
Abstract
One in 15 Australians over 65 experience dementia, and are commonly supported by spouses. Evidence demonstrates declining wellbeing for these caregivers as their role continues. There are indications of improvement once caregivers transition out of the role (recovery) but alternate suggestions that caregiving stress may be too damaging to be appeased (wear and tear). It seems plausible that reason for transition (care recipient’s move into residential care or death) will affect caregivers’ outcomes. A synthetic cohort method compared caregivers’ stress and wellbeing prior to, and one and two years post-transition. There was evidence of wear and tear for physical wellbeing but recovery for psychological wellbeing over time; with little difference based on reason for transition. Caregiver outcomes seem to be a function of the action rather than the reason for transition, but factors such as age must be considered when designing methods to support post-transition wellbeing.
Approximately 4% of individuals aged 65 to 70, and 25% aged over 85 will experience dementia, with an expected threefold increase in the next 40 years (Alzheimer’s Association, 2012). Worldwide, this equates to the diagnosis of over 7.5 million new cases each year (World Health Organization (WHO), 2012). Reflecting an international trend, Australian family caregivers provide 80% of informal care for those with dementia, without reimbursement (Productivity Commission, 2011). While there is a lack of evidence regarding the number of caregivers in the role at any one time, some data indicate that almost 10% of Australians aged over 50 (i.e. almost 1.5 million people) are currently touched by Alzheimer’s disease (AD) as a caregiver (Pfizer Australia, 2004).
Dementia caregivers are acknowledged to be vulnerable to high stress and consequent poor wellbeing due to characteristics such as the random progression of the disease, problem behaviours and comorbid conditions. Spouses are commonly the primary choice for this role. Often on duty for 24 h a day, seven days a week, perhaps for a period of 10 years or more, spouses can have an additionally exigent experience because of the intense, prolonged time in the role, co-residence, the relationship with the care recipient, and the caregiver's own age-related issues (Aneshensel, Pearlin, Mullan, Zarit, & Whitlatch, 1995; Kim, Chang, Rose, & Kim, 2012; Mace & Rabins, 1981; Vitaliano, 1997). Decline in wellbeing as time in the role increases is common, with poor self-rated health and high levels of depression frequently recorded.
Transition from caregiving
Rodin and Salovey (1989) proposed that changes to wellbeing among older adults, usually attributed to ‘normal’ biological processes, may actually be the result of psychosocial reactions to events such as bereavement or institutionalisation of a spouse. Given this hypothesis, the transition from the primary caregiving role provides a useful dynamic with which to explore outcomes following removal of a chronic stressor. Aside from the situation in which a care recipient passes away, transition is typically the result of their move to formal care. While it is preferable to ‘age in place’, staying in the family home for as long as possible (Bond & Clark, 2002), it is common that at some point the caregiving relationship is no longer functional for either the caregiver, the care recipient, or both (Gaugler, Yu, Krichbaum, & Wyman, 2009). It may be that the stress and responsibility become overwhelming for the spouse caregiver (Annerstedt, Elmståhl, Ingvad, & Samuelsson, 2000), or that placement in residential aged care (RAC) reflects the complex needs of care recipients as the disease progresses (Buhr, Kuchibhatla, & Clipp, 2006). That is, the move to RAC reflects a trade-off between caregivers’ feelings of obligation and desire to keep their loved one at home and the increasing challenge of care recipients’ needs (Liken, 2001).
Recovery versus wear and tear
There are competing theories concerning outcomes following the cessation of caregiving. One proposal is that caregivers ‘recover’ following the removal of chronic stress (Gold, Reis, Markiewicz, & Andres, 1995; Lawton, Moss, Hoffman, & Perkinson, 2000; Sury, Burns, & Brodaty, 2013). Alternatively, ‘wear and tear’ suggests that health is not recovered due to the cumulative effects of chronic stress, and may even decline further (Eloniemi-Sulkava et al., 2002; Schulz, Belle, Czaja, McGinnis, & Stevens, 2004). A brief summary of evidence for these theories follows, according to whether transition is occasioned by residential placement or death.
Following placement, isolation and loneliness, reflecting wear and tear, are commonly cited (Waldrop, 2007). Yet social re-integration, paralleling recovery, is also noted (Bond, Clark, & Davies, 2003; Zarit & Whitlatch, 1992). For example, Ory, Hoffman, Yee, Tennstedt, and Schulz (1999) found that over 50% of caregivers indicated a lack of spare time to spend with other family members and a need to cease pleasurable personal activities due to ongoing caregiving commitments. However, other evidence suggests that with RAC placement the opportunity arises to spend more time engaging in social activities (Bond et al., 2003; Gold et al., 1995). Similar patterns emerge for bereaved ex-caregivers, with evidence that for up to three years they exhibit levels of loneliness, depression and low positive affect comparable to continuing caregivers and significantly different to non-caregivers (Robinson-Whelen, Tada, MacCallum, McGuire, & Kiecolt-Glaser, 2001). In contrast, increased participation in social activities has been reported as a positive outcome and coping strategy in regards to the negative consequences of bereavement (Seltzer & Li, 2000; Utz, Carr, Nesse, & Wortman, 2002). It seems that these types of social factors may contribute to psychosocial vulnerability, with more support decreasing an individual’s sense of vulnerability.
Some sources indicate poor psychological wellbeing following RAC placement (e.g. guilt, depression, anxiety), while others highlight improvement (Infurna, Gerstorf, & Zarit, 2013; Schulz, Hebert, & Boerner, 2008). Post-transition depression has been linked to psychological wellbeing throughout the caregiving journey, greater subjective health impairment and being older or particularly being a spouse caregiver (Gaugler, Mittelman, Hepburn, & Newcomer, 2009). However, it has been suggested that immediate improvements in mental health are common, with stability or improvement likely as time since the transition increases (Bond et al., 2003; Gaugler, Pot, & Zarit, 2007). Psychological wellbeing for bereaved caregivers also shows contradictory results. High pre-loss depression, low mastery, high levels of overload and burden, poor overall health, and being engrossed in the role can be indicative of high levels of post-bereavement depression (Aneshensel, Botticello, & Yamamato-Mitani, 2004; Li, 2005), the pattern of which has been described as curvilinear (Schulz, Newsom, Fleissner, Decamp, & Nieboer, 1997). Ex-caregivers tend to experience a peak in depression during transition, often followed by immediate improvement, followed by a recurrence of symptoms at a less severe level (Schulz et al., 2003; Zhang, Mitchell, Bambauer, Jones, & Prigerson, 2008). While there is some evidence that depressive symptoms may re-emerge within a year, there is an alternate belief that the longer a caregiver is out of the role, the less depression they report (Grant et al., 2002). In regards to recovery, some reports suggest that maintenance of, or improvement in, wellbeing is likely once the caregiver has transitioned due to bereavement (Schulz et al., 2008). Bond, Clark, and Davies (2003) found improved psychological wellbeing in their bereaved caregivers with accounts that over the two year period this group moved toward the population norm for depressive symptoms.
Changes in physical wellbeing are likely to reflect increased opportunities for self-care following transition (Gräsel, 2002) but again findings are contradictory. Some studies report no improvement or poorer physical health after transition, for relinquished and bereaved caregivers, with reference to 1 and 24 month periods (Eloniemi-Sulkava et al., 2002; Lieberman & Fisher, 2001). While Bond et al. (2003) highlighted early improvement for bereaved spouse caregivers, as time since transition increased a decline in physical health was demonstrated. In some cases (e.g. Grant et al., 2002), just as for caregivers whose care recipients move into RAC, those who lose their partner do demonstrate an improvement in serious medical conditions. For example, Gräsel (2002) referred to a decrease in somatic symptoms and subsequently better health (i.e. nearing population norms). Better physical health may be reported as a result of physical care-related tasks ceasing (Gold et al., 1995; von Känel et al., 2011).
Summary and aims
The literature is clear that changes in wellbeing occur following transition from the caregiver role but there remains a need to clarify whether outcomes reflect recovery or wear and tear, whether the reason for transition affects these consequences, and whether other personal attributes may explain outcomes. Transition studies often rely on cross-sectional and/or qualitative data, relatively small samples, retrospective accounts, or are biased by the recency of the event (Schulz et al., 1997). Additionally, studies often combine participants regardless of their reason for transition yet these situations are unique, potentially resulting in different consequences. The current study aimed to address some of these shortcomings by examining a range of variables relevant to chronic stress, psychosocial vulnerability, psychological and physical wellbeing. The focus was on spouses because they constitute the largest cohort of dementia caregivers, and it promoted homogeneity in the sample, controlling for confounds such as relationship, co-residence and time spent together which have been shown to affect caregiver outcomes (Gallicchio, Siddiqi, Langenberg, & Baumgarten, 2002). The research involved longitudinal quantitative methods, taking into consideration the reason for transition, and comparing caregivers according to whether their spouse had moved into RAC, passed away or whether both of these events had occurred. Further, by taking account of the impact of ‘normal’ biological processes the study aimed to investigate whether age or transition is more likely to account for wellbeing outcomes.
Methods
Study design
The parent program from which data for this study were extracted comprised a longitudinal design with data collected at years 1, 2, 3, 5, 6 and 7 (NB: the 24 month gap in between years 3 and 5 was due to complex funding issues). There were 260 participants recruited at baseline, including 200 caregivers (120 ‘new’ caregivers who had been in the role less than 12 months and 80 ‘experienced’ caregivers who had been in the role for at least two years) and 60 age- and sex-matched community members, randomly selected from the South Australian electoral role. From year 2, caregivers no longer actively in the role due to their spouse either having moved into RAC (relinquished) or passing away (bereaved) were defined as ‘ex-caregivers’. For the purpose of this paper the focus is on caregivers and ex-caregivers.
Participants and procedure
Caregivers were recruited through the Memory Disorders Study Unit at Adelaide’s Repatriation General Hospital, and were spouses of individuals with a confirmed diagnosis of AD. All participants were visited in their homes by research nurses and assisted to complete questionnaires. Participants were treated according to the ethical standards of the Australian Psychological Society, with approval granted by the Research and Ethics Committee of the Repatriation General Hospital, an associated teaching hospital of Flinders University.
Data analysis
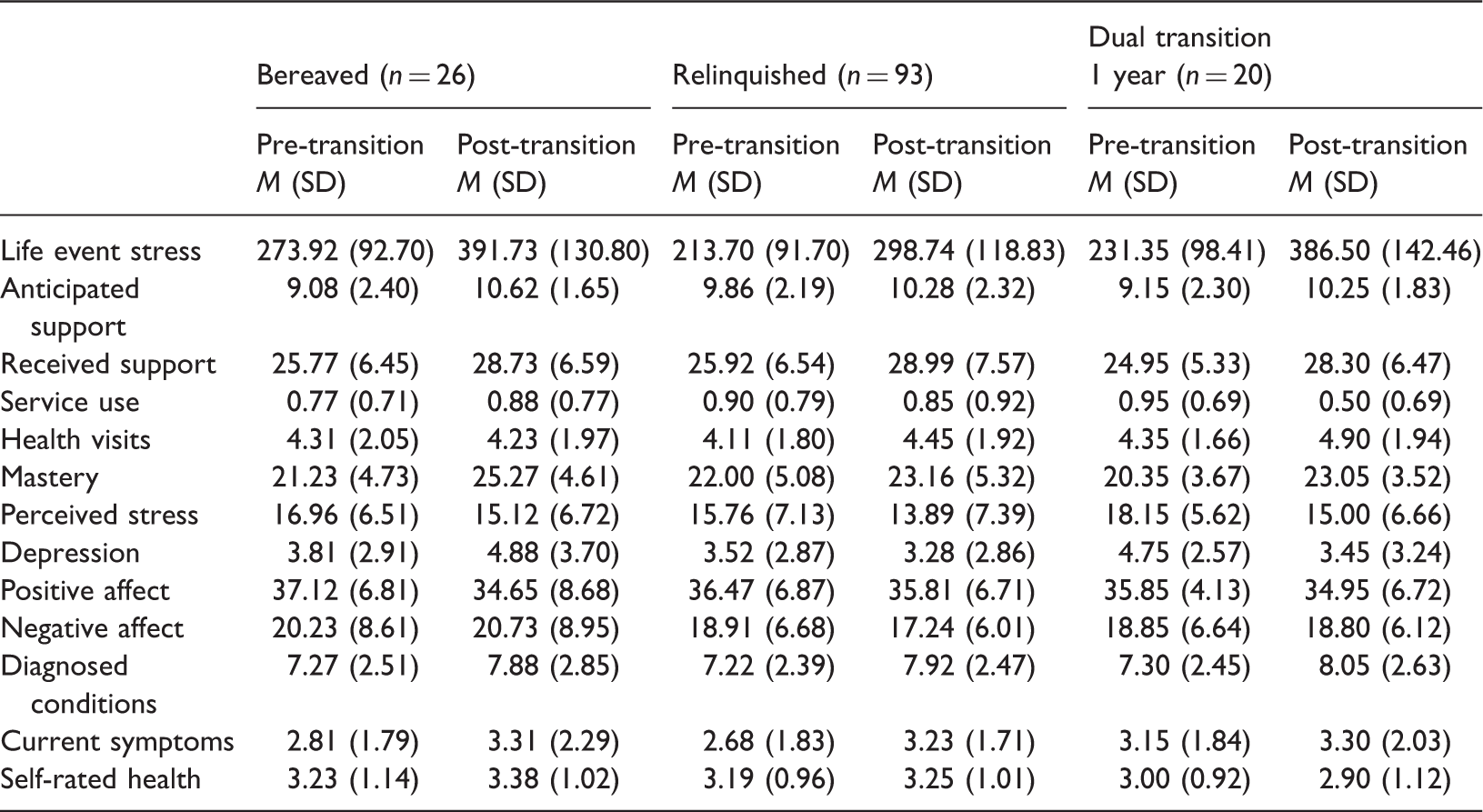
For the current research a specific data set was constructed using the synthetic cohort method (Campbell & Hudson, 1985). This strategy is beneficial in longitudinal research when timing of a key event (such as transition from caregiving) is not controlled; that is, the event occurs at different times for different individuals within a multiwave data set. To enable the impact of the event to be explored more reliably, sample sizes can be increased by pooling observations, centred on the event of interest, with fixed amounts of pre- and post-event data retained. Observations in the current research were pooled for participants who had experienced transition in any year with data retained as follows: data from the last interview prior to transition (while still a caregiver) and the first interview after transition (1 data set), and the interview two years post-transition (a second data set). For the one year post-transition analyses there were bereaved ex-caregivers (n = 26), relinquished ex-caregivers (n = 93) and dual transition 1 year ex-caregivers (n = 20; those whose spouses had moved to RAC and passed away within the same 12 month period).
Using this approach, when two years of post-transition data were required, those who transitioned in year 7 had to be excluded. The two year post-transition assessment period also required the creation of an additional group for those individuals who relinquished in the first year but were bereaved by the second (dual transition 2 years). When considering two years post-transition there were bereaved (n = 20), relinquished (n = 54), dual transition 1 year (n = 18) and dual transition 2 year ex-caregivers (n = 27; care recipient moved to RAC in first year post-transition but died before the second interview). Although this method does not allow for a control group comparison, each individual acts as their own control as individuals’ experiences post-transition are compared to their pre-transition circumstances.
Measures
The interview schedule assessed demographic information (contextual variables), chronic stressors, psychosocial vulnerability and psychological and physical wellbeing.
Demographic information
Age and gender of participant were sought. From year 2, ex-caregivers were questioned about the circumstances of their transition (‘death of spouse’, ‘spouse in RAC’) and its timing (months since the change had occurred).
Chronic stress
The Geriatric Schedule of Recent Events (Amster & Krauss, 1974) is a 35-item checklist of common life events specific to the elderly. Respondents indicate the events experienced in the past 12 months. Scores are derived using a weighting system in which points are allocated according to the stress occasioned by each event. For example, ‘death of spouse’ is considered most stressful (125 points) and ‘vacation’ the least stressful (16 points). Life events are predictive of both physical (Fuller & Larson, 1980) and mental health (Vedhara, Shanks, Anderson, & Lightman, 2000).
Psychosocial vulnerability
Both anticipated and received social support were measured. Anticipated support relates to whether the respondent feels that significant others would be willing to help them in the future (Krause, 1997) and was assessed using three items, with a total score ranging from 4 to 12 where high scores demonstrate more anticipated support. Received support relates to actual support offered by significant others and in the current research was measured using 11 items, with respondents asked to consider the frequency of support in the past year (‘never’ to ‘very often’). There was a possible range of scores of 11 to 44 with higher scores indicating more frequent support. Construct validity is shown by high correlations between received support and desire for dependence (Nagurney, Reich, & Newsom, 2004); predictive validity is evident in relationships between social support, stress and wellbeing (Krause, 1997).
A measure of service use based on the checklist from the Australian Longitudinal Study on Ageing (ALSA; Luszcz et al., 2007) was used. Respondents were asked whether they currently used, or had used in the past 12 months, the services of: Meals on Wheels, Royal District Nursing Society, Domiciliary Care or Respite. A composite service use measure (0–4) was calculated. In addition, respondents considered a checklist of 16 health professionals (Fillenbaum, 1988) and indicated which they had consulted in the past 12 months (e.g. dietician, psychologist, etc.). Number of health visits was obtained by summing responses.
The Mastery Scale (Pearlin & Schooler, 1978) consists of seven items which appraise personal control and coping ability. Respondents select their answer from a 5-point scale (‘strongly agree’ to ‘strongly disagree’), and total scores range from 7 to 35 with higher scores suggesting a greater sense of mastery. This measure has been used extensively in research on stress and psychological resources (Cairney, Corna, Wade, & Streiner, 2007).
The Perceived Stress Scale (PSS-10; Cohen & Williamson, 1988) measures the degree to which respondents believe their lives to be unpredictable, uncontrollable and overloaded. They consider how often each of the described thoughts or emotions has been experienced in the past month using a 5-point scale (‘never’ to ‘very often’). Higher scores (range 0–40) suggest greater perceived stress. Both internal consistency and test–retest reliability, examined over a 12 month interval, are sound (Golden-Kreutz, Browne, Frierson, & Andersen, 2004).
Psychological wellbeing
The short form of the Geriatric Depression Scal
The Positive and Negative Affect Scale (Watson, Clark, & Tellegen, 1988) incorporates two 10-item mood scales consisting of emotional descriptors. Respondents indicate the extent to which they experience that emotion on a 5-point scale (‘very slightly or not at all’ to ‘very much’). Both positive affect (10 items) and negative affect (10 items) scores are obtained (range 10–50 for each). High scores on positive affect suggest energy and enthusiasm while low scores reflect displeasure and lethargy. High negative affect scores reflect distress and negative mood while low scores demonstrate serenity. The scales have high reliability (Molloy, Pallant, & Kantas, 2001) and construct validity with other measures of affect such as the Hopkins Symptom Checklist and the Beck Depression Inventory (Watson et al., 1988).
Physical wellbeing
Both objective and subjective measures were included. Respondents were asked which, if any, of a list of 20 medical conditions they had been diagnosed with and/or were displaying current symptoms of (e.g. arthritis, cancer), using an ALSA checklist (Luszcz et al., 2007) and paralleling those incorporated in other national ageing studies (e.g. Fillenbaum, 1988). Responses were summed to create scores for diagnosed conditions and current symptoms, reflecting a technique discussed by Vilhjalmsson, Kristjanasdottir, and Sveinbjarnardottir (1998) who found that multiple chronic conditions result in higher illness burden. Self-rated health was assessed using a single question: ‘in general, would you say your health is’: ‘excellent’, ‘very good’, ‘good’, ‘fair’ or ‘poor’. Studies have demonstrated the ability of this measure to predict hospital admission, nursing home placement, mortality and morbidity (Idler & Benyamini, 1997; Wolinsky & Tierney, 1998).
Results
Pre- and one year post-transition comparisons of bereaved, relinquished and dual transition 1 year ex-caregivers.
F values for main effects and interactions for pre-transition and one year post-transition models.
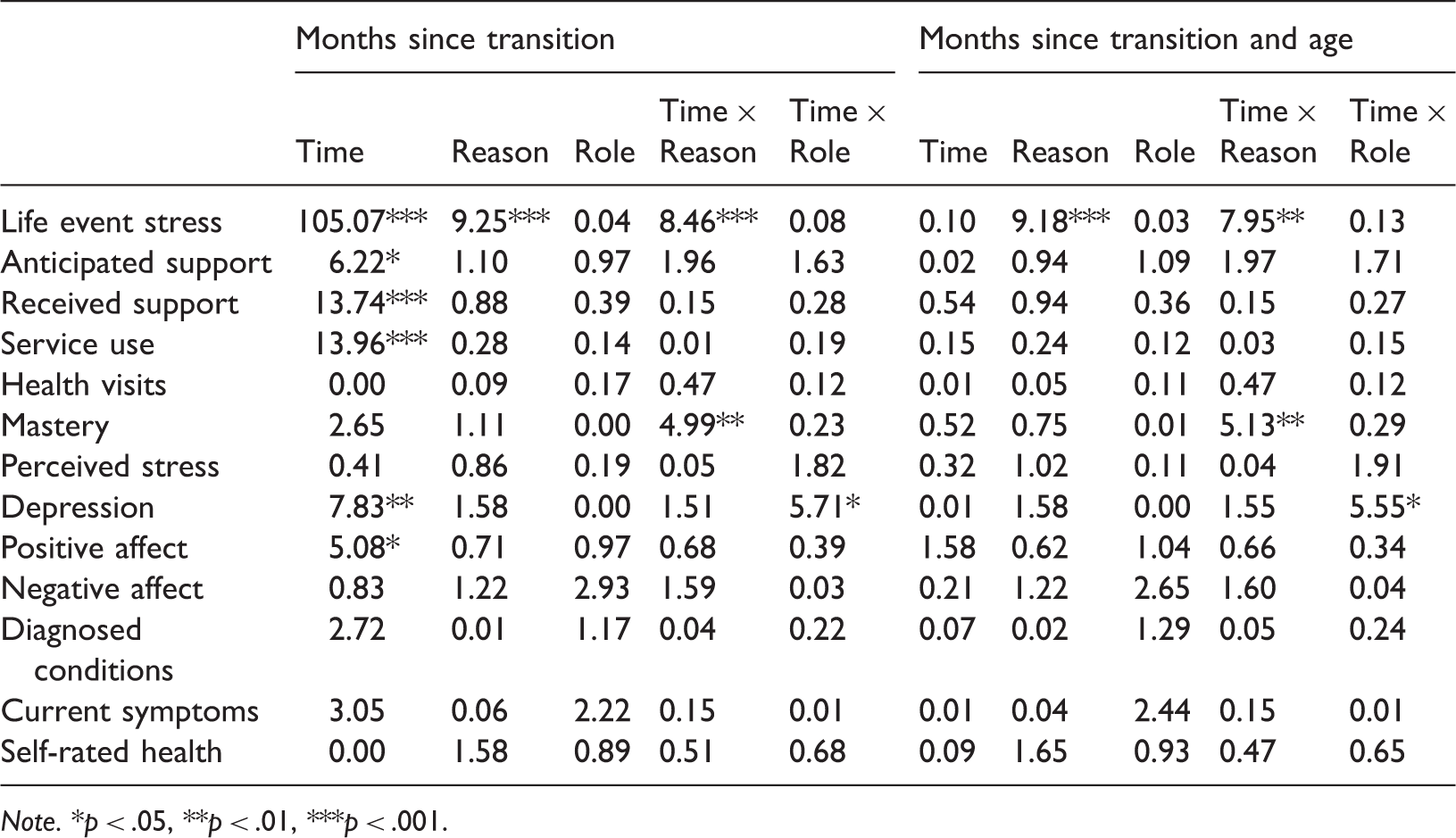
Note. *p < .05, **p < .01, ***p < .001.
Descriptive data for wellbeing according to reason for transition: three time points.

F values for main effects and interactions for three transition time point models.
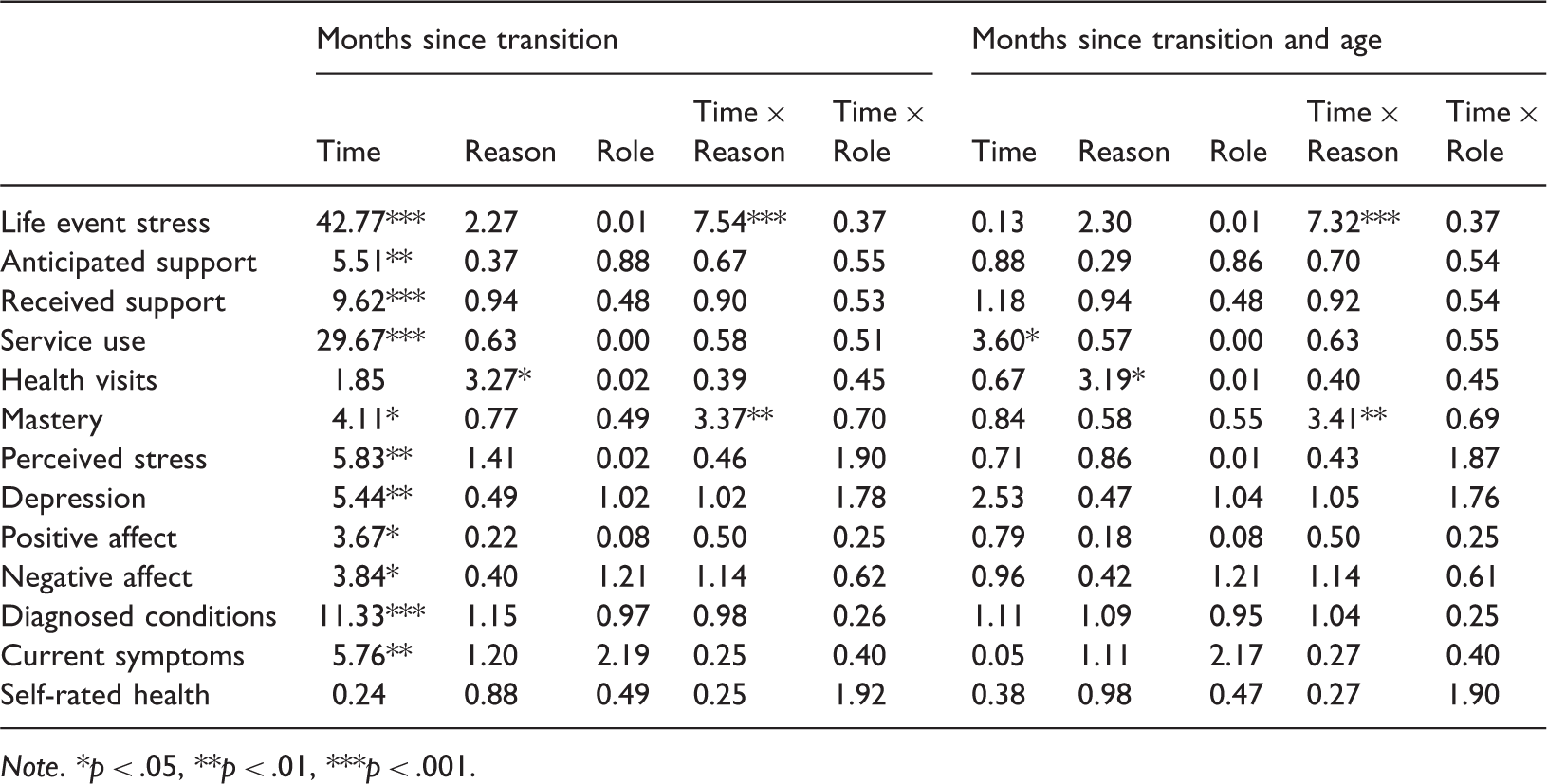
Note. *p < .05, **p < .01, ***p < .001.
Discussion
There are both two main reasons for transition (move to RAC or death) and two main hypotheses for subsequent caregiver wellbeing (recovery or wear and tear). Few studies have explored ex-caregiver wellbeing over time as a function of reason for transition, particularly with the impact of dual transitions included. This was a key objective of the current research. While the sample representing some of the transition states was small, the opportunity to conduct this comparison was valuable. Findings demonstrated few differences based on reason for transition, with chronic stress the most common difference, and likely a reflection of the nature of the measure. Further evidence indicated that for all ex-caregivers there was a tendency for psychological recovery but physical wear and tear. However, these patterns were predominantly due to age effects rather than the specific impact of caregiving.
For psychological wellbeing, there was some evidence of a decline in the year immediately after transition; based on previous findings (Kellett, 1999) it seems that this pattern may relate to guilt, a sense of letting a loved one down, doing the one thing their partner asked them not to do, or concern at the nature of care provided in RAC. However, wellbeing improved as the time since transition increased, reflecting possible relief, more time for themselves, or an opportunity to ponder their experience and find value in their efforts (Kinney & Stephens, 1989; Large & Slinger, 2013). Specifically, ex-caregivers demonstrated greater positive affect and mastery, and less stress, negative affect and depression over time, reflecting findings of other studies (Infurna et al., 2013). Perhaps the lessons learned by caregivers through their career lead to the strength and courage to face challenges. The findings may also support the notion of eustress, described as positive responses to stressors (Lazarus, 1966; Le Fevre, Kolt, & Matheny, 2006). For many, caregiving is a privilege, offering new challenges, chances to learn unique skills, providing drive and direction (Pallant & Reid, 2013).
In relation to physical wellbeing, findings consistently illustrated declining health among ex-caregivers. This wear and tear may be the result of a long term role with little respite, a lack of resilience, an accumulation of stress, prior health history, or limited self-care resources (George & Gwyther, 1986; Schulz et al., 1997; Utz, Caserta, & Lund, 2011). In general, as results suggested that physical wellbeing declines, while psychological wellbeing improves, a sophisticated future consideration of the theories of recovery and wear and tear would need to involve direct examination of specific outcomes and the covariates that may affect them. That is, the reality of caregiver outcomes may be a case of feeling better but doing worse.
Interestingly, the psychological ‘recovery’ for ex-caregivers was largely explained by age. The notion of ‘wellbeing’ refers not only to an absence of sickness but also the presence of optimal health and functioning over a range of domains (Gerrig, Zimbardo, Campbell, Cummings, & Wilkes, 2009). This finding therefore perhaps illustrates a case of ‘positive’ ageing, with evidence that despite stereotypes, older adults can and do show improvements on psychological variables (Duggleby, Swindle, Peacock, & Ghosh, 2011; Ranzijn, 2002). The role of age does suggest that this chance to reflect on achievements and life post-transition may be relevant to older adults generally and should be encouraged. It must be acknowledged, however, that most of the decline in physical wellbeing was also accounted for by age rather than the transition from the role. Declines in physical wellbeing are common with age, and come on top of the debilitating effects of the physical tasks associated with caregiving (Kiecolt-Glaser & Glaser, 1994). In this light, future research should attempt to extricate caregiving factors from age-related issues for an improved understanding of the mechanisms of recovery versus wear and tear.
The results consistently showed few differences in the pattern of outcomes based on reason for transition. While there are indications of changes in wellbeing post-transition, it seems they are a result of the change itself rather than the specific reason for the transition. Strategies to support ex-caregivers, therefore, implemented during this phase, could be of great benefit regardless of the reason for transition. This was reinforced in a recent randomised controlled trial in which spouse dementia caregivers were provided with counselling during their care recipient's move to RAC. Results indicated that offering individual, family or ongoing telephone counselling and regular support groups significantly reduced caregiver burden and depression at the time of transition and in the long term (Gaugler, Roth, Haley, & Mittelman, 2008). Similarly, Schulz, Hebert, and Boerner (2008) recommended providing support for caregivers prior to the care recipient’s death. Gaugler, Mittelman, Hepburn, and Newcomer (2012) emphasised the need to consider who is at risk of negative outcomes post-transition and specifically tailor supports to this cohort rather than assuming that all caregivers will benefit. Based on the current research, perhaps there is value in this idea of addressing risk and taking into account ex-caregivers’ age and baseline wellbeing.
Additional practical solutions and support for ex-caregivers during transition may come in the form of continuing welfare payments, grief counselling, and education about available resources. Currently, the Australian Government ceases caregiver support payments after the care recipient has been in respite for 63 days (Department of Human Services, 2012b), or seven fortnights after bereavement (Department of Human Services, 2012a). Yet this study has illustrated that it may be two years before an ex-caregiver ‘recovers’. Further, it is important that RAC staff members are aware of what the ex-caregiver might be experiencing as it is often the dyad that requires ongoing attention and support (Pallant & Reid, 2013). Similarly, the pattern of rapidly declining service use is an area in need of improvement. As noted by Duggleby, Swindle, Peacock, and Ghosh (2011) caregivers who seek information and assistance to deal with transitions report higher quality of life. It therefore needs to be determined why ex-caregivers no longer use services or whether there are services better suited to their needs, and/or whether this cohort knows about the supports available to them. Perhaps new technologies may enable better provision of support. Finally, while declining health seemed to be a reflection of age, attending to physical wellbeing via health promotion activities while caregivers remain in the role may delay the progression of physical illness (Utz et al., 2011).
While age was responsible for much of the change in wellbeing, there are likely to be additional factors at play. The conflict between results supporting recovery and those indicative of wear and tear may be a function of operational definitions and methodological choices, palliative care experiences, relationship with the RAC facility, or an individual’s experience of non-caregiving related stressors, as discussed in previous research (Gaugler et al., 2007). Additionally, a key factor likely to affect bereaved and relinquished ex-caregivers is grief. While anticipatory grief is influential for both groups, it is bereaved ex-caregivers who most commonly manifest ‘complicated’ or ‘prolonged’ grief reactions. Overlap between grief and depression is commonly acknowledged in the literature with both seemingly worse immediately post-transition (Maciejewski, Zhang, Block, & Prigerson, 2007; Middleton, Raphael, Martinek, & Misso, 1993). This may have affected the outcomes noted for the current participants. Further, there is the potential that patterns of ex-caregiver wellbeing may have been influenced by confounds such as pre-transition experience, advanced care directives and relationships with the RAC facility or staff (Gaugler, Leitsch, Zarit, & Pearlin, 2000; Mullin, Simpson, & Froggatt, 2013), none of which were explicitly explored in this research but should be considered in future studies.
Some researchers suggest that it can be difficult to determine reasons for and emotions around relinquishment in a retrospective manner as the stressful nature of the decision will lead to rationalisation of the choice made (Zarit & Whitlatch, 1992). Bond and Clark (2002) also described the difficulty cross-sectional studies have in only being able to explore the decision and antecedents at one time point instead of examining their dynamic form. One of the potential shortcomings of the current study is common in research of this nature, that is, the effect of time. Previous research has suggested that including participants who are six months post-transition is effective in reducing the likelihood of acute reactions to the event confounding results (Gräsel, 2002; Lieberman & Fisher, 2001). In the current study, recent ex-caregivers may have been 1 month or 11 months post-transition at the time of interview, which could influence findings. Future research may benefit from accounting for both time in and time out of the role in post-transition investigations. Further, the longitudinal nature of this study allowed the caregivers to act as their own controls by applying the synthetic cohort design (Campbell & Hudson, 1985). However, while this approach was able to maximise the available sample, it could possibly have led to the impact of significant environmental events being overlooked, such as the introduction of caregiver financial incentives (e.g. Department of Human Services, 2012a, 2012b).
Conclusion
The availability of longitudinal data which included the experiences of ex-caregivers provided the opportunity to assess both the effect of transition on wellbeing and whether the reason for transition had an impact on outcomes. Transitioning from the caregiver role ostensibly involves the lifting of a burden and literature indicates that wellbeing will improve. However, more recent studies have suggested that wear and tear resulting from the chronic stress of caregiving is associated with ongoing health problems. When assessed in the current research there was evidence of wear and tear for physical wellbeing but recovery over time on measures of psychological wellbeing, though much of this change was attributable to age effects. Additionally, there is limited research comparing ex-caregivers based on their reason for transition, defined in this research as ‘relinquished’, ‘bereaved’, or ‘dual transition’. Results suggested that the act of transitioning itself has the greatest impact on wellbeing, rather than the reason for the transition. These findings are valuable for framing both future research and informing future practice in terms of supports for ex-caregivers.
Footnotes
Acknowledgements
The authors wish to acknowledge the significant contribution to this project by the late Dr Michael S Clark.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Alzheimer’s Association (USA); Ian Potter Foundation; Australian National Health and Medical Research Council; Flinders University Faculty of Health Sciences; and Flinders Medical Centre Foundation.