
Abstract
This focus group study explored experience of Korean American personal care aides caring for older Korean Americans with dementia symptoms. Personal care aides described dementia caregiving as challenging, demanding and stressful, yet they cared for their clients with love and affection, particularly with jeong (i.e., a Korean cultural concept of love, affection, sympathy, and bondage). They learned about dementia mostly through their caregiving experience and expressed their need and strong desire to learn more about dementia. They felt for family struggle and observed family conflict and filial obligation. They advocated the value of personal care aides’ involvement in dementia care. This study revealed a pressing need for dementia training for personal care aides and called for an outreach effort to recruit and train direct care workers with potential of providing culturally competent care for traditionally underserved ethnic minorities.
Keywords
Introduction
With rapid aging of the baby boomer population, the demand for long-term care for older adults is increasing. This has generated a growing concern for how to provide necessary health care and personal care for older adults who develop chronic illness, disabilities, and cognitive impairment as they age (Hussein & Manthorpe, 2005; Smith & Baughman, 2007). Family members (unpaid informal caregivers) play a major role in caring for older adults. However, the availability of family caregivers is shrinking due to demographic (e.g., decreased fertility rates) and socioeconomic trends (e.g., changes in family structures and increased participation of women in the labor force; Brodsky, Habib, & Mizrahi, 2000; Hussein & Manthorpe, 2005). Caregiver support ratio, the number of potential caregivers (adult children, aged 45–64) for each person aged 80 and older (those who are most likely need support and services) is projected to decline from more than seven potential caregivers to one older adult in 2010 to 3 to 1 by 2050 (Redfoot, Feinberg, & Houser, 2013). Moreover, most older adults prefer “aging in place”—remaining in their homes and community as long as possible with accommodated support such as home- and community-based services (HCBS) and they consider institutional care as a last resort (Davey, de Joux, Nana, & Arcus, 2004; Kane, 2005; Lehning & Austine, 2005). All of these factors have escalated the demand for formal paid caregivers who provide care and services for older adults (Freeman & Spillman, 2014).
Direct care workers (DCWs) are formal paid caregivers and provide hands-on care at people’s homes as well as care facilities (Seavey, 2011). In the United States, they provide an estimated 70% to 80% of paid hands-on care (Paraprofessional Healthcare Institute [PHI], 2011) and 8 of every 10 hours of paid services are provided by a DCW. Considering older adults’ strong preference to remaining in the community over institutional care, the number of DCWs working in the community setting is expected to exceed those working in institutional settings by nearly two to one by 2018 (PHI, 2010a). In some states, this trend is already evident: for example, three quarters of DCWs in California work in home- and community-based settings (PHI, 2010b).
While various titles are used for DCWs, such as home health aide, home care aide, personal care aide, personal assistant, home attendants, homemakers, personal care staff, and resident care aide (Seavey, 2011), US occupational code officially recognizes two job titles: home health aide and personal care aide. The former provides medically related routine tasks such as changing bandages and applying topical medication, thus, it is under the category of health care support occupation; and the latter provides self-care tasks (i.e., activities of daily living (ADL)), everyday tasks (i.e., instrumental activities of daily living (IADL)) and social support, thus, it is categorized as personal care and service occupation (U.S. Bureau of Labor Statistics, 2010; Seavey, 2011).
Particular interest of the current study is personal care aides (PCAs) caring for older adults with dementia symptoms. The number of people affected by dementia is on the rise. It is estimated that approximately 5 million Americans 65 and older had Alzheimer’s disease (AD), the most common type of dementia, in 2015, and the number is expected to reach 13 million by 2050 (Hebert, Weuve, Scherr, & Evans, 2013). AD is an irreversible, progressive brain disease that can last up to 20 years, during which its cognitive and behavioral symptoms only exacerbate as the disease progresses (Alzheimer’s Foundation of America, n.d.). Although the demand of DCWs, such as PCAs, in dementia care is rapidly increasing, research that examined the role and experience of DCWs is scant because care for persons with dementia is often provided by family caregivers. Moreover, these limited studies about DCWs were mostly conducted in institutional settings (i.e. nursing homes and assisted living facilities), mainly focusing on training issues and job satisfaction (e.g., Ejaz, Noelker, Menne, & Bagaka’s, 2008; Hughes, Bagley, Reilly, Burns, & Challis, 2008; Menne, Ejaz, Noelker, & Jones, 2007). Studies about DCWs in dementia care are even scarcer. A handful of such studies report that, compared to DCWs working in general units in nursing homes and assisted living facilities, DCWs who care for older adults with dementia tend to experience higher levels of stress, work constraints and interpersonal conflicts (Scott & Cassie, 2007; Zimmerman et al., 2008).
Despite the growing demand for DCWs, the long-term care industry has struggled with recruiting and sustaining DCWs, mainly because DCW is not viewed as a desirable career opportunity with its demanding nature of work, lack of respect, and low wages (Acker, Pletz, Katz, & Hagopian, 2015). In a shortage of native workers, foreign-born workers, including foreign workers who are directly recruited from other countries and immigrants who are already in the country, are identified as potential sources of new workers and their participation in the workforce has been increasing (Priester & Reinardy, 2003; Stone & Wiener, 2001). The rate of growth in foreign-born workers in the US or U.S. health care workforce is approximately twice that of the native workers (Lowell, 2012). For example, 45% of PCAs was foreign-born in California (Seavey, 2011). Despite a potential significant role of foreign-born workers in dementia care, no study has specifically looked at their experience as DCWs. Available research is mainly about workforce shortage and growth of foreign-born workers (e.g., Lowell, 2012; Priester & Reinardy, 2003; Stone & Wiener, 2001) or administrators’ view on foreign-born workers (e.g., Acker et al., 2015). It is still largely unknown the role and experience of a growing number of foreign-born PCAs providing dementia care in the community setting. Our study addressed this gap by exploring the experience of foreign-born Korean American (KA) PCAs who provide care for KA older adults with dementia symptoms in home setting.
Like other dementia research in general, research about dementia caregiving in KAs has been mainly in the context of family caregiving (unpaid informal caregiving) (e.g., Casado & Lee, 2012; Casado, Lee, Hong, & Hong, 2015; Jang, Kim, & Chriboga, 2010; Lee & Casado, 2011) and no research has examined the role of paid formal care, such as care provided by PCAs. Research has indicated that KAs prefer service providers of the same ethnicity and that shared cultural background could facilitate effective delivery of culturally responsive service in dementia care (Casado et al., 2015). However, how matching cultural and linguistic backgrounds between providers and clients plays out is yet to be studied. As foreign-born PCAs can be a vital workforce in long-term care, there is an urgent need for research to better understand their role and experience. To our knowledge, our study is one of the first research that examined foreign-born PCAs caring for clients of the same ethnicity. Specifically, we explored KA PCAs’ experience and perspectives concerning three areas: (a) dementia caregiving; (b) knowledge and beliefs about dementia; and (c) family caregiving.
Methods
Research design and data collection
This study was based on an exploratory qualitative approach and was conducted using a focus group approach. In the original study, we conducted a total of six focus groups over a 6-month period: four focus groups with 23 KA family caregivers and two focus groups with 10 KA PCAs of older KAs with dementia symptoms. This study reports the findings from the two focus groups with PCAs. (Findings from other four focus groups with family caregivers are reported elsewhere (Casado et al., 2015)). Each focus group lasted approximately one to one and a half hours and was held at a Korean church-based senior center in mid-Atlantic metropolitan area. Focus group interviews were carried out using a structured interview schedule with open-ended questions. As the purpose of this study was to understand participants’ experience and perceptions on specific key issues that we had identified as important in understanding dementia caregiving and service needs among KAs, we used a straightforward strategy (Stockdale, 2002) and asked specific questions in each of the three issue areas mentioned earlier.
Because the primary language of all participants was Korean, all focus group interviews were conducted in Korean by a trained bilingual/bicultural facilitator. We used “rapid bilingual appraisal” model (Whelan, 2004) where a bilingual/bicultural researcher facilitated focus groups while another bilingual/bicultural individual interpreted the proceedings to the non-bilingual principal investigator (PI) in the room. We used this approach because it allowed the non-Korean bilingual PI to fully engage in the data collection while ensuring the natural flow of focus group interview (Garrett, Dickson, Lis-Young, Whelan, & Roberto-Forero, 2008). All focus group proceedings were audio-recorded for analysis with participants’ permission. Focus group participants received $50 cash as compensation for their time and traveling. The research protocol of the study was approved by the University’s institutional review board.
Participants
Characteristics of Korean American personal care aides (N = 10)

Data analysis
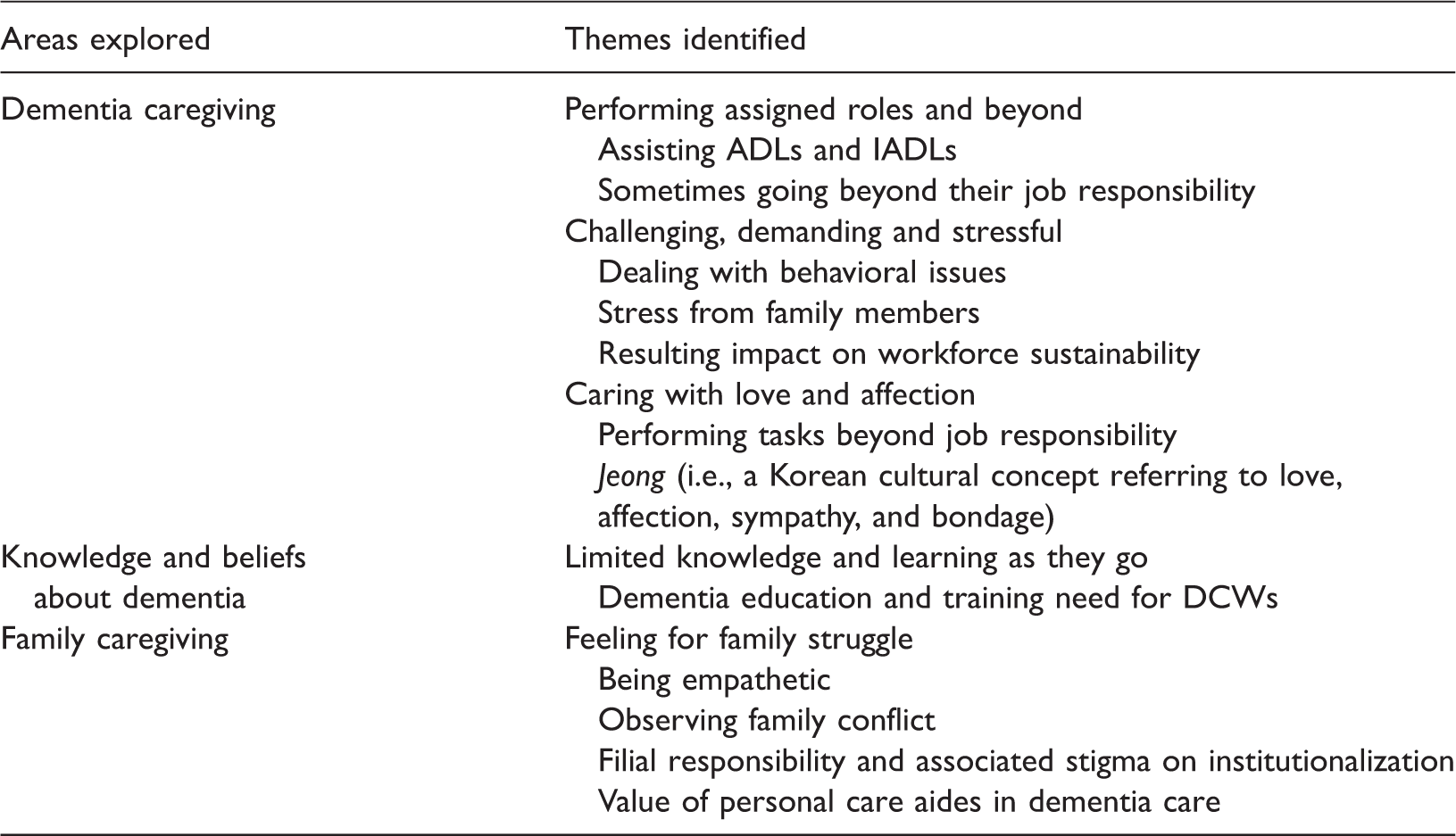
Themes identified in the accounts of Korean American personal care aides of older Korean Americans with dementia symptoms
Results
Dementia caregiving
Performing assigned roles and beyond
In describing the care they were providing, PCAs noted that they were performing assigned roles to their occupation by their hiring home health agencies including assistance with ADL needs (e.g., bathing, dressing, feeding, and using toilet or changing diapers) and supportive work for IADL needs (e.g., shopping, cooking, house cleaning, and laundry). PCAs talked about their assigned roles: “I do cooking and give her bath”; and “I helped them to put clothes on and also feed them. I give them a bath.” One PCA described assisting her client with intimate ADL needs in more detail: “… I wipe her and clean her. When she can’t take care of her urine or feces, I wipe her and cleanse it off. When she could not feed herself, I go up to her bed, and hold and feed her …” PCAs also reported providing companionship, such as spending time with their clients, or often taking them out for a walk. For example, one PCA described the time with her client as “… sometimes I sing her favorite hymns with her and read the bible to her.” Another PCA added, “I am just a friend [to her client].”
In terms of relative importance of their roles and tasks, PCAs frequently spoke of the importance of food in meeting nutritional needs and maintaining physical health of their clients. They shopped for groceries and cooked Korean meals for their clients although they felt that it was not part of their job responsibility. They felt that their clients’ physical health improved because of such nutritional care. For example, one PCA said: I cooked vegetables and she ate it well, and I noticed that her physical health got better because she ate well … when I prepare food and ask her to eat, she doesn’t eat by herself … That client’s family members (also) think her physical health has gotten better. I think if a person eats well, there may be an improvement in their physical health.
Another PCA shared a similar experience: She ate canned food and the milk supplement for seniors, only those, and she did not eat anything else so her physical health was in decline.… when I prepare food … encourage her to eat by saying “it is delicious.” She follows exactly what I eat and where my chopsticks go ….That client’s family members think her physical health has gotten better.
Challenging, demanding and stressful
PCAs often spoke of challenges in dealing with the behavioral issues of their clients that were typical of dementia clients, such as forgetting/not remembering things, repeating over and over, lying, being suspicious about others, hiding things, and wandering out. One participant shared her experience of dealing with forgetfulness and repetition: The more you listen to what patients with dementia say, the more stress you get. Imagine. They say the same thing over and over. I said to her “you said that already” and she says it again. She said “I have to eat now” and I say to her “you already ate.” And when I tell her to eat, she says “I already ate.” Again and again and over and over. It leads to arguments and that gives me stress.
Another participant talked about her frustrating experience with misplacing things and lying, which are typical early-stage symptoms: She couldn’t recognize shampoo and put it in a refrigerator. She put hair lotion on her face …. when I open the fridge, I found shampoo in there. I got so frustrated and also got mad at the family members. I got mad at the client, too. I told her that it is shampoo and took it back to the bathroom, but soon enough it came right back in the fridge. One time when we were looking for her denture, my client kept saying that the next door neighbor stole it. At first, I thought to myself “there are many thieves in this apartment.” But they were all lies (untrue). She placed the denture in a place she thought secure and later she couldn’t remember … so thought that the neighbor stole it. Then later, I found the denture in an empty container for hot pepper paste. One time I was so shocked. It was time for the patient to go to bathroom, but refused to go. And after a while, I smelled something weird. When I asked him (patient), did you use the bathroom?, he said “no and I am not going to go, I don’t have any desire to go.” I told him, “it’s time to go,” and he will say “no, I am not going.” And you know what happened next? He was wearing a Depend [diaper] and because it was uncomfortable, he had put his hands in and then put in on the wall and then he took off his clothes. (big sigh) ‘What would the family have done if they saw this?’ I wanted to run away. After they defecated, they hid it underneath the pillow, so then what’s going to happen?
PCAs recounted providing care for dementia clients as “demanding” and “stressful.” One of the main sources of their stress appeared to be the family of their clients. They often commented on challenges in dealing with family members, mainly because family members had misconception about PCA’s role and often expected PCAs to do things that were, as they described, usually done by a “housemaid.” They noted that because of such high demand and stress, not many KAs who received license for PCAs actually were working as PCA. One PCA explained: People [PCAs] go to work, but they quit because it’s hard to work with families who do not properly recognize the roles of PCA. We are paid just little more than $10 an hour, and even a sandwich maker can earn the same amount of money without this kind of stress and undermined dignity/respect. In the beginning, people started working as a PCA with a good attitude/heart and then they got hurt, so they quit and never went back …. I have seen many KAs who graduated [the PCA training program], but they don’t work as a PCA. They told me it is better to work at a restaurant.
Caring with love and affection
For many PCAs, it seemed that caring for their clients had become personal. Despite their many challenges, PCAs reported caring for their clients beyond their duty because they were concerned for them. PCAs reported often doing things that were not part of the job responsibility of PCA. They shopped for groceries for their clients using their own money, cooked meals for the weekend, cleaned the house and did other household work despite feeling that the type of work was not their job responsibility. In describing their work, a PCA commented on needs of “love” beyond job responsibility: I also think that besides professionalism, a PCA needs love. There is a patient who defecated or urinated on themselves …. Even though I tell her not to touch it, she doesn’t know, so she does it …. Then, she wipes it on towel next to me and it smells and is dirty.… I cannot shout at her …. You need to just remind her not to do it and gently explain to her like “You touch this again. I told you this is yucky yucky (soft and kind voices and tones).” Then I wash her carefully …. If all you have is professionalism [you cannot do that] … there needs to be love. You have to be patient.
Knowledge and beliefs about dementia
Limited knowledge and learning as they go
While all PCAs are trained and certified, they acknowledged limited knowledge about dementia and how to deal with its symptoms when they started working for their clients. They recalled that they had learned very little about dementia in their training. With limited knowledge about AD, PCAs described AD mostly using symptoms they observed in their clients. Although PCAs were aware that AD was a progressive brain disease, they had various misconceptions about the disease. Some PCAs suggested that people with certain personal qualities—such as being “obsessive” or “sensitive”—were more likely to develop dementia. One PCA also suggested emotional state and genetics as possible causes of developing dementia, saying “Usually it may be because of loneliness and not having things to do. I heard that there are a lot of symptoms. I am not sure exactly, but I heard it’s because of genetics, loneliness, depression.”
They reflected learning about the illness and its symptoms through their experience. One PCA reflected: “I didn’t know that [about dementia]. My first time experience with clients was rough and I thought about whether I should continue or not … I learned from my experience and it’s gotten better.” Another PCA also recounted: I didn’t know much details about the disease, so I had a very difficult time when she asked me the same question over and over—like fifteen times …. We need to know more about the disease so we can be more patient while dealing with them. I signed up for a class at night school about Alzheimer’s. I thought I would need that … I think information [about AD] will help me, so I collect informational resources whenever I go to hospitals, like pamphlets and brochures on AD. I think they have helped me a lot.
Family caregiving
Feeling for family struggle
We asked PCAs about their observation of family members providing dementia care. Although some family members of their clients presented additional stress to PCAs, PCAs also expressed their empathy for family caregivers. They remarked that it would be difficult for the family members as, unlike PCAs, it was a 24/7 responsibility for them. PCAs sympathized with the family about what they were going through. One PCA commented: Family members have seen the patients when they had a normally functioning brain, so when the patients change due to dementia, they cannot comprehend it …. Think about it. You lived with this adult who was normal and now all of sudden he acts like a baby. It’s so hard for them to accept that and to live with. It must be terribly hard for them. They would argue like “why don’t you take care, why only I have to do it?” If it’s just one or two years, it’s okay, but when it becomes like 5, 6, 7 years, then conflicts occur within the family … Like the old saying “there is not piety for a lingering illness.” When the disease becomes prolonged, the conflicts get worse.
Discussion
Our focus group study is one of the first studies of KA PCAs providing care for older KAs with dementia symptoms. The study revealed their experience and perspectives of dementia caregiving for KAs in three specific areas: dementia caregiving, knowledge and beliefs about dementia, and family caregiving. While our participants performed tasks ascribed to their roles and responsibilities, dementia caregiving was challenging, demanding and stressful to them as found in DCWs in institutional settings (Scott & Cassie, 2007; Zimmerman et al., 2008). They saw dementia as “the scariest illness” and “most horrible illness.” Experiencing the challenge of dementia caregiving, PCAs expressed empathy for family caregivers who were, unlike them, with 24/7 caregiving responsibility.
Like DCWs in institutional settings (Brodaty, Draper & Low, 2003; Schonfeld, 2003) and dementia family caregivers (e.g., Hinton, Chambers, Valeásquez, Gonzalez, & Haan, 2006; Schoenmakers, Buntinx, & Lepeleire, 2009), PCAs had difficulty with behavioral symptoms of dementia. They expressed that their experience of dealing with those behaviors were more challenging in the beginning because of lack of knowledge about dementia and its symptoms. They acknowledged that they learned very little about dementia in their PCA training and had to learn about the disease through their experience as they cared for their clients. As found in KAs in general (Lee, Diwan, & Yeo, 2010), our PCAs attributed dementia to having certain kind of personalities or not maintaining a stimulating living environment, which can cause unnecessary blame of persons with dementia for bringing the illness. These findings call for an urgent need for dementia training for PCAs in the community setting. In our study, PCAs were equivocal about the need and desire for more education and training about dementia as a part of their regular PCA training. Training about dementia was also identified as one of unmet continuing education needs by DCWs in long-term care settings (Menne et al., 2007). Dementia training is directly related to the quality of care provided and prior training on dementia and better dementia knowledge were identified as predictor of DCWs’ confidence for dementia care (Hughes et al., 2008). Given that the most difficulties KA PCAs experienced were with behavioral issues, trainings should emphasize topics such as how to deal with behavioral symptoms and how those symptoms can change as the disease progresses. In terms of the format of training, DCWs in home health agencies preferred printed materials over interactive learning (such as role playing) and also preferred shorter and frequent sessions over longer and all day sessions. Those preferences are understandable given the nature of their work—for example, home visits in different areas and resulting unpredictable schedules (Menne et al., 2007). Such training reflecting PCAs’ particular needs for contents and modes of delivery will be more efficient and can better prepare PCAs on what to expect in their caregiving demand over the course of the disease.
Dementia training for PCAs can be also helpful for enhancing job satisfaction, which is directly related to chronic turnover and vacancy in the workforce (Seavey, 2011). Our participants corroborated that high demand and stress of PCA tasks resulted in workforce instability. A study shows that DCWs who were better trained on dementia reported more job satisfaction (Zimmerman et al., 2008). Providing initial or continuing dementia training for PCAs can be a small step to address job satisfaction issue at organizational level. As reported by our participants, the demand of dementia caregiving can affect the health of caregiving professionals. Addressing this potential adverse health effects on DCWs, Ejaz and colleagues (2008) note the importance that employers provide programs to reduce DCWs’ stress and strains such as health screening and health promotion. At the same time, a larger effort should be made to address longstanding and pressing issues related to workforce turnover such as low wages and compensation, working conditions, and workload (Seavey, 2011).
Another notable finding is the potential significance of the shared cultural background between service providers and clients, especially in care for ethnic minorities. Given limited proficiency in English for first generation KA immigrants, it is understandable that older KAs and their families prefer to have providers with whom they can communicate. Our study, however, indicates that the significance of having providers with shared cultural background may be beyond just having a common language. PCAs in our study frequently mentioned the jeong (i.e., a Korean cultural concept referring to love, affection, sympathy, and bondage) as they talked about their caregiving experience. Feelings such as compassion for, emotional attachment to, affection on and affective bonding with older clients are expressed by DCWs in institutional LTC settings as the most gratifying part of their job and motivation for remaining in the field regardless of cultural match (Ball, Lepore, Perkins, Hollingworth, & Sweatman, 2009; Brannon, Barry, Kemper, Schreiner, & Vasey, 2007; Dodson & Zincavage, 2007; Parsons, Simmons, Penn, & Furlough, 2003; Sung, Chang, & Tsai, 2005). To our PCAs, a shared Korean background particularly made them feel personally and emotionally closer to their KA clients although some acknowledged difficulty of drawing boundary between their personal and professional feelings. Being Koreans themselves, PCAs developed jeong toward their clients and felt that they understood their KA clients better, could be more patient with them, and sometimes did tasks outside their job responsibility. This concept of jeong seemed to be an important factor that kept PCAs to continue their work despite the challenging work and low pay.
Cultural match between providers and clients has been identified as one of the strategies for culturally competent service delivery (Casado et al., 2015; Lee & Bronstein, 2010). Shared cultural background could mean having the sense of communality where shared values and history render better understanding of and affection toward their clients. In this regard, cultural match could be a potential effective catalyst for formal dementia care in KAs. Additionally, it is reported that emergence of foreign-born workers have generated challenges such as cultural and religious differences, language barriers, and discrimination by clients toward foreign-born workers (Acker et al., 2015; Ejaz et al., 2008). Our results provide some evidence that cultural match may be a potential benefit in developing a trusting client–family–provider relationship, and perhaps crucial for success of formal services for KAs with dementia and their families.
PCAs’ observation of family caregiving illustrates KA cultural norms and responsibility regarding caregiving for old age. Similar to experience shared by KA dementia family caregivers (Casado et al., 2015), PCAs observed strong sense of filial responsibility and resistance to institutional care in KA family. As pointed out by a participant, “sending” their older family members to a nursing home is perceived as not fulfilling their responsibility and can bring shame to the family. At the same time, when the disease prolonged, they observed that conflicts among family members arose over primary caregiving responsibility as evidenced in other studies (Casado & Sacco, 2012; Casado et al., 2015). Although a strong resistance to institutionalization still exists, there is an indication that KAs can be open to using home- and community-based services (HCBS) in dementia caregiving (Lee & Casado, 2011). Yet, KA dementia caregivers reported little use of available HCBS due to lack of knowledge about services and access barriers (Casado et al., 2015). There is a need to raise awareness of and to promote utilization of appropriate HCBS including use of DCWs in KAs that could alleviate family caregiver burden and distress and extend their ability to continue caring for their family members in the community setting.
DCWs in institutional settings reported that conflicts with family members decrease when care expectations are similar between DCWs and family members and they wanted respect and affirmation of their roles as professional caregivers (Abrahamson, Suitor, & Pillemer, 2009; Kemp, Ball, Perkins, Hollingsworth, & Lepore, 2009). Our study also points to the importance of clear expectations related to the role of DCWs in KA families as our PCAs noted stress due to some family members’ misconceptions about their roles, being perceived as a housemaid rather than a paraprofessional worker. When promoting HCBS utilization in KAs, therefore, it would be important to clarify the exact nature of services and responsibility of providers, including PCAs, involved.
It should be noted that this study has several limitations. First, the study was conducted with a small purposive sample of PCAs and, thus, the findings of this study should not be generalized to KA PCAs as a group. Second, our study explored three specific areas identified as important in dementia caregiving literature and there may be other aspects of formal dementia care not touched in our study. Another potential limitation is translation related issues. We used a direct translation–transcription method. Although two bilingual researchers worked independently during the translation process to ensure accuracy, it is possible that certain nuances of language could have been compromised during the process.
Despite these limitations, our study is the first to examine the experience of KA PCAs and provides important insights and suggestions for future research. First, our study suggests that shared cultural background may be an important factor that could help and motivate KA PCAs to continue their work. It would be meaningful to examine whether this phenomenon can be seen in other ethnic groups. Second, while our PCA participants expressed that managing a professional boundary sometimes became difficult due to emotional bonding and affection they had developed with their clients, they did not elaborate on how they could maintain the boundary. It would be worth exploring their trials and efforts of maneuvering the professional boundary with family members in the future research. Lastly, as our study focus was on specific areas of dementia caregiving from PCA’s perspectives, we did not explore their perspectives in other aspects of their work experience, such as experience within their agency environment and work conditions. Given the growing role of foreign-born PCAs and their potential value in long-term care, future study should hear voice of foreign-born PCAs about their experience.
Conclusion
Our study points to the urgent need for dementia training for PCAs. Given the expected increase of older adults with AD, PCAs will encounter more clients affected by the disease. PCAs are well positioned to recognize and report any changes in their clients’ conditions (Seavey, 2011) including warning signs and potential symptoms of dementia, yet this potential role of PCAs are underutilized in our health care system (PHI, n.d.). We believe that training and education about dementia can provide an opportunity to expand and enhance roles that PCAs can play in dementia care. Our study also highlights the significance of culturally competent service delivery in dementia caregiving. Given a shortage of culturally and linguistically competent health care providers for ethnic minorities (Mui, Kang, Kang, & Domanski, 2007), it calls for an outreach effort in ethnic communities in recruitment and training of DCWs who have potential of providing culturally competent care for traditionally underserved ethnic minorities.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The original focus group study was funded by School of Social Work, University of Maryland, USA.