
Abstract
Objectives
Literature regarding Montessori-based activities with older adults with dementia is fairly common with early stages of dementia. Conversely, research on said activities with individuals experiencing late-stage dementia is limited because of logistical difficulties in sampling and data collection. Given the need to understand risks and benefits of treatments for individuals with late-stage dementia, specifically regarding their mental and behavioral health, this study sought to evaluate the effects of a Montessori-based activity program implemented in a long-term care facility.
Method
Utilizing an interrupted time series design, trained staff completed observation-based measures for 43 residents with late-stage dementia at three intervals over six months. Empirical measures assessed mental health (anxiety, psychological well-being, quality of life) and behavioral health (problem behaviors, social engagement, capacity for activities of daily living).
Results
Group differences were observed via repeated measures ANOVA and paired-samples t-tests. The aggregate, longitudinal results—from baseline to final data interval—for the psychological and behavioral health measures were as follows: problem behaviors diminished though not significantly; social engagement decreased significantly; capacities for activities of daily living decreased significantly; quality of life increased slightly but not significantly; anxiety decreased slightly but not significantly; and psychological well-being significantly decreased.
Conclusion
Improvements observed for quality of life and problem behaviors may yield promise for Montessori-based activities and related health care practices. The rapid physiological and cognitive deterioration from late-stage dementia should be considered when interpreting these results.
Introduction
Researchers predict an estimated 7.1 million American citizens over the age of 65 will be diagnosed with Alzheimer’s disease (AD) by 2025, a 39% increase from the current number of 5.1 million (Alzheimer’s Association, 2015). In response to this alarming growth, health care programs have begun to reevaluate the efficiency of services and quality of care provided to older adults with dementia. In doing so, clear gaps in the literature have been identified. Most notably, a majority of research on health-care and related practices for residents with dementia have focused their attention on individuals in the beginning or middle stages of the disease (Mitchell et al., 2006; Volicer, 2005). While these individuals experience problematic symptoms, it is apparent that minimal research has focused specifically on the care of those with late-stage dementia.
Declining functioning has undoubtedly contributed to the lack of research on individuals with late-stage dementia. Thus, an understanding of evidence-based care practices for late-stage dementia is still needed. Moreover, the end-of-life care individuals with dementia receive is highly important to consider as medical advances have resulted in increased longevity for older adults. Since AD is currently incurable, it is essential that dementia care programs mitigate the risks for poor behavioral and psychological health outcomes.
Montessori-based activity (MOBA) programs have been previously used in long-term care settings to rehabilitate residents’ mental and physical capacities and improve overall quality of life (QoL) (Bognar, 2003). As a result of the need for more research of evidence-based practices for late-stage individuals, the purpose of the current study was to longitudinally evaluate the impact of an eight-month MOBA program implemented at a long-term care facility in the southern United States. Psychological and behavioral outcomes were assessed among a sample of 43 older adults with AD. With the expectant increase in the prevalence of dementia, it is our ethical obligation to address the current gap in the literature because the mental health needs, treatment, and research of residents living with late-stage dementia should not be overlooked. A greater understanding of the effects of a MOBA program for individuals with late-stage dementia residents can benefit those experiencing the disease, caregivers, long-term care providers, and the broader health care system.
Literature review
To reiterate, many dementia studies have focused solely on residents in mild to moderate stages of dementia. The current literature points to the need to examine the following outcomes among residents with late-stage dementia: problem behaviors, social engagement, capacity for activities of daily living (ADLs), QoL, anxiety, and psychological well-being. The research presented here will provide a scope of the literature as it pertains to individuals with mild to moderate dementia. Factors contributing to poor mental and behavioral health are discussed below, as well as findings supporting the role of MOBA programs in long-term care facilities.
Mental health
QoL
QoL refers to the overall measure of social, health, well-being, and economic indicators in society (Diener & Suh, 1997). QoL indicators subjectively explain a person’s values across a broad range of life domains (Felce, 1997). As defined in this study, individuals with good QoL view their lives and resources as valuable and productive, whereas those with poor QoL perceive their lives and resources (whether tangible or intangible) negatively. When individuals with dementia experience the loss of vital mental and physical capabilities, poor QoL and symptoms of mental illness can be difficult to differentiate. Nonetheless, some key predictors of positive QoL for individuals with dementia are positive relationships with children, good financial status, social engagement, higher ADL functioning, and higher cognitive functioning (Logsdon, McCurry, & Teri, 2007; Nikmat & Almashoor, 2013). These results would suggest that persons with late-stage dementia may report poor QoL due to decreased cognitive and physical functioning. Yet, as others (e.g., Banerjee et al., 2006; Edelman, Fulton, Kuhn, & Chang, 2005; Hoe, Hancock, Livingston, & Orrell, 2006) have found, significant predictors of QoL can differ depending on the rater (caregiver vs. care recipient), and measures of functioning may not accurately reflect QoL. Thus, QoL research is scarce for individuals with severe cognitive impairment who cannot complete self-report measures.
Anxiety
A 2008 review by Seignourel, Kunik, Snow, Wilson, and Stanley (2008) estimated that 5–21% of individuals with dementia were diagnosed with an anxiety disorder while 8–71% reported anxiety symptoms. Anxiety symptoms contribute to negative outcomes such as accelerated cognitive decline, lower QoL, behavioral disturbances, and problems completing ADLs (Hynninen, Breitve, Rongve, Aarsland, & Nordhus, 2012).
Findings have identified the following specific causes of anxiety, including those with dementia: loss of skills, difficulty in relationships with others, and physical or environmental problems (Qazi, Spector, & Orrell, 2010). Fostering social relationships, person-centered care, and meaningful activities have emerged as protective themes related to the management of anxiety for individuals with dementia (Qazi et al., 2010).
Previous research has recommended additional studies be conducted to examine anxiety among persons with late-stage dementia in order to inform psychosocial interventions (Seignourel et al., 2008). Similar to anxiety, poor psychological well-being or depression can contribute to poor psychological outcomes for older adults with dementia.
Psychological well-being
Psychological well-being is related to an individual’s affect and interactions, and negative affect and interactions can be indicative of depression. The prevalence of depression among those with dementia has not been definitively determined. This is the result of variation in measurement, sampling of heterogeneous dementia diagnoses, and difficulty differentiating depressive symptoms from dementia symptoms. Thus, gaps exist in the current literature; nevertheless, several studies have contributed to the knowledge of psychological well-being and dementia.
Andreasen, Lönnroos, and von Euler-Chelpin (2013) found persons with dementia were twice as likely to develop depression compared to individuals without the disease. By comparison, Nikmat and Almashoor (2013) found 70% of individuals with dementia exhibit signs of depression. While studies vary in their reports of prevalence, Knapskog, Barca, and Engedal (2014) investigated factors related to depression among persons with dementia. Results showed that greater ADL impairments, younger age, and previous depression diagnosis were all associated with decreased psychological well-being (Knapskog et al., 2014).
Behavioral health
Problem behaviors
Behavioral symptoms of dementia, such as agitation and aggression, have been identified in approximately 40% of persons with a diagnosis (Kunik et al., 2010). Additional behaviors among individuals experiencing late-stage dementia include wandering, disruptive vocalizations, and inappropriate sexual behaviors (Ornstein & Gaugler, 2012). These symptoms, often termed problem behaviors, can be difficult for caregivers to prevent, monitor, and reduce. These symptoms, which caregivers can perceive as aggressive or disruptive, are often attempts by the individual with dementia to communicate pain or voice physiological needs (Morgan et al., 2012).
Overall, behavioral and psychological symptoms of dementia are associated with increased caregiver burden and depression (Ornstein & Gaugler, 2012). Findings suggest dementia-related behavioral symptoms may be mitigated by identifying and addressing possible biopsychosocial triggers such as illness or lack of social stimulation (Salzman et al., 2008). A 2012 meta-analysis conducted by Brodaty and Arasaratnam (2012) found that individually tailored interventions aimed at providing skills training, education, and support for caregivers were most successful at decreasing behaviors such as agitation and aggression (in addition to others). Behavioral interventions (e.g., redirection, positive reinforcement) tailored to the individual with dementia may also be effective in decreasing behaviors such as wandering and aggression but warrants further research (Ayalon, Gum, Feliciano, & Areán, 2006). Social engagement is another targeted behavioral outcome shown to decrease stress and improve functioning among individuals with dementia.
Social engagement
Dementia symptoms can negatively impact the capacity to engage socially with family members, peers, caregivers, and nursing home staff. Consequently, a lack of social engagement or participation in stimulating activities for individuals with dementia has been associated with increased behavioral symptoms, depression, and functional impairment (Kang, 2012; Magliocco, 1997). Related to social (dis)engagement, apathy, a lack of concern, boredom, or disengagement from activities, is one of the most common symptoms of dementia (Chow et al., 2009; Robert et al., 2005; van Reekum, Stuss, & Ostrander, 2005). Interventions targeting social activity and social support were found to improve overall cognitive functioning and promote positive social engagement (Judge, Camp, & Orsulic-Jeras, 2000; Krueger et al., 2009). A lack of social engagement for those with AD is often accompanied by declines in capacities for ADLs.
ADLs
For residents of long-term care facilities, the inability to use the bathroom, eat, sleep, and walk can increase stress and dependence on caregivers (Andersen, Wittrup-Jensen, Lolk, Andersen, & Kragh-Sørensen, 2004; Bullock & Hammond, 2003). Studies have shown that caregiver dependence is predictive of nursing home placement and mortality (Cohen-Mansfield, Marx, Lipson, & Werner, 1999; Yaffe et al., 2002). Research has also shown that declines in ADLs contribute to an overall decline in residents’ QoL and increases risks for falling and fractures (Allan, McKeith, Ballard, & Kenny, 2006; Andersen et al., 2004; Ballard, Bannister, Solis, Oyebode, & Wilcock, 1996). Despite the risks, interventions focused on skill-building, environmental guidance, and endurance activities (e.g., walking, balance exercises) are related to increased feelings of competence and self-efficacy for ADLs, as well as improved perceptions of QoL (Logsdon et al., 2007). Studies examining factors and interventions that contribute to or alleviate risks for poor psychological outcomes have also been identified in the literature.
Montessori-based activity programs
Originally designed to teach young children cognitive and social skills, the Montessori education model encompasses individualized instruction designed to enhance practical life skills and sensorial experiences (Montessori, 2014). Montessori practices have been found effective for children as they simplify tasks, provide immediate feedback, and promote individualized supervision and learning (Lillard, 2008). Long-term care facilities began applying Montessori practices to the care of older adults with dementia as a result of several noted parallels with school-aged children (Orsulic-Jeras, Schneider, Camp, Nicholson, & Helbig, 2001). Similar to how children learn life skills, long-term care facilities for geriatric populations began to adopt MOBAs that rehabilitated residents’ mental and physical capacities (Camp, 2010).
The individualized design and intellectual stimulation associated with MOBAs may increase social engagement and decrease agitation among older adults with dementia in adult day care settings (Judge et al., 2000; van der Ploeg et al., 2013). Furthermore, Montessori materials may enhance attention, social engagement, affect, as well as decrease agitation among long-term care residents with dementia (Judge et al., 2000; van der Ploeg et al., 2013; Vance & Johns, 2003). Other studies have shown MOBAs increased participation in residential care settings, decreased problem behaviors, and helped meet the psychological needs of residents (Giroux, Robichaud, & Paradis, 2010). A systematic review (Sheppard, McArthur, & Hitzig, 2016) of 14 studies indicated strong evidence to support the use of MOBAs to decrease difficulties with eating and mixed—though generally positive—evidence showing an increase in engagement and positive affect. The use of MOBAs to improve cognitive functioning was not well supported by the evidence assessed in the same review.
Studies assessing the use of MOBAs among individuals with late-stage dementia are scarce although some studies using mixed-severity samples have been conducted. Orsulic-Jeras and Judge (2000) conducted a study of the effect of MOBAs on engagement and affect in 16 residents of long-term care facilities diagnosed with late-stage dementia. They found that participants in the Montessori program exhibited more active engagement in activities, pleasurable affect, and less anxiety compared to a control group. A similar study by Camp and Skrajner (2004) assessed engagement and affect in a resident-led Montessori program with four resident leaders with milder dementia and nine residents with advanced dementia. In the participants with advanced dementia, the researchers observed an increase in active engagement during Montessori activities compared to baseline and standard activities but did not find evidence to support an increase in positive affect, such as pleasure. In both studies, the samples were relatively small, and the majority of participants with advanced dementia were overwhelmingly female. In addition, studies of Montessori-based interventions often inconsistently describe their participant inclusion/exclusion criteria and details of the programs themselves, which creates further difficulties in examining the evidence for their effectiveness (Sheppard et al., 2016). Thus, research findings seem to support the use of MOBAs, but evaluations of these practices in long-term care facilities and among those with late-stage dementia require further exploration.
Method
The purpose of the current study was to evaluate the implementation of an eight-month MOBA program among residents with late-stage dementia living in a long-term care facility, most of whom were diagnosed with AD. MOBA program activities included the following: customized lesson planning, immediate feedback, intellectually stimulating exercises, sensory puzzles and games, group readings, and engagement in household activities. The primary goal was to focus on maintaining abilities that do not diminish in late-stage dementia (e.g., feeling happiness, understanding facial expressions, experiencing touch). Activity leaders developed lesson plans for each participant based on his or her interests and capabilities. Though lesson plans were tailored to the individual, the majority of activities were group-oriented. These activities were integrated into every facet of the resident’s daily activities (including basic ADLs) where possible and conducted seven days per week. The length of time for individual activities varied, with a simple hand massage lasting around 5 minutes and laundry sorting lasting from 30 to 60 minutes. Group activities lasted about 30 minutes on average. Participants had the right to refuse participation in any activity and were provided with alternatives where appropriate. For example, a resident who was sensitive to multiple stimuli was invited to take a walk with a staff member in lieu of participating in a group activity. Finally, staff were allowed to modify activities according to the resident’s ability to ensure success. To illustrate, staff modified a flower arranging activity to allow a resident with severe motor impairment to successfully participate by pointing and verbally communicating to a staff member about arranging the flowers. Thus, the MOBA program provided a balance of structure and flexibility in daily activities. It is important to note that MOBA program activities occurred for every resident in the study sample for the vast majority of her/his waking hours, excluding intervals of autonomy/privacy such as eating and using restroom facilities.
Staff were extensively trained in the MOBA approach. Certified MOBA instructors conducted three monthly, in-house training sessions, each 1–2 days in length, totaling 26 hours. Staff members who attended the trainings included administrators, nursing/clinical staff, direct care workers, programming and activity leaders, food and beverage staff, environmental services staff, and a member from the Board of Trustees. The instruction agenda discussed the following topics: MOBA care philosophy, principles, the types of dementia, communication adaptations for different stages of dementia, managing challenging behaviors, personal care, approach to activities, and MOBA techniques (e.g., threading, skill assessment, etc.). The training concluded with two phases of an embedding process in which three MOBA instructors visited Hope Village for three consecutive days in both October and November 2013. The instructors worked beside staff to embed MOBA programming and principles learned in the prior training sessions. Further, a lead social worker at the facility was selected to oversee all programming. In addition to receiving MOBA training, the social worker attended additional conferences and trainings lead by MOBA and continued to work with and train activity leaders to reinforce the MOBA approach and ensure that Montessori approaches were followed throughout the study.
This study did not exclusively focus on clinical diagnoses of specific types of dementia (e.g., AD, vascular dementia), but used a sample of residents experiencing symptoms of advanced or late-stage dementia. Older adults with late-stage dementia were identified by two criteria: a medical diagnosis of late-stage dementia and the facility’s threshold for level of care. Threshold for level of care refers to the severity of the individual’s cognitive decline and the subsequent attention needed from the long-term care staff. An observed score of 4 or 5 on the facility-based threshold of care assessment indicated the resident was not able to independently complete the activity (e.g., unable to feed themselves, completely dependent for mobility, needed assistance bathing). For example, an individual scoring a 4 would require significant assistance in mobility, dressing, toileting, eating, etc. while an individual scoring a 5 would be bed-bound, fully incontinent, and nonverbal. Accordingly, participants in this study possessed high scores across numerous categories of the threshold level of care assessment, indicating exceedingly poor functioning. Due to time constraints, a standardized measure (e.g., Mini-Mental State Examination (MMSE)) was not used to determine participants’ cognitive ability; however, residents scoring a 4 or 5 on the facility-based measure were determined to be comparable to stage 6 or 7 on Reisberg, Ferris, de Leon, and Crook’s (1982) Global Deterioration Scale, indicating severe or very severe cognitive decline. The study took place in a long-term care facility in the Deep Southern region of the US (e.g., Alabama, Mississippi, Louisiana) named, for the purpose of this study and to ensure anonymity of participants, Hope Village.
Design and sampling
The research design for this study was an interrupted time series design. Permission to conduct the study was granted by the appropriate academic institutional review board and Hope Village administration. Participants included all Hope Village residents deemed by nursing staff as late- or end-stage dementia at the time of the study (N = 43). The sample initially appears to be small; nonetheless, we affirm the number of participants in this study to be meaningful, especially given the dearth of evaluations of interventions among individuals with late- or end-stage dementia (Volicer, 2005). Prior to implementation, informed consent from participants’ primary caregivers was obtained. Severity of cognitive impairment among the participants did not allow for self-consent or self-report on data. To compensate for these limitations, Hope Village staff facilitated discussions with caregivers and care recipients about the aims and methods of the study in order to obtain assent from care recipients.
Participants were evaluated in three-month intervals, with the first occurring in the early implementation of MOBA (baseline) in February 2014. Each participant was evaluated prior to the starting the MOBA program in order to establish a clear baseline. Evaluation of participants was observation-based with corresponding measurements. Each participant was observed and coded by trained Hope Village staff to maintain confidentiality. Non-identifying demographic data were obtained via chart records. All participants participated daily in MOBA, and all participants’ chart records included a physician’s diagnosis of AD or dementia.
Measures
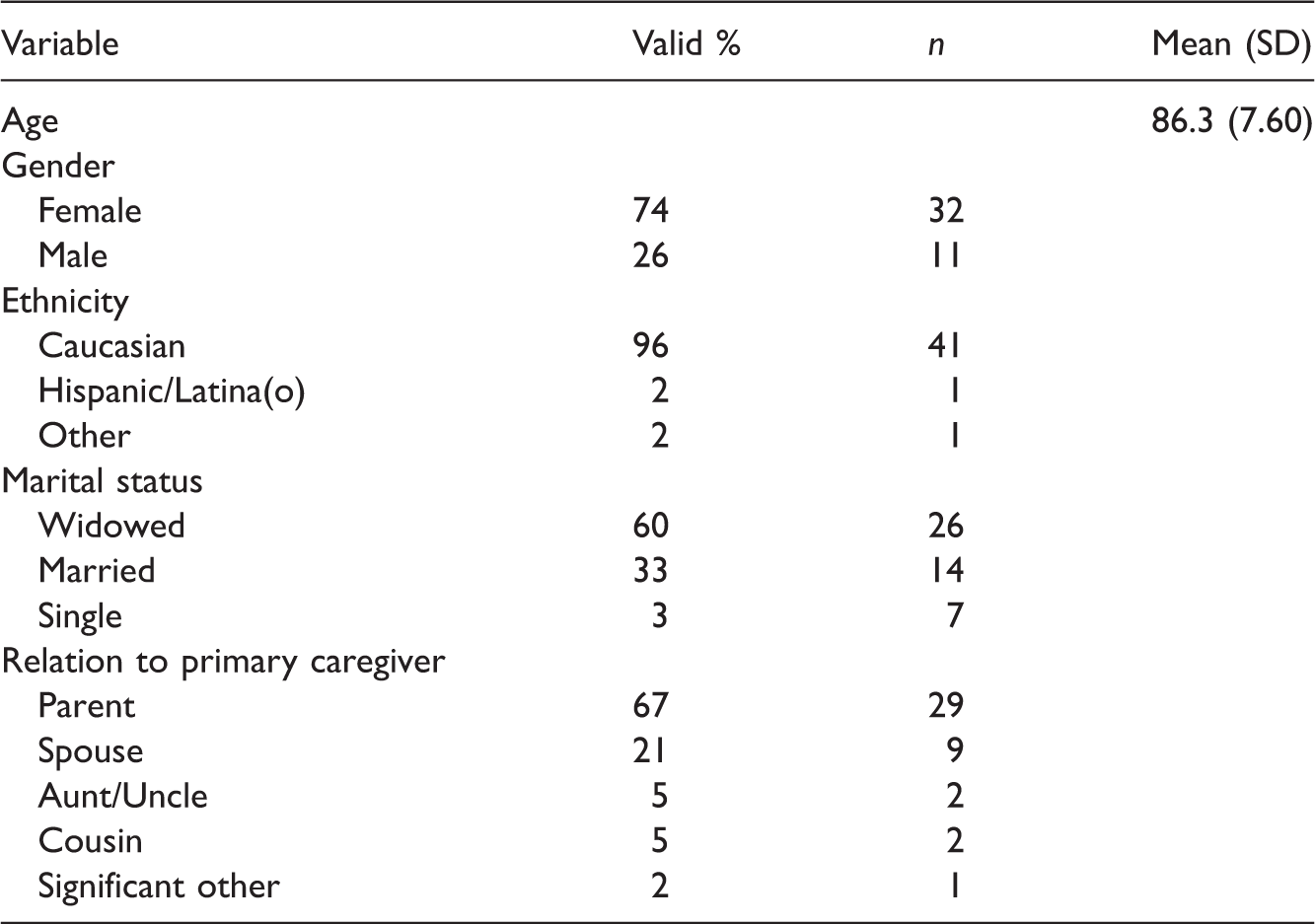
Demographic data were collected relating to age, gender, ethnicity, marital status, and relationship to caregiver. In choosing each behavioral and psychological health outcome scale, precedence was placed on selecting observation-based measures tailored to individuals living with dementia and designed for use with a proxy or caregiver when possible. While more current or gold standard scales may have existed for some outcomes (e.g., Katz ADL and Lawton IADL scales), the researchers prioritized using measures specifically designed for assessing those living with dementia. These scales are described below.
Problem behaviors
The frequency of problem behaviors subscale from the 24-item Revised Memory & Behavior Problems Checklist, or RMBPC, was selected for its brevity and specificity to problem-behaviors in individuals with dementia (Teri et al., 1992). Examples of items on the RMBPC include destroying property and dangerous behaviors to self and others. Global scores were calculated via the sum of responses for each item. Range of possible global scores on the RMBPC scale is 0–24, with higher scores indicating greater frequency of problem behaviors over the past seven days. A satisfactory Cronbach’s alpha of 0.78 has been reported on this measure (Roth et al., 2003). The RMBPC has been validated for use in assessing problem behaviors among individuals with dementia and was previously strong construct validity through confirmatory factor analyses and convergent validity with similar depression and cognition measures (Roth et al., 2003; Teri et al., 1992)
Social engagement
The six-item Index of Social Engagement, or ISE, is one of the only standardized, observation-based social engagement measures for use with older adults (Mor et al., 1995). Examples of items on the ISE include ease of interacting with others and pursuit of facility activities. Each item contained a yes/no response format, with yes = 1 and no = 0. Global scores were calculated via the mean of scored items. Range of possible global scores is 0–6, with higher scores indicating greater levels of social engagement over the past seven days. A reliability alpha of .79 has previously been reported (Mor et al., 1995). The ISE has been previously validated for use among older adults across care setting, functional ability, country and shows strong construct validity (Mor et al., 1995; Schroll, Jonsson, Mor, Berg, & Sherwood, 1997).
Activities of daily living
The 20-item Bristol Activities of Daily Living Scale, or BADL, was selected for its appropriateness as an activity of daily living (ADLs) instrument for individuals with dementia that can be completed via proxy assessment (Bucks, Ashworth, Wilcock, & Siegfried, 1996). Global scores were calculated via the mean of scored items (to accommodate item responses of not applicable). The range of possible global scores on the BADL is 0–3, with higher scores indicating greater capacity to conduct common ADLs over the previous two weeks. As we could not find reliability statistics on the BADL in prior research, Cronbach’s alpha on this measure was determined in the current study at 0.647. Previous studies have shown strong construct validity as demonstrated through a four-factor solution to match its four theoretical domains (IADLs, self-care, orientation, and mobility), convergent validity with nurse-rated ADL performance and cognitive functioning, and sensitivity to change over time (Bucks et al., 1996; Byrne, Wilson, Bucks, Hughes, & Wilcock, 2000).
Quality of life
The Quality of Life-Alzheimer’s Disease Scale, or QoL-AD, was selected for its brevity, strong reliability, ease-of-administration, and widespread use in QoL research for individuals with dementia (Logsdon, Gibbons, McCurry, & Teri, 1999). This 13-item, four-point Likert response measure was created specifically for use with persons with dementia and was developed using input from individuals with dementia, caregivers, and dementia experts. A strength of this measure is that it may be used as a self-assessment, proxy-assessment, or both. Examples of items on the QoL-AD include physical health, energy, mood, and ability to do things for fun. Global scores range from 13 to 52, with higher scores indicating a greater QoL. While the lookback period for this measure is not specifically indicated, the scale instructs caregivers to rate items according to the care recipient’s functioning within the past few weeks. Reliability alpha in previous research was observed at 0.82 (Thorgrimsen et al., 2003). The QoL-AD has been validated for use with individuals across severity levels of dementia (Hoe, Katona, Roch, & Livingston, 2005; Thorgrimsen et al., 2003) and shown to have good content (Thorgrimsen et al., 2003) and convergent validity with measures of QoL, cognition, functional status, mood, and general health (Hoe et al., 2005; Logsdon et al., 1999; Thorgrimsen et al., 2003).
Anxiety
The Rating for Anxiety in Dementia, or RAID, is a short, 18-item anxiety measure selected for its specificity in assessing anxiety over the previous two weeks in individuals with dementia (Shankar, Walker, Frost, & Orrell, 1999). While other measures may be more widely used, the RAID is shorter, easy to administer, and the items capture more specific anxiety symptoms. Its psychometric properties are sound (Shankar et al., 1999). Examples of items on the RAID include worries about health, finances, and family; edginess; and sleep disturbances. One response option on the RAID is “unable to evaluate,” which can leave missing scores. As such, global scores were calculated via the mean of scored items (rather than summing all items). The original development study showed a strong internal consistency coefficient 0.83 with evidence supporting its construct validity and convergent validity with other anxiety measures, expert ratings, and Diagnostic and Statistical Manual of Mental Disorders (4th Edition) (DSM-IV) criteria (Shankar et al., 1999).
Psychological well-being
The Psychological Well-Being in Cognitively Impaired Persons scale, or PWB-CIP, is an 11-item, five-point Likert response measure chosen for its brevity and for its appropriateness as a proxy measurement for well-being in individuals with cognitive impairment over the past 24 hours (Burgener, Twigg, & Popovich, 1995). Although the psychometric properties of this measure have not been extensively tested, other well-being measures are not typically intended for use as a proxy measure or made specifically for individuals with cognitive impairment or dementia. Examples of items on the PWB-CIP include various facial expressions and positive verbal responses. Global scores were calculated via the sum of responses for each item. Reliability alphas of this measure in previous research have been shown to range from 0.79 to 0.82 (Burgener et al., 2005). The PWB-CIP was previously shown to be a valid measure for use in individuals with cognitive impairment across care setting, geographical setting (Burgener et al., 2005). The scale also has good construct validity through significant correlations with measures of personality characteristics, cognition, depression, behavioral factors, and social engagement (Burgener et al., 2005).
Analytic strategy
Sample characteristics were reported via frequencies/percentages for non-parametric variables (e.g., gender, ethnicity) and central tendency for the parametric variable of age. Descriptive statistics for all of the behavioral health outcome variables were reported via central tendency. Paired-samples t-tests were conducted to determine whether aggregate or mean scores of a given outcome variable were significantly different between data intervals. To examine the influence of each categorical demographic factor (e.g., gender) on an outcome variable, a t-test or ANOVA was conducted. To examine the influence of each parametric, demographic factor (e.g., age) on an outcome variable, linear regression was conducted. Missing data for a given scale item were computed via mean substitution derived from the remainder of the same scale items for the specific data collection interval. Significance threshold was set at the traditional standard of 0.05.
Results
Sample characteristics
Sample characteristics (N = 43).
Problem behaviors
To iterate, the range of possible global scores on the RMBPC scale is 0–24, with higher scores indicating greater frequency of problem behaviors. The sample in reported RMBPC aggregate global scores as follows:
interval 1 showed a mean RMBPC global score of 5.2 (SD = 3.66); interval 2 showed a mean RMBPC global score of 5.2 (SD = 3.78); and interval 3 showed a mean RMBPC global score of 4.8 (SD = 3.50).
Statistical differences between data collection intervals among RMBPC global scores were observed as follows:
no significant change between intervals 1 and 2 (t = 0.882, p = .38); no significant change between intervals 2 and 3 (t = 0.01, p = .99); and overall, no significant change between intervals 1 and 3 (t = 0.849, p = .40).
No demographic factor in this study showed significant influence on RMBPC scores. See Figure 1 for illustration of these longitudinal changes.
Longitudinal change in Revised Memory & Behavior Problems Checklist (RMBPC) scores (frequency of problem behaviors).
Social engagement
To iterate, the range of possible global scores on the ISE is 0–6, with higher scores indicating greater levels of social engagement. The sample in this study reported ISE aggregate global scores for each data interval as follows:
interval 1 showed a mean ISE global score of 3.0 (SD = 2.19); interval 2 showed a mean ISE global score of 2.8 (SD = 1.92); and interval 3 showed a mean ISE global score of 2.6 (SD = 2.24).
Statistical differences between data collection intervals among ISE global scores were observed as follows:
no significant change between intervals 1 and 2 (t = 1.121, p = .27); significant decrease between intervals 2 and 3 (t = 2.065, p < .05); and overall, significant decrease between intervals 1 and 3 (t = 2.197, p < .05).
No demographic factor demonstrated significant influence on ISE scores. See Figure 2 for illustration of these longitudinal changes.
Longitudinal change in Index of Social Engagement (ISE) scores (social engagement).
Activities of daily living
To iterate, the range of possible global scores on the BADL is 0–3, with higher scores indicating greater capacity to conduct common ADLs. The sample in this study reported BADL aggregate global scores as follows:
interval 1 showed a mean BADL global score of 1.2 (SD = 0.79); interval 2 showed a mean BADL global score of 1.1 (SD = 0.75); and interval 3 showed a mean BADL global score of 1.0 (SD = 0.76).
Statistical differences between data collection intervals among BADL global scores were observed as follows:
significant decrease between intervals 1 and 2 (t = 2.115, p < .05); no significant change between intervals 2 and 3 (t = 0.640, p = .53); and overall, significant decrease between intervals 1 and 3 (t = 2.948, p < .01).
Again, no demographic factor in this study exerted significant influence on BADL scores. See Figure 3 for illustration of these longitudinal changes.
Longitudinal change in Bristol Activities of Daily Living Scale (BADL) scores (capacity for activities of daily living (ADLs)).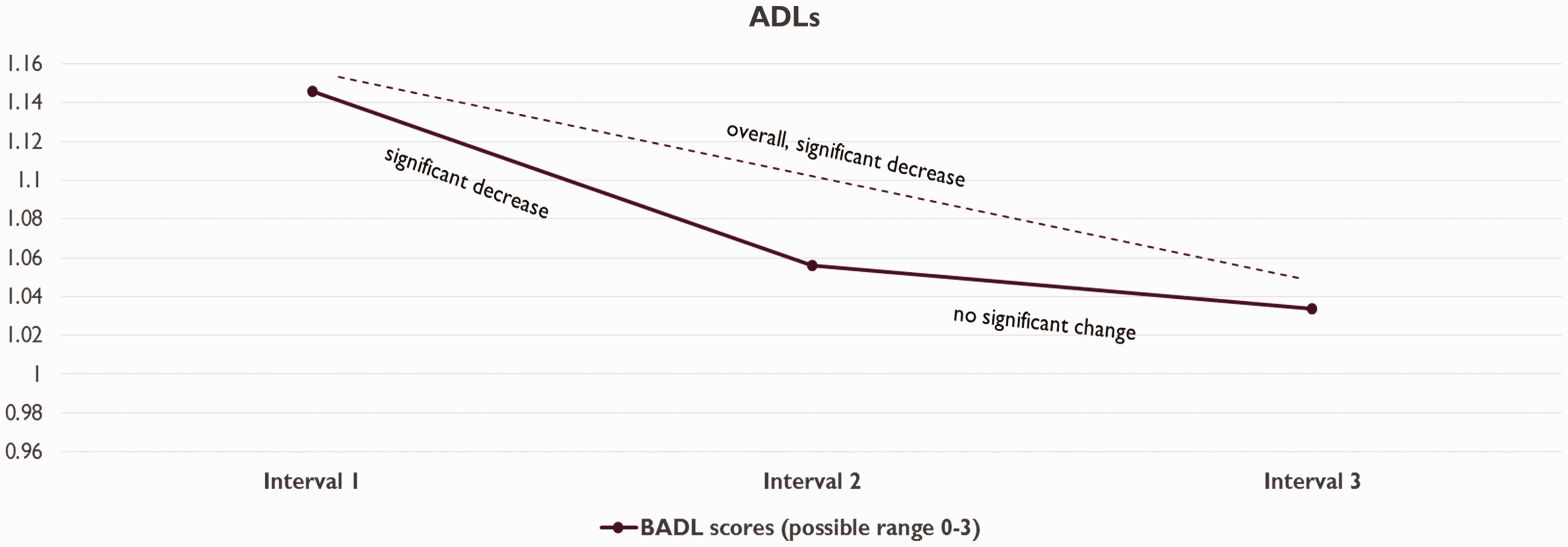
Quality of life
The range of possible global scores on the QoL-AD scale is 13–52, with higher scores indicating higher QoL. The sample in this study reported QoL-AD aggregate global scores as follows:
interval 1 showed a mean QoL-AD score of 27.2 (SD = 8.03); interval 2 showed a mean QoL-AD score of 28.6 (SD = 7.58); and interval 3 showed a mean QoL-AD score of 27.8 (SD = 8.34).
Statistical differences for QoL-AD scores among data collection intervals were as follows:
significant increase between intervals 1 and 2 (t = − 2.29, p < .05); significant decrease between intervals 2 and 3 (t = 3.061, p < .01); and no significant change between intervals 1 and 3 (t = 0.44, p = .66).
Caregiver’s relation to care recipient, specifically widowed persons showed significantly higher quality life than single persons at baseline (p < .01). The remaining demographic factors showed no significant influence on QoL-AD scores. See Figure 4 for illustration of these longitudinal changes.
Longitudinal change in Quality of Life-Alzheimer’s Disease Scale (QoL-AD) scores (quality of life).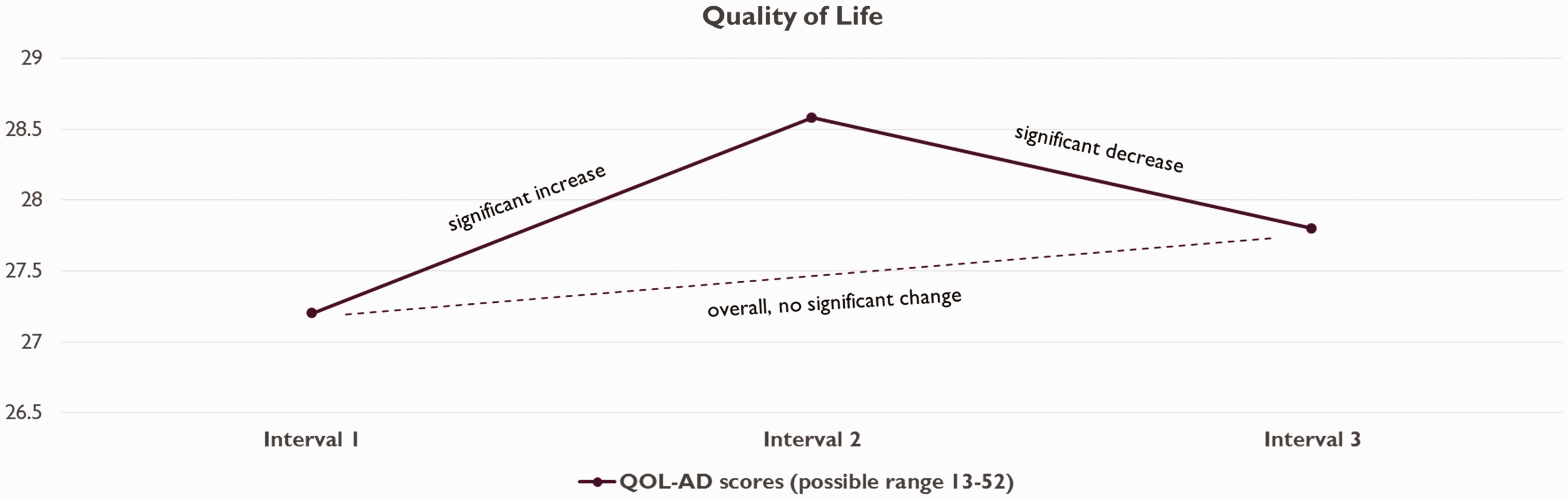
Anxiety
The range of possible global scores on the RAID scale is 0–3, with higher scores indicating greater severity of anxiety. The sample in this study reported RAID aggregate global scores as follows:
interval 1 showed a mean RAID score of 0.3439 (SD = 0.35); interval 2 showed a mean RAID score of 0.2893 (SD = 0.35); and interval 3 showed a mean RAID score of 0.3025 (SD = 0.31).
Statistical differences for anxiety among data collection intervals were as follows:
no significant change between intervals 1 and 2 (t = 0.482, p = .632); significant increase between intervals 2 and 3 (t = − 2.353, p < .05); and no significant change between intervals 1 and 3 (t = 0.66, p = .514).
No demographic factors showed significant influence on RAID scores. See Figure 5 for illustration of these longitudinal changes.
Longitudinal change in Rating for Anxiety in Dementia (RAID) scores (anxiety).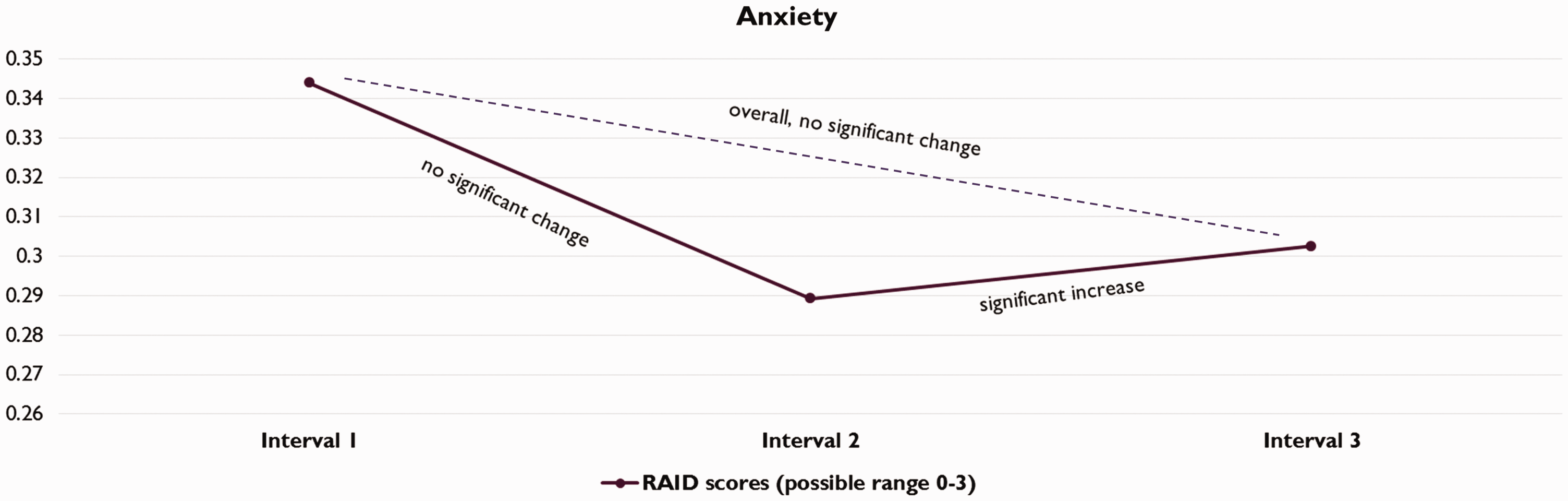
Psychological well-being
The range of possible global scores on the PWB-CIP scale is 11–55, with higher scores indicating higher levels of psychological well-being. The sample in this study reported PWB-CIP aggregate global scores as follows:
interval 1 showed a mean PWB-CIP score of 42.5 (SD = 8.18); interval 2 showed a mean PWB-CIP score of 40.4 (SD = 9.48); and interval 3 showed a mean PWB-CIP score of 41.2 (SD = 6.90).
Statistical differences for psychological well-being among data collection intervals were as follows:
significant decrease between intervals 1 and 2 (t = 2.03, p < .05); significant increase between intervals 2 and 3 (t = 2.98, p < .01); and significant decrease between intervals 1 and 3 (t = 2.97, p < .01).
No demographic factors showed significant influence on psychological well-being scores. See Figure 6 for illustration of these longitudinal changes.
Longitudinal change in Psychological Well-Being in Cognitively Impaired Persons scale (PWB-CIP) scores (psychological well-being).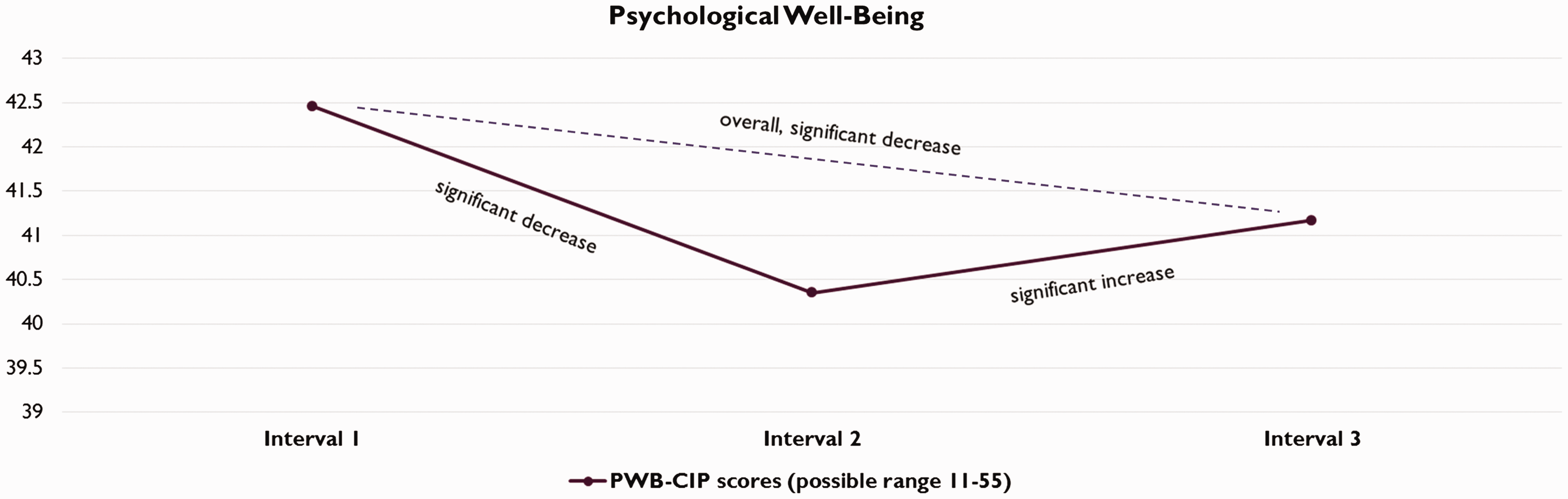
Discussion
The results of this study indicated the effects of Hope Village’s MOBA program moderately reduced problem behaviors, yet significantly decreased social engagement and ADL capacities for a sample of individuals diagnosed with late-stage dementia. Ostensibly, the trends in this study might appear dissimilar from other studies. Yet, this study focused on late stage dementia, whereas previous literature included early-to-middle stage dementia and/or mixed samples. Also, the current study examined mostly distinct domains, as compared to previous studies (exception: problem behaviors). Therefore, a comparison to previous studies would be somewhat unfair.
As previously discussed, studies of MOBAs have shown an increase in activity engagement (Camp & Skrajner, 2004; Giroux et al., 2010; Orsulic-Jeras et al., 2000; Sheppard et al., 2016), decrease in behavioral symptoms of dementia (van der Ploeg et al., 2013), and improvement in eating behaviors (Sheppard et al., 2016) among individuals with dementia. The current study, however, showed a decrease in social engagement, overall ADL functioning, and a mild decrease in problem behaviors in participants overall. Though a comparison of this result to the aforementioned studies on engagement seems warranted, the current authors took a slightly different tack by assessing social engagement—a substantive difference from prior observations on activity engagement. For ADL functioning, the prior literature mentioned decline in eating behaviors among MOBA recipients, a distinct aspect of ADL functioning. The current study observed overall ADL functioning and noted a similar decline, though no measure of specific eating behavior was used.
The remaining three, health outcome domains showed mixed results, thereby rendering their overall (entire study period) results somewhat confounding:
QoL increased initially but diminished in the final period; anxiety decreased initially but elevated in the final period; and psychological well-being decreased initially but elevated in the final period.
In viewing these results, it is important to consider that a decrease in social engagement may have been influenced by the individualized design and structure of the MOBA. A focus on personalized tasks and immediate feedback from facility staff may have influenced the time residents were allotted for engagement with others. Further, since dementia symptoms worsen over time, loss of the ability to speak, hear, and memory loss, may have negatively influenced residents’ competencies for socialization and ADLs. Loss of other abilities may also explain the decrease in problem behaviors (e.g., loss of physical or cognitive motor skills). Most notably, moderate changes in ADL capacities between time intervals possibly indicate that the MOBA helped to decelerate the loss of these capacities, although the inclusion of a control group would be needed to formally test this assertion. As previous MOBA research has heavily examined eating behaviors (Sheppard et al., 2016), future research may benefit from focusing on each ADL domain as a separate outcome rather than as a single construct. This finding may be deemed especially important as existing research points toward the importance of maintaining ADL capacities in order to improve overall QoL (Logsdon et al., 2007). As such, long-term care facilities aimed at improving the overall QoL for residents may consider the use of MOBAs.
It is important to briefly note the limitations of this study and implications for future research. Utilizing a quasi-experimental, interrupted time series design may have been the most ethical decision regarding the sample of late-stage dementia residents in a long-term care facility; however, introducing randomized assignment to treatment and control conditions would have increased internal validity. Further, quasi-experimental designs are subject to contamination by confounding variables. In the case of the current study, maturation could be a contaminating factor as rapid physiological and cognitive deterioration from late-stage dementia is a medical consequence. The use of observational methods with a small sample may have affected the reliability of the data gathered in this study. Social desirability, observer biases, and a lack of inter-rater agreement between nursing staff members should be noted. In contrast, the uses of said methods were needed due to the inability to collect self-report data and for recording longitudinal changes amidst a hard to reach population. Future research with a larger sample and greater assurances of differentiated experiences of late-stage dementia residents is recommended to enhance understanding of MOBAs on behavioral and social outcomes. Future research should also consider using QoL measures and multiple observers (e.g., social workers, doctors, caregivers, etc.) to augment the reliability of the data.
In summary, this study was needed as residents with late-stage dementia warrant the same level of research attention as other medical or clinical populations. Health care professional hold an ethical obligation to research difficulties and resiliencies among these individuals and overcome methodological challenges to redress gaps in the literature. The results of this study have considerable implication for long-term care providers as the potential maintenance of ADL capacities may not only support a better QoL among residents, but also alleviate demands on long-term care facilities staff and resources. Effective MOBAs may also help counteract the expectant economic strain of dementia on caregivers, long-term care facilities, and the health care system as a whole. Altogether, the findings of this study support the use and future research of MOBAs for targeting behavior problems among residents with late-stage dementia in long-term care facilities, yet its effect on social engagement and ADLs warrants additional investigation.
Footnotes
Authors’ Note
All ethical standards and independent objectivity were strictly obeyed via the LSU Institutional Review Board and Poydras Home administrators.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Poydras Home of New Orleans.