
Abstract
Background
There are a number of therapies currently available to assist healthcare professionals and carers with non-pharmacological treatment for people living with dementia. One such therapy that has been growing in clinical practice is doll therapy. Providing dolls to some people living with dementia has the potential to enhance personal well-being through increased levels of communication and engagement with others. Despite its potential for benefits, the practice is currently under-developed in healthcare literature, probably due to varied ethical interpretations of its practice.
Aim
To undertake a critical review of the published literature on doll therapy, using the Critical Appraisal Skills Programme Checklist (CASP) tool, in order to determine the potential benefits and challenges of this therapy for people living with dementia.
Design
A comprehensive literature search, incorporating the CINAHL, Medline, Embase, PubMed, Joanna Briggs, Cochrane Library and PsycINFO data bases, was conducted.
Conclusions
Despite many commentaries and anecdotal accounts of the practice, this review identified only 11 empirical studies that were eligible. The majority of studies found that the use of dolls could be therapeutic for some people living with dementia by reporting increased levels of engagement, communication and reduction in episodes of distress. Some studies identified limitations to the therapy including; confusion over the ownership of the doll and healthcare professional uncertainty about issues pertaining to autonomy.
Relevance to clinical practice
According to this review, doll therapy has the potential to increase the well-being of some people living with dementia. This review illuminates that some healthcare professionals feel uncomfortable about its use in clinical practice. The operationalisation of doll therapy in clinical practice has been shown to be inconsistent with different approaches to the practice being advocated. This highlights the need for further empirical research to identify best practice and education to increase awareness in both healthcare professional and carer populations.
Keywords
Introduction
The number of people living with dementia is increasing globally. Indeed conservative estimates suggest that the number of people affected will increase almost three fold, from 40 million to 115 million people (Alzheimer’s Disease International, 2012). Due to the clinical manifestations of dementia (which can include communication difficulties, distressed behaviours, despondency, withdrawal and anxiety), there has been a plethora of research around therapies and non-pharmacological interventions that can serve to increase the autonomy and well-being of those people living with dementia (Downs & Bowers, 2008).
The therapeutic use of dolls has been one such technique that has been growing in clinical practice over the last number of years. This therapeutic use of dolls, which is widely known as doll therapy, is usually led by the person living with dementia and includes behaviours like holding, talking to, feeding, cuddling or dressing the doll (Mitchell, 2014). Providing a baby doll seems to have the potential to greatly enhance the well-being of some people who are living with dementia (Gibson, 2005). This enhancement of well-being has been described as: increased engagement with others, increased dietary intake, improvement in communication and a reduction in anxiety (Mitchell & Templeton, 2014). These benefits to well-being have been supported by a range of anecdotal evidence (i.e. authors who have written on personal experiences of doll therapy for people living with dementia, but not carried out empirical investigation) and this includes work by Heathcote and Clare (2014), Moore (2001) and Verity (2006).
It has been postulated that the rationale for these improvements in well-being are associated with attachment needs. Many commentators have attributed John Bowlby’s work on attachment theory (Bowlby, 1969) as the central rationale as to why doll therapy has the potential to be therapeutic for people living with dementia (Mitchell & O’Donnell, 2013; Stephens, Cheston, & Gleeson, 2013). Attachment has long been identified as a key psychological need for people living with dementia due to the new challenges, anxiety and uncertainties that are faced as a result of advancing disease (Kitwood, 1997; Miesen, 1993). Interestingly, Bowlby’s conceptual work on attachment theory was originally focused on child populations (Bowlby, 1969). In actual fact it was Bere Miesen (1993) who first applied attachment theory to people living with dementia. Miesen (1993) surmised that parent fixation, or the way some people living with dementia continually search for their parents, is an expression of an attachment need. This searching behaviour was perhaps evidence that the person living with dementia was in an unknown, insecure environment and sought reunion with a family in order to feel safe. If attachment needs are not met in times of anxiety or uncertainty, there is potential for that person to see their level of well-being diminish and in turn lead to distress (Kitwood, 1997; Miesen, 1993).
The theoretical underpinnings of doll therapy borrow the idea of attachment from Bowlby (1969) and the application of this to people living with dementia by Miesen (1993). With attention to the ‘doll’, the theoretical work of Winnicott (1953) is also utilized (Bisiani & Angus, 2013; Mitchell & O’Donnell, 2013). Winnicott (1953), again basing his psychological theory on child populations, noted that a ‘transitional object’ is sometimes used by children when they are separated from their parents as it enables them to feel a greater level of security in an uncertain environment (Loboprabhu, Molinari, & Lomax, 2007). Winnicott (1953) suggested that soft toys, blankets or even repetitive behaviours or phrases were used by children as a transitional object during times of uncertainty. The work of Bowlby (1969), Miesen (1993) and Winnicott (1953) then provide some theoretical underpinnings that are useful when considering how doll therapy can support people living with dementia.
A major limitation in using these theoretical underpinnings to understand doll therapy is undoubtedly in their application to child populations. An alternative theoretical lens that has been considered for people living with dementia is the concept of personhood, which incidentally has as its core an emphasis on promoting attachment. Kitwood (1997) was an early champion with regards to promoting personhood in people living with dementia. Personhood is defined by Dewing (2008) as being the different parts of human beings that make them a person. With regards to people living with dementia personhood is arguably more concealed due to the clinical manifestations of the disease (Nolan, Davies, Brown, Keady, & Nolan, 2004; Smebye & Kirkevold, 2013). As a result of these clinical manifestations, Kitwood (1997) famously warned that people living with dementia were at a greater risk of having their personhood eroded. This erosion was said to be perpetuated by, what Kitwood (1997) termed as, Malignant Social Psychology. Kitwood (1997) theorised that Malignant Social Psychology would not only reduce the personhood of a person living with dementia, but also increase stigmatisation associated with the disease. Importantly Kitwood listed a number of depersonalising tendencies associated with Malignant Social Psychology, one of which was infantilisation, or treating people living with dementia like they were children. When considering the therapeutic use of dolls for people with dementia, it is pertinent that it is distinguished and differentiated from forms of play therapy which are associated with child populations. This differentiation is particularly important when considering, not only the therapy itself which will always have the potential to infantilise if not supported appropriately, but also the sparse theoretical underpinnings to its use in practice, which were firstly borrowed from child psychology prior to in-depth empirical investigation.
While some may argue that providing a doll to a person living with dementia has the potential to infantilise (Boas, 1998; Cayton, 2001; Salari, 2002), there is evidence to suggest that if this therapy is understood, developed and utilised correctly, that it has the potential to recapture the personhood of individuals who are living with dementia. This assertion is based on Kitwood’s (1997) ideology of Positive Person Work, bioethical considerations (Mitchell & Templeton, 2014) and the very ethos of person-centred care (McCormack & McCance, 2010). When considering the work of Professor Tom Kitwood (1997), Malignant Social Psychology is juxtaposed to Positive Person Work. While Malignant Social Psychology has the potential to undermine personhood, Positive Person Work has the potential to build personhood when considering the person living with dementia. Positive Person Work corresponds to types of interaction that people living with dementia should be supported to have and include play, facilitation and validation (Kitwood, 1997). These positive interactions have the potential to occur during therapeutic engagement with dolls. With regards to play, which is differentiated from child’s play, Kitwood (1997) suggests that people living with dementia should be supported to spontaneously express themselves by carrying out activities with no specific directed goal. In addition to this, Kitwood (1997) states that appropriate play therapy in dementia care should be led by the person because it has the potential to facilitate spontaneity and self-expression. When considering facilitation, Kitwood (1997) encouraged formal and informal caregivers to enable those living with dementia to do what they were otherwise not able to do. Facilitating therapeutic engagement with dolls has been suggested as fulfilling a maternal need for some people with dementia (Heathcote & Clare, 2014). Validation may also be important as it has been noted that a number of people living with dementia who engage with the doll therapy believe their doll to be a living baby for whom they care (Mitchell & O’Donnell, 2013). If these experiences with the doll are validated, Kitwood (1997) states that the results can help the person living with dementia to become more connected with others and their life can be more meaningful.
When considering the bioethical principles associated with doll therapy for people living with dementia, Mitchell and Templeton (2014) noted the importance of autonomy and beneficence. Importantly, they advocated that the rights of a person living with dementia should be upheld and so if the person living with dementia made the decision to engage with a doll they should be afforded this right (Mitchell & Templeton, 2014). If the effects of doll therapy were therapeutic, for example, increased dietary intake, improved communication, reduction in episodes of distress (Mitchell, 2014), then the principle of beneficence was fulfilled. With these in mind, Mitchell and Templeton (2014) were among the first authors to assert that doll therapy could be a person-centred approach to care.
Person-centred care is an approach that places an importance on the development of the therapeutic relationship between the patient and healthcare professionals (McCormack & McCance, 2006, 2010). This approach to care is not only underpinned by mutual respect for the patient as a person, but also as an approach that seeks to consider the person’s holistic needs as opposed to previous medical models of care (Edvardsson, Sandman, & Borell, 2014; Hill, Roberts, Wildgoose, Perkins, & Hahn, 2010; Sidani & Fox, 2014). Through collaboration and negotiation with people living with dementia and their care partners, healthcare professionals are able to facilitate shared decision-making about care, which may or may not include doll therapy. Importantly, a doll should not be forced on a person living with dementia, instead healthcare professionals should facilitate the person in making a choice, for example leaving the doll in a communal area or asking the person if they would like to hold the doll. According to Mitchell and Templeton (2014), the decision to engage with dolls is considered as a non-complex decision, vis-à-vis even if a person is living with late-stage dementia they should still be able to make this choice. Note, this non-complex decision-making is different to complex decision-making which is usually made by a multi-disciplinary healthcare team and the next-of-kin with the person’s best interests in mind, for example decision-making about medical interventions. The decision of whether or not to engage with doll therapy should therefore always be with the person, or if this is not possible, with the person in mind.
Aims
To undertake a critical review of the published literature on the therapeutic use of dolls in order to determine the potential benefits and challenges of this therapy for people living with dementia.
Rationale for review
As illustrated, therapeutic engagement with dolls has the potential to be beneficial to the well-being of people living with dementia. This is coupled with the fact that the therapy is also cost-effective. Despite these perceived micro and macro benefits there has been a paucity of empirical investigation on the therapeutic use of dolls for people living with dementia. There are also a number of theories, ranging from child psychologies to person-centred psychologies, which have been used interchangeably to describe the reasons for its effectiveness. The paucity of clinical guidelines and associated ethical tensions provide a strong rationale for carrying out this review.
On review of the existing evidence base, it would also appear that no reviews of the literature have been carried out on doll therapy for people living with dementia. This review will serve to support healthcare professionals to understand the potential benefits and disadvantages of doll therapy identified from empirical evidence. In addition to this, the review will also demonstrate how doll therapy has been utilised in different clinical settings to date.
Methods
Search strategy
A comprehensive search of the literature was carried out in April 2014 using the following terms: dementia, Alzheimer’s Disease, people with dementia, doll therapy, doll, soft toy, baby doll, play therapy and residential care institutions. These terms were used in the following databases: CINAHL, PsycINFO, Medline, Embase, Internurse, Cochrane Library, Joanna Briggs Institute, PubMed and NHS Evidence.
Inclusion criteria and exclusion criteria
There is a paucity of empirical evidence on the phenomenon of doll therapy for people living with dementia. As a result there were minimal exclusions applied to this review, except those studies that were not written in English language, those studies that were not carried out with people who are living with dementia and those which were not empirical. During the searching stage of this review, it was found that Fernandez, Arthur, and Fleming (2013) have published a systematic review protocol on the effect of doll therapy in managing behaviours that challenge in people living with dementia. This review has not yet been completed and appears to have a primary emphasis on measuring behaviour change, like ‘agitation, verbal aggression and physical aggression’, through validated scales. The purpose of this review differs as it seeks to not only explore the benefits and challenges of doll therapy for people living with dementia within a practice context, which consequently will take into account factors associated with well-being and ill-being and in turn may include what Fernandez et al. (2013) term agitation, verbal and physical aggression’, but also explore additional factors related to theoretical underpinnings and bioethics. Figure 1 provides an overview of the results from the search strategy that found 11 studies eligible for inclusion.
Results from the search strategy.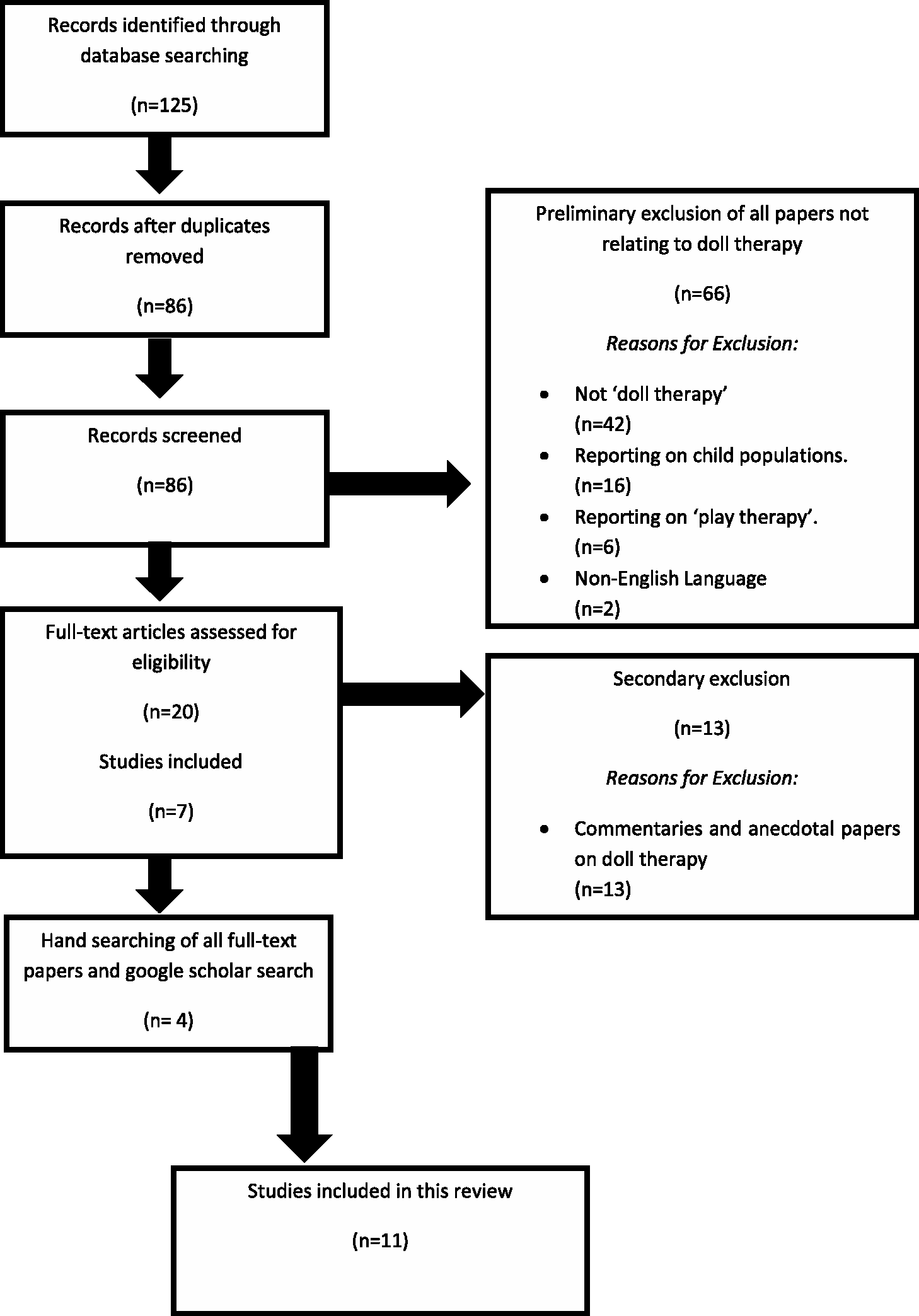
Study characteristics
Study setting
Over half of the included studies were carried out in the UK. Six studies were carried out in England and one in Scotland. In addition to this, two studies were carried out in the USA, while one study was identified in Japan and one in Australia. It is also interesting to note that, five studies (Alander, Prescott, & James, 2015; Ellingford, Mackenzie, & Marsland, 2007; Fraser & James, 2008; James, Mackenzie, & Mukaetova-Ladinska, 2006; Mackenzie, James, Morse, Mukaetova-Ladinska, & Reichelt, 2006) were carried out by personnel from the same centre, the Newcastle Challenging Behaviour Service (UK). This concentration of studies in the United Kingdom may raise some questions over generalisability.
The settings for the included studies, which incorporated people living with dementia, were most often long-term care facilities or nursing homes (Bisiani & Angus, 2013; Cohen-Mansfield, Thein, Dakheel-Ali, Reiger, & Marx, 2010; Ellingford et al., 2007; James et al., 2006; Mackenzie et al., 2006; Stephens et al., 2013; Tamura, Nakajima, & Nambu, 2001). Only two studies investigated doll therapy within a hospital setting (Green et al., 2011; Minshull, 2009).
Research design
The majority of studies sought to investigate the phenomenon of doll therapy through observational data collection of people engaging with doll therapy (Bisiani & Angus, 2013; Cohen-Mansfield et al., 2010; Green et al., 2011; Stephens et al., 2013; Tamura et al., 2001). Four studies sought to examine healthcare professional perceptions on the use of doll therapy through the administration of questionnaires (James et al., 2006; Mackenzie et al., 2006) and semi-structured or focus-group interviews (Alander et al., 2015; Fraser & James, 2008). The one remaining study conducted a retrospective analysis of case notes pre and post-doll therapy (Ellingford et al., 2007).
Sampling
Across the 11 included studies a total of 448 people living with dementia and 49 healthcare professionals were recruited (n = 497). It should be noted that the study conducted by Cohen-Mansfield, Thein, Dakheel-Ali, Reiger, and Marx (2010) examined the impact of different stimuli (one of which was doll therapy) for people living with dementia. It is the only study that is included in the review that does not explicitly evaluate doll therapy and included 193 people living with dementia which is almost half of the participants of this review. In relation to the number of participants in this review, the mode was 14 participants, the median was 14 participants and the mean number of participants was 45. Seven of the eleven studies included in this review were conducted with 16 participants or less (Alander et al., 2015; Bisiani & Angus, 2013; Fraser & James, 2008; James et al., 2006; Mackenzie et al., 2006; Minshull, 2009; Stephens et al., 2013; Tamura et al., 2001). There were no studies that sought to investigate the phenomenon from the perspective of care partners (relatives or informal carers).
Summary of included studies.

Study appraisal
All studies included in this review were appraised using the Critical Appraisal Skills Programme Checklist (CASP), which was developed in the United Kingdom. Based on the checklist questions, each study was given a score and placed into the category of low, medium or high quality. With regards to this review, seven studies were deemed to be high quality (Alander et al., 2015; Bisiani & Angus, 2013; Cohen-Mansfield et al., 2010; Fraser & James, 2008; James et al., 2006; Mackenzie et al., 2006; Stephens et al., 2013), one study was medium quality (Tamura et al., 2001) and three were low quality (Ellingford et al., 2007; Green et al, 2011; Minshull, 2009). With regards to the lower quality studies, the rationale for this scoring was mostly due to limited details about methodological approach. It is worth acknowledging that the three lower quality studies included 190 participants of the 497 participants included in the review, which is almost 40%. It is also worth highlighting again that, while Cohen-Mansfield et al. (2010) were judged to have a high quality study based on the CASP, their study used a variety of stimuli interventions, which included dolls, and this accounted for almost 40% (193 participants). In total then, there were 101 participants (20%) included in this review, which were deemed to be high quality and concentrated solely on the use of doll therapy.
Findings
Benefits of doll therapy
All studies included in this review clearly articulated a number of benefits that were associated with doll therapy. The most commonly reported benefit was improvement in communication between the person living with dementia and other residents or care staff (Alander et al., 2015; Bisiani & Angus, 2013; Ellingford et al., 2007; Fraser & James, 2008; James et al., 2006; Mackenzie et al., 2006; Minshull, 2009; Stephens et al., 2013; Tamura et al., 2001). The use of dolls gave people living with dementia a means to engage with care staff or residents. In the study by James, Mackenzie, and Mukaetova-Ladinska (2006), it was reported that a group of women who engaged with their dolls began to sit together and connect as a group. James et al. (2006) reported that this group began what was affectionately known as the ‘mother’s group’ (p. 1095). In addition to this, Minshull (2009) reported that some of her participants actually began to better articulate their language and as a result express themselves more clearly to others. In one example, Minshull (2009) recalls how one particular person living with dementia was ‘normally incoherent in speech’ (p. 37) pre-doll therapy. Post-doll therapy Minshull (2009) reported that this same person was able to better articulate their language through the doll by communicating phrases like “baby…tickle her toes…oh pretty colours [regarding doll’s pink cardigan]” (p. 37). The re-establishment of these communication channels is arguably essential when considering the therapeutic relationship between the person living with dementia and healthcare professionals. This notion was supported in the findings of Fraser and James (2008) who conducted semi-structured interviews with healthcare professionals, which included representation from nursing, psychology, occupational therapy and psychiatry. Fraser and James (2008) identified communication as an important theme as healthcare professionals were able to establish new communication channels with people in their care. Fraser and James (2008) proposed that healthcare professionals could frequently use the doll as a starting point for communication and even talk to the doll and the person living with dementia as means of further developing the therapeutic relationship.
While improvements in communication were important, other activities of daily living were shown to be enhanced through engagement with dolls (Roper, Logan, & Tierney, 2000). Considering maintenance of a safe environment, many studies reported reductions in distressing behaviour experienced by people living with dementia (Bisiani & Angus, 2013; Fraser & James, 2008; James et al., 2006; Mackenzie et al., 2006; Stephens et al., 2013). This distressing behaviour has been mainly described in the literature as: agitation, wandering, anxiety, despondency and disengagement from others. During a single case-study on the phenomenon, Bisiani and Angus illustrated how one resident’s (Mary) previous daily experiences of “trying to leave the facility and asking for attachment/child were all together eradicated” by doll therapy (p. 456). This was supported by the work of Green et al. (2011), who noted that prescription of certain anti-psychotic medications was reduced in populations who engaged with dolls.
An improvement in dietary intake, or the activity of eating and drinking, was also identified as a potential benefit of doll therapy (Bisiani & Angus, 2013; Mackenzie et al., 2006; Stephens et al., 2013). This increased dietary intake was as a result of a better dining experience (as the doll provided immediate company) and increased awareness about food (as the person would sometimes give their own doll food). The studies in this review also found that residents who were previously reluctant to be assisted with elimination and washing/dressing needs, were more approachable when engaging with a doll (Bisiani & Angus, 2013; Fraser & James, 2008; James et al., 2006; Mackenzie et al., 2006; Stephens et al., 2013). The rationale behind this was related to the calming affect that the doll appeared to have on users. Indeed, through analysis of questionnaires administered to healthcare professionals, Mackenzie, James, Morse, Mukaetova-Ladinska, and Reichelt (2006) found that the most common change in ‘emotional status’ observed in people engaging with doll therapy was that of being ‘calmer’ (p. 443).
Finally, benefits associated with working and playing, sleeping and mobilisation were also described in the literature. According to the findings of this review, therapeutic engagement with dolls has given rise to a number of behaviours including touch, cradling, cuddling, kissing, carrying, talking and singing (Alander et al., 2015; Bisiani & Angus, 2013; Cohen-Mansfield et al., 2010; Ellingford et al., 2007; Fraser & James 2008; James et al., 2006; Mackenzie et al., 2006; Minshull, 2009; Stephens et al., 2013; Tamura et al., 2001). These behaviours are most perceived as therapeutic and fulfilment of behaviour associated with play. However, as illuminated by Bisiani and Angus (2013), some people who engage with doll therapy are also meeting working needs. For example, Mary was observed to be asking healthcare professionals to ‘babysit’ when she had other tasks that needed to be carried out (p. 456). Improvement in the quality of sleep was another benefit identified by two studies in the literature (Bisiani & Angus, 2013; Stephens et al., 2013). Presumably, a person with dementia (with increased general well-being as a result of doll therapy), is more likely to settle into a better quality of sleep; however this was poorly explored in the evidence. Interestingly one study (Bisiani & Angus, 2013) even identified better mobilisation of a resident (Mary, the resident living with a dementia observed in their single case-study). This was attributed to reduction in episodes of anxiety that manifested as hyper-ventilation and tremors (which had previously been so severe that they had caused falls). Figure 2 provides an overview of the reported benefits of doll therapy.
Reported benefits of doll therapy (based on all of the empirical studies identified in this review).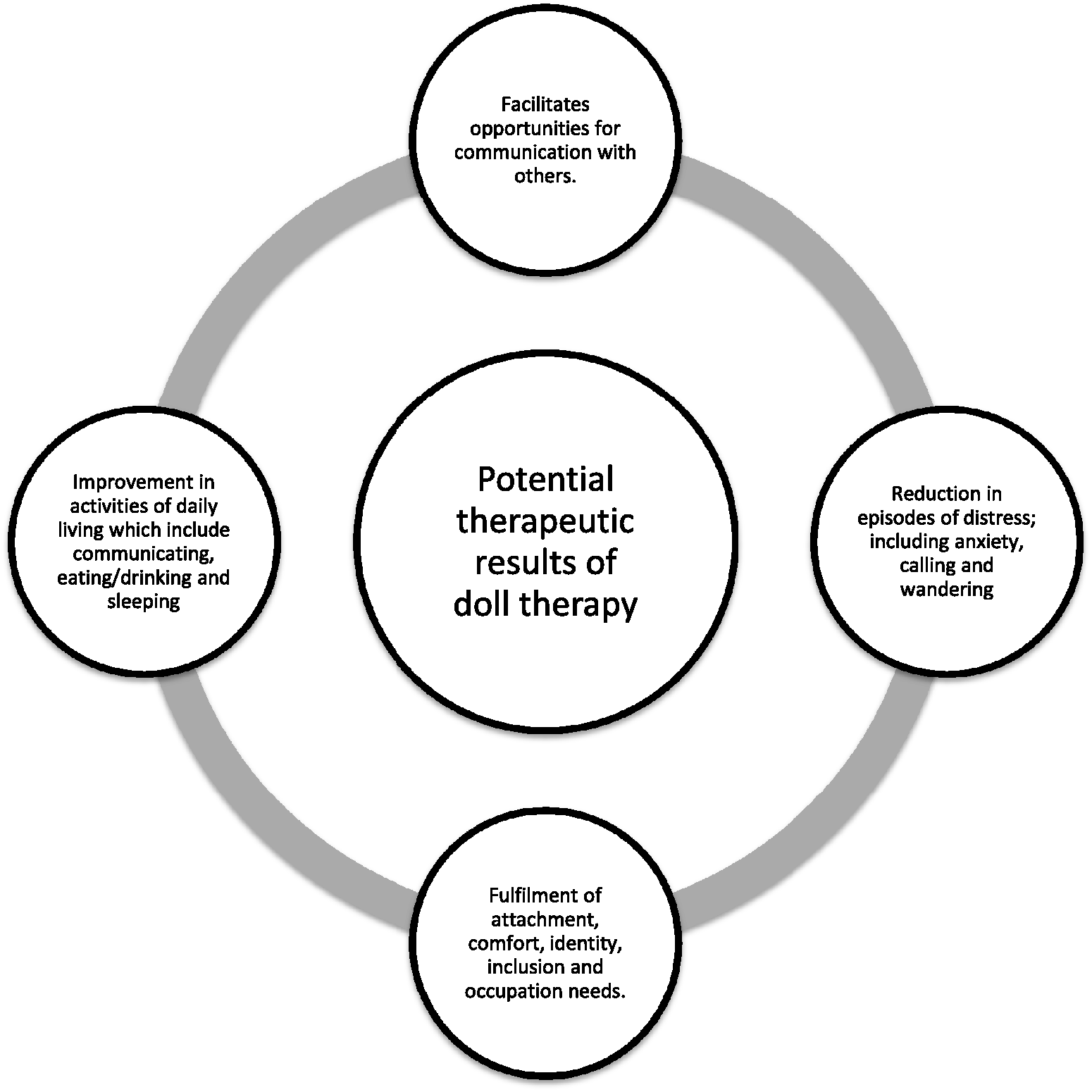
Potential challenges of doll therapy
While there were a number of benefits that were associated with doll therapy, a number of challenges were also identified. According to this review, the therapeutic use of dolls for people living with dementia was approached in two main ways, either as an intervention or a therapy. In the case of an intervention, which corresponds to dolls being offered to people for a set period of time, this was less common (Cohen-Mansfield et al., 2010; Minshull, 2009; Tamura et al., 2001). Naturally, these studies could not assess the long-term impact of dolls in the way that the other studies could. The therapeutic engagement of dolls was deemed as a ‘therapy’ when it was provided to people living with dementia over a longer period of time (i.e. months-permanent). As a long-term ‘therapy’, healthcare professionals were not required to engage directly with the doll therapy (i.e. people living with dementia used the dolls without direction) (Alander et al., 2015; Bisiani & Angus, 2013; Ellingford et al., 2007; James et al., 2006; Mackenzie et al., 2006; Stephens et al., 2013). This was in contrast to the interventional studies, where healthcare professionals guided or led people living with dementia, on how to use the dolls. These differing approaches raise questions about how best to operationalise doll therapy in practice.
Considering the person living with dementia, there were a number of studies identified in this review that reported limitations with regards to doll therapy. While it has already been reported that doll therapy has clear benefits associated with its use, some studies have noted its effect is not always long-term. Indeed the findings suggest that some of the people who engaged with dolls appeared to lose interest in the activity over a sustained period of time (Stephens et al., 2013; Tamura et al., 2001). Ironically, while one of the key attributes of doll therapy was reduction in distressing behaviour, there were some instances where doll use caused distress for people living with dementia (Alander et al., 2015; Bisiani & Angus, 2013; James et al., 2006; Mackenzie et al., 2006; Stephens et al., 2013). In particular, people who engaged with dolls could become possessive of their doll and refuse to be parted from it (James et al., 2006; Stephens et al., 2013). This possessive behaviour can manifest as either desirable, because the person living with dementia has forged a therapeutic attachment with their doll, or undesirable, because the person can become distressed if they are separated from their doll.
Healthcare professional attitudes were found to be a potential barrier to engagement with doll therapy (James et al., 2006; Mackenzie et al., 2006; Minshull, 2009). In the study carried out by Mackenzie et al. (2006), the authors found, through use of questionnaires, that some people thought the use of dolls was “babyish…demeaning…patronising…inappropriate” (p. 442). These attitudes were observed in practice through the work of Minshull who noted that during her doll therapy intervention, “nursing assistants were sniggering” (p. 37). Interestingly, the authors who identified staff scepticism as a potential issue appeared to correct this through education (Mackenzie et al., 2006; Minshull, 2009). Administration of literature, information sessions and on-the job experience were shown to increase healthcare professional awareness and practice with doll therapy.
Emerging theoretical underpinnings
As alluded to, there have been some scant theoretical underpinnings as to how doll therapy can enhance the well-being of people living with dementia based on the theories of attachment and person-centred care. Two studies identified in this review have produced comprehensive explanatory models based on grounded theory methods that are significant in relation to emerging theory on doll therapy (Alander et al., 2015; Fraser & James, 2008). Fraser and James (2008) developed a model, based on empirical investigation, to assist practitioners in understanding the rationale for improvement in well-being for people living with a dementia who engage with dolls. Fraser and James (2008) acknowledged the importance of attachment in their model, but importantly recognised there were a number of other equally pivotal factors which included; inclusion, comfort and identity. Importantly these factors directly correspond with what Kitwood determined were the fundamental needs of the person with dementia (Kitwood, 1997).
In addition to these factors, which correspond directly to previous theory on doll therapy, Fraser and James (2008) reported emerging factors which relate to activity, innate drivers and memories. Doll therapy could offer an opportunity for people living with a dementia to engage in meaningful activity and as a result provide people living with a dementia with a sense of purpose, examples of this may include nursing, feeding, dressing or singing to the doll). On innate drivers, Fraser and James (2008) found that participants believed that people engaging with dolls were responding to instinct-like behaviours, for example, the innate wish to engage in social contact. Through grounded theory analyses it was also suggested that doll therapy could evoke pleasurable memories for the person living with dementia.
Alander, Prescott, and James (2013) used grounded theory to explore older adults’ views and experiences of doll therapy. This ultimately supplements Fraser and James’ (2008) work, which drew on a healthcare professional group. Alander et al. (2015) found that there were a number of intrapersonal features which directly influenced the well-being of people living with dementia and these included; ownership of a doll, purpose, role and attachment. In addition to these intrapersonal features, Alander et al. (2015) found that there were also a number of external interpersonal factors that could promote a person’s well-being and these included; companionship, communication with others and greater inclusion. Interestingly Alander et al. (2015) note that the majority of older adults involved in this study considered that intra/interpersonal factors were more likely to outweigh any practical or ethical concerns.
In addition to the two studies that sought to generate theory (Alander et al., 2015; Fraser & James, 2008), only two other studies identified in this review made explicit reference about their theoretical underpinnings (Bisiani & Angus, 2013; Stephens et al., 2013). These two studies drew on Bowlby’s attachment theory (1969) and the theory of personhood by Kitwood (1997). Stephens, Cheston, and Gleeson (2013) also utilised Winnicott’s transitional object theory (1953). Interestingly the studies identified in this review that do underpin their research with theory are the more recent, which perhaps illuminates the emerging development of research into doll therapy. Undoubtedly an explicit theoretical foundation is important with regards to doll therapy because, as found in this review, healthcare professionals may be resistive to using the therapy and therefore making the case from a sound theoretical basis is important.
Summary
The findings of these empirical studies have illuminated a number of potential benefits in the use of doll therapy for people living with dementia. In particular, the studies have associated therapeutic engagement with dolls as a means to promote the well-being of people living with dementia, particularly through improvements in activities of living. The empirical studies included in this review provide some insight to potential challenges associated with doll therapy but in less depth when compared to the benefits of the practice. Limited professional awareness about appropriate utilisation of the therapy, problems pertaining to doll ownership and negative pre-existing ideologies about the therapy appear to be the main challenges of the therapy according to the review.
Discussion
There is evidence in the literature to suggest that the use of dolls can provide therapeutic gains for some people living with dementia. The empirical evidence appears to provide some direction on how best to utilise doll therapy. Clear division exists on whether dolls should be used as an intervention or as a therapy and also whether this should be in a nursing home facility or on a hospital ward. The only guidelines that exist on the use of doll therapy were reported by the authors from the Newcastle Challenging Behaviour Service (Mackenzie, Wood-Mitchell, & James, 2007). The authors of these guidelines were best placed to provide these, given their empirical investigation of doll therapy over the past decade (Alander et al., 2015; Ellingford et al., 2007; Fraser & James 2008; James et al., 2006; Mackenzie et al., 2006). Despite their expertise and enterprising work, there are obvious questions pertaining to the transferability of doll therapy to other clinical settings. Ostensibly then, many healthcare professionals associate doll therapy as controversial or contentious (Mitchell, 2014). Yet as evidenced in this review there are a number of people, both healthcare professionals, older adults and people living with dementia who do support its use, largely because of the benefits they have witnessed first-hand (Alander et al., 2015). Unfortunately there was no evidence of how any care partners perceived doll therapy as this group did not make up any of the participants in the review. Empirical research to date has largely focused on the observed well-being of doll therapy and opinions of healthcare professionals. Only Alander et al. (2015), who sought opinions from older adults (some who lived with dementia and some who engaged with doll therapy), has carried out investigation differently. As a result of this, it is difficult to determine how care partners or informal caregivers would perceive doll therapy.
The utilisation of doll therapy in clinical practice is not automatically right or wrong, however if the therapy is practiced or utilised in a meaningful way, it has the potential to be truly person-centred. Person-centred care is underpinned by respect, understanding and an enablement of practices that facilitate self-determination (McCormack, Dewing, et al., 2010; McCormack, Karlsson, et al., 2010). Due to the paucity of literature on doll therapy it is important that knowledge about appropriate practices and underpinning theory is delivered effectively. As demonstrated in this review, one of the key challenges to doll therapy was preconceptions or education of healthcare professionals who are key in enablement of the therapy. The learning culture of a clinical environment is particularly important and McCormack, Dewing, and McCance (2011) assert that any sustained learning will only occur in a supportive context.
The application of doll therapy to the person-centred nursing (PCN) framework, developed by McCormack and McCance (2006, 2010) from their previous work on person-centred practice with older people (McCormack, 2003) and the experience of caring in nursing (McCance, 2003), is particularly useful when considering the contents of this review. McCormack and McCance’s (2010) PCN framework comprises four constructs: pre-requisites, the care environment, person-centred processes and outcomes (McCance, McCormack, & Dewing, 2011; McCormack, Dewing, et al., 2010; McCormack, Karlsson, et al, 2010; McCormack & McCance, 2010; McCormack, Roberts, Meyer, Morgan, & Boscart, 2012). This framework is particularly useful because, as illustrated, the majority of empirical investigation on doll therapy has occurred in care homes and, as such, nurses are the main representative from the healthcare professional group. Nurses are therefore the most likely healthcare professional group to facilitate doll therapy in clinical practice. The PCN can be an effective tool for nurses to operationalise the practice of doll therapy and are considered as follows:
Pre-requisites: This construct focuses on the attributes of the healthcare professional, which should include professional competence, well-developed interpersonal skills and commitment to their role. When considering doll therapy, engagement with dolls can only work if this is facilitated by the healthcare professional. This review has demonstrated that the people living with dementia who are likely to glean benefits from doll therapy must be enabled or empowered by others. As all of these studies were conducted in clinical settings the enablement is likely to be facilitated by a nurse. Care environment: This construct focuses on the context in which care is delivered and should provide organisational systems that are supportive, facilitate a sharing of power between person and nurse and there is potential for innovation and risk-taking. Building upon the previous construct, the care environment should be equipped in a manner to allow nurses to engage with doll therapy. Given the limited, but encouraging, evidence that is on offer, doll therapy might be considered as an innovative approach for some people living with dementia. For those practitioners who are less convinced, the therapy may represent an opportunity of a balanced risk given the potential benefits for the person living with dementia. Person-centred processes: This construct focuses on delivering care through a range of therapeutic avenues that incorporate the person’s (patient) beliefs, values, shared decision-making and the provision of physical care. This construct is also underpinned by sympathetic presence. As demonstrated, doll therapy can facilitate and support person-centred processes because of the potential for improvement in many facets of daily living activities that have been identified in this review. Outcomes: This is the central component of the PCN model and should include outcomes like; satisfaction with care, involvement in care, increased well-being and promotion of the therapeutic environment. Doll therapy has the potential to enhance meaningful engagement with people who are living with dementia and in addition it has the ability to connect with the innate caring quality of the person (i.e. caring for a baby).
Limitations
One factor that was unclear from the empirical studies included in this review was the staging of dementia and the associated benefits from doll therapy. When considering the illness trajectory associated with dementia (Lunney, Lynn, Foley, Lipson, & Guralnik, 2003; Murtagh, Preston, & Higginson, 2004; World Health Organisation (WHO), 2004), there is no obvious stage (for example, in early or late dementia) where engagement with dolls is the most therapeutic. That being stated, given the nature of the findings, it is probably a therapy that is most utilised by people in the middle to late stages of the illness. The consequence of this however, is that there has been no empirical investigation in relation to therapeutic engagement with dolls outside a formalised care setting. When considering the potential benefits and affordability of the therapy, it is surprising doll therapy does not occur at the homes of people living with dementia with facilitation or support from informal caregivers or care partners. As a result, there are no practice guidelines for doll therapy outside a clinical setting.
An area of note that was not overly developed in the literature was in relation to the gender of people who engaged with dolls. While it is probably unsurprising that the vast majority were female, a number of studies documented male engagement with dolls. This perhaps offers an interesting lens of future inquiry because, based on the results of this review, it is unclear if gender alone correlates with levels of engagement or well-being and, in addition, if healthcare professionals perceive any differences with regards to theoretical underpinnings or bioethical principles between men and women. Another limitation identified through this review pertains to the theoretical underpinnings of doll therapy for people living with dementia. From the review, there were inconsistent references to how doll therapy has the potential to enhance the well-being of people living with dementia. Those studies that did underpin their research with theory used attachment, the concept of personhood or a combination of both. Limited reference to theoretical underpinning is understandable given the paucity of research in this area.
In addition it should be also be noted that there have been no randomised controlled trials that have been carried out to assess the efficacy of the therapeutic use of dolls, many of the studies have been conducted in the same geographical areas and, when considering the appraisal of the evidence, there were 101 participants (20% of the overall participants) included in this review, which were deemed to be high quality and concentrated solely on the use of doll therapy for people living with dementia.
Conclusion
The number of people living with dementia who are benefiting from therapeutic engagement with dolls is increasing. While empirical investigation has been limited, there are a number of encouraging results as well as many anecdotal accounts of its success. The results of doll therapy are unique to the person and so it is impossible to predict what benefits a person living with dementia will have, if any, when engaging with a doll but this review suggests improvements in overall communication, engagement with others, dietary intake and general well-being. Despite the growing evidence of potential benefits to people living with dementia, doll therapy is still broached with caution by some. The main challenges to doll therapy appears to due to pre-existing ideas from healthcare professionals who are crucial to enablement of it in practice. These pre-existing ideas are often due to a result of limited education on the therapy and its appropriate application to Positive Person Work (Kitwood, 1997); the bioethical principles of autonomy and beneficence (Mitchell & Templeton, 2014) and most importantly the concept of person-centred care (McCormack & McCance, 2010). While the PCN framework offers a very useful structured approach to facilitating doll therapy in a person-centred way, one must still acknowledge the paucity of high-quality empirical evidence. There is a pressing need for further empirical study so as healthcare professionals can be provided greater evidence for the use of dolls in clinical practice. While any type of empirical investigation would be extremely useful, a pertinent aspect that is missing in this review at present is the voice of the care partner.
Relevance to clinical practice
What does this research add to existing knowledge in gerontology?
This review provides evidence to suggest that therapeutic engagement with dolls can be beneficial to some people living with dementia. The review has highlighted that many healthcare professionals have poor education on the use of dolls for people living with dementia. It demonstrates the lack of robust empirical studies focusing on the effectiveness of doll therapy. What are the implications of this new knowledge for the care with older people?
Some people living with dementia have been supported through doll therapy to maximize their levels of independence and well-being. A number of the activities of daily living were enhanced through use of dolls, particularly communication, eating/drinking, maintaining a safe environment and sleep. Utilisation of doll therapy has the potential to be a person-centred practice. How could the findings be used to influence policy or practice or research or education?
Further empirical research on the phenomenon is particularly pertinent, especially with informal carers and family members. This knowledge should equip healthcare professionals with knowledge and confidence so as to maximize this non-pharmacological, low-risk, cost-effective therapy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.