
Abstract
Background
People with dementia usually prefer to live in the community. Research is needed to identify the ‘tipping point’ for residential care entry and to highlight how people with dementia can be supported to remain at home as long as possible. Few previous studies have examined caregivers’ perceptions and explanations for the reasons people with dementia need to enter residential care in Australia.
Aim
To explore the factors contributing to people with dementia entering residential care in Perth, Western Australia, from the perspectives of informal carers and care staff.
Method
This phenomenological study used purposive sampling to recruit informal and formal caregivers of people with dementia. Semi-structured in-depth interviews were conducted with 13 family carers and 11 home care staff. Data were thematically analysed to identify individual, carer and contextual factors that impact on residential care entry.
Findings
The majority of participants identified a combination of factors as the ‘tipping point’ to residential care entry; a few also identified the cause as a sudden event or specific issue. Factors identified included deterioration related to worsening cognition, changed behaviours and a decline in the performance of activities of daily living; co-occurring health conditions; safety concerns; carer no longer able to meet care needs; impact of providing support becoming too much for the informal carer; lack of family or social support and needing assistance from services that were unavailable or inaccessible. Factors assisting people with dementia to remain living at home longer were family and social support, formal services and dog ownership.
Conclusion
This study identified individual, carer and contextual factors that contribute to people with dementia entering residential care in Australia. The ‘tipping point’ was recognised as when the needs of a person with dementia outweigh the capacity of their informal and formal carers, services and supports to care for them.
Introduction
It is estimated that 459,000 people in Australia are living with some form of dementia (Dementia Australia, 2020); this is projected to rise to 1,100,890 in 2056 due to an ageing and increasing population (Brown et al., 2017). Approximately 30% of people with dementia in Australia live in residential care (Australian Institute of Health and Welfare, 2012), and 52% of all people in residential care are estimated to have dementia (Brown et al., 2017). Residential care for a person with dementia in Australia has been costed at US$88,000 per year (Gnanamanickam et al., 2018). Admission to residential care has been associated with increases in behavioural symptoms for people with dementia and their carers experiencing guilt, depression and feeling like a failure (Sury et al., 2013). European (Afram et al., 2014) and international (Toot et al., 2017) research has identified that people with dementia enter residential care due to a range of factors, related to the person, carer(s), health services and surroundings. These factors often vary between countries, potentially due to differences in healthcare systems and cultural contexts (Verbeek et al., 2015). There is a need for more country-specific research regarding factors related to residential care entry for people with dementia (Risco et al., 2018). As it has been proposed that people with dementia usually prefer living and being cared for at home (Gomes et al., 2013), research is needed to investigate the ‘tipping point’ to residential care entry in Australia.
Background
Previous Australian (Brodaty et al., 2014), European (Risco et al., 2015) and international (Toot et al., 2017) research has examined individual factors that result in people with dementia requiring residential care. These studies identified declining cognitive abilities (Brodaty et al., 2014; Toot et al., 2017), behavioural and psychological symptoms of dementia (BPSD; Brodaty et al., 2014; Toot et al., 2017) and declining functional abilities, including incontinence, toileting and dressing issues, as factors (Brodaty et al., 2014; Risco et al., 2015). However, Toot et al. (2017) were not able to conclude whether entry into residential care was associated with declining functional abilities and physical health. Australian research has identified that key BPSD factors, such as hallucinations and appetite issues, were linked with entry to residential care (Brodaty et al., 2014). In comparison, international research identified the main factors as aggression, hallucinations, anxiety, depression and psychosis (Toot et al., 2017).
Carer factors have also been investigated in relation to their impact on entry to residential care for people with dementia. Caregiver burden (Afram et al., 2014; Toot et al., 2017), dependency (Afram et al., 2014) and no longer being able to meet care needs (Afram et al., 2014) have been linked to entry into residential care for people with dementia. While Brodaty et al. (2014) did not find a statistically significant association with caregiver burden or demographic variables, living alone was viewed as likely to be associated with moving to residential care.
The Australian Government provides services which assist people with dementia to remain living at home, including the Commonwealth Home Support Program (CHSP) and home care packages (Duckett, 2018). The CHSP provides people aged over 65 years and their carers with services which may include household maintenance, home care, meals and personal care (Duckett, 2018). People with greater needs may receive either a basic, low-level, intermediate or high-level home care package to assist them at home, depending on their assessed needs (Department of Health, 2019). Australian studies have argued that these service systems are not working well (Day et al., 2017; Gill et al., 2018). For example, limited low-level, intermediate and high-level care packages are currently available, with eligible people waiting over 12 months on average to access them (Department of Health, 2019). Reports indicate that currently 62,942 people are waiting for a package at their approved level, with another 49,295 offered an interim package whilst they wait (Department of Health, 2019). People often have to access private community and in-home services to remain at home while waiting (Day et al., 2017). Another Australian study has shown that people who use care services in Australia live at home longer, with greater service use equating to better outcomes (Jorgensen et al., 2018). These Australian studies provide relevant knowledge about the issues with and benefits of service use; however, study samples do not specifically include people with dementia.
Several studies have explored the factors related to people with dementia entering residential care (Afram et al., 2014; Brodaty et al., 2014; Toot et al., 2017), though rich detail about local perspectives and experiences is lacking due to limited Australian qualitative research. Additionally, few previous studies have examined both informal and formal caregivers’ perceptions and explanations. A qualitative understanding of the experiences of informal carers and care staff relating to residential care entry of the people with dementia they care for may assist services and policymakers better cater for identified needs.
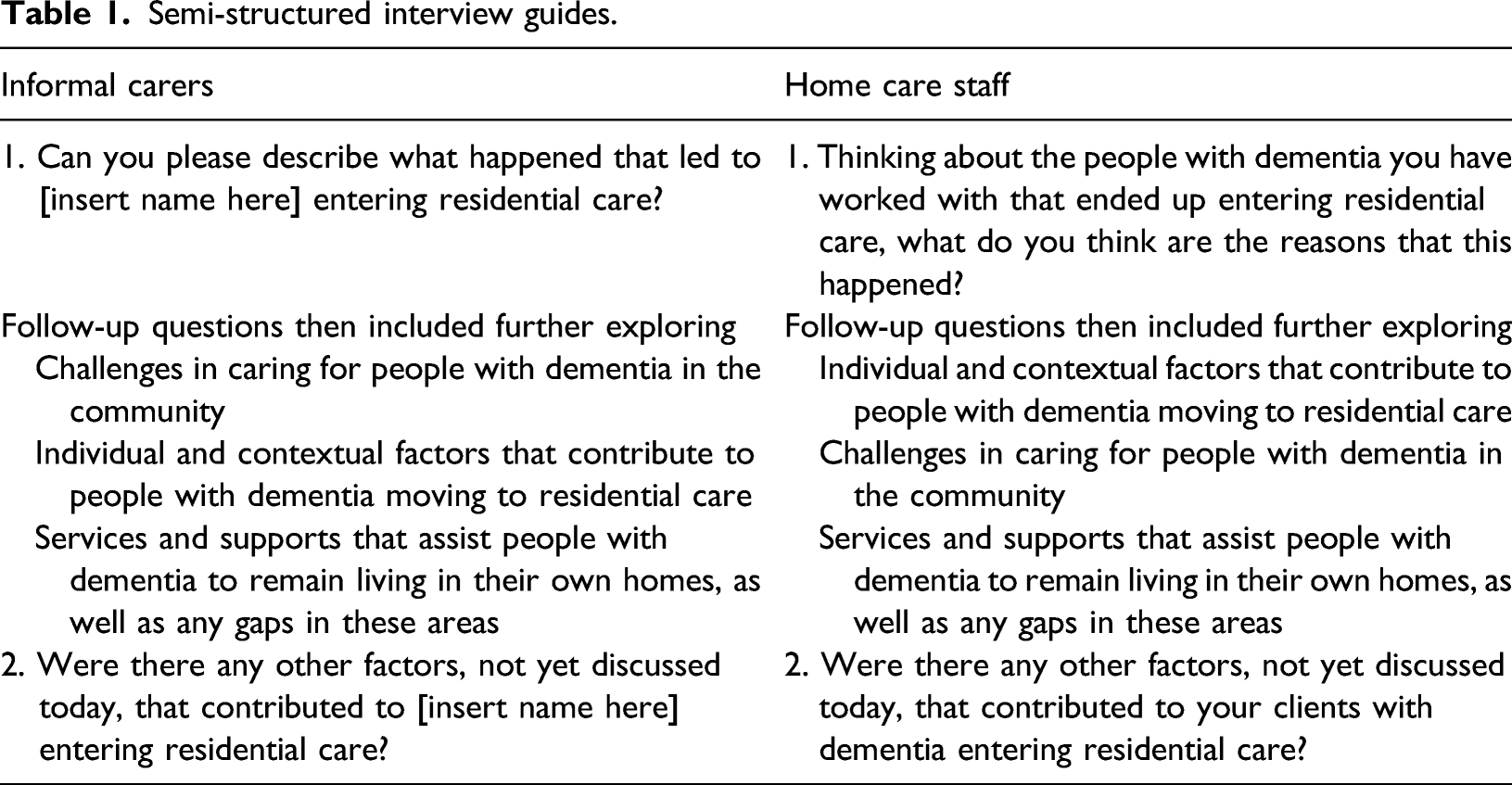
This study explored the factors that result in people with dementia transitioning to residential care in Perth, Western Australia (WA), from the perspectives of informal carers and community care staff. Specific objectives were to explore 1. individual and contextual factors that contribute to people with dementia moving to residential care, 2. challenges in caring for people with dementia in the community and 3. services and supports that assist people with dementia to remain living in their own homes, as well as any gaps in these areas.
Methods
Semi-structured interview guides.
Participants
Demographic information of participants.
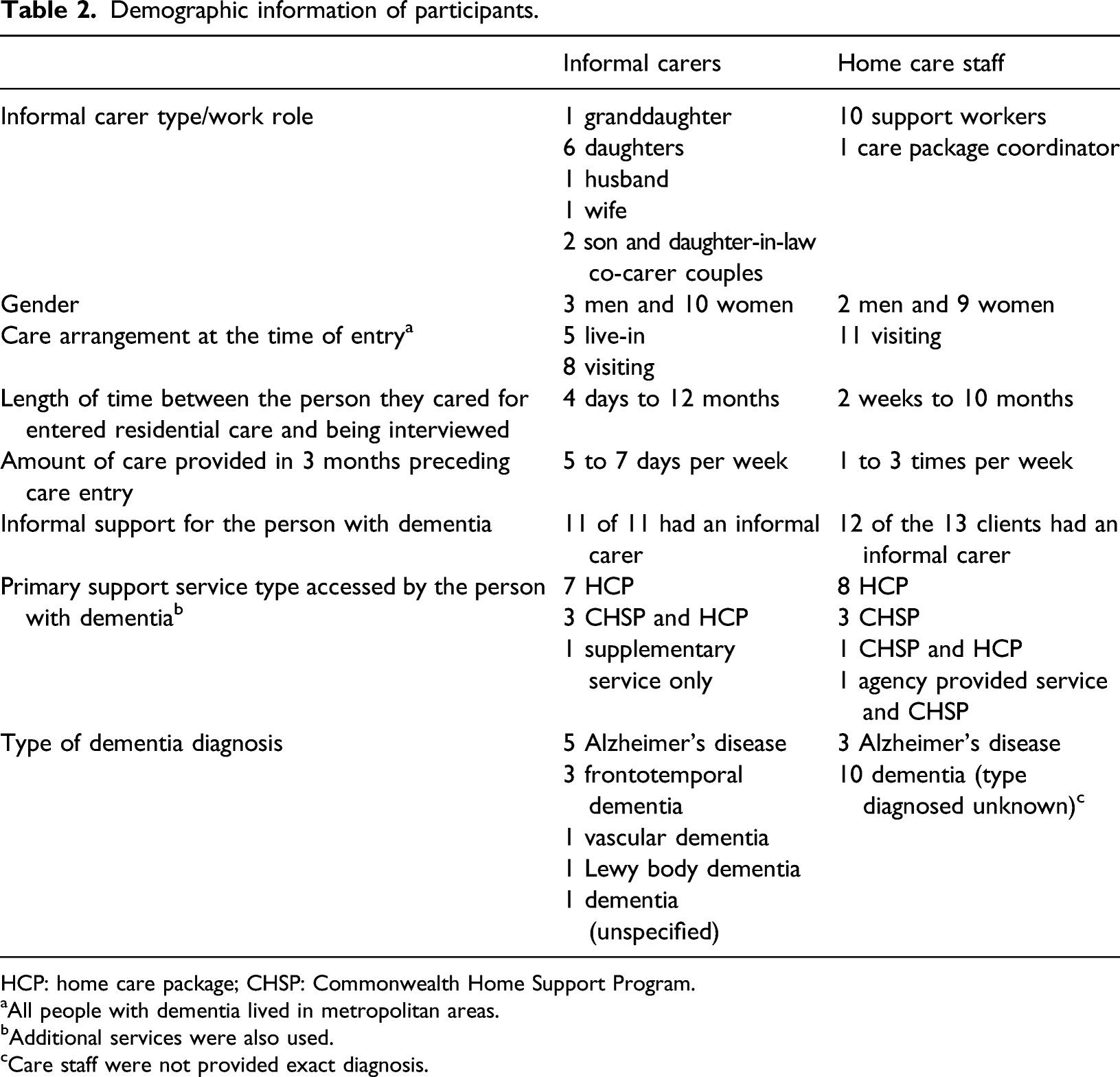
HCP: home care package; CHSP: Commonwealth Home Support Program.
aAll people with dementia lived in metropolitan areas.
bAdditional services were also used.
cCare staff were not provided exact diagnosis.
Procedures
Interviews took place between April and August 2019. Participants chose the interview time and venue (generally their home or at the university). Participants were provided with the interview questions via email beforehand if they desired to view them, as well as the participant information statement, and consent form. Participants provided written informed consent before their interview took place. Interviews were face-to-face and ranged between 41 minutes and two hours 11 minutes (average 70 minutes). Interviews were carried out by one researcher (TM), a social work student and early career researcher, with one conducted jointly with a co-researcher (CM). All were audio recorded with permission.
Analysis
All interviews were transcribed verbatim and analysed using Braun and Clarke’s (2006) six-phase model of thematic analysis concurrently during data collection, enabling consistent monitoring of saturation of themes. Researchers familiarised themselves with the interview data by repeated readings of transcripts, developing initial codes and organising them into potential themes, potential themes being reviewed and honed, the themes named and defined and then included in the report and supported by extracts. Co-coding was completed by all researchers using NVivo 12 (QSR International, 2018) to establish consensus. A reflexive journal (Probst, 2015) was maintained to examine beliefs and experiences impacting on data analysis in order to limit any bias. Member checking (Liamputtong, 2013) was carried out with all participants, with representation letters summarising key themes sent to participants for scrutiny to ensure accuracy. One participant requested amendments. Pseudonyms were assigned to protect participant confidentiality.
Findings
Informal carers and care staff identified the ‘tipping point’ of people with dementia needing to enter residential care as either due to a combination of factors or a sudden event or specific issue. The themes identified were individual factors, carer-related challenges and contextual factors related to entry, as well as contextual and individual factors that supported staying at home. Individual factors linked to entry included deterioration related to worsening cognition, changed behaviours and a decline in the ability to perform activities of daily living; co-occurring health conditions and safety concerns. Carer-related challenges included the carer no longer being able to meet the person’s care needs and the impact of supporting a person with dementia becoming too much for their informal carer. Contextual factors were a lack of family or social support and needing greater assistance from services. Factors that supported the person with dementia to stay at home longer were family and social support, service assistance and dog ownership. A conceptual framework of factors related to residential care entry based on the study findings is illustrated in Figure 1. Conceptual framework of factors related to residential care entry for people with dementia.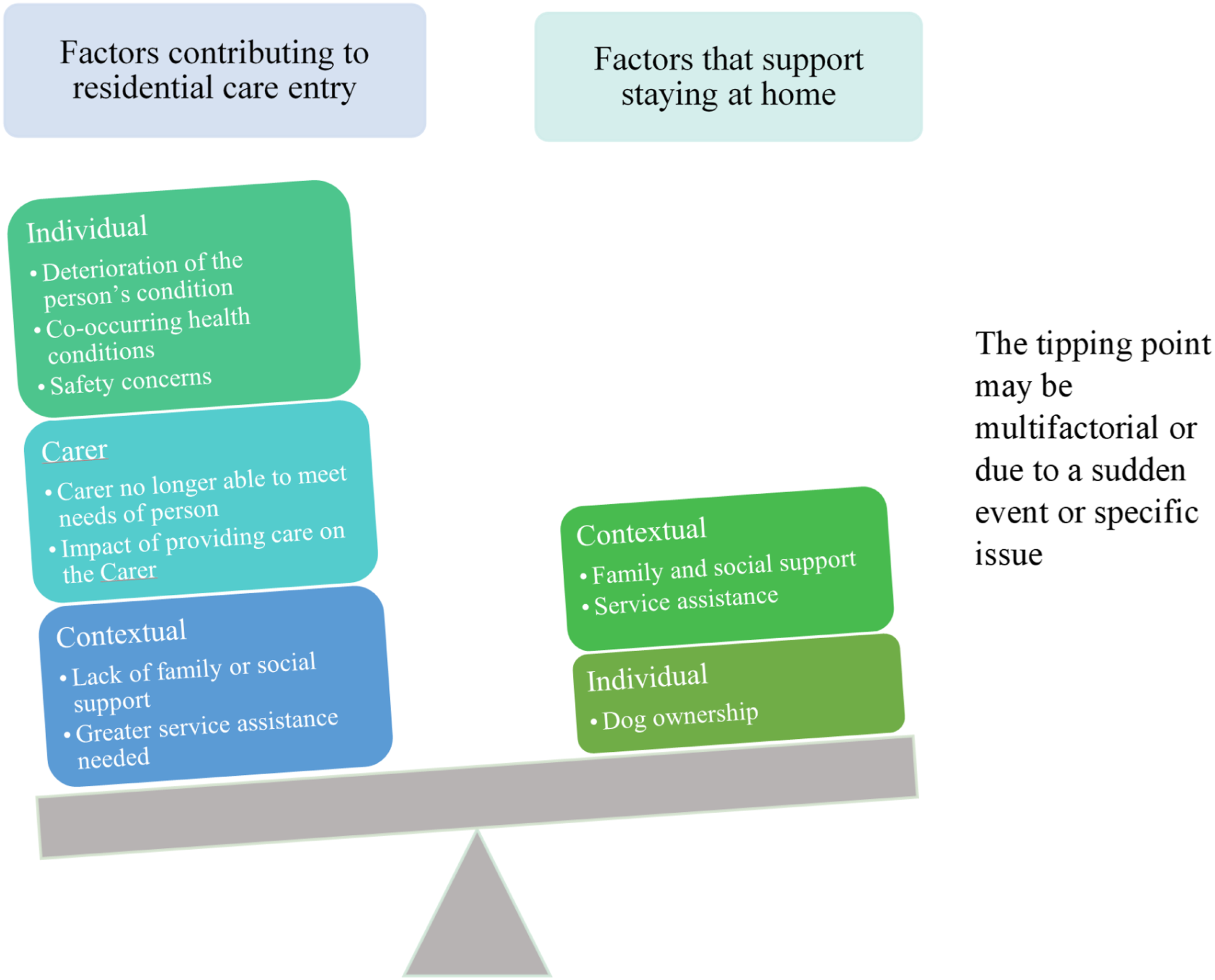
Tipping point: Multiple factors or a sudden event or specific issue
The majority of informal carers and care staff expressed that a combination of factors led to the people they cared for with dementia needing to transition to residential care. Zoe (support worker) stated, ‘I think it was just those (sic) combination of everything together and it was inevitable’. Alternatively, a few participants identified that the people with dementia they cared for entered residential care mainly due to a sudden event or specific issue, with one factor the catalyst for entry to residential care. For example, Sally (informal carer) described that ‘the line in the sand was incontinence’ for her mother moving into residential care.
Individual factors
Deterioration
Nearly all informal carers and care staff mentioned that deterioration related to worsening cognition, changed behaviours or a decline in the ability to perform activities of daily living contributed to the people they cared for with dementia to need to enter residential care. The main cognitive factors that were identified as contributing factors were memory loss, disorientation or confusion, incontinence and speech difficulty. Zoe (support worker) stated: His dementia was getting worse. He was forgetting where he was. He would constantly ask questions … : “Where am I?”; “What am I doing here?”; “I'm not quite sure what I'm supposed to be doing”. It just got a little bit too much all around.
Peter (informal carer) explained that his wife was admitted to hospital and then to residential care due to an incident where ‘she became incontinent … and she didn't know where she was’. Aaron (support worker) identified informal carer dependency as a reason his client entered residential care as ‘he was not able to talk’ and his ‘anxiety level got terrible. You know, he would not leave his wife [client’s informal carer] alone’. Key changed behaviours identified as contributing factors by several informal carers and care staff were anxiety, wandering, sleep disturbance, aggression or agitation and hallucinations or delusions. Olivia (informal carer) described that ‘100%, the aggression, the wandering, the complete lack of sleep for days’ were reasons why her grandfather entered residential care. Wendy (support worker) outlined, ‘he would just get really annoyed and he did get a bit violent towards the main carer, so, for her own safety and for his safety as well, I think that was one of the main things’. Hannah (informal carer) said that ‘it all came to [a] head with the hallucinations really’, as her mother used to think ‘there’s people coming in through the window’. Key factors related to activities of daily living identified by informal carers and care staff as reasons for the transition to residential care were difficulty with eating or drinking, walking, showering and dressing. Vanessa (informal carer) explained that her husband needed to enter residential care because ‘he needed assistance with all activities of daily living’, such as he could not walk and needed help with eating, drinking, showering and dressing.
Co-occurring health conditions
Approximately, a third of the informal carers and a couple of care staff identified co-occurring health conditions as a factor. These conditions were mainly physical health issues, such as a seizure, broken hip, arthritis and heart condition(s). Sarah (informal co-carer) described that ‘his heart and his pain [from his heart] would’ve been the two, on top of his dementia, that I think had the biggest impact’ on the decision to transition her father-in-law to residential care. Louise (support worker) described a client with dementia who was sent to hospital and then transitioned to residential care because the client could not walk unassisted after ‘she had broken her hip’ from a fall.
Safety concerns
Most informal carers and care staff identified safety concerns as a factor. Two main safety concerns were mentioned: falls and wandering. For example, Lucy (support worker) stated that ‘when she started to wander, Bianca [client’s informal carer] thought it was best that she go into a facility where she was safe’. In addition, Layla (informal carer) described that ‘ultimately, it was because he [her father] had the fall. That was the straw that broke the camel’s back …. I had to admit then, that he wasn’t safe’.
Carer-related challenges
No longer being able to meet the care needs
A large number of informal carers and care staff identified no longer being able to meet the demands of caregiving as linked to entry to residential care. Penelope (informal carer) described that: Mum really had to go into care. There was nothing more that we could do really at home. And once mum definitely couldn't walk anymore, I physically couldn't look after her. I couldn't pick her up, I couldn't get her in and out of bed. So yeah, the time was right.
Additionally, Lucy (support worker) stated: ‘her daughter had to make that horrible hard decision to put her into care, ‘cause we [herself and other support workers] just couldn’t be there 24 hours a day’.
Impact of supporting a person with dementia becoming too much for their informal carer
The majority of informal carers and almost half of the care staff identified that one of the factors was that the impact of supporting a person with dementia became too much for their informal carer. The main issues identified by care staff as contributing factors were the impacts on the informal carer’s mental health and the informal carer not coping. Aaron (support worker) shared that ‘the family felt that mother was not coping looking after dad [his client]’ as their mother developed depression. In comparison, several informal carers mentioned that they themselves were not coping and identified negative impacts of caregiving on their work, mental health, physical health or social life. Olivia (informal carer) described the demands of caring for her grandfather as negatively impacting on ‘every single part’ of her life, and said she did not have enough time to work or for her social life, ‘carers have to make that choice, and choose residential care, because you can’t sacrifice yourself to care for somebody else, because then you both lose’. Care staff less frequently identified that the impact of providing support on informal carers’ work life, physical health or social life contributed to the decision to enter care.
Contextual factors
A lack of family or social support
Approximately half of the informal carers and care staff perceived that a lack of family or social support contributed to the people they cared for transitioning to residential care. A lack of family support included either a family member not adequately assisting the person with dementia or the rest of the family not supporting the person by helping ensure all care needs were met. Cecilia (informal carer) mentioned that ‘I think if it had been possible for my brother and sister to share the load that would have helped me’ to support her father to remain living at home. The main gaps in social support included a lack of support from friends or neighbours. Ben (support worker) cared for a client that lived alone and had no informal carer. He identified that ‘it could have been a family and or friends; but yes, just anybody really, that would have perhaps just helped him stay there at home for longer’.
Needing greater assistance from services
Most informal carers and care staff commented that greater assistance from services was required in order for the people they cared for to remain living at home longer. The main issues identified were a need for increased home support from a range of services and professions, including support workers, nurses, occupational therapists or physiotherapists; limited availability of home care packages or appropriate higher-level package and a lack of access to residential respite care due to it being difficult to access, with it needing to be booked well in advance and expensive. Louise (support worker) mentioned that her client could have returned home from hospital instead of entering residential care ‘if she had all the right support’, including another support worker, an occupational therapist and a physiotherapist to help her to recover from her broken hip and to ease the care demands on her son. Rebecca (support worker) stated that ‘they said it will be at least another six to 12 months before her home care package is released. And so basically, he [client’s informal carer] had no option. He wasn’t coping’. Penelope (informal carer) explained that difficulty accessing residential respite care was a contributing factor: ‘you just think, “Oh, man. All I want is a break”, and waiting 4 months, that’s forever down the track’.
Factors that support staying at home
Family and social support
The majority of informal carers and care staff identified the contextual factor of family and social support as assisting people with dementia to remain living at home longer. Beneficial family support included having a family member carer or having other family members support either the person with dementia or informal carer. Chantelle (support worker) explained that her client ‘had three daughters, and I think they all helped keep her home’. The main helpful social support identified by participants was assistance from neighbours and friends. For example, Nina (informal carer) described that some of the neighbours definitely helped her mother remain living at home longer, ‘they kept an eye out’ for her.
Service assistance
Numerous informal carers and care staff reported that the support of various healthcare workers, attendance at day facilities and residential respite care assisted the people they cared for to remain at home longer. The support viewed by many participants as beneficial included assistance by support workers, a general practitioner, a home care package coordinator, nurses, an occupational therapist, a physiotherapist, an exercise physiologist and a hospital social worker. Heidi (home care package coordinator) stated that ‘we had regular support staff going in [to care for the client], feeding back to me. So with all [of] them, that definitely helped him stay at home longer’. Participants identified that attendance at day facilities was beneficial because it gave informal carers a break or was an opportunity for social interaction for people with dementia. Gwyneth (support worker) explained that day facility access ‘gave John [client’s informal carer] peace for a day, … kept him able to have a little bit of sanity, sort of, to keep her at home’, whereas Cecilia (informal carer) described, ‘if [her father] hadn’t had some where to go during the day, I’d have been worried and he would have deteriorated in his health because he wasn’t having any social interaction, he wasn’t getting out of the house’. Participants also discussed that residential respite care was beneficial because it gave informal carers a break. One informal carer spoke about positive benefits for both the carer and the person with dementia: It [residential respite care] helped me not have a mental breakdown. It helped me recuperate a little bit health-wise. So it helped. I guess it helped him [her father with dementia] as well because then he was getting the care that he needed. It was positive. Layla (informal carer)
In contrast, Rebecca (support worker) mentioned her client ‘declined even further’ in residential respite care due to the facility not adequately caring for her as a result of being understaffed.
Dog ownership
A few informal carers (two informal carers and a co-carer couple) and one support worker identified dog ownership as an individual facilitator for people with dementia to remain living at home longer. Participants described that the main benefits of this were that it ‘orientated’ thinking due to needing to care for the pet, provided ‘companionship’ and gave meaning to their life. For example, Hannah (informal carer) outlined that dog ownership had been beneficial for her mother because it gave her mother ‘purpose’, as her mother had to ‘look after the dog, feed the dog’. Sarah (informal co-carer) described that ‘the other thing that kept him [her father-in-law] at home was his dog’, ‘she orientated him, he’d worry about whether she’d had some food, and those sorts of things’, ‘kept him company’ and ‘he could always talk to the dog’. Ben (support worker) explained that the ‘companionship’ of a dog assisted his client, who lived alone and had no informal carer, to live at home longer, ‘the dog gave him [his client] a lot of joy because they’d been friends for so long’.
Overall, informal carers and care staff identified numerous factors that contribute to people with dementia needing to transition to residential care. Informal carers and care staff identified either multiple factors or a sudden event or specific issue led to the tipping point to needing to move to residential care for people with dementia. The factors identified by participants were deterioration, co-occurring health conditions, safety concerns, carer no longer being able to meet the care needs, impact of supporting a person with dementia becoming too much for their informal carer, a lack of family or social support and needing greater assistance from services. The factors identified by participants as supporting staying at home were family and social support, service assistance and dog ownership.
Discussion
This study identified that the majority of participants perceived that a combination of individual, carer and contextual factors led to the tipping point for people with dementia needing to transition to residential care, though a few participants identified that this was due to a sudden event or specific issue. The finding that the tipping point is due to a range of factors is consistent with past European (Afram et al., 2014) and international (Toot et al., 2017) research that also identified entry to residential care as generally multifactorial. For example, Toot et al. (2017) identified that the person, their carer(s), health services and surroundings can all impact on residential care entry for people with dementia. The implication is that services and supports aimed at assisting people with dementia to remain living at home need to be broad enough to address a range of individual, carer and contextual factors.
The individual factors identified by participants as contributing to people with dementia entering residential care were deterioration related to worsening cognition, changed behaviours and a decline in the ability to perform activities of daily living; co-occurring health conditions and safety concerns. Many of these findings were consistent with prior Australian (Brodaty et al., 2014), European (Risco et al., 2015) and international (Toot et al., 2017) research. For example, previous research similarly identified declining cognition (Brodaty et al., 2014; Toot et al., 2017), BPSD (Brodaty et al., 2014; Toot et al., 2017) and declining functioning (Brodaty et al., 2014; Risco et al., 2015) were linked to entering residential care. Research by Toot et al. (2017), however, was unable to conclude if physical health was linked to entering residential care due to inconsistent findings in the studies reviewed for their systematic review. Therefore, this study adds further evidence that co-occurring health conditions, such as physical health issues like a broken hip and heart condition(s), are causes for entering residential care. The study findings, which have several similar findings to those of previous research, have demonstrated the importance of services and supports being targeted at addressing individual factors of people with dementia.
The carer-related challenges identified by participants as having contributed to people with dementia entering residential care were the carer no longer being able to meet the care needs and the impact of supporting a person with dementia becoming too much for their informal carer. These findings are supported by European (Afram et al., 2014) and international (Toot et al., 2017) studies, but not Australian research (Brodaty et al., 2014). For example, Brodaty et al. (2014) found that the level of carer burden did not predict earlier residential care entry. In contrast, the carer-related findings of this current study were consistent with European and international studies that found that carers no longer being able to meet the care needs (Afram et al., 2014) and carer burden (Afram et al., 2014; Toot et al., 2017) were factors linked to entering residential care.
The findings of the current study also identified variations between informal carer and care staff views. For example, care staff did not recognise at the same rate as informal carers that the impact of providing support for the person with dementia on informal carers’ work life, physical health or social life often contributed to the decision to enter residential care. This is significant and in line with an Alzheimer’s Disease International (2019) study exploring stigma-related knowledge, attitudes and experiences in relation to people living with dementia. This international study found that, of the 18,377 carer participants, caring for a person with dementia impacted on the health of 52%, the social lives of 62% and the work of 49%. The carer-related findings from the current research provide evidence of a greater need for services and supports to assist informal carers while also demonstrating that the impacts of supporting a person with dementia are not fully recognised by care staff. It should also be recognised that caregiving may be defined and experienced in multiple ways, as individual, relational, social and instrumental, though is often primarily identified as task-based (Nolan et al., 1995) by the service system. Carers’ understandings of care and links to the relationship with the person with dementia they care for have not been unpacked in this study but could be an area for further exploration in relation to how changes in the balance of the relationship impact on transition to residential care.
The contextual factors identified by participants as having contributed to people with dementia entering residential care were a lack of family or social support and needing greater assistance from services. Alternately, participants identified family and social support, service assistance and dog ownership as factors assisting people with dementia to remain living at home longer. The finding that a lack of family or social support was an impetus for entry to residential care supports Brodaty et al’s. (2014) finding that living alone was likely to be linked to entering residential care earlier. Additionally, the finding that service assistance supports people with dementia to remain living at home longer is consistent with Jorgensen et al’s. (2018) study, which identified that Australian care service users live at home longer. However, barriers exist to accessing timely support, with recent findings by the Aged Care Royal Commission that wait times to access a home care package range from three to more than 12 months (Royal Commission into Aged Care Quality and Safety, 2019). A surprise finding was the benefits of dog ownership; however, international research has identified the links between pet ownership and improved physical, mental and social health for older people (Gee et al., 2017). Therefore, further research into the specific impacts of dog/pet ownership for people with dementia may be important. The current study has identified gaps in services and supports and a number of factors that services can provide greater support around, with the aim of helping people with dementia to remain living at home for as long as possible.
Overall, the findings of this study may assist service providers and policymakers to better understand the individual, carer and contextual factors related to people with dementia entering residential care. This information will promote the development of more effective strategies to support people with dementia and their carers in the community. Helping people stay at home longer would also support the wishes of many people with dementia (van der Roest et al., 2009). Delayed entry to care may reduce the high cost of residential care for the government and family members (Gnanamanickam et al., 2018) and defer other aspects, such as increases in BPSD for the person with dementia and carers experiencing guilt, depression and feeling like a failure, both of which are linked to entry to care (Sury et al., 2013).
The study had both strengths and limitations. Two limitations were that the study sample consisted of a lack of linguistic diversity and amount of cultural diversity is unknown. For example, the sample did not include non-English speakers, and participants were not asked about what cultural group they belonged. The next limitation was that all participants were recruited from Perth, WA. Therefore, caution needs to be taken if generalising the findings to other populations. Another limitation was that interviews were retrospective, relying on participants’ memory of factors related to entering residential care for up to 12 months after the event. Finally, the study did not include the perceptions of people with dementia, who potentially may have identified different factors important for support and service design. In contrast, the strengths of the study included having a sample size large enough to achieve data saturation (Saunders et al., 2018), the wide range of types of dementia represented in the informal carer findings and the qualitative methodology that explored participant’s perspectives and understandings of why the people with dementia they cared for had entered residential care.
Conclusion
This study identified that the tipping point for people with dementia living in the community to enter residential care was largely multifactorial, though a few participants also identified a sudden event or specific issue as the cause. The research found that people with dementia entered residential care for a combination of reasons: dementia-related deterioration, co-occurring health conditions, safety concerns, the carer no longer being able to meet the care needs, the impact of supporting a person with dementia becoming too much for their informal carer, a lack of family or social support and needing greater assistance from services. Alternatively, the study found that services and supports that assisted people with dementia to live at home longer included family and social support, service assistance and dog ownership. Overall, the tipping point may occur when the needs of the person with dementia outweigh what the carer and other services and supports can provide. The findings of this study contribute to Australian and international research and address qualitative research gaps in this area. Additionally, the study identifies a range of individual, carer and contextual factors for service providers and policymakers to target for service and policy development in order to better support people with dementia to remain living at home.
Footnotes
Acknowledgements
The authors would like to thank the informal carers and care staff who gave their time to participate in the study. They would also like to acknowledge Alzheimer’s WA who provided the initial idea for the research, gave feedback around the design and assisted with recruitment. Lastly, the authors acknowledge the support of Juniper, Carers WA and all the other organisations who assisted with recruitment.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical Approval
The Human Research Ethics Committee (HREC) at Curtin University approved this study (HRE2019-0015). Additionally, the study was approved by a participating agency’s own HREC (EC App 134) before data collection specific to that agency.