
Abstract
The need for meaningful activities that enhance engagement is very important among persons with dementia (PWDs), both for PWDs still living at home, as well as for PWDs admitted to a nursing home (NH). In this study, we systematically registered behaviours related to engagement in a group animal-assisted activity (AAA) intervention for 21 PWDs in NHs and among 28 home-dwelling PWDs attending a day care centre. The participants interacted with a dog and its handler for 30 minutes, twice a week for 12 weeks. Video-recordings were carried out early (week 2) and late (week 10) during the intervention period and behaviours were categorized by the use of an ethogram. AAA seems to create engagement in PWDs, and might be a suitable and health promoting intervention for both NH residents and participants of a day care centre. Degree of dementia should be considered when planning individual or group based AAA.
Background
Worldwide estimates count 47.5 million persons with dementia (PWDs) today (World Health Organization (WHO), 2015). A range of health care services is needed for this group, from home-based services and respite care such as attending a day care centre (DCC) to residential care at a nursing home (NH). In Norway, about half of the total population of PWDs live in their own home (Lystrup, Lillesveen, Nuygård, & Engedal, 2006) and the most frequent unmet need for home-dwelling PWDs are daytime activities (Miranda-Castillo et al., 2010). DCCs are established to provide meaningful activities for home-dwelling PWDs and, at the same time, provide relief to family carers (Norwegian Ministry of Health and Care Services, 2015; Söderhamn, Aasgaard, & Landmark, 2014; Söderhamn, Landmark, Eriksen, & Söderhamn, 2013). About 20% of the dementia population in Norway who live at home attend a DCC once or twice a week (Vossius et al., 2015). Experience of attending a DCC is found to provide social fellowship, meaningful engagement, a sense of meaningful life and well-being (Brataas, Bjugan, Wille, & Hellzen, 2010). For PWDs at NHs, the need for meaningful activities that enhance engagement is equally important, as NH residents are frequently reported as participating in few activities and to be unoccupied most of the day (Smit, de Lange, Willemse, Twisk, & Pot, 2015). A high prevalence of inactivity, apathy and sedentary behaviour is commonly reported (Bates-Jensen et al., 2004; MacRae, Schnelle, Simmons, & Ouslander, 1996), and having an opportunity to participate in activities and activities that amount to something is important for increasing a sense of independence and positive self-image (Allen, 2011). During periods of activity, NH residents with dementia express positive affects much more often than during the periods of inactivity (Schreiner, Yamamoto, & Shiotani, 2005).
Engagement may be defined as “the act of being occupied or involved with an external stimulus” (Cohen-Mansfield, Dakheel-Ali, & Marx, 2009). For both home-dwelling PWDs and PWDs in NHs, engagement may prevent and improve behaviour problems and increase alertness, reduce boredom and agitation, increase positive emotions (Cohen-Mansfield, Thein, Dakheel-Ali, & Marx, 2010) and enhance quality of life (QoL) (Smit et al., 2015).
Animal-assisted interventions (AAIs) have become a regular activity in NHs and among dementia patients (Bernabei et al., 2013; Cohen-Mansfield, 2001). AAI is “a goal oriented and structured intervention that intentionally includes or incorporates animals in health, education and human service for the purpose of therapeutic gains in humans” (International Association of Human-Animal Interaction Organizations (IAHAIO), 2014). Animal-assisted activities (AAAs) is a sub-discipline of AAI, e.g. visits by dogs and their handlers for ‘meet and greet’ activities (IAHAIO, 2014). AAAs are usually conducted on a voluntary basis by individuals who do not have an education in health or a degree in human services, but they may also work formally and directly on specific documentable goals (IAHAIO, 2014).
Research in the AAI field is increasing, and studies have already documented the beneficial effects of AAI for elderly persons and PWDs in relation to agitation, depression, QoL, social interaction, loneliness, balance, etc. (Bernabei et al., 2013; Filan & Llewellyn-Jones, 2006; Friedmann et al., 2015; Majic, Gutzmann, Heinz, Lang, & Rapp, 2013; McCabe, Baun, Speich, & Agrawal, 2002; Olsen, Pedersen, Bergland, Enders-Slegers, & Ihlebæk, 2016a; Olsen, Olsen, Pedersen, Bergland, Enders-Slegers, Patil et al., 2016b; Perkins, Bartlett, Travers, & Rand, 2008; Richeson, 2003).
The conceptual framework devised by Cohen-Mansfield et al. “the Comprehensive Process Model of Engagement” (2009) may be used to understand some of the aspects of AAI, and to provide a link between the activity and the outcomes seen in studies of this group. The model claims that engagement with a stimulus is affected by environmental characteristics, the participant and the stimulus itself.
Environmental characteristics are described as surroundings, such as time, place, number of people present and temperature, as well as the manner of stimulus presentation. In an AAI intervention, this can refer to the design of the intervention, including group vs. individual intervention, as well as how the sessions are utilised. Participant characteristics constitute cognitive function, demographic characteristics, general level of activity and interest. These are all aspects that influence interaction with the dog as well as its handler in an AAI. Stimulus characteristics such as social vs. non-social, and human vs. non-human may influence the level of engagement. In an AAI, the dog serves as an adjunct for the handler, who represents the social human dimension in addition to the live, social, non-human attributes of the dog. The model further explains how environmental characteristics, participant characteristics and stimulus characteristics create engagement and have an impact on the participants’ affect and behaviour (Cohen-Mansfield et al., 2009). By reducing boredom and loneliness and increasing interest and positive emotions, the change in the level of engagement is found to influence problem behaviours such as agitation (Cohen-Mansfield et al., 2009; Cohen-Mansfield, Libin, & Marx, 2007).
Direct observation of engagement has been used to assess levels of engagement among PWDs (Cohen-Mansfield et al., 2009; Cohen-Mansfield, Marx, Dakheel-Ali, Regier, & Thein, 2010; Cohen-Mansfield, Thein, Dakheel-Ali, Regier, & Marx, 2010). In the Comprehensive Process Model of Engagement, engagement is measured according to five dimensions, which are: rate of refusal of the stimulus; duration of time the participant was occupied or involved with a stimulus; level of attention to the stimulus (e.g. facial feedback, eye tracking); attitude towards the stimulus (e.g. smiles, laughs, negative facial expressions); action towards the stimulus (e.g. holding it or talking to the stimulus itself or another resident) (Cohen-Mansfield et al., 2009). A few observational studies have reported on behaviours occurring among the participants during human–animal interaction (Cohen-Mansfield, Thein, Dakheel-Ali, Regier, & Marx, 2010; Hauge, Kvalem, Pedersen, & Braastad, 2013; Marx et al., 2010; Pedersen, Nordaunet, Martinsen, Berget, & Braastad, 2011), but there is still a need for more knowledge about AAI in terms of engagement among PWDs. The main objective of this study was to systematically register behaviours related to engagement in a group AAA intervention for PWDs in NHs and among home-dwelling PWDs attending a DCC, and a second aim was to investigate possible differences between the two populations.
Methods
Design and research sites
The study was conducted as part of two cluster randomized controlled trials (RCTs) (Olsen, Pedersen, Bergland, Enders-Slegers, & Ihlebæk, 2016a; Olsen, Pedersen, Bergland, Enders-Slegers, Patil et al., 2016b). In the RCT trials, the intervention was found to have a positive effect on depression, balance and QoL (Olsen, Pedersen, Bergland, Enders-Slegers, & Ihlebæk, 2016a; Olsen, Pedersen, Bergland, Enders-Slegers, Patil et al., 2016b). In the present study, only data from the intervention groups were used, as no observational data from the control groups were collected. The project is registered in ClinicalTials.gov (identifier: NCT01998490 and NCT02008630), a service of the US National Institutes of Health.
Out of 90 eligible NHs, 10 adapted NHs for PWDs in the Norwegian counties: Østfold, Vestfold, Oslo and Akershus agreed to participate in the project. In addition, 16 (out of 108) adapted DCCs for home-dwelling PWDs were recruited to the project. The institutions included had to ensure that they had the facilities required to carry out this kind of intervention. They had to abstain from any dog-visiting activities for three months prior to the intervention, as well as any other dog-visiting activities during the intervention period and three months after the end of the intervention.
After randomisation, each institution was given the opportunity to recruit 5–8 participants. The inclusion criteria were: being 65 years of age or older, having dementia or a cognitive deficit measured as a score of less than 25 on the Mini-Mental State Examination (MMSE) (Folstein et al., 1975; Strobel & Engedal, 2009). The exclusion criteria were: people afraid of dogs or with an allergy to dogs.
The possible benefits of a 12-week intervention with AAA for PWDs were studied. Groups of AAA were videotaped early and late in the intervention, and different behaviours that occurred during the filming were systematically mapped.
Sample
A total of 58 NH participants and 80 DCC participants agreed to participate in the RCT project. The control group included 30 NH participants and 38 DCC participants while 28 NH participants and 42 DCC participants were included in the intervention group, which is the population in this study. The deaths of three NH residents excluded them from the analyses. One of the DCC participants withdrew from the intervention and was therefore excluded. Participants who were only present at one of the video-recordings were also excluded from the analyses (n = 4 NH participants and n = 13 DCC participants). Thus, the study population consisted of 21 NH participants and 28 DCC participants.
Intervention and intervention content
The intervention consisted of 30-minute AAA sessions twice a week for 12 weeks in groups of 3–7 participants. The AAA sessions were led by a qualified dog handler. A protocol for conducting AAA sessions ensured equal intervention sessions between units. The protocol was deliberately designed to be able to standardise the intervention as much as possible, both across sessions and across the different institutions. The time span of 30 minutes was chosen due to the short attention span typical of dementia.
For each session, the participants were randomly seated in a semicircle. Every session started with a greeting round, where each participant got to pet the dog and give it treats. The handler then started the different activities, which could be: petting the dog, giving the dog a treat or throwing a toy for the dog to fetch. The programme theory underpinning the protocol was based on several principles, such as dementia knowledge, AAI competence and health care workers’ knowledge of the patients. Even though the sessions were designed to follow the protocol, they could also be individually tailored. No activities were mandatory, and the sessions included activities that naturally occurred between the participants, and between each participant and the dog. A health care worker was present during all sessions.
Dogs and their handlers
In an AAI the dog serves as an adjunct to the dog handler. Therefore, both the dogs and their handlers, who were also the dogs’ owners, were carefully selected for the study.
The dogs had to conduct and pass a screening test containing different elements according to their suitability. Different traits, such as aggressiveness, sociability, anxiety and the dog’s behaviour when handled, were assessed by dog trainers and ethologists at the Norwegian Centre of Anthrozoology. In this study, all the handlers were female, and most of them had either a bachelor’s degree or prior experiential learning in biology or social care. Both dogs and handlers then had to complete at least one course in AAI for visiting dogs. All the handlers were informed both orally and in writing about the protocol for the sessions in order to increase similarity between sessions and institutions.
Several different breeds of dogs were involved, most of them were large breeds: Standard Poodle (N = 2), Collie (N = 2), Flat Coated Retriever (N = 1), Golden Retriever (N = 1), Alaskan Malamute (N = 1), Border Collie (N = 1), Springer Spaniel (N = 1), Portuguese Water Dog (N = 1), Pomeranian (N = 1) and Shetland Sheepdog (N = 1), Mix (N = 4). There were seven male (one neutered) and nine female dogs. Their ages varied between 2.5 and 13 years old, with an average age of 5.6 years. The dogs were kept both on and off a lead, depending on the interaction. No dogs were forced to do anything they were not comfortable doing and no activities were mandatory for the participants.
Assessments and procedures for data collection
The MMSE was used if a dementia diagnosis had not been made, the Clinical Dementia Rating (CDR) Scale and sociodemographic characteristics on age, gender, education, use of walking aids, social contact, hobbies and animal contact were collected at baseline by pre-trained health care workers working in the units. The video-recordings were carried out early (week 2) and late (week 10) during the intervention period.
The MMSE was used to assess global cognition for patients not yet diagnosed with dementia. The MMSE consists of 20 items concerning orientation, word registration and recall, attention, naming, reading, writing, following commands and figure copying. Scores between zero and 30 are assigned, where a higher score indicates better performance (Folstein et al., 1975). A cut-off score of 24–25 is related to cognitive impairment and is said to provide a reliable diagnosis of dementia. Although this cut-off score is not valid for younger individuals and highly educated individuals, where a higher cut-off should be applied (O'Connor, Pollitt, Treasure, Brook, & Reiss, 1989), it should be considered valid for our population of older adults with a moderate level of education and it was therefore applied.
The CDR Scale is a five-point scale used to assess six domains of cognitive and functional performance applicable to dementia (Engedal & Haugen, 1993; Hughes et al., 1982; Nygaard & Ruths, 2003). CDR staging is a valid substitute for a dementia assessment among NH residents to rate dementia and determine the severity of dementia (Engedal & Haugen, 1993; Nygaard & Ruths, 2003). A CDR of 0 implies no cognitive impairment, 0.5 = very mild dementia, 1 = mild, 2 = moderate and 3 = severe dementia.
The video-recordings were standardised, using a camera Sony HXR-NX30E, a camcorder recording full HD with Balanced Optical SteadyShot™ and a tripod VCT-PG11RMB. The camera was placed in the room before the participants arrived to avoid interference with the intervention. The recordings were done by members of the project group, who were all trained in where to place the camera in the room and how to behave and introduce the camera to the participants. All of the participants were told that the camera was on, and they had signed a written consent beforehand. The camera was placed in the room so the camera eye could record participants, the dog and the handler at all times.
An ethogram, which is a catalogue of behaviour descriptions (Martin & Bateson, 1986), was used to categorise the different behaviours from the video-recordings. The ethogram provides an objective description of the different behaviours that occur in the intervention, and has previously been used in other studies of human–animal interaction (Berget, Skarsaune, Ekeberg, & Braastad, 2007; Hauge et al., 2013; Pedersen et al., 2011).
Ethics
The project was conducted in accordance with the Helsinki Declaration and was approved by the Regional Committee for Medical Research Ethics. Participants were aware of the conditions for their participation, since the randomisation was done at institutional level. A procedure was developed to evaluate the participants’ capacity to provide informed written consent, which was obtained by pre-trained health care workers. PWDs with sufficient capacity were informed about the project and asked to provide written consent. For participants with reduced capacity, health care workers and/or the next-of-kin made the decision on behalf of the elderly and provided proxy written consent. The written consent contained information about the project, the intervention, different assessments (including the fact that they would be videotaped) and the possibility to withdraw from the project at any time. In addition, participants were informed about the video-recordings the day before recording and on the day the session was to be recorded.
Video analyses
Ethogram.
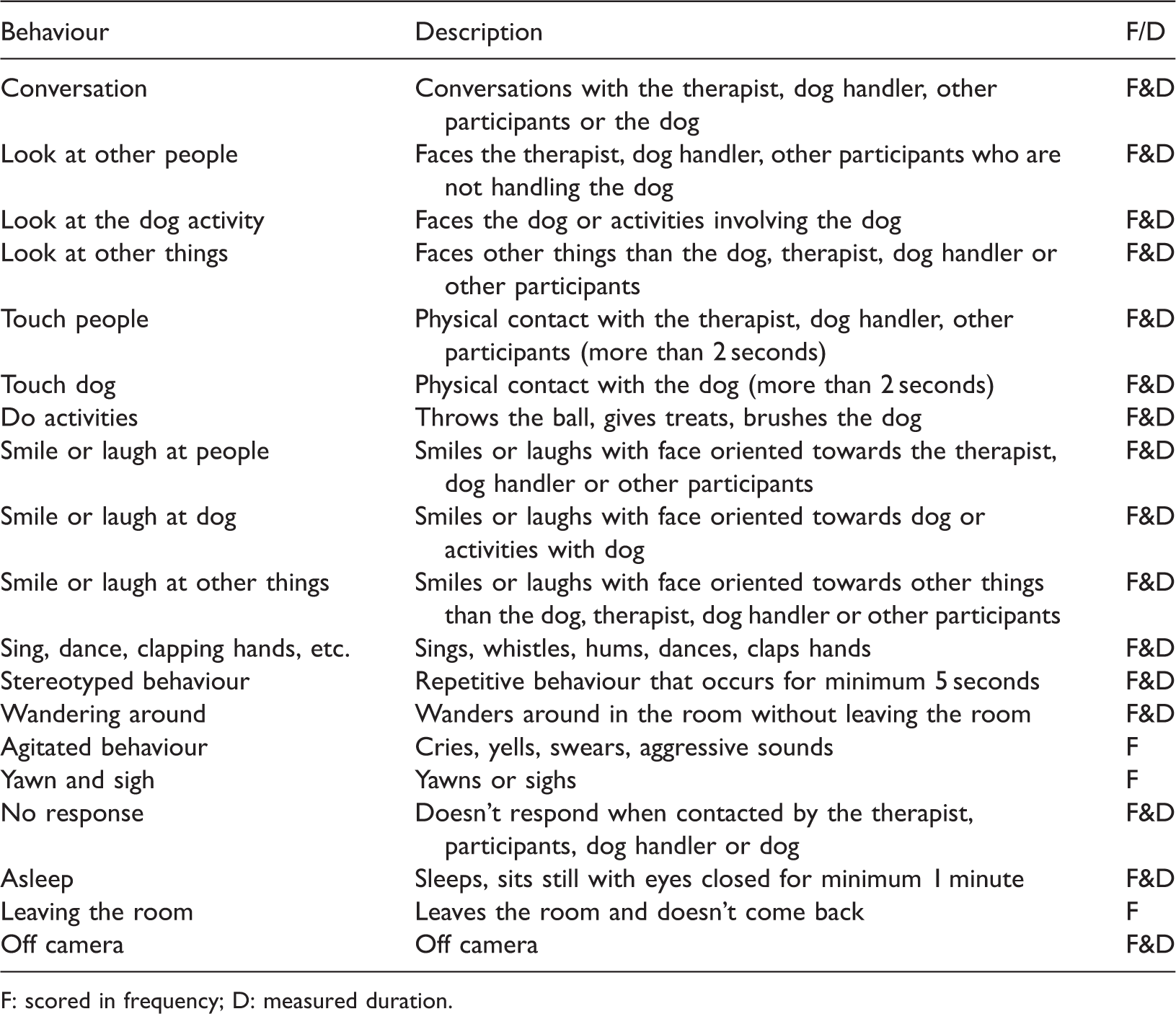
F: scored in frequency; D: measured duration.
The videos were randomised between the observers, and then analysed in a random order, so there was no dependence on whether the recordings were done early or late in the intervention.
For one recording of a group of five participants, the video was analysed five times, registering behaviours for each participant at a time.
Intraclass correlation coefficient
To test the level of agreement between those rating the video-recordings, they all blindly analysed the same two videos. The intraclass correlation coefficient with a Two-Way Mixed model and Absolute Agreement showed a mean average measure of 0.9, range 0.76–1.0. The mean single measure was 0.71, range 0.45–0.98. Values between 0.75 and 1.0 are considered excellent inter-rater reliability (Hallgren, 2012).
Statistics
All analyses were computed using the statistical software IBM SPSS Statistics for Windows, Version 23.0. Armonk, NY: IBM Corp. An analysis of variance (ANOVA) was used to test the differences in means between groups.
Descriptive statistics were used to present demographic data using frequency distribution. Video registrations in Solomon Coder were imported into SPSS for further calculation. Time was registered in seconds. Time off camera was subtracted from the total time for each participant, and, due to differences in the total time of each session, the percentage of total time for each behaviour was calculated. Since there were only minor differences in durations or frequencies of the behaviour from early to late in the intervention period, a mean value for both recordings was calculated and serves as descriptive data for this study (Table 3).
The degree of dementia was previously found to influence the effects of AAA in PWDs (Olsen, Pedersen, Bergland, Enders-Slegers, Patil et al., 2016b). Consequently, we stratified all participants into level of CDR (0, 0.5 and 1 = mild, 2 = moderate and 3 = severe), and compared means.
Results
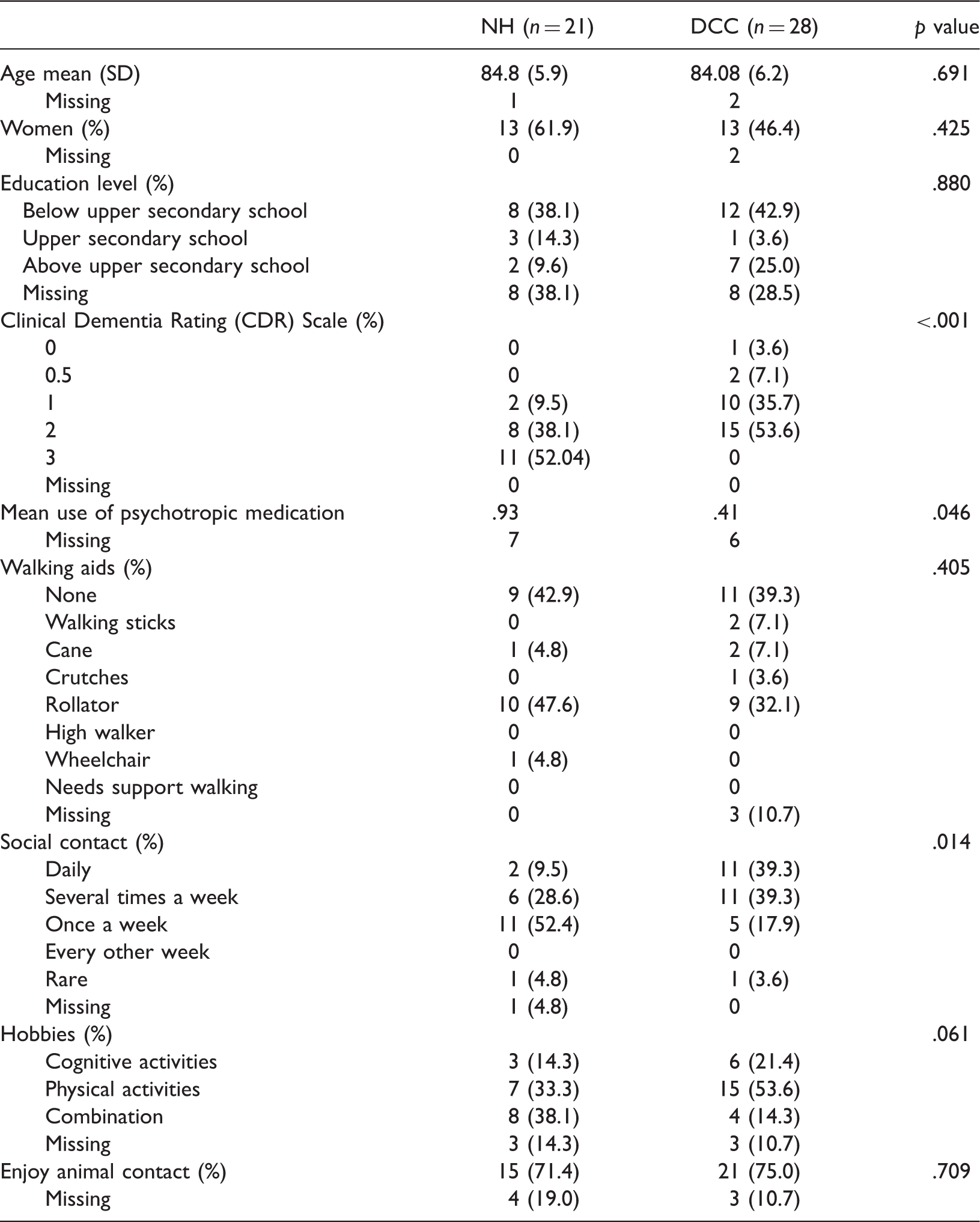
Sociodemographic characteristics.
Mean time spent as percentage of total time of the session on Different Behaviours (SD).

Only four of the NH participants did not have a dementia diagnosis, and the mean MMSE for these participants was 15.3 (SD = 6.7, range: 7–23). For DCC participants, the mean MMSE for the eight participants without a dementia diagnosis but with a MMSE score was 18.4 (SD = 6.2, range: 8–26). Around 40% of participants in both groups did not use any walking aids, however, 47.6% of NH participants used a rollator (32.1% of DCC participants), and one NH participant used a wheelchair. The participants were somewhat engaged in hobbies, but DCC participants were more engaged than NH participants in physical activities. The majority of the participants reported that they enjoyed contact with animals (>70%) (Table 2).
There was a significant difference in the degree of dementia between NH participants and DCC participants (p < .001), as the majority of NH participants had a score of severe dementia (52%), while none of the DCC participants were assessed as having severe dementia, and the majority of DCC participants had moderate dementia (53.6%) (Table 2). NH participants showed significantly higher use of psychotropic medication than DCC participants. Most participants had regular social contact, with over 90% of both populations meeting family or friends at least once a week. However NH participants still had significantly less social contact.
Behaviours targeting either the dog or other people had the highest mean percentage times. These behaviours were: Look at dog-activity; Smile or laugh at dog; Conversation; Look at other people; Touch dog; Do activities with dog; Touch people; Smile or laugh at people. Mean values showed that actions towards the dog, such as observing it, smiling, talking to it or petting it, were the behaviours with the longest duration in AAA sessions in both populations (Table 3). Since this intervention was conducted as a group activity, time spent in contact with the dog had to be equally divided between the participants, which limited direct contact with or being able to do activities with the dog to 5–6 minutes for each participant. Most of the participants utilised that time to the full, and the mean time spent petting the dog was around 10% of the total time for participants at both NHs and DCCs. There was a small amount of stereotyped behaviour, and some of the NH participants occasionally slept during the session (Table 3). There were surprisingly few differences between the two populations; NH participants spent significantly less time smiling or laughing, and engaged less in conversation. They also spent more time asleep compared to DCC participants (Table 3).
When comparing the participants stratified by degree of dementia (CDR), we also found only a few differences in behaviours. Participants with severe dementia slept (mean = 15.3 %, SD = 24.7) significantly more (F = 6.60, p = .003) than those with mild (mean = .3%, SD = .99) or moderate (mean = 1.2%, SD = 2.61) dementia, and they spent significantly less time (F = 6.74, p = .003) looking at the dog-activity (mean = 60.7%, SD = 22.63) than those with mild (mean = 77.7%, SD = 10.3) or moderate (mean = 78.8%, SD = 10.42) dementia (stratified data not shown in table).
Discussion
In this study, few behavioural differences were found between NH participants and DCC participants during AAA, even though there was a significant difference in the degree of dementia between NH participants and DCC participants. There were also significant differences in the use of psychotropic medication and social contact, where NH participants had higher use of psychotropic medication and significantly less social contact than DCC participants. Behaviours targeting either the dog or other people had the highest mean percentage times, and actions towards the dog, such as observing it, smiling, talking to it or petting it, were the behaviours with the longest duration in AAA sessions in both populations. NH participants spent significantly less time smiling or laughing and engaged less in conversation. They also spent more time asleep compared to DCC participants. Participants with severe dementia slept significantly more than those with mild or moderate dementia and they spent significantly less time looking at the dog-activity than those with mild or moderate dementia.
According to the Comprehensive Process Model of Engagement by Cohen-Mansfield et al. (2009), environmental characteristics are one of three dimensions affecting the impact of a stimulus. In this study, the team of dog and handler constitute the stimulus, and the group activity design was an important environmental factor that could influence the participants’ attention towards the dog. One of the purposes of the group activity design was to facilitate social interaction between the participants. It is suggested that group activities in which the participants themselves can influence the development of the activity are most effective (Cattan, White, Bond, & Learmouth, 2005). In AAA, voluntary participation is a key factor, as no activities are mandatory. The participants interact with the dog, the dog handler and the other participants in whatever way and to the extent they choose. They can sit and simply observe, they can respond to the contact initiated by the dog, they can try to engage the dog themselves, they can observe the social interaction between the other group members or they can choose to actively interact with the others. Group activities are found to create a sense of belonging, and the group represents a secure environment that contributes to strength, inspiration and joy (Sundsteigen, Eklund, & Dahlin-Ivanoff, 2009). The results show that in addition to being engaged with the dog, social interaction with the dog handler and other participants also had high durations. The participants looked at other people, smiled to them and talked with them. The dog in AAA has previously been reported to have a social catalyst effect (Beetz, Uvnas-Moberg, Julius, & Kotrschal, 2012), and reviews on AAI on PWDs have concluded that this kind of intervention may increase social behaviour and interaction (Bernabei et al., 2013; Filan & Llewellyn-Jones, 2006; Perkins et al., 2008). Other environmental characteristics that could be important in this study were time and place. To ensure predictability for the participants, the institutions were asked to make a room available for the intervention away from other activities or people, and that the same room be used for all sessions. The location was therefore familiar to the participants. Predictability was also ensured by sessions always being held from between 12:00 and 13:30, just before dinner time.
The second factor influencing a stimulus according to the Comprehensive Process Model of Engagement (Cohen-Mansfield et al., 2009) is personal attributes. Important attributes that may affect stimuli and the level of engagement in this study could be interest in animal contact, degree of dementia and use of medication. The overall level of interest in the dog probably reflects the fact that the majority of the participants stated that they enjoyed contact with animals before the intervention period started. Participants with severe dementia slept significantly more than those with mild or moderate dementia, and were less attentive towards the dog. It has previously been reported that persons with severe dementia engage less in activities than those with mild or moderate dementia (Smit et al., 2015). Furthermore, the use of psychotropic medication is known to be associated with apathy (Tripathi & Vibha, 2010). Moreover, all participants with severe dementia were NH residents, and it is reported that institutionalised PWDs are sedentary most of the time (Król-Zielińska, Kusy, Zieliński, & Osiński, 2010; Salguero, Martinez-Garcia, Molinero, & Marquez, 2011).
The last important factor in the model is stimulus attributes. In this intervention, the social attributes of the dog may affect the participants’ level of engagement. Dogs and humans share prosocial qualities of social competence, and some aspects of dogs’ social competence can be considered to function similarly to that of humans (Miklosi & Topal, 2013). For instance, dogs can recognise human emotions (Albuquerque et al., 2016), and humans represent dogs’ emotions in a somewhat similar way to their own (Konok, Nagy, & Miklósi, 2015). In this study, we deliberately chose to use different breeds of dogs. This was done to reduce the individual effect of the dog, as it has been found that participants show different levels of engagement towards the dog depending on the size/breed (Marx et al., 2010). The level of engagement has been found to be highest in responses to live social stimuli (Cohen-Mansfield, Marx, Thein, & Dakheel-Ali, 2011), and compared to a similar study with the social robot seal Paro (Joranson et al., 2016), participants looked at the dog-activity 1.4 times more than participants looked at Paro. In AAA, the dog serves as an adjunct, so it is actually the dog and handler dyad that acts as a stimulus. In many ways, the qualities of the handler are as important as the qualities of the dog. In a group activity, the dog handler has to be attentive to the needs of each individual, and not only the participants, but also the dog. This requires major skills and experience, as the dog handler must be able to identify the needs and mediate the intervention to be suitable for all participants involved, while also ensuring it is individually tailored. Appropriate guidance on interacting with stimulus is important to be able to benefit from the activity, and individual tailoring increases the effectiveness of the stimuli even more (Leone, Deudon, Piano, Robert, & Dechamps, 2012).
All the factors discussed above interact to create engagement during an activity and one of the model measurement dimensions is duration of time, i.e. how long the participant was occupied or involved with a stimulus. In this study, the behaviours; Look at dog-activity; Smile or laugh at dog; Touch dog; Do activities with dog could be regarded as involvement with a stimulus. Thereby demonstrating that the participants were able to engage in the AAA. The dog clearly had the participants’ attention, as they spent six times as much time looking at the dog than other people or other things. As the abovementioned behaviours showed the longest duration in the AAA sessions, it could be claimed that the activity creates engagement. The high degree of involvement, as well as indications of a positive attitude (high level of smiles and laughter) which is another dimension in the model, further implies that the intervention created engagement among all participants. There are a few notable exceptions however; DCC participants showed more behaviours like smiling or laughing at the dog, were engaged in more conversation and slept less during the session. This may be related to the significantly lower degree of cognitive loss and less use of medication.
The conceptual framework model declares that engagement can subsequently result in a change in affect that may influence the presentation of behavioural problems (Cohen-Mansfield et al., 2009). Consequently, the engagement shown in this study can be associated with the results of our previous study (Olsen, Pedersen, Bergland, Enders-Slegers, Patil et al., 2016b), where we, in line with other studies, found AAA to have an effect on depression in NH participants with severe dementia (Friedmann et al., 2015; Majic et al., 2013; Olsen, Pedersen, Bergland, Enders-Slegers, Patil et al., 2016b). In the current study, the registered data show that participants smiled about 20% and 30% of the time. Although we did not investigate differences in mood over time, improved mood through interaction with a dog has been found earlier (Marcus et al., 2013).
Engagement in activities beyond routine care is an important indicator of QoL in NHs. Having the possibility to participate in activities and activities that amount to something is important for increasing a sense of independence and positive self-image in NH residents (Allen, 2011). Change in affect and behaviours as stated in the model are key factors related to QoL among elderly PWDs, and it is plausible that an activity that enhances engagement could influence QoL as seen in the study by Olsen, Pedersen, Bergland, Enders-Slegers, Patil (2016b). Improving QoL has been identified as one of the primary goals of dementia treatment (Logsdon, McCurry, & Teri, 2007), and a significant improvement in QoL among NH residents was also previously found after being part of an AAI (Nordgren & Engstrom, 2014). Both NH residents and home-dwelling PWDs have been found to have a series of unmet needs, such as a need for social contact, sensory stimulation and a need for a meaningful activity (Cohen-Mansfield, Dakheel-Ali, Marx, Thein, & Regier, 2015). It is likely that an intervention such as AAA answers these kinds of needs to some extent, as these data show that the participants from both residences spend a lot of time displaying social behaviours, including touching the dog or other people. Furthermore, there is a need for new and innovative approaches to traditional health care, and activities that enhance engagement may have a great impact on PWDs’ QoL (Smit et al., 2015). Our study indicates that AAA could be a basis for creating such engagement.
Strengths and limitations
This study has several strengths and weaknesses that need to be taken into consideration when interpreting the results. Using ethograms provides an opportunity to objectively study the behaviours that occur in an intervention. The behaviours that were to be measured were clearly and unambiguously defined after pre-watching the videos, making them easily understood by the different observers. A detailed description was written before the analysis started. However, a limitation of ethograms is that not all members of a group studied behave in the same way (Martin & Bateson, 1986), making it possible to miss some important information that may have been picked up using qualitative methods. Using video-recordings could constitute a limitation if the participants’ awareness of the camera made them more self-conscious and that this influenced their behaviour. However, study participants are generally found to forget the camera and behave normally as soon as the activity has started (Malterud, 2011).
Another limitation to the study is that we had limited knowledge on comorbid somatic diagnosis, which may affect behaviour. Furthermore, we had no information on behavioural and psychiatric symptoms, such as agitation and depression among DCC participants. It is reasonable to assume that the NHs residents had poorer health in general, as indicated by the significant differences between the groups in psychotropic medication and use of walking aids, and the few differences in behaviour reported may be due to this. It could be that the groups of participants should be more homogenous regarding gender, age, physical and cognitive function, in order for the AAA to be better suited for all participants in the group. Or it may be that severe dementia patients would benefit more from individually based AAA, as one-on-one socialising is found to give the highest ranking for duration, attention and/or attitude towards a stimulus (Cohen-Mansfield, Marx, Dakheel-Ali, Regier, & Thein, 2010). The significant standard deviation found for time spent on the different behaviours within the two populations could also indicate that AAA needs to be tailored to the individual patients. However, the few differences in behaviour seem to indicate that the group AAA created engagement in both groups.
Conclusion
Based on the high duration of behaviours related to the dog activity, and indications of positive attitudes with a high level of smiles and laughter, AAA seems to create engagement in PWDs both among NH residents and among participants of DCCs. AAA may be a suitable and health promoting intervention for both NH residents and users of DCCs. The degree of dementia should be considered when planning individual or group-based AAAs. Activities should be tailored to the participants’ needs and interests. A flexible schedule and provision of resources and accommodation are also imperative to engage participants in their preferred activities despite limited functioning.
Footnotes
Acknowledgements
We extend our sincere thanks to the participants and the dogs and their handlers. We would also like to thank cooperating partners, institutions and health workers.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The first-named author owns a share in the Norwegian Centre of Anthrozoology, which was a partner in the study project.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: grant no. 217516 from the Oslofjordfondet and RFF Hovedstaden, NMBU, and cooperating partners (The Norwegian Centre of Anthrozoology, Buskerud and Vestfold University College, Centre for Development of Institutional and Home Care Services in Vestfold and Nøtterøy Municipality). Cooperating partners supported the project with internal financing.