
Abstract
Background
Glymphatic dysfunction is implicated in neurodegenerative disorders and may contribute to the elevated risk of mild cognitive impairment (MCI) in type 2 diabetes mellitus (T2DM) patients. The diffusion tensor imaging along the perivascular space (DTI-ALPS) index has been proposed as a non-invasive imaging surrogate that may reflect aspects of glymphatic system activity.
Objective
We investigated the relationship between ALPS index, cognition, brain structure, and plasma Alzheimer's disease biomarkers in T2DM patients.
Methods
Two independent cohorts were analyzed: Cohort 1 included 60 age, sex, and education matched participants (20 T2DM with MCI, 20 T2DM with normal cognition, and 20 healthy controls); Cohort 2 comprised 35 elderly T2DM patients assessed for plasma AD biomarkers. All participants underwent MRI for ALPS index calculation and structural imaging. Cognition was evaluated using the Mini-Mental State Examination and Montreal Cognitive Assessment.
Results
The ALPS index was significantly lower in T2DM patients with MCI compared to cognitively normal T2DM patients and healthy controls, and showed discriminative ability for MCI. Lower ALPS index correlated with poorer cognitive scores and was associated with brain atrophy. Mediation analysis indicated that the volume of the right opercular inferior frontal gyrus mediated the relationship between ALPS index and cognition scores. Furthermore, the ALPS index negatively correlated with plasma pTau217 adjusted by age and sex in T2DM patients.
Conclusions
A lower ALPS index is associated with cognitive impairment, brain atrophy, and plasma tauopathy, which may serve as a promising non-invasive imaging biomarker for early identification of neurodegeneration risk in T2DM patients.
Keywords
Introduction
Type 2 diabetes mellitus (T2DM) affects approximately 530 million adults worldwide, positioning it as a major chronic disease threatening global health. 1 Individuals with T2DM face a 2- to 3-fold increased risk of developing mild cognitive impairment (MCI) and Alzheimer's disease (AD).2,3 However, the mechanisms linking T2DM to cognitive impairment and its progression to AD remain incompletely elucidated. Growing evidences suggest that dysfunction of the glymphatic system may contribute to cognitive decline in T2DM.4–7 The glymphatic system plays a critical role in clearing neurotoxic waste products such as amyloid-β (Aβ) and tau, which are central to AD pathogenesis. 8 This clearance process involves cerebrospinal fluid (CSF) influx along periarterial spaces into the brain parenchyma, where it mixes with interstitial fluid to facilitate the removal of metabolic wastes toward meningeal lymphatic vessels and cervical lymph nodes. Key to this process are aquaporin-4 (AQP4) water channels located on astrocytic end-feet, which support convective fluid transport.9,10 In T2DM rats, AQP4 expression is notably reduced, leading to impaired glymphatic function. 11 T2DM rat had suppressed clearance of interstitial fluid in the hippocampus and hypothalamus, suggesting that an impairment of the glymphatic system contributes to cognitive deficits. 12 These findings highlight glymphatic impairment as a potential mediator of cognitive decline in T2DM-related dementia, underscoring the need to evaluate glymphatic function in T2DM patients to clarify its role in AD risk and identify possible therapeutic targets.
Diffusion tensor imaging along the perivascular space (DTI-ALPS) has emerged as a promising method for non-invasively deriving the ALPS index, which remains an indirect surrogate rather than a direct measure of glymphatic clearance.10,13 This technique quantifies water diffusion anisotropy relative to the orientation of perivascular spaces surrounding deep medullary veins. 13 Studies have reported reduced ALPS index in prediabetic and T2DM patients, correlating with insulin resistance.5,7 Moreover, the ALPS index has been linked to AD biomarkers, including CSF Aβ42 levels, tau/Aβ PET deposition, and cognitive performance in AD patients.10,14 These observations support the utility of ALPS index in evaluating glymphatic impairment in T2DM and its association with cognitive decline in AD. Within the ATN framework, plasma biomarkers such as Aβ40, Aβ42, pTau181, pTau217, and neurofilament light (NfL) have gained recognition for diagnosing and tracking AD progression. 15 Consequently, peripheral levels of these biomarkers may be influenced by glymphatic efficiency. 16 While plasma pTau species, NfL and Aβ are well-established AD markers, their relationship with glymphatic function in T2DM patients remains unexplored.
This dual-cohort study aims to investigate the relationship between glymphatic system metrics derived from DTI-ALPS, cognitive impairment, brain atrophy, and plasma neurodegenerative biomarkers in T2DM patients. Specifically, we seek to determine: (1) whether glymphatic dysfunction, reflected by reduced ALPS index, correlates with cognitive deficits and structural brain changes; and (2) whether the ALPS index associates with plasma levels of Aβ, pTau, and NfL. By integrating neuroimaging and plasma biomarkers, this research aims to elucidate the association of glymphatic system metrics derived from DTI-ALPS in T2DM-related cognitive impairment, offering new insights into the potential mechanisms linking T2DM to AD.
Methods
Participants
This retrospective study utilized data from an established elderly cohort recruited across multiple medical centers between 2013 and 2019 in Wuhan, China.17–20 To account for variations in MRI acquisition protocols and research questions, participants were divided into two cohorts (Figure 1). Cohort 1 included 104 individuals who underwent brain MRI between 2013 and 2016. After applying inclusion and exclusion criteria, 60 participants were selected and stratified into three age-, sex-, and education-matched groups: 20 T2DM patients with mild cognitive impairment (T2-MCI), 20 T2DM patients with normal cognition (T2-NC), and 20 healthy controls with normal cognition (HC-NC). Cohort 2 enrolled 35 T2DM patients between 2018 and 2019. A detailed participant selection flowchart and inclusion/exclusion criteria are provided in Supplemental Figure 1. The study was approved by the Ethics Committee of Tongji Medical School (No. [2013] S071) and registered at ClinicalTrials.gov (NCT01830998). All procedures adhered to the Declaration of Helsinki, and written informed consent was obtained from each participant.

Study design and ALPS index calculation.
Inclusion and exclusion criteria
Healthy controls were required to have no T2DM or any other previously diagnosed medical conditions. T2DM diagnosis followed the 2006 World Health Organization criteria. Inclusion criteria were: (1) age ≥ 50 years; (2) long-term residence (≥ 5 years) in the local area; and (3) ≥ 6 years of education with the ability to complete neuropsychological assessments. Exclusion criteria included: (1) significant auditory or visual impairment; (2) history of head trauma, stroke, brain tumor, epilepsy, or other central nervous system disorders that could cause dementia or pre-existing dementia before T2DM onset; (3) use of medications known to affect cognitive function; (4) alcohol use disorder; (5) diagnosed psychiatric conditions such as depression, acute stress disorder, or post-traumatic stress disorder; (6) severe sleep disorders; (7) significant cerebrovascular damage, including cerebral infarction, cervical or cerebral vessel stenosis, or white matter hyperintensities with Fazekas grade ≥ 2; and (8) poor-quality MRI scans due to motion artifacts. Healthy controls were required to be ≥ 50 years old, have ≥6 years of education, exhibit normal cognitive function, and have no major underlying diseases.
Criteria for mild cognitive impairment and normal cognition
All participants underwent detailed medical history review and physical examination. Cognitive status was evaluated using the Mini-Mental State Examination (MMSE), Montreal Cognitive Assessment (MoCA), and Activity of Daily Living (ADL) scale, administered by trained neurologists. MCI was defined according to Petersen's criteria: (1) subjective memory complaint; (2) preserved activities of daily living; (3) generally intact cognitive function; (4) objective memory impairment relative to age-matched norms; (5) MMSE score between 24 and 27. Normal cognition was defined as that people were required to have no subjective cognitive complaints, preserved activities of daily living, MMSE (≥28) scores within age- and education-adjusted normal ranges.
Image acquisition and processing
All participants underwent MRI on 3.0 T scanners equipped with a 32-channel head coil. Cohort 1 was scanned on a Discovery MR750 system (GE Healthcare, USA), and Cohort 2 on a Skyra system (Siemens Healthineers, Germany). Both cohorts acquired high-resolution 3D T1-weighted images and DTI. For Cohort 1, T1-weighted images were obtained using a BRAVO sequence (TR = 8.16 ms, TE = 3.18 ms, matrix = 256 × 256, FOV = 256 × 256 mm2, slice thickness = 1 mm, flip angle = 12°). DTI was acquired with 64 diffusion-encoding directions (b = 1000 s/mm2) plus 5 b0 volumes (TR = 8500 ms, TE = 80.8 ms, matrix = 128 × 128, slice thickness = 2 mm). For Cohort 2, T1-weighted images used an MPRAGE sequence (TR = 2200 ms, TE = 2.45 ms, matrix = 256 × 256, FOV = 256 × 256 mm2, slice thickness = 1 mm, flip angle = 8°). DTI parameters matched those of Cohort 1 except for TR = 8200 ms, TE = 75 ms, and system-specific bandwidth settings.
T1-weighted images were processed using the Computational Anatomy Toolbox (CAT12, http://dbm.neuro.unijena.de/cat) within Statistical Parametric Mapping software (SPM12, http://www.fil.ion.ucl.ac.uk/spm). Preprocessing included bias field correction, skull stripping, and normalization to Montreal Neurological Institute (MNI) space via the DARTEL algorithm. Automated segmentation yielded gray matter (GM), white matter (WM), and CSF maps. Total intracranial volume (TIV) was calculated as the sum of GM, WM, and CSF volumes. Regional GM volumes were extracted from 136 regions defined by the neuromorphometrics atlas. Cortical thickness was estimated using surface-based morphometry in CAT12.
DTI-ALPS analysis
DTI data were preprocessed in FSL (v6.0.5, University of Oxford, UK, https://fsl.fmrib.ox.ac.uk), including eddy current and motion correction, and brain extraction. Diffusion tensors were fitted with DTIFIT to generate fractional anisotropy (FA) and directional diffusivity maps (Dxx, Dyy, Dzz). These maps were linearly registered to the JHU ICBM-FA template. Four spherical regions of interest (ROIs) were bilaterally placed on projection and association fibers adjacent to the lateral ventricles in standard space. These standardized ROIs were then applied to every subject's registered maps, and mean diffusivity values were extracted in batch using fslstats, ensuring consistent ROI placement and eliminating variability from manual delineation.

This standardized ROI placement reduced operator-dependent variability and improved reproducibility. We defined ROI in the left brain as ALPS-L, ROI in the right brain as ALPS-R and mean ALPS (ALPS-M) = (ALPS-L + ALPS-R)/2.
Plasma biomarker measurements
Blood samples were obtained from patients with T2DM in Cohort 2. Following collection, the samples were processed to isolate platelets, white blood cells, red blood cells, and plasma. Prior to analysis, frozen plasma samples were thawed on ice and allowed to reach room temperature. Subsequently, they were vortexed and centrifuged at 2000 g for 5 min. Analysis for pTau181, pTau217, NfL, Aβ42, and Aβ40 was performed using the specified Fujirebio reagent kits (81288, 81472, 81215, 81298, 81301, Fujirebio, Japan) on a chemiluminescence immunoassay system (Lumipulse G1200, Fujirebio, Japan) according to the manufacturers’ protocols.
Statistical analysis
Continuous variables are presented as mean ± standard deviation, categorical variables as frequency. Continuous variables were compared using one-way ANOVA with Tukey's post-hoc test. All analyses were conducted using IBM SPSS Statistics (version 26.0) and GraphPad Prism (version 9.0.0). Statistical significance was set at a two-sided p-value < 0.05. Partial correlation analyses were performed to evaluate the associations between ALPS index and MMSE/MoCA scores adjusting for age, sex, and education in Cohort 1. The associations between ALPS index brain structural measures were examined using Pearson correlation. Benjamini-Hochberg false discovery rate (FDR) correction was applied for multiple comparisons involving brain regional volumes (134 regions), and that the threshold for significance was set at FDR-adjusted p < 0.05. Receiver operating characteristic (ROC) analysis was performed in Cohort 1 to evaluate the ability of the ALPS index to discriminate participants with MCI from cognitively normal (NC) subjects. The AUC was used to quantify diagnostic performance. Mediation analysis was employed to test whether brain structural measures mediated the relationship between ALPS index and cognitive performance. A three-variable regression model was constructed with the ALPS index as the independent variable, cognitive scores as the outcome, and brain structural metrics as mediators. Mediation analyses were conducted using the PROCESS macro in SPSS. For the plasma biomarker analyses in Cohort 2, we applied Pearson correlation without adjustment and linear regression with/without covariates (age, sex and education).
Results
Participant characteristics
Table 1 summarizes the demographic and clinical characteristics of participants in Cohort 1 and Cohort 2, based on the participant selection flowchart (Supplemental Figure 1). Cohort 1 comprised 60 participants matched for age, sex, and education level, including 20 T2DM patients with mild cognitive impairment (T2-MCI), 20 T2DM patients with normal cognition (T2-NC), and 20 healthy controls with normal cognition (HC-NC). The T2-MCI group exhibited the lowest scores on the MMSE and MoCA, as well as the lowest ALPS-index values (all p < 0.05). No significant differences were observed among the three groups in terms of age, sex, educational level, or APOE4 carrier status (Table 1 and Figure 1). Cohort 2 consisted of 35 elderly T2DM patients with a mean age of 65.3 years (SD = 6.8), including 15 males (42.9%), and a disease duration ranging from 1 to 30 years (median: 10 years). Among them, 15 patients (42.9%) were diagnosed with MCI and 20 (57.1%) had normal cognition. Peripheral blood samples were collected from all participants, and plasma AD biomarkers—including pTau181, pTau217, NfL, Aβ40, and Aβ42—were measured (Table 1). Cohort 1 was used to examine the relationship between the ALPS index, cognitive function, and brain structure in a well-matched case-control framework. Cohort 2 was to validate the association between the ALPS index and plasma neurodegeneration biomarkers in an elderly T2DM population (Figure 1).
Clinical characteristics of the 2 cohorts.
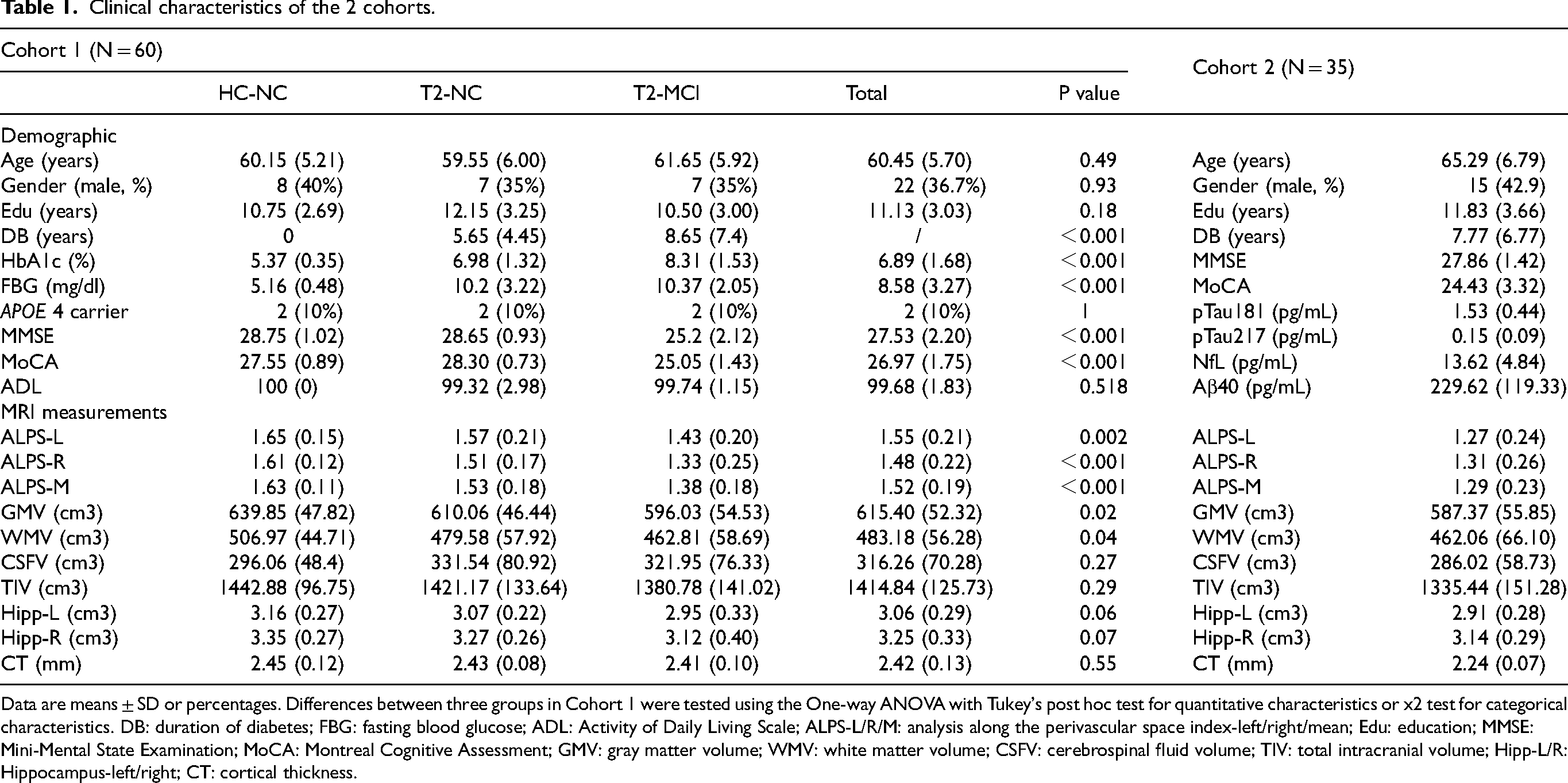
Data are means ± SD or percentages. Differences between three groups in Cohort 1 were tested using the One-way ANOVA with Tukey's post hoc test for quantitative characteristics or x2 test for categorical characteristics. DB: duration of diabetes; FBG: fasting blood glucose; ADL: Activity of Daily Living Scale; ALPS-L/R/M: analysis along the perivascular space index-left/right/mean; Edu: education; MMSE: Mini-Mental State Examination; MoCA: Montreal Cognitive Assessment; GMV: gray matter volume; WMV: white matter volume; CSFV: cerebrospinal fluid volume; TIV: total intracranial volume; Hipp-L/R: Hippocampus-left/right; CT: cortical thickness.
Decreased ALPS index correlates with cognitive impairment and distinguishes MCI from cognitively normal individuals
In Cohort 1, we analyzed the correlation between ALPS index values and cognitive scores (MoCA/MMSE). The ALPS index was positively correlated with both MoCA (ALPS-L/R/M, r = 0.44/0.34/0.44, p = 0.001/0.009/0.001) and MMSE scores (ALPS-L/R/M, r = 0.41/0.33/0.42, p = 0.002/0.012/0.001) adjusted by age, sex, and education (Figure 2A, B). Compared to the HC-NC group, both T2-NC and T2-MCI groups showed significantly lower ALPS index values (p < 0.05 and p < 0.001, respectively) (Figure 2C). Moreover, the T2-MCI group had a lower ALPS index than the T2-NC group (p < 0.01) (Figure 2C). We further evaluated the diagnostic performance of the ALPS index in distinguishing T2-MCI from HC-NC and T2-NC individuals. As shown in Figure 2D and 2E, the ALPS-index demonstrated moderate diagnostic efficacy: for ALPS-M, the area under the curve (AUC) was 0.89 for T2-MCI versus HC-NC, and 0.78 for T2-MCI versus T2-NC.

Association between ALPS index and cognitive performance in cohort 1.
Brain structural metrics, including hippocampal volume and cortical thickness (CT), are recognized indicators of neurodegenerative changes and are closely associated with cognitive function. 21 In Cohort 1, both hippocampal volume and CT were positively correlated with MMSE and MoCA scores (Supplemental Table 1). However, their discriminative ability between T2-MCI and HC-NC or T2-NC was limited—for example, hippocampal volume and CT—and inferior to that of the ALPS-M index (Supplemental Figure 2). These results indicate that a decreased ALPS index is associated with cognitive impairment, and that the ALPS index outperforms hippocampus volume and CT in discriminating between MCI and cognitively normal individuals.
Local brain atrophy mediates the relationship between ALPS index and cognition performance
Voxel-based morphometry (VBM) and surface-based morphometry (SBM) were performed on structural MRI data from Cohort 1 to assess the relationship between the ALPS-index and various brain structural metrics, including GMV, WMV, CSFV, TIV, CT, and regional volumes across 134 brain regions. The ALPS index was positively correlated with GMV and CT, and negatively correlated with CSFV (Figure 3A). Regionally, the volumes of 38 brain regions with ALPS-M (Supplemental Table 2 and Figure 3B), 37 regions correlated with ALPS-L and 16 regions with ALPS-R (Supplemental Table 2 and Supplemental Figure 3), but only the right opercular part of the inferior frontal gyrus (OpIFG-R) still keep significant after FDR adjustment (Supplemental Table 2). Besides, The OpIFG-R showed the strongest correlation with the ALPS index (ALPS-L/ M, r = -0.47/-0.42/-0.45, FDR adjusted p = 0.023/0.048) (Figure 3B, Supplemental Figure 3, Supplemental Table 2). Mediation analysis confirmed that the volume of the OpIFG-R significantly mediated the association between the ALPS index and MMSE/MoCA scores (Figure 3C, D). Furthermore, T2-MCI patients exhibited reduced OpIFG-R volume compared to both T2-NC and HC-NC groups (Supplemental Figure 4). These findings collectively suggest that a lower ALPS index is associated with cognitive impairment in T2DM patients, and that regional brain atrophy (particularly OpIFG-R) may lie on the pathway linking ALPS index to cognition. Causal interpretations are not warranted due to the cross-sectional design.
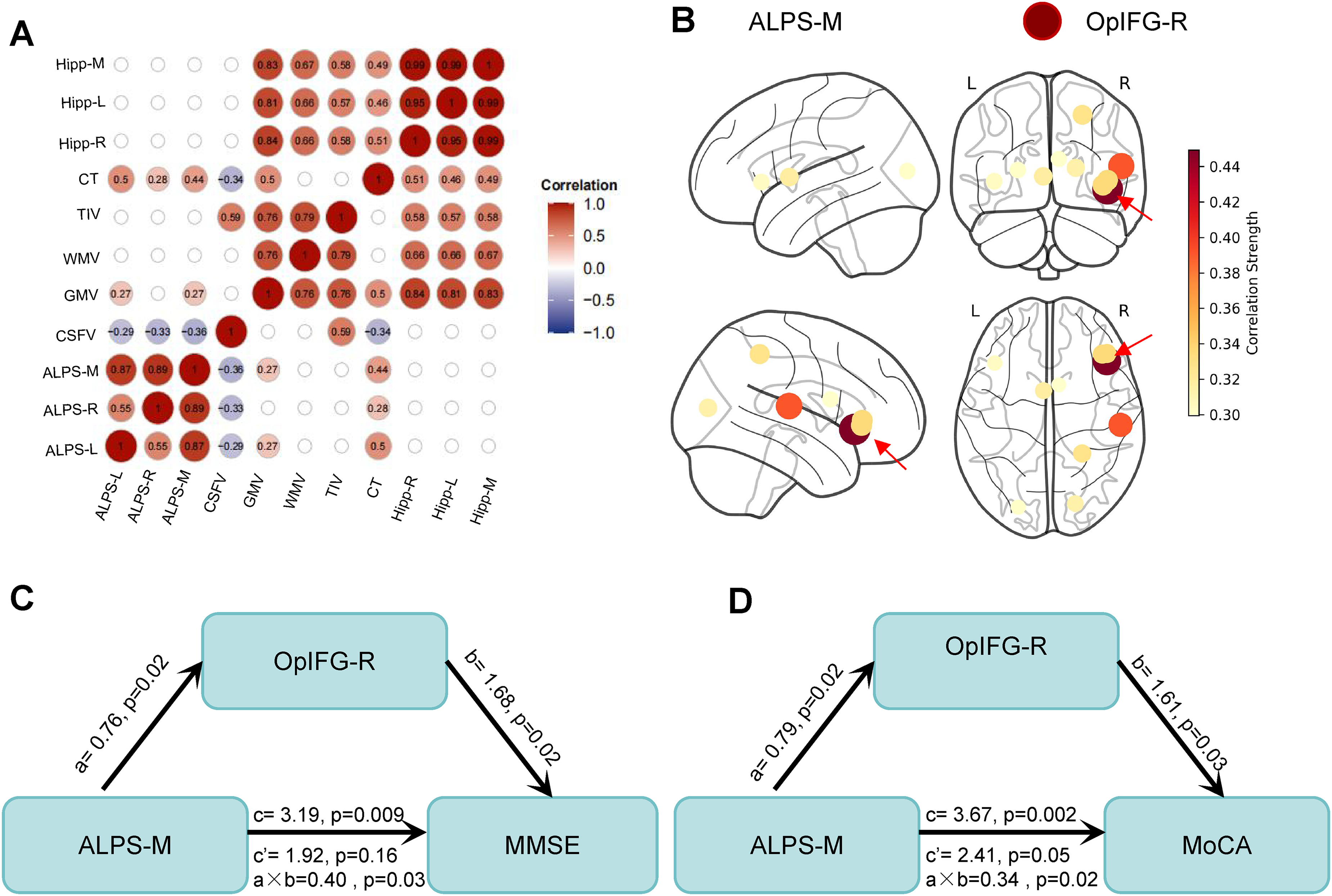
Relationships among ALPS index, brain structure, and cognition in cohort 1. (A) Voxel-based and surface-based morphometry analysis of structural MRI data from Cohort 1 (n = 60), showing correlations between ALPS index and global brain structural metrics including gray matter volume (GMV), white matter volume (WMV), cerebrospinal fluid volume (CSFV), total intracranial volume (TIV), and cortical thickness (CT). (B) Brain regions showing significant correlations (p < 0.05, without FDR adjustment) with ALPS-M index. Circle size represents the strength of correlation (r-value). The right opercular part of the inferior frontal gyrus (OpIFG-R) exhibited the strongest correlation. ALPS-M, ALPS-mean. (C, D) Mediation analysis demonstrating that the OpIFG-R volume mediates the relationship between ALPS index and cognitive performance. c: total effect; c’: direct effect; a × b: indirect effect (structural equation modeling).
Associations between ALPS index and plasma neurodegeneration biomarkers in T2DM patients
Plasma biomarkers, including pTau181, pTau217, NfL, Aβ40, and Aβ42, are widely used to detect pathological changes preceding the clinical onset of AD-like dementia. In Cohort 2, the ALPS index remained significantly correlated with several brain structural metrics, including CT (ALPS-M: r = -0.343, p = 0.044), hippocampus volume (ALPS-R versus hippocampus-R: r = -0.364, p = 0.031), and the volume of the OpIFG-R (ALPS-L: r = -0.418, p = 0.012) (Supplemental Table 3). Furthermore, the ALPS index exhibited significant negative correlations with plasma levels of pTau181 (ALPS-R/M, r = -0.411/-0.382, p = 0.014/ 0.022/) (Figure 4A-C), pTau217 (ALPS-L/R/M, r = -0.429/-0.451/-0.482, p = 0.010/0.007/0.003) (Figure 4D-F), and NfL (ALPS-R/M, r = -0.422/-0.339, p = 0.012/0.047) (Figure 4G-1) without adjustment. Liner regression analysis demonstrated that plasma pTau217 still associated with ALPS index (ALPS-M) adjusted by age, sex and education (Supplemental Table 4). In contrast, no significant associations were observed between the ALPS index and Aβ40, Aβ42, or the Aβ42/Aβ40 ratio (all p>0.05) (Figure 5). These results not only corroborate the association between the ALPS index and brain structural integrity but also reveal a distinct relationship between ALPS index and plasma biomarkers of neurodegeneration in T2DM patients.
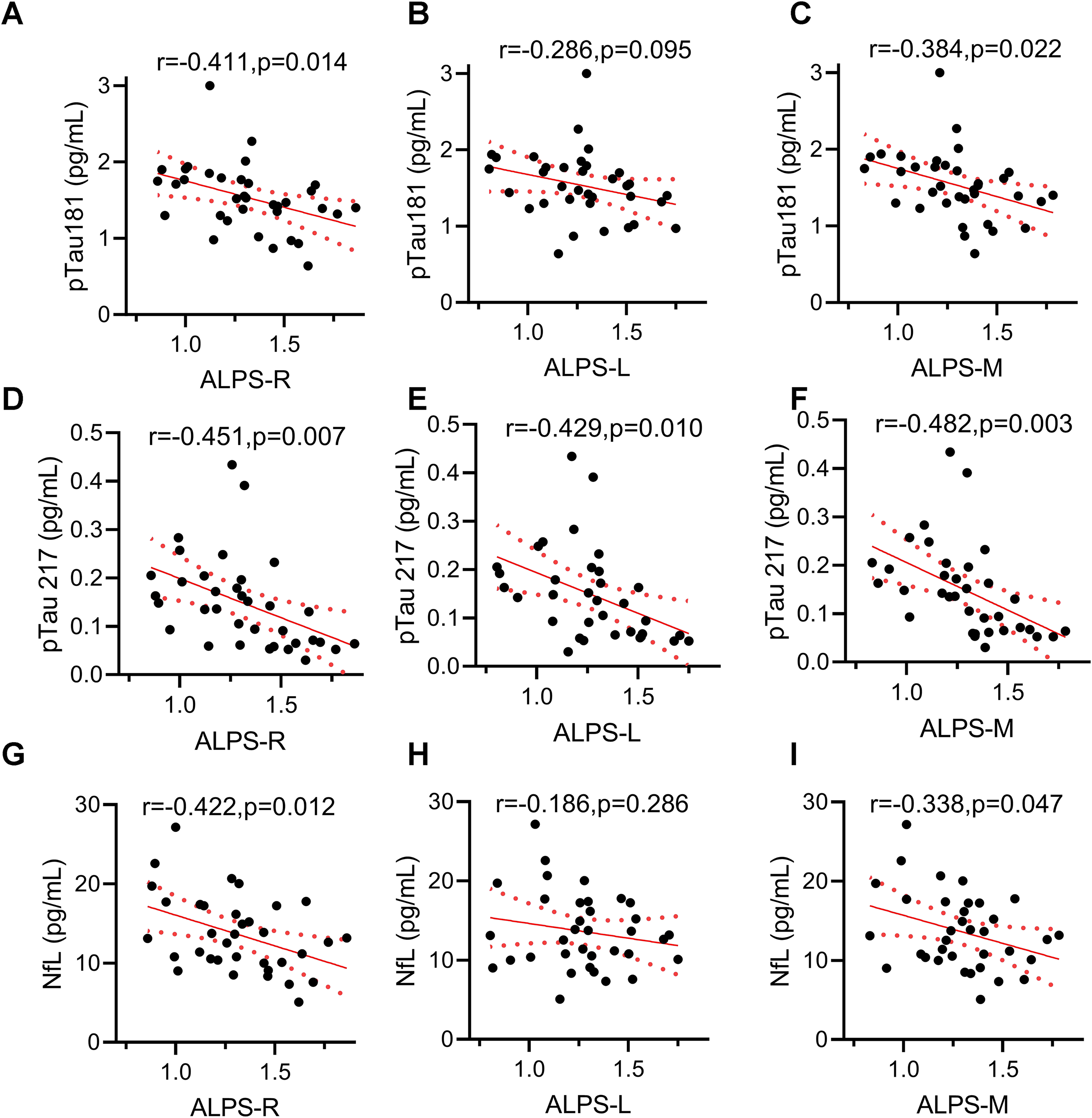
Decreased ALPS index correlated with higher plasma pTau181, pTau217 and NfL in cohort 2. Correlation between ALPS index and plasma (A-C) pTau 181, (D-F) pTau 217 and (G-I) NfL. N = 35 from T2DM patients in Cohort 2, analysis by Pearson correlation without adjustment.
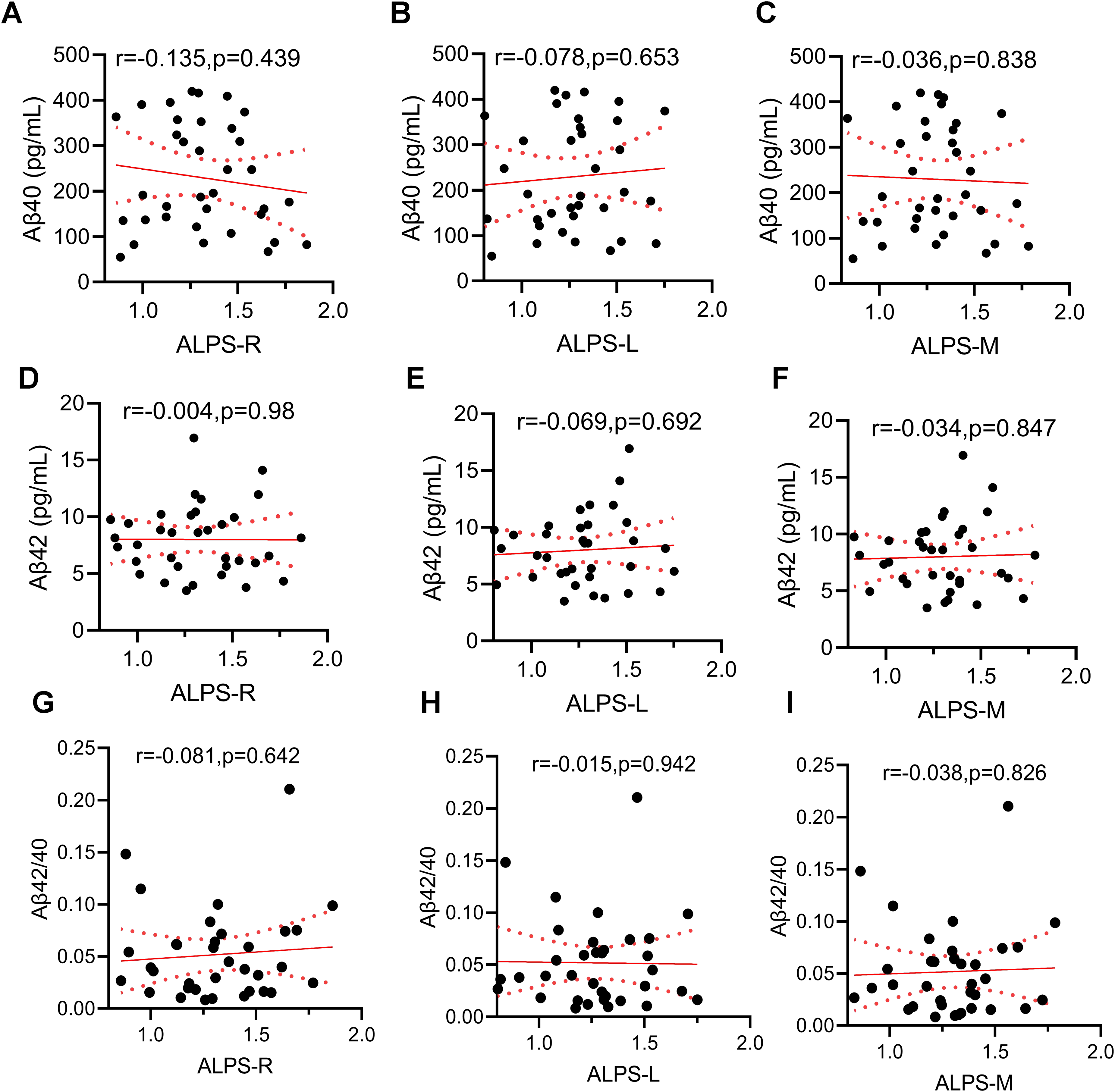
No correlation between ALPS-index with plasma Aβ40, Aβ42, and Aβ42/40 in cohort 2. N = 35 from T2DM patients in Cohort 2, analysis by Pearson correlation without adjustment.
Discussion
T2DM significantly increases the risk of cognitive impairment and AD, yet the underlying mechanisms remain incompletely understood.2,22 In this dual-cohort study, we show that a lower ALPS index in T2DM is consistently associated with poorer cognition, structural brain differences, and higher plasma neurodegeneration biomarkers. Specifically, we found that the ALPS index was significantly lower in T2DM patients with MCI compared to those with normal cognition, suggesting potential utility for identifying T2DM patients with cognitive decline. Moreover, ALPS index was correlated with neurodegeneration (N) markers, including higher CSFV, lower GMV, and reduced CT. Mediation analysis further revealed that atrophy of OpIFG-R partially mediates the relationship between ALPS index and cognitive performance. Notably, the ALPS index exhibited significant negative correlations with plasma tauopathy biomarkers and NfL (Figure 6). These findings support the ALPS index as a feasible, non-invasive imaging marker that may reflect glymphatic-related neurodegenerative processes in T2DM, while further validation is needed before clinical translation.

This schematic summarizes the main associations observed in the dual-cohort study. The ALPS index is an indirect diffusion-based imaging surrogate that has been proposed to reflect aspects of glymphatic system activity, but it does not directly measure glymphatic flow. Lower ALPS index was associated with cognitive impairment, brain atrophy (particularly in the right opercular inferior frontal gyrus), and elevated plasma pTau181, pTau217, and NfL in T2DM patients. These associations are correlational and do not imply causality. Alternative interpretations (e.g., vascular or white matter contributions) are discussed in the text.
Our results align with prior studies reporting reduced ALPS index in T2DM cohorts, and corroborate the association between glymphatic function and cognitive performance.5,7,23 Beyond confirming these observations, our study extends existing knowledge by establishing an integrative link among glymphatic activity, brain structural integrity, plasma biomarkers, and cognitive performance in T2DM. Existing evidences indicated that gray matter atrophy in T2DM follows a spatially patterned and severity-dependent trajectory, with progressive volume loss observed across frontal, limbic, and cerebellar regions as cognitive function declines.24,25 Meta-analytic findings further support that T2DM patients with MCI exhibit pronounced and persistent atrophy in regions such as right superior frontal gyrus, medial orbital gyrus, left superior temporal gyrus, and right talonavicular fissure, underscoring the link between structural degeneration and disease progression.26,27 The glymphatic–meningeal lymphatic system serves as a critical pathway for clearing brain metabolic wastes, including tau and Aβ.28–30 Impaired glymphatic function may lead to the accumulation of neurotoxic proteins and neurodegeneration, as suggested by prior experimental and clinical evidence.28–31 Given the OpIFG's role in executive control and language-related processes, regional susceptibility in this area may be clinically relevant to the cognitive profile observed in T2DM. 32 Our exploratory mediation analysis suggested that OpIFG-R volume statistically accounted for part of the association between ALPS index and cognitive scores; however, given the cross-sectional design, these findings do not imply causality and should be considered hypothesis-generating. The observed statistical mediation is consistent with the hypothesis that regional brain integrity may lie on the pathway linking glymphatic-related metrics to cognition, but alternative directional or confounding relationships cannot be excluded.
A key novel contribution of this work is the identified correlation between the ALPS index and plasma neurodegeneration biomarkers in T2DM patients—to our knowledge, this is among the first studies to link the ALPS index with plasma pTau181, pTau217, and NfL in a T2DM cohort. This finding is consistent with emerging evidence from neurology cohorts where glymphatic dysfunction, assessed via intrathecal contrast-enhanced MRI, correlates with elevated plasma total-tau and NfL. 33 Previous PET-based studies also link ALPS index reduction to tau pathology in Braak-stage-specific regions. 34 It should be noted that plasma tau species and NfL are relatively non-specific markers of neurodegeneration, and the absence of CSF or PET biomarker validation in this study limits the pathological specificity of these associations. Future studies incorporating multimodal biomarkers, such as CSF assays and amyloid/tau PET imaging, are needed to clarify the underlying pathology and determine whether ALPS index alterations specifically relate to AD–related processes in T2DM. Interestingly, we did not observe significant associations between the ALPS index and plasma Aβ, despite prior reports of ALPS-index-related Aβ deposition detected by PET in subjective cognitive decline (SCD) and AD progression. 35 The lack of association with plasma Aβ measures may reflect differences in compartmentalization and clearance dynamics between tau-related and amyloid-related species, which warrants targeted studies using PET/CSF or longitudinal sampling.
Methodologically, the DTI-ALPS approach offers a non-invasive, contrast-free alternative to invasive glymphatic assessment techniques such as intrathecal gadolinium-based contrast agent infusion, which carries risks of neurotoxicity and clinical impracticality. 36 In our cohort, the significantly lower ALPS index in T2-MCI patients relative to T2-NC and HC-NC supports the relevance of glymphatic impairment to cognitive vulnerability in T2DM. The discriminative capacity of the ALPS index for MCI further supports its potential as an early biomarker in T2DM management. According to the National Institute on Aging and Alzheimer's Association (NIA-AA) biological ATN framework for AD, plasma Aβ (A) and tau (T) represent core pathological biomarkers, while neurodegeneration (N) markers —such as brain structural measures and NfL—are less specific to AD but also closely associated with cognitive impairment. 37 In our study, the ALPS index outperformed hippocampus volume and CT in distinguishing MCI from cognitively normal individuals. Previous studies have also demonstrated that the ALPS index exhibits excellent classification performance for SCD versus normal controls, and that a lower ALPS index predicts a higher risk of cognitive progression. 35 Whether the ALPS index could serve as a novel N biomarker warrants further validation in larger cohorts.
Several limitations warrant consideration. First, although the ALPS index is widely used as a glymphatic proxy, its direct validation against pathophysiological measures in humans remains limited. Intrathecal gadolinium-enhanced MRI and gBOLD-CSF coupling methods could be other multimodal validation in future studies. 38 Second, the retrospective and cross-sectional design of our study, coupled with a modest sample size, limits causal inference and statistical power. Future longitudinal studies with larger cohorts are essential to track ALPS index dynamics and their predictive value for cognitive outcomes. In addition, the ALPS index may be influenced by sleep quality, white-matter microstructural alterations and vascular factors commonly present in T2DM, a metabolically and vascularly heterogeneous condition in which microvascular complications and overall vascular risk burden may also affect glymphatic transport.38,39 Moreover, although the ALPS index is widely used as an imaging surrogate, it reflects diffusion anisotropy along perivascular spaces rather than direct glymphatic flow and may be influenced by factors such as free-water in small-vessel disease and age-related changes 40 ; therefore, mechanistic interpretations should be made with caution. Finally, the ALPS index reflects global rather than regional glymphatic function, which may reduce its sensitivity to focal proteinopathies in early AD stages. Emerging imaging techniques capable of quantifying regional glymphatic activity may help address this limitation in future studies.
Conclusion
In summary, our findings indicate that A lower ALPS index (an indirect imaging surrogate for glymphatic-related metrics) is associated with cognitive impairment, brain atrophy, and plasma neurodegeneration biomarkers in T2DM patients. These insights enhance our understanding of glymphatic pathophysiology in T2DM and highlight the potential of the ALPS index as a practical tool for early risk stratification and intervention guidance. Further validation in diverse populations and elucidation of molecular mechanisms underlying glymphatic failure will be critical next steps toward translating these findings into clinical practice.
Supplemental Material
sj-docx-1-alz-10.1177_13872877261462893 - Supplemental material for Glymphatic system metrics derived from DTI-ALPS are associated with cognitive impairment, brain atrophy, and plasma tauopathy biomarkers of type 2 diabetes patients: Analysis in dual-cohort
Supplemental material, sj-docx-1-alz-10.1177_13872877261462893 for Glymphatic system metrics derived from DTI-ALPS are associated with cognitive impairment, brain atrophy, and plasma tauopathy biomarkers of type 2 diabetes patients: Analysis in dual-cohort by Yang Gao, Weiqiang Liang, Gandig Wang, Zhipeng Xu, Yanchao Liu, Yaqing Wang, Yarong Wang, Yao Zhang, Yuchen Deng, Jie Zhou, Yuying Wang, Huan Li, Lei Gao, Mengqi Tu, Minhua Yu, Sirui Li, Jie Zheng, Jian-Zhi Wang and Haibo Xu in Journal of Alzheimer's Disease
Footnotes
Acknowledgements
We are grateful to the patients in this study for their generous participation and their clinicians for including them in this study. We thank all the people who contributed to this program.
Ethical considerations
The study was approved by the Ethics Committee of Tongji Medical School (No. [2013] S071) and registered at ClinicalTrials.gov (NCT01830998).
Consent to participate
The written informed consent was obtained from all participants.
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the China Postdoctoral Science Foundation General Program (grant number 2024M762504), China Postdoctoral Science Foundation-Hubei Joint Support Program (grant number 2025T084HB).The funders neither played a role in the study design, conduct, data collection, analysis, interpretation, nor participated in the preparation, review, approval of the manuscript.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Yang Gao and Jian-Zhi Wang are Editorial Board Members of this journal but were not involved in the peer-review process nor had access to any information regarding its peer-review.
Data availability statement
Data supporting the results of this study are available from the corresponding author Yang Gao (gaoyangbest@whu.edu.cn).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.