
Abstract
Cosmetic enhancement technologies have been subject to extended sociological and feminist critique, but botulinum neurotoxins (Botox) have been sidelined in this discussion. This has occurred despite Botox’s popularity and accessibility as a non-surgical cosmetic procedure. While Botox shares many similarities with cosmetic enhancement technologies such as cosmetic surgery, we argue that the fields and the socio-spatial organisation of Botox – where Botox is performed and by whom, which we collectively call contextual Botox – not only differentiate it from other cosmetic enhancement technologies but expose how Botox has gone beyond normalisation to become hypernormalised, a domesticated, mundane technology that has largely disappeared into the flows and routines of everyday life. In addition, Botox is a distinct medical and social practice that is multifaceted, being determined by the contexts in which it is found and the forms of cultural capital therein. It is for these reasons, in addition to being the most popular form of cosmetic enhancement, that Botox should be critically scrutinised.
Keywords
Introduction: BOTOX® to Botox
I dye my hair and I do other things [like Botox], so what? (Anna Bligh, in Cogdon, 2009: 35) I’ve had a bit of Botox, which these days feels like having a facial. (Rebecca Gibney, in Watson, 2009: 30) I mean, for me, it’s [Botox] like cleaning my teeth, you know? Something makes your teeth whiter or something stops you having lines. (Simon Cowell, in Jefferies, 2010: 3)
While many people lack the finances to afford Botox, it is more financially accessible than the thousands of dollars (and enduring pain) of more invasive cosmetic enhancement technologies (CETs) (Reel et al., 2008). Prices for Botox treatment vary according to why it is being used, where it is injected, and the consumer’s gender, with one dermatologist noting that Botox for frown lines is slightly cheaper for women than men (Cogdon, 2009). As Botox is relatively affordable and easily accessible in familiar social places, this renders it banal, as mundane as having a haircut or a facial, though at slightly more cost.
To date, little research has examined the socio-cultural factors shaping Botox use, with greater attention granted to ‘extreme’ CETs of cosmetic/aesthetic surgery. Botox has been overlooked as a comparatively harmless, non-invasive procedure. As examined in this article, Botox as a social and medical practice is similar to but also substantially different from other CETs, particularly cosmetic surgery. These divergences and the general accessibility of Botox, warrant sociological and feminist investigation.
This article addresses this shortfall by highlighting how Botox is a mundane socio-cultural artefact due to its association with other everyday practices and its incorporation into familiar environments. The article briefly defines Botox as a product, and examines the existing social literature on cosmetic surgery. This research assists with thinking through how Botox could be theoretically conceptualised, and reflects the shortfall of social research on injectable CETs. Drawing on this existing knowledge, press releases from professional organisations, and media reports (including interviews with medical professionals), we show that Botox is a similar and different medical and cultural artefact to cosmetic surgery. The discussion then demonstrates how Botox is distinguishable from other CETs due to the fields and socio-spatial organisations it is found in, and the types of knowledges and interactions occurring in these spaces. We collectively call this contextual Botox, which broadly relates to where is it performed and by whom, and how this relates to knowledge and power.
We argue the domestication of Botox is evidenced in the movement of Botox from medical contexts to everyday environments that serve to decontextualise it, increase its everydayness, and mask its potential dangers. Accompanied by the relative affordability, procedural ease, and accessibility of Botox, the inherent risks of Botox have become separated from it as a medical product and a procedure, making it appear harmless and similar to more benign non-invasive, non-surgical and familiar cosmetic enhancements. This illustrates how Botox has gone beyond normalisation to become hypernormalised, dissolved into the heterogeneity of other readily available body maintenance products and technological equipment employed in everyday environments to make modern life ‘easier’. Thus, the medical and cultural meanings of Botox and the fields in which it is associated are shifting, and this product becomes fluid in the process. As a result, the mundaneness of Botox must be treated seriously.
What is Botox?
Botox is botulinum neurotoxin. It is produced by the organism clostridium botulinum, and is the most poisonous toxin known. By inactivating proteins known as the SNARE complex, botulinum neurotoxin causes the muscles to contract and blocks the nerves, resulting in paralysis. In diluted forms such as found in Botox, this lasts from 3 to 4 months at which time nerve endings are repaired (Lipham, 2004; Ting and Freiman, 2004). Thus, botulinum neurotoxin is a lethal substance, and desirable aesthetic and medical product.
In the 1980s, two dilute strains of botulinum neurotoxin, A and B, became the first biological toxins approved to treat human diseases such as hyperactive muscles, involuntary muscle contractions, and tremors and spasms in the face, trunk and limbs (Ting and Freiman, 2004). During the treatment of strabismus (crossed eyes) and blepharospasm (uncontrolled blinking), Canadian ophthalmologist Jean Carruthers and her patients discovered a side effect of Botox: it reduced the appearance of frown lines (Benedetto, 2003; Ting and Freiman, 2004). Today, diluted forms of botulinum neurotoxin wage war against a readily identifiable and despised enemy: wrinkles. 1
As a medical and aesthetic tool, Botox is used for a range of on-label (approved) and off-label (unapproved) treatments. These include excessive sweating, migraines, involuntary neck muscle contractions, Parkinson’s disease, cerebral palsy in children, multiple sclerosis, anal fissures, various forms of pain, and vocal disorders (Benedetto, 2003; Klein, 2002; Ting and Freiman, 2004). The primary way Botox has captured the public imagination, however, has been its aesthetic uses. For example, in addition to treating lines and wrinkles, Botox and other injectables can be used to assist individuals to wear stilettos for an entire day (Wilson, 2009) or to tighten sagging cleavage (Macrae, 2009). One female journalist has claimed that having Botox and injectable fillers restored her family’s harmony because she looked less grouchy (Castagnoli, 2013). The markets for Botox are clearly diverse – it has become a ‘cure all’ for a variety of health and aesthetic concerns (Benedetto, 2003; Klein, 2002; Nissen, 2006; Wunder, 2004), as well as a tool for maintaining peace at home and improving one’s work position (Castagnoli, 2013; Hughes, 2012). Botox, therefore, is an investment in one’s public and private life, a form of what Holliday and Cairnie (2007) would term ‘body capital’.
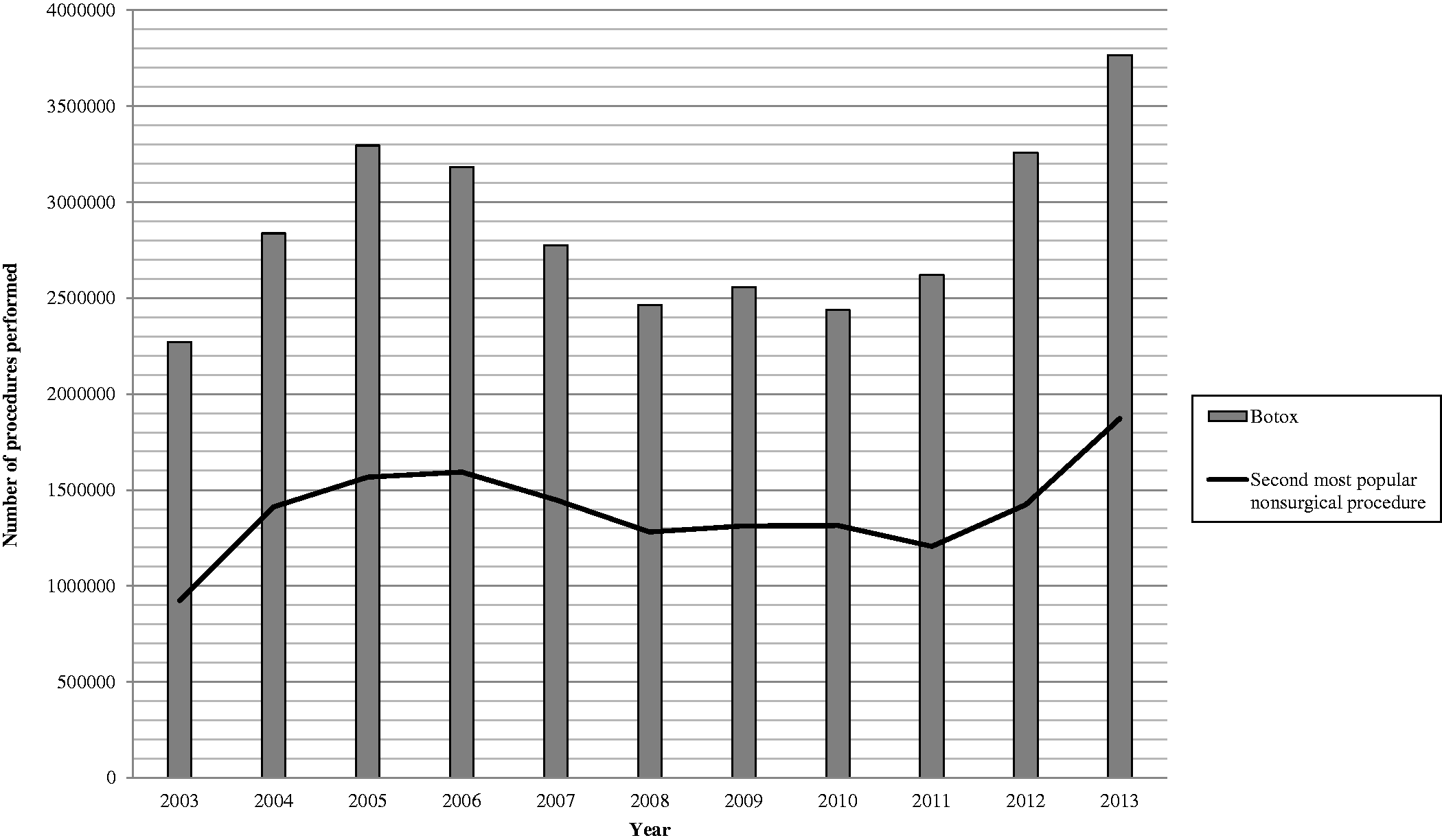
While Botox has captured public imagination, it is still botulinum neurotoxin. Botox injections have been fatal in some patients due to Botox travelling from the injection site to other areas of the body, including paralysing respiratory muscles (Stewart, 2010; US Food and Drug Administration, 2013). Other potential side effects include pain, haemorrhage, infection, drooping eyes, flu-like symptoms, drooling, fever, nausea and headaches (Adverse Drug Reactions Advisory Committee, 2009; Mandeville and Rubin, 2004). Despite these issues, Botox use is significant and increasing. Since approved by the American Food and Drug Administration (FDA) on 15 April 2002 for specific cosmetic purposes (Lipham, 2004), Botox has been the top non-surgical cosmetic intervention in the United States. From 2003 to 2013, Botox procedures were consistently double that of the second most popular non-surgical cosmetic enhancement (laser hair removal in 2003–2005, 2008, and hyaluronic acid in 2006–2007, 2009–2013); in 2012 and 2013, consumption outstripped the other top five non-surgical cosmetic enhancements combined; and during 2013, its use more than tripled the top five surgical cosmetic procedures combined (see Charts 1 and 2).
2
These figures also underestimate Botox use as they exclude non-member procedures and medical tourism (Holliday and Cairnie, 2007). Clearly, Botox use is significantly higher than all other CETs.
Comparison of the number of the top five surgical and non-surgical cosmetic enhancement procedures performed in the United States, 2003–2013. Comparison of the number of procedures performed in the United States, 2003–2013 – Botox and the second most popular non-surgical cosmetic enhancement technology.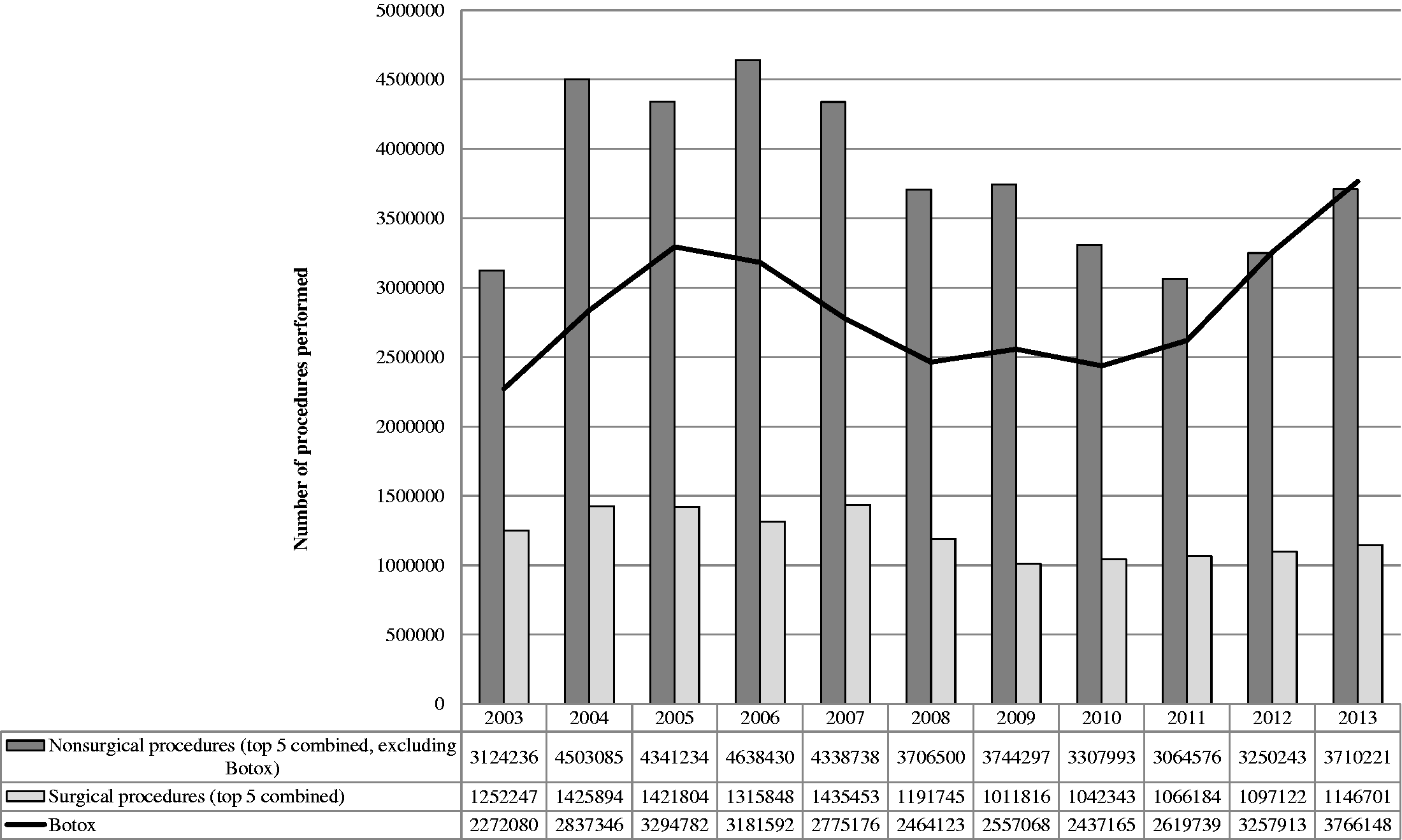
Despite these statistics, Botox is yet to be taken seriously as a social and medical phenomenon within sociology, cultural studies, or feminist studies. Overlooking this practice as worthy of empirical investigation oddly runs alongside an ever increasing discussion of CETs as social phenomena by feminist and socio-cultural theorists alike.
How can we conceptualise Botox in relation to surgical forms of CETs?
Contrasting with plastic and reconstructive surgical procedures seeking to restore or correct bodily function and appearance (e.g. for people with severe burns or physical disfigurement), we define CETs as non-surgical and surgical procedures that alter, change or modify the surface, function and appearance of the body purely for aesthetic purposes. This includes cosmetic/aesthetic surgery and non-invasive procedures such as chemical peels and laser resurfacing, and injectables such as hyaluronic acids and Botox. The most extreme and expensive CETs, cosmetic surgery, has been subject to intense interrogation in existing feminist and socio-cultural research.
One feminist perspective frames CETs as women’s oppression in a Westernised patriarchal culture, offering narrow and unrealistic feminine bodily ideals (Hesse-Biber, 2007). Cosmetic surgery is criticised as ‘correcting’ women’s bodies to better fit with ideals of femininity, founded in real and imagined images of youthfulness and beauty. This highlights the power imbalance of a wealthy, male, professional surgeon defining standards of female attractiveness (Polonijo and Carpiano, 2008), and carving into physically healthy women’s bodies for aesthetic purposes due to their perceived social deviance (Akass and McCabe, 2007). Through such practices women are victims of exploitation (Morgan, 1991), deemed pathological and in need of a ‘cure’ (Blum, 2007).
Other feminist accounts challenge the notion that women are cultural ‘dopes’ or ‘puppets’ unsuspectingly enrolled into a patriarchal, oppressive feminine bodily culture. Research with women who have had cosmetic surgery indicates that they undergo these procedures to look ‘normal’, not like the dominant feminine ideal (Davis, 2003). Women are not tricked by patriarchal culture, but create and shape confident, adaptable and desirable selves (Davis, 1995). They are ‘savvy cultural negotiators, attempting to make out as best they can within a culture that limits their options’ (Gimlin, 2001: 106). From this agentic perspective, cosmetic surgery can empower and is not just about beauty (Davis, 1995) but, as Gimlin’s (2001) work demonstrates, this is only achieved within normative femininities.
These two approaches have differing perspectives on cosmetic surgery: as oppressive, patriarchal and structural, and as liberatory, empowering and individualistic. Socio-cultural accounts of CETs, however, rethink cosmetically enhanced bodies in terms of the social, cultural and economic factors producing the conditions in which cosmetic surgery is made possible and desirable (Elliott, 2008). This indicates CETs are used to discursively mark out particular feminine subjectivities (Balsamo, 1992), with social discourses about women’s bodies informing physician ideas on women’s choices (Parker, 2009) and their own surgical techniques. Thus, client and practitioner interpretations of CETs are filtered through wider social constructions of women’s bodies and cosmetic surgery that are more complicated and nuanced than oppressive or liberatory arguments. In addition, Shapiro (2015) notes, If they [women] cannot or choose not to engage in these types of beautifying body work, they experience social stigma, discrimination and marginalization; if they do participate, they risk being viewed as powerless creatures swept asea by dangerous practices they should have been strong enough to resist. (p. 112)
While Botox has not been extensively critiqued, we can speculate how each perspective may conceptualise this CET. One feminist argument could be mounted against Botox because it represents the material practice of women’s oppression and their desperation to achieve appropriately gendered bodies that align with dominant Western ideals of youthful feminine beauty. Submitting to Botox injections means women are complicit in their own oppression and are disempowered. In contrast, a differing feminist perspective enables an understanding of how, by ‘stopping time’, Botox may make it possible for women to attain an imagined and historically unattainable female body – a confidence inspiring body devoid of wrinkles and makes them feel normal. Thus, Botox can offer women ‘liberation’ from the ‘war against ageing’, a future free from worrying about being ‘traded in’ for a younger model by their partners or the workplace. Botox can make normal (i.e. wrinkle free) female bodies that fade into the backlight of everyday gendered normality and remove bodily induced angst (Shapiro, 2015).
In a socio-cultural paradigm, Botox appears broadly as a bodily technology that resurfaces the body and is not necessarily analysed from a gender perspective. While the emphasis in socio-cultural accounts is ‘how subjectivity and embodiment are inscribed by surgical accounts and practices in the very production of normative and non-normative bodies’ (Doyle and Roen, 2008: 5), Botox can create muted subjectivities that could be situated as deviant (e.g. faces that have limited expressive capacity or do not emote because they are paralysed), atypical of those normally encountered in everyday life. Jones (2012) notes how, although Botox creates mute subjectivities, it is also part of a range of injectables creating temporary, mutable and fashionable looks for women. Arguably, Botox is the fashion artefact which now speaks for itself, a dynamic in which the physician is even more muted because the reputation of Botox precedes clinical knowledges and minutiae processes like informed consent.
Our examination complements the socio-cultural approach by focusing on how Botox is made a medical and cultural artefact through dynamic interactions between social, cultural, economic, medical and political factors. Our approach is influenced by Bourdieu’s concept of field: ‘arenas of production, circulation, and appropriation of goods, services, knowledge, or status, and the competitive positions held by actors in their struggle to accumulate and monopolize these different forms of capital’ (Swartz, 1997: 117). As such, a field is a social space constituted by specific rules, languages, activities and relations. Each field, however, can include individuals with competing interests. Furthermore, a field may have overlapping interests with another field, which can bring these into conflict over capital and resources. For example, Botox is an artefact that intersects with different fields – political, medical, beauty and domestic – that come into competition with each other and are altered by, and alter, the artefact itself. These fields intersecting with Botox create a hierarchy, with divisions and struggles for power that connect to inequalities in economic capital (which refers to material resources such as wealth and profits), cultural capital (such as skills, knowledge and educational credentials), and social capital (networks of connections and acquaintances, and memberships to particular groups) (Bourdieu, 1986).
Our approach goes beyond current understandings of CETs by engaging with structural factors – and not patriarchal culture or gender – that operate within differing contexts, in conjunction with agents therein, to create Botox as an artefact before it reaches the consumer. In other words, our focus is on the complicated structural components that interact with, affect, and are influenced by, the field, context, and the provider and consumer. Significantly, while injectables like Botox may appear mundane in light of the pain and recovery time produced by surgically invasive procedures, they should not be sidelined in academic research. It is particularly important to consider how the field (such as relations between knowledge and place) creates different forms of Botox that construct different relationships between divergent providers, and between provider and consumer. So while we acknowledge the varying approaches to CETs, we illustrate how Botox is located in broader socio-cultural and socio-spatial frameworks as a medical and cultural artefact that marks it as profoundly different to other CETs and worthy of theoretical and empirical investigation in its own right.
The domestication of mundane Botox
[…] mundane technology in everyday life constantly shapes humans, and humans shape it. It enables and constrains various modes of comportment. (Michael, 2000: 41)
In contrast, Botox is a mundane technology. 3 According to Michael (2000), mundane technologies are ‘technologies whose novelty has worn off; these are technologies that are now fully integrated into, and are an unremarkable part of, everyday life’ (p. 3). While Botox still captures the public imagination, it is a mundane technology precisely because it is increasingly aligned with other non-invasive CETs that are ‘normal’ and do not warrant serious attention. As the quotes in the ‘Introduction’ section show, Botox is becoming (or has become) part of beauty regimes that, pardon the pun, do not raise eyebrows. It is an additional feature within the self-maintenance routines of everyday life. In other words, it is a mundane technology because it has transcended the medical field, entering a number of fields that are not special or endowed with specialised and privileged forms of cultural and social capital.
The different forms of contextual Botox.
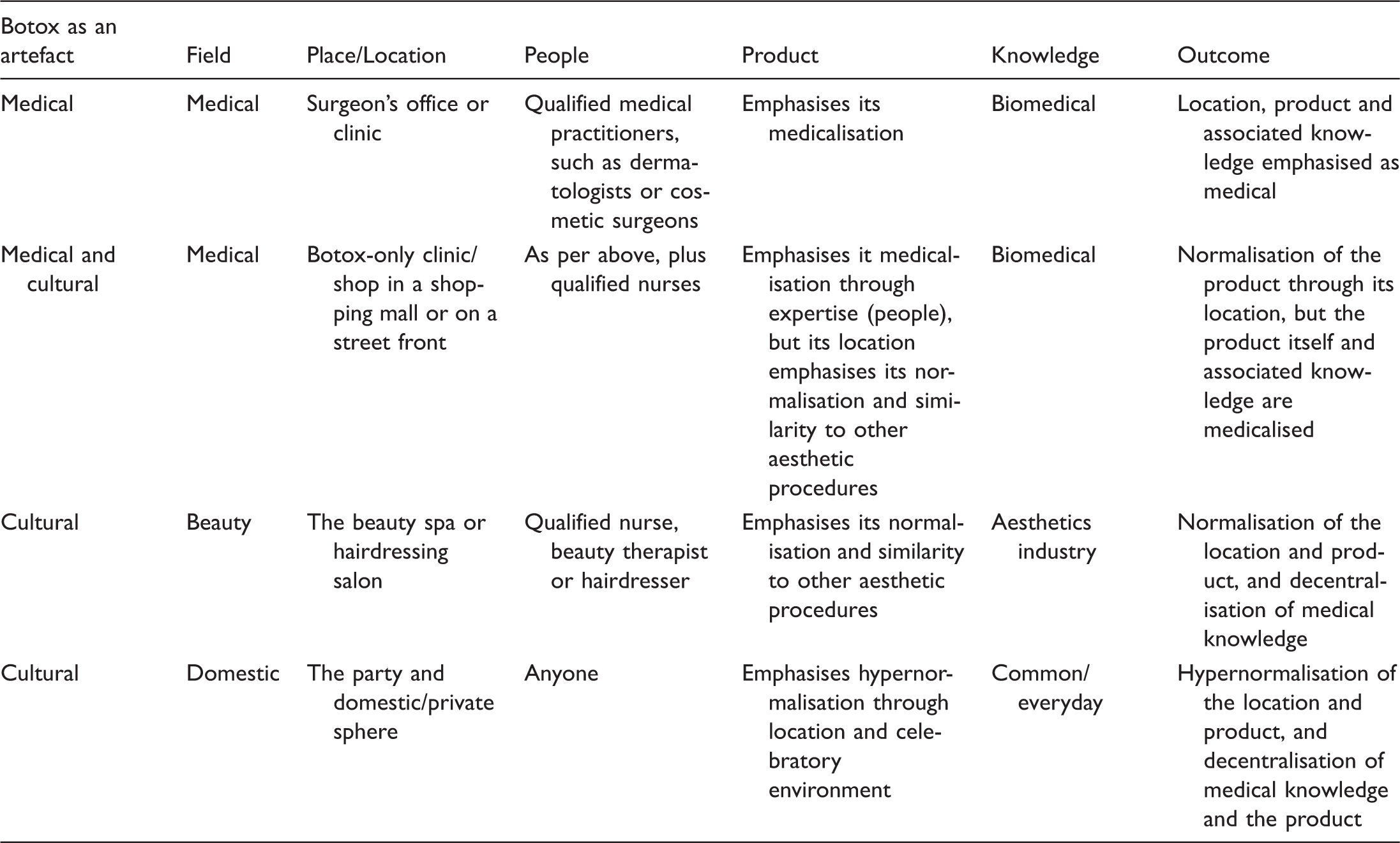
Each location in Table 1 is matched with how the product can be conceptualised as a medical and cultural artefact, and the relationship to production and circulation of knowledge due to its position in place and field. This results in tension between medical and broader cultural conceptualisations of Botox. For example, when Botox is administrated in surgery or a medical practitioner’s office (our first form of contextual Botox), it is located in a medical field that ensures the seriousness and control of the product as medical is maintained and which, in Bourdieusian terms, strongly aligns economic and cultural capital (Bourdieu, 1986). This is because, for example in Australia, Botox is a prescription medicine (classified as S4) meaning it can only be stored, supplied and used by a qualified practitioner. It also cannot be directly marketed to consumers under the brand name by the manufacturer or provider, but a provider can advertise that they supply ‘anti-wrinkle treatments’ (Therapeutic Goods Administration, 2013). 5 These regulations indicate the seriousness of the product by restricting who can have direct access to it, and who (and who not) receives product information. This assumes who has the capacity to understand and evaluate knowledge. 6 The outcome is the creation of a field of power (Swartz, 1997) (dominance of medical authority) that shapes dynamics in the other fields where Botox is located (see Table 1). This privilege of social and cultural capital, and the alignment between the medical and political fields, legitimises the medical profession’s exclusive access to the economic capital associated with Botox. As a result, Botox becomes symbolic of the power relations between different fields.
Medical claims over Botox and its use – a demonstration of cultural capital – are witnessed in calls for further regulation. These emphasise a desire to monitor the product and its supply, and to ensure authority and control over the product including its location, distribution and provision. Botox regulation as a medical product means it should be confined and restricted to a particular field and what relates to that field (context, knowledge, etc.), which reinforces the privileged control of, and strong alignment between, economic and cultural capital for medical professionals. This forms Botox as a medical artefact, an identity that, if it holds, would constrain alternate uses and understandings, and thus reduce the fields in which Botox can be found and the different forms of contextual Botox. The medical pressures to regulate Botox beyond its listing as a prescription medicine, however, are not necessarily successful. This allows other fields of Botox to emerge, and new contexts and forms of cultural capital. For example, after a call in 2007 to regulate Botox in the United Kingdom, the government ‘backed away’ (Climbdown over Botox regulations, 2007: 1), and emphasised consumer responsibility by giving Botox parties ‘the all-clear’ in 2010, provided that practitioners displayed ‘a quality mark’ (Smith, 2010: 13) (see Table 1). Such politicisation of Botox, whereby it transcends medical control and places a value on consumer cultural capital, does not suit the construction of it as only a medical artefact located in the medical field, resulting in continual calls to ban Botox parties internationally (e.g. Doctors call for ban on Botox parties, 2013). Such battles are an attempt to ensure Botox is located in the ‘correct’ field, with those high in cultural capital. This replicates and reinforces claims made to disciplinary authority (Foucault, 1991 in O’Farrell, 2005).
There is little doubt Botox is invested with potential harms in such calls for heightened regulation, yet there is little consistency. This is evidenced by the dislocation of Botox from traditional medical environments and practices (our third and fourth forms of contextual Botox), which challenges medical dominance and control. This demonstrates how the fields in which Botox is found come into conflict. It is important to note, however, that such reconceptualisations emerge from inside and outside of the medical field. For example, as previously indicated, the politicisation of Botox through regulation directs who can have access to it and where it can be administered, facilitating its emergence in new fields and places. Significantly, the regulations (political field) do not mean that only a registered medical doctor can perform Botox injections. This highlights how fields with an interest in Botox overlap. Here, there is a tension between who can prescribe and who can inject Botox. In Australia, a qualified nurse can inject a client with Botox under a medical doctor’s supervision ‘at a distance’, meaning the medical doctor does not need to be physically present or available on-site as long as they can be contacted and written consent for the injections has been provided (Australasian Society of Cosmetic Medicine, 2005). This allows Botox to emerge in non-medical contexts such as beauty salons, as long as the regulations are followed. In this process, locating Botox in the medical field changes and is challenged – medical authority is maintained in its expertise over the body due to regulatory requirements (cultural capital), while taking advantage of expanding markets and contexts for Botox (economic capital). Simultaneously, there is a desire to retain medical power over Botox, and thus maintain the privilege of control over how place, people and knowledge are interlinked. Movements of this injectable outside of medical contexts, however, expose conflicts of interest related to regulation, product control and disciplinary authority. This aids to reconfigure the hierarchical relationship between provider and consumer, and increase economic capital through new fields and entrepreneurialism. These slippages mean that sustaining a strong identity for Botox as a medical artefact restricted to the medical field becomes challenging: Botox should not be done in a spa where you don’t always know exactly who is injecting you and where it is presented in the same context as a hot stone massage or a facial scrub. Nor should it be done in someone’s house where the doctor can’t control the cleanliness or the lighting. (Dr Elkwood, plastic and reconstructive surgeon, in Singer, 2007: G3)
The cultural demand for and financial benefits from Botox have altered how medical contexts are designed and located in social space. The contexts of Botox reconfigure the medical field (our first and second forms of contextual Botox), and alter Botox as an artefact. For example, the movement of specialists to contexts outside of traditional medical environments – our second form of contextual Botox – indicates Botox’s attractiveness as economic capital to medical practitioners, but this also helps promote the decontextualisation of Botox through the alterations of place and an increasing normalisation. By placing Botox clinics in mainstream, convenient environments, Botox becomes highly accessible and is not differentiated from other consumable beauty products found widely in such locations. Therefore, while Botox-only clinics are differentiated from beauty spas (our third form of contextual Botox) in theory, the shop-front location makes them hard to separate in practice and within the social imagination. This is because elements of these different fields overlap, resulting in the social distancing of the product from being a regulated pharmaceutical. It is a quick fix: ‘People just need to be educated that it’s fast, it’s cheap, and it’s not intimidating’ (Dr Rose, plastic and reconstructive surgeon, in Singer, 2007: G3). The medical desire to economically benefit from Botox means the movement to non-clinical contexts challenges the authority that medical experts also seek to claim over Botox. They weaken their social capital and, potentially, their cultural capital. Such changes, however, may experience resistance (the CPSA) and acceptance (Elkwood and Rose) from within the medical field, yet are both reactions to the same pressures exerted from external (political) and less dominant (beauty and domestic) fields, while also revealing the relationship between Botox and economic capital.
Elkwood’s quote also connects to the fourth form of contextual Botox indicated earlier – Botox at home and Botox parties (domestic field). These developments highlight the (mass) commercialisation of the product (Mandeville and Rubin, 2004), its capturing of the public’s imagination, the possibly lucrative entrepreneurial potentials (economic capital), and the exploitation of social fears of ageing. This process hypernormalises Botox by removing all medical contexts and knowledges associated with the procedure and the product, thus removing claims to disciplinary power and control, and making it socially familiar and everyday. The field has shifted from medical to domestic, which lessens the strength of cultural capital.
Botox parties involve groups of clients who socially gather and receive Botox injections. These may occur in a clinic, but also in beauty salons, hotels and people’s private homes. It might have a dress-up theme such as Halloween, Boot Camp or a nursery rhyme (Clough, 2007). These practices imply Botox is playful, worth celebrating, superficial like a costume, and even frivolous because it is less hideous than what it allegedly prevents: vile wrinkles. For organisations like the American Society for Aesthetic Plastic Surgery (ASAPS, 2008), Botox parties are fraught with potential dangers. Again, however, the call of Botox as economic capital and cultural artefact can lure medical specialists outside their traditional contexts, as well as entice illegal Botox markets. For example, Shearer Palmer (2004) reports that As I waited for a routine skin check at my dermatologist’s office, a flyer caught my eye. My doctor was offering a special: If a patient organized a Botox party with six or more guests, he would give the organizer free Botox injections and bring complimentary hors d’oeuvres to the party. (p. 13a) In this atmosphere of ‘Botox parties’ where champagne-sipping socialites are injected with botulinum toxin, it is easy to forget that botulinum toxin is a potent neurotoxin and that its very long term effects are still unknown. (Dr Misra, neurophysiologist, in Simpson, 2013: 1)
At a Botox party, according to the medical field, providers need to ensure they have explained the risks, benefits and possible alternatives, and that clients have understood this information, raised their concerns and made an informed decision. This presumes that such guidelines are adhered to in the medical field. It can also be questioned whether this is possible in the collective, non-threatening environment of a Botox party. The location of Botox in a different (domestic) field means that injections become a symbol of group belonging and solidarity, as opposed to an individual, private intervention. They enable, reinforce and create social capital by bringing people together who all have an interest in Botox, and are likely to be considering it for their aesthetic concerns.
This decontextualisation and decentralisation of Botox means the medical field no longer holds control over the product, and their knowledges become irrelevant. While it could be argued this empowers the consumer to assert their needs outside of the patriarchal institution (and field) of medicine, this is only achieved through significant risks. The procedural confidentiality for the consumer and the provider’s ability to ‘cautiously direct the patient at obtaining emotional and psychological help’ when they have unreasonable expectations of Botox (Benedetto, 2003: 466), are compromised at best. Even if there is a ‘Botox room’ separate from the primary party environment, it will be immediately evident if the procedure has been done: Are there drops of blood? Is any swelling or redness evident? Is frowning possible? Did you have it? The ‘other room’ cannot provide privacy in a peer communal environment – Botox occurs in a public domain where it is openly shared and discussed, and everyone knows what you have had done. In this case, the emotionless face is not a ‘poker face’, as the reduced capacity for expression reveals all. This hypernormalisation of Botox through its domestication exposes the distancing of Botox from being a medical artefact and its reconstitution as a cultural artefact, and the fields shifting from medical to domestic. The contexts and provider–consumer relationship radically change.
As seen by our fourth form of contextual Botox, the decontextualisation and dislocation of Botox from medical product to aesthetic product, and the movement from medical specialisation to everyday practice, takes normalisation to new levels unattainable by cosmetic surgery. Botox has been hypernormalised. This is perhaps best illustrated by the availability of faux-tox and DIY Botox kits, the latter of which are available via the Internet and have previously sold on eBay (Poulter, 2009). Videos can also be found on YouTube showing and instructing users on how to prepare and insert Botox (see https://www.youtube.com/watch?v=TWEPgoDBPw0). Here, Botox is decentralised from the medical in terms of context, knowledge and delivery, and recontextualised in the domestic field, with medical contexts and knowledges completely removed. Potential dangers become obscured behind an image of an everyday beauty product. The complete distancing of Botox from medicalisation thus renders the origins of this substance invisible, and the regulations from the political field silenced. At the same time, Botox parties reconfigure the power dynamic between provider and consumer in ways not possible by CETs that require anaesthetic, as the exclusive control medical professionals have over this product and its profits are challenged. The consumer becomes empowered to assert control – to some extent – over their own body modification practices and contexts. To reassert their fields of power, clinicians therefore highlight how such recontextualisation is problematic: It’s become socially acceptable to buy online, but it’s not medically acceptable at all and the public need to be certain of the quality of products they are purchasing from overseas websites because you simply don’t know what you are getting. (Dr Caswell, from the CPSA, in Smethurst, 2012: 98)
Conclusion
Botox has evolved into a social phenomenon that is different than most [injectables]. (Steven Basta, Chief Executive Officer of BioForm, in Prior, 2007: 6)
Using Bourdieu’s concepts of field and capital, we have shown how intersections and competitions between different fields and the mobilisation of capital – be it economic, social, cultural – alter Botox as an artefact. For example, the medical field seeks to maintain exclusive control and ownership of Botox and its use by drawing on their social and cultural capital, which could enable them to maximise Botox’s economic capital. The political field, however, determines the regulation of Botox, and this opens new opportunities for the medical field as well as challenging their exclusivity. This creates tensions in the medical field, and allows Botox to enter other fields. While this entry into new fields, which we identify as beauty and domestic, opens and creates new markets, this is achieved only through significant risks. The use of field and capital has also allowed us to explore the multiple ways in which Botox may be interpreted, depending on the field and context in which it is found and conceptualised, and the knowledge and practices evident therein. Such an approach is useful for examining artefacts that are found in multiple contexts, what this means in relation to the use of capital, and the competition between and invested interests within fields. This creates the many forms of contextual Botox.
While Botox might connect with feminist ways of thinking, and could be conceptualised as an oppressive apparatus or even as a playful party trick, it is also a bodily technology complicated by its deadliness, its historical and contemporary applications (including warfare), and the elaborate alignments between place, people, product and knowledge. Our argument is that regardless of what configurations and outcomes emerge, including consumer and provider experiences, it is a technology that deserves serious attention because Botox is significantly different from other CETs, and because its configurations and reconfigurations distinguish it from cosmetic surgery. Existing literature on CETs fails to account for these distinct differences, thus subsuming Botox into other cosmetic practices. A failure to understand the divergent configurations of CETs means a failure to adequately understand them as a whole and individually. Overlooking these differences means Botox is becoming invisible to and in the scholarship. The challenges that Botox’s construction as a cultural artefact poses to medicalisation, and the tensions between this artefact’s medical and cultural configurations, are undervalued.
Due to the lack of sociological, feminist, and cultural studies attention to Botox, our examination has heavily relied on media reports and press releases from professional bodies and the existing research on surgical CETs. This should not deter from the significance. There is no doubt that Botox is being marketed in ways that feed off the vulnerabilities of those seeking it (Parker, 2009). There is also no doubt Botox cannot be overlooked simply because it has not yet been the subject of extensive social research. Furthermore, the medical and social attention afforded to Botox emphasises the social currency of this product. Press releases from medical associations, and media reports including interviews with specialists, are important sources of information to understand how Botox is politicised, being discursively formed as an artefact, located in different contexts that create heterogeneous forms of distinctiveness, and being circulated in the public imagination.
Socio-spatial organisation and how that relates to fields, people and knowledge production, are central to how Botox is constructed and experienced. As a medical and cultural artefact, Botox is rewritten by the fields and contexts in which it is found and the interweaving of multiple factors that are not easily reducible. Contextual Botox has been an analytical tool for us to understand what is happening with this artefact. Therefore, while Botox is a medical product and a cultural phenomenon, it is also much more – and less – than that. It is something that should still be raising eyebrows.
Footnotes
Acknowledgements
We would like to thank the anonymous reviewers for their supportive and helpful comments. A much earlier version of this article was presented at The Australian Sociological Association (TASA) 2009 conference.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.