
Abstract
Fourteen people attending an adult day programme were recruited to a structured horticultural therapy programme which took place over 10 weeks. The effects were assessed using Dementia Care Mapping and questionnaires completed by family carers. High levels of wellbeing were observed while the participants were engaged in horticultural therapy, and these were sustained once the programme was completed. This study adds to the growing evidence on the benefits of horticultural therapy for people with dementia who have enjoyed gardening in the past.
Keywords
Introduction
Living well with dementia is no longer considered as simply optimum care, it is a fundamental human right (Alzheimer Scotland, 2009). The dementia disease trajectories are such that people living with dementia can often experience a reduction in their wellbeing as a result of the disease processes. The development of person-centred practices in dementia care is important in enabling people to ‘live well’ as these serve a dual role in enhancing personhood and diminishing potential episodes of distress (Brooker, 2007; McGreevy, 2016). Pharmacological advances have proved valuable in the arena of dementia care, but there has been a tendency to over rely on their use in practice (Banerjee, 2009). As a result of these currently advocated practices, emphasis is now placed on approaches which are non-pharmacological in orientation (Department of Health, 2001, 2005, 2006, 2009, 2010; National Institute for Clinical Excellence, 2011).
When considering these non-pharmacological approaches to dementia care, it is important to afford personalisation of the specific approach as it is often positively correlated with increased levels of success (Mitchell & Agnelli, 2015a). Often personalisation of non-pharmacological approaches to care comes through knowledge of a person’s life history, which is usually recorded by healthcare professionals in correspondence with the person living with dementia (Baker, 2015). For example, a person living with dementia who used to own a dog may find pet therapy beneficial (Williams & Jenkins, 2008), another who frequently becomes unfamiliar with their surroundings may find reality orientation helpful (Woods, Woods, Aguirre, Spector, & Orrell, 2012) or perhaps a very maternal person may take great pleasure from doll therapy (Mitchell, McCormack, & McCance, 2016).
As illustrated there are many non-pharmacological approaches that have been evidenced to benefit people living with dementia. An emerging approach to supporting people living with dementia that has been flourishing recently is the use of horticultural, or garden, therapy (Blake & Mitchell, 2015). Horticultural therapy enables people living with dementia to spend part of their day in an outside environment. This in itself can promote wellbeing, particularly if the person spends large portions of their day inside (Duggan, Blackman, Martyr, & Van Schaik, 2008). Importantly, reduction in freedom coupled with restricted physical activity may lead to higher levels of distress (Scherder, Bogen, Eggermont, Hamers, & Swaab, 2010). In summary, access to appropriately designed outdoor spaces can lead to enhanced wellbeing, reduction in distress, a potential reduction in developing depression and, given the evidence available on cognitive stimulation, a chance at decelerating the dementia disease (Connell, Sanford, & Lewis, 2007; Pollock, 2012).
With these benefits in mind, it is hardly surprising that the use of horticultural therapy in dementia care has been increasing. Secure therapeutic gardens or outdoor spaces offer people living with dementia a range of potential activities that include gardening, sensory reminiscence, animal care or simply the opportunity to sit, walk or view an environment more natural than that of a nursing home or hospital ward (Blake & Mitchell, 2015; Detweiler et al., 2012; Gonzalez & Kirkevold, 2013).
Service development
Alzheimer Outreach Services of McCormick Home is a community support programme attached to a long-term care home (McCormick Home) serving clients living with dementia and their caregivers. It has been operating since 1985 as a not-for-profit specialized adult day programme located in South-Western Ontario, Canada.
During the 2006 rebuild of McCormick Home, Alzheimer Outreach Services was provided with a generous garden space, designed and landscaped to make it a ‘dementia friendly’ environment based on best practice knowledge available at that time (Gigliotti, Jarrott, & Yorgason, 2004; Schols & van der Schriek-van, 2006). Having used the garden extensively for the past eight years, staff experience indicated that the design could be improved to invite more engagement and independent client involvement in the garden-related activities. The McCormick Home Foundation worked with an architect to design six independent garden flower beds that could be used for a therapeutic garden project for those living with dementia. The independent garden flower beds were designed to be easily accessible for the clients of Alzheimer Outreach Services. The completed outside environment includes a large outdoor pad with two pergolas, an interactive water display, a garden shed and the newly constructed raised garden beds.
This study has examined the new type of garden design combined with recreational programming which promotes more autonomous and robust client engagement in gardening related activities. It was postulated that this could inject more meaningful activity for the clients and in turn result in a sustained enhancement of wellbeing and engagement.
Aim
The aim of this mixed-methods study was to assess if and how day programme providers could increase client engagement in horticultural activities on both physical and emotional level by adopting an improved garden design and recreational programming that is built on client strengths (i.e. interest and past history with gardening) and promote client self-determination compared to more traditional and more staff directed day programme activities.
Methods and data collection
A mixed-methods approach was considered as the best way to carry out this exploratory research project.
First, a validated observational tool was used so as to determine if the person living with dementia was in a state of wellbeing during horticultural therapy. The observational tool used was ‘dementia care mapping’, which is a tool wherein researchers assess apparent wellbeing and engagement in people living with dementia (University of Bradford, 2016). This is achieved by recording a behaviour category code and a score of between −5 and +5 for the person’s level of wellbeing or engagement every 5 minutes (Algar, Woods, & Windle, 2016; Ballard & Aarsland, 2009). In this study, observations were structured and recorded every 5 minutes per participant for 1–2 hours while participants were involved in horticultural therapy.
The rationale for this choice of tool was so as to determine what types of behaviour occurred most often during horticultural therapy and how much participants appeared to enjoy the sessions. The dementia care map was carried out by a continuous member of the research team so as to allow for consistency throughout the map as findings can be subjective. During 15% of the dementia care maps, a second member of the research team carried out separate data collection so as to ensure inter-rater reliability. The inter-rater reliability was between 90 and 98% across these co-observations.
In addition to the dementia care map, the research team also recorded narrative notes based on the horticultural therapy so as to establish what sorts of ‘horticultural’ activities took place and how these appeared to impact on perceived participant wellbeing. This is important so as to enable presentation of thematic findings which can encourage future study replication. The final piece of data collected was through administration of questionnaire to the care partners of the participants so as to determine if horticultural therapy had a lasting impact (i.e. once the person living with dementia left the facility and returned home). The caregiver questionnaire was drafted by the previous director of Alzheimer Outreach Services and mailed to each caregiver to complete for each day their family member attended the garden project. These were sent back at the end of the 10 week programme, and the response rate was 100%.
Prior to recruitment, this study received ethics approval from the research ethics board at the principal investigator’s home institution.
Recruitment
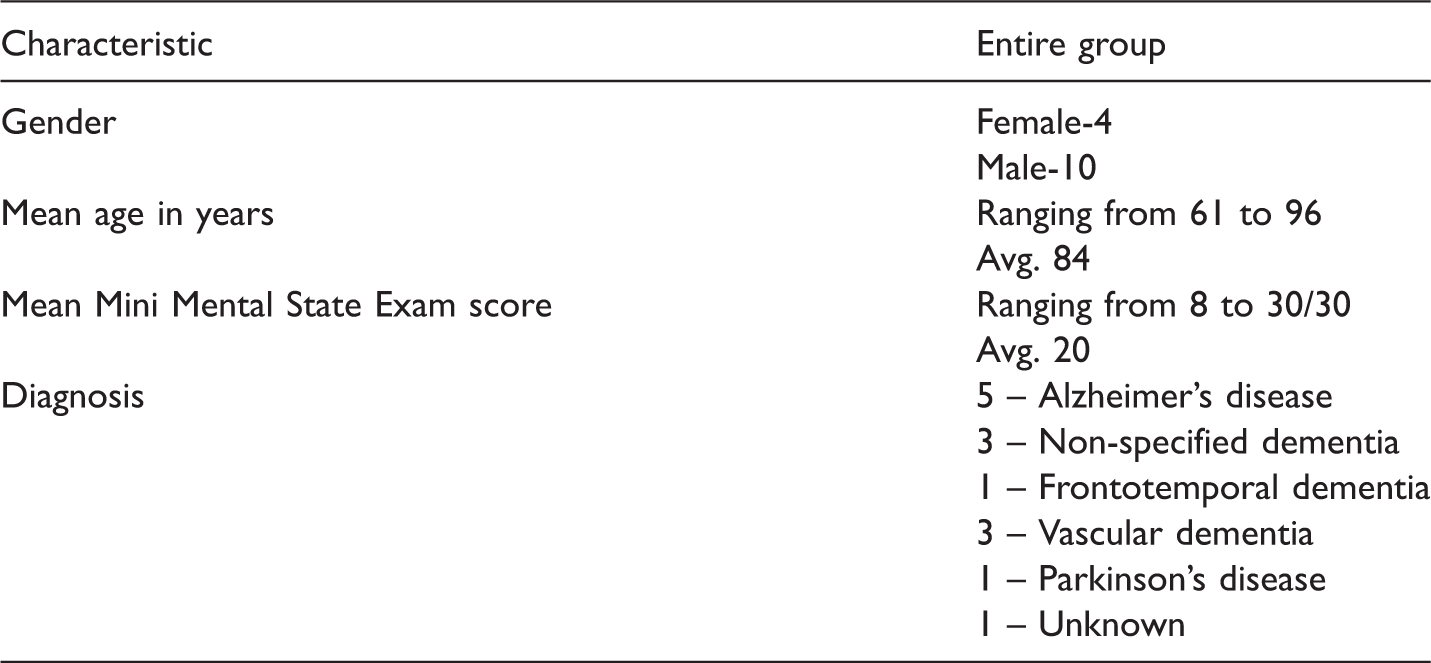
People who were already participants in the day programme were purposively selected by the coordinator of Alzheimer Outreach Services who fit the eligibility criteria and inquired about their interest in participating in the study. To be eligible for this study, participants had to fulfil three criteria: a score of 16–26 in the Mini Mental State Examination, a diagnosis or suspected diagnosis of dementia and a previous interest in gardening. Interested participants were then contacted to review the letter of information and to obtain consent. In the cases where the coordinator identified a person who met the criteria but was unable to provide his/her own consent, the coordinator contacted the client’s power of attorney to inquire about their interest in participating or as acting as a proxy respondent for their loved one.
Participant demographics.
Results: Dementia care mapping
Dementia care mapping confirmed that horticultural therapy enhanced the wellbeing of participants who took part in this study. To summarise, over 75% of the time participants were in wellbeing whilst engaging in horticultural therapy. Between 15 and 20% of the time participants were in a neutral mood while engaging with horticultural therapy. There was only a small amount of occasions when horticultural therapy was perceived as negative by participants, indeed only around 5% of the time. In other words, horticultural therapy was observed to be extremely positive for participants in this study.
The following are a detailed breakdown of the results. Based on an average of the 35 dementia care maps (completed over a 40-hour period), the following results were found:
Wellbeing
60.42% of the time people were either extremely engaged or in a state of extremely high wellbeing (this was scored as 5/5 in the dementia care map). 17.00% of the time people were either very engaged or in a state of high wellbeing (this was scored as 3/5 in the dementia care map). These combined findings meant that 77.42% of the time participants were in a state of visible wellbeing or engagement with horticultural therapy.
Neutral
17.05% of the time people were in a neutral mood, neither exhibiting high or low wellbeing nor engagement (this was scored as 1/5 in the dementia care map).
Illbeing
31% of the time people were slightly disengaged or in slight illbeing (this was scored as −1/5 in the dementia care map). 0.11% of the time people were disengaged or in illbeing (this was scored as −3/5 in the dementia care map) 0.11% of the time people were extremely disengaged or in extreme illbeing (this was scored as −5/5 in the dementia care map). These combined findings meant that 5.53% of the time participants were in a state of visible illbeing during horticultural therapy.
In addition to the scoring the mood and level of engagement of participants, we were also able to determine, through behavioural category coding, what sorts of behaviours participants exhibited while engaging with horticultural therapy. These were important to illuminate as they provide an overview of the sorts of things, observed over 40 hours, that people living with dementia may like to do within the garden.
The main behaviour category codes that were identified during horticultural therapy were behaviours: ‘L’ (33.9%) which is related to leisure or exercise-related activity, ‘B’ (12.9%) known as ‘borderline’ which is related to watching (i.e. watching others, animals, activity, etc.), ‘A’ (8.06%) which is related to articulation or directly talking with others, ‘I’ (7.69%) which is related to intellectual activity like reading an instruction manual or preparing equipment and ‘F’ (6.15%) which is related to the eating of food in the garden area.
Results: Narrative notes
Following thematic analysis of the narrative notes (Braun & Clark, 2006), the following four themes were identified as being most pertinent: combining structured/unstructured activity, the importance of teamwork, garden reminiscence and positive risk-taking.
One of the most interesting findings from this study was that participants did not exhibit significant differences between levels of wellbeing or engagement whether activities were structured (i.e. led by a member of the recreation team) or unstructured (i.e. led by the person without direct influence from the recreation team). The structured activities which occurred most frequently included: a herb garden tour which was led by the recreation team, an educational presentation about bees by the recreation team, sensory activities such as smelling/tasting herbs, facilitation of pet therapy to the garden, music therapy, making frozen yoghurt, shelling peas for lunch and erection of a protective wire fence for the flower beds. The unstructured activities which occurred most frequently included: planting seeds, watering plants, picking up branches, weeding, grass-cutting and tidying of shed-tools. Arguably the mix of structured and unstructured activity was a key benefit to participants as, on one hand, they were afforded autonomy to undertake tasks as they saw fit and, on the other hand, they were provided with a degree of direction so as to enhance their overall experience of horticultural therapy.
Another pertinent theme which emerged was the importance and enhancement of teamwork amongst participants engaged with horticultural therapy. Throughout data collection, it was observed that a number of participants, each of whom cared for their own specific plots, would water the plants or remove weeds from the plots of other participants who were not able to attend on the specific day. During horticultural therapy, participants were also observed to be working together to achieve certain goals, for example, one person would cut grass and the other would tidy the grass away, another would set the hose up and the other would water the garden area, and so on. Undoubtedly, common objectives solidified the experiences and promoted shared communication about horticultural therapy or living with dementia.
Reminiscence can occur in almost any environment but a striking finding of this study was the number of participants who talked about their past with others whilst engaged in horticultural therapy. Participants chatted with each other and care staff about their occupation, their experiences working in the garden before, birds that used to eat in participant gardens, time working in a grocery shop (which would sell the products that were being grown in the garden), the current weather and long hot Canadian summers that they experienced. In almost every occasion, reminiscence was associated with extremely high levels of wellbeing. It also fostered a deep and meaningful rapport between the participants who frequently engaged with each other in an unstructured manner.
The following risks and barriers were noted from this study: consideration related to falls, light sunburn, potential dehydration, consumption of non-ripened food from the sensory pot, feeling too warm even when sitting in shade and fatigue through overstimulation. As noted earlier in the dementia care maps, these findings did not occur frequently but do require noting so as to highlight the potential areas for risk so as to allow others to learn from these.
Results: Care partner questionnaire
According to care partners, the participants frequently and spontaneously, talked about her/his garden club experience at Alzheimer Outreach Services on the day they participated. Furthermore, participants in the day programme talked about their garden experiences on days other than when they were in the garden. When asked what her/his emotional expression was when talking about her/his gardening at Alzheimer Outreach Services, among the list of choices provided to family caregivers, (Happy, Enthusiastic, Neutral, Upset, Dissatisfied, Critical), ‘happy’ and ‘enthusiastic’ were the most frequently reported emotions. Additional comments from family caregivers suggested that participants viewed their work in the garden as a personal accomplishment, being recognized by staff and others as good at gardening. At times being ‘upset’ was expressed when an undesirable or unexpected event occurred, i.e. a flower in their personal plot wilted or died. Family caregivers were asked if their family member’s attitude about the gardening experience influence their emotional status for a period beyond the immediate discussion, and indeed this was the case, often times for hours after the discussion, sometimes for the entire day.
Discussion
When framing these findings within a person-centred context, it seems fitting to consider the pioneer of person-centred dementia care, Professor Tom Kitwood. While Kitwood’s work has been around for nearly 25 years, it is still relevant today and forms the bedrock for a number of emerging policies and practices in dementia care (Mitchell & Agnelli, 2015b). Kitwood (1997) noted some time ago that there were five important psychological needs that people living with dementia had. In short, if these five needs were met the person living with dementia could sustain wellbeing. These needs were: comfort, identity, occupation, inclusion and attachment. It is noteworthy that the aforementioned results from this research study map across to Kitwood’s (1997) original model.
To summarise, comfort was a key aspect of horticultural therapy as participants enjoyed spending time relaxing in their garden areas sometimes even taking the time to rest, watch the wildlife or have their lunch. When considering identity, the participants each brought their own unique personalities to horticultural therapy, and this was very evident during frequent periods of reminiscing where participants shared their life experiences with one another. The need of occupation is one which is often hard to facilitate in dementia care but horticultural therapy provided multiple opportunities for this as working outdoors was a key part of the participants lives (for example, weeding, cutting the grass, tidying tools in a shed, etc.) Inclusion was a core part of horticultural therapy as all participants had a role in the development of their own garden space as they had to prepare their plot, plant their seeds, care for their plants and maintain their individual areas. In addition, all participants were involved in shelling peas and making herb butter from produce and herbs grown in their plots. Finally, the need of attachment was ever-present throughout the therapeutic garden project which, as noted, was not a one-off activity. The 10 week programme allowed participants to develop their garden space over-time and gave them something to focus on outside of their dementia. The McCormick Home Foundation produced a short video which noted the various positive experiences which participants and care partners shared throughout this initiative (Women’s Christian Association, 2015).
While the findings of this study were extremely positive, there were some less positive aspects which have also been noted (i.e. sunburn, dehydration, potential distress). Importantly, these should be framed in a positive light given the majority of findings that have emerged from the data set. People with dementia are often considered as a vulnerable group of people, and while to some extent, this is true it should not automatically condemn them to a life of prescribed disengagement (Swaffer, 2014). As such, there is a certain degree of positive risk-taking which should take place when engaging in horticultural therapy.
Limitations
The main limitations of this study are that this study focused on people in the early stages of dementia so application to people living in the advanced stages of the disease may be difficult. A second limitation may be the number of participants (14) which will make generalization of data difficult. That being stated, a longitudinal approach (over 10 weeks and 40 hours of observation) meant recruitment had to be small.
Conclusion
This research project has illustrated how horticultural therapy can benefit people living with dementia. This non-pharmacological approach to care probably leads to such high levels of wellbeing and engagement because many people living with dementia spend more time indoors as their disease progresses. It has been illustrated that horticultural therapy can be unstructured and structured, or self-led and carer-led, as both are mutually beneficial as demonstrated in the findings of this study. Most importantly, access to an outside space is a human right and all care partners and practitioners should facilitate this where possible and embrace potential positive risks.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the McCormick Home Foundation, the Westminster College Foundation, the Centre for Research and Innovation (2015-07-RIF), Fanshawe College and WCA.