
Abstract
This study examined the effect of a Multicomponent Training (MT) intervention on cognitive function, functional fitness and anthropometric variables in institutionalized patients with Alzheimer’s disease (AD). Thirty-seven institutionalized elders (84.05 ± 5.58 years) clinically diagnosed with AD (mild and moderate stages) were divided into two groups: Experimental Group (EG, n = 19) and Control Group (CG, n = 18). The EG participated in a six-month supervised MT program (aerobic, muscular resistance, flexibility and postural exercises) of 45–55 minutes/session, twice/week. Cognitive function (MMSE), physical fitness (Senior Fitness Test) and anthropometric variables (Body Mass Index and Waist Circumference), were assessed before (M1), after three months (M2) and after six months (M3) of the experimental protocol. A two-way ANOVA, with repeated measures, revealed significant group and time interactions on cognitive function, chair stand, arm curl, 2-min step, 8-foot up-and-go (UG), chair sit-and-reach (CSR) and back scratch tests as well as waist circumference. Accordingly, for those variables a different response in each group was evident over the time, supported by a significantly better EG performance in chair stand, arm curl, 2-min step, UG, CSR and back scratch tests from M1 to M3, and a significant increase in MMSE from M1 to M2. The CG’s performance decreased over time (M1 to M3) in chair stand, arm curl, 2-min step, UG, CSR, back scratch and MMSE. Results suggest that MT programs may be an important non-pharmacological strategy to improve physical and cognitive functions in institutionalized AD patients.
Introduction
The world’s population is ageing at an exponential rate, accompanied by an increase of age-related pathologies (Castro-Caldas & Mendonça, 2005) such as dementia and Alzheimer’s disease (AD). The World Health Organization (WHO) estimates that 47.5 million people worldwide are living with dementia, a figure that might increase to 75.6 million by 2030, and to 135.5 million by 2050 (WHO, 2015). In Europe, 8.7 million people lived with dementia in 2012, including 182,526 Portuguese citizens (Alzheimer Europe, 2013). AD is the most common cause of dementia and may contribute to 60–70% of cases. After age 65, the risk of this neurocognitive disorder doubles every five years (Prince et al., 2013).
The benefits of moderate exercise in relation to chronic degenerative diseases are well known (Barnes et al., 2007), contributing towards the prevention and reduction of morbidity and mortality of the elderly (Barnes et al., 2007). Regular exercise reduces vascular risk, obesity, levels of inflammation markers and it improves metabolism (Rovio et al., 2005). Besides improving general health status, strong evidence shows that functional fitness and cognitive function in older adults can be improved by regular physical activity (Heyn, Abreu, & Ottenbacher, 2004).
Functional fitness is universally accepted as an indicator of health status and quality of life in older adults (Justine, Hamid, Mohan, & Jagannathan, 2011). It comprises aerobic capacity, muscle strength, and static/dynamic balance agility and flexibility (Justine et al., 2011). During the aging process, there is a natural decline of physical functioning that is amplified by the progression of AD, including the loss of ability to perform Activities of Daily Living (ADLs), thus leading to higher levels of dependency (Noro & Aro, 1996).
Due to cognitive-behavioral functioning impairment and compromised ability to perform ADLs inherent to AD progression (Melrose et al., 2011), older adults with AD tend to lose their autonomy. This has devastating consequences for both the diagnosed individual and the entire family, who both are no longer able to cope with these demands. As a result, patients often require institutionalization (Brodaty et al., 2014). Usually, institutional settings lack physical activity opportunities, a situation that further emphasizes the decline of functional fitness contributing in turn to a faster progression of AD.
Although there are a growing number of publications on exercise programs for people with dementia, the studies reveal a wide variety of methodologies applied to different stages of dementia, resulting in inconsistent or even contradictory outcomes (Heyn et al., 2004).
The majority of studies have assessed the effectiveness of aerobic training on cognitive function and brain health. The literature points out that aerobic training can increase blood flow in the brain and regulate neurotrophic factors which, in turn, have been associated with improvements of cognitive functions, neurogenesis, angiogenesis and brain plasticity (Rovio et al., 2005). Aerobic training is also associated with higher cortical tissue on the temporal, parietal and frontal lobes, which are the key areas associated with cognition (Colcombe & Kramer, 2003) and brain activation patterns (Voss et al., 2011). Fewer exercise intervention studies have examined the effects of resistance training on cognitive function. However, there is some evidence that resistance-only training contributes to functional plasticity in brain regions associated with executive function and increased levels of IGF-1, thought to be related to the preservation of cognitive function (Cassilhas et al., 2007).
Thus, Multicomponent Training (MT), 1 such as combined aerobic exercise and strength training programs, may have a larger effect on cognition than aerobic or resistance training alone (Kirk-Sanchez & McGough, 2014; Smith et al., 2010). Although MT has been less investigated, studies have shown that it is an effective approach to improve functional fitness in healthy older adults (Justine et al., 2011), and is also beneficial for cognitive function in older adults with cognitive impairment (Suzuki et al., 2013).
The present study was designed to determine the effect of multicomponent training on cognitive and functional fitness in institutionalized AD patients following three and six months of training. Due to its wide applicability and feasibility, it is pertinent to assess to what extent MT (integrating several important physical abilities to perform the ADLs, and involving playful and social group activities and cognitive stimulation) can contribute to AD therapy as a low cost alternative to mitigate symptoms, alleviate disease progression (thus allowing the preservation of physical and brain health of patients with AD) and offset the lack of physical activity opportunities in institutions.
Hypothesis
A six-month MT program can promote cognitive and physical functions in institutionalized older adults with mild to moderate AD.
Methods
Study design
Nine nursing homes took part in this quasi-experimental non-randomized study. Four nursing homes implemented the MT training intervention for six months (Experimental Group (EG)); while five haven’t participated in structured physical activity program and maintained with their normal routine, during the same period (Control Group (CG)). 2
Participants
Of 12 nursing homes invited, nine nursing homes in suburban areas Viseu, Portugal, accepted to be part of this study. Participants were recruited from these institutions, 49 older adults from both genders clinically diagnosed with AD, aged 69–94 years, volunteered to participate in this study.
The eligible subject pool was restricted to older adults with the following characteristics: age ≥65 years, not engaged in any regular exercise training in the last year, institutionalized for more than six months, diagnosis of AD at mild or moderate stage according to Clinical Dementia Rating (CDR) (Morris, 1993) and lack of any diagnosed or self-reported musculoskeletal or cardiovascular disorders that contraindicate participation in moderate exercise and testing. A 70% minimum attendance rate to the exercise sessions was required for participants in the EG.
After initial screening, all participants, formal caregivers, and institutions received a complete explanation of the purpose, risks and procedures of the study. A written informed consent was provided. The investigation was in full compliance with the Helsinki declaration (World Medical Association, 2009) and the nine institutions where the intervention took place approved all methods and procedures. The Ethical Commission of the Faculty of Sports of the University of Porto also approved this study. The participants’ flow diagram is represented in Figure 1.
Participants flow diagram from initial screening to the end of the study.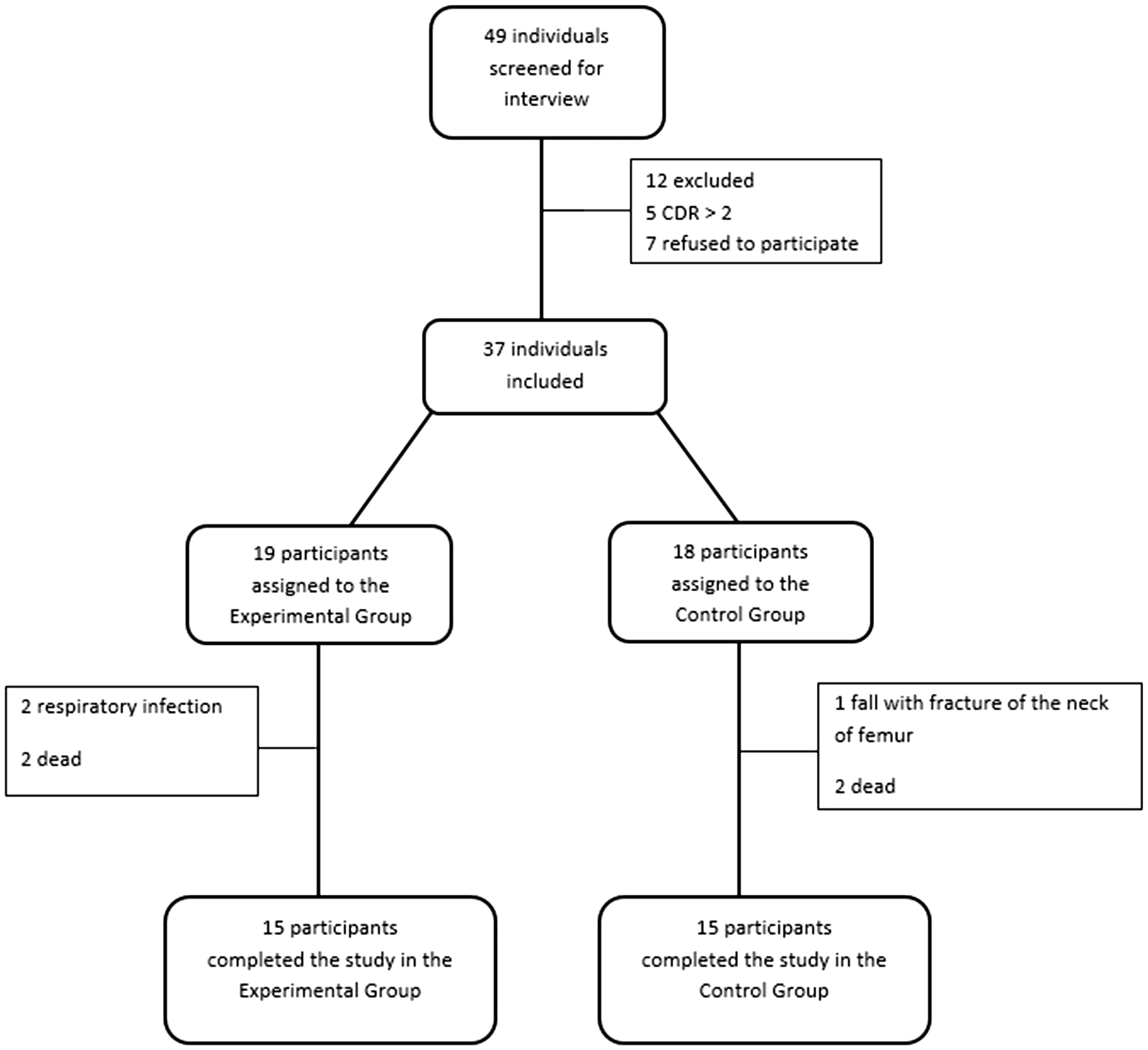
Exercise intervention
The EG completed a six-month MT program following the recommendations of the American College of Sports Medicine (ACSM) (Nelson et al., 2007), including aerobic, muscle strengthening, flexibility, balance and postural exercises with two sessions per week on non-consecutive days. Sessions contained 4–7 participants and took place in specific rooms with peaceful and pleasant music environment. Sessions lasted for 45–55 minutes and were conducted by the same exercise trainer in all settings. The sessions were divided into three main parts: Warm-up (5–10 minutes, including postural and stretching exercises for general activation), specific training (30–35 minutes, including 15 minutes of moderate aerobic exercises + 15–20 minutes motor and muscular tasks for strength and coordination/balance training) and cool down (5 minutes with respiratory and flexibility exercises). In order to make the exercise program more efficient and attractive, we established regular similar routines that prioritized enjoyable and familiar exercises (as simulating walking, running, biking, rowing) (Teri, Logsdon, & McCurry, 2008). Due to the frailty condition of the participants and for safety reasons, sessions were mainly chair-based and routines of functional exercises with low coordination requirements were emphasized so participants could achieve the session’s goals.
Sociodemographic and clinical characteristics
Characteristics of the participants.
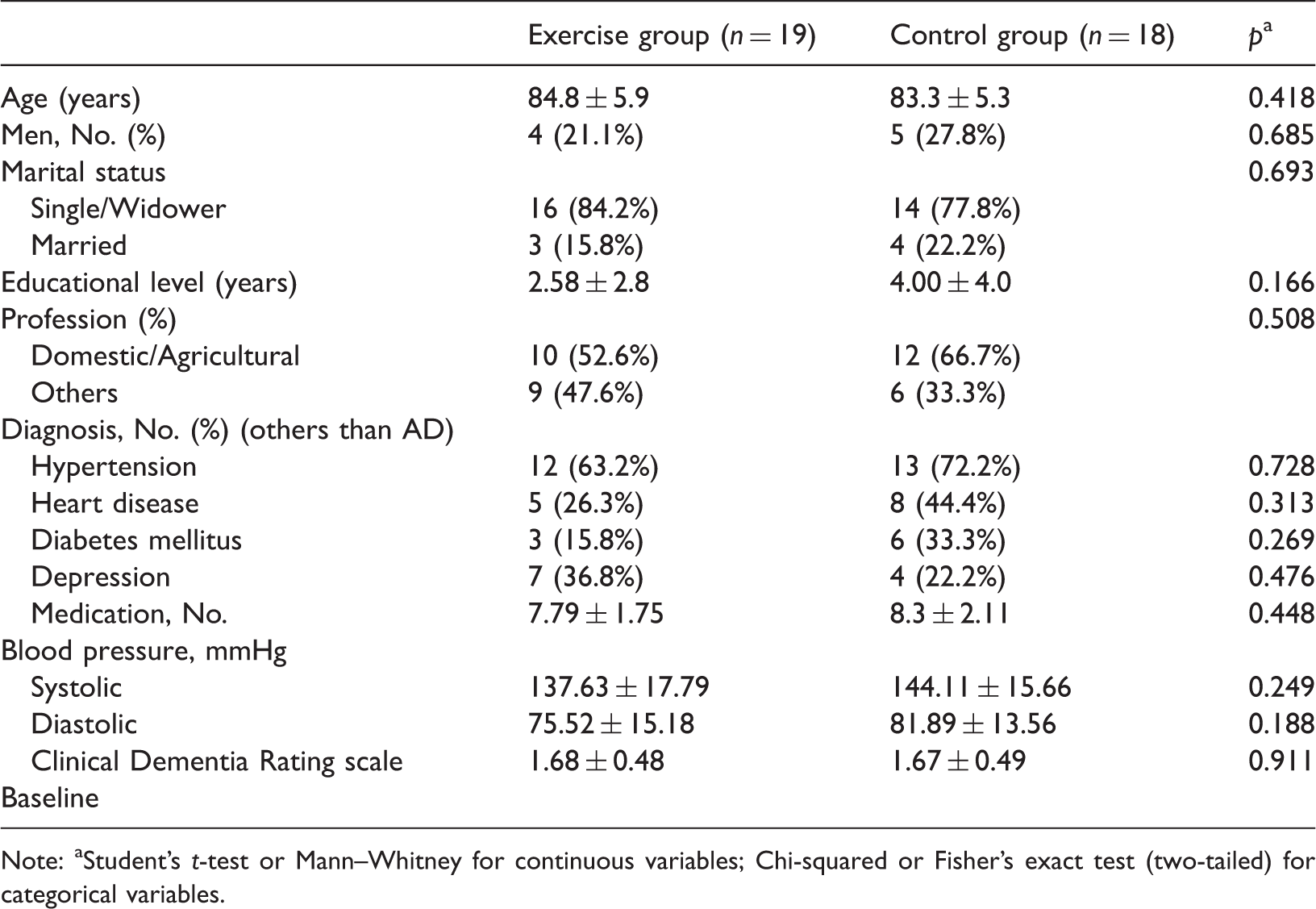
Note: aStudent’s t-test or Mann–Whitney for continuous variables; Chi-squared or Fisher’s exact test (two-tailed) for categorical variables.
Outcome measures
All following measures were assessed at baseline and after three and six months of experimental protocol.
Dementia stage
The CDR test (Morris, 1993) was used only at baseline to distribute the participants according to their cognitive stage. CDR is an instrument that assesses the existence and prevalence of the various stages of dementia. It comprises six cognitive-behavioral items covering memory, orientation, judgment and problem solving, community activities, home and hobbies, and personal care. The cut-off points were CDR = 1 (mild dementia stage) and CDR = 2 (moderate dementia stage).
Anthropometry
Anthropometric variables included Body Mass Index (BMI) and Waist Circumference (WC). BMI was determined using the standard formula: weight divided by height squared (kg/m2). Body weight was measured to the nearest 0.1 kg with a digital weight scale. Participants were weighed barefoot wearing light clothing. Height was measured to the nearest 1 mm with a standard stadiometer. Participants were required to maintain the Frankfurt plane, standing as tall as possible with hands hanging by their sides, and taking a deep breath before the measurement. WC was assessed at the midpoint between iliac crest and the bottom of the ribcage using a spring-loaded measuring tape.
Functional fitness
The Senior Fitness Test (Rikli & Jones, 2013) battery for older adults was used to assess functional fitness associated with maintaining physical independence in later life. The test items included: chair-stand test—to assess lower-body strength; arm curl test—to measure upper-body strength; 2-min step test—to assess aerobic endurance; chair sit-and-reach test—to assess lower-body flexibility; back scratch test—to assess upper-body flexibility; and 8-foot up-and-go (UG) test—to assess agility and dynamic balance.
Cognitive function
The Mini-Mental State Examination (MMSE) was used for a global cognitive evaluation (Folstein, Folstein, & McHugh, 1975). It is a widely used method for assessing cognitive mental status. This instrument is clinically used to detect and follow the course of an illness and can also be used as a research tool to screen for cognitive disorders and follow cognitive changes in epidemiological studies. It assesses orientation, attention, immediate and short-term recall, language and the ability to follow simple verbal and written instructions. Furthermore, it provides a total score that categorizes the individual on a scale of cognitive function (Folstein et al., 1975). Ranging from 0 to 30. MMSE normative values consider the subject educational level. Operational cut-off values for the Portuguese population are 22 (for 0 to 2 years of literacy), 24 (for 3 to 6 years of literacy), and 27 (for more than 6 years of literacy) (Morgado et al., 2009).
Statistical analysis
All statistical analyses were conducted with the SPSS IBM Statistical Software version 20.0 for Windows with a significance level of 0.05. For the baseline comparisons between EG and CG, data for all participants are presented as absolute (proportions) and relative (percentages) frequencies for categorical values, as means with standard deviation (SD) for interval data. The Chi-square test or Fisher exact test was used to compare categorical data, and Student’s t-test or non-parametric Mann–Whitney was applied for interval data (Table 1).
A two-way (group and time) factorial ANOVA, with repeated measures on one factor (time) was used to determine the differences between and within the EG and the CG for dependent variables. Bonferroni Post-hoc analysis was used to determine the differences between the three time-points.
Results
Recruitment
The process of recruitment and screening of participants lasted for two months. Of the 49 participants who were assessed for eligibility, 12 were excluded. A severe stage of dementia was the reason for the exclusion of five individuals and seven older adults declined to participate in the study after being informed of the details.
The intervention included 37 participants, divided into two groups: EG (n = 19; mean age = 84.8 ± 5.9 years) and CG (n = 18; mean age = 83.3 ± 5.3 years). In the EG, two participants dropped out due to respiratory infections and two died. In the CG, three dropouts were registered, one due to a fall and a femoral neck fracture, and two due to death. Thus, the dropout rate from the initial assessment and group’s allocation until the end of the study was 18.9%, resulting in 15 participants for both groups. Figure 1 shows the participant flow from screening to the end of the study.
Attendance rate for the EG was calculated by dividing the number of exercise sessions completed by participants by the full amount of sessions they were expected to perform throughout the study. The attendance levels were 85% or over. The reasons for missing exercise sessions were behavioral disorders (33.3%), acute diseases (26.7%), unwillingness to participate in a particular exercise session (20%) and other reasons (20%). The dropouts occurred between the 12th and 46th session from a total of 48 MT sessions.
Subject characteristics
The sociodemographic and clinical characteristics of participants at baseline are shown in Table 1. No significant differences at baseline were found between the groups.
The 37 participants in the study were predominately females (75.7%) and single or widowed (81.1%). Apart from AD, in both groups (EG and EC), participants were mainly diagnosed with hypertension, minor heart condition, diabetes mellitus, and depression. The CDR (EG = 1.68 ± 0.48: CG = 1.67 ± 0.49) allowed ensuring that the stage of dementia of all participants ranged between mild (n = 12) and moderate (n = 25).
The number of participants who did not complete the study was similar in each group (p = 0.737). Dropout participants had no statistically significant differences compared to the other older adults in any descriptive parameters. None of the reasons for dropping out (including deaths) were directly or indirectly related to possible adverse effects of the exercise program.
Pre-test, three-month test, and post intervention test outcomes for body composition, functional fitness, and cognitive variables.

Note: °Statistically significant difference from M1 to M2 (p < 0.05); °°Statistically significant difference from M2 to M3 (p < 0.05); °°°Statistically significant difference between M1 and M3 (p < 0.05); *Statistically significant difference.
Anthropometry
In the baseline values, no significant group differences were found in BMI and WC. For WC a different response in each group was evident over time, supported by a significant decrease of WC in the EG from M1 to M2 (p < 0.05) and from M2 to M3 (p < 0.05). During the intervention, the CG presented a subtle, though not statistically significant, increase in the WC test. There was a significant main effect of time on WC (p = 0.027) and of group and time interactions on WC (p < 0.001). No changes—neither significant interactive nor main effects of time and group—were observed for BMI.
Functional fitness
No significant group differences were found at baseline for all functional fitness variables. Different responses in each group became evident over time. A significantly better performance in the EG in the Chair Stand test from M1 to M2 (p < 0.05) and from M1 to M3 (p < 0.05) was found. Also, significant main effects of time (p < 0.001) and interaction (p < 0.001) were observed in the chair-stand test. The CG had a worse performance in the chair-stand test over time, although not statistically significant. The EG improved its performance over the time, being statistically significant from M1 to M2 and from M1 to M3 on arm-curl test (p < 0.05), CSR test (p < 0.05) back-scratch test (p < 0.05), and 2-min step test (p < 0.05). The CG had a statistically significant decrease in their performance, between M1–M3, on arm-curl test (p = 0.047) and CSR test (p = 0.020). Thus, there were significant interactive and main effects of group on arm-curl test (p = 0.045), CSR test (p < 0.05) back-scratch test (p < 0.05) and 2-min step test (p = 0.021). In the back-scratch test significant interactive (p = 0.022) and main effects of time (p = 0.002) and group (p < 0.001) were observed. From M1 to M2 (p < 0.05) and from M1 to M3 (p < 0.05), the EG significantly improved their performance in this test. In the UG test, groups responded differently resulting in a significant interaction from M1 to M3 (p = 0.029).
Cognitive function
At the baseline, no significant group differences were found in cognitive function. A significant increase in MMSE from M1 to M2 (p = 0.016) was observed in the EG, while a significant decrease of performance of the CG was observed over time M1 to M3 (p = 0.016). Analysis revealed significant group and time interactions on MMSE (p = 0.008) and significant main effects of time for this same variable (p = 0.036).
Discussion
The present study tested and confirmed the hypothesis that a six-month MT program can improve cognitive and physical functions in institutionalized older adults with mild to moderate AD.
As expected, anthropometric measurements (BMI and WC) showed that, at baseline, participants were generally overweight. Indicators of obesity and overweight have been associated with dementia (Dahl et al., 2010; Luchsinger et al., 2004) and with poor neurocognitive outcomes (Whitmer et al., 2005). Medical conditions frequently related to obesity and overweight (dyslipidemia, hypertension, type 2 diabetes) are also known contributors to cognitive decline and dementia (Hayden et al., 2006; Skoog et al., 2006). However, several clinical settings have also reported associations between lower BMI and dementia at mild severity, increasing with advancing disease severity and duration (White et al., 1998). Although no significant changes were observed for BMI in both groups, the EG’s WC significantly decreased after three months and again at the end of the intervention, whereas the EG’s WC increased during the intervention period. Reducing WC may have relevant health implications, as it has been highly correlated with visceral fat (Molarius et al., 1998). Despite being a frequent and widely accepted measurement of adiposity in young and middle-aged adults (Schreiner et al., 1996), considering age-related changes in fat and fat-free mass in elderly populations (Harris et al., 2000), the influence of BMI on health risks and dementia has been controversial. The literature points out that WC is as good as measure of excess adiposity as BMI among older adults or even better (Leitzmann et al., 2011).
Normal aging is also characterized by the functional fitness decline. With increased physical impairment, the ability to perform ADL decreases (Zhu & Chodzko-Zajko, 2006). In elderly patients with AD functional decline becomes more pronounced and while the disease progresses, physical function becomes increasingly compromised. Limitations in ADLs become more evident, gradually leading to the loss of autonomy. Our data show that the CG follows this trend, with a decline in all dimensions of functional fitness. In opposition, our MT program seems capable of preventing this tendency.
Age-related loss of muscle mass and strength (sarcopenia) are magnified by the lack of physical activity opportunities in the institutional settings leading to frailty faster (Santana-Sosa, Barriopedro, Lopez-Mojares, Perez, & Lucia, 2008). The CG followed this trend, with their performance declining in both lower and upper limbs strength tests, being significant in the arm-curl test (upper limbs strength test) from M1 to M3. A significant improvement in the upper and lower muscle strength tests was observed in the EG from M1 to M2 and from M1 to M3. Thus, our results are in accordance with the literature that considers the increment of physical activity as an important therapeutic tool for the attenuation of this loss (Santana-Sosa et al., 2008). Particularly, frailer older adults with some physiological impairment can improve their levels of strength remarkably (Chandler et al., 1998).
Ageing has a similar effect on flexibility. The decline of this capacity ranges from 20% (hip) to 40% (ankle flexion) by 70 years of age (ACSM, 2009). As a consequence, the risks of injury, falling, and back pain, increases (ACSM, 2009). Our data show that the EG was able to significantly improve their flexibility after three and six months, in both upper and lower limbs. Other studies support these results (Toraman & Ayceman, 2005), showing that the decrease of flexibility can be mitigated or even reversed through physical exercise (Batista et al., 2009).
Regarding the UG test, EG improved their performance during the intervention while a significant decrease was observed in the CG, although this difference was not statistically significant. Agility, balance (Toraman & Ayceman, 2005), and lower limb muscular strength (Santana-Sosa et al., 2008) are the capacities that are important to perform the UG test. All these capacities were trained and were included in our MT intervention. Therefore, MT boosts better results than one type of training that contemplates only one of these capabilities.
According to the literature, an increase in aerobic fitness, as observed in the present study, raises the blood flow and cerebral perfusion preserving critical areas of cognition in older adults (Cotman et al., 2007). Higher levels of aerobic capacity are associated with reduced whole-brain atrophy in persons with AD, thus enhancing the cognitive function (Colcombe & Kramer, 2003). They also reduce the risk of cardiovascular and all-cause mortality (Zhu & Chodzko-Zajko, 2006). The MT program was able to improve significantly the participant’s aerobic fitness after three and six months. These results are supported by previous studies that have shown significant improvements in aerobic capacity after MT (Takeshima et al., 2007; Toraman & Ayceman, 2005) in non-demented older adults.
The improvements observed in the present study have significance for functional fitness which has consistently been linked with better health status, the ability to perform ADL and consequently with better quality of life (Forbes et al., 2013). Similar results were observed by Santana-Sosa et al. (2008), who conducted a 12-week MT program for patients with AD which succeeded in inducing significant improvements in patients’ functional performance.
The Seattle Protocols, a series of evidence-based interventions conducted by Teri et al. (2008), showed that physical activity is beneficial and feasible for community-residing individuals with dementia and cognitive impairment (Teri et al., 2008).
The benefits of chronic exercise on cognitive function have been reported (Kaliman et al., 2011; Stevens & Killeen, 2006), studies found it to be linked to positive changes in brain structures, affecting angiogenesis, neurogenesis, and up-regulation of neuroprotective molecules as well as brain volume and functional architecture (Kaliman et al., 2011).
However, others studies have reported that exercise has no effect on cognition (Holliman et al., 2001; Steinberg et al., 2009). In this study, we observed a significant increase in MMSE from M1 to M2 and from the M1 to M3 in the EG. The literature provides evidence that supports the trend from M1 to M2 and from M2 to M3. We believe that, despite the benefits of physical exercise on cognition that could justify better results in the EG from M1 to M2, the neurogenerative nature of AD may justify the decline from M2 to M3. However, between M1 and M3, the results show a slight and not statically significant improvement in the cognitive function, in the EG while the CG had a statistical significant decrease of this function in the same period of time. These data suggest that MT exercise programs can improve (as in M1 to M2) or at least help preserve cognitive abilities for a longer period of time (as in M1 to M3).
The main limitation of this study was the small sample size, the lack of randomization for group assignment and dietary assessment. Recruiting voluntary AD older adults willing to commit with a six-month intervention was challenging and several institutions were therefore involved. Although the same exercise trainer supervised all classes, working with different settings with different conditions may have disturbed the homogeneity between exercise sessions.
It is important to highlight the low drop-out rate of our sample, which not only allowed us to maintain a consistent number of participants to conduct the full six months exercise program, but also reinforces the idea that mild to moderate AD older adults can and should be engaged in MT exercise program in order to improve or maintain functional and cognitive performance.
Besides the proliferation of different types of intervention for AD older adults, the key strength of our study is that our MT program attempted to adapt the physical exercise recommendations of ACSM for older adults (Nelson et al., 2007) to a population with highly specific characteristics (elderly with AD, in institutional settings). We believe that the positive results are also linked with extremely low level of physical activity and physical fitness at the baseline. According to the literature, exercise can produce short-term, highly improvements even frailer older adults (Fiatarone et al., 1994). Thus, we believe that our results underline that the adaptation of these recommendations is viable and allows this population to enjoy the benefits of improved levels of physical and cognitive functioning associated to physical exercise.
In sum, this study confirms that six months of MT program can positively affect physical and cognitive functions in institutionalized older adults with AD. Due to the frailty of the participants, higher physical fitness contributes for a better performance of ADL and delay the deterioration inherent to AD. Additionally, due its wide application and feasibility, the implementation and dissemination of such exercise program, as a low-cost alternative therapy, could be an important instrument for relevant health promotion policies such as national dementia plans.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.