
Abstract
Background
In Australia, informal caregivers (family, friends and neighbours) play a crucial role in supporting people with dementia to remain at home. Within the community aged care policy, informal caregivers are acknowledged as assisting with managing care. However, they usually receive very limited dementia care education and training to support them in their role. The World Health Organization (WHO) developed iSupport for Dementia, a comprehensive online dementia education and skill training programme, to address the gap in supporting informal caregivers.
Aim
The aim of the study was to identify stakeholders’ perspectives regarding adapting the WHO iSupport for use by informal caregivers of people with dementia in Australia.
Methods
An interpretive description study design was used. Data were collected in focus groups with informal caregivers and care staff of dementia and aged care service providers conducted in May–July 2018. A thematic analysis was utilised to analyse data and identify findings.
Results
In total, 16 informal caregivers and 20 care staff participated in the study. Five themes were identified. First, informal caregivers perceived iSupport as an opportunity to provide an online one-stop shop to meet their education needs and their needs to manage care services. Second, both informal caregivers and care staff believed that an integrated caregiver network moderated by a health professional was much needed to enable informal caregivers to share learning experiences and enhance social support. Third, both informal caregivers and care staff strongly suggested that dementia and aged care service providers had a role to play in promoting the iSupport. Fourth, informal caregivers were concerned about the time commitment to participate in the iSupport programme. Finally, informal caregivers expected the iSupport to be user-friendly.
Conclusion
Stakeholders perceived the adaptation of the WHO iSupport in Australia would strengthen informal caregiver education and optimise support for informal caregivers.
Keywords
Introduction
In Australia, informal caregivers (family, friends and neighbours) recommend that the government develops and implements a programme of integrated support which meets their needs, improves workforce participation, helps to balance work, life and caring responsibilities, and reduces adverse physical and mental health outcomes (Alzheimer’s Australia, 2016). However, whilst almost 78% of adults in Australia use the internet to find health-related information (Australian Institute of Health and Welfare, 2018), there is a lack of trustworthy and free online dementia education and skills training programmes for informal caregivers that offer flexibility within a self-directed learning environment. Moreover, dementia and aged care are subsidised by the Australian Government under the ‘Aged Care Act 1997’ (Australian Government ComLaw, 1997) and regulated via a consumer-directed care and person-centred care policy (Australian Government & Aged Care Quality and Safety Commission, 2019). Informal caregivers are required to navigate care services via the Australian government ‘My Aged Care’ website, including self-identifying service providers and monitoring service provision (Australian Government, 2020b). Informal caregivers felt unprepared and overwhelmed in this role due to the lack of knowledge about dementia care and care services (Gill et al., 2018).
The World Health Organization (WHO) has developed the iSupport for Dementia, an evidence-based online dementia education and skill training programme for informal caregivers (Pot et al., 2019). Adapting iSupport for use in an Australian context is an opportunity to address the gap in dementia education for informal caregivers and assist them to better utilise care services. To facilitate the adaptation of the iSupport programme, the WHO has built an online generic version and is accessible by users via the website: https://www.isupportfordementia.org/en (WHO, 2019a). A booklet of the iSupport for Dementia has also been published for caregivers who are unable to access or do not use the internet (WHO, 2019b). So far, iSupport for Dementia has been adapted in India, and other countries such as Australia, Brazil, China, Japan, The Nethelands Portugal, the United Kingdom and the United States are in a progress to adapt the programme (WHO, 2020). It is anticipated that the iSupport for Dementia has the potential to improve the universal access to dementia education and training for caregivers of 50 million people living with dementia (WHO, 2019a).
Background
The generic version of the WHO iSupport programme was developed to support the implementation of the WHO Global Action Plan on the Public Health Response to Dementia through an international collaboration (Pot et al., 2019). iSupport includes five learning modules: (1) general information about dementia, (2) information related to being a carer, (3) self-care, (4) providing care for the person with dementia and (5) addressing symptoms of dementia (WHO, 2019a). There are 23 learning units under these modules. The programme covers dementia care from early to end stage. Informal caregivers are encouraged to select learning units that suit their individual situation. The iSupport programme embeds person-centred dementia care, interactive learning activities and case scenarios to enable informal caregivers to learn about dementia care and to develop skills for self-management of their own stress when caring for persons living with dementia at home (Pot et al., 2019). iSupport applies techniques such as cognitive behavioural therapy, psychoeducation, relaxation, assertiveness skills training and problem-solving skills to improve caregivers’ self-efficacy (Pot et al., 2019).
In the generic iSupport programme, informal caregivers are encouraged to seek help from care service providers to reduce caregiver burden. This learning design enables WHO member states to embed country-specific dementia and aged care services into the programme. For example member states can incorporate care services to help informal caregivers to understand when and how to use services, and how to monitor them. This educational process is essential for informal caregivers to reduce their stress when navigating care services in a consumer-directed care model.
Systematic reviews showed that well-designed online education programmes improved confidence, self-efficacy, social support and mental health for informal caregivers (Egan et al., 2018; Oliver et al., 2017). In the ‘iCare Stress Management e-Training Program’, informal caregivers showed decreased stress (Kajiyama et al., 2013). However, the dropout rate in the intervention groups was high (39%) in a 3-month trial. The absence of programme facilitators might have contributed to this situation. In the 6-month ‘Master over Dementia’ online programme, a coach was appointed to engage caregivers in learning, review homework and provide feedback to informal caregivers (Blom et al., 2015). The programme demonstrated improved mental health well-being for informal caregivers evidenced by decreased symptoms of depression and anxiety. The dropout rate in the intervention group was 25%, lower than the ‘iCare Stress Management e-Training Program’.
Online education alone may not have a positive impact on care outcomes if there is a lack of strategy to engage informal caregivers in translating knowledge into everyday care activities (Bott et al, 2019; Whitlatch & Orsulic-Jeras, 2018). Creating an enabling environment for caregivers to share their experience in applying knowledge in care practice is equally important (Andersson et al., 2017; Solli et al., 2018; Whitlatch & Orsulic-Jeras, 2018). Studies on effective online support for informal caregivers identified these core components of an enabling environment for informal caregivers: organisations’ support to deliver education and skills training to informal caregivers, support groups and coaching for informal caregivers, and telehealth to monitor and relieve caregiver burden (Brown et al., 2018; Egan et al., 2018; Hopwood et al., 2018; Oliver et al., 2017). Recent meta-analyses confirmed that online caregiver support groups via forums and video-streaming meetings contributed to improved self-efficacy and social support for informal caregivers (Oliver et al., 2017). Online support groups also enabled informal caregivers to mobilise their dementia knowledge and learn from role models (Hopwood et al., 2018; Oliver et al., 2017; Parra-Vidales et al., 2017). Caregiver support groups need to be conducted for a minimum of 20 weeks to improve self-efficacy (Oliver et al., 2017). A group with a small number of informal caregivers is desirable to enable it to be tailored to the needs of individuals (Hopwood et al., 2018).
Theoretical perspective
Bandura’s self-efficacy theory was applied as a theoretical framework to inform the present study (Bandura, 1993). This theory was originally developed to assess student learning in formal education. According to this theory, a learner will experience a learning journey through cognitive, motivational, affective and knowledge to action processes (Bandura, 1993). Cognitive processes require learners to be familiar with core knowledge and skills in a practice area (Bandura, 1993). Engaging learners to set their own care goals in collaboration with learning facilitators is viewed as an effective strategy to activate the learner’s intrinsic motivation to learn (Bandura, 1993). Learning from role models is another strategy to stimulate the learner’s motivation to learn (Bandura, 1993). Affective processes mean learners will inevitably encounter difficulties and experience emotional stress; therefore, support to deal with difficult situations is essential (Bandura, 1993). Knowledge to action processes requires learners to select a course of action that suits their situation (Bandura, 1993).
The WHO iSupport is an ideal programme for informal caregivers to build dementia knowledge and skills as it is evidence based. Creating an enabling environment, for example through caregiver support groups, will motivate informal caregivers to learn and help overcome difficulties and emotional stress. Moreover, sharing knowledge and experiences in dementia care with peers will facilitate informal caregivers to select a course of action to improve their practices and care outcomes.
Aim of the study
The aim of the study was to identify stakeholders’ perspectives on adapting the WHO iSupport programme for use by informal caregivers of people with dementia in Australia.
Method
An interpretive description study design was applied to address the study aim (Thorne, 2016). This qualitative approach enables researchers to collect data in a naturalistic context. This approach particularly values the perspectives of iSupport stakeholders about the best way to deliver the iSupport programme.
Participants and data collection
The study was conducted in one Australian state in community aged care settings in collaboration with two large dementia and aged care service provider organisations. One organisation was a branch of a national dementia service that supported approximately 34,918 people living with dementia and their caregivers. The other organisation provided community aged care services to 10,000 older people.
Informal caregivers were invited to participate in the study if they were: (1) 18 years of age or older, (2) a primary informal caregiver of a person with dementia and (3) in the caregiver role for at least 1 year. Caregivers were excluded if they were unable to comprehend written and spoken English as they were required to access and read the WHO online English version of the iSupport programme and provide feedback. Care staff were invited to the study if they were employed as caregiver support group coordinators or case managers of dementia care services. Participating organisations distributed participant information packs to potential participants who then contacted the principal researcher if willing to participate.
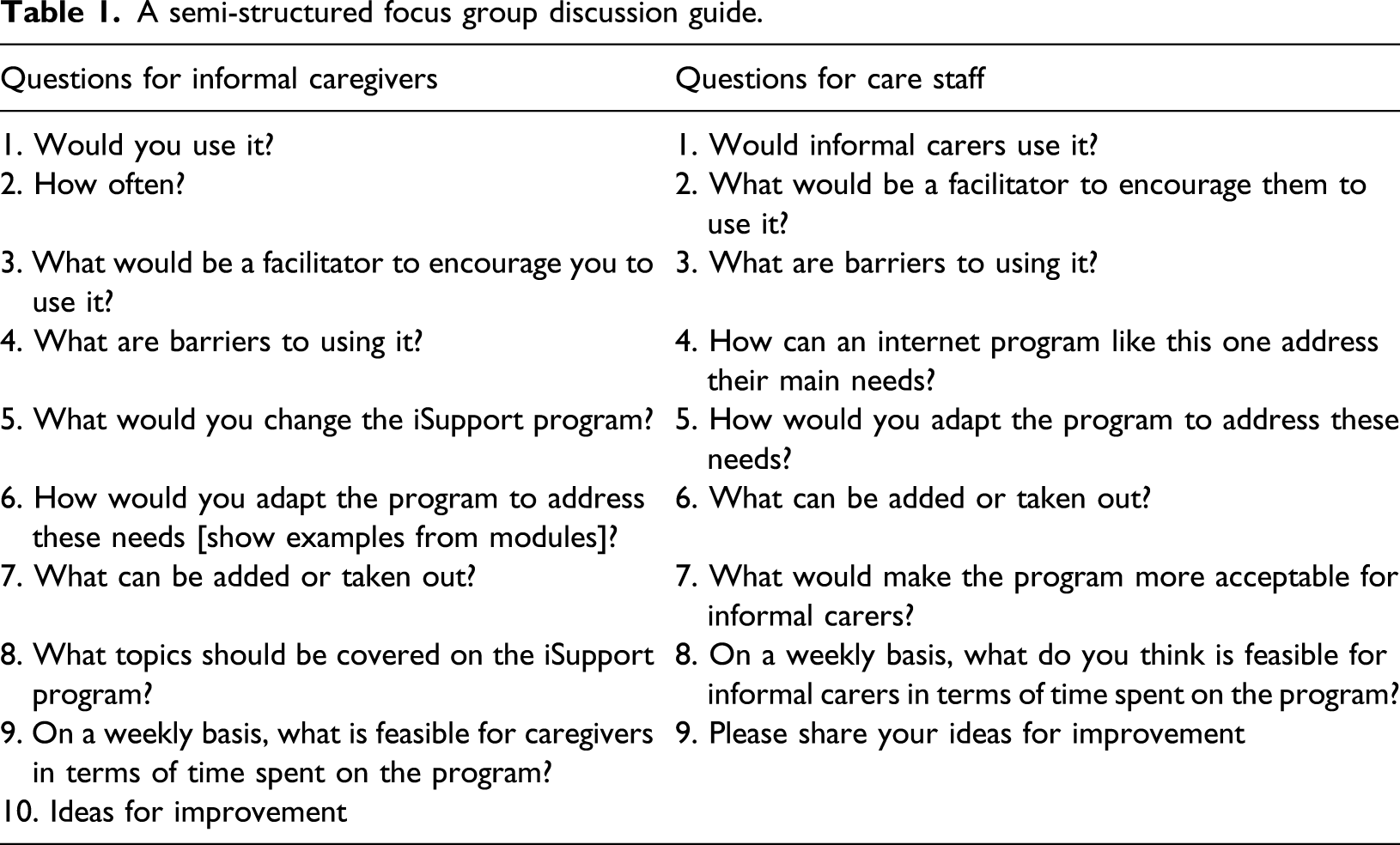
A semi-structured focus group discussion guide.
Data analysis
A 4-step thematic analysis procedure that reflected the interpretive description design was applied to data analysis (Thorne, 2016). First, each transcript was read by two researchers to gain understanding of participants’ views of how to adapt the iSupport to an Australian social context. Second, meaningful words in each transcript were highlighted and coded. Third, these codes were compared across all transcripts and were further reduced as categories based on similarities of meaning. Fourth, regular team meetings were held to elaborate the potential themes from the coding process and to reach a consensus. The final themes addressed the aim of the study.
Ethical considerations
Ethical approval for this project was gained from the Social & Behavioral Research Ethics Committee of Flinders University (Project number: 7900). Informed consent was discussed with participants in face-to-face meetings prior to focus group discussions. Participants were reassured of their rights to either participate or to decline to participate in the study. Participants were also reassured that their identities and any information they shared in the focus group would maintain confidentiality in any reports of the study. Data from audio recordings of focus groups were stored in a secured and password-protected platform, Flinders University OneDrive, according to the university policy.
Study rigour
The study complied with credibility, dependability, confirmability and transferability for qualitative research (Lincoln & Guba, 1985). Credibility was achieved using audio recording of focus groups and transcribing verbatim. At the end of each focus group, the researchers provided participants with a summary of the main points discussed and an opportunity to revise. Two of the researchers (LX and LJ) built a sustainable research collaboration with the participating organisations and established rapport with study participants through their long-term engagement with them. Dependability was addressed by adhering to the study design and methods, and using excerpts from transcripts to support findings. Two researchers (LX and AMP) were the main contributors to the WHO iSupport for Dementia Programme and played a key role in ensuring the Australian adaptation met the international WHO iSupport adaptation guidelines. Regular online meetings and email communication with the WHO iSupport team were undertaken to discuss adaptation issues and to gain approval for recommended changes to the iSupport programme. Confirmability was emphasised by taking notes on non-verbal communications during each focus group discussion and using these notes to support the data analysis, and by team member cross-checking of data analysis. Transferability of the findings was addressed by discussing the social context of the study and applications of findings.
Findings
In total, 16 informal caregivers and 20 care staff participated in the study. The mean age of informal caregivers was 74.5 years, 65% were female, and 88% were spouses of the person with dementia. The average time in their role as informal caregivers was 5 years. The mean age of the persons with dementia who the informal caregivers cared for was 77.9 years. The mean age of care staff was 47 years, and 88% were female. Staff on average had worked in dementia care services for 8 years. Staff participants included nurses, social workers and care coordinators with 75% holding a diploma or bachelor’s degree.
Five themes were identified from the data analysis. Informal caregivers perceived iSupport as an opportunity to provide an online one-stop shop to meet their education needs and their needs to manage care services. Both informal caregivers and care staff believed that an integrated caregiver network moderated by a health professional was much needed to enable informal caregivers to share learning experiences and enhance social support. Both informal caregivers and care staff strongly suggested that dementia and aged care service providers had a role to play in promoting the iSupport. Informal caregivers were concerned about their time commitment to participate in the iSupport programme. Informal caregivers expected the iSupport to be user-friendly. These themes are discussed in the following.
Opportunity for an online one-stop shop for informal caregivers
Informal caregivers had the opportunity to access the WHO iSupport portal and felt the need for such a programme. They discussed this in informal caregiver focus group 1: Informal caregiver: As a [family] carer you feel like you are swimming in a dark room and question yourself – this is when you need information like this [iSupport]. Informal caregiver: Would look at it as soon as worried about something different or unexpected. Informal caregiver: It [iSupport] is a bit of an index. If I wanted to reduce my stress, I could go just straight to it.
Most care recipients who were cared for by informal caregivers in the study were in the moderate to late stage of dementia. Informal caregivers faced challenges when dealing with changed behaviours and they suggested: Dealing with frustration and things relevant to later stages are more important and would like to learn behaviours – anything to help later stages like refusing to do things (informal caregiver focus group 1).
Informal caregivers would like to see the Australian iSupport connected with existing dementia and aged care services as they discussed in informal caregiver focus group 1: Informal caregiver: So the way it works is it will give you the number or the website address to go to directly. It’s one way of you actually connected to the services that are available. Informal caregiver: I would like to know where to go to get help: need section about access to support, respite care and scenarios, information on medical specialists in dementia, flowchart of contacts for specialists, contact with people that can help.
Managing care services was a significant part of informal caregivers’ role and they sought online communication with service providers about this: So you’ve got a box in there [on the website] you ask for help, and you type a question there, it actually goes as an email back to someone who will come back to you and respond (informal caregiver focus group 1).
Informal caregivers’ information needs also relate to their role in coordinating care services for the care recipients. Informal caregivers felt they needed to know these types of information about services as they discussed in informal caregiver focus group 1: Informal caregiver: Where are the support groups? And things like support groups listed in there, correct time and place, build in links. Informal caregiver: Issues about putting someone in care as it is very difficult. Informal caregiver: Need something on coping after [the person] moved to residential care or passed away.
Care staff reflected on their clients from diverse backgrounds who spoke a language other than English at home and had different care needs associated with their ethnicity and culture. Care staff strongly recommended the need to have ‘iSupport for the Aboriginal and Torres Strait Islander peoples and for CALD [culturally and linguistically diverse] communities’ (Staff focus group 1).
Integrated online caregiver network
All informal caregivers in the study had some involvement in face-to-face caregiver support group activities. They reflected on the benefits gained from these activities and strongly recommended that an online caregiver support platform via iSupport would make it easy for them to share their learning experiences, as they discussed: Everyone must have same or similar problems and what has worked for them. I can see where Dick’s offering his discovery that works for him and he thinks actually other people be able to learn from that and he’d like to tell somebody online straightaway (informal caregiver focus group 1).
Care staff echoed the same recommendations: You know, someone might not have thought about doing that, so that could be a link for them [informal caregivers] to read the discussions within their groups and help each other (Staff focus group 1).
As informal caregivers experience a range of costs and in some cases a loss of income due to their caring role, they were seeking access to low-cost support subsidised by the government. Online caregiver support was viewed as a low-cost option for them: We like to see the iSupport to pull them [online caregiver forum and information on dementia] together, so we’ve got everything we need and we’ve got covered. We mentioned we generally try and cover all the government services first because they’re either free or fee limited. So, we don’t go into all the private services because we can’t afford the services (informal caregiver focus group 2).
Informal caregivers strongly recommended that an online caregiver network attached to iSupport would also improve social support for them as they discussed in informal caregiver focus group 2: I hear people sort of saying that they’re isolated at times or feel isolated from help. Is there any consideration to have an online blog so they can type questions to link to other carers?
Informal caregivers would prefer to stay in the same group they formed in face-to-face meetings through their dementia care service providers as they discussed in informal caregiver focus group 1: Informal caregiver: The website needs to link up to the group, and I can just share comments and people can answer you, I did this, and I did that. Informal caregiver: I prefer video-streaming meetings rather than online chat.
These discussions supported the affective processes of learning in self-efficacy development. Informal caregivers developed social bonds and relationships with group members and felt safe to disclose their attitudes and emotional reactions to the challenges they encountered.
Role of dementia care staff in promoting the iSupport to informal caregivers
Care staff were concerned about the various levels of computer literacy among informal caregivers who were predominantly older females and had not previously been exposed to online education and training. Care staff felt informal caregivers might encounter difficulties in logging in and utilising iSupport. Care staff suggested strategies that would support informal caregivers to feel comfortable to utilise iSupport: If we have a coordinator to get [informal] carers together and introduce them to it [iSupport] and that might encourage them to then go and have a look themselves, or, as a group, we sit around a laptop or something and say okay, this is what it looks like, and just show them a little bit, and that will actually break down some of those barriers (Staff focus group 1).
Care staff also identified the need to have iSupport to complement the face-to-face education they usually provided to informal caregivers via home visits, as they discussed in staff focus group 2: Care staff: If the person with dementia is in the room when we’re doing the home visit, sometimes it’s a little bit difficult to talk around changes and responses to the changes. It makes that person with dementia feel uncomfortable and think that they don’t have any of these changes and responses we talk about. Care staff: So if they could have this [iSupport] and we say, ‘Look on here see what’s happening then give, if you want to give us a call we can talk, or we can talk about it a bit more’. Care staff: So give them just something they can do in private without us having to talk.
Care staff perceived stimulating informal caregivers’ motivation to learn more about dementia care was a way to engage them in iSupport. Care staff reflected on their experience in working with informal caregivers in face-to-face forums to discuss problems encountered in home care settings. They believed that the forums were the right place and right time to motivate informal caregivers to learn the iSupport and to discuss how to translate knowledge into everyday care, as they discussed in staff focus group 2: They [informal caregivers] usually go to our face-to-face forums regularly and you could actually encourage them to do it [iSupport] and trial some recommended actions.
Care staff particularly embraced iSupport implementation in rural and remote areas where resources and support mechanisms for informal caregivers were limited. As they said: It’s also good for rural areas because we’ve got staff at XX [a rural place] and XX [a rural place] and so forth and they’re finding it difficult because of distances to clients and their isolation’ (Staff focus group 2).
Care staff also suggested the involvement of local councils in promoting the iSupport: It would be other service providers and local council. It’s everyone working together, having it on a training board where they can see where local courses are coming up or whatever I think that would probably be very useful as well (Staff focus group 2).
Discussions on iSupport implementation strategies revealed the need to have a systemic approach to promote the programme to informal caregivers in country regions. In order to do so, a careful plan and consultations with stakeholders during the iSupport development phase are much needed.
Time commitment to participate in the iSupport programme
Informal caregivers fully contributed to their caregivers’ role and felt overwhelmed. Therefore, finding a quiet time by themselves to study iSupport in the house would be a challenge, as they discussed in informal caregiver focus group 1: Informal caregiver: Sometimes if you’re very, very tired and you have to read and you’ve got a computer, it’s just too hard. Informal caregiver: Time is a barrier. Haven’t got time to sit and fiddle around. Need to get suggestions and help quickly. Informal caregiver: In later stages, you don’t seem to have time to do anything but provide care.
Informal caregivers perceived physical and mental stress associated with their caregiver duties was a factor affecting their energy to learn iSupport. Keeping iSupport simple but helpful for informal caregivers in problem-solving would help to overcome time challenges. Care staff were also concerned about the time informal caregivers would commit to learning iSupport, as they discussed in staff focus group 2: Care staff: My issue is it’s around their time to be able to access something like this [iSupport] with a person with dementia who may want their attention the whole time. Care staff: I think in early stages probably more time but as it gets, and I don’t know if they’d do it. Care staff: It might work better for a secondary carer [informal caregiver], especially for the older person [informal caregiver]. The secondary carer can do this and maybe help around strategies and things to put into place for their mum or dad.
Engaging the family as a unit in iSupport may be particularly suitable for older female informal caregivers who also often have low health literacy and computer literacy. This strategy may also enhance support from family members in dementia care, especially in the late stage of dementia.
Expectations of user-friendly iSupport
Reflecting on their busy schedule and duties, informal caregivers expected the iSupport to help them to identify solutions for problems they encountered in a much easier way as they discussed in informal caregiver focus group 2: Whereas if you had a short video clip that you go, oh I just need the half an hour and you click on the video clip that may be helpful.
Providing short videos with voice-over explanations may be quicker for informal caregivers than reading information. Informal caregivers also expected the iSupport search function would assist to identify specific learning units easily, as they discussed in informal caregiver focus group 2: Informal caregiver: Make links to solutions to specific problem. Informal caregiver: Need to be able to get to specific behaviours without having to go through whole programme. Informal caregiver: If you’ve got a problem you could just open the programme and sit down and type in your question and perhaps something will come up that is relative to your question.
Building a website solution that incorporated user-friendly keywords for searching, grouping learning modules and units in an order that suited informal caregivers’ learning needs, and linking related learning units may address these expectations. Informal caregivers also expected information technology used in the iSupport to have these features, as they discussed in informal caregiver focus group 2: Informal caregiver: Programmes can be too complex – keep structure simple. Informal caregiver: Information is all about but difficult to find – need to be able to find easily. Informal caregiver: Leave computer and come back and click up where you left off. Informal caregiver: Could programme work on voice recognition – something like Google Home to get solutions – get an answer in a hurry?
Informal caregivers would like the iSupport to enable them to easily seek help from care service providers, as they discussed in informal caregiver focus group 1: You used a system like these links [hyperlinks built in the iSupport] where you send an email to someone. You ask for help you. That might be a way of doing it rather than ringing someone up.
Discussion
Informal caregivers in our study wanted to have access to not only an online dementia education and training programme but also an enabling environment via an integrated caregiver network to learn, share and translate dementia care knowledge into everyday care and to socialise with others. Care staff discussed their role in promoting the iSupport to informal caregivers and implications for practice development. Challenges regarding availability of time to use the iSupport were discussed by informal caregivers, and their suggestions on ways to overcome need to be considered. For example the programme design needs to enable quick searching of learning units based on informal caregivers’ learning needs. Informal caregivers’ expectations of a user-friendly iSupport platform have implications for the development of a web-based solution using advanced information technology. These findings add new knowledge to the WHO iSupport international community about how best to support caregivers via an Australian perspective.
Informal caregivers in our study were eager to learn from iSupport. The findings supported the dementia caregiver literature showing that informal caregivers usually encounter enormous challenges in their day-to-day care activities starting from the beginning of memory loss to the end of life care for people with dementia. These challenges can trigger informal caregivers’ motivation to learn about dementia care throughout their whole caregiving journey (Sousa et al., 2016; Whitlatch & Orsulic-Jeras, 2018). Meeting individualised learning needs for informal caregivers may be difficult in a face-to-face education programme considering their diverse learning needs influenced by many personal and environment factors. However, this challenge may be addressed in a well-designed online programme like iSupport if flexible self-directed learning is encouraged and accommodated. Based on adult education principles, strategies to achieve effective self-directed learning include, but are not limited to, self-learning assessment prior to and after learning activities, learning planning, interactions with others to share and gain feedback, and reflection on own experiences to enhance learning (Knowles, 1984).
The need to link existing care services and to better communicate with service providers that informal caregivers identified in our study revealed their unmet needs in seeking help. The finding was in line with other studies (Black et al., 2019; Theleritis et al., 2019; Xiao et al., 2016). In Australia, a consumer-directed care model is used to access and implement government-subsidised community aged care services. In this mode, informal caregivers of people with dementia are required to select and purchase care services and to monitor their quality (Dementia Australia, 2019; Kaambwa et al., 2015). Meeting informal caregivers’ information and communication needs is a way to strengthen consumer-directed care.
Informal caregivers in our study perceived the importance of interacting with peers when participating in the iSupport programme. This finding supported the affective processes of learning in self-efficacy development (Bandura, 1993). Three caregiver support network models were identified in the literature: (1) private blogs led by informal caregivers (Anderson et al., 2017), (2) a generic online support network for informal caregivers that is independent from care service providers (Andersson et al., 2017) and (3) a health professional–led integrated network for informal caregivers that incorporates online support, face-to-face meetings, phone support and information provision (Solli et al., 2018). The private blogs led by informal caregivers showed advantages of self-management to achieve social support. However, this model was questioned for potentially detrimental care outcomes if informal caregivers followed actions from others that were not suitable for their situations (Anderson et al., 2017). The generic online support network model was welcomed by working caregivers to overcome time constraints to participating in social support. Advisors were available in this model for informal caregivers to make general enquiries. However, this model may not provide substantial support for informal caregivers to negotiate with care service providers. In Australia, this model is applied to the ‘Carer Gateway’ that accommodates online support for caregivers from all care areas nationwide and is managed by the Department of Social Services (Australian Government, 2020a). The health professional–led integrated network model overcomes disadvantages in the private blogs model and the generic online support model. In our study, informal caregivers preferred the health professional–led integrated network model for informal caregivers. The finding supported the study by Kovaleva et al. (2019) that face-to-face group interactions, additional to online contacts, were much needed to enable informal caregivers to build rapport and social bonds with peers in order to achieve positive group interactions.
The role of care service providers in promoting iSupport and engaging informal caregivers in the programme as identified in our study supported the study by Blom et al. (2015) where a coach was employed to engage informal caregivers in the online programme, review their homework and provide feedback. Considering the high dropout rate reported in online education programmes, appointing an iSupport facilitator is a strategy to engage and retain informal caregivers in the programme. Moreover, behavioural and psychological symptoms of dementia (BPSD) were the main source of stress for informal caregivers and triggered their learning needs (Nakanishi et al., 2018; Whitlatch & Orsulic-Jeras, 2018). However, effectively responding to BPSD requires informal caregivers to carefully investigate the potential causes and triggers of BPSD, and trial individualised interventions to mitigate the impact. An iSupport facilitator would be in an ideal position to provide timely support for informal caregivers to respond to BPSD and reduce their stress.
Strengths and limitations of the study
The strength of the study is demonstrated by the researchers following the WHO iSupport Adaptation and Implementation Guide. The findings add new knowledge to the WHO iSupport database to facilitate knowledge exchange in supporting informal caregivers. However, due to the use of a qualitative study design, findings cannot be generalised but can be transferred to similar social and cultural contexts. In addition, in this study, informal caregivers cared for people in the moderate and late stages of dementia and were from the mainstream cultural backgrounds in Australia. Therefore, findings cannot be generalised to informal caregivers who care for people in the early stage of dementia or to Aboriginal and Torres Strait Islander peoples, ethnic minority groups or those who are identify as LGBTIQ+ (Lesbian, Gay, Bisexual, Transgender, and Intersex and Queer).
Implications for policy, resource and practice development
Findings have implications for policy development to strengthen support for informal caregivers. It is imperative to invest in the iSupport to complement face-to-face education and training for informal caregivers and to support aged care service providers and other stakeholders to promote the iSupport. The iSupport can be a self-directed education and training programme for informal caregivers when they need it from time to time throughout their caregiving journey. The iSupport can also be advanced to meet the expectations of informal caregivers to interact with peers through an integrated caregiver support network managed by dementia and aged care service providers. In this case, iSupport would be an adjunct to care services for clients. Informal caregivers’ expectations of user-friendly iSupport using information technology have implications to co-designing with stakeholders a web-based solution to meet their needs.
Conclusion
While informal caregivers are the cornerstone of care and play a crucial role in enabling people with dementia to remain at home for as long as possible, they receive minimal education and training in dementia care compared to professional care workers. This study identified the need to adapt the WHO iSupport programme to an Australian social context to complement existing dementia and aged care services. Adaptations should focus especially on assisting informal caregivers to provide effective person-centred care for people with dementia and to understand how to successfully utilise formal care services to reduce caregiver burden. Informal caregivers in the study also expected an integrated support network to accompany the iSupport that included online, face-to-face and phone contacts with peers and dementia and aged care service providers to share and enhance their learning. They also preferred that the network was managed by their care service providers. Informal caregivers in the study expected a user-friendly iSupport using information technology that enabled them to identify relevant learning units and learning materials in an easy way. The development and implementation of iSupport have the potential to contribute to universal access to dementia care education for informal caregivers and thereby improve the health and well-being for people with dementia. The knowledge exchange in adapting the WHO iSupport across countries can have a positive impact on international collaboration in supporting informal caregivers in dementia care.
Footnotes
Acknowledgements
We would like to acknowledge our appreciation to the participants of this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by a Flinders University Seeding Grant.