
Abstract
The experiences and needs of spouses of residential care facility residents with dementia, regarding friendship, love, intimacy, and sexuality were explored. Understanding of how spouses make sense of their experiences was pursued. Semi-structured interviews were held with nine spouses of people with dementia, living in high intensive 24-hour care units within residential care facilities. The results show that friendship, love, intimacy, and sexuality were still embedded in the couples’ marital lives, but all in their own way. Changing roles and a shift in purpose of the relationship recurred. Although intimacy was found to be still important in the lives of spouses, emotional, and practical residential care facility barriers were experienced by the spouses, of which the absence of communication were most important. Our findings on the experiences of spouses with regard to intimacy and sexuality can help residential care facility staff and policymakers to recognize the needs of couples and take these into account.
Introduction
An increasing number of people are diagnosed with dementia, even up to 260,000 people are estimated to live currently with dementia in the Netherlands (Alzheimer Nederland, 2015). Admission to a residential care facility (RCF) is inevitable when cognitive and physical disabilities progress and care needs exceed the possibilities of the informal care network. Such an admission leads to a general decline of quality of life (QoL) in both people with dementia (residents) (Gonzalez-Salvador et al., 2000) and their spouses (Mullin, Simpson, & Froggat, 2013); older couples, who have been together for most of their lives, are separated.
With regard to the lives of spouses, both the impact of the dementia process and the admission to an RCF of their loved one have been described. For example, a change of roles within the relationship (Harris, 2009; Mullin et al., 2013) and the gradual loss of the person with dementia, causing a severe psychological burden for the spouse, were found (Baikie, 2002; Mullin et al., 2013). Moreover, conflicting feelings between increasing responsibility on the one hand and the necessity to let their spouse with dementia go on the other, have been reported (Mullin et al., 2013).
Despite negative myths and taboos, a growing number of studies show that intimacy and sexuality remain important for the QoL of people in old age (Droes et al., 2006; Lindau et al., 2007; Rheaume & Mitty, 2008). For older people and people with dementia in particular, the broad definition of sexuality as defined by the World Health Organization (WHO (Producer), 2006) seems accurate and appropriate. Here, physical sexuality is described as a part of a wide spectrum of intimacy; intimacy and sexuality are seen as lifelong elements of being human and considered important for maintaining self-worth (Hajjar & Kamel, 2004; Swartz, Diefendorf, & McGlynn-Wright, 2014; Tsatali, Tsolaki, Christodoulou, & Papaliagkas, 2010; WHO (Producer), 2006). However, a decrease in physical sexuality and sexual satisfaction was found in community-dwelling couples with one partner suffering from dementia (Davies et al., 2010; Dourado, Finamore, Barosso, Santos, & Laks, 2010; Harris, 2009). Two types of experiences were described; one experience is a decrease in physical sexuality, replaced by intimacy and closeness on other levels. A second experience is of negative feelings resulting from a total decrease in both intimate and sexual satisfaction (Harris, 2009). It is assumed that the experience of love, intimacy, and sexuality is even more compromised after admission to an RCF, in comparison with what people were used to (Hajjar & Kamel, 2004; Lichtenberg, 2014).
Research regarding intimacy and sexuality in the RCF has so far focused on knowledge and attitudes of caregivers, observed intimate, and sexual behavior of residents and the description of a protective care culture in RCFs (Benbow & Beeston, 2012; Hajjar & Kamel, 2004; Roelofs, Luijkx, & Embregts, 2015). Hajjar and Kamel (2004) summarized known barriers to the experience of intimacy and sexuality in RCF’s. Whether these barriers are actually experienced by residents with dementia and their spouses is unclear. In wider terms of love, intimacy, and sexuality, the experienced impact on spouses of the dementia process and admission to an RCF have not been researched before. This seems important to inform care practice and policy to possibly improve the QoL of residents with dementia and their spouses. This improvement is important, in the light of the known paradigm shift in care practice and research from a more curative care perspective to a client-centered perspective, where QoL is the main focus of care (Actiz, 2012a, 2012b; White-Chu, Graves, Godfrey, Bonner, & Sloane, 2009).
The aim of this study was to explore the experiences and needs of spouses of nursing home residents with dementia, regarding friendship, love, intimacy, and sexuality. Furthermore, we try to understand how spouses make sense of their experiences. Through this understanding we expect to contribute to both research and practice regarding the perspectives of spouses of residents with dementia on what is a mostly neglected aspect of their lives.
Methods
Study design
A qualitative research design was selected to collect and analyze perspectives of the spouses. Specifically, interpretative phenomenological analysis (IPA) (Smith & Osborn, 2007) was used to shape the study design and analysis, as this was developed to enable researchers to explore people’s experiences and how they make sense of their experiences, and has been previously used in health psychology research (Brocki & Wearden, 2006; Larkin & Thompson, 2012).
Participant recruitment
Participants were recruited from specialized, intensive 24-hour nursing home care units for people with dementia, form three RCFs located in the south of the Netherlands. The intensive care is provided within closed care units, which accommodate 6 to 10 people with moderate to severe dementia. Ethical approval by the Tilburg University Ethics Committee (reg. nr. EC-2014.27) and the executive boards of the three participating organizations was obtained. No exclusion of participants took place based on legality or length of the relationship, gender, or age. Participants enrolled by sending back a reply form that was attached to an information letter on the study, which was sent to their home. Initially 10 spouses enrolled, one withdrew from the study before the interview took place. All nine participants gave written informed consent. Interviews were audio-recorded and transcribed. Transcripts were anonymized and subject identification codes were used as encryption to the recordings.
Data collection
Interviews were conducted between January and October 2015 and lasted between 30 and 60 minutes. The interviews took place according to the preference of the respondent, either at their home (n = 6), or the RCF where their spouse with dementia lived (n = 3). The importance of a location where people feel safe and comfortable speaking on such sensitive topics is evident and well documented (Smith & Osborn, 2007; Tarzia, Bauer, Fetherstonhaugh, & Nay, 2013)
The first author (TR) interviewed all the participants. She is a psychologist, working in a nursing home-RCF, and experienced in conversations on sensitive topics with older adults and people with dementia.
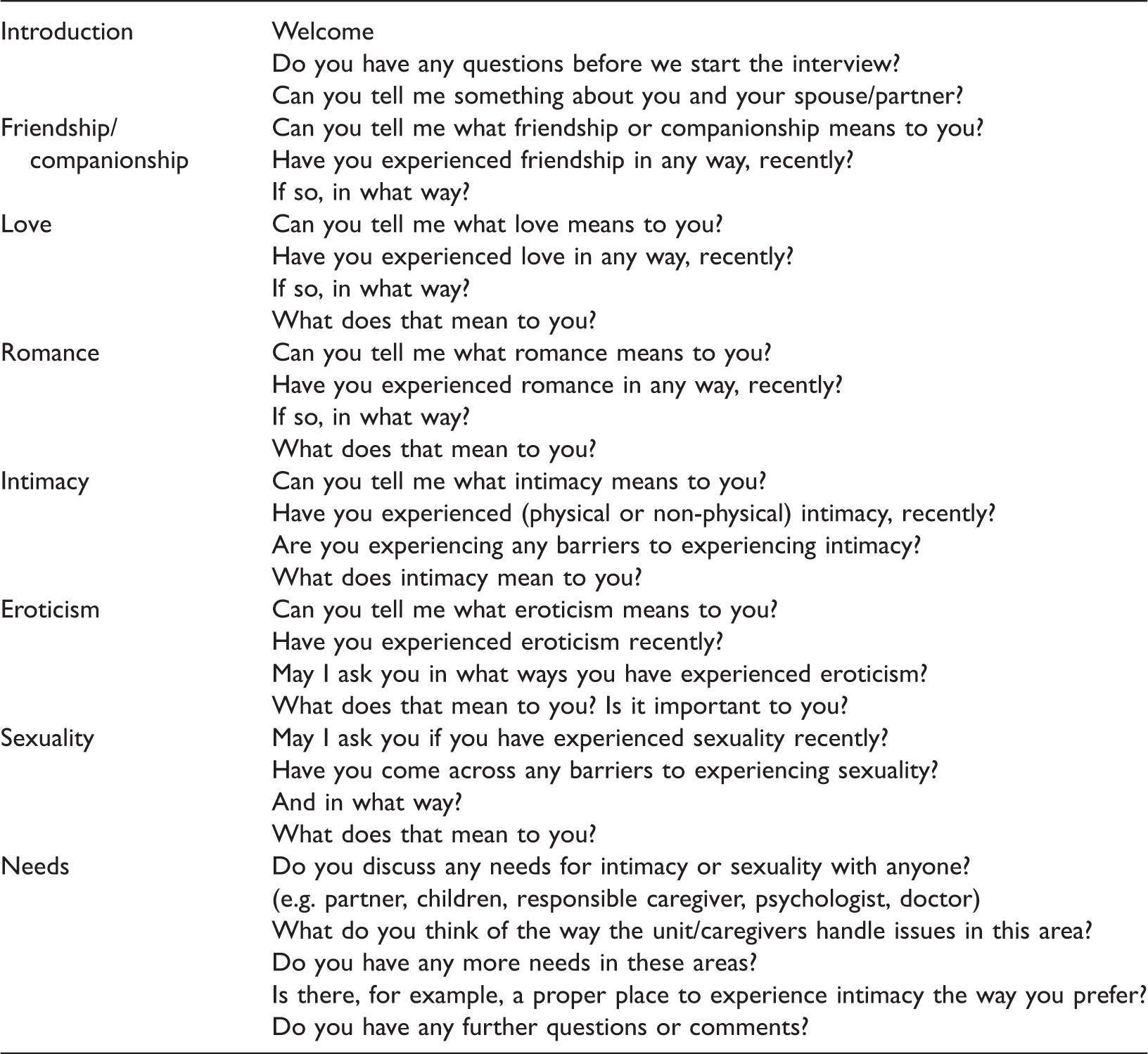
Initial topic list and interview guide.
Data analysis
An iterative and inductive process, in accordance with the “analytic process in IPA” of collection and analysis of data was performed (Larkin & Thompson, 2012; Smith & Osborn, 2007). During data collection, discussion among all the authors influenced the initial interview guide. First, questions regarding eroticism disappeared from the list, because participants tended to find these questions unclear. Second, the topics “romance” and “love” merged into one (love) as the respondents answered similarly to the questions on both topics. Finally, the focus of the interviews broadened, as the love and relationship history was more embedded in the medical or clinical history of the respondent and partner with dementia than expected.
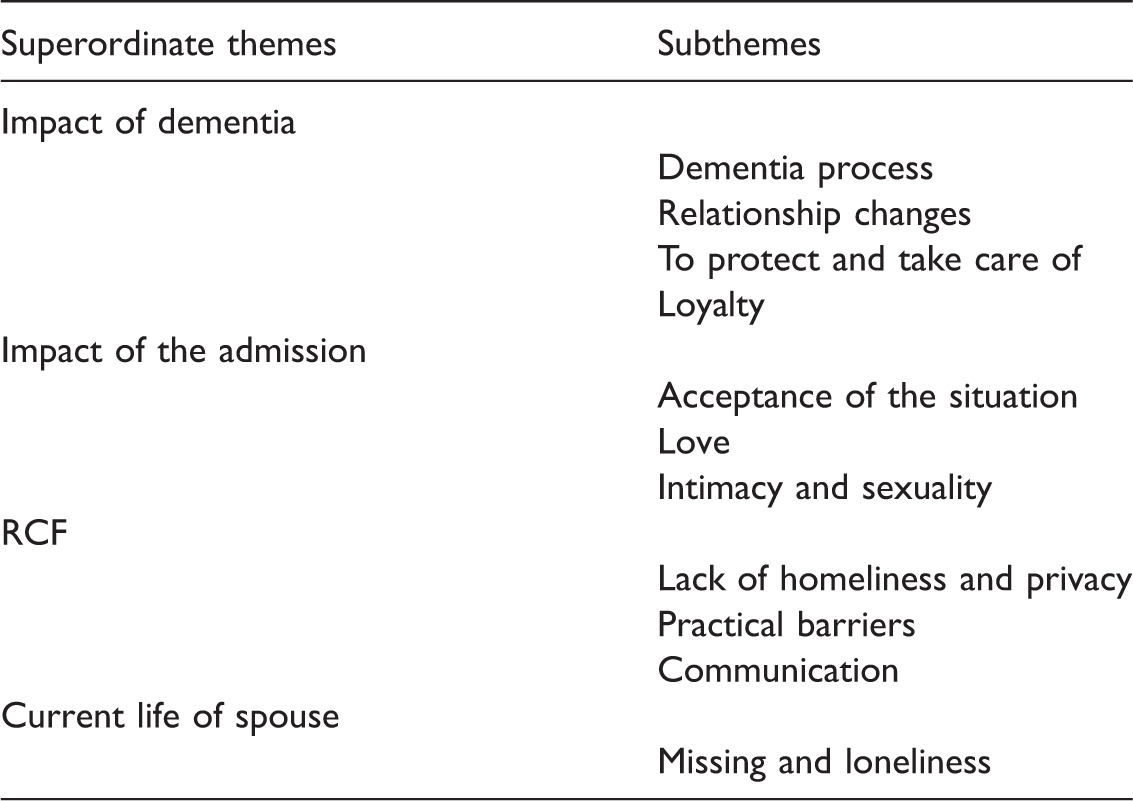
Superordinate themes and subthemes.
Results
Participant characteristics.
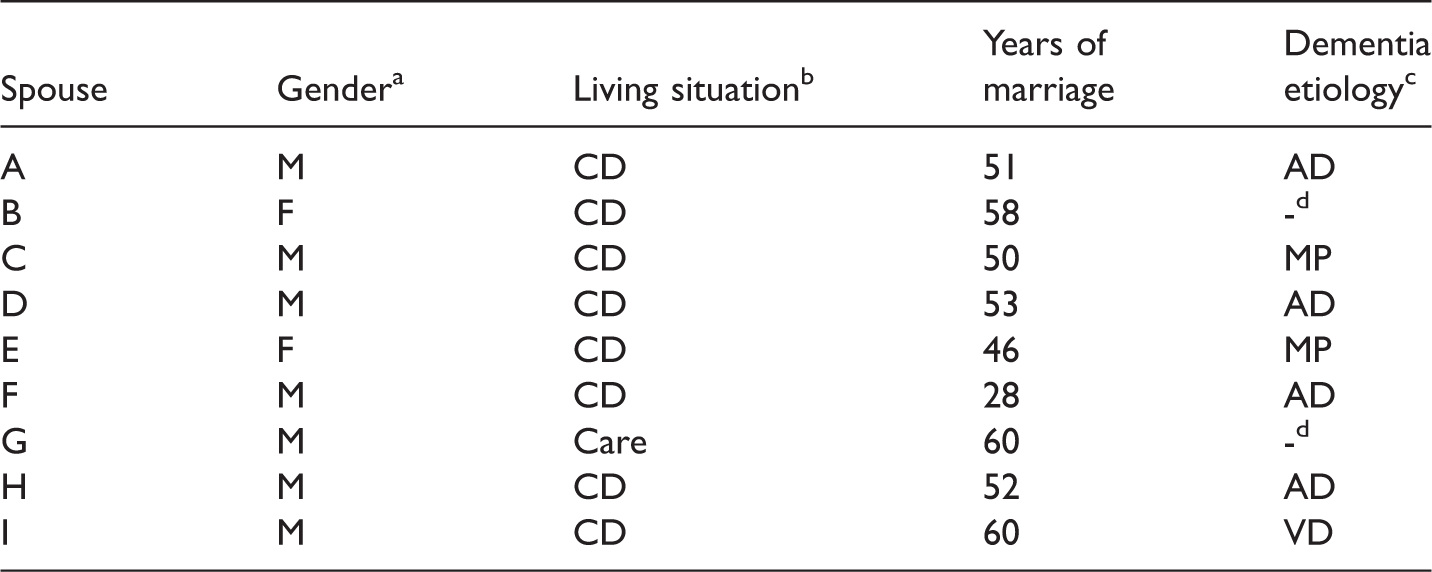
Gender—M: male, F: female.
Living situation—CD: community dwelling, care: independently living in care homes.
Dementia etiology—AD: Alzheimer’s disease, MP: Parkinson’s disease, VD: vascular dementia.
Unknown.
Impact of dementia
Dementia process
All spouses shared the process of how their loved one became ill and the consequences this process had for their relationship and their own life. They recognized several symptoms of dementia, such as forgetfulness, disorientation or deterioration in thinking and behavior. Several spouses (A, B, D, E, F, H) indicated that they did not recognize the start of the dementia process right away. They explained that in retrospect, the impairment in cognitive functioning started far before they realized at that time. Different experiences of the process were described with regard to the course of the dementia process. Spouse E, whose husband suffered from Parkinson’s disease, described a slow, progressive process with increasing physical and cognitive disabilities. Behavioral deterioration in her husband caused difficulties between the couple, as he was not able to perform normal daily activities anymore and also developed behavioral disinhibition. In frustration she expressed: “The way that he eats, well that is just disgusting.”
In contrast, spouse I, whose wife was affected by a stroke, referred to the abrupt start of physical and cognitive disabilities.
Relationship changes
All spouses described the impact of dementia on their relationship. A role change between the spouses was much discussed. As spouse C revealed: “The equality disappears.”
Spouse F described the role change between him and his wife in a different way: “(I see her) as a patient … Not as my spouse anymore.”
He further explained that there was a moment in which he first experienced this role change. At this point he also started to fear that he was taking advantage of his wife, in terms of experiencing sexuality together. However, he was not able to specify precisely when he started to feel this, or what disabilities caused the change in view. He puts this forward as: “She was just ‘too far’ by then.”
The male spouses also described a practical consequence of the role change. Spouse I, for example, described how he needed to take over all the work in the house, which was first carried out by his wife.
Several spouses (A, C, D, H, I) considered friendship as an important aspect of their current relationship. Respondent I considered friendship to be a substitution for the romantic relationship there was before. The spouse with dementia was literally called a “friend” by spouses A, E, and I, as a description for the different, but close bond they still experienced as a couple. Spouse E argued that friendship or companionship within a relationship is a necessity for a marriage to last in general: “Without being friends … you won’t follow through for 46 years, you know?”
However, spouses C, E, and F experienced that even friendship became impossible due to the progression of dementia and specifically due to disabilities in verbal communication.
To protect and take care of
As part of the role change within the couples, spouses shared both implicit and explicit increasing feelings of protection and responsibility for the well-being of their loved one. Spouse A expressed this as follows: “I will, as much, as much as I can, provide her with a good life, as long as I live.”
With regard to the current experience of love, spouses defined love as “to care for” and “to give” (A, B, D, F). Respondents described also taking more physical care of their loved ones. Spouse F described himself initially performing manicures and pedicures for his wife and eventually helping her with all daily caring tasks, such as taking showers and toilet visits. After admission to an RCF, several spouses, such as spouse D, helped the care staff with daily care tasks: “I just put her to bed at night, and also in the afternoon.”
Several spouses expressed that they had no problem with these care tasks, whereas others, described physical and emotional strains and consequently a decline in their current experience of love, resulting from the care tasks they took on: “I walked away for a minute, and at a certain point I returned and … He was pooping in the shower. Well, that’s very hard for me.” (Spouse E)
Loyalty
In spite of the difficult situation and the change in the relationship due to the dementia process and the admission to an RCF, the vows the spouses took when getting married were put forward several times as an expression of their loyalty. With regard to the possibility of becoming involved with another partner, several spouses reacted dismissively. Spouse I shared a more general dilemma in this perspective: “Sometimes I think: How long will this take?”
He asked himself this question, as he felt that he could not go on with his life emotionally, until his wife passes away.
Spouse G shared his feelings of loyalty with regard to intimacy. He now responds positively to the expressions of intimate needs of his spouse by hugging her, as ‘an act of civilization’, but argues that he feels uncomfortable doing this.
Impact of admission
A repeatedly shared story concerned the period just before the person with dementia was admitted to an RCF. In this period it became clear that the capacity of their spouse and the couple’s social or care network were stretched to the limit. The struggle to persevere in a 24-hour care schedule and the hesitancy and dilemma surrounding the admission to an RCF were voiced by spouses A and B as follows: “… I did not think I would miss her so much … because, yes, all those problems, she was aggressive all day … and … In those times (living at home) I said to myself: I will be glad when she is gone …” “. Yes. The final period that he was still at home … yes, I am sorry, I hated that man. (…) But not anymore, you know!”
Acceptance of the situation
Spouses described various processes of working towards acceptance of the situation. Through emotional statements (i.e. crying, anger, frustration) they drew an image of the difficulties they faced in coping with the dementia process and the inevitable admission to an RCF (A, D, E, F, H). Spouses A and H found it very hard to describe these feelings. Spouse H started crying at the start of the interview, and stated that he had a very hard time leaving his wife at the RCF in the evening. “It is very hard, one to cope with, and two, to describe what happened to me.” (Spouse A)
Spouse H also described the difficulty his wife has in coping with her current situation: “She hopes she will be dead by tomorrow.”
More implicitly, spouses shared a tendency to gradually say goodbye to their loved one and their life together throughout the dementia process and after the admission. Spouse F puts it as follows: “It is a really slow process, with ups and downs.”
He described how he started saying goodbye to his wife at the very moment the diagnosis of Alzheimer’s disease became known. Spouse B experienced the process as if her husband is dying gradually, as the dementia process worsened: “He is actually dying, little by little.”
In contrast, spouse I described the process of the admission as a quick and abrupt process that forced him to say goodbye to their life together very quickly.
Some spouses also shared words of acceptance regarding the dementia process and the admission of their loved one to the RCF, such as spouse D: “I just accepted it, well I still do.”
Relief that the spouse with dementia was not aware of his or her own situation was also expressed, such as by spouse I: “Well, she doesn’t know. Fortunately, I think she still does not know.”
Love
The experience of love varied among the spouses. Where some still experienced love in the current situation, other spouses reported the loss or total absence of love along the way of the dementia process. Spouses A, C, E and I indicated that love and romance are still very important in their marriage. Spouses A and C still expressed admiration for and attraction towards their loved one: “The crazy thing is, she sits in … in that wheelchair … but actually I am still just as crazy about her as when she was 17 years old …”
Other spouses described their love as “thinking of each other” (respondent H), different intimate expressions such as “cuddling” (respondent I) and “holding hands” (respondent D) or descriptions of frequent visits to their loved ones in the RCF (respondent H). Spouse A even shared that he felt more love for his wife after her admission, because the difficult period at home had ended.
Through an emotional statement (frustration and crying) by spouse E, it becomes clear that she has great difficulty with the absence of romance and love in her current life: “You know, my husband was always very romantic. Every birthday or anniversary he gave me a large bouquet of red roses. Now he doesn’t give them anymore.”
Spouses B and G shared the current absence of experiences of love. Spouse G described the couples’ current connection as follows: “We are like this: Are you still alive?”
Intimacy and sexuality
Although spouses mostly did not mention to experience a physical sexual relationship with their loved one; intimacy was reported to still be very important to most of the couples. The spouses also incorporated their impression of the need of their loved one in their experiences. Spouses A, C, D, and I mentioned that they thought that their loved ones needed intimacy. Spouse C quoted his wife expressed her wish to sleep together: “Let’s lie down together.”
Other spouses mentioned that their spouses expressed their need for intimacy in a physical way: “She comes over and hugs me and says: I am so happy with you!” (Spouse A). “She just grabs my hand” (Spouse D)
Although they seemed to enjoy these expressions of the need for intimacy by their loved ones, spouses A, C, G, and I also shared the difficulties, concerns, and dilemmas they experienced in this context. First, practical barriers for being intimate were mentioned, such as a loved one being in a wheelchair, which limits both the possibility of moving close together and touching each other in any way. Second, spouses shared that they discouraged expressions of intimacy by their loved one, as they cannot fulfill their request to, for example, sleep together. This barrier led to frustration between couples, as spouse C shared that his wife did not understand why they could not sleep together and asked him: “We still have a right to each other, don’t we?”
The spouses B, F, G, and H mentioned the absence or closure of the need for and expression of sexuality. Spouse H described that their relationship had never been very physically intimate and spouse D described intimacy (and also sexuality) as something that “… takes second place now …”, due to the illness of his wife. Additionally, spouse I stated that his only condition for any form of physical intimacy was that his wife would initiate that contact. At the same time he was unsure about her physical abilities to have sexual intercourse.
In contrast, experiences of intimacy were also found to still be very important by spouses. Spouses A, C and I specifically shared their experience of intimacy as a way of “being together”: “To stroke her body and her hair, oh, then I notice. Yes, she quite likes that. Because then we are together.” (Spouse I)
The way in which this intimacy is experienced varied. Spouse D described sitting in the bedroom with his spouse, in an old leather chair, holding hands. Spouse A said that he shared intimate moments with his wife during long walks together.
Residential care facility
Lack of homeliness and privacy
Most spouses described the RCF as an uncomfortable place to experience love, intimacy or sexuality in the way they would like to (A, B, C, G, I). A lack of privacy was frequently mentioned as a cause for feeling unsafe and uncomfortable. Examples included the fact that every caregiver has a master key (spouses A and C), that they enter bedrooms without knocking (spouse A) and the use of cameras in the RCF (spouses A and D). Spouse C described the RCF as an “unnatural situation,” which was caused by a “lack of homeliness.” He however mentioned the vain attempts of the caregivers to simulate a home-like situation by naming the shared living area a “living room”. The fear of gaining a negative reputation with caregivers or other family members was also shared.
Spouse G felt belittled by the caregivers, because he was asked to leave the unit the moment his wife goes to bed at night. Several spouses shared the fact that they were convinced that they were prohibited from bringing their loved one back home with them for visits.
Practical barriers
The spouses mentioned several practical barriers to experiencing intimacy and sexuality, including environmental and architectural factors, such as shared bathrooms and lack of space in the bedroom to place a double bed. Opposite views were expressed concerning the creation of a separate, special room for couples to be intimate. Spouse A spontaneously suggested this as a potential solution that would allow him to experience intimacy: “Just a separate room, where … those other people … don’t come in …”
Spouse C on the other hand was worried about obtaining a negative reputation with the caregivers: “Oh, they are doing ‘something’ over there … In room number 13.”
Communication
To improve the situation for couples within the RCF, the improvement of communication was suggested. Caregiving staff should speak more openly about intimacy and sexuality. Disappointed in his wife’s caregivers, spouse A stated: “They know she always asks me: I want to sleep with you … And that’s why I find it important to discuss this. They are all people who studied to do this job and they must feel something too. They are people of flesh and blood.”
Furthermore, spouse E shared another insight. Before her retirement, she had worked in an RCF as a physical therapist. She noticed an increase in openness in the RCF regarding intimacy and sexuality in general, now as a spouse of a resident with dementia.
Current life of spouse
With respect to the meaning of the relationships after the admission of their loved ones, several spouses described their visits to the RCF. They however found it very important that their spouse with dementia still recognizes them, and saying hello and goodbye was described as important. “She is very happy when I come over. She sees me when I come in.” (Spouse H)
The absence of this recognition was described as a burden: for example, spouse F explained that he felt less connected to his wife because she doesn’t recognize him anymore.
Spouse A shared the daily strain put on him when leaving the RCF, as his wife becomes upset by that event. She doesn’t understand the situation: “I really don’t like it … that I have to leave secretly, because I know she feels that.” (Spouse A)
Missing and loneliness
“I miss her VERY, VERY, much.” (Spouse A) Although desperately missing their loved one was reported by different spouses (A, B, C, D E, F, I), the detailing of this feeling was put forward in two different ways. Firstly, spouses shared missing their spouse physically in their proximity on a daily basis. Secondly, they shared their experience of missing the person who their loved one had been, before they became ill.
Spouse I said that he and his wife had spent only one night apart since their marriage, before the admission. Spouse D explained that he visited his wife frequently because he misses her: “Yes, of course I miss her. That is why I go there (RCF).”
He mentioned “coming home to an empty house” and “getting in to an empty bed” as examples of daily life activities. He sometimes even talked to his wife, although she was no longer in the house, and further explains how he takes solace from the knowledge that she does the same in the RCF, so a caregiver told him.
And also the absence of the meaning this person had in their life was shared: “He always was my great support and anchor in life.” (Spouse B)
In this context, “lovesickness” was also mentioned. Lack of recognition and reciprocity in contact and communication was shared as the most devastating aspect to the bond between the couples.
Spouse C shared a story of his daily life in which he admitted to becoming “extremely jealous” of a friend who had to discuss making appointments with his wife. The fact there was no longer a need to discuss these day-to-day matters with his spouse put a strong emotional strain on him. More spouses shared a strong emotional strain caused by missing their loved one in their daily life: “That is the worst there is. All the rest is secondary.” (Spouse D)
Discussion
A qualitative exploration was conducted on the experiences and needs of spouses of RCF residents with dementia, regarding friendship, love, intimacy, and sexuality. The interviews were in-depth, rich reflections of these experiences in a difficult period of the spouses’ lives. Both the impact of dementia and the admission of their loved ones were described in detail, as spouses narrated the life they had had together. Furthermore, the way in which the spouses made sense of the topics of friendship, love, intimacy, and sexuality was deeply embedded in these stories, as these topics remained important parts of their married lives and cannot be seen in isolation.
Different stories were shared about the course of the illness, probably partly due to differences in the etiology. However, all spouses described a very difficult period, just before the admission of their loved ones to the RCF. Admission became inevitable, as the increasing care needs exceeded the capabilities of the spouses and their private network. This admission caused conflicting feelings of relief, anger and sadness and confirms the image that was drawn previously by Mullin et al. (2013). These conflicting feelings additionally influenced the experience of love for the spouses.
Changing roles within the relationship affected the lives of the spouses greatly. The purpose of the relationships shifted from being a married couple into a relationship in which the physical care for, and protection of, the spouse with dementia became most important. This finding is consistent with previous findings on general spousal experiences of living with a partner with dementia (Harris, 2009; Mullin et al., 2013). Spouses in the current study made sense of this change in different ways. Some tended to define their relationship as a friendship, with a decrease in or even closure of intimate and sexual lives together. Others took the opportunity to fulfill their new caring role including love and intimacy. These findings are in line with the two types of experiences, which were described by Harris (2009). On an emotional level, the role change meant losing an equal spouse. This caused feelings of frustration, loss, anger, and sadness. However, the results in this study gave a closer insight into the way spouses make sense of their experiences. Feelings of loss were, for example, described on two different levels. First, the actual missing of the physical loved one with dementia in daily life. Second, the missing of the person the loved one once was and the role or meaning they had in the spouses’ life.
Love, emotional and physical intimacy were experienced as important aspects of being together as in contrast needs for merely physical sexuality were not shared. Consequently, direct physical limitations for expressing sexuality, due to age-related physical illness (e.g. erectile problems) such as mentioned in previous research, were not mentioned in this study (Baikie, 2002; Hajjar & Kamel, 2004). Feelings of admiration and attraction were still experienced. Love and togetherness were expressed in different ways: through protection or taking care of the loved one, frequent visits to the RCF and by acts of intimacy, such as cuddling and holding hands. The feeling of being together was mainly expressed on the level of intimacy, which implies intertwinement of these two aspects.
The barriers to experiencing intimacy in the context of a RCF were shared. In addition to feelings such as a lack of privacy, an unnatural situation and a lack of homeliness, participants also pointed at practical barriers, such as a shared bathrooms and small bedroom sizes. However, professional caregivers seem to play a more important role in the possibilities of expressing and experiencing love, intimacy and sexuality of couples than previously known. First, the risk of developing a questionable reputation with the caregivers was shared. Second, communication with caregivers was considered an important aspect, regarding the improvement of the possibilities to experience intimacy and sexuality by the spouses. It is interesting to further focus on this role of caregivers in future research and its implications for clinical practice.
Strengths and limitations
A major limitation of this study is the composition of the sample and its size. A small sample of spouses enrolled to participate in the study. This resulted in participants who were willing and not embarrassed to talk about a sensitive topic like intimacy and sexuality, which probably not applies to all spouses of residents with dementia. Given the sensitive topic, this was, however, expected and predicted in the literature (Tarzia et al., 2013). These limitations compromise the generalizability of the found results. Despite this shortcoming, the study offers a first in-depth, rich spousal (client) perspective on this neglected theme of intimacy and sexuality. Furthermore, IPA guidelines (Larkin & Thompson, 2012; Smith & Osborn, 2007) were used to design this study. This methodology was chosen, as it is well described and has been used in previous research on general spousal experiences (Brocki & Wearden, 2006; Mullin et al., 2013). IPA provided an opportunity to study the experiences of a small sample of spouses (Smith & Osborn, 2007). We feel the aim of exploring the experiences and needs of spouses of nursing home residents with dementia, regarding friendship, love, intimacy, and sexuality was therefore achieved.
Research on the topics of love, intimacy, and sexuality of (older) people with dementia is scarce. Specifically, the client perspective, including the experiences of spouses of residents with dementia in this area, is lacking in the international scientific literature as far as we know (Roelofs et al., 2015). This seems striking considering the importance of intimacy and sexuality for the QoL (Bouman, Arcelus, & Benbow, 2007; Weeks, 2002) and the very private nature of friendship, love, intimacy, and sexuality. This study contributes to filling the knowledge gap on experiences of love, intimacy, and sexuality by including spouses of residents in order to provide a more complete image.
Directions for future research and clinical implications
Through this study, we found friendship, love, intimacy, and sexuality to be still embedded in the couples’ marital lives, despite the great impact of the dementia process and admission, all in their own way. This indicates that the wide spectrum of intimacy, which was suggested before (Swartz et al., 2014; Tsatali et al., 2010; WHO (Producer), 2006), might be the basis of future research. In addition, in line with the client-centered paradigm, it is important to include the client perspective in future research, as individual differences are great (Rheaume & Mitty, 2008).
Results from this study can help clinical RCF practice to understand more about the journey spouses have completed and the process they go through regarding the relationship with their spouse with dementia. Specifically, our findings on the experiences of spouses with regard to intimacy and sexuality in the RCF can help RCF staff and policymakers to recognize the needs of spouses. The results might also help them to adapt the care process to the needs of clients as well as their partner, for example in providing more opportunities to experience intimacy and sexuality as wanted, and to enhance communication opportunities. However, to do this, educational programs are needed for RCF staff to enhance adequate knowledge and skills, and by this optimize QoL of people with dementia and their spouses.
Footnotes
Acknowledgements
We sincerely thank the participants and the three participating RCF organizations: Schakelring Waalwijk, de Riethorst-Stromenland Geertruidenberg, Volckaert Dongen.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.