
Abstract
This article discusses the conceptualization of global social policy in its dimension of prescriptions on national social policy. By studying the global health systems discourse and comparing it to the discourse on pensions, the applicability and validity of common notions of contestation and struggle between global social policy actors and their ideas are discussed. On the basis of conceptual considerations on global social policy ideas and discourses, the reasons for the differences between the two discourses are elaborated on. The article offers conclusions as to the conceptualization of global social policy prescriptions with regard to notions of the ‘war of positions’ and the promises of the ASID (agency, structure, institution, discourse) framework.
Introduction
Global social policy and governance are typically characterized by fights over ideas and positions. We find that most of the global social policy literature suggests that global actors and coalitions compete for influence at transnational and national policy arenas. This goes along with opposing models and prescriptions supported and disseminated by different global social policy actors (most prominently, Deacon, 2007; Deacon et al., 1997; and the contributions in Yeates, 2008b). Within the ASID (agency, structure, institution, discourse) approach suggested by Deacon and Stubbs in this special issue, such discourses can be conceptualized in a more structured way within multifaceted, complex, hierarchical systems of power, the institutional legacy of global social policy actors and individual and collective action and mechanisms, but the notion of discourse remains one of fundamental contestation – a ‘war of positions’. Missing are serious attempts to ensure that such characterizations are of general applicability across different fields of global social policy. This article addresses the question: Is it valid to conceptualize global social policy as primarily contestational, both in terms of the content of policy models and the relationship between the actors involved?
The use of global social policy studies for the development of a more conceptual understanding of the scope or forms of global social policy has been rather limited and attempts to make global social policy less ‘a-theoretical’ (see Yeates, 2008a: 15) are only beginning. It is the aim of this article to make a contribution to conceptualizing global social policy by way of adding another social policy field for more profound generalizations of what global social policy is. The focus is on the dimension of policy prescriptions for national social policy. First, the article discusses the meaning of global social policy in this particular dimension. Then, a summary description of the global discourse on pension systems is followed by presenting the findings of an original analysis 1 of the global discourse on health systems. On the basis of a comparison between the two discourses and the reasons for the differences between them, a discussion of what the findings imply for the concept and a theory of global social policy and its implications for future research concludes the article.
Global social policy as prescriptions
‘Global social policy’ as a concept can be developed in different ways as can be seen from the other articles to this special issue. Deacon (2007: 1) defines global social policy as consisting of two things, namely social policy prescriptions for national social policy and supranational social policies (global redistribution, global social regulation and global social rights). The boundaries between the two forms are not clear-cut, and some global social policy topics and debates cross-cut them. Furthermore, global social policy has been studied in different ways, for example, as discourses, as governance mechanisms, as solutions to global social problems, or as transnational processes (e.g. trade, care chains). In this special issue, Deacon and Stubbs suggest the ASID framework as a generic tool to study global social policy in its various dimensions. This article limits itself to making a contribution to our knowledge on the ‘prescription’ side only, and applies different dimensions of the ASID framework for this purpose. The following sections discuss the meanings of global social policy actors and their relationship with each other, prescriptions and discourses.
Global social policy is understood as being shaped and driven by international actors. Deacon’s approach (Deacon, 2007; Deacon et al., 1997) primarily focuses on institutional and policy elites; while Yeates (1999, 2008a) has long emphasized the importance of considering a wider range of global policy actors in the analysis of global social policy. Without the intention to challenge the need to take into account various (kinds of) actors in global social policy more generally, this article focuses on international organizations, for reasons of comparability. The global discourse on pension systems has primarily been studied as one between international organizations and associated epistemic communities. In order to make a meaningful comparison and a contribution to the conceptualization of global social policy, the study on health system prescriptions reported here also focuses on international organizations.
International organizations as global social policy actors may have a number of different functions when it comes to providing models for national social policy. They may act as financial institutions with the power of using loan conditionalities; they may be providers of, and surveillance mechanisms for, transnational regulation and rights; they may be sources of normative standards; they may function as research institutions producing and communicating knowledge about social policy issues; or they may provide spaces for national governments to gather for policy exchange and mutual learning. This particular analysis is focused on (the secretariats of) international organizations in their function as providers of ideas or knowledge, and it reflects the terms used in the global social policy literature by Deacon (Deacon, 2007; Deacon et al., 1997).
Global social policy ideas as prescriptions can be conceptualized in different ways, can concern numerous issues and can have different levels of generality. Ideational approaches to the study of social and public policy have been developed and employed, amongst others, by Hall (1993, 1999), Béland (2009; Béland and Cox, 2011) and Campbell (2002). Ideas can relate to the broadest level questions such as the usefulness and general characteristics of a welfare state as a whole, as well as they can concern very detailed technical matters, as we can see in the discussions on indicators following the release of the World Health Report 2000 (WHO, 2000; for the discussion, see, for example, Pedersen, 2002; Shaw, 2002). One can also distinguish between broad ‘global’ (~universally applicable) concepts and prescriptions directly related to a particular country or context. Cross-cutting these distinctions are prescriptions related to different social policy fields such as pensions, education, labour policy and health systems. Capturing this analytically is a highly complex task and involves different kinds of abstractions: the prescriptions need to be conceptualized as ideas and knowledge; with regard to their content, they need to be merged with models (categories for comparing social policy systems). Each of these elements comes with a different logic and different challenges and debates around them. Regarding the content of ideas, comparative research on national social policies has shown the value of comparing the characteristics and development of different social policy fields within one country. What we can see is that, despite particular national cultures that characterize a welfare state as a whole, the different social policy fields may follow different logics and developments (see, for example, Anderson, 2001; Béland and Hacker, 2004). Health and pensions are often seen to be the key social policy fields with huge national budgets devoted to them. Basing a global social policy definition on only one of these fields may miss important common or divergent characteristics of the other one.
Prescriptions are not just there ‘naturally’, and they are, furthermore, not static but in a process of constant revision, addition, rethinking, rediscussion. Schmidt (2008) summarizes a stream of concepts around programmatic ideas that appears to be most useful in this context. Programmatic ideas include a definition of problems to be solved; a list of issues to be considered; a formulation of goals to be achieved; norms, methods and instruments to be applied; together with ‘ideals that frame the more immediate policy ideas proposed to solve any given problem’ (Schmidt, 2008). While this refers to the level of generality, in terms of the type of content, the concept of cognitive or causal ideas is helpful. Such ideas provide recipes, guidelines and maps for political action; they serve to justify policies and programmes by speaking to their interest-based logic and necessity.
In terms of their impact, it is important to see that ideas may matter in two ways: on the one hand, in the form of shared ideas they serve the goals of achieving consensus across institutions and between member states at the international level; on the other hand, contested ideas between different actors at the global level can be observed (McNeill, 2005: 57). This notion is also reflected in Stone’s knowledge terms, developed for the study of global public policy. Stone (2002: 2–3) talks about actors with a policy orientation who are increasingly involved in the global spread of knowledge. Their expertise and status authorizes them to speak on particular policy matters. Influence can be made up of contestational discourse on the best solution to a problem, but it can equally exert influence through consensual knowledge (Stone, 2002: 5). Experts within and around international organizations ‘help transfer the intellectual matter that underpins policies. They can provide the rhetoric, the language and scholarly discourse to give substance and legitimacy to certain preferred positions’ (Stone, 2002: 6). Such concepts have been employed, for example, studying the World Bank by St Clair (2006) and Broad (2006).
For studying social policy as prescriptions, more specification is needed in terms of the particular models of social policy systems that can be identified and compared. Common analysis of comparative social policy and welfare states analysis most often draw on a number of ideal types of welfare state models, and set their particular analysis of one or more countries in relation to this overarching framework. To some extent this is possible, and has been done, in studying global social policy ideas as well. However, given the idea and the knowledge-like nature of global social policy prescriptions, there are significant differences in studying, classifying and comparing what we observe as the models of particular actors (in contrast to an actual national institution). The categories and indicators used need to be adjusted to comparing concepts and models, with origins in particular disciplines or organizational backgrounds, instead of having statehood categories like national histories and legacies in mind. One connected issue is the concern about using Western models of welfare states for the study of global social policy, given that the latter has an important origin in developmental studies and is often rather critical towards defining and distinguishing particular sectors of social policy. In the sense of analytical pragmatism and the rather modest scope of this article to add some insights from one policy field, other than pensions, this article nevertheless distinguishes social policy fields and compares them.
Last but not least, it needs to be taken into account that these prescriptions do not just stand next to each other and are comparable; instead, they are developed, discussed and transformed in relation to each other. Hall has usefully framed policy-making as a process of social learning and explained how ‘powering’ and ‘puzzling’ often go together. This involves interaction between actors, and this is where the discourse enters the picture. Schmidt refers to ideas as the ‘substantive content of discourse’ (2008). Ideas may develop their applications, potentials, persuasive power not only in multi-level processes of vertical policy influence, but also in more horizontally located processes of ideas exchange. As part of the ASID framework, Moulaert and Jessop (2006) define discourse as the ‘intersubjective production of meaning’. Concerning discourse and international organizations, the work by Barnett and Finnemore (1999) and Dostal (2004) is particularly instructive.
A number of global social policy studies report that different international organizations and associated networks or epistemic communities promote different, contradictory policy models, generating global discourses about desirable national social policy. In 1997, Deacon et al. described this as evidence for a new ‘locus of the future ideological and political struggles for better global and national social policies’ (1997: 10) at the global level. This has, importantly, informed policy research and strengthened the characterization of contestational relationships of global policy actors and their ideas. We find competing agencies at the level of mandates, roles or responsibilities given to, or defined by, the respective actors themselves when it comes to justifying the engagement in a particular policy field. Common statements are, for example, that one international organization, such as the WHO, is more mandated to fulfil a particular global task than another organization, such as the World Bank (Koivusalo and Ollila, 1997, 2008). Particularly characterizing Deacon’s work are contestations at the level of ideas. This contest of ideas is expressed in the different approaches promoted by epistemic communities within and around the World Bank and the International Monetary Fund (IMF) (safety net social liberalism), the ILO, the European Union (EU) and the Council of Europe (conservative corporatism) and the United Nations Children’s Fund (UNICEF) and the United Nations Development Programme (UNDP) (Deacon et al., 1997). Deacon (2007: 171) summarizes:
Thus the ideas about desirable national policy carried out and argued for by the international organisations … reveals something approaching a ‘war of position’ between those agencies and actors within them who have argued for a more selective, residual role for the state together with a larger role for private actors in health, social protection and education provision and those who took the opposite view.
The following section illustrates such a ‘war of position’ in the field of pensions.
The global discourse on pension systems
Both Orenstein (2005) and Ervik (2005) have analysed the role of global policy actors in the development, transfer and implementation of the ‘new pension reform’. The global discourse on pension policy has been characterized in the following way. It was the ILO that, during the 1940s, was the internationally leading organization in debates on pension models and the diffusion of ideas about them. The ILO’s ideas were formulated in its Declaration of Philadelphia (1944). This included the model of a unified, national pension insurance system under a central social security administration and a unified set of (old-age and disability) pension benefits which was rather influenced by the Bismarckian German idea of an old-age pension system (a pay-as-you-go [PAYG] system). This approach is sceptical about private financing and supports taxation or social security contributions.
However, building on the case of Chile, which implemented a specific set of pension reforms, the World Bank standardized, theorized and developed a model that became widely spread through the publication of its flagship report Averting the Old Age Crisis (World Bank, 1994). The pension model promoted is comprised of three pillars. The first of these is public, ensuring a rather low basic pension (redistribution). The second pillar is a compulsory private pillar based on defined contributions rather than defined benefits, funded and managed privately (savings). The third pillar is open to any desire for further protection funded privately. In this way, the redistributive and income-related benefits function in different pillars. Later publications on pensions, as well as the formulation and review of the World Bank’s social security strategy (Holzmann, 2009; World Bank – Human Development Network, 2001) continue the reasoning of earlier work (though we might be about to see a shift as a consequence of the global financial crisis). This model of a multi-pillar pension system has been influential in national pension reforms and taken up in scholarly literature as well, and the connected concepts have also streamlined further World Bank activities. At the same time, the popular model and dissemination policies of the World Bank generated a disagreement between different international organizations (World Bank, IMF, US institutions vs ILO, International Social Security Association [ISSA]) and international epistemic communities on the best pension model. This debate was, amongst other things, about public vs private pension schemes, the link between social security/pensions and economic growth/globalization and the definition of the problem. The World Bank model turned out to be more prominent and influential than that of the ILO because of ‘a clearly focused research agenda; a platform that emphasized ancillary benefits for economy-wide savings and investment …; consistency with neoliberal reform agenda; limited opposition from vested interest groups; coordination of campaigning organisation and ability to leverage various resources more effectively’ (Orenstein, 2005: 192ff.; see also Brooks, 2004). However, Deacon (2007: 170) argued that:
Although the World Bank took over the general leadership role in the 1980s and 1990s, and argued for and secured the role-back [sic] of the state system of pensions in favour of privatised and individualised forms, the ILO fought long and hard to expose what it regarded as flaws in the dominant World Bank thinking on pensions by arguing that there was no demographic imperative leading to privatisation, that the European-type schemes are reformable and sustainable, and that the privatisation strategy is merely a cover to increase the share of private capital savings.
Accordingly, the global discourse on pensions has been importantly characterized by competing international organizations that stand for different policy models. Some major global social policy actors engage in discourses over appropriate national social policy arrangements in an uneven, competitive and overlapping global social governance structure that, through institutional legacies, enables or restricts actors to promote certain ideas. This notion has shaped the general perception and characterization of global social policy (in the field of global policy prescriptions, but even beyond that) that it is driven by a ‘war of position’ – contestational relationships between actors and ideas. Nevertheless, contributions to other than global pensions discourses are scarce, and much less comprehensively and thoroughly studied, or the focus is often on issues that are only marginally connected to social policy as a matter of coverage, access or financing. For example, in Hulme and Hulme (2008), education is used as an example to exemplify characteristics and processes of policy transfer. Referring to Robertson (2005) and other authors (Lefrere, 2007; Rutkowski, 2007; Wickens and Sandlin, 2007), the chapter suggests that in education there are similar patterns of controversial ideas as in pensions. However, a look at the literature referred to could also lead to the conclusions that, on the one hand, it is rather focused on concepts of learning or literacy (Robertson, 2005; Wickens and Sandlin, 2007), and on the other, it does not provide for a detailed analysis and findings on the policy ideas of the different actors addressed here (Lefrere, 2007; Rutkowski, 2007). Another example would be labour policy issues, that are, however, primarily located in aspects of transnational social policies such as global regulation or human rights, ILO conventions or corporate social responsibility (CSR). O’Brien (2008) briefly addresses issues of policy models such as the ILO Decent Work agenda, and the implications of conditional loans by international financial institutions (IFIs). There is evidence for a typical controversy between the World Bank/IMF ideas (more flexible and cheap labour to increase competitiveness) and those of the ILO (without proper labour market institutions, macroeconomic stabilization plans risk failure). Certainly, all these issues matter for social policy in a broader sense, but they conceal a more specific understanding of particular dimensions of global social policy that, in turn, could facilitate a more appropriate conceptualization of global social policy as a whole. This implies that the characterization of global social policy as inherently contestational is not based on comprehensive comparative analysis including a number of different social policy fields. The question then arises, to what extent these generalizations hold true when taking into account other social policy fields. For this purpose, the following section reports an analysis of the global discourse on health systems in a comparative perspective with pensions.
The global discourse on health systems
What can be learnt from studying another global social policy discourse – here exemplified with the global discourse on health systems? Certainly, there are some contributions touching upon issues like user fees (e.g. Evans and Morries, 1995; Gilson et al., 1995; McPake, 1993) or single functions of health systems (Lee and Goodman, 2002), that also indicate fights over ideas. With regard to actors and structures, it has been argued that the WHO was the only international organization with a ‘normative mandate’ in the field of health; and that the World Bank was not sufficiently mandated to intervene in the health field despite the fact that it had been active in this area (Koivusalo and Ollila, 1997, 2008). Differences have been identified regarding the support of so-called comprehensive primary health care (PHC) approaches, usually connected to the WHO and other UN social agencies, and those of selective health approaches, associated with UNICEF and the IFIs (see, for example, Koivusalo and Ollila, 1997). 2 There are, thus, indicators that support the ‘common picture’ of a ‘war of position’.
Nevertheless, in a comprehensive sense, the global discourse on health systems has been studied only to a limited extent. Further, on the predominant positions on health systems, the literature is not coherent. While some (e.g. Buse et al., 2002; Cutler et al., 1999) claim that health policy has been subject to the same ideological shift towards privatization and basic public support, others (e.g. Deacon, 2007; Lee and Goodman, 2002) have suggested that global ideas on health systems are not extreme examples for promoting privatization.
The global health systems discourse can look at a longer and a more diverse history than that on pensions. Already in the 1970s, both the WHO and the ILO uttered ideas and activities in the field of health systems, and to some extent struggled over positions (Siddiqi, 1995). Since the 1980s, the World Bank has increased its activity, and became the most important global health actor in terms of financial and staff resources (Koivusalo and Ollila, 1997). Following the failed attempt of the WHO to restore its position in providing advice on health systems, the OECD has significantly increased its activities in the field since about 2000 (Deacon and Kaasch, 2008). Apart from some more marginal UN bodies, since its creation in 1995, the WTO has also developed to be influential with regard to the health sector, though in a somewhat indirect and yet rather speculative sense, less in terms of providing health system models.
In terms of the multiplicity and variety of actors involved, the field of health systems appears to be more complex and multifaceted than that of pensions. The WHO, the World Bank, the ILO and the OECD all, in one or another way, are mandated to provide prescriptions for health systems. However, these activities are partly based on different contexts and different kinds of mandates that need to be taken into account for understanding different positions in a discourse. The WHO and ILO do have clear mandates for engaging with health systems (as social policy fields), but the World Bank, the OECD and some UN bodies derive their mandates from processes of tailoring and broadening existing mandates, for example on fighting poverty (World Bank and some UN bodies), or on general economic and social policy (OECD and some UN bodies). This leads to a ‘typical’ picture of overlapping agencies (as characterized in the work of Bob Deacon), however if, and in what way they compete is a different question.
There is a fight over positions, in that each organization attempts to both define itself in terms of being the most important, competent, or legitimized actor concerning health systems. The ILO, for example, presents itself as the best-suited organization, 3 while the World Bank and the WHO are increasingly pressured to justify their engagement in the topic, which can be observed in various publications. The OECD seeks to demonstrate its legitimacy on the matter by frequently hinting at special member state requests. The division of labour between them is not clear, which increases the need for continuous justification of the engagement in health system issues. Despite individual mandates, roles and forms of competition between international organizations, global social policy in the field of health systems is also characterized by collaboration, cooperation and different forms of networks (across ‘competing’ actors).
Turning the focus to ideas and models, though, the notion of competing actors is not clearly replicated. What we find is rather a high level of uncertainty about best models, coming with vague positions and consensual knowledge. The positions can be summarized as follows:
There is no organization that does not support universal coverage (at least for basic care in a development context).
Health financing should preferably be organized publicly, with an emphasis on pre-payments and big risk pools. When it comes to concrete interventions in developing countries, however, community financing schemes are preferred as first steps towards more encompassing insurance coverage.
The system of financing could be either social insurance style or taxation, or elements of both; there is no ‘one-size-fits-all’ approach, but rather, discussions about advantages and disadvantages of either model.
Strategic purchasing is frequently an issue, but increasingly treated with caution.
It is generally not a market-based model that is recommended. If the US model is mentioned, it is as a bad example (e.g. Roberts et al., 2008).
This implies that the hesitation to make clear recommendations, particularly with regard to the system of financing (taxation and/or social insurance) and the rather vague public–private mix in provision, makes it difficult to clearly identify any particular welfare state or health system type in the models or ideas of the international organizations. The ideas of all organizations are taken from high-income, European welfare states that manage to achieve (close to) universal health care coverage; however, neither type is clearly advocated. Rather, one could say that those elements that distinguish particular health system types are brought into the discussion while not resulting in one coherent (theoretical) model.
Only with regard to the definition of the benefit package are we faced with significant differences. However, the approaches differ in terms of a process- vs content-focus. This means, for example, that a concept such as the one of the WHO Commission for Macroeconomics and Health (WHO CMH, 2001) tries to define the content of, or the criteria for, defining an appropriate benefit package; while ideas from the ILO or in the Alma-Ata tradition always importantly contain reflections on the process of how to decide upon the benefit package (such as including particular groups of the population, social partners, etc.).
Before concluding on a too-harmonized picture, it has to be said that the approach employed by the World Bank Group’s International Finance Corporation (IFC) significantly differs. The IFC explicitly supports only private providers (and in the future possibly also private insurers) without sufficiently taking into account more comprehensive concepts and concerns about health systems as a whole. This is astonishing, as such ideas are provided by other organizations of the World Bank Group. The IFC’s ideas do not match those of the World Bank and appear not to be sufficiently coordinated with other World Bank activities.
The OECD is somewhat different, but less in terms of the basic content than in terms of the context in which its activities take place (mainly high-income countries) and the related approach to the guidance of national health systems. The OECD approach has been characterized as even-handed and of high quality. This is at least true for the prescriptions coming from its Directorate for Employment, Labour and Social Affairs (DELSA) (Deacon and Kaasch, 2008; Kaasch, 2010). However, it needs to be taken into account that it is only partly comparable to the much more comprehensive agenda of other international organizations, both in terms of membership and approach to the topic.
This does not imply that there are no different opinions on specific issues, or that international organizations are not being criticized by other actors. For example, the Global Health Watch (2005, 2008) has indeed come up with a more explicit call for public, taxation-financed systems. However, having mainly focused on international organizations, strong and opposing international epistemic communities could not be identified. The advocacy coalitions behind the main health reports do not seem to have been powerful enough to push the agendas in an effective way.
Further, while historical shifts can be observed, these cannot only be understood as a shift from oppositional models towards more similarities (such as no more mention of user fees by the World Bank). On the other hand, shifts have occurred in relation to the respective function of the health system in focus at a particular point of time. The focus has shifted from provision to financing (WHO and World Bank), or financing to provision (OECD and ILO), to currently a particular emphasis on regulation. Some have interpreted this as a sign of the retreat of the state from financing and provision to a merely regulatory role. Looking at the findings of this analysis reported here, such a view cannot be fully supported. Regulatory concerns rather appear as a matter of strengthening the state’s position in health care overall (in settings where there are perceived lacks), with considering private providers (and to a more limited degree also private insurers) to the extent that they contribute to efficient and quality care, but not at all at the expense of universal and equitable access.
In conclusion, we see a multiplicity of global health actors that have not replaced each other while developing their mandates and roles in this dimension of global social policy. There is no one most important organization and no clear division of labour, thus a certain degree of competition exists, and we observe various forms of collaboration. The relative importance of particular organizations has somewhat shifted, but none of them is free of continuously struggling for a stable role in this particular social policy matter. Global prescriptions on health systems are not characterized by significantly contested ideas that can be related to particular health systems or welfare state ideal types. The documents of different international organizations are not all the same – reflecting characteristics of the respective organizations such as original mandates or staff composition. There are different ideas expressed on some health system aspects, however, these do not add up to the promotion of contesting models of health systems – this hesitation to propose determined and clearly distinguishable models of health systems appears as a typical feature of the global discourse on health systems.
Making sense of different global discourses: Pensions and health systems compared
Contrasting the characteristics of the global pension discourse with ideas on health systems leads to the general conclusion that, while there are some similar structures, the discourses show fundamental differences. Table 1 summarizes the differences between the two global social policy fields.
Comparing health system and pension discourses.
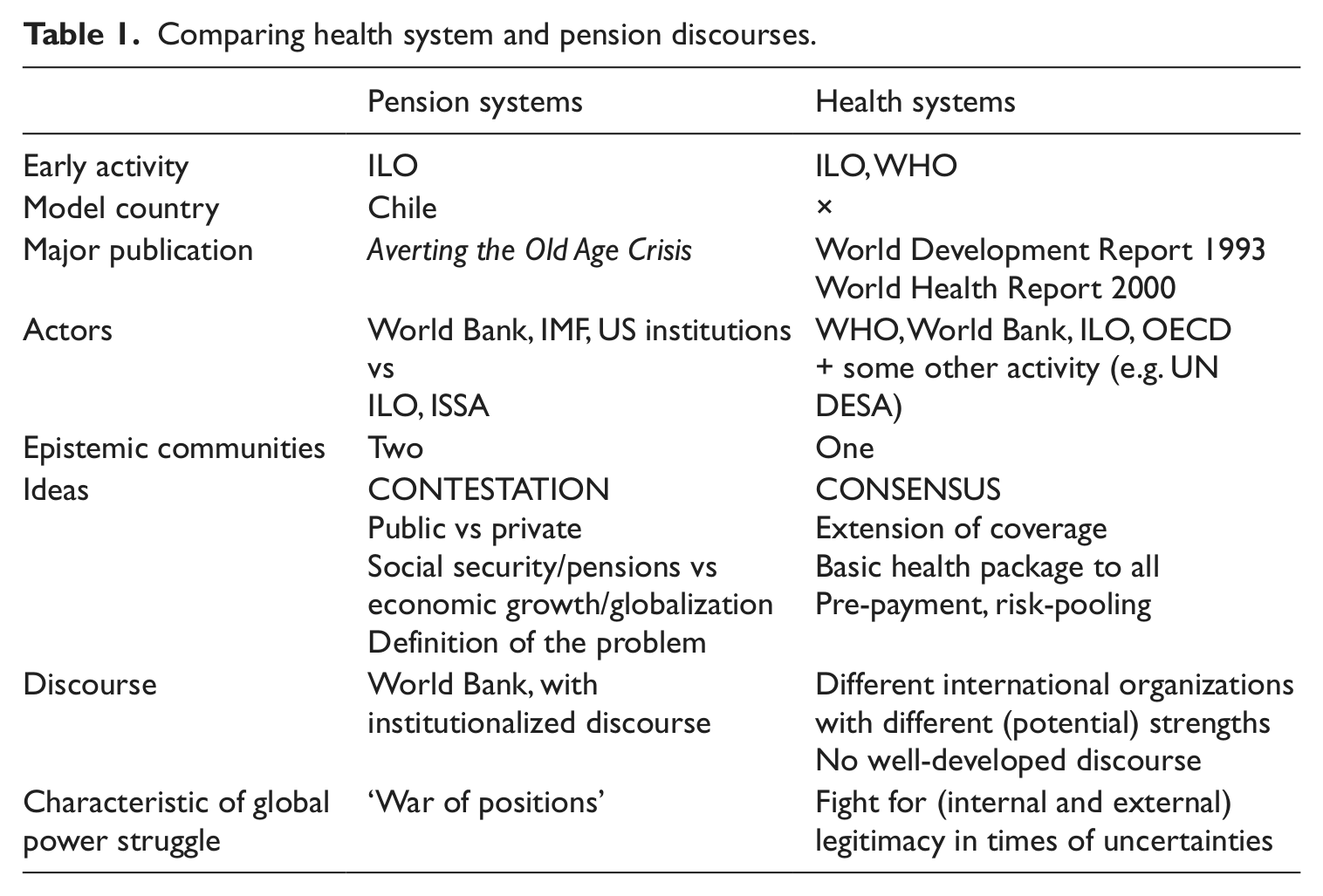
Looking at the actors involved, the two global social policy fields feature similar structures. Both fields include UN social agencies, as well as the international financial institutions, particularly the World Bank, as important global social policy actors. Due to the fact that health systems are more complex than pension systems (see, for example, Béland, 2010), the actor set is more complicated and multifaceted. A look at the history shows that health systems have a longer tradition in the activities of international organizations. However, when the pensions discourse arose, it appeared to be much stronger than that on health systems. This strengthens the case for considerate analyses including agency, structure and institutions for the characterization of global social policy, in order to identify gradual differences.
Regarding global ideas, the implications of this analysis are more severe. Global ideas about health systems are much less characterized by contestation about distinctive models than those on pensions. One or several comprehensive health system models that could be related to actual health systems or ideal types such as NHS systems (UK, Nordic countries), or particular types of insurance systems (such as in Germany), or a marketized system (as we find in the US), cannot be identified. This means that none of the organizations goes for any one ideal type of health systems. Instead, they opt for some sort of mix in between extreme cases. The ideological debates that have been stated to be a key characteristic for global social policy have to be carefully revisited. There are, indeed, ideological debates about many aspects of the provision, financing and regulation of health systems; however, we do not find one big, system-wide site of ideological contestation. Nevertheless, the increasing global concern about health systems over the past years might, of course, lead to more clear-cut models that differ from one organization to the other more clearly and result in something comparable to the pensions discourse in the future. Possibly, though, if one understands the privatization advocacy in the pension field as a deliberate policy strategy to push privatization, not one to solve the problems of old age, health systems might just not lend themselves to support privatization in a similar way. Even voices in support of user fees have become rather careful over the course of time.
Consensual knowledge shared by international organizations (with the exception of the IFC) prevails when it comes to important elements and issues of health systems such as the extension of coverage, at least a basic health package to all, pre-payment and risk-pooling. It is important to see the difference to the pensions discourse: the health system ideas and concepts, while based on different normative starting points and being expressed in somewhat different words, do not add up to clear public–private distinctions; they do not define the same problem in a fundamentally different way; and they do not provide evidence for a major disagreement about the function of a health system as one observes in the pensions discourse where it is about a system to support social security or one to support economic growth and globalization.
Thinking about possible reasons for these differences, one explanation could be the fact that there is much less of one dominant European way of organizing health systems as there is for pensions. The dominant pension model within Europe (except for the UK) is a Bismarckian-style PAYG system. Hence, the ILO and EU are likely to favour such a model. There is no such convergence for health systems that feature different kinds of insurance and taxation models in different European countries. This could explain the constant discussions and elaborations on advantages and disadvantages of taxation vs insurance models in health without ever coming to a statement about which one is better. One might, of course, also argue that an open playing field without strong models could generate more contestation over different ideas, but analysing what is going on in health systems it appears rather as a significant uncertainty about best solutions that are also characteristic for many national health system debates.
At the same time, when it is about developing countries, the more concrete interventions and suggestions usually focus on community schemes that – at least concerning health financing – are not meant to represent the ‘final system’, but a medium-term means to increase access to insurance and health care, and start a system of risk-pooling. While similar approaches to explaining the basic problems of the specific social policy field have been observed between pensions and health, the health system models resulting from these different starting points have been found not to be fundamentally different, at least not significantly in terms of the role of the state, and along the public–private or centralized–decentralized scales, although there are different emphases, as between the balance of public–private. In contrast to pensions, private actors are not preferred because they support economic growth, but because, on the one hand, they are a reality and, on the other, because of perceived failures in the public delivery of services. The reasoning is completely different. The actors involved do not emphasize the differences, be this as a matter of uncertainty as suggested above, or as a conscious strategy not to reproduce the struggle over pensions (explicitly in ILO, 1999).
Another interesting difference is that while publications on health systems use and refer to good practices in particular countries, there is no such prime example of a health system. Most notably, the US is typically mentioned as the bad case. Thus, there is certainly no ‘Chile’ for the health system that would serve as a source for developing a model that could both spread as a worldwide idea about how to organize a pension system, and serve as a concrete case for policy learning in World Bank projects and advisory activities and seminars (for example, in other Latin American countries and in Central and Eastern Europe).
In terms of the structure of the discourse, there are some differences, too. The Alma-Ata Declaration, the 1993 World Development Report Investing in Health and the World Health Report 2000 on health systems (WHR 2000) are frequently referred to in global health literature both by international organizations and also parts of the academic literature, but it would be an exaggeration to state that these had a similar impact as Averting the Old Age Crisis. The communication process – which has been particularly conscious and extensive for the Averting report (Orenstein, 2008) – has been different and weaker. Further, obviously the Alma-Ata Declaration and the proposed PHC model have not proven to be sufficiently convincing in terms of providing a clear concept of policy guidance and an applicable model, and not sufficiently successful at country level to provide for a convincing model case, either. Finally, the WHR 2000 was flawed by combining a framework of health systems with a contested ranking of countries as to their performance, killing off much of what could have been developed out of it in terms of modelling and policy advice. This means that there is no one document of reference in health. This fact might also be the reason for the lack of a clear oppositional model or contesting ideas (in addition to explanations made earlier such as conscious avoidance of controversial discourse, or uncertainty as to the topic of health systems).
Reasons for these differences could also be in the nature of health systems being associated with so much more than systems of social protection or redistribution. Comparing the pension discourse to that of health raises questions concerning the respective long-term vs short-term/emergency character of proposed models. While for pensions it is obviously about generalized, global, long-term redistribution models and issues of encouraging capital growth through savings, that is not the case for all models on health systems, or not as important as in pensions. The global reflections of health systems are often simultaneously concerned about emergency care, short-, medium- and long-term ideas and perhaps a reason for not coming up with one rather concrete model of health systems is the very fact that such a broad task goes beyond what a health system model can achieve.
While there are certainly different networks (see Lee and Goodman, 2002) and also differences in ideas or expressions that characterize different documents, this does not add up to clearly distinguishable groups of organizations and epistemic communities promoting conflicting policy models. The international organizations involved rather seem to be struggling with similar difficulties of not possessing final ideas, strong tools, or convincing arguments for going one way or another.
Or could the reasons for differences between the discourses be the lack of strong (global) market ideologues in health? This would be an important contrast to the pension discourse that has been characterized by market proponents such as Robert Holzmann and Estelle James. The only truly divergent ‘voices’ (in terms of international organizations) with regard to health systems seem to be coming out of the IFC.
In summary, the two global social policy fields of health and pensions are remarkably different when it comes to the forms and levels of competition or contestation between global health actors and their ideas. For health systems, it is rather uncertainty and consensual knowledge on the general structures and basic aims of health systems, while differences are in some specifics (for example how to approach the issue of benefit packages) and on the normative aim expressed in documents. In contrast, with pensions, demonstrating ‘we have the best solution’, and able to push this through against resistance, seems to be part of the game. The reasons are connected to the nature of the content of global social policy discourses, as well as to positions and strategic decisions concerning global social governance positions, and have important implications for the conceptualization of global social policy more broadly.
Conceptualizing global social policy prescriptions
What do the differences between the global social policy fields of pensions and health systems imply for a general understanding of global social policy? How can we conceptualize the prescription side of global social policy by more, or other, than notions of contestation and competition?
In terms of global social governance, instead of competing for an exclusive right to shape national social policy in the field of health, international organizations are increasingly pressured to justify their own activities in the field as such, and to keep up institutional and member states’ support for these very activities. By doing this, they acknowledge other, ‘competing’ actors instead of downgrading them in an attempt to make themselves part of the same group and to signal comparative advantages. This is not only a rhetorical means but also reflected in the mutual use of each other’s work as well as collaborative activities in producing and communicating ideas. However, in contrast to the actor constellation in pensions, both the World Bank and the ‘counterpart’ WHO have been shown to lack power and support simultaneously. There is a shared concern in both organizations about too few staff knowledgeable on health systems. The WHO, though, sees its work much more constrained by this issue. While the World Bank also lacks expertise on health systems, it comes with more powerful means (conditionalities and knowledge) to disseminate its ideas. The difficulty of providing a meaningful and conclusive role in providing health system models might prevent a fully developed struggle at the level of actors. At the same time, the OECD, an organization outside the UN system, appears as a rather successful new health actor with considerably expanding activities – a constellation that is only beginning to be reflected in the global social policy literature. This means that the field of health systems is more multi-actored and more ambiguous than that of pensions. This is partly connected to the complexity of the topic, but also to the lack of continuous political support to the knowledge production activities of international organizations. While the consensus over basic rights to health and connected public provision is striking, the development of clear prescriptions is hampered by the lack of success stories in national settings and international involvement in the field.
Competition is part of the game in this dimension of global social policy, but it is not the only characteristic, and thus there is a more complex and more nuanced relationship between global social policy actors that needs to be taken into consideration as a contextual factor of global social policy studies. We need to move beyond concepts of clearly identifiable antagonistic actors to a view to their potential to legitimize their positions and their actions. Only strong positions seem to facilitate a strong competition, not the open playing field. Comparing the discourses on health systems and pensions does not lead to conclusive evidence on whether the health systems discourse will develop into more antagonistic models (as the WHO and/or ILO are getting back more strength), or the pensions discourse is about getting increasingly uncertain in its positions (amongst other things, as a consequence of lost private pension savings due to the global financial crisis).
Further, the relationships between international organizations and their mandates, their scope of activities and other global social policy actors appear to be much more complex than suggested by the characterization of overlapping and competing agencies. While it is true that international organizations usually do not dissolve and, thus, the competition between them does not imply complete replacement of one or another actor, continued support to particular activities is fluctuating and requires regular decisions at different levels of decision-making within the organizations. This is at least valid for the more continuous work going on at the secretariats. There are time-limited working groups like the WHO’s commissions that are given specific tasks and are therefore protected from justifying their work while doing it. The OECD example also shows that activity-specific mandates for particular time-frames (though with the option of extension) can be more productive and easier to justify. The increased support to OECD activities has happened at the same time when the WHO has been struggling to keep up with health system work and at the World Bank there have also been concerns about reductions in health systems staff (thus limited allocations from the World Bank secretariat budget). The case of the World Bank, though, also testifies to the complexity of legitimacy and support for international organizations in general and their health work in particular. This can be illustrated by Norway, which has decided to give extra-budgetary contributions to the health system research activity of the World Bank, at the same time as the very same country is considering refusing regular contributions to the World Bank due to discontent with policies of conditional loans. 4 Further, the case of the ILO’s role in policy models for health systems shows that the mandate itself is not enough when so few staff are devoted to a particular activity. This implies that there are considerable constraints in keeping up a position once it is established, but that this is not necessarily due to another international organization being more powerful. The analysis of the international organizations engaged in policy models for health systems has shown that there is more concern about getting health-system-related activities properly running and extending them, than there is one of a (destructive) competition between international organizations. To that end, international organizations have also been engaged in various forms of collaborative activity in order to join forces on health systems. It is not a simple, two-sided up-and-down process with regard to the most powerful actor; and positions are not fixed in the longer term.
If an adequate description of global social policy discourses is to take proper account of health systems, it would need to distinguish different dimensions or forms of global policy ideas. There are differences at the level of the underlying normative stance of different international organizations or documents within particular traditions. This, however, has not – as in pensions – led to fundamentally different health system models proposed by these actors. Accordingly, a more comprehensive definition of global social policy as global discourses would have to take into account that the ‘war of positions’ does not characterize all social policy fields in the same way and would have to recognize notions of similarities or consensus.
Further, the difficulty of associating health system ideas produced and communicated by global actors with particular types of welfare state or health system arrangements has been partly explained by the perception of a lack of knowledge and not possessing a ‘best model’ on the part of the international organizations. Current models or reform ideas can be at best characterized by adjectives like incomplete or fragmented: they do not add up to a comprehensive set of policy advice to approach health systems as a whole. Thus, an appropriate definition of global social policy would not only assume the promotion of best models, but also include concepts of global uncertainty about desirable social policy.
Only by increasingly taking into account the character of different social policy fields and connected global discourses will it be possible to find out what is the exception and what is the rule. While pensions has been used to formulate the ‘rule’, Orenstein (2008: 8ff., referring to Nelson, 2004) states that:
… pension policy is unusual in being dominated by a clear set of ideas promoted by a powerful international organization and its partners. Other policy areas may display greater fragmentation in transnational policy advice, less focused transnational campaigns, and more resistant domestic politics. No doubt, the campaign for pension privatization has been particularly well organized and successful.
Adding the health systems discourse to the picture, global social policy approaches need to be more open to other dimensions of differences than the public–private dichotomy that often prevails.
Another related issue is that of the possibility of intended consensus. What does this imply, and how can it be conceptualized in global social policy analysis? Are there ‘wars of position’ hidden behind politically correct statements that only simulate consensus? Do staff within international organizations put constraints on thinking about options because they are afraid of being criticized and losing ground in terms of justifying their health engagement? And how do we gain evidence for these findings?
Last but not least, it has been shown that the actor constellations or advocacy coalitions sharing a particular normative position (no matter how that translates into a final policy model) are not always, or not sufficiently, described by distinguishing between international financial institutions and social agencies. The analysis of global ideas about health systems has rather suggested that there are, amongst other things, the following groupings: (a) the IFC versus all others when it concerns the question of explicit support to private actors in health systems; (b) the World Bank and the ILO versus the WHO (Alma-Ata tradition) on the question of how to start building up health systems – with the aim of improving health as such or with the aim of (re)establishing equity; (c) the World Bank and the WHO (WHR 2000) together on the analytical concepts of health system functions and their basic components; (d) at the same time the OECD produces high-quality and even-handed work but only on very specific aspects of health systems and avoids statements about most desirable health policy; and (e) the WTO approaches the field within a completely different logic and does not provide explicit models of health systems and/or their functions. Given the foregoing, it seems impossible to allocate actors into clearly distinguishable health system advocacy coalitions, and new explanatory attempts are needed to capture other than two-sided forms of contestation. One explanation for this picture could be that it is experts, not organizations, driving the discourse. These experts – apart from IFC staff – share more than they contest. Accordingly, global social policy prescriptions do not only emerge from, and develop out of, a struggle over positions, but may equally be driven by common concerns and ‘puzzling’ across organizations.
The fact that we find such differences between two global social policy discourses in the dimensions of prescriptions by international organizations suggests that if we want to come to general conclusions and definitions of global social policy in the dimension of prescriptions to national social policy-making, we need to study and to take into account the different characteristics of different social policy fields. This would require, amongst other things, organized and coherent comparative studies of other social policy discourses. By combining aspects of agency, structures, ideas and discourse, the ASID approach is useful for comprehensive and systematic analyses of global social policy – nevertheless, in my view, it does not prevent global social policy analysis from adopting a more careful distinction between analytical and normative approaches.
Footnotes
Acknowledgements
This article reports part of my PhD research. The project was supervised by Bob Deacon, and the article also reflects much of the – consensual as well as contestational – exchanges we had. Thanks for that!
Notes
Author biography
![]() ). Among her recent publications is forthcoming The Welfare State as Crisis Manager: Explaining the Diversity of Policy Responses to Economic Crisis (with Peter Starke and Franca van Hooren, Palgrave Macmillan).
). Among her recent publications is forthcoming The Welfare State as Crisis Manager: Explaining the Diversity of Policy Responses to Economic Crisis (with Peter Starke and Franca van Hooren, Palgrave Macmillan).