (95% CI 49.50–50.54) in 1990 to 52.15 (95% CI 51.63–52.66) in 2023, with projections accelerating to 56.22 (95% CI 52.93–59.50) by 2035. Brazil displays a distinct non-linear pattern, peaking at 91.27 (95% CI 90.53–92.02) in 2015 before declining to 83.51 (95% CI 82.85–84.17) in 2023. Most other nations demonstrate stable or declining incidence trends, with Saudi Arabia showing the most pronounced projected decrease to 29.12 (95% CI 22.86–35.38) by 2035, while Indonesia represents a notable exception with projected increases following a period of historical stability (Figure 7A). The prevalence analysis reveals similarly heterogeneous patterns. Russia demonstrates sustained growth, increasing from 303.53 to 315.36 per 100,000 (95% CI 313.94–316.79) in 2023, and is projected to reach 337.69 (95% CI 323.20–352.19) by 2035. India maintains elevated rates at 249.83 (95% CI 249.30–250.36) in 2023, while South Africa shows increasing trends. In contrast, Brazil exhibits a declining pattern, decreasing from its 2015 peak of 502.30 (95% CI 500.48–504.12) to 464.68 (95% CI 463.09–466.28) in 2023. The most substantial prevalence reductions are observed in Saudi Arabia and the UAE, with Saudi Arabia projected to decline to 160.10 (95% CI 129.14–191.05) by 2035 (Figure 7B).
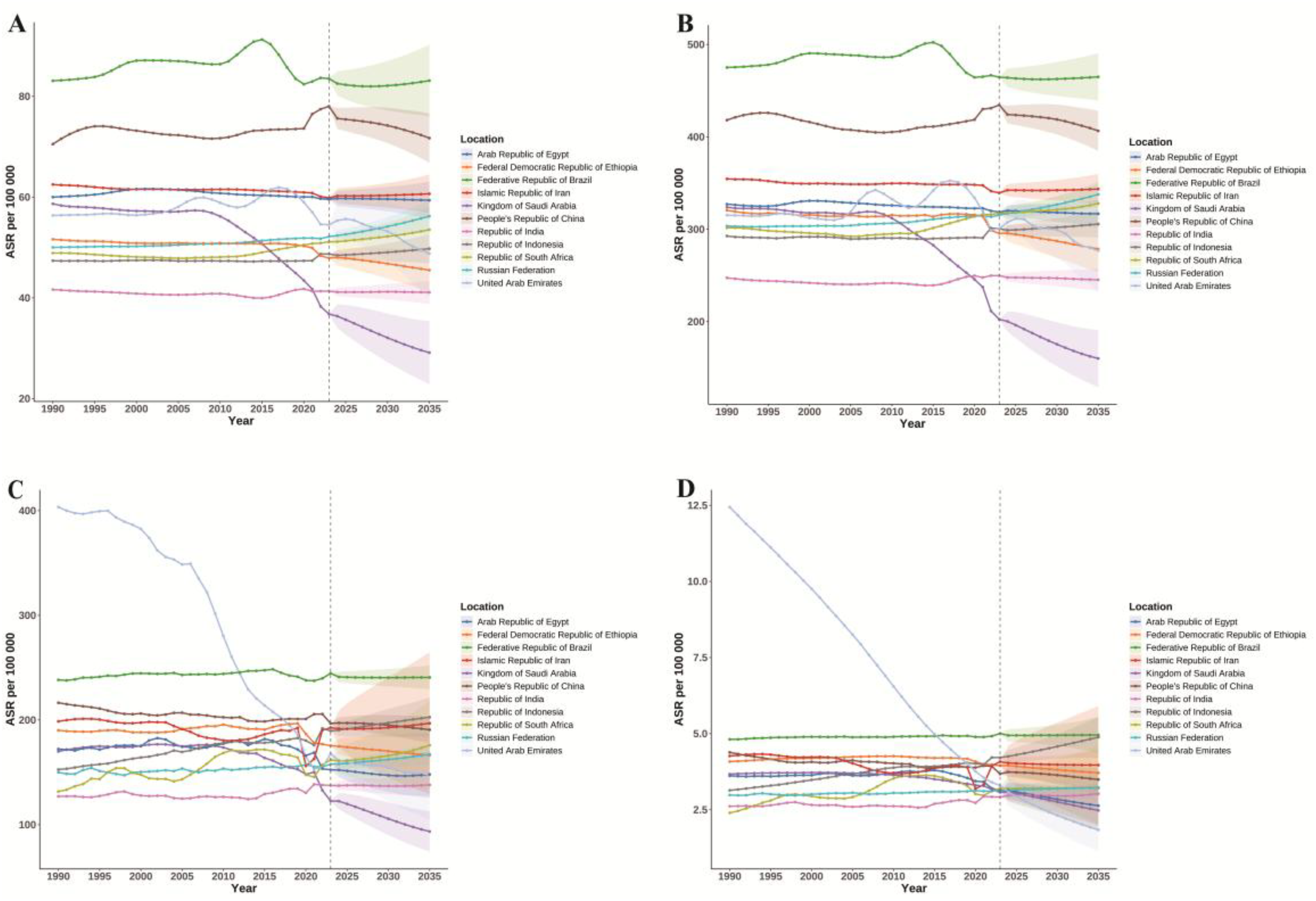
Divergent national trajectories in early-onset Alzheimer's disease and other dementias burden across BRICS countries: a Bayesian age-period-cohort analysis, 1990–2035. (A) Incidence rate. (B) Prevalence rate. (C) DALYs rate. (D) Mortality rate.
The analysis of DALYs further underscores these cross-national disparities. China has shown consistent improvement, with DALYs decreasing from 216.46 (95% CI 215.87–217.04) in 1990 to 196.69 (95% CI 196.33–197.04) in 2023. In contrast, South Africa has experienced the most significant increase, rising from 131.65 (95% CI 128.77–134.53) to 161.89 (95% CI 159.78–163.99) in 2023. Saudi Arabia has achieved a remarkable reduction in DALYs, decreasing to 122.63 (95% CI 120.26–125.00) in 2023, with projections indicating a further decline to 93.51 (95% CI 74.15–112.87) by 2035 (Figure 7C). Mortality analysis reveals striking international variations. The UAE has demonstrated extraordinary improvement, decreasing from 12.44 (95% CI 9.35–15.54) in 1990 to a projected 1.84 (95% CI 1.12–2.55) by 2035. Saudi Arabia shows substantial declines, reaching 3.07 (95% CI 2.83–3.32) in 2023. In contrast, Russia and India exhibit increasing mortality trends, while Indonesia is projected to experience the steepest increase to 4.88 (95% CI 4.20–5.56) by 2035, highlighting significant concerns for future dementia management in these populations (Figure 7D).
Discussion
This analysis delineates the complex and divergent trajectories of EOAD and other dementias across the BRICS nations from 1990 to 2023. Our findings reveal that these trajectories are not solely a function of demographic scaling; rather, they are profoundly influenced by distinct etiological pathways and societal transitions, necessitating a decisive departure from one-size-fits-all global health approaches.
The decomposition analysis provides critical insights into the fundamental drivers of the epidemic. While population growth serves as the primary engine behind the rising absolute case numbers, the widely varying contributions of population aging, ranging from negligible in Ethiopia and India to paramount in the UAE, reflect the starkly different stages of demographic transition within the bloc. This heterogeneity suggests that the window of opportunity for preventive intervention varies in its degree of openness. The anomalous negative contribution of aging in Russia is particularly instructive, potentially revealing a cohort effect shaped by historical socioeconomic upheavals and high mid-life mortality from competing causes, which may have selectively depleted the pool of individuals surviving to the ages of peak dementia risk.
The persistent and significant female preponderance across nearly all metrics and countries is one of the most consistent findings of this study. Attributing this disparity solely to female longevity or diagnostic artifacts would be an oversimplification. A more plausible explanation involves a multifactorial synergy. The biological plausibility is supported by the neuroprotective role of estrogen, the loss of which post-menopause may unmask a female-specific vulnerability to AD pathology, potentially interacting with the APOE ε4 allele in a sex-specific manner.17,18 This biological substrate is then compounded by lifelong social determinants: lower educational attainment, economic dependency, and the profound psychological stress associated with gendered caregiving roles, which may independently contribute to cognitive reserve depletion. The reversal of this pattern in Saudi Arabia and the UAE, where the male burden was higher for certain metrics, presents a crucial natural experiment. It strongly implies that region-specific cultural, behavioral, or environmental factors—such as differential patterns of vascular risk factors, occupational exposures, or healthcare utilization—can override or modulate the more commonly observed global sex disparity.19–22
The risk factor attribution analysis powerfully shifts the narrative from correlation to actionable, mechanistic causality. The significant burden of ambient particulate matter pollution in Iran, Saudi Arabia, and the UAE provides compelling, population-level evidence for the role of environmental neurotoxins.23–27 The proposed mechanism involves fine particulate matter (PM2.5) inducing systemic inflammation and oxidative stress, enabling it to traverse the blood-brain barrier and potentially promote amyloid-beta aggregation and tau hyperphosphorylation—core pathological hallmarks of AD.28–32 In parallel, the substantial burden from household air pollution in Ethiopia and India highlights a different facet of the air quality crisis, one intrinsically linked to energy poverty. The considerable impact of metabolic risks, particularly high fasting plasma glucose, firmly positions early-onset dementia within the spectrum of dysmetabolic disease. Chronic hyperglycemia drives cerebral microvascular dysfunction and induces brain insulin resistance, a state often referred to as “Type 3 Diabetes” characterized by impaired neuronal glucose utilization and heightened inflammatory signaling, creating a hostile environment for neuronal survival.33–37
Projections for 2035 illustrate a continuing divergence, serving as a report card on both current and future health system preparedness. The expected declines in Saudi Arabia and the UAE likely reflect the successful implementation of public health policies aimed at non-communicable diseases and environmental controls. China's projected stabilization, following a period of increase, may indicate the initial benefits of its national air quality and health promotion campaigns. In contrast, the rising incidence in Russia and the increasing mortality in Indonesia serve as clear warning signs of systems under strain, potentially due to deficiencies in primary care, dementia recognition, and the integrated management of cardiometabolic comorbidities.
In conclusion, the challenge of early-onset dementia within the BRICS bloc presents a mosaic of distinct epidemics, each characterized by its own demographic momentum, risk profile, and social context. Our findings compellingly advocate for precision neurology and tailored public health responses. Mitigating this looming crisis necessitates nationally prioritized strategies that target the predominant local risk drivers, whether through stringent environmental regulations, systematic management of metabolic syndrome, or the implementation of gender-sensitive cognitive health initiatives. The future burden will be shaped not only by demographic inevitabilities but also by the policy choices made today.
This study has several limitations. The findings are derived from modeled GBD 2023 estimates, and their accuracy is contingent upon the quality and completeness of the underlying source data from each country, which may be affected by under-diagnosis or inconsistent reporting. Furthermore, systematic differences in health system capacity, diagnostic infrastructure, and healthcare accessibility across BRICS nations represent an important unmeasured factor that may substantially influence the estimated burden of EOAD. In countries with limited neurological specialty services or low dementia literacy, case ascertainment is likely to be incomplete, potentially leading to a systematic underestimation in the GBD modeling outputs. Conversely, heightened diagnostic intensity in well-resourced healthcare systems may contribute to higher reported rates. While the GBD 2023 framework employs sophisticated statistical approaches to harmonize data from heterogeneous sources, residual confounding from differential health system performance cannot be fully excluded. These concerns regarding cross-national comparability warrant cautious interpretation of the observed inter-country differences in age-standardized rates. Future studies that integrate health system performance metrics, such as the Healthcare Access and Quality Index, may help disentangle true epidemiological differences from ascertainment artifacts. Second, while our projections are robust, they are based on historical trends and cannot account for future medical breakthroughs or public health policies that may alter the disease trajectory. Additionally, the BAPC projections to 2035 are predicated on the assumption of temporal stability in age, period, and cohort effects. We did not conduct formal sensitivity analyses, such as alternative prior specifications, leave-one-out cross-validation, or ensemble forecasting approaches, to evaluate the sensitivity of the projections to model specifications. The choice of second-order random walk priors, although standard for ensuring smoothness in age-period-cohort modeling, may yield quantitatively different forecasts under alternative prior formulations. Consequently, the projected estimates should be regarded as plausible trajectories conditioned on historical trends rather than definitive forecasts. Future studies should incorporate sensitivity frameworks to formally assess the robustness of the projections.
Conclusion
The burden of EOAD and other dementias across BRICS nations is increasing in absolute terms, primarily driven by population growth. However, this overarching trend masks sharply divergent national trajectories in age-standardized rates, which are influenced by varying aging rates, significant gender disparities rooted in both biology and society, and distinct risk factor profiles. This epidemiological heterogeneity highlights the critical necessity for precise public health strategies. Future efforts must prioritize nationally tailored interventions that address key local determinants, whether targeting air pollution, managing metabolic disorders, or implementing gender-sensitive approaches, to effectively mitigate the impending personal, societal, and economic impacts of early-onset dementia.
Footnotes
Acknowledgements
Our sincere thanks go to the researchers and institutions behind the Global Burden of Disease project. Their collaborative efforts have created an invaluable resource, and the data they have made publicly available provide a foundational understanding of global health conditions and trends.
Ethical considerations
Not applicable
Consent to participate
Not applicable
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.