
Abstract
Leisure has emerged as a prominent research theme within the growing body of knowledge on dementia, with a focus on physical activity. Yet participation in any form of leisure presupposes an ability to freely choose to partake in activities and to negotiate one’s way around key barriers. In the case of dementia, the ability to undertake leisure activities is subject to a greater range of barriers, structured in a hierarchical manner that contributes to social exclusion if not addressed. This study based on focus groups with people with dementia and their family members conducted in Dorset, UK illustrates a range of barriers to leisure participation. How to create or maintain leisure opportunities for those living with dementia where households affected by dementia do not adopt avoidance behaviour, compounding a sense of isolation and exclusion is a challenge. Leisure can be an important strategy framed as a form of resistance to the social disabilities experienced by those living with dementia and it is potentially isolating impact.
Introduction
Within leisure research, the quality of life paradigm has been a research focus that highlights the interconnections between socialisation, leisure, physical activity and well-being as a basis for personal fulfilment as a dimension of quality lifestyles. One facet of the quality lifestyle debate is the way individuals and groups use their spare time; time use research (Lader, Short, & Gershuny, 2006) illustrates the negotiation that occurs within time budgets between work and non-work time. Leisure time that exists within non-work time is used for both in-home and out of home leisure creating opportunities for time and space for family bonding, renewal and enjoyment. Leisure activity occurs in a time-space continuum ranging from the home through to the pursuit of out of home leisure and recreation activities including less frequent events (e.g. domestic and international holidays which constitute tourism). In this paper we argue that the pursuit of leisure and tourism activities out with the home among those living with dementia is critical to maintaining their quality of life, particularly after diagnosis in seeking to slow its impact on well-being through active leisure lifestyles (Bherer, Erickson, & Liu-Ambrose, 2013; Cheng et al., 2013; Genoe & Dupuis, 2014). Indeed, these studies point to the transformative effect which leisure and tourism experiences can have on the well-being of those groups excluded from leisure activities when barriers to participation are removed. Participating in leisure activities has benefits beyond those associated with remaining physically active when one develops dementia (Bowes, Dawson, Jepson, & McCabe, 2013), in that leisure pursuits can promote both social (via interactions with others) and mental (via intellectual stimulation) well-being. In households affected by dementia, we explore how participation in leisure is transformed by barriers that make it a complex undertaking. In these settings, leisure time is no longer dissected by the work- non-work dichotomy. Instead, leisure time is defined through an increasingly dependent relationship between family members and the person affected by dementia. This is because dementia is a set of symptoms typically characterised by loss of memory, leading to behaviour changes and a decline over time in the ability to independently conduct every day activities (Alzheimer’s Society, 2013b).
We explore the barriers and challenges to leisure participation using a focus group method to understand the dementia inter-dependency relationship between persons diagnosed and their family members. This is important as ‘Dementia is a disease of particular concern because the decline in memory and other cognitive functions that characterizes this condition also leads to a loss of independent function that has a wide-ranging impact on individuals, families and healthcare systems’ (Plassman et al., 2007, p. 125). The paper endorses the need articulated by Sedgely, Pritchard, and Morgan (2011) that more humanist participatory research approaches are adopted that incorporate principles of critical gerontology, so that the voices and perspectives of older people are heard and understood in studies of ageing, leisure and tourism. Such an approach is also embedded in the critical duality of the ability of carers and persons with dementia to enjoy a holiday experience (Houston, 2010) as opposed to notions of separation between carer holidays and the use of respite care for the person with dementia. Such a perspective is underpinned by a growing recognition of dementia as a national (Department of Health, 2012b) and international policy issue (World Health Organisation (WHO), 2012).
Framing the interconnections between dementia and leisure
Leisure is a key element of a post-modern society, but with ageing population structures in many developed countries, there is a recognition that we need to rethink the way tourism and leisure infrastructure is configured to the needs of an ageing demographic (United Nations World Tourism Organization (UNWTO), 2010). Yet the ‘accessibility agenda’ within leisure and tourism is not necessarily inclusive or all-encompassing if specific groups are overlooked (including those with dementia) who become allocated to the category of ‘disabled’. The consequence is that the physical needs of certain groups (such as those confined to wheelchairs or other conditions such as blindness or deafness) have been subsumed in research on disability, leisure and travel (e.g. Freeman & Selmi, 2005; Israeli, 2002; Poria, Reichel, & Brandt, 2010; Yau, McKercher, & Packer, 2004). Yet dementia remains a largely hidden theme within the operational dimensions of leisure and tourism, with no mention in the UNWTO (2010) report on ageing and tourism.
The incidence of dementia also has a profound effect in relation to ageing because time use studies illustrate the increase in leisure time with age, particularly among those over 45 years of age (Lader et al., 2006). Therefore, dementia has a more profound effect when aged over 45 years, as it has the potential to induce a time-space compression in the leisure behaviour of those with dementia (as well as their carers). The leisure worlds of people with dementia can be reduced dramatically as coping with the condition can see previously active individuals’ time-space prisms of leisure reduced to home-based activity or compressed to narrowly prescribed service specific out-of home domains. Breaking the vicious cycle of time–space compression of those living with dementia is crucial, by understanding what barriers to participation exist and how to remove them. Recreational activity also performs a vital role in reducing common behaviours associated with dementia such as reducing apathy and feelings of dependency; such activity may also help to reduce the agitation associated with dementia. Yet the spatial behaviour associated with ‘wandering’ as a trait of dementia (Landau, Werner, Auslander, Shoval, & Heinik, 2009) highlights the potential problem of increased risk of harm and a resultant need for supervision of leisure activities.
The paper commences with a review of the literature on leisure and dementia, focusing on the key strands of leisure research that informed this study and the drivers of change at a policy level (dementia friendly communities, DFCs) (Local Government Association, 2012). This is followed by a discussion of the context of the study and the research design, findings and implications for creating leisure opportunities for those living with dementia. The principal research question this study set out to address was: what are the barriers to leisure participation experienced by households affected by dementia? The specific research objectives of this paper are:
To explore the views and experiences of people with dementia and their family members in relation to barriers to leisure participation and how this influenced their resulting leisure behaviour. To understand how such barriers might be addressed to maximise opportunities conducive to facilitating greater leisure participation among households affected by dementia.
Whilst the study is exploratory in nature, the findings have importance for the construction and design of generic DFC principles into leisure and tourism environments, with significance for communities and policy-makers globally. The principles of social inclusion are central to our argument that leisure can contribute to and enhance well-being to enable people with dementia to live fulfilling leisure lives.
Literature review: Conceptualising the leisure-dementia nexus
Dementia begins to create potential barriers to leisure participation (including tourism) thereby impacting upon the freedom of individuals to engage in many activities they previously undertook. The literature from leisure studies (Roberts, 2011) illustrates that the contribution of leisure to well-being is well established but through the life course of families and individuals, major life changing events such as dementia transform the leisure-well-being relationship in two ways. First, it challenges the unitary state of leisure and well-being relationships, disrupting participation through being able to access opportunities and participate. Second, if the barriers associated with dementia can be addressed, then leisure activities have the potential to make a major positive contribution to enhancing individual and family well-being. Kleiber (1999) indicated that leisure is a vital force for self-expression. Yet this is conditional upon needs being realised and barriers removed to participation socially and spatially. Previous studies of the meaning of leisure for people living with dementia (Genoe & Dupuis, 2011) are congruent with much of the social psychology literature on the benefits of leisure (i.e. day trips and daily leisure) and holidays (Tedrick, 1999). Genoe and Dupuis (2011) epitomise one strand of an evolving interest in leisure and dementia that demonstrate the benefits of leisure for people with dementia such as enabling people to ‘be me, to be with others, the pursuit of freedom, finding balance, making a difference, growing and developing and having fun’ (Dupuis et al., 2012). The critical role of daily leisure activities create the opportunity for mental stimulation from the various environmental stimuli and therefore out of home leisure (daily leisure pursuits such as walking in the park or open spaces or gardens, or less regular day trips and holidays) contribute to the stimulus of new and sometimes familiar environments out of the daily routine. As a result, research interest in leisure and dementia to date has clustered around three principal themes as shown in Figure 1.
Key themes in the leisure-dementia research literature.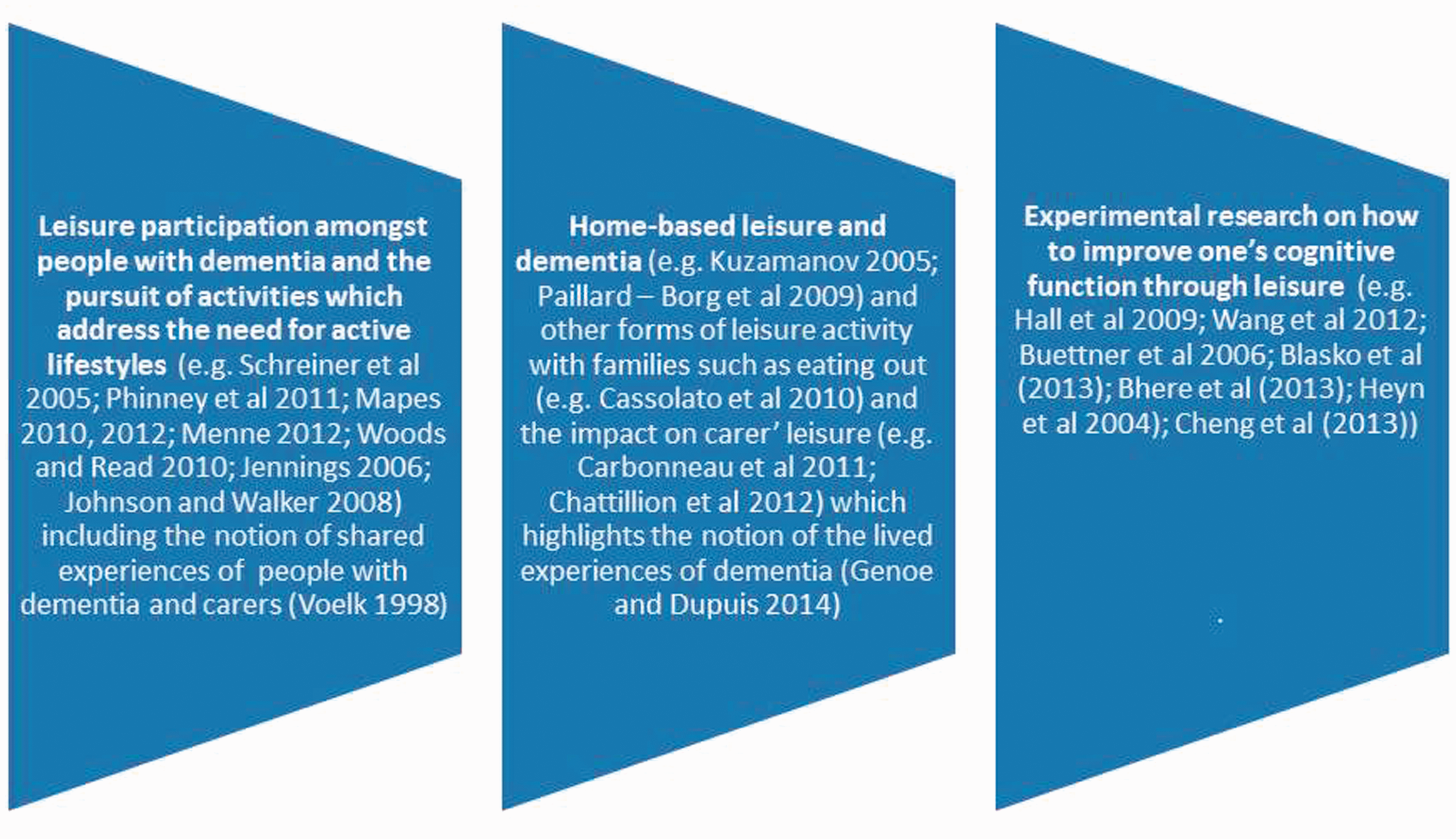
A theme of growing significance alongside the recognition of dementia as a global issue is perceptions of dementia and its associated symptoms tend to be negative. Indeed, the label of dementia is associated with fear since discourse surrounding dementia has focused on the debilitating, demeaning and despairing features (Genoe 2010, p. 309). There is a consequent need to explore the discourse of leisure and dementia, and as Genoe (2010) argues, a key role of understanding and enabling individuals with dementia to acquire the power to resist these stereotypes. Leisure and tourism represent one form of resistance to address the stigma of dementia, where participation can help individuals in their intentional resistance to negative conceptualisations of dementia, whilst also building their individual confidence to live with dementia. This can be part of a much wider empowerment that helps individuals to make informed life choices, challenging the identity and independence loss associated with dementia (Genoe, 2010).
However, among the major challenges for expanding the leisure horizons and opportunities of people with dementia and their carers is in understanding how to conceptualise the notion of dementia as a condition that leads to barriers to accessing leisure. Within leisure studies, there is a long tradition of conceptualising the barriers which exist to leisure among the population per se and more specifically to individual groups. The leisure literature suggests that leisure constraints exist as barriers to most people’s leisure time which is not without restraints (such as barriers due to a lack of time, money or social role responsibilities). Thus, barriers tend to be negotiated and a number of models of the barrier concept exist (e.g. Crawford & Godbey, 1987). For example, Crawford, Jackson, and Godbey (1991) identify three principal barriers to leisure: intrapersonal (i.e. those associated with one’s psychological state which were felt to inhibit leisure); interpersonal (i.e. those associated with one’s social setting such as family) and structural constraints (i.e. those barriers which were outside of the control of the individual) as outlined by Scott (2003). A reflective review of the leisure constraints literature (Godbey, Crawford, & Shen, 2010) found that subsequent studies have confirmed similarities across cultures. Smith (1987) provided a slightly different classification of barriers to leisure participation among people with disabilities, focusing on intrinsic barriers (e.g.health, dependency on caregivers, a lack of knowledge and social ineffectiveness); environmental barriers (e.g. access, attitudinal which leads to avoidance behaviour) and interactive barriers (e.g. the situational). The key point from the barriers literature is that barriers to leisure participation are often dynamic but can block or inhibit enjoyment/satisfaction and thereby impact on well-being. Recent studies of ageing and leisure illustrate the key role of constraints (Dhurup, 2012; Liechty & Genoe, 2013) but as Scott (2003) suggests, structural constraints tend to dominate the leisure literature. However, the issue with dementia is far more complex as the hierarchical nature of these constraints means that removing one specific barrier in itself may be insufficient to stimulate latent leisure behaviour should the barriers to participation be removed. This was reinforced by Gladwell and Bendini’s (2004) analysis of caregivers, where (with the exception of finance), physical barriers to leisure were negotiated (e.g. transport), only to be blocked by social barriers (e.g. concerns over safety) illustrating the need for a transformational policy agenda focused on developing DFCs where leisure opportunities are enhanced and social exclusion that affects households affected by dementia is reduced.
Dementia, leisure and policy drivers: Developing DFCs
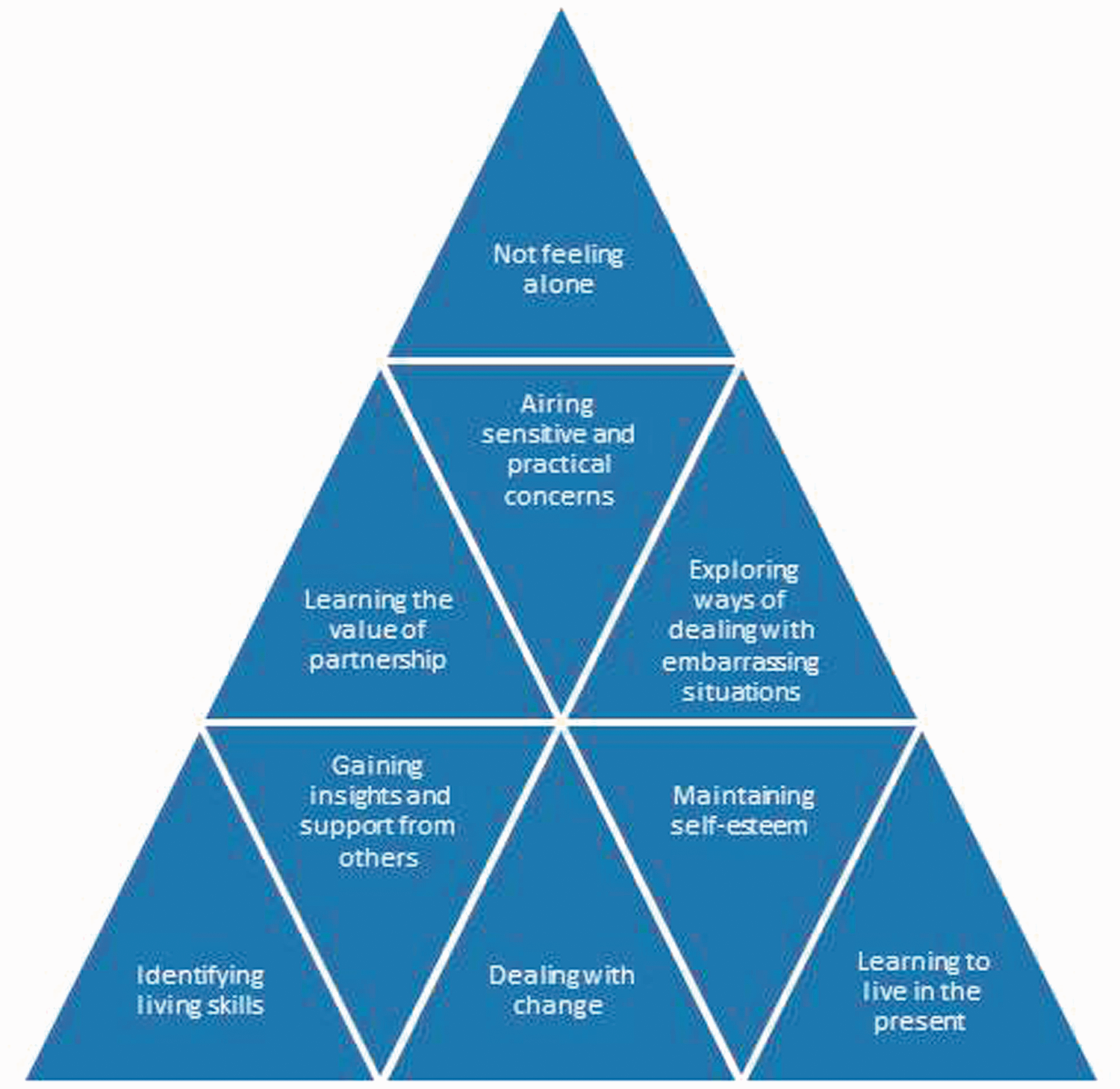
In the UK, discourse around DFCs stems from the ideology currently being articulated by the UK Prime Ministerial Group on dementia (Department of Health, 2012a) to help ‘people live well with dementia’ (Alzheimer’s Society, 2013a) (Figure 2). Such measures are critical given the cost of dementia to the UK economy estimated to be £23 billion each year, largely due to the need to provide support and services (Luengo-Fernandez, Leal, & Gray, 2010). Therefore, there are clear economic and quality of life imperatives to reduce the cost of support services where more innovative solutions to assist in improving the well-being of those affected by dementia without major social costs to the state and third sector bodies. Leisure as a concept offers one direction for researchers and policy-makers to focus on social inclusion for those living with dementia by rethinking the negative connotations of time–space compression by pursuing more active and out of home solutions to social care and well-being. This may also have community benefits as the success of the dementia (memory) café concept, originating in the Netherlands in 1997 (Morrisey, 2006). The idea offers those affected with the condition or their family members an opportunity to reduce their feelings of loneliness and isolation (Alzheimer’s Society, 2013b) among many other benefits (see Figure 3), where a simple leisure innovation can enhance the well-being and leisure lives of those with dementia. Creating DFCs includes developing an environment where people can access local services such as shops and banks as well as local facilities such as parks, transport and libraries, which if extended to other leisure settings such as tourism could enhance the lives of those with dementia. In the case of tourism, rethinking the way those affected by dementia access destination infrastructure (e.g. transport, accommodation, attractions as well as the infrastructure they use in the leisure time in the resort) is required. The transformational agenda here is to initially address the barriers those affected by dementia face, which inhibits them from participating. As Innes (2009) argues, the parallels can be understood if dementia is viewed as a social disability requiring an interventionist approach predicated on the widening access agenda inherent in a social inclusion philosophy. The aim here is to achieve a strategic shift from those affected by dementia from a marginalised and stigmatised position to one where they are part of mainstream society and able to enjoy leisure lifestyles that are not affected by negative perceptions and stigma that characterise experience of dementia from initial diagnosis through to their experience of accessing support and services. As the Prime Minister Dementia Challenge (Department of Health, 2012a) illustrates, a social inclusion approach is crucial so that significant sections of society are not isolated and unable toparticipate freely because of the negative stigmatising consequences impacting on experiences of living with dementia. However prior to outlining our research design, it is appropriate to examine why Dorset was chosen as our fieldwork location.
The development of dementia friendly communities in the UK. Source: Alzheimer’s Society (2013a). The impact of dementia café’s as a site of leisure. Source: Developed from Morrisey (2006, p. 29).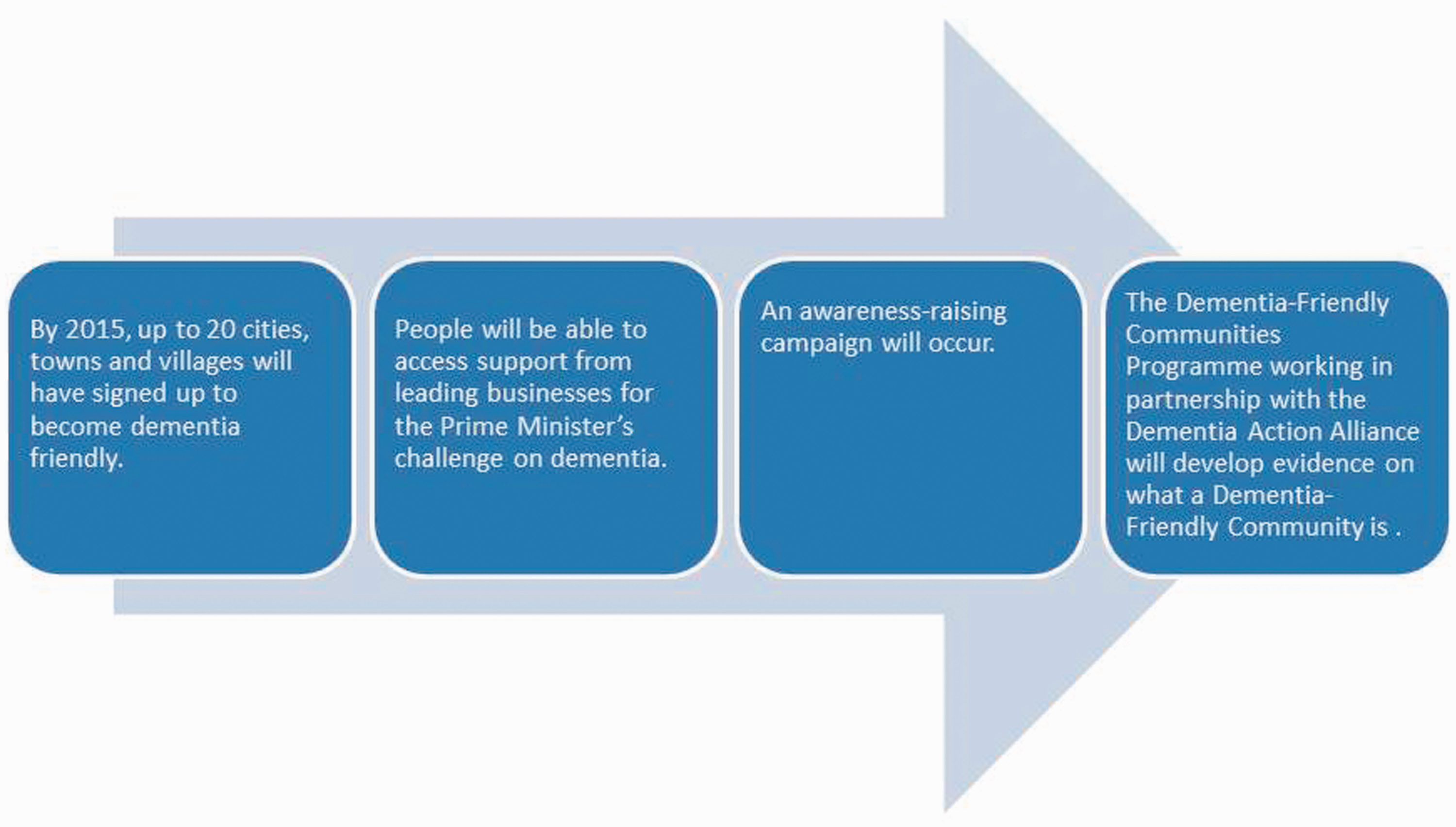
Dorset as a study location for dementia
Dorset has many unique features from a demographic and gerontological perspective since it has an above average concentration of people aged over 65 years of age (23% compared to the 16.8% English average). With the probability of the onset of dementia increasing among the over 65 age group, the spatial distribution of cases has implications for dementia care and support services. From a geographical perspective the clustering of the ageing population in retirement areas in the UK, particularly in or near to coastal areas is a long-established concept within the geography of ageing (Law & Warnes, 1976) with the antecedent impact on local areas in terms of the implications for service provision and delivery. As the 2012 Registrar General’s mid-year population estimates show, the population aged over 65 years of age is 17.9% for England and Wales; 20.3% for South West England and 26.3% for the Dorset County Council area making it an important region for the analysis of gerontological issues. Spatial variations in the geographical clustering of the ageing population are reflected at a local level within Dorset with concentrations in key coastal areas (e.g. Christchurch with 30.6%, the highest proportion of over people aged 65 or over in the UK). The region comprises a coastal conurbation running from Christchurch in the east to Poole in the west (with Bournemouth as its central point) juxtaposed with rural West Dorset’s small towns and villages and additional coastal areas running from Poole to Lyme Regis in the west. There have been comparatively few studies of dementia within this retirement region despite the ageing population. This makes the region an important natural ‘research laboratory’ for ageing since Dorset County Council (2010) illustrated the scale of the impending dementia problem for the region. In 2010, around 7700 people were estimated to have dementia. By 2025, this was expected to rise to almost 12,000 people that would place considerable stress and strain on existing services. Therefore against this background, it is clear that a study focused on the diverse ageing populations with the region would be an important starting point to understand the dementia-leisure domain.
Research design
Number of participants per focus group.
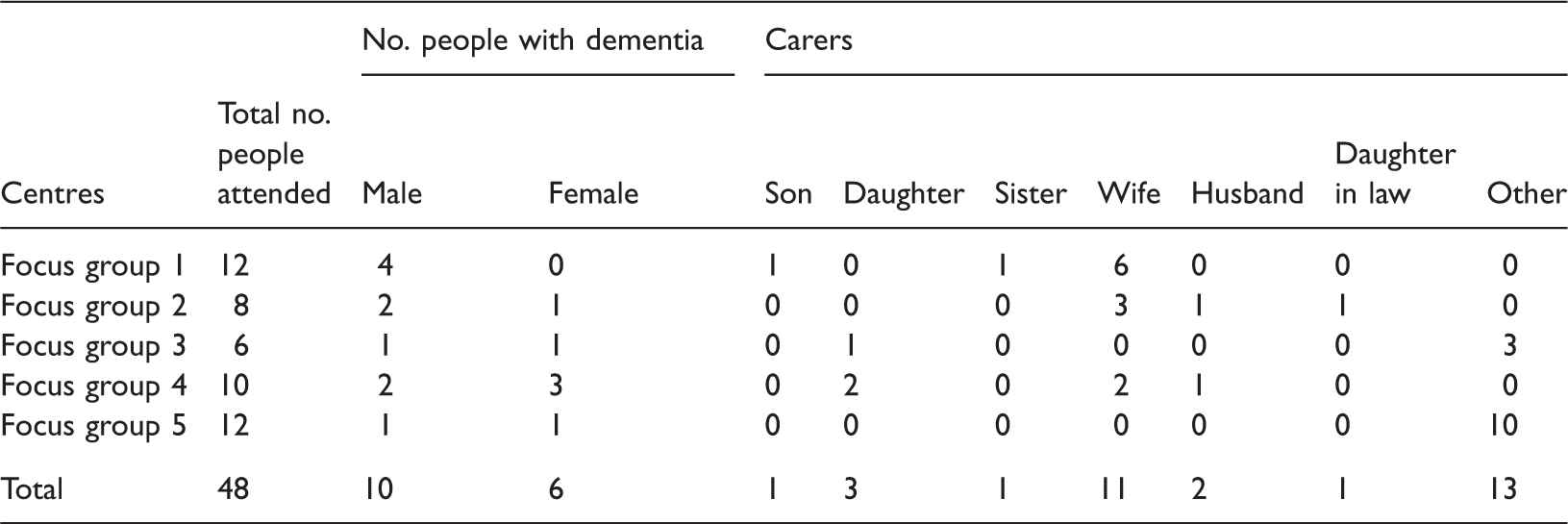
Information sheets were given to potential focus group participants prior to the research taking place. Consent forms completed by all participants’ confirmed their participation was voluntary, that the participant could leave at any time and that all data collected would be kept confidential and de-identified where necessary. Consent processes advocated by Dewing (2007) were followed, such as ongoing consent and being aware of verbal and non-verbal signs of when a person may no longer be comfortable and willing to continue to participate. Following ethics approval, information sheets were sent to the Age UK and Alzheimer’s Society venues for dissemination before the focus groups took place to attract potential participants.
A Dorset wide geographic spread was sought for the focus groups, given the known distribution of Memory Cafes in the region which attracted attendance from both urban and rural areas. As a result, a balance of areas conveniently located to the Bournemouth-Poole conurbation and the rural West Dorset region were selected. The rationale behind location selection was to provide a wider insight into the accessibility and or barriers faced by people with dementia when accessing tourism and leisure from across the region. The locations provide a representative catchment for the diversity of environments in Dorset (coastal towns, market towns and rural areas served by the market towns) to capture a wide range of experiences, views and opinions.
A thematic analysis was undertaken to provide in-depth detail on the views of people with dementia and their carers’ (Bryman, 2008; Tang et al., 2007). Themes were developed both before analysis, based on the project aims, and during analysis to pick up new and emerging themes within the data where the data was examined for recurrent themes aligned to issues highlighted in the literature review around the barriers to leisure participation. This approach to qualitative analysis meant that a series of codes were developed and applied across all of the transcripts based on a coding scheme generated by one member of the research team, each code was checked by a second research team member enabling codes to be verified or developed following discussion. NVivo9 was used for data management purposes.
Analysis of the focus groups
The analysis of the focus groups sought to consider the dementia-leisure nexus and experiences of respondents in relation to wider themes within the ageing literature, with the barriers to leisure participation used as the conceptual framework as a basis to derive and understand the key themes in the study (Figure 4) where the following themes emerged.
Barriers to leisure participation and dementia.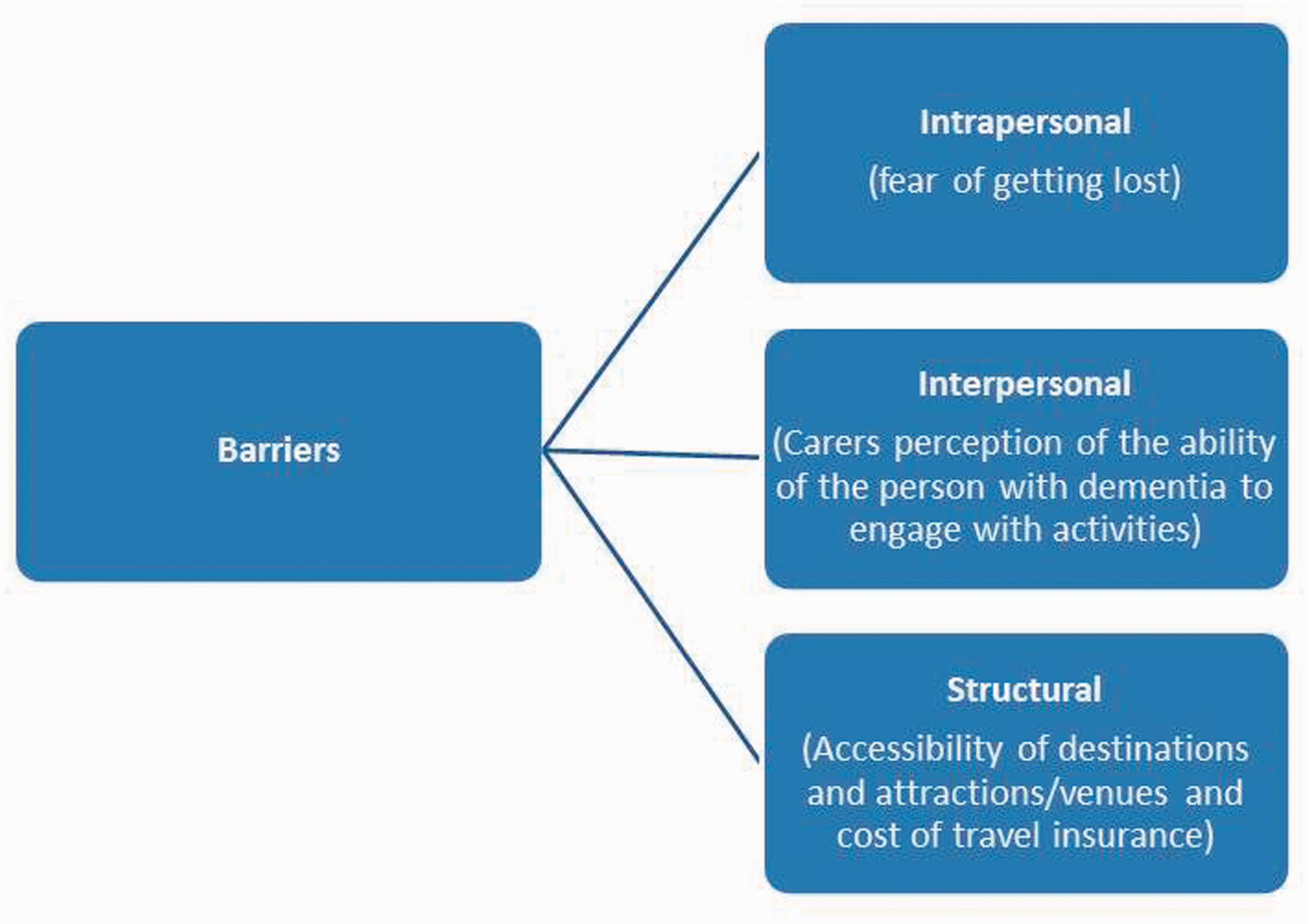
Accessibility
Accessibility was a recurrent theme across the focus groups and has parallels with the large literature that has developed around disability and leisure. Recent studies of ageing and transport (Zeitler & Buys, in press) highlight the dependence upon the car and transition needed towards more age-friendly environments. Siren and Haustein (2013) also point to the growing demands for community transport in rural areas to better meet the needs of those no longer able to drive, a major contemporary policy issue. It is therefore not surprising to find these themes occurring across the focus in the sub-themes.
Accessibility of transport
Mobility is fundamental for leisure to occur out of the home, to connect the demand (the participants) with the supply or resource-base (i.e. an attraction or venue) including motorised and non-motorised modes of transport. For those dependent upon the availability of public transport one participant living in a small coastal town commented that; “We find it very difficult because we don’t have a car, and transport is a real problem. I mean we like to go to Poole but can’t get there on public transport. So a lot of tourist places are closed to us really”. FG1C(4) “He drove all the time and even now, he’s had to give up the car keys. And I don’t drive I haven’t driven for years, so I wouldn’t drive myself at my age now”. FG1C(1) “They’re going to start the Durlston bus again this weekend, I think. Now that’s very useful. It’s two an hour and it stops at the pier. Well, (name) loves the pier, but we haven’t been able to do it because it’s a long way from our house”. FG1C(4) “The problem with Swanage is it’s always a long journey…..you get on the bus and you’re a minimum an hour to get to Bournemouth or Poole”. FG1C(2) “ I don’t think I’ want to risk it actually because there are too many, you know if the bus didn’t turn up, if it’s late, if anything happened, there are just too many probables that…. If you have a person who would get anxious would be just too much to handle, I think”. FG5C(28)
Yet where bus services were accessed, the provision of the freedom bus pass to the over 60s was a “life saver” FG4C(23)
Focus group participants experienced multiple difficulties at large rail interchanges (e.g. the short time in changing to connecting trains, navigation and physical access to other platforms combined with the support their partner with dementia needed): “I think British Rail could be more helpful…They don’t take into consideration that you’ve got five minutes to get from that train to that train. You might have a flight of stairs, you might have (name of person with dementia), two suitcases”. FG1C(4) “If you have a mobility problem, which I have and (name of person with dementia)… with steps. I mean steps are a no go. And for example I wanted to go back to (name of county) and go on the train. You have to change at Birmingham, Birmingham is a nightmare. It’s an enormous station steps everywhere and you say, ‘Can I have station assistance, if it’s available?’ What do you do? There is eight minutes between changing form one platform to the next. If you go to London… You haven’t got time unless you’re really fit… and you cannot guarantee that someone is going to appear with two wheelchairs because neither of us can do it. And this is someone who is articulate”. FG4C(21) “I look online and see where the train’s going and where it stops. And at Wolverhampton… you just wait on the same platform which is lovely”. FG1C(4)
Accessibility of toilets
Public toilet provision has become a national issue of concern in the UK, despite its absence from substantive debate in the academic literature on leisure as central to the visit experience, the ability to urinate with dignity was important to our participants. The House of Commons (2008) report illustrated the scale of decline in public toilet provision in the UK: 5410 in 2000 and 4423 in 2009, a 16% drop. This has combined with public sector cuts to public toilet provision, a potential misuse of the Disability Discrimination Act as an excuse to close many public toilets despite the vital role these facilities play in everyday leisure and business life. The House of Commons (2008, 3) illustrates the effect of these changes on the aged causing ‘the isolation of vulnerable groups unable to go out without the assurance of access to public toilets’ which compounds access issues for groups such as those with dementia and their carers. Not surprisingly, this issue was mentioned by participants in all focus groups. The concerns related to confusing signage, the need for ‘unisex toilets’, the location of public toilets and toilets on trains. In the Dorset region (including Bournemouth, Poole and Christchurch), a total of 67 publicly maintained toilets exist with a further 10 non-Council run premises to cater for a resident and large leisure/tourism population.
At three of the focus groups participants identified problems with distinguishing the gender of public toilets where pictorial signage was used instead of the more traditional wording of ‘ladies and gents’: “One thing in general I’m worried about going to places we don’t know is the toilet system. Sometimes it’s just a little man and woman, and there’s not a… you know, like a stick man and woman, and there’s not a lot of differentiation, you know…” FG1C(2) “Is that a skirt or is that trousers? I’m not sure! (Laugh). But it could be ladies inside couldn’t it?” FG4C(22) “It’s very variable I mean I find… that the signs they use, you’ve got to really, sort of, study to see which the men is and which is the women”. FG5C(25)
In fact, carers at two of the focus groups identified a need for toilets that both the carer and person with dementia could use together: “You’d think that they could have a sort of one disabled unisex, where you can both go in, you see. A bit like the mother and baby rooms…” FG1C(5) “We went down to the Victoria Coach Station. (Name of person with dementia) wanted the loo. You can imagine the chaos. I had to collar someone to take (name of person with dementia) you see. And then the lady came out and she said, (Name of person with dementia) still in there (laugh). I had to collar another lady; I said ‘can you make sure (Name of person with dementia) alright in there. You see it’s always quite difficult with the loos”. FG1C(5) … if I want to go and I leave him outside, he’s gone. The toilet again, it always seems to be the toilet isn’t it. And a toilet big enough for two people to go in, otherwise you go in, you’ve lost him and… FG3C(19) “… it don’t always work those RADAR keys. Ours doesn’t work in Cornwall…. they are supposed to be (universal) but you’ll find, you know that sometimes they don’t unlock” FG3C(19) “…and of course, you know, when she’s got to go, she’s got to go, so you don’t hang around for a half hour or more, you know” FG1C(2) “More of nightmare when dad has a moment that he needs to get to the loo quickly we’ve got to find it. And where that is wherever it is.” FG3C(18)
Accessibility of venues
Participants at three focus groups highlighted the problems they faced accessing visitor attractions, holidays and holiday accommodation because their partners had physical disabilities in addition to dementia, in particular inaccessibility to a venue if in a wheelchair: “I’m governed by pushing a wheelchair, so Lulworth [castle and sea cove] and places like that are completely out, because there’s no way you can go down things like that,…but he would like to go to places that he remembers from a child”. FG3C(13) “We went on coach holidays and every year we went to Scotland looking at places. We loved that. We’ve been all over the place on a coach but with a wheelchair you can’t get on”. FG3C(13) “I know we’re not talking about physically disabled but the tourist industry have got two different ideas about what is wheelchair friendly, what is wheelchair dependent friendly and that kind of thing because they’ll say something is wheelchair friendly if you’ve only got to go up three steps.…I’ve had to ask them for a mirror because the basin’s, the basin’s here, the mirror’s up on the wall here, he’s sitting, the back of the wheelchair’s in the bedroom, I can’t get him onto the toilet. There’s a sink like this under the shower, a shower tray that no way can I get him over that, and yet they’re saying oh yeah, yeah we’re fine for somebody who’s wheelchair dependent”. FG3C (16) “…we’ve found that a disabled toilet, you know…you find you can’t get a wheelchair and a carer and a person (in) and move”. FG3C(14)
Fear of getting lost
One of the principal issues carers raised was the fear of losing the person with dementia which meant that some family members no longer took the person with dementia on holiday: “But it wasn’t a holiday for me because I kept having to make sure that he wasn’t annoying anybody else, for a start, and not wandering off”. FG1C(4) “Not for a couple of years now. It got to the stage where, in fact he would wander out at night. We usually went self-catering…And I woke up one night and he’d gone. We were in Tenerife in an apartment…I daren’t go out and look for him because if he did come back you know, I wasn’t there. So I called security and they found him two floors down and brought him back”. FG1C(1) “I lost him in Southampton, you know the big shopping centre…I had all the security out. And they got him on security cameras and it showed how quickly he went. I was with a friend because it was the only way I could cope with it. And we just turned and looked at some clothes and he… apparently followed somebody else that looked a bit like us, straight out the door and down the stairs and he’d gone and left the building. It took them about four hours to find him”. FG1C(1) “I think well the only problem we did once in Poole… walked off somewhere and we’d sat him down ‘cos he can’t walk so far and he’d got up and gone… he ended up getting home on the bus… we had everybody out looking for him… friends and everything and he just turned up”. (FG1C)1
Carer’s perception of the ability of the person with dementia to engage with activities
Carers sometimes limited their engagement with leisure activities, believing that the person with dementia would not enjoy the activity or would become bored: “So it’s too much of a chore really to go to local centres now. We did in the early stages but it’s got to the stage now where we just don’t tackle it, because he doesn’t particularly appreciate it, he’s happier wandering around the garden. He doesn’t really appreciate it when he gets there and he will probably drop asleep in the car most of the way. And there doesn’t really seem a lot of point”. FG1C(1)
Leisure experiences and dementia
Despite the reporting of barriers, a number of respondents reported a number of sites where the visitor experience was dementia-friendly and they therefore chose to visit as the sites were local, familiar to them, and unlikely to be crowded at off-peak times. As one carer explained: “If it is very busy, anywhere where there’s a sort of strange place that he doesn’t know his way around, there are a lot of people so, to be honest, we try to avoid touristy places in season and go a bit, you know, off season, which off course you can do if you live in Dorset, it’s a bit more difficult if you’re visiting, but I think, that’ the main thought, he doesn’t like a new place with lots and lots of bustle and noise and distraction” FG5C(28) “We love museums and we like National Trust properties. To have an interesting place to visit that you feel is a normal day out and where they have a decent café that you can sit and have a rest… and with disabled friendly toilets. And if you can get a light lunch that isn’t going to cost you the earth, that’s even better”. FG4C(21) “I think his main criteria now; (referring to relative with dementia) is it very far? Will there be a loo and can I have a cup of tea. Which is fairly basic, but those are the things that concern him”. FG5C(28) “…we belong to the National Trust, we go to Kingston Lacey [National Trust property] and that’s nice because you can, there’s walks round there and you can get a meal or a coffee or whatever you want but, you know, it’s the sort of thing that (name of person with dementia) likes to do”. FG3C(16) “It’s my favourite place (in reference to Lulworth Cove). So many places you can go while you are down there. You can park the caer, and we take the dog with us and walk left or right”. FG3PWD(10) “…there’s a lovely restaurant when you go in there, that is really convenient to most people. You’ve not got much walking to do if you want to just go there and go in for a coffee and a wee snack or what have you. If you feel like it you can walk so far”. FG2PWD(8) “We went shopping yesterday and we had two lots of coffee and we had lunch and we didn’t go out until ten fifteen and we were home at four o’clock. So you can see how much time was spent on the social part of eating and drinking”. FG4C(21) “Oh we just go out and have a good look at the scenery, see what scenery we’re seeing, rivers, things like that”. FG5PWD(10) “Oh it’s beautiful. You walk along the prom, it’s lovely you know. It’s a good long walk along the front. It’s beautiful, it is, I’m not kidding”. FG3C(12) “I prefer the fresh air” FG5PWD(20) “…things that spark off any interest and things that he can remember from earlier years he likes, you know, looking at museums and things, oh I remember using one of those, you know, is that really old enough to be in a museum? That sort of thing he likes, because he can make some sort of connection”. FG5C(28) “Well he does like Monkey World [local attraction], things are closing down, (for him) you know, so they tend to… yes he likes anything living, I think he gets a response, so animals, birds” FG5C(28) “I love swans and cygnets and you can’t beat it. You can’t it’s gorgeous. It really is…… I mean the swans just sit down right in front of you and the nests they’re right at the side….It’s absolutely fantastic. It’s a sight worth seeing”. FG2C(6) “I enjoyed going to the Abbotsbury Swannery and Abbotsbury Gardens” FG2PWD(8)
Carers felt that they sometimes needed to make people aware that the person they were caring for had dementia as a coping strategy to avoid embarrassment or misunderstanding in public situations. In particular, if they felt that the person was saying or doing something that they perceived would breach conventional behaviour: “It’s some of the remarks that my husband passes about people, you know, and you just think… (whispers), you know they just ignore it then… You know, I’m waiting for someone to turn round”. FG3C(19) “I usually say something, you know, if he’s gone to the toilet or something, I’ll say well, he’s got a bit of trouble with his memory and that. And people are usually quite good but it depends. If he sees people walking along the street and he’ll say oh you look nice and things like that, you see”. FG1C(1) “Dad’s slow, you know physically and you know, there’s this, sort of, can’t get by and I’m trying to leave room……and there is that impatience yes”. FG5C(28) “I mean, it’s… sometimes, the concept of people with memory problems is quite difficult to grasp. To ever conceive that you might not remember your own name is very difficult….they need to understand and be more empathetic”. FG5C(21) Innovations to improve leisure participation.
Conclusion
This exploratory study has shown that in parallel with research on leisure and participation, there are multiple problems in the way dementia compounds the access to, engagement in and enjoyment derived from leisure activities spanning across the leisure spectrum from the day trip through to the conventional holiday. There is a distinct set of barriers that may operate dialectically or hierarchically to detract from the pursuit of leisure that is anything more than spatially confined to the immediate locale of the respondents home region (i.e. West Dorset). Spatially, this can be depicted as a compression of their leisure behaviour to create very defined and regular patterns of activity dependent upon the right facilities to accommodate the intrapersonal needs (i.e. the psychological state of the carer and person with dementia) to reduce the stress associated with social and physical obstacles. The consequence is leisure by default, where avoidance behaviour, that is taking steps to avoid a situation perceived as potentially challenging, and where opportunity is constrained by the multiple barriers that make any leisure activity extremely challenging in an inter-dependency relationship. The changes to the carer and person with dementia’s leisure lives can be profound and constraining, where holidays and activities many take for granted are no longer feasible due to the availability of opportunities, appropriate accommodation and support services. The conditions required for enjoyment and satisfaction to occur within these leisure lives are particularly challenging, with a very defined set of environmental, interactive and intrinsic factors (as described by Smith, 1987). To offer a setting conducive to dementia-friendly leisure capable of yielding positive personal benefits (i.e. happiness, satisfaction, personal fulfilment and a contribution to well-being) further research needs to be developed that is firmly embedded in social inclusion literature. The findings presented in this paper highlight that further study is required of how the positive benefits of leisure affect well-being in situ during periods of active out of home leisure and through reflection how these might be brought back to the home. This is vital if we are to fully appreciate the benefits of creating enhancing leisure environments where hierarchical barriers are removed for those affected by dementia both in their communities and in their own homes. Whilst it is not realistic to expect all visitor attractions or destinations to adopt a dementia friendly status, it is clearly a market opportunity for certain well established attraction brands such as the National Trust that have by their demographic appeal, made significant progress in creating such settings. The current policy focus on dementia as a national and international area for action to address the social exclusion many with dementia face. This illustrates that addressing structural problems associated with tourism and leisure provision more generically is needed (i.e. improving basic facilities like toilets) and that a fundamental step change is needed in public and private sector thinking and planning. The way we plan and develop dementia friendly status or dementia accessibility in our communities needs to recognise that concerted action on some areas will also have a major boost to visitor satisfaction and yield economic benefits in a growing consumer group. We need to understand the challenges arising from dementia for those living with the condition so as to empower families (including the person diagnosed) to live and enjoy greater independence from formal services in the management of their condition so that obstacles are easily negotiated or removed. If, as we would expect, the findings in this region are typical of the situation in other areas of the UK and overseas, then beginning to understand the spatial and temporal constraints imposed by a lack of suitable transport and suitable venues to visit on day trips is a key challenge for the public, private and third sector to work in partnership to address. The basis of dementia friendly attractions highlights that exemplars of best practice exist where leisure time can be enjoyed. The difficulty is that these appear to be limited in scale and scope, so a far more selective process of participation is conditioned meaning that many forms of leisure are weather dependent and only accessed through car travel and often selected based on prior positive or negative experiences of visiting a location/attraction. Social and spatial isolation is not a situation any household affected by dementia needs imposed upon them. Whilst many households take daily and special leisure times (e.g. days out and holidays) as a time for relaxation, unwinding and social bonding, it is evident from the voices of our participants’ that managing leisure behaviour can be the complete antithesis of this. These experiences are far more prevalent than one would expect in a society that has now accepted the need for interventions and action to address the mobility and leisure needs of the less able bodied (Freeman & Selmi, 2010). Yet in the case of dementia it remains a hidden and unseen problem. Dementia as a condition is more than a decade behind the positive anti-discriminatory legislation and action taken for the disabled to address barriers to leisure. However, as ‘dementia’ a condition that is going to grow in scale and significance, making fundamental changes to the way leisure and tourism provision is accessed is a major challenge that will require a better understanding of not only the barriers but the real value-adding individual experiences receive where dementia enhancing environments are developed and work to improve or maintain well-being.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by ‘Bournemouth University Research Development Fund’.