
Abstract
This study examined public stigma associated with Alzheimer’s disease (AD) among Korean Americans and identified factors affecting their public stigma. Data used in the study were collected using a cross-sectional survey with 268 Korean Americans. Guided by attribution theory, different domains of public stigma were assessed: pity, antipathy, and social distance. Hierarchical regression analyses were conducted to examine the effects of sociodemographic characteristics, exposure to AD, social networking, and AD knowledge on each stigma domain. The influence of emotional attributions (pity and antipathy) on behavioral attributions (social distance) in the stigma process suggested in attribution theory was also examined. Results show that pity is most prevalent followed by social distance and antipathy. Being more proficient in English, knowing fewer relatives/friends with AD, and knowing less about AD risk factors are associated with having more pity stigma. Being less socially engaged and knowing less about AD risk factors are related to having more antipathy stigma. Being younger and more proficient in English and having stronger antipathy stigma are associated with having more social distance stigma. Findings reveal multifaceted nature of public stigma associated with AD in Korean Americans and suggest that we need to work on both positive and negative sides of public stigma for stigma change. Findings of different factors associated with each public stigma domain can be considered when trying to foster and/or reduce certain stigmatic beliefs and behaviors associated with AD.
Introduction
Alzheimer’s disease and related dementias (ADRD) have become a public health priority due to their tremendous burden on affected individuals, families, and society (World Health Organization, 2012). In the U.S., national plans were developed to address various aspects of ADRD, and they suggest reducing stigma associated with ADRD as a priority action item (Centers for Disease Control and Prevention and the Alzheimer’s Association, 2013; U.S. Department of Health and Human Services, 2017).
Stigma refers to a “social cultural process by which members of marginalized groups are labeled by others as abnormal, shameful, or otherwise undesirable” (Jones & Corrigan, 2014, p. 9). In mental health research, stigma has received much attention in the context of serious mental illnesses such as depression, schizophrenia, and bipolar disorders due to its negative consequences: Stigma can cause persons with mental illness to deny the condition and refuse to seek diagnosis and treatment (Corrigan & Kosyluk, 2014). Family members of individuals with mental illness can experience psychological distress and burden generated by stigma (Ostman & Kjellin, 2002) and it can adversely affect caregiving and support. Among different types of stigma, public stigma has been widely studied because it can be a basis of other types of stigma such as self-stigma and structural stigma (Jones & Corrigan, 2014; Larson & Corrigan, 2008) and therefore it is central in reducing stigma (Byryn, 2001). Public stigma occurs when the general public assigns stereotypes to a group and acts on discriminatory behaviors (Jones & Corrigan, 2014; Larson & Corrigan, 2008). Public stigma results in daily life discrimination in interpersonal interaction as well as interactions with various systems in society (Jones & Corrigan, 2014; Rusch et al., 2005). Existing research about public stigma associated with mental illnesses reports stigma such as fear, dangerousness, withdrawal, avoidance, blame, and shame (Corrigan & Kosyluk, 2014).
Research on stigma associated with Alzheimer’s disease (AD) is developing yet relatively limited. Two recent systematic reviews of empirical studies addressing different types of dementia stigma located only 48 studies from 1990 to 2012 (Werner, 2014) and 51 studies from 2004 to 2014 (Herrmann et al., 2018). Albeit limited, the existing research indicates that public stigma associated with AD is different from public stigma of mental illnesses. For example, fear and dangerousness prevalent in serious mental illnesses are not common in AD public stigma (Werner et al., 2010; Werner, Mittelman, et al., 2011). Information about correlates of public stigma associated with AD can be used for effort toward stigma change. Werner (2005) found that higher familiarity with someone with AD was associated with more stigma (i.e., prosocial and aggression feelings) whereas no such relationship was found in another studies (Blay & Peluso, 2010; Werner & Davidson, 2004). Among sociodemographic characteristics, men expressed more stigma (i.e., rejection feeling) in one study (Werner & Davidson, 2004) while gender was not found to play a role in another study (Blay & Peluso, 2010). Studies also reported possible effects of education in stigma where higher education was associated with lower levels of stigma (Blay & Peluso, 2010; Werner, 2005). Overall, no clear pattern has emerged about correlates of AD stigma and this underscores a need to conduct more research to examine the context of AD public stigma.
Another gap identified in the existing research about AD stigma is that many studies are atheoretical. Seventy-three percent of the studies in Werner’s systematic review (2014) did not use any specific theoretical framework and conceptualized AD stigma in a colloquial way. There are two commonly used theoretical frameworks in mental health research when examining stigma. The first one is modified labeling theory which contends negative consequences of mental illness labeling on individual’s self-stigma and social ties (Link et al., 1989). The second one is attribution theory which identifies stigma as a process with different attributions. That is, stereotypes (cognitive attributions) yield prejudice (emotional attributions), which leads to discrimination (behavioral attributions) (Friske, 1998; Ottari et al., 2005).
Our review could locate only few studies about AD public stigma based on a theoretical background. For example, using modified labeling theory, Wadley and Haley (2001) found that, compared to major depression diagnosis, AD diagnosis (labeling) evoked more sympathy, less anger, and greater willingness to help. Studies based on attribution theory (Blay & Peluso, 2010; Stites et al., 2018; Werner & Davidson, 2004) found that there were two sides of emotional attributions in AD public stigma and AD elicits more positive emotions (e.g., compassion, concern, sympathy, and pity) than negative emotions (e.g., embarrassment, disgust, and disgrace). Behavioral attributions also have two sides and the rates of prosocial reactions (e.g., desire to help, warmth, and friendliness) were higher than antisocial reactions (e.g., irritation, desire to distance, and indifference) (Blay & Peluso, 2010). Attribution theory suggests interrelationship between different attributions of stigma, and one study found that positive emotional attributions (e.g., sympathy, concern, and compassion) decreased behavioral attribution (e.g., discrimination) and negative emotional attributions (e.g., rejection, ridicule, and impatience) increased discrimination (Werner, 2005). While these studies provide some insights in understanding multifaceted aspects of public stigma related to AD, more studies that are theoretically grounded are still needed so that we can systemically assess and build evidence of potentially multidimensional nature of public stigma associated with AD.
An additional area that requires our attention is a paucity of studies that directly addressed AD stigma in a minority population such as Asian Americans. This point is well addressed in Herrmann et al.’s (2018) systematic review of studies on dementia stigma during a recent decade. Asian Americans are one of the two ethnic minority groups in the U.S. with the largest projected increase of older adults in their population (Vincent & Velkoff, 2010). This projection has resulted in growth of AD caregiving research in the population (Miyawaki, 2015), yet research on AD stigma in this population is still scarce. Our review could locate only a handful of empirical studies of which the main focus is AD stigma in Asian Americans. In a study of lay Chinese Americans, Woo and Mehta (2017) reported several stigmatizing views associated with AD, such as difficulties in communication, being impulsive and unpredictable, and social distancing. Another study of older Korean Americans (KAs) found that 14% of the study’s participants expressed feeling shame for having a family member with AD (Jang et al., 2010). Overall, these previous studies have provided a beginning understanding about stigmatic beliefs associated with AD in Asian Americans. However, lack of theoretical framework and the use of a colloquial conceptualization of stigma are apparent in the existing research involving Asian Americans.
Evidence about correlates of public stigma associated with AD in the Asian American context is inconclusive and it urges more research about the topic. Women were less likely to have a stigmatizing view than men in Chinese Americans (Dao & Woo, 2014) whereas no role of gender was found in KAs in relation to their feeling of shame (Jang et al., 2010). Having family members with dementia/AD was not associated with dementia stigma in Chinese Americans (Dao & Woo, 2014) and KAs (Jang et al., 2010). Lower level of education, lower level of acculturation, and less knowledge of AD were associated with increased feelings of shame among KA older adults (Jang et al., 2010).
Based on the literature review and gaps identified in the existing research described above, this study attempted to expand the existing body of research about public stigma associated with AD in Asian Americans with the following research questions and rationale: First, what is the nature and magnitude of public stigma associated with AD in KAs? Guided by attribution theory, the study investigated the nature and magnitude of distinctive stigma attributions (domains), namely, emotional (positive and negative) and behavioral attributions. Our study focused on the fifth largest subgroup of the Asian American population, KAs (U.S. Census Bureau, 2015), because subgroup approach is needed when studying Asian Americans due to the heterogeneity of their immigration history, culture, and socioeconomic status (Yeo, 2009). Second, what are the correlates of public stigma in KAs? Informed by prior studies which show a need to develop further understanding about the context of public stigma, we examined correlates of each AD stigma domain such as age, gender, education, and exposure to AD, all of which were used in prior research reviewed earlier. In addition, English proficiency was examined because it could play a role in immigrant populations like KAs in terms of attaining information from mass and social media outlets. Social networking was also examined because more social engagement and more use of technology in networking can generate more opportunities of gathering disease knowledge and information online and offline. Although it was suggested that AD knowledge can play a role in reducing stigma (Lee & Casado, 2015; Lee et al., 2010; Werner & Davidson, 2004), AD knowledge and stigma were rarely examined together. Therefore, we added AD knowledge in the analysis. Lastly, guided by attribution theory, we examined the influence of emotional attributions to behavioral attributions in the stigma process.
Methods
Participants and data collection
Data used in the study were part of a community participatory research project in a metropolitan area in the mid-Atlantic region of the U.S. where a university and a local Korean community agency formed a partnership to develop and carry out a research project. The eligibility criteria included having a Korean ethnic background (self-identification), being age 40 years or older, and being Korean or English speaking. Using convenience sampling, two bilingual and trained KA research team members recruited lay KAs residing in the community from locations such as community events and activities, Korean business sites, churches, and community centers. A total of 268 participants were recruited and participated in the study.
A cross-sectional survey was used for data collection. The survey materials were first developed in English and were later translated into Korean using Brislin’s (1970) back-translation methods. All participants completed the survey in Korean through self-administration (n = 250) and face-to-face interview (n = 18), depending on their preferences. All study procedures were approved by a University Institutional Review Board.
Measures
Public stigma was assessed using the lay person’s stigma, a dimension in the Family Stigma in Alzheimer’s Disease Scale (FS-ADS; Werner, Goldstein et al., 2011). FS-ADS was developed and tested for its validity specifically for AD context based on Corrigan (2007)’s conceptualization of stigma as a process of different attributions. We used 19 items from the lay person’s stigma dimension in two areas, emotional attributions (13 items) and behavioral attributions (6 items). The 19-item scale showed excellent reliability with the study sample, with internal consistency of α = .90. To identify potential distinctive domains of public stigma associated with AD, we conducted an exploratory factor analysis with the 19 items, which yielded three distinctive factors: pity (6 items; sadness, concern, sympathy, sorrow, pity, and compassion), antipathy (4 items; shame, embarrassment, disgust, and disgrace), and social distance (6 items; limiting social contact, limiting family ties, avoiding, ignoring, keeping away from the person, and keeping the person away from the public). Three items (fear, uneasiness, and dread) were excluded because of their cross-loadings on pity and antipathy factors. For pity and antipathy domains, participants were asked to what extent they agreed/disagreed that other people feel about a person with AD in the following ways, with a five-point Likert scale (1 = strongly disagree to 5 = strongly agree) using each descriptive word listed above. For social distance domain, participants were asked to what extent they agreed or disagreed with six statements describing behavioral reaction from a person with AD. For all three domains, summative scores were used, with higher scores indicating having more stigma about each domain. All three domains showed excellent reliability with the study sample: α = .94 for pity, α = .91 for antipathy, and α = .90 for social distance.
AD knowledge was measured using the Alzheimer’s Disease Knowledge Scale (ADKS; Carpenter et al., 2009), a 30-item true/false scale. The ADKS is designed to measure seven different domains of AD knowledge and beliefs including risk factors, assessment and diagnosis, symptoms, course of illness, life impact, caregiving, and treatment and management of AD. Each item was coded as 0 = incorrect and 1 = correct and summative scores were calculated with a possible range of scores from 0 (no correct answers) to 30 (all correct answers). The scale showed good reliability with the study sample, with internal consistency of α = .71.
Social networking was measured in two ways. First, social engagement was measured using four items from Social Engagement Composite Measure (Thomas, 2011). Participants were asked how often they talk on the phone with friends and relatives, get together with friends, attend meetings, clubs or organizations, and attend religious services, respectively. They answered with ratings of 1 = never through 6 = more than once a day/week. Summative scores were calculated indicating higher scores as being more socially engaged. The internal consistency of α for this four-item scale was .63, and the small number of items might explain the relatively low level of consistency. Second, use of technology in social networking was assessed by asking whether they use Facebook, Twitter, email, and texting with 0 = no and 1 = yes for each item. Summative scores were calculated, and higher scores indicate using more technology in social networking.
Exposure to AD was assessed in two ways. First, we measured the degree of their exposure by asking whether the person(s) with AD they had known was/were: neither family nor friends (0), either family or friends (1) or both family and friends (2). We also asked whether they have been a caregiver of a person(s) with AD (1= yes).
Sociodemographic characteristics included age (in years), gender (1 = male), education (0 = no college education, 1 = college education or higher), annual household income (1 = less than $20,000 through 6= $100,000 or higher), marital status (1 = married), U.S. born (1 = yes), and years in the U.S. English proficiency in comprehension, speaking, and reading was measured with ratings of 1 = not well at all through 4 = very well in each area and summative scores were calculated with higher scores indicating being more proficient in English.
Analysis
Descriptive statistics were used to summarize the sample and the magnitude of each domain of public stigma associated with AD. To examine relative strengths and significance of proposed correlates of AD stigma, we conducted three separate hierarchical regression analyses on each of three stigma domains. We entered the variables in the following steps: (1) sociodemographic characteristics of age, gender, education, and English proficiency; (2) exposure to AD; (3) social networking; and (4) AD knowledge. For step 4, since the AD knowledge scale used in the study encompasses various domains of knowledge, we sought to examine how certain AD knowledge domains and stigma domains are related. Three AD knowledge domains—life impact, risk factor, and caregiving—emerged as having significant association with at least one stigma domain in the correlation analysis and were included in step 4 of the regression analyses. Lastly, for the model of social distance stigma domain, we added an additional step (step 5) with two stigma domains addressing emotional attributions, pity and antipathy, in order to examine potential influence of emotional attributions on behavioral attributions as suggested in the attribution theory. All analyses were conducted using IBM SPSS Statistics 24.0.
Results
Table 1 presents the characteristics of the study sample and summarizes study variables with their descriptive statistics. The mean age of the participants was 55.7. The majority of the participants were female (60.8%) and married (81.9%), and almost half (47.4%) had college degree or higher. All participants were foreign-born and their average length of stay in the U.S. was 19.6 years. Annual household income varied, and the most reported income was $40,000 to less than $60,000 (28.7%). Approximately 21% reported having AD caregiving experience. Among the domains of AD knowledge, assessment and diagnosis and life impact showed highest accuracy (70.3% and 67.0%, respectively) and caregiving showed lowest accuracy (48%).
Descriptive characteristics of study sample and study variables (N = 268).
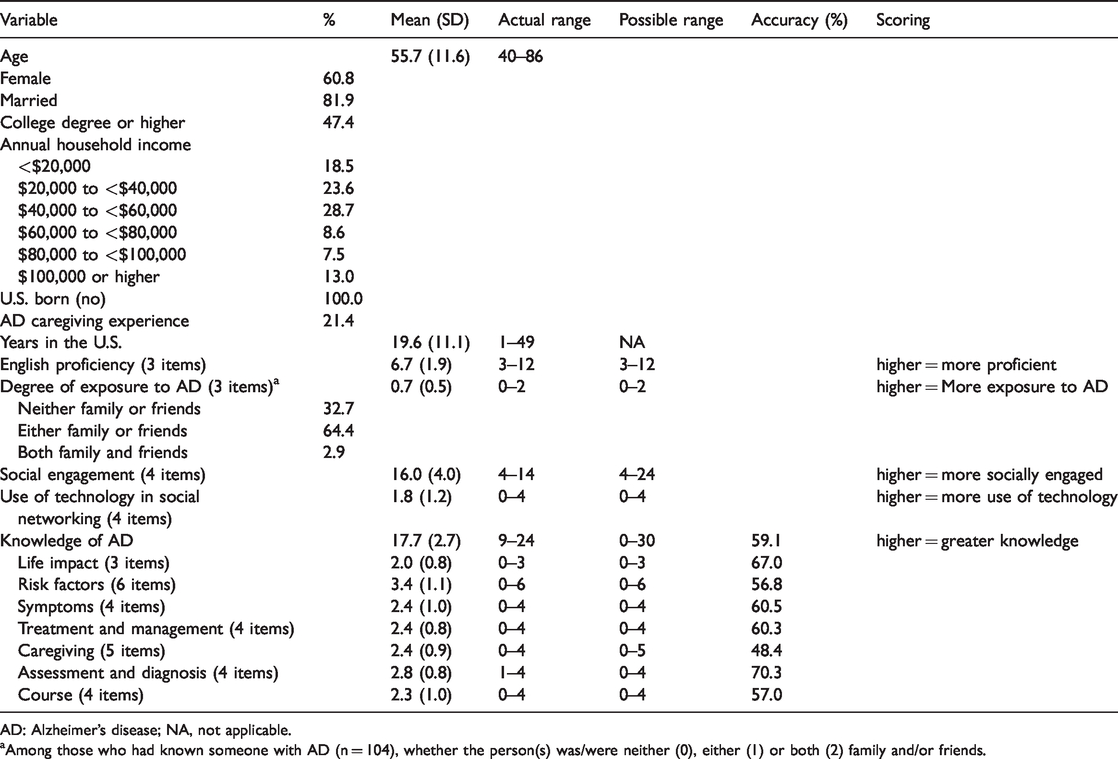
AD: Alzheimer’s disease; NA, not applicable.
aAmong those who had known someone with AD (n = 104), whether the person(s) was/were neither (0), either (1) or both (2) family and/or friends.
Table 2 presents the magnitude of three domains of public stigma. Mean score of pity domain is 19.1 (out of 30.0) and the majority of participants expressed their agreement (strongly agreed or agreed) with six items in this domain ranging from 50.2% (sorrow) to 61.2% (concern). Social distance domain was less prominent with six items ranging from 45.7% (limit social contact) to 31.6% (limit family ties) and its mean score is 17.6 (out of 30.0). Antipathy domain was least prevalent, and its four items ranged from 26.7% (shame) to 9.1% (disgust) with a mean score of 8.9 (out of 20.0).
Public stigma associated with Alzheimer’s disease.
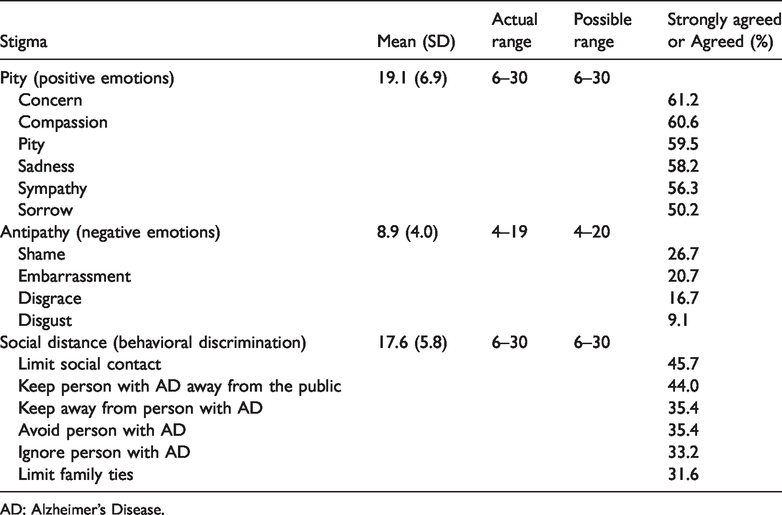
AD: Alzheimer’s Disease.
Table 3 summarizes the results of the final steps of hierarchical regression analyses on three stigma domains and presents significant correlates of each stigma domain. No multicollinearity was detected using variance inflation factors and tolerance values among independent variables in all three models of stigma domains. For pity domain, English proficiency (β = .38 p < .01), degree of exposure to family and/or friend with AD (β= –.21, p < .05), and AD risk factor knowledge (β= –.24, p < .05) emerged as significant with a significant model fit (adj R2 = .21, F = 3.14, p < .01). In other words, those who are more proficient in English, know fewer relatives and/or friends with AD, and know less about AD risk factors are more likely to have stigma reflecting pity. For antipathy domain, social engagement (β= –.26, p < .05) and AD risk factor knowledge (β= –.26, p < .05) were significantly associated (adj R2 = .11, F = 2.03, p < .05). That is, those who are less socially engaged and know less about AD risk factors are more likely to have stigma reflecting antipathy. For social distance domain, age (β= –.31, p < .05), English proficiency (β = .27, p < .05), and antipathy (β = .35, p < .01) were significantly associated (adj R2 = .22, F = 2.96, p < .01). That is, those who are younger and more proficient in English, and have stronger stigmatic belief of antipathy are more likely to have stigma reflecting social distance.
Hierarchical regression of public stigma associated with Alzheimer’s disease.
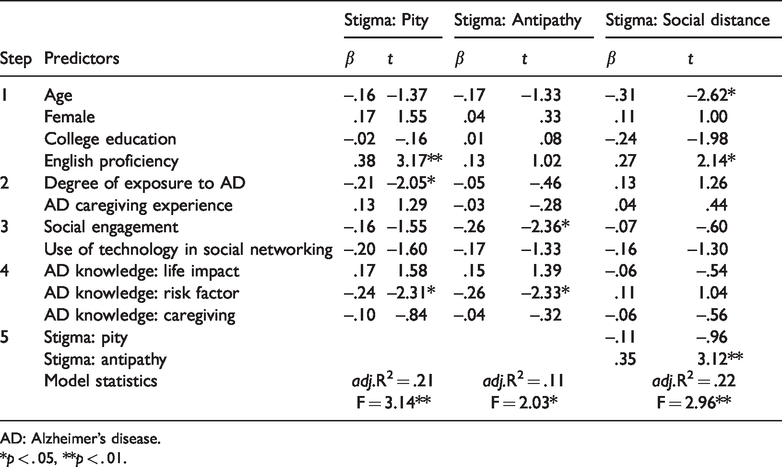
AD: Alzheimer’s disease.
*p < . 05, **p < . 01.
Discussion
The current study aimed to examine the nature and magnitude of public stigma associated with AD in KAs and its correlates. Our study revealed the multidimensional nature of public stigma associated with AD in KAs. The domains of pity and antipathy correspond to emotional attributions in attribution theory. In our KA sample, positive emotions of pity were more prevalent than negative emotions of antipathy. At least half of the participants agreed on all six items related to positive emotions whereas the items indicating negative emotions are endorsed by about a quarter at most. This finding is consistent with prior research that AD elicits more positive than negative emotions (Blay & Peluso, 2010; Stites et al., 2018; Werner & Davidson, 2004). More positive stigmatic beliefs can be due to less blaming the person and family affected by AD for causing the disease unlike serious mental illnesses where the affected individuals and families are often perceived as responsible for the conditions (Corrigan & Kosyluk, 2014; Larson & Corrigan, 2008). An Asian cultural tendency to view dementia as a normal aging process (Lee et al., 2010) can also explain more positive stigmatic beliefs in KAs: The view can reduce expectations for older adults and create a buffer, which results in a “soft stigma” compared to severe mental illnesses (Liu et al., 2008).
Another explanation of prevalent positive stigmatic beliefs in KAs is the labeling effect. As we specifically used the labeling of Alzheimer’s disease in the survey questions, it is possible that participants responded assuming someone in the questions was known to have AD. According to Wadley and Haley (2001), helping intentions are more favorable when the AD diagnosis is present rather than no diagnosis, which is contrary to the labeling theory that explains labeling of mental illness leads to negative consequences (Link et al., 1989). Given this positive impact of labeling in AD context in KAs, encouraging early diagnosis can be beneficial, not only for the purpose of care and treatment but also for altering appraisal of potential AD symptoms of disruptive and problematic behaviors into positive stigmatic beliefs such as compassion and sympathy. Additionally, studies show that under the influence of Asian cultural norm of face-saving, Asian American dementia caregivers avoid public disclosure due to the fear of stigmatization and, as a result, delay seeking diagnosis and services (Guo et al., 2000; Hinton et al., 2000). Given the evidence of positive stigmatic beliefs in KAs, it is important to raise awareness among KAs that AD does not always evoke negative stigmatic beliefs of shame, embarrassment, and disgrace, and this can motivate timely help-seeking and reduce unnecessary fear and concern about AD for the purpose of face-saving. Corrigan and Kosyluk (2014) suggest identifying and working on the positive sides of stigma for stigma change because it can yield positive attitudes and our findings can corroborate their approach.
The social distance domain corresponds to behavioral attribution in attribution theory, which leads to stigmatic behavioral reaction, mainly discrimination. In our study, beliefs about social distance in the AD context are more prevalent than negative emotions but less common than positive emotions. It is plausible that cultural framing of AD in our society influences discriminating behaviors. In mental health research, it is well documented that public stigma is influenced by prejudicial social norms displayed in media and public outlets, hence public stigma is a socially constructed identification (Jones & Corrigan, 2014). AD portrayed in the media and other outlets tends to show advanced or the most severe stages (Devlin et al., 2007; Garand et al., 2009; Herrmann et al., 2018; Iliffe et al., 2005). This narrow disease model of losing identity and social dimensions can generate perceptions of dehumanization (Iliffe et al., 2005). People may feel uncomfortable when communicating and interacting with individuals affected by AD, and may, therefore, avoid them or maintain distance from them. This is, however, different from discriminating behaviors toward other serious mental illness, which stem from fear and danger (Corrigan & Kosyluk, 2014). A study with Chinese Americans (Woo & Mehta, 2017) supports this interpretation that they expressed stronger stigmatizing view related to communication and interaction (e.g., difficulty in communication, not understanding other people’s worry, and being impulsive and unpredictable) than danger of individuals with dementia. This socially constructed narrow disease model can act as a barrier to developing an accurate understanding about the disease (Iliffe et al., 2005). There needs to be a cultural shift of reframing AD from a depiction as a living dead to a realistic portrayal of slowly evolving conditions over an extended period of time (Johnson et al., 2015; Riley et al., 2014). This effort of reframing can not only ensure dignity of the affected individuals (Jones & Corrigan, 2014) but also help us reduce a perception of inconvenience, hence, decrease stigmatic behavioral discrimination.
In regard to correlates of public stigma of AD, our findings point to several factors we can consider when trying to foster and/or reduce certain stigmatic beliefs and behaviors in KAs. For the pity domain, those who are more proficient in English, know fewer relative and/or friends with AD, and have less knowledge about AD risk factors are more likely to have positive stigmatic beliefs reflecting pity. It is possible that those who are more proficient in English can be more familiar with the narrow disease model prevalent in mass and social media outlets. Therefore, they regard the disease in a form of the most severe conditions and feel more emotions such as compassion, sympathy, concern, and sorrow. Corrigan and Kosyluk (2014) suggest increasing exposure and interpersonal contact with the stigmatized group for stigma changes. Our finding supports the suggestion in that KAs with more exposure to AD are likely to have less positive stigmatic beliefs. KAs with more exposure to AD can have more realistic expectations and beliefs about AD; therefore, they can have less emotional reactions such as pity, concern, sadness, sympathy, and sorrow. Although these emotional reactions reflecting pity are relatively positive compared to emotional and behavioral reactions in the other two domains, they may not always be welcomed by the individuals and families affected by AD.
It is interesting that having less knowledge about AD risk factor is significantly associated with more positive stigmatic beliefs as well as more negative ones (antipathy domain). Although a prior study with KAs reported that less AD knowledge was related with increased feelings of shame (Jang et al., 2010), the role of knowledge in relation to the positive stigmatic beliefs is unclear. Increasing AD knowledge has been emphasized to promote early diagnosis and interventions (e.g., Lee et al., 2010). Given our finding of a dual role of AD risk factor knowledge in stigmatic beliefs, educational attempts to increase AD knowledge among KAs should be mindful that, while increasing AD knowledge can reduce negative stigmatic beliefs, it may also reduce some positive emotions such as concern and sympathy for individuals affected by AD.
Another correlate to the antipathy domain is social engagement, and our finding shows that those who are less socially engaged with people and organizations are more likely to have negative stigmatic beliefs toward individuals affected by AD. It is possible that more social isolation leads to less opportunity to share and receive information including disease information in social settings. A targeted approach to socially inactive individuals can be considered to reduce their negative stigmatic beliefs.
For the social distance domain, those who are younger and more proficient in English and have more negative stigmatic beliefs are more likely to show behavioral discrimination. Our finding suggests a need of addressing discriminative beliefs toward the individuals with AD in younger KAs. In connection with the earlier finding that English proficiency was related to positive stigmatic beliefs (pity domain), the finding about English proficiency in the social distance domain shows its dual role in AD public stigma: Individuals with more English proficiency are likely to have more positive stigmatic beliefs yet have more behavioral discrimination. That is, although they may feel more compassion, concern, and sympathy, they want to avoid affected individuals in communication and interaction. As discussed previously, the role of English proficiency in this context can be due to a more exposure to the narrow disease model of AD. This finding suggests that an effort to reframe the narrow disease model can also help reduce discriminating behaviors toward persons affected by AD among KAs.
We examined a potential influence of emotional attributions (positive (pity) and negative (antipathy) emotions) on behavioral attributions (discriminating behaviors (social distance)), which is described as a stigma process in attribution theory. Only negative emotional attributions were found to be associated with behavioral attributions, that is, stronger negative stigmatic beliefs are likely to yield more discriminating behaviors. A similar finding is reported in Werner (2005) where rejection feelings increase discrimination. Our study identified two demographic groups that are more likely to have negative stigmatic beliefs, KAs with lower levels of social engagement and knowledge about AD risk factors, and they can be targeted in efforts to address behavioral discrimination toward individuals with AD in KAs.
Some limitations should be considered when understanding our findings. The use of a cross-sectional survey limits our study’s ability to establish causal relationships among the study variables. Convenience sampling restricts generalizability of the findings outside the study context. Particularly, it should be noted that all of our participants are foreign-born where 59% of KA population is (Pew Research Center, 2017). Social desirability bias can be considered, which is often found in the collectivist culture, such as Asian Americans (Lalwani et al., 2006).
For future research, cognitive attributions and positive behavioral attributions of AD public stigma in KAs can be considered. Cognitive attributions are the first step in the stigma process described in attribution theory and they were not included in our investigation. There are studies reporting strong stigma attached to cognitive attributions of AD such as deteriorating physical and cognitive functioning and aesthetic appearance (e.g., Werner, 2014; Werner et al., 2010). Our study only covered negative behavioral attributions (discrimination). There is an indication that behavioral attributions can be positive and prosocial reaction attached to AD is reported (Blay & Peluso, 2010). Including cognitive attributions and positive behavioral attributions in the future research can provide a more comprehensive picture in understanding AD public stigma process. The role of domain-specific AD knowledge in public stigma can be another area for future research. We found that only risk factor domain played a significant role in positive and negative stigmatic beliefs. While it is unclear why only this particular domain affects the stigmatic beliefs, our study demonstrated that it is worth treating AD knowledge as a multidimensional construct rather than a unidimensional one when examining its impact on public stigma of AD. Our findings clearly demonstrate a need to reframe the existing narrow disease model of AD to reduce negative stigmatic beliefs and behaviors. How to reframe the narrow disease model (e.g., examining factors associated with having the narrow disease model) can be a focus of future research. The current study examined stigma associated only with AD, and future research can look into stigma associated with other types of dementias so that we can develop an understanding about the potential variations in stigmatic beliefs and reactions associated with AD and related dementias.
In conclusion, given the limited information about AD-related stigma among ethnic minority populations, our study revealed multifaceted nature of public stigma associated with AD and its correlates in KAs. While making efforts to reduce negative stigmatic beliefs, it is important to raise awareness of positive stigmatic beliefs existing in KAs. Knowing that AD is not always perceived as negative and generates positive emotions can encourage early diagnosis when potential early symptoms arise. Positive stigmatic beliefs can help KA families reduce their burden and stress in a way that they do not unnecessarily worry about the concealment of the condition for the purpose of face saving and can focus more on care and support. Multivariate findings broaden our understanding of the context of each stigma domain and show that different sets of factors affect each stigma domain. Particularly, a dual role of English proficiency and AD risk factor knowledge in different stigma domains suggest certain group of people and subject areas we need to pay particular attention to when trying to decrease negative stigmatic beliefs and discriminating behaviors while promoting positive stigmatic beliefs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Agency for Healthcare Research and Quality (R03 HS22947).