
Abstract
Investment in improving community-based dementia care is underway in the United Kingdom, but we do not know how well it meets the needs of people with dementia and those who care for them. The aim of this study was to explore the service use and reported unmet needs of people with dementia in two samples recruited a decade apart. We interviewed 122 carers from Central Scotland and London in 2000–2001 and 84 carers from South-East England in 2010–2011 using the same interview schedule. The two samples of carers had similar demographics. The later groups were more likely to be spouses, slightly older, not working, ethnically diverse, have better perceived health and better access to a car. The people with dementia in each sample had similar characteristics and levels of disability. Carers in the later sample reported more met need for activities of daily living, although up to a third were still not getting sufficient help with some activities. Nearly half of both samples reported verbal aggression and nearly a fifth physical aggression, yet most have not received advice on how to manage this. There is a more evident role of the practice nurse (p = 0.01) and less evident use of community nurses (p = 0.0005), psychiatric nurses (p = 0.006) and health visitors (p = 0.0003) in the more recent sample.
Introduction
In 2012 there were an estimated 800,000 people in the United Kingdom with a form of dementia, and numbers are set to increase (Alzheimer’s Society, 2013a). Dementia costs the UK economy £23 billion per year, twice that of cancer (Alzheimer’s Society, 2013b).
The report ‘Dementia: a public health priority’ (World Health Organisation and Alzheimer’s Disease International (WHO & ADI), 2012) recognises dementia as one of the major causes of disability and dependency internationally. Dementia is not only overwhelming for the people who have it, but also for their caregivers and families. Most care is provided by family and other informal support systems in the community and the presence of a carer reduces institutionalisation. However, changing population demographics are likely to reduce the availability of informal carers in the future, and provision of care can result in significant physical, emotional and economic strain on the caregiver. There are currently 670,000 family and friends acting as primary caregivers for people with dementia in the UK (Alzheimer’s Society, 2013c).
A European cross-national study (Schneider, Murray, Banerjee, & Mann, 1999) of 288 spouse carers for people with Alzheimer’s disease (the most common form of dementia) demonstrated a high level of burden and mental distress in spouse carers.
A systematic review of services providing information and/or advice to people with dementia and/or their caregivers identified a serious lack of studies focusing on the impact of service provision on people with dementia and very limited understanding of how services affect quality of life or neuropsychiatric symptoms. They found 13 studies investigating the effects of services that included information and/or advice as a prominent part of the intervention, none of which were based in the UK. This review identified some support for the value of information provision, but concluded studies are needed to determine the specific elements that are effective (Corbett et al., 2012).
There have been studies that have analysed needs and service use among caregivers, such as a survey of 64 UK carers who were concerned about coping with cognitive decline, early diagnosis and getting support from their general practitioner (Nurock & Wojciechowska, 2007). A study of 45 carers in Wales reported that the greatest difficulties lay in coping with the demands on carer’s time and the emotional strain of caring (Cascioli, Al-Madfai, Oborne, & Phelps, 2008) whilst interviews with 152 community dwelling people with dementia and 128 carers showed the greatest unmet needs were for daytime activities, companionship and help with psychological distress (Miranda-Castillo et al., 2010). When searching the literature we were unable to find any studies that identified changes in service use by people with dementia or their carers within the UK over the last decade.
Service availability in the last decade has changed. The NHS Plan (2000) boosted investment and led to the National Service Framework for Older People, which promoted earlier recognition for people with dementia, improved access to treatment, specialist services and social care (Department of Health (DoH), 2000a, 2001). In general practice, the Quality and Outcomes Framework for dementia introduced in 2004/2005 is expanded in 2014/2015 to include a new indicator of recording the name and contact details of the carers of people with dementia (National Institute for Health and Care Excellence (NICE), 2013). This is in keeping with recent increased recognition of the role of carers such as through the Carers and Disabled Children Act 2000 (DoH, 2000b) and the Carer’s Equal Opportunities Act (2004), as well as clarification of capacity through the Mental Capacity Act (MCA, 2005) The National Institute for Health and Care Excellence has published national guidance on care for patients with dementia (NICE, 2006 updated 2011) highlighting the rights of carers to receive an assessment of needs and be offered psychological therapy if appropriate. In 2009 the National Dementia Strategy set new standards for dementia care and provided a strategic framework within which local services could improve dementia services, address health inequalities and provide a guide to the content of high-quality services for dementia (DoH, 2009). Building on this, the Prime Minister launched the Dementia Challenge in 2012, setting out plans to go further and faster in improving dementia care, with a focus on raising diagnosis rates and improving the skills and awareness needed to support people with dementia and their carers (DoH, 2012).
Clearly, there has been significant work undertaken to improve quality of life for people with dementia and their carers and much has been achieved, but Dementia 2012 shows that at present people are still not living well with the condition (DoH, 2012). In this paper, we aim to explore how service use of carers for people with dementia recruited a decade apart compares and to assess their remaining unmet needs.
Method
Thirty-five family practices were recruited in 2000–2001 in central Scotland and in London and 21 family practices in urban and rural South East England (Metropolitan North London, Essex, Hertfordshire and Bedfordshire) were recruited in 2010–2011. These family practices identified patients diagnosed with dementia where there was a carer by the following process (Downs et al., 2006):
Patients with diagnosed or ‘probable dementia’ of any kind in the opinion of the GP and/or a specialist were identified by the GP. Carers giving a substantial amount of unpaid care on at least a weekly basis, as defined by The Carers (Recognition and Services) Act, 1995 were identified by practice. Documentation on whether the carer was aware of the diagnosed or probable diagnosis of dementia was done by practice.
Carers were excluded if their GP felt that approaching them would be inappropriate for medical reasons.
One hundred and twenty-two carers were recruited and interviewed between 2000 and 2001. Eighty-four carers were interviewed between 2010 and 2011. Consent for interview was obtained from the carers following Medical Research Ethics Committee approval which was granted by Southampton Ethics Committee (reference 09/H0502/77).
The two samples in this study are part of a randomised controlled trial in the evidence-based interventions in dementia (EVIDEM) programme (Iliffe et al., 2010). The two randomised controlled trials (Downs et al., 2006; Iliffe et al., 2010) were undertaken a decade apart and aimed to test the effectiveness of different educational interventions in improving knowledge and skills in the identification, diagnosis and management of dementia. Carers’ accounts of their encounters with family practice in the first sample have previously been published, but at that time did not include analysis of specific service use (Downs et al., 2006).
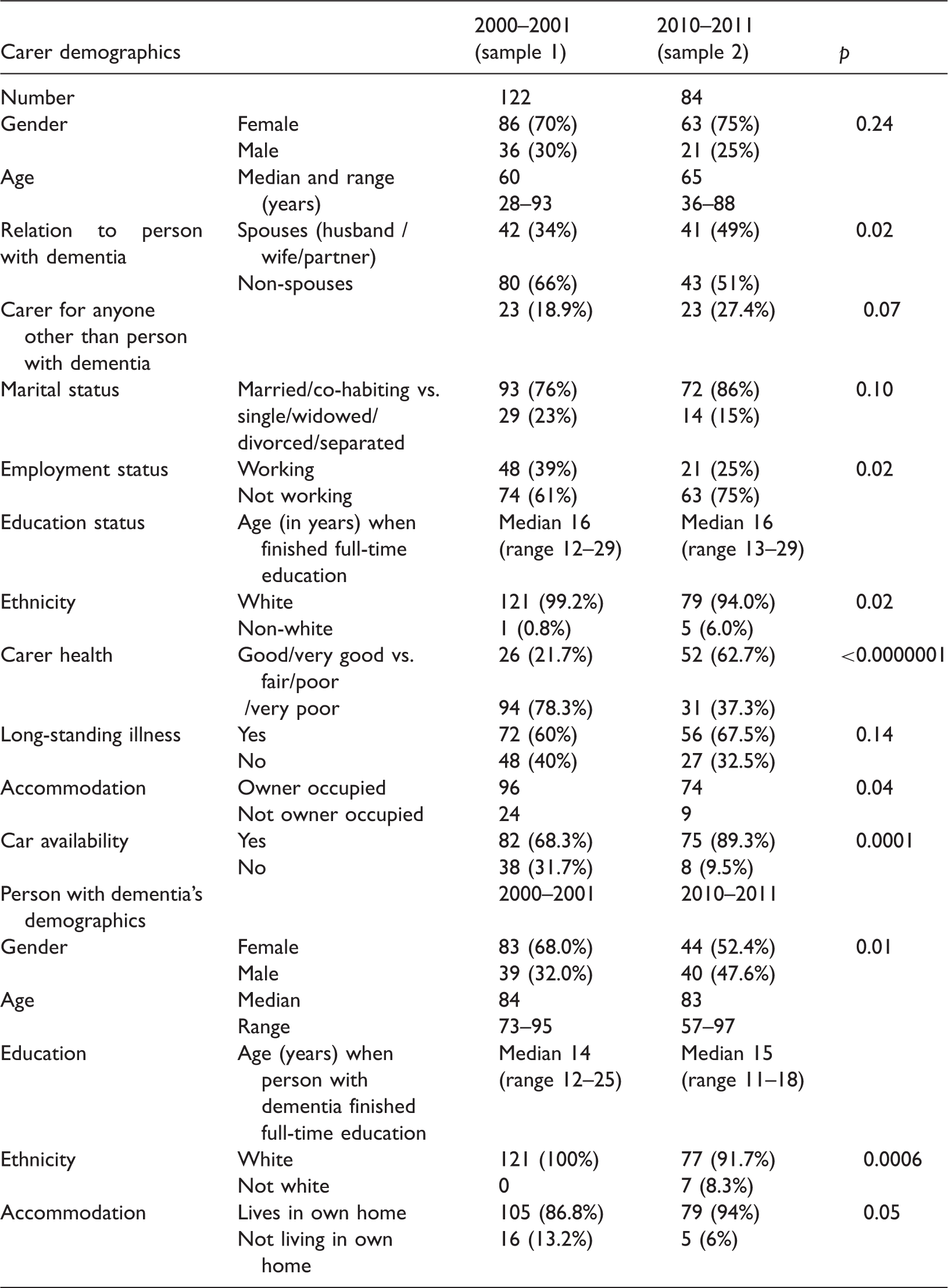
Demographics of carers and people with dementia.
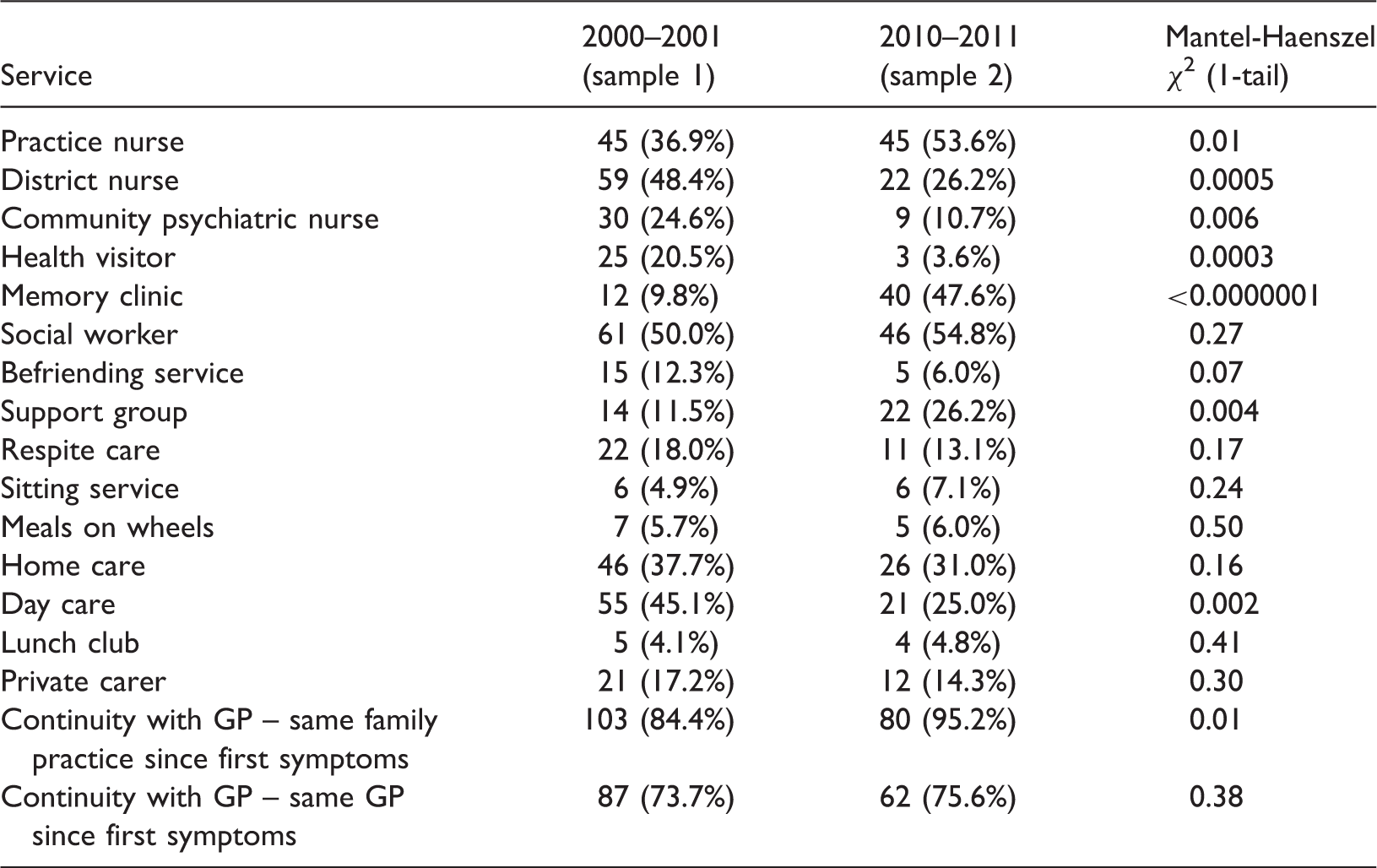
Current service use.
Activities of daily living among people with dementia: ‘Yes’ answers for capabilities.
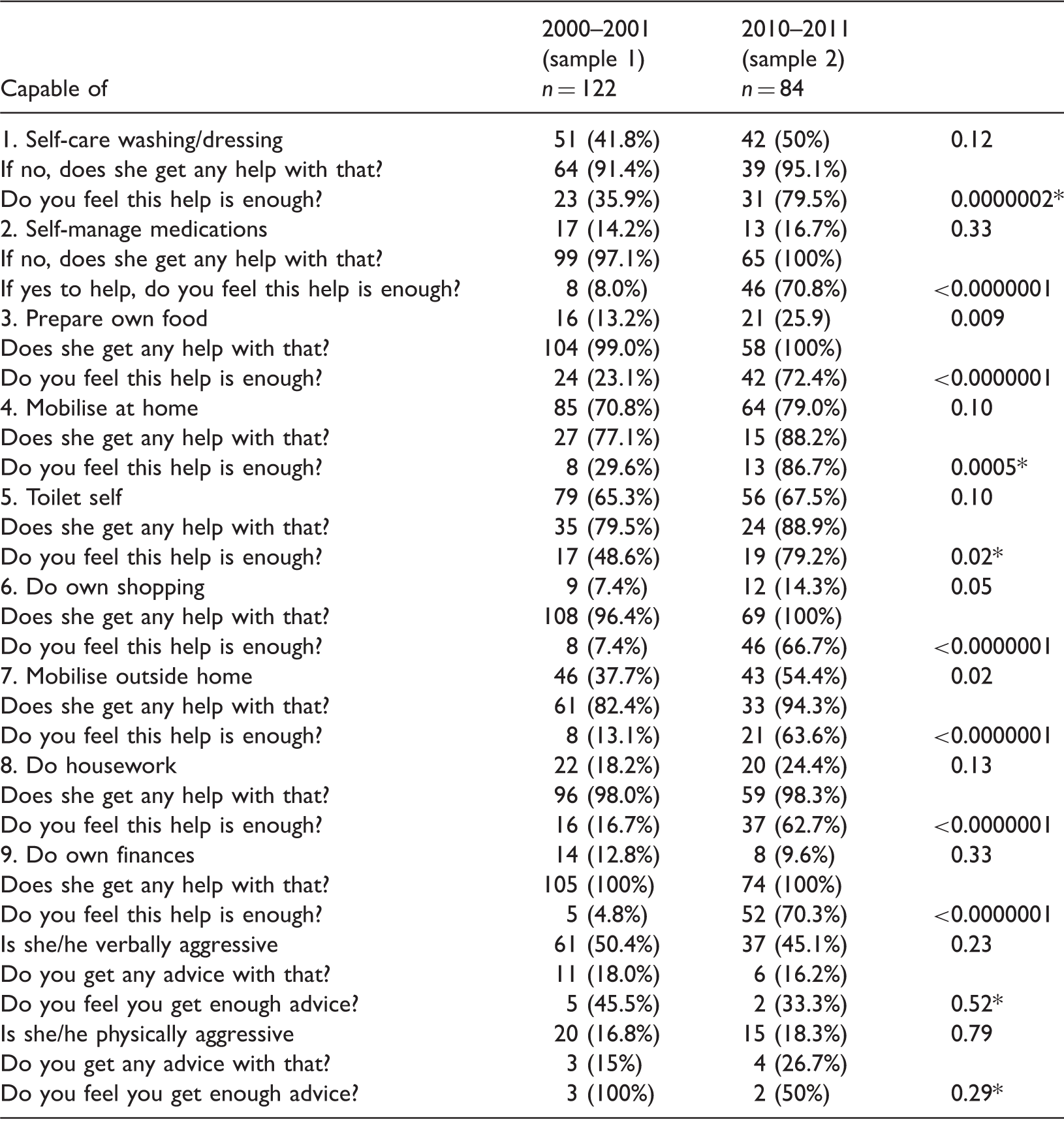
The number of ‘no’ respondents has been removed for simplicity (data available on request).
Mantel-Haenszel χ2 (1-tail) test used to measure probability, but* indicates that Fisher exact analysis rather than Chi-square due to small numbers involved.
Each person with dementia was given a score of 1 for each of these nine activities of daily living if they were unable to do that activity independently, in order to create an unweighted disability score.
Results
In the first sample, 193 carers were invited of which 129 (67%) expressed an interest in being interviewed. Two of these carers cancelled appointments and five did not give complete the interview giving a final sample of 122 (94.5% of those expressing an interest). In the second sample, 283 carers were invited of which 90 (32%) expressed an interest in being interviewed, and 84 (93.3% of those expressing an interest) provided consent and were subsequently interviewed.
Demographics of carers and people with dementia
Table 1 shows carer demographics. Carers in the two samples were broadly similar in terms of gender, marital status, education and other caring responsibilities. The more recent 2010–2011 groups were older (median 65 compared to 60), were more likely to be the spouse of the person with dementia (p = 0.04), more were not working (p = 0.03), had wider ethnicities (p = 0.03), better perceived health (p < 0.000001) despite slightly higher numbers having long-standing illness (67.5% compared to 60%, p = 0.3) and better access to a car (p = 0.0002).
Table 1 also shows a breakdown of the demographics of people with dementia in the study, illustrating similarities in terms of age, education and accommodation. The 2010–2011 group was more evenly balanced by gender and reported a wider range of ethnic origins.
Table 2 shows that the two samples were similar in terms of the ability of the person with dementia to self-care, self-manage medications, mobilise at home, manage toileting, do their own housework and their own finances. Carers also reported similar levels of verbal and physical aggression. The two samples were different in terms of the ability of the person with dementia to prepare their own food, do their own shopping and mobilise outside the home. There is also a difference in whether help for each of these features is sufficient, showing an improvement from sample 1 to sample 2 for self-care, self-managing medications, preparing own food, mobilising at home, self-toileting, mobilising outside the home, doing their own housework and doing their own finances. There was no significant difference in terms of sufficiency of advice for dealing with physical and verbal aggression.
Up to a third of people with dementia needing help with a specific activity in the second sample were still not getting sufficient help, in their carer’s opinion. Furthermore, nearly half of carers in the 2010–2011 group reported the person with dementia was verbally aggressive (45.1%) and nearly a fifth were physically aggressive (18.3%), but the majority of carers reporting these problems had had no advice on how to manage this.
Unweighted disability scores
People with dementia in the two samples had similar degrees of disability with the same median and range of unweighted disability scores (median 6, range 0–9). The mean in the first sample was slightly higher at 6.15 (std. deviation 2.14) compared to 5.31 (std. deviation 2.57) for the second sample.
Table 3 shows that the two samples were similar in terms of proportions of people with dementia currently being in contact with social workers, using befriending services, respite care, sitting service, meals on wheels, home care, lunch clubs and private carers.
There were significantly more carers who contacted practice nurses about the person with dementia in the later sample than the earlier (53.6% compared with 36.9%, p = 0.01), increased continuity with the same practice in the later sample (84.4% compared with 95.2%, p = 0.01), although continuity with the same GP was unchanged (73.7% compared with 75.6%, p = 0.38). There was a lower use of district nurses, from 48.4% in sample 1 to 26.2% in sample 2 (p = 0.0005), less health visitor contact from 20.5% to 3.6% (p = 0.0005) and fewer contacts with CPNs, from 40.2% to 14.3% (p = 0.00006). Those who received help generally found it useful.
Factors affecting service use
Practice nurse use was associated with having a non-spouse carer (p = 0.022), but no other factors were significant. No factors including spouse carer had a significant impact on use of district nurse or community psychiatric nursing services.
Figure 1 summarises the similarities and differences between the two samples.
Comparison of two case studies.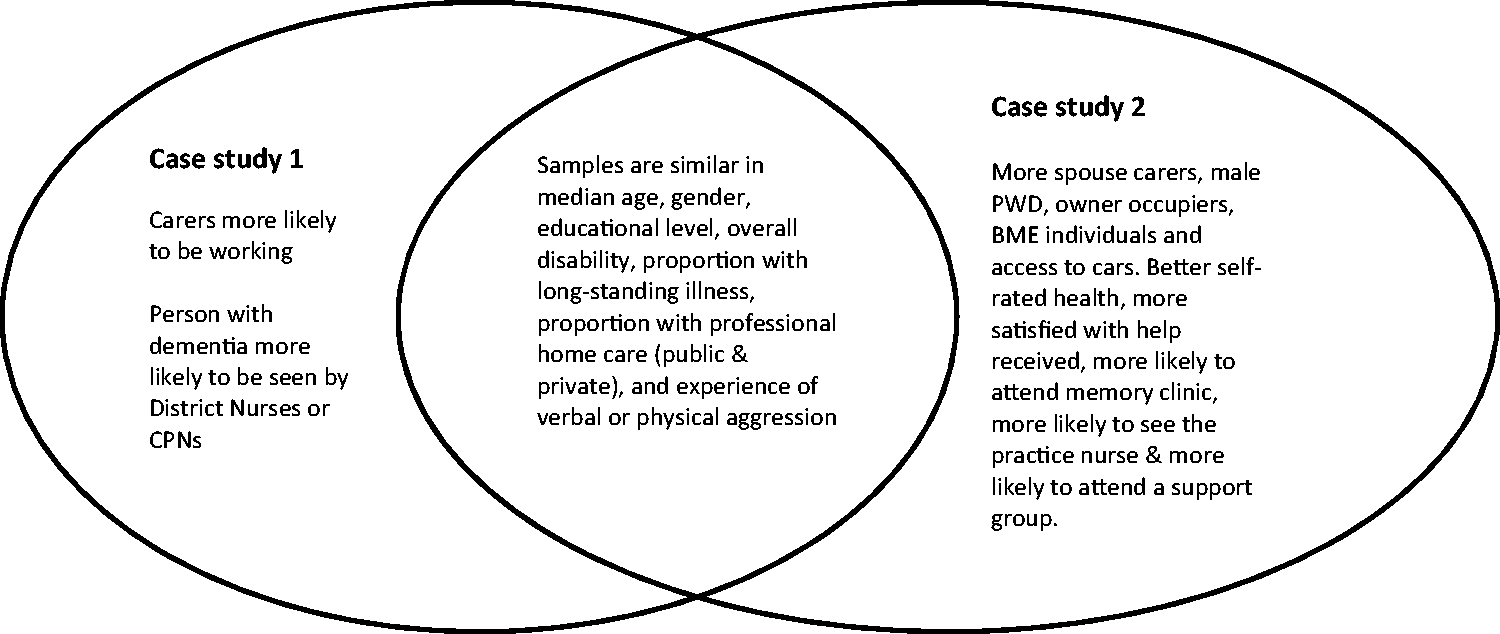
Discussion
Summary
Two samples of carers and people with dementia recruited 10 years apart from different areas as part of a larger educational study were in many ways remarkably similar in terms of broader demographics and disability. However, people with dementia received more assistance with activities of daily living in the later sample. This reduction in unmet need for aspects of health, medico-legal and social care may in part be explained by differences in the carers, who were more likely to be the spouse of the person with dementia, older, retired, with better perceived health despite long-term illness in the second sample.
This reduction in unmet need may also be related to national policies over the last decade and to changes in service use. There is a more evident role of practice nurses particularly for non-spouse carers and less evident use of community nurses, psychiatric nurses and health visitors in the most recent sample. Advice regarding aggression both physically and verbally remains a significant challenge that we are not yet meeting.
Comparative studies always prompt more questions. For example, in sample 2 there were more spouse carers, and more men with dementia, but also less contact with CPNs; higher wellbeing in carers may allow dyads to function with less external support. Contacts with practice nurses are more common in sample 2, but we do not know if these are Dementia QOF register contacts to review dementia, or encounters for management of comorbidities. This greater access to practice nurses may have implications for their continuing professional development. The prominence of memory clinics in sample 2 is consistent with their recent growth in numbers, but have they taken CPNs away from contact people with dementia and their carters later in the disease process? Greater use of support groups in sample 2 may be evidence of the third sector growing as NHS provision shrinks.
Strengths and limitations
This study compares two different samples of people with dementia and their carers, a decade apart, giving a unique insight into the differences in service use at a time when there has been significant focus on dementia care. Using the same survey instrument in both samples has allowed direct comparisons between the two groups to be made. Recruitment of carers in the earlier sample yielded a higher response of interest (67%) than in the later sample (32%). Ethics approval for the earlier sample allowed for a follow-up to initial non-response. This follow-up to non-response was not granted for the later sample and this may have influenced response rates. The two studies were a decade apart, and in that time patients registered with family doctors have received an increasing amount of communication from their doctors, so we may be seeing an element of ‘response fatigue’.
The survey is limited to responses of carers, and by sampling different geographical regions that could be influenced by population and health service system differences. Recruitment was part of an educational intervention study, and people who take part in such trials are nor representative of the broader community of people with dementia and their carers. However, we have demonstrated the two groups of people with dementia are largely similar in terms of level of disability, age and education suggesting there are broad similarities between the two groups, as well as statistically significant differences in service use and in unmet need.
Comparison with existing literature
Our finding of less unmet need in the second sample with older carers matches previous findings from the European study of co-residence spouse carers of people with Alzheimer’s dementia, showing greater caregiver burden for younger carers, financial dissatisfaction, behavioural problems and perceived negative social reactions (Schneider et al., 1999). A review of the literature between 1996 and 2006 identified dementia caregiving has been associated with negative effects on caregiver health and that individually developed interventions including diversity of services will decrease burden (Etters, Goodall, & Harrison, 2008). Burden and depression for caregivers are strongly associated with aggression, agitation and night-time disturbances (Gallicchio, Siddiqi, Langenberg, & Baumgarten, 2002; Gaugler, Kane, Kane, & Newcomer, 2005) and factors that increase stress on caregivers are predictors of nursing home placement (Hope, Keene, Gedling, Fairburn, & Jacoby, 1998).
The lack of support for dealing with physical and verbal aggression we identified in this study matches a previous study of people with dementia from 2005 to 2007 which identified the most frequent unmet needs for people with dementia living at home were daytime activities, company and help with psychological distress (Miranda-Castillo et al., 2010).
Changes in service use may be explained by change in healthcare professional numbers. The Centre for Workforce Intelligence (2012a, 2012b) notes the number of health visitors has fallen since 2004. The size of the mental health nursing workforce has been stable since 2006. The finding of the increased role of memory clinics is not surprising. They were first set up in the 1980s and by 2010 there were 246 (Scholtz, 2010). The majority of qualified nurses work in acute settings, with only 22% in designated community settings (Centre for Workforce intelligence, 2012c). This does not explain why fewer people in the later sample were in contact with a CPN or why contact with practice nurses has increased. It is known that the Quality and Outcomes Framework has changed the nature of practice nursing in recent years with an increased role of the practice nurse for long-term conditions (Centre for Workforce Intelligence). We know from a recent survey that only 37% of GPs feel they have received adequate basic training on dementia (Alzheimer’s Society, 2013c) but do not know if similar figures are true for practice nurses.
Implications for research and/or practice
Better recognition of carers and understanding the increasing role of practice nurses may help primary care to reduce the unmet needs among carers for people with dementia. Recognition of and support to manage physical and verbal aggression are particularly important.
Footnotes
Acknowledgements
We thank the carers who granted us interviews, and the family practices that recruited them for us.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethics approval was granted by Southampton Ethics Committee (reference 09/H0502/77).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this articlel: This article presents independent research funded by the National Institute for Health Research (NIHR) under its Programme Grants for Applied Research scheme (RP-PG-0606-1005). The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.