
Abstract
The aim of this study was to identify factors associated with family resilience in families caring for a parent with dementia. A mixed-methods approach was followed to collect data from a convenience sample drawn from the Cape Metropolitan area in the Western Cape, South Africa. The study sample comprised 47 families in which adult children were caring for a parent with dementia. The quantitative data analysis was conducted using analyses of variance (ANOVA), Pearson’s product–moment correlation coefficients and a best-subsets multiple regression analysis. Qualitative data were analysed using thematic content analysis. It was found that acceptance, optimism, positive communication patterns, family connectedness, spirituality, social support, economic resources and the effective management of symptoms helped these families adapt to the burdens of dementia care. In addition to expanding the literature regarding family resilience, the findings could be used to develop interventions tailored to the needs of these families caring for a parent with dementia to create a family environment that enhances adjustment and adaptation.
Dementia is a clinical syndrome characterised by the progressive decline of cognitive functions. It has a prevalence of about 5% in the general population over the age of 65 and 20–40% in those over the age of 85 (Sadock & Sadock, 2007). In 2013, an estimated 44.35 million people were living with dementia worldwide and, due to population ageing, it is expected that this number will triple by 2050 (Alzheimer’s Disease International, 2014).
South Africa’s healthcare system is burdened with overcrowded hospitals; a lack of treatment resources and a shortage of health professionals in the public sector. As a result, institutional care tends to be quite expensive (Department of Health, 2001). Patient care for individuals with long-term or terminal illnesses like dementia thus falls upon family members (Chang, 2009). These families often face considerable physical, psychological, emotional, social and financial burdens (Chang, 2009; Gilliam & Steffen, 2006; Schulz & Martire, 2004). However, despite the difficulties of dementia care, most families are able to cope with their situation and continue to function well as a family unit. So why do some families cope well with dementia care while others fall apart? A contextual framework for this question is provided in the family resilience paradigm.
Walsh (2003) defines resilience as “the ability to withstand and rebound from crisis and adversity” (p. 1) and describes it as a dynamic process involving positive adaptation. Resilience enables families to respond effectively to crisis situations and, as a result, to recover and grow from the experiences undergone. Family resilience contributes to family well-being and counteracts difficulties that impair family functioning (Heru & Ryan, 2006). More resilient families are usually more accepting of the changes in the behaviour of the dementia patient, better prepared for the inevitable changes in their own lives brought about by the illness, more open to the development of new coping strategies in response to the demands of dementia care and experience better psychological adjustment (Majerovitz, 1995). Exploring resilience factors that families utilise to deal with the demands of caregiving thus could provide useful strategies that can be incorporated into the development and evaluation of intervention programmes. This study used a combination of McCubbin and McCubbin’s (1996) Resiliency Model of Family Stress, Adjustment and Adaptation and Walsh’s (2002, 2003) Family Resilience Framework as a theoretical framework to explore this subject.
In McCubbin and McCubbin’s (1996) Resiliency Model, the family resilience process is divided into two phases: the adjustment phase and the adaptation phase. The adjustment phase is characterised by minor adjustments made by the family in an attempt to deal with the demands of a stressor event. The adjustment process is characterised by the family’s appraisal of the stressor, the availability of established patterns of functioning and effective problem solving and coping skills within the family unit, the family’s vulnerabilities and the family’s accessibility to relevant resistance resources. If a family is unable to mobilise the family adjustment process effectively, a state of maladjustment develops, which typically results in a condition of family crisis. When faced with a family crisis, the family soon realises that their efforts to adjust are inadequate and thus enters the adaptation phase. During the adaptation phase, families need to make significant changes in their internal structures and patterns of functioning to restore balance and harmony within the family system. Bon-adaptation is achieved once a family has successfully integrated the demands of a stressor event into the family’s established patterns of functioning and balance and harmony are restored (McCubbin & McCubbin, 1996).
Walsh’s (2002, 2003) Resilience Framework approaches family resilience from a developmental and ecological perspective. The framework describes the family as an open system that evolves continuously over time and is highly influenced by the historical, cultural and social systems in which it functions. Walsh (2002, 2003) also distinguished between three family domains that promote family resilience: (a) family belief systems, which facilitate family appraisal processes, promote optimism and foster transcendence and spirituality; (b) family organisational patterns, which refer to family flexibility, family cohesion and the utilisation of social and economic resources and (c) family communication patterns, which promote free emotional expression, encourage collaborative problem solving and clarify ambiguous situations (Walsh, 2002, 2003).
The current study forms part of a larger study on resilience in families caring for a loved one diagnosed with dementia. The larger study focused on families in which the spouse or adult children of the patient took on the role of primary caregiver. Studies warn that the nature of the relationship between caregivers and dementia patients could account for significant differences between these subgroups (Pinquart & Sörensen, 2011). Some studies, for example, found that spouses caring for a partner with dementia have a higher risk of depression (Pinquart & Sörensen, 2011; Schoenmakers, Buntinx, & Delepeleire, 2010; Zanetti, Frisoni, Bianchetti, Tamanza, Cigoli, & Trabuchi, 1998), experience more mental fatigue (Nagatomo, Akasaki, Uchida, Tominaga, Hashiguchi, & Takigawa, 1999) and have poorer relationships with the patient (Spruytte, van Audenhove, Lammertyn, & Storm, 2002) than children caring for a parent with dementia. Spouses also tend to use less informal support, perceive their physical health to be worse (Pinquart & Sörensen, 2011) and often experience social isolation (Schoenmakers et al., 2010).
Conversely, children caring for a parent with dementia are often of working age, thus facing additional stresses associated with balancing their caregiving duties with their professional duties. Children of dementia patients have to execute their caregiving duties while maintaining a healthy relationship with their own spouse and children as well (Schoenmakers et al., 2010). The caregiving environment and its impact on the family unit might be influenced by these differences. To optimise family adaptation, intervention strategies thus need to be tailored to the different needs of these subgroups (Pinquart & Sörensen, 2011). Family resilience factors of these family subgroups (spouses and adult children) should thus be explored separately. Consequently, the primary aim of this study was to identify, explore and describe resilience factors that are present in families caring for a parent diagnosed with dementia. Results obtained from spouses caring for their partner with dementia are reported in the study by Deist and Greeff (2015).
Method
This study was exploratory and descriptive in nature. It utilised a cross-sectional survey research design to collect both qualitative and quantitative data from a convenience sample based in the Cape Metropolitan area of the Western Cape, South Africa. The unit of analysis was the family – a group of two or more people linked through kinship, marriage/domestic partnership or adoption who reside in the same household (Nam, 2004).
Participants
Two organizations – Dementia South Africa and Alzheimer’s South Africa (Western Cape branch) – were approached and asked to help identify possible candidates for this study. Both organisations provide support to families caring for people with dementia. The organisations invited the researcher to attend their monthly family support groups. A specific slot during the meeting was allocated to the researcher, in which she was able to discuss the study. Members who were not interested in the study were allowed to leave before the researcher addressed the group. In addition, Dementia South Africa posted a flyer advertising the study on their Facebook page. Grootte Schuur Hospital and Panorama Memory Clinic – who both specialise in the field of memory and dementia care in the Western Cape – were also approached and asked for assistance in identifying possible participants. Panorama Memory Clinic invited the researcher to attend their monthly support group meetings. Flyers advertising the research study were displayed in Panorama Memory Clinic’s waiting room as well. Grootte Schuur Hospital invited the researcher to attend their weekly Geriatrics clinic and Memory clinic. Medical staff approached the family members who accompanied dementia patients and asked them whether they would be willing to participate in this study. If the families agreed, a hospital staff member introduced the researcher to the volunteer. None of the individuals approached by the researcher declined to participate.
Data were collected from 47 families in which an adult child was caring for a parent with dementia. The participating families all fulfilled the following criteria: (a) a family member had been diagnosed with dementia; (b) the child of the dementia patient acted as primary caretaker; (c) the diagnosis had been made at least one year previously; (d) the dementia symptoms were moderate to profound; (e) the person diagnosed with dementia had been living with the family for at least six months; and (f) the participant was fluent in either English or Afrikaans. Only one family member, who was chosen by the family unit to act as the family representative, took part in the data collection process.
In the South African census, citizens are asked to describe themselves in terms of five racial groups based on biological characteristics, geographic ancestry, ethnicity and cultural heritage. These racial categories, which were derived from apartheid classifications, are Black African, White, Coloured (people of mixed ethnic origin), Indian or Asian, and Other/Unspecified. Of the 47 participants in this study, 30 (64%) were coloured, 11 (23%) were white, four (9%) were black and two (4%) identified themselves as ‘Other race’. Most of the participating families identified English (n = 26; 55%) or Afrikaans (n = 17; 36%) as their home language. Family representatives were aged between 20 and 64 (mean = 47.2; SD = 9.6), and most of them were women (n = 38; 81%). The dementia patients were aged between 57 and 90 (mean = 77.4; SD = 7.9) and were mostly females (n = 37; 79%). Most families listed three adults (n = 22; 47%) living together in the household. Four families (9%) had two adults living in the same household; eight families (17%) had four adults living in the same household and 13 families (28%) listed five or more adults in the household. In 2011, 3% of Western Cape households had a monthly income of $160 or less; 31% earned between $160 and $640 a month; 13% earned between $640 and $1,280 a month; and 26% earned more than $1,280 a month (City of Cape Town, 2012). In comparison, the participating families in the current study (N = 47) were economically slightly better off, with 11% earning between $100 and $200 a month, 26% earning between $200 and $500 a month, 30% earning between $500 and $1 000 a month, and 34% earning more than $1,000 per month.
Measures
A structured questionnaire was used to collect the biodemographic information of the participating families. Qualitative data were collected through a semi-structured interview in which participants were asked about family traits and resources that helped the family unit to deal with the burdens of dementia care. Qualitative data collection was terminated once the data started repeating themselves and the interviews delivered no more new themes (n = 21). Seven self-report questionnaires were used to collect quantitative data. These measures were selected based on earlier research regarding family resilience and are in accordance with McCubbin and McCubbin’s (1996) Resiliency Model of Family Stress, Adjustment and Adaptation.
The total score of the Family Attachment Changeability Index 8 (FACI8) was used to measure the dependent variable in this study – family adaptation. The FACI8 consists of 16 items rated on a 5-point Likert scale and has two subscales. The attachment subscale measures the level of family cohesion. The changeability subscale measures the level of family flexibility (McCubbin & McCubbin, 1996). In this study, the attachment and changeability subscales obtained internal reliability coefficients (Cronbach’s alpha) of .65 and .76, respectively.
The Family Crisis Oriented Personal Evaluation Scale (F-COPES) was used to determine what problem-solving and behavioural strategies families utilised when faced with hardship. It consists of 30 items rated on a 5-point Likert scale. The items are divided into five subscales measuring different types of coping skills, viz. (a) reframing the situation to make it more manageable; (b) passive appraisal, in which families accept the situation and minimise their reactivity towards it; (c) acquiring social support from relatives, friends, neighbours and extended family; (d) seeking spiritual and religious support and (e) mobilising family members to seek and accept help from others (McCubbin & McCubbin, 1996). In this study, the internal reliability (Cronbach’s alpha) of the F-COPES (Total Score) was .79.
The Family Hardiness Index (FHI) was used to assess the internal strength and durability of the family unit when confronted with a crisis. This index consists of 20 items that are rated on a 5-point Likert scale and is comprised of three subscales: (a) commitment, (b) challenge and (c) control. The commitment subscale measures the family’s dependability, ability to work together and sense of internal strengths. The challenge subscale measures the family’s propensity to positively reframe stressor events, be innovative, learn new things and actively seek out new experiences. The control subscale measures the family’s perception regarding their control over family life (McCubbin & McCubbin, 1996). In the current study, the FHI obtained an overall internal reliability (Cronbach’s alpha) of .72.
The Family Problem Solving and Communication (FPSC) Index was used to evaluate the communication patterns used by families during crises. It consists of 10 items rated on a 4-point Likert scale and has two subscales. The Affirming Communication subscale identifies positive communication patterns that express care and support and tend to calm a situation. The Incendiary Communication subscale identifies negative, provocative communication patterns that often intensify stressful situations (McCubbin & McCubbin, 1996). The overall internal reliability (Cronbach’s alpha) of the FPSC in this study was .88.
The Family Time and Routine Index (FTRI) was used to identify the types of activities and routines families engage in and the value they attribute to these practices. The scale consists of 30 items that are rated on a 4-point Likert scale and is divided into eight subscales: (a) parent–child togetherness – which assesses the family’s emphasis on routines that encourage communication between parents and children; (b) couple togetherness – which measures the family’s emphasis on predictable communication between spouses; (c) child routines – which evaluate the family’s emphasis on routines that promote a sense of independence and order in children; (d) meals together; (e) family time together – which determines the family’s propensity to regularly spend time together; (f) family chores routines – which evaluate the family’s attempts to create routines that encourage children’s responsibilities at home; (g) relatives connection routines – which measure the family’s emphasis on establishing predictable routines that promote a meaningful connection with relatives and (h) Family management routines – which evaluate the family’s emphasis on routines that promote an atmosphere of family organisation, order and accountability (McCubbin & McCubbin, 1996). In this study, the FTRI attained an overall internal reliability (Cronbach’s alpha) of .96.
The Relative and Friend Support Index (RFS) was used to identify the extent to which families utilise friend and relative support to help them cope with stressor events. It consists of eight questions rated on a 5-point Likert scale (McCubbin & McCubbin, 1996). In this study, the RFS had an internal reliability (Cronbach’s alpha) of .80.
The Social Support Index (SSI) was used to measure the degree to which the participating family (a) has integrated into their community; (b) finds support in their community; and (c) makes use of community resources for emotional, esteem and network support. The index consists of 17 items rated on a 5-point Likert scale (McCubbin & McCubbin, 1996). The internal reliability (Cronbach’s alpha) of the SSI in this study was .76.
Procedure
Ethical clearance for this study was obtained from Stellenbosch University’s Ethical Research Committee (protocol number HS694/2011). Three recruitment methods were used to obtain volunteers: (a) recruitment at Groote Schuur Hospital’s weekly Memory Clinic and Geriatrics Clinic, (b) recruitment through the dementia support groups of Dementia South Africa and Alzheimer’s South Africa and (c) recruitment through pamphlets advertising the study. Every volunteering family was presented with a written consent form that discussed all relevant information regarding the study. The main points of the study also were discussed verbally and the families were given a chance to ask questions regarding any uncertainties. The families were reminded that participation was voluntary and that confidentiality and anonymity were assured. Due to the sensitive nature of the illness, dementia patients did not take part in the data collection process.
Results
Quantitative results
The relationship between family adaptation (as measured with FACI8) and several demographic variables was calculated using Spearman correlation coefficients. Household income (r = .37, p = .01) and the number of adults in the household (r = .33; p = .03) were the only variables that had a significant, positive correlation with family adaptation.
Pearson product–moment correlations between independent variables and the level of family adaptation.
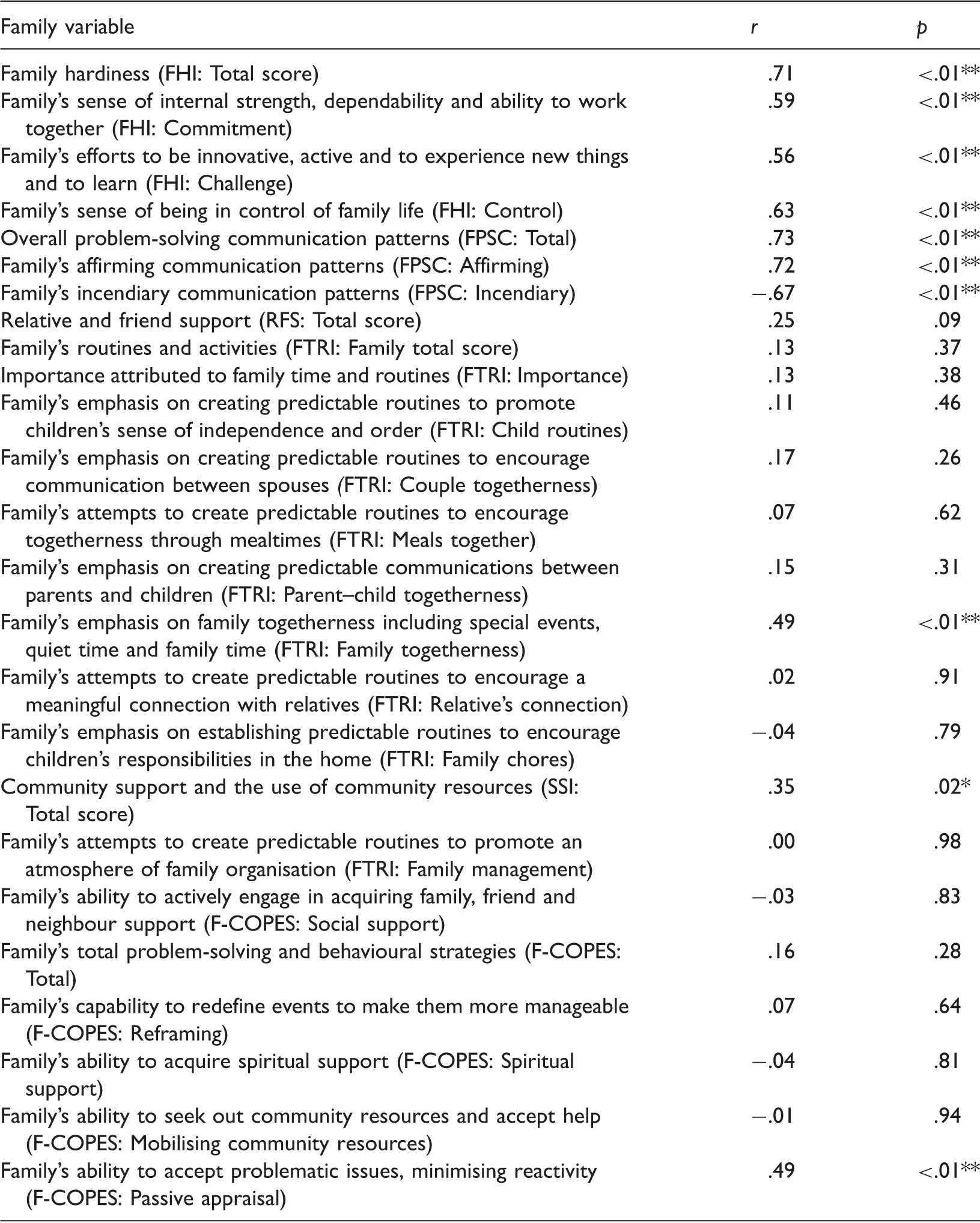
Note: Measured with FACI8. N = 47. FACI: Family Attachment Changeability Index; F-COPES: Family Crisis Oriented Personal Evaluation Scale; FHI: Family Hardiness Index; FPSC: Family Problem Solving and Communication Index; FTRI: Family Time and Routine Index; RFS: Relative and Friend Support Index; SSI: Social Support Index.
p ≤ .05. **p ≤ .01.
Best-subset multiple regression analyses were done to determine the combination of independent variables that best predicted family adaptation. The best subset identified a set of five variables as the best predictors: (a) the family’s overall problem-solving communication patterns (FPSC: Total); (b) community support and the use of community resources (SSI: Total); (c) the family’s capability to redefine events to make them more manageable (F-COPES: Reframing); (d) the family’s ability to seek out community resources and accept help (F-COPES: Mobilising community resources) and (e) the family’s ability to accept problematic issues, minimising reactivity (F-COPES: Passive appraisal). The family’s overall problem-solving communication patterns (t(41) = 4.82, p < .01) were the only statistically significant predictor of family adaptation. A multiple R2 value of .56 indicates that the set of variables identified accounted for 56% of the variation in the FACI8 scores. However, when compared with other subsets, the best subset’s multiple R2 value might differ only slightly. It thus could be argued that the variables identified as best in predicting the level of adaptation might be included due to chance. The different sets of variables obtained in the 20 best subsets were thus compared with each other to control for this limitation. Family problem-solving communication (FPSC: Total score) and the Passive appraisal of a crisis situation (F-COPES subscale) were both identified in all the subsets compared, and the Reframing of a crisis situation (F-COPES subscale) was present in 15 (75%) of the 20 best subsets, thus validating these variables as significant predictors of family adaptation.
Qualitative results
Qualitative data were gathered via semi-structured interviews. Due to time constraints, qualitative interviews were conducted only until data saturation was achieved (n = 21). The participating families were interviewed on a first come, first served basis. The qualitative subsample was a good representation of the full sample; 76% of the interviewees were female, 52% were coloured (n = 11), 33% were white (n = 7) and 10% were black (n = 2). The data were analysed via thematic content analysis, and the themes that emerged most often were social support, financial stability, religion and spirituality, optimism, positive communication patterns, family connectedness, acceptance and the management of the illness. Similar themes were identified in all racial and gender groups.
The source of support mentioned most often was physical and emotional support from family members (n = 19; 90%). A white, female participant cherished the emotional support provided by her sister: ‘Me and my younger sister, we communicate very well. We discuss [the illness], and we support each other quite a lot’. Another participant, a coloured male, emphasised the importance of physical support from family members: ‘Each one has a role to play. During the day, I am not there. My dad’s niece actually comes in to help my wife look after him. And as far as his medication is concerned – that is where my sister comes in; she will take care of the medical side of things. I am on the financial side of everything’.
Most participants also mentioned the positive impact of hired help on family adaptation (n = 13; 62%). Hired help included nurses or dementia caretakers hired by the family, elderly day-care facilities, or respite care where families could drop off dementia patients for a few nights. Participants explained that they used these services as a way to take a break from the physical burdens of dementia care. A coloured, female participant said: ‘I take my mother to the day care. It gives me a break so I can go shopping. I felt that, when she was home, I couldn’t go anywhere. Now we take my mother to the day care. It helps. It’s just like the Re-Spite care – but that’s a different place where they sleep over. When [my husband], for example, sees we need a break, we book my mother in there. It doesn’t feel nice to leave her there, but you come back with new courage; you have new strength to go on with what is waiting ahead’.
Other sources of social support utilised by the participating families were support from friends (n = 5; 24%); support from dementia support groups (n = 7; 33%); support from doctors (n = 6; 29%); and professional help (n = 2; 10%). Only 14% of the participating families (n = 3) mentioned community support as a resilience resource; 43% of the participants (n = 9) believed that the community provided no support at all. When asked about community support, one participant, a black male, said: [The community is] not helpful. In the past, they always made a joke of her. Even the neighbours, when she walks in the road, they just tell her: ‘Go away, go!’ But she has a problem with hearing cars – it’s dangerous! She shouldn’t walk alone. So I must always be there. They don’t help.
The families who made use of financial support (n = 6; 29%) got financial backing from family members. A white, female participant said she got most of her financial backing from her brothers: ‘Financially [my brothers] support me. I get as much financial support as I want’. None of the financial support mentioned was provided by government.
The participants also warned against the negative effects of continuous exposure to the stressors associated with dementia care. They emphasised the need to take a break from caregiving now and then to focus on their own well-being and the well-being of the family unit. One participant, a black man, warned: ‘You deal with dementia every day; it’s quite hectic. You need to go out and have a bit of fun, and then you can come back and deal with it again. You become a very impatient person if you don’t take a break now and then’.
Another participant, a coloured woman, explained how communication fostered an understanding between family members. As a result, they were more aware of each other’s feelings and thus better able to support each other on an emotional level. ‘You need to talk [to each other], otherwise things start brewing up, and you don’t even know what's going on in your own home – you won’t know about problems in your own family’.
Patience was also identified as an essential characteristic when living with a dementia patient. Participants emphasised that negative communication patterns were ineffective ways of dealing with problems and that they were better able to cope with a situation once they had calmed themselves. A coloured, female participant explained: ‘Standing there shouting – what’s the point? It’s not going to work. It’s not going to make him understand. I found screaming doesn’t help. It makes him more agitated’.
Furthermore, the love family members felt for the dementia patient also made caregiving less burdensome. Family representatives who described the patient as a loving parent explained that caring for the dementia patient was simply the method by which the family expressed their gratitude for the support they had received in the past. In the words of a white, female participant: ‘After everything [my mother] gave us, it’s almost a kind of ‘payback’ out of love for what she’s done. I think that it’s just how we were brought up. We had a lot of support and now we want to support her’.
Another factor that affected the management of the illness was information-seeking; 62% of the participants (n = 13) believed that information regarding dementia and dementia care facilitated adaptation. One participant, a coloured woman, elaborated: ‘I Google and read a lot about dementia. I read books on psychology now as well, just to give for me an idea [of what to expect]’. The participants explained that, by educating themselves and each other on the nature and symptomatology of the illness, they were better able to understand the behaviour of the patient, thus making it easier to accept and manage the situation. The internet and dementia societies, like Dementia South Africa and Alzheimer’s South Africa, were the most used sources of information.
Discussion
The primary objective of this study was to explore resilience factors utilised by families in which adult children acted as the primary caregiver of a parent diagnosed with dementia.
In the qualitative interviews, social support was the only family resource identified as a crucial resilience factor by all participants. These findings enjoy theoretical support in terms of the Resiliency Model of McCubbin and McCubbin (1996) and the Resilience Framework proposed by Walsh (2002, 2003). In the current study, families made use of familial support, support from friends, hired help (e.g. nurses or day-care services), dementia support groups, community support and support from health professionals (i.e. doctors, psychologists and social workers) to help them adjust to their burdens.
Physical and emotional support from family members was the most popular source of support. The importance of familial support could offer a possible explanation for the statistically significant, positive correlation found between the number of adults in the household and family adaptation. Larger families meant more hands to assist with the task of caregiving, thus alleviating the severity of the stressor. However, the quantitative results showed no statistically significant correlations between familial support and family adaptation (see Table 1). The instruments used to measure this variable – the Social support subscale of the F-COPES and the RFS – might be the cause of this divergence. Both scales include items that focus on support from friends and neighbours; neither focusses exclusively on familial support. Only 24% of the participants found social support in friends, while 33% struggled with social isolation. By including items that focus on support from friends and neighbours, the true correlation between family adaptation and familial support could be skewed. Nonetheless, several other family resilience studies have identified support from family and friends as a major feature in the adaptation process of families caring for a chronically ill family member (Carnes & Quinn, 2005; Greeff & Thiel, 2012; Greeff & Wentworth, 2009; Preece & Sandberg, 2005).
The quantitative results of the present study emphasise the importance of community support in the family resilience process. The degree to which families found support in their community had a positive correlation with family adaptation (see Table 1). In the multiple regression analysis, both the degree to which families found support in their community (as measured by the SSI) and the mobilisation of the family to seek and accept help from others (as measured by the Mobilisation subscale of the F-COPES) were identified. However, the contribution of these variables was not statistically significant. Only 14% of the participants mentioned community support as an effective resilience resource, while 43% of the participants reported a lack of community support in the interviews. Even so, the positive effect of community support on the families of chronically ill patients has been emphasised in previous resilience studies (Greeff Van Steenwegen, & Ide, 2006; Greeff & Wentworth, 2009; Jonker & Greeff, 2009).
Financial stability also had a positive effect on family adaptation. A significant positive relationship between household income and family adaptation was revealed in the quantitative results. In the qualitative interviews, the majority of the participants declared that they were coping without any financial assistance. Some families received financial aid from other relatives to help them cope with the financial burden of dementia care. Previous studies on family resilience also showed that good financial management and a satisfactory economic status have a positive relationship with family well-being (Black & Lobo, 2008; Carnes & Quinn, 2005; Walsh, 2003).
The qualitative results of this study show that religion and spirituality helped several families adapt to living with a loved one diagnosed with dementia. However, the quantitative results revealed no significant relationship between family adaptation and spiritual and religious support (see Table 1). Similar results have been found in other family resilience studies (Greeff & Thiel, 2012; Greeff et al., 2006; Jonker & Greeff, 2009). The measuring instrument used in these studies (F-COPES: Spiritual support) could be the cause behind the discrepancies found in the quantitative and qualitative results. The measure focusses on support from religious or congregational affiliation and neglects the spiritual support provided through personal or familial rituals (e.g. meditation, prayer and family Bible study). Nonetheless, several studies on family resilience acknowledge the positive association of spirituality with family adaptation (Carnes & Quinn, 2005; Greeff & Joubert, 2007; Walsh, 2002; 2003).
Optimism was identified as a vital family resilience factor in the current study. The qualitative data revealed that most families actively sought out ways to maintain a positive attitude to help them cope with their situation. These findings are echoed in the work of Walsh (2003), who found that an optimistic view of life fostered hope for the future and provided families with the strength to rise above adverse circumstances. Greeff and De Villiers (2008) and Greeff and Wentworth (2009) also identified optimism as a characteristic that facilitates the family resilience process.
A statistically significant positive correlation was found between family hardiness and family adaptation. This implies that family adaptation had a positive relationship with the family members’ ability to work together and depend on each other in times of hardship (FHI: Commitment); the ability of a family to reframe crises positively, learn new things and actively seek out new experiences (FHI: Challenge) and the family’s perception of control regarding their own life (FHI: Control). This connection between family hardiness and family adaptation has been discussed in other family resilience literature as well (Greeff & Thiel, 2012; Greeff et al., 2006; Greeff & Wentworth, 2009; McCubbin & McCubbin, 1996; Preece & Sandberg, 2005).
The independent variable with the strongest significant correlation with family adaptation was family problem-solving communication patterns (FPSC: Total). In addition, family adaptation had a strong, positive correlation with communication patterns that conveyed support and care (FPSC: Affirming communication subscale) and a strong, statistically significant negative correlation with negative, provocative communication patterns (FPSC: Incendiary communication subscale) (see Table 1). These findings were supported in the best-subset regression analysis, in which the family’s overall problem-solving communication patterns were identified as the independent variable that best predicted variation in family adaptation. These findings also were supported by the qualitative data. Participants emphasised the importance of patience in the resilience process and thus avoided negative communication patterns. They encouraged positive, open communication that fostered a culture of love and understanding within the family unit. These findings enjoy theoretical (McCubbin & McCubbin, 1996; Walsh, 2002, 2003) and empirical support (Black & Lobo, 2008; Greeff & Thiel, 2012; Greeff & Wentworth, 2009; Jonker & Greeff, 2009).
In the qualitative interviews, the majority of the participants identified factors that promoted family connectedness as an important resilience characteristic. This result was confirmed by the quantitative findings of the current study, which revealed a positive, statistically significant correlation between the family members’ ability to work together and depend on each other in times of hardship (FHI: Commitment subscale) and family adaptation, as well as a significant positive correlation between routines that encouraged family members to spend time with each other (FTRI: Family time together) and family adaptation. A similar theme regarding family connectedness was reported in Jonker and Greeff (2009). Likewise, Preece and Sandberg (2005) found that conflict in the family was related to higher levels of family distress. Greeff and Wentworth (2009) and Black and Lobo (2008) reported a positive relationship between family adaptation and family routines that promote various forms of family togetherness. The theoretical framework of Walsh (2003) also describes cohesiveness among family members as an important family resilience resource.
In the qualitative results, acceptance was identified as a family resilience quality. The participants explained that adaptation was only possible once the condition of the patient (and the effect of the illness on the family unit) had been accepted. The quantitative results reiterated these findings (see Table 1). Passive appraisal had a significant positive correlation with family adaptation, implying that family adaptation tended to be better in families who accepted their situation and who minimised their reactivity towards it. Passive appraisal was also identified as one of the independent variables that best predicted family adaptation by the best-subset multiple regression analysis. Even though this finding was not statistically significant, passive appraisal was identified in the 20 best subsets of the regression analysis, thus validating the importance of passive appraisal in the prediction of variation in family adaptation. Walsh’s (2002, 2003) Resilience Framework explains that the family’s ability to accept a crisis event (like caring for a family member with dementia) has a significant influence on their competence in selecting adequate coping responses. However, some studies have mixed findings regarding passive appraisal as a family resilience quality. The results of the current study are supported by those of Bester (2009) and Greeff et al. (2006), who found a significant positive correlation between family adaptation and passive appraisal. In contrast, Jonker and Greeff (2009) found a significant negative correlation between family adaptation and passive appraisal.
Family adaptation also tended to be easier if family members perceived their situation as manageable. Factors that influenced the perceived manageability of the illness included personal biases, the use of medication, the use of effective, tried-and-tested caregiving strategies, and other stressors faced by the family unit. Furthermore, knowledge regarding dementia, its symptoms and methods for managing the symptoms was identified as a key element in the resilience process. The quantitative results revealed a tendency that suggested a positive relationship between family adaptation and the family’s ability to reframe a situation to make it more manageable. It also was identified as a predictor of family adaptation in the best-subset multiple regression analysis. McCubbin and McCubbin’s (1996) Resiliency Model and Walsh’s (2002, 2003) Resilience Framework both identified a family’s appraisal of a stressor event as crucial in the family’s adjustment and adaptation processes.
Conclusion
The body of information presented in this study provides helpful insights into the resilience factors of families in which adult children act as the primary caregiver of a parent diagnosed with dementia. Acceptance, optimism, positive communication patterns, family connectedness, spirituality, social support, economic resources and the effective management of symptoms were all identified as protective factors that helped these families adapt to the burdens of dementia care. These identified factors can be utilised in future studies to help expand our knowledge about the family resilience process. Furthermore, the results could be incorporated into the development and evaluation of intervention programmes that help families caring for dementia patients to maximise family adaptation.
However, the study is not without limitations. First, the sample was relatively small. Furthermore, the racial distribution of the sample was not representative of all the races in South Africa. The generalizability of the results thus are restricted. Second, the family unit was represented by a single family member. The personal biases of one family representative could have an influence on the validity of the results. Finally, data collection consisted of the once-off gathering of data at a single point in time. Considering the degenerative nature of the illness, the adaptation of the family unit as the dementia progresses is of great importance. Future researchers should attend to these limitations in order to obtain a better understanding of the resilience qualities utilised by families living with a parent diagnosed with dementia.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.