
Abstract
Purpose
This study examined the impact of a Montessori mealtime intervention for people living with dementia to support the mealtime experience of residents and mealtime care practices of staff in a memory support unit. The mealtime intervention was part of a broader culture change project.
Method
An observational research design was used to evaluate changes in the mealtime experience and care practices across three time points (baseline, post-implementation, maintenance), spanning 30 months. Five video recordings of the lunch time service (range: 19–32 min) were analysed. The coding protocol comprised pre-determined indicators related to accepted dimensions of person-centred care. Resident and staff behaviours were quantified across four categories: providing choice and preferences, promoting the social side of eating, supporting independence and showing respect towards residents. Staff behaviours that reflected personal enhancing actions and personal detractors were also coded during each mealtime service.
Results
A significant increase in staff providing residents with the opportunity for choice and a subsequent significant increase in residents demonstrating choice behaviours was evident. Staff and residents both significantly increased their interactional behaviours, with greater social interaction between staff and residents. Staff further demonstrated greater support for mealtime independence that reached and maintained significance during the final two sampling points. Significant gains observed post implementation were largely maintained and, on specific measures, further increased over time. A significant increase in staff use of personal enhancing actions during mealtime care was also evident. Variability in individual staff and resident behaviour highlighted the complexity of mealtime care and culture change processes.
Implications
The study provides novel evidence to support the use of a Montessori mealtime intervention to achieve more person-centred mealtime care, and which resulted in a more respectful, enabling and social dining experience. Clinical implications and direction for future research are presented to build on these findings.
Introduction
Mealtimes are a central aspect of daily life for people with dementia living in aged care homes, vital to healthy nutritional intake and well-being (Watkins et al., 2017). Taking place several times a day, mealtimes present important opportunities for social interaction and honouring of individual preferences, culture and identity (Chaudhury et al., 2017; Genoe et al., 2012). To meet the medical, nutritional and psychosocial needs of residents, mealtime care should be holistic and person-centred, providing the opportunity for choice, supporting independence, showing respect for individual residents, and promoting the social side of eating and drinking (Reimer & Keller, 2009). Implementing person-centred mealtime care is, however, inherently challenging given the complex and multi-factorial nature of both the structure of mealtimes and the motor and cognitive skills needed for safe and efficient oral intake (Caspar et al., 2020; Hung & Chaudhury; 2011; Reimer & Keller, 2009; Watkins et al., 2017). Care staff play a central role in providing feeding assistance and enabling resident choice, nutrition and enjoyment of food, yet organisational structures and systems, such as insufficient staff supports and time pressure, can undermine the mealtime experience and the quality of interactions between staff and residents (Milte, et al., 2017; Watkins et al., 2017). Past research has found that mealtimes are often highly proceduralised and task-focused, and organised around institutional and staff factors rather than the needs of residents (Herke et al., 2018; Hung & Chaudhury, 2011). Staff mealtime care practices have been shown to be variable and interactions between residents and staff minimal and often incongruent with person-centred care principles (Bennett et al., 2015; Hung & Chaudhury, 2011). As a result, opportunities to promote personhood during mealtimes can be missed, with the psychosocial components of mealtimes often overlooked and considered secondary to maximising nutritional status (Hung & Chaudhury, 2011). As a result of these challenges, people living with dementia and their family members often perceive the mealtime experience to be poor, even though maintaining choice and individual preferences around eating and drinking remain important to the person (Milte et al., 2017). As such, there is a pressing need for further mealtime intervention research, seeking creative and sustainable solutions to improve the mealtime experience and ensure mealtime care practices are dignified and person-centred to maximise quality of life in addition to supporting safe and efficient oral intake.
To date, most mealtime intervention studies for people with dementia in aged care homes have targeted food consumption, mealtime function and responsive behaviours during mealtimes, such as agitation (Fetherstonhaugh et al., 2019; Hung & Chaudhury, 2011). Many of these interventions have focused on making modifications to physical aspects of the dining environment. For example, enhanced lighting and colour contrast (e.g. between the plate and table) have been found to increase food intake (Brush et al., 2002), while smaller dining rooms (Schwarz et al., 2004) and playing music during meals (Hicks-Moore, 2005) have resulted in more positive resident behaviour and engagement during mealtimes. More homelike mealtime environments have also been found to improve oral intake and protect against malnutrition (Nijs, de Graaf, Kok, & van Staveren, 2006), with further potential to enhance autonomy and comfort during mealtimes (Chaudhury et al., 2017). These interventions have had success in enhancing aspects of the dining experience, however, this has not necessarily meant that mealtime care practices have become more person-centred, but neither has this been consistently measured (Fetherstonhaugh et al., 2019). For example, Chaudhury and colleagues (2017) found that renovations to the mealtime environment improved the general ambience and homeliness of the dining space as well as enhanced opportunities for residents to have autonomy and engage in mealtime rituals, however, instances of negative mealtime care interactions persisted. This included observed instances of staff ignoring residents during the mealtime service, talking about residents in their presence and labelling them with reference to food texture (e.g. ‘This one is lactose free’; Chaudhury et al., 2017, p.891). With reference to person-centred care, such staff actions represent personal detractors that can undermine the personhood and well-being of a person with dementia, as opposed to personal enhancing actions, or positive person work, that are thought to promote dignity, respect and personhood (Kitwood, 1997). Considering this finding, Chaudhury et al. (2017) suggested that a more systemic approach was required, embedding mealtime interventions within broader organisational and staff culture change initiatives, to drive the holistic changes needed to optimise person-centred mealtime care.
Multi-component interventions that target mealtime culture, organisational policies and care practices, as well as the social and physical environment and the individual care needs of residents, represent highly complex interventions, requiring conceptual and practical frameworks to support the change process and translation of person-centred mealtime practices into routine care (Caspar et al., 2020; Chaudhury et al., 2017; Fetherstonhaugh et al., 2019; Reimer & Keller, 2009; Watkins et al., 2017). The Montessori approach has been identified as one potential framework to provide a pathway to service-wide person-centred care, with potential to significantly improve the mealtime experience (Brush, Douglas, & Bourgeois, 2018). Montessori educational methods were first applied to dementia care as the basis for creating interventions for people with dementia and as a way of providing structure and order in the care environment (Camp, 2010). Montessori-based programming draws upon rehabilitation principles and techniques, including task breakdown, the provision of immediate feedback, guided repetition and sequencing, as well as the provision of meaningful activities to facilitate learning and engagement (Booth et al., 2020; Camp, 2010). Montessori methods have been applied as non-pharmacological interventions for people with dementia on an individual and group basis, with evidence of positive outcomes for constructive engagement (i.e. direct interaction between the person with dementia and a target activity), reduction in agitation and use of pharmacological medications and improvements in affect and quality of life (Brush, Douglas, & Bourgeois, 2018; Mbakile-Mahlanza et al., 2020; Roberts et al., 2015; van der Ploeg et al., 2013; Yuen & Kwok, 2019). Perhaps where the Montessori approach has demonstrated greatest potential is in its broader application as a philosophy of care, transforming how care is delivered and how people with dementia are viewed and related to (Roberts et al., 2015). Montessori models of care allow for a more person-centred approach, focused on the abilities, interests and holistic needs of the person; and on the considered design of prepared environments that enable choice, enhance function and provide purposeful activity and meaningful engagement (Booth et al., 2020; Brush et al., 2018). Several organisations internationally, including the United States and Australia, have implemented Montessori approaches in aged care homes to transform the culture of care and improve quality of life outcomes for residents (see Brush et al., 2018; Roberts et al., 2015).
With specific reference to mealtimes, Montessori-based interventions have been applied to improve independent eating skills and reduce feeding dependency in people living with dementia in aged care settings (Lin et al., 2010; Liu et al., 2015; Sheppard, McArthur, & Hitzig, 2016; Wu et al., 2014). Protocols for Montessori interventions for eating have involved repeated and individually graded practice of procedural skills for mealtime activities, such as hand-eye coordination, scooping, squeezing, pouring and differentiating edible and non-edible foods (Lin et al., 2011). Familiar and personally salient food items are typically used during training sessions, served as snacks, rather than practiced during regular mealtimes (Lin et al., 2011). These studies suggest that Montessori activities can be used to maintain and improve the self-feeding skills of residents with dementia. However, to our knowledge, research to date has not looked specifically at the implementation of Montessori mealtime interventions as a strategy for supporting staff use of person-centred mealtime care practices and embedding more positive person work into routine care.
Current study
The current study aimed to evaluate whether a Montessori mealtime intervention implemented in an aged care memory support unit for people with dementia would enhance person-centred mealtime care practices of staff and result in a more social and respectful dining experience for residents. The intervention was multi-faceted, comprising staff education in a Montessori-based model of care (named by the Organisation as Care with Purpose), the creation of a more homelike and enabling mealtime environment, and re-design of organisational policies and procedures to improve mealtime care practices in line with Montessori principles. It was predicted that a significant increase in the frequency of positive staff and resident behaviours would be demonstrated within all categories of person-centred mealtime care (Reimer & Keller, 2009) following implementation of the care innovation and, further, that these changes would be maintained over time. The improvements would reflect residents having greater opportunity for choice, more positive social interaction, increased independence and greater respect shown towards residents during mealtimes. A significant increase in staff use of personal enhancing actions and a reduction in use of personal detractors during mealtime care were also predicted. This would provide evidence of a shift towards more person-centred care.
Method
The project had ethical approval through Curtin University Human Research Ethics Committee (HRE2016-0056). An observational study design was followed, with longitudinal data collection conducted from 2015 to 2018. A novel coding tool was developed for the purposes of the study, to enable staff practices, interactions and procedures occurring during mealtime care to be recorded and analysed against a common theoretical framework.
Participants
The study took place in a memory support unit housed within an aged care organisation in Perth, Western Australia. The resident population was limited to 17 at any one time, reflecting the size of the memory support unit. Residents in the unit changed over the study period. All residents admitted to the unit were living with memory loss, with severity of symptoms ranging from mild to severe as assessed on the Mini Mental State Examination (MMSE; Folstein et al., 1975). Overall, the severity of cognitive impairment of the individual residents increased over time, at variable rates, which is expected in the context of dementia. Organisational criteria for residents to be admitted to the memory support unit included living with memory loss and reduced orientation, an ability to mobilise and adequate alertness and capacity to complete daily activities like showering with assistance from a maximum of one carer. The leadership team reported that the admission criteria evolved over time with the management team accepting residents with more advanced dementia to the unit. This meant that the overall severity of cognitive impairment in residents admitted to the unit also increased over the time of the study. Residents remained living in the memory support unit until they required a comfort care model, to minimise disruption to their familiar environment and routine. This meant that the care demands for care staff increased across the time of the study. Ten regular care staff were recruited to provide consistency for the residents and to foster a cohesive team. A Leader of Care Innovation was appointed to work across the organisation, serving as a link between management and care staff, assisting in the orientation and training of new staff and providing mentoring on the floor. Staff turnover occurred during the study period, most notably for afternoon and night shift staff, with less turnover of day shift staff, who were more likely to be employed full time. Furthermore, the Leader of Care Innovation went on parental leave during the study period. A lifestyle staff member took over this leadership role for the memory support unit, later stepping into a Lifestyle Leader role across the whole organisation. When this occurred, a Lead Carer role was established in the unit. Having a leadership role meant that for any day shift, there was always at least one of the Montessori leaders available on the floor to provide mentoring and support, as well as at least one of the core Montessori care staff.
Montessori mealtime intervention protocol
The Organisation’s model of care, Care with Purpose, embedded principles of the Montessori approach in all aspects of care and provided the broader context for the mealtime intervention. The aim of this model was to provide a more personalised and engaging environment, where meaningful activities, roles and memory supports were integrated within daily routines and interactions with residents. The mealtime intervention was multi-faceted, with three main foci: (1) structural, physical and aesthetic changes to the mealtime environment, (2) procedural changes to the mealtime service and relevant policies in line with Montessori principles and (3) training and communication processes for all staff in Montessori methods for dementia and the mealtime intervention.
Environmental modifications
Montessori principles and relevant evidence from the dementia mealtime literature were used to review the existing mealtime environment and inform the modifications made to the physical dining space. This included making the dining room more dignified and homelike through use of table cloths, removing all plastic from the service (e.g. replacing stained beige plastic mugs with white china tea cups and mugs), placing condiments on the tables for meals, minimising noise during mealtimes (e.g. vacuuming) and ensuring that simple food was prepared and cooked in the unit each day, drawing benefit from the smell and experience of mealtime related activities (e.g. use of coffee percolator and bread maker). Clothing protectors were also replaced with fabric serviettes. Montessori principles informed external memory supports and orientation cues in the mealtime environment, including signage to support wayfinding, a menu board, task breakdown cards in the kitchen (e.g. how to make a cup of tea) and labelled cupboards. A locked door to the kitchen was removed, providing residents with full access to the kitchen. Buffets, drink stations and snack fridges were installed to provide access to food and more opportunities for choice. Residents were encouraged to serve their own meals independently or with the assistance of a staff member. Residents were also actively involved in mealtime activities, such as setting tables, folding serviettes, writing the menu board and peeling vegetables.
Policies and procedures
Policy and procedural changes were introduced to help facilitate the Montessori mealtime intervention. For example, in the period prior to the intervention, residents were given a choice of two menu items using a meal choice form, which was completed on a six-monthly basis by the facility manager, with limited input from residents. Drinks were poured prior to the meal and food delivered on a trolley in metal serving dishes that were stored on a bench or in the oven until served. The chef provided enough food for the residents’ order, with few additional servings. The staff would serve the resident their meal, often placing their dessert on the table next to the main meal. Residents who required feeding assistance were positioned around the edge of the dining room and medications were routinely dispensed during meals. Significant changes were made to these procedures, extending the duration of the breakfast and lunch service to allow residents to eat at a more relaxed pace, providing additional food to ensure all residents had the option of the two main dishes on offer and of second helpings, and to serve themselves drinks. The evening meal remained the same as prior to the intervention, due to the higher workload and lower staff ratios at that time (i.e. no lifestyle or therapy staff available to assist). Residents with additional mealtime needs, including dysphagia, received individualised assessment and care. Modified diet and fluid recommendations were overseen by a qualified speech-language pathologist. Instructions and procedure sheets were developed for staff, including photographs of what the environment should look like. Strategies were also put in place to optimise daily communications between staff to ensure staff were adequately informed about residents’ mealtime preferences and support needs.
Training and communication processes
All staff employed in the organisation during the study period, including catering staff, attended a 1 day Montessori training program delivered by a certified Aged Care Montessori and Dementia Consultant. This training was offered twice per year and provided a comprehensive overview of the Montessori philosophy and practical ways to design activities and prepare environments to facilitate meaningful engagement. Staff were also invited to attend a 1 day Montessori leader training session, with additional training opportunities in dementia, mental health, managing aggression, and Montessori job roles available to staff. The Montessori consultant continued to work alongside the leadership team, providing ongoing mentorship. This included direct feedback when visiting the unit twice per year, as well as trouble shooting over the phone as required. In the first 3 months of the project, senior staff in the organisation (e.g. Executive Manager Residential Care, Leader Care Innovation) spent approximately 3 to 6 hours in the unit each week to provide orientation to new staff, assist existing staff with any issues they were facing (e.g. responsive behaviours during evening meals), improving systems (e.g. easily identifying which residents had or had not eaten during buffet-style meals) and thanking staff for their efforts. After the Leader of Care Innovation went on parental leave, the Lifestyle Leader assumed the mentoring role, providing consistent role modelling and assistance on the floor. Regular team and family meetings were held to foster knowledge of individual residents (e.g. interests, abilities and support needs) and to work collaboratively to solve problems and celebrate successes, including those related to mealtime care.
Procedure
Video recordings
Video footage was taken by organisation staff during several different mealtimes over a 30 month period, including videos of morning tea and lunch time service. Five videos of the lunch time service, ranging in length from 19 to 32 min, were selected from a total of 7 available recordings based on comparable content and length, allowing like for like comparison. The selected videos comprised two baseline videos taken in November 2015 during the initial stages of the intervention (baseline 1 (B1) and 2 (B2)), one video taken in August 2017, 18 months post-implementation (Post Imp), and two videos taken in August 2018, 30 months post-implementation to monitor maintenance of change (maintenance 1 (M1) and 2 (M2)). All recordings were taken on a weekday and during the day shift. Video data captured both physical and social aspects of the mealtime environment, including resident and staff behaviour and interactions in the kitchen and dining spaces. The research team recorded and tracked the number of staff and residents that were captured in each video across 5 minute time increments, to assist coding, analysis and interpretation of the data. Furthermore, staff from the organisation reviewed the residents captured in each mealtime video, confirming that the mix of residents in terms of stage of dementia and severity of cognitive impairment was comparable at each time point. The camera was set up within the room in a stationary position and not operated during recording. Multiple recordings were taken during the evaluation period to ensure that the presence of the camera was not novel to staff or residents. Provisions were made to stop the recording at any time if a resident, staff member or family member indicated concern or a preference not to be videoed; however, this did not occur during the study period. The videos selected for analysis were chosen based on video quality, ensuring that the mealtime environment and staff-resident interactions were visible and a minimum of six residents were present in the frame at any one time. The selected videos were transcribed to represent the sequences of events, aspects of the environment and interactions between and behaviours of staff and residents. Verbatim quotes were recorded where audible to provide direct examples of staff and resident interactions.
Video coding protocol
Person-centred mealtimes coding protocol.
Frequency counts for each indicator were recorded and tallied by two authors using the video transcripts and repeated observation and viewing of the video footage. The collaborative coding process allowed operational definitions to be refined during coding, while ensuring a rigorous approach. Any discrepancies were discussed and checked by returning to the video footage and operational definitions and seeking input from the other members of the research team as required. There was some overlap in counts across the behaviour indicators, for example, a specific staff behaviour could be counted as providing choice, as well as a personal enhancing action (e.g. facilitating). Similarly, a staff action could be coded as social interaction (e.g. verbal engagement that is mealtime related), providing feeding assistance (e.g. verbal prompting or encouragement; ‘As best you can’), as well as a personal enhancing action (e.g. warmth). As such, the counts were not independent and reflected the more dynamic and multi-dimensional nature of mealtime care where different physical and relational actions could occur simultaneously.
Data analysis
To measure stability during the pre-intervention period and the significance of change over time, behaviour counts were compared using Fisher’s exact test (two tailed) at different timepoints. Baseline stability was assessed across the two pre-intervention timepoints. Where the baseline was stable for a measure, the baseline scores were averaged. On measures where a significant difference was evident between the two baselines, the higher score was used for comparison to provide a more conservative comparison.
Results
To examine the impact of the Montessori mealtime intervention on mealtime care practices and resident and staff behaviours, coded data from the video recordings, across the 14 indicators, were compared over time. The results are outlined below with respect to each of the four elements of person-centred mealtime care, with the direct evidence layer preceding the personal enhancers and detractors where applicable.
Providing choices and preferences
Layer 1: Direct evidence
Direct evidence of staff providing residents with increased choice during mealtimes was seen over the sampling period (see Figure 1). While numerical increases from the average at Baseline (B) (10.5) to Post Imp (18) were not significant (Fisher exact z = 1.22, p = .223 two tailed), significant increases were observed at both M1 (39) (Fisher exact z = 3.91, p < .001 two tailed) and M2 (37) (Fisher exact z= 3 .70, p < .001 two tailed). The increased opportunity for choice related most notably to the main meal (B = 1.5; M1 = 14; M2 = 7) and dessert (B = 0.5; M1 = 9; M2 = 9). A significant increase in the choice behaviours of residents, however, was observed from Baseline (4) to Post Imp (15) (Fisher exact z = 2.29, p = .022 two tailed) and maintained at M1 (22) (Fisher exact z = 3.33, p < .001 two tailed) and M2 (28) (Fisher exact z = 4.07, p < .001 two tailed) (see Figure 1). Residents showed increased choice behaviour at Post Imp, M1 and M2, with respect to each of the categories related to drinks, main meal and dessert. Residents were observed to have more genuine food, drink and mealtime options (e.g. where to sit) that were not evident during the baseline period. Summary of coded video data scores for choice over time.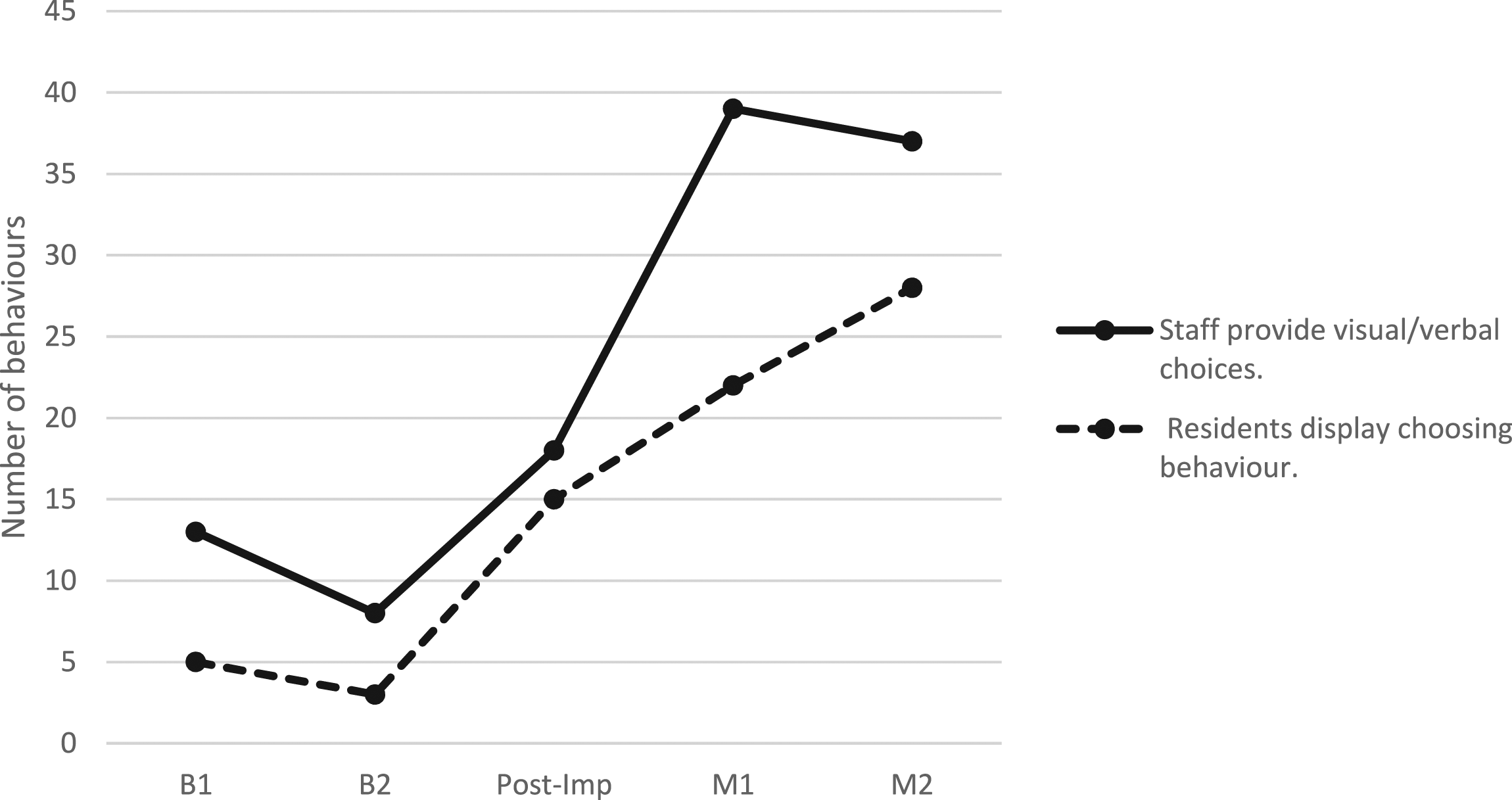
Layer 2: Personal enhancers and detractors
Staff demonstrated a significant increase in personal enhancing actions promoting choice, increasing significantly from the average at Baseline (5) to Post Imp (19) (Fisher exact z = 2.65, p = .008 two tailed) and maintained at M1 (27) (Fisher exact z = 3.71, p < .001 two tailed) and M2 (35) (Fisher exact z = 4.58, p < .001 two tailed). The increase in personal enhancing actions related predominantly to staff facilitating food choices (B = 1; Post-Imp = 11; M1 = 11; M2 = 16), for example, by providing visual and verbal supports to assist choice (e.g. drawing a resident’s attention to items on the buffet or dessert trolley to provide visual choice, often with verbal encouragement, e.g. ‘Have a look’ (M2)). The quality of choices available to residents was also observed to change over time, with staff providing richer information to support choice, for example, progressing from ‘Would you like salt and pepper?’, ‘Have you finished?’, and ‘Would you like coffee?’, each at Baseline, to ‘We’ve got lamb chops and pork and lentil’ (Post Imp), ‘Would you like a little bit of both?’ (Post Imp), ‘What would you like to drink? Orange juice or lemon?’ (M2).
A reduction in staff use of personal detractors opposing choice was evident in the post-implementation videos. A significant decrease in personal detractors was seen from an average at Baseline (19) to Post Imp (3) (Fisher exact z = 3.20, p = .001 two tailed) and maintained at M1 (0) (Fisher exact z = 4.13, p < .001 two tailed). The number of personal detractors increased slightly at M2 (6), however, this remained significantly lower than baseline (Fisher exact z = 2.40, p = .016 two tailed). There were occasions of outpacing choice recorded during the Baseline period (2), Post Imp (3) and M2 (3), where residents were not given sufficient time to make food or drink choices. Instances of imposition were high at Baseline (17), but also noted again at M2 (3), where residents, while fewer in number, were not given an opportunity for choice, for example, ‘Get you some dessert’ (B1).
Promoting the social side of eating
Layer 1: Direct evidence
The number of observed social interactions between staff and residents increased significantly from the perspective of both staff and resident behaviour (see Figure 2). Staff showed a significant increase in the frequency of social interactions with residents, increasing from Baseline (57.5) to Post Imp (96) (Fisher exact z = 3.02, p = .002 two tailed) and maintained at M1 (125) (Fisher exact z = 4.92, p < .001 two tailed). A further significant increase was evident from M1 (125) to M2 (167) (Fisher exact z = 2.40, p = .017 two tailed). Most notably, this reflected a significant increase in staff verbal engagement with residents that related to the mealtime (e.g. explaining staff actions, providing verbal encouragement to eat; B =23.5; Post Imp = 48; M1 = 56; M2 = 71; Fisher exact z = 2.78, p = .005 two tailed, Fisher exact z = 3.53, p < .001 two tailed, Fisher exact z = 4.78, p < .001 two tailed, respectively). An increase in staff verbal engagement with residents that was socially oriented and not task related was also evident (e.g. greetings, chatting; B = 7; Post Imp = 13; M1 = 18; M2 = 27). Staff attention to residents through forward-facing postures and listening behaviours showed a steady increasing trend, reflecting significant gains at both M1 (Fisher exact z = 2.28, p = .023 two tailed) and M2 ((Fisher exact z = 1.96, p = .05 two tailed) from baseline activity. Summary of coded video data scores for social interaction over time.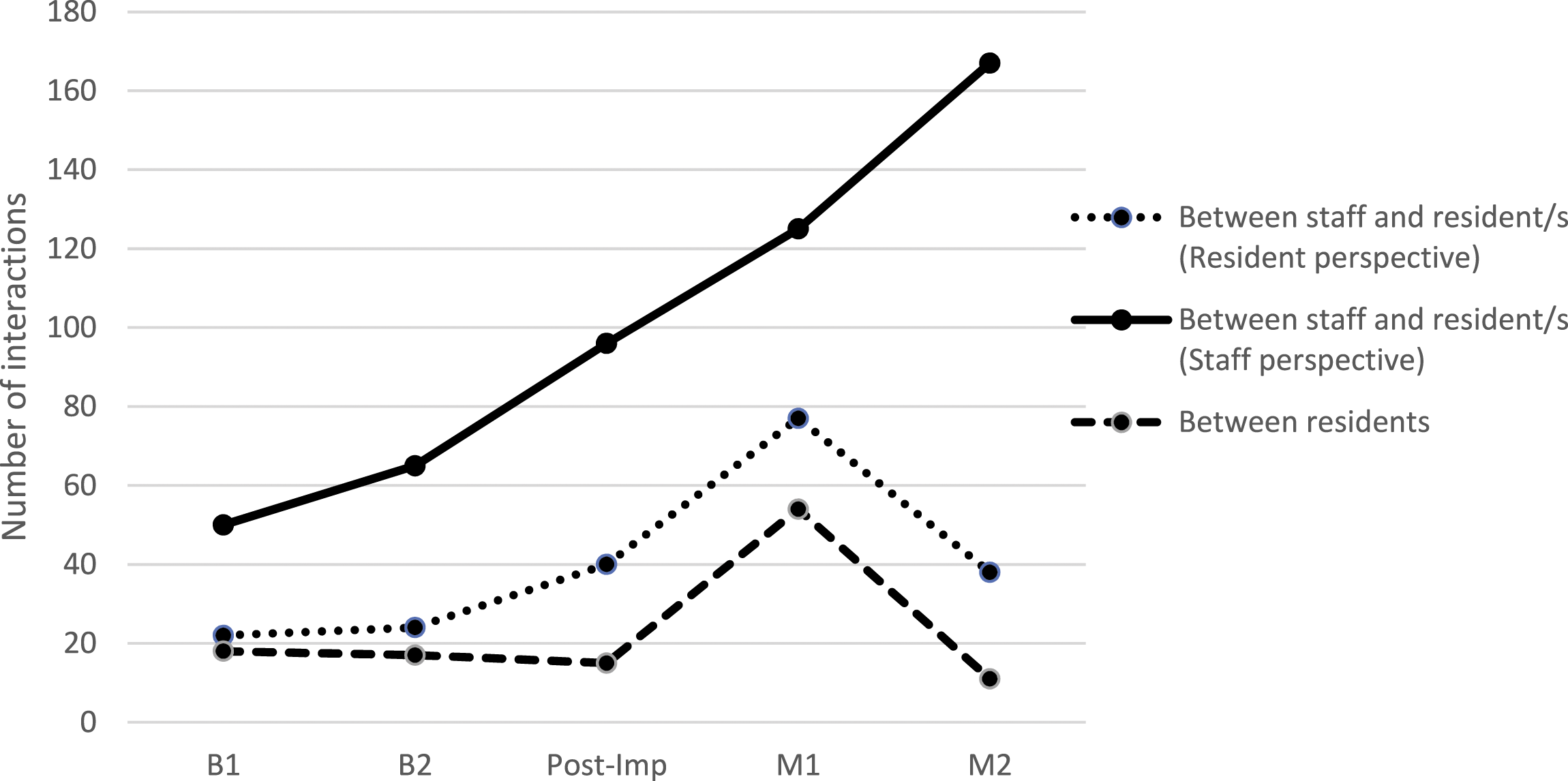
Residents also showed a significant increase in the total number of positive social interaction behaviours, with frequency increasing from Baseline (23) to Post Imp (40) (Fisher exact z = 2.02, p = .044 two tailed). A further significant increase was evident at M1 (77) (Fisher exact z = 5.30, p < .001 two tailed). The significant gains from Baseline (23) were not maintained, however, at M2 (38) (Fisher exact z = 1.79, p = .073 two tailed). The increase in positive social interaction behaviours at Post Imp was primarily evidenced by increased attention to care staff by residents demonstrated through use of forward-facing postures and listening behaviours (B = 5.5; Post Imp = 12; M1 = 23; M2 = 12). An increase in chatting behaviour directed to staff was also evident (B = 5.5; Post Imp = 12, M1 = 13; M2 = 9). Social interaction between residents remained relatively stable across all time points (B = 17.5; Post Imp = 15; M2 = 11), except for M1 (55), where a significant increase was evident from B1 (Fisher exact z = 4.29, p < .001 two tailed). The behaviours that showed greatest increases at M1 involved a resident attending to another resident, using body language indicating listening, and chatting behaviours directed to another resident.
Layer 2: Personal enhancers and detractors
Staff demonstrated a significant increase in personal enhancing actions promoting the social side of eating, from average at Baseline (5) to Post Imp (22) (Fisher exact z = 3.08, p = .002). This increase was maintained at M1 (27) (Fisher exact z = 3.71, p < .001) and M2 (35) (Fisher exact z = 4.58, p < .001), with an increase in counts that demonstrated belonging, validation and fun shared between staff and residents.
A significant difference in frequency of personal detractors opposing the social side of eating was noted across the Baseline period, that is, from B1 (31) to B2 (9) (Fisher exact z = 3.32, p < .001 two tailed). Care that was task focused was evident during the B1 mealtime service with instances of objectification (16; e.g. staff serving meals or clearing plates without speaking to or making eye contact with the resident), invalidating (8; e.g. failing to acknowledge residents’ emotional state) and withholding (4; e.g. not giving attention to resident when they are anxious or seeking help). Irrespective, this further decreased significantly at both Post Imp and M1 (0) (Fisher exact z = 2.67, p = .008 two tailed). Instances of detractors increased again at M2 (13), attributed to a single staff member and including examples of ignoring (7), objectification (3) and mockery (3), which were discrepant to other staff actions observed in the M2 mealtime.
Supporting independence
Layer 1: Direct evidence
A significant increase in positive mealtime assistance was evident across the Baseline period, that is, from B1 (12) to B2 (31) (Fisher exact z = 2.74, p = .006 two tailed), with B2 then taken as the more conservative time point for comparison (see Figure 3). Staff provision of feeding assistance then remained relatively stable at Post Imp (21) (Fisher exact z = 1.25, p = .2.12 two tailed), M1 (45) (Fisher exact z = 1.49, p = .136 two tailed) and M2 (46) (Fisher exact z = 1.60, p = .111). There was a significant increase from baseline (B = 8) in staff using combined verbal and physical prompts to the maintenance period (M1 = 24, Fisher exact z = 2.65, p = .008 two tailed; M2 = 27, Fisher exact z = 3.04, p = .002 two tailed). Here, staff were seen to actively encourage and assist residents to access the buffet to select what they wanted to eat through verbal/tactile prompts and physical assistance to promote self-service, as well as to encourage self-feeding. Summary of coded video data scores for feeding assistance over time.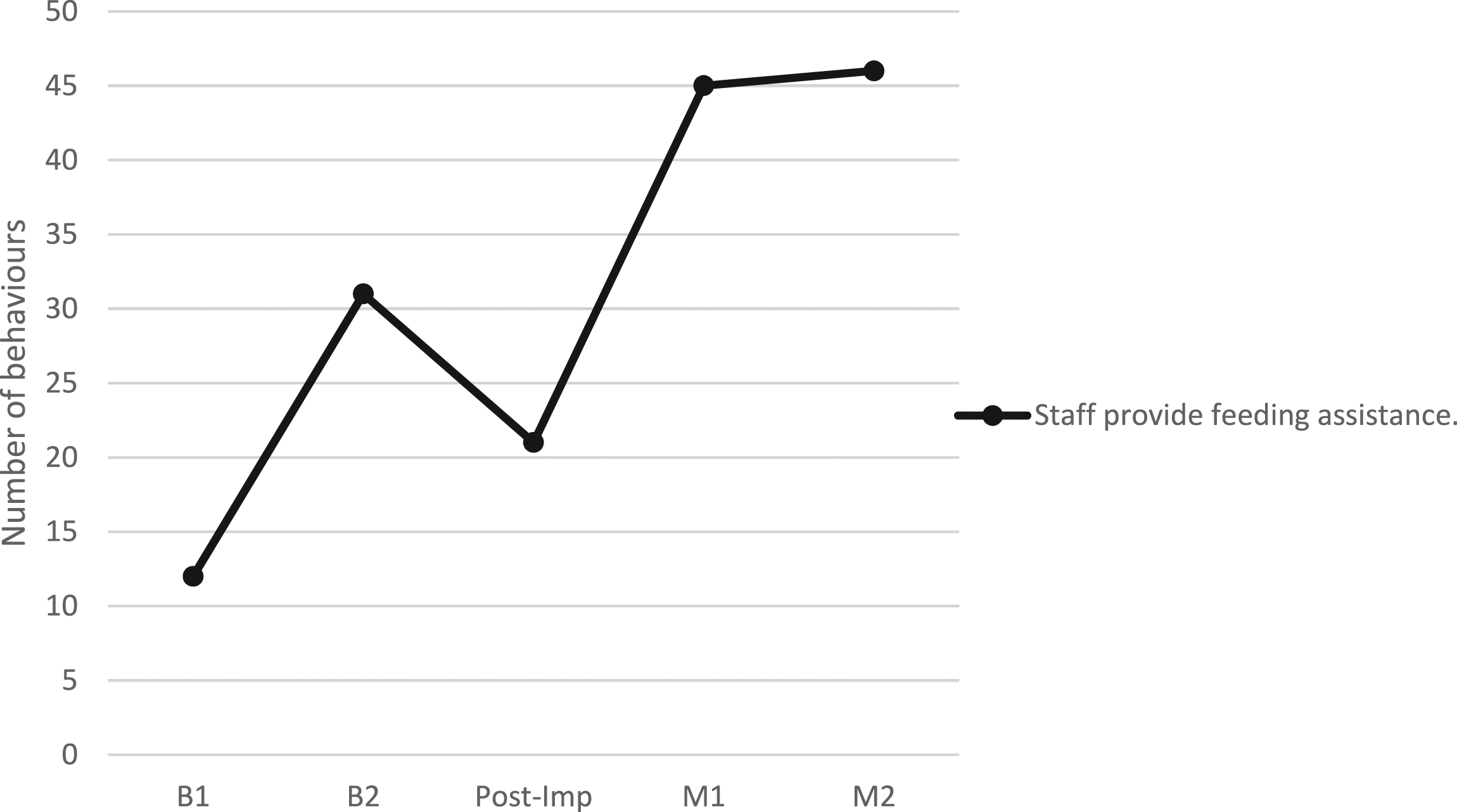
Layer 2: Personal enhancers and detractors
A significant increase in personal enhancing actions promoting independence was evident from B1 (0) to B2 (18) (Fisher exact z = 3.67, p < .001), hence the B2 score was used as the baseline measure. This remained stable at Post Imp (23) (Fisher exact z = .62, p < .532), but significantly increased at M1 (45) (Fisher exact z = 3.37, p < .001) and this increase was maintained at M2 (41) (Fisher exact z = 2.86, p = .004). Behaviour was characterised by an increase in facilitation (Baseline = 15; Post Imp = 8; M1 = 23; M2 = 23) and empowerment (Baseline = 0; Post Imp = 9; M1 = 17; M2 = 10) that supported feeding independence. In facilitating independence, staff were observed to provide more tailored support in the post implementation mealtimes (e.g. staff member cuts up food and places morsel on end of fork and leaves on plate for resident (M2)) and more verbal explanations of what was on the plate to bring attention to the meal (e.g. ‘silverside and fish’ M2; ‘It’s got a little bone in it ok’ M1). Examples of celebration were also evident at Post Imp (4) and M1 (3) that recognised residents’ achievements and their contribution to mealtime activities (e.g. ‘…come and sit down over here after all your hard work’ (Post Imp)).
A significantly higher frequency of personal detractors opposing residents’ independence in the mealtime was also evident at B1 (28) in comparison to B2 (3) (Fisher exact z = 4.31, p < .001), such that the second baseline measure was used to measure change. The earlier behaviours, however, reflected a high level of disempowerment (16; e.g. ‘Put your arm down please, I’m trying to feed you’; staff taking over feeding; staff leaving residents for extended periods of time without assistance) and outpacing (7; e.g. staff placing dessert before the main meal had been finished; not giving sufficient time to chew when providing feeding assistance with residents pulling their head away). Examples of infantalisation (3; e.g. mouth scraping) were also observed at B1. With the more conservative measure used, the number of personal detractors opposing residents’ independence maintained at Post Imp (1) and M1 (0). While not significant, a small numerical increase was evident, at M2 (6), with all personal detractors relating to a single staff member. This included examples of infantalisation and disparagement (e.g. ‘You didn’t drink your drink. Drink your drink.’).
Respect
Layer 2: Personal enhancers and detractors
A significant increase in staff use of personal enhancing actions that showed respect towards residents was evident from B1 (7) to B2 (20) (Fisher exact z = 2.31, p = .021) such that the second measure (B2) was again used for comparison. A significant increase was seen from Baseline (20) to Post Imp (40) (Fisher exact z = 2.45, p = .014), maintained at M1 (47) (Fisher exact z = 3.18, p < .001) and M2 (64) (Fisher exact z = 4.69, p < .001). Over time, there was a noticeable increase in staff behaviours that displayed genuineness (B = 0, Post Imp = 7, M1 = 8, M2 = 18) and warmth (B = 11, Post Imp = 15, M1 = 18, M2 = 28), with staff behaviours showing concern and affection towards residents conveyed through physical actions (e.g. affectionate tap on the shoulder), verbal statements and a respectful, compassionate tone of voice (e.g. ‘Here you go my love’ M1, ‘Enjoy!’ M1, ‘This is yours over here darling’ M1, ‘Come with me, we’ll go to the kitchen’ M2). Examples of terms of endearment being used by staff were only coded as respectful when they were used in a relational context and where the resident responded positively, showing a sense of genuine connection.
Staff use of personal detractors that did not show respect towards residents were only observed during Baseline (2) and M2 (11). Compared to Post Imp and M1, the baseline period was characterised by much higher levels of disruption, with staff breaking residents’ frame of reference and through a high level of kitchen noise and staff conversations that were task focused and did not include or involve residents. At B2, there was an instance of a staff member respectfully waking a resident for the meal, however, they then made a joke to another resident ‘Can you set an alarm clock’, coded as mockery. An instance of accusation was also noted earlier in the baseline period whereby a staff member stated ‘You’re not straight’ in an abrupt tone that lacked warmth to a resident who did not appear able to reposition themselves independently. At M2, all personal detractors related to a single staff member who created significant disruption during the mealtime service (e.g. created loud kitchen noise, interrupted a resident eating their meal to administer medication).
Enhancers and detractors
Figure 4 provides a summary of the personal enhancing actions and personal detractors demonstrated by staff during each mealtime. This profiles the positive person work that characterised each mealtime service and shows the increase in use of personal enhancing actions post implementation, as well as the reduction in personal detractors at Post Imp and M1. The M2 profile demonstrates a high level of personal enhancing actions, in particular a very high level of respect shown towards residents, in conjunction with the re-emergence of personal detractors. All of the personal detractors at M2 related to a single staff member, which disrupted the cohesion and overall feel and experience of this mealtime service. Summary of coded video data scores for personal enhancing actions and personal detractors for each mealtime service.
Discussion
This study aimed to evaluate whether a multi-faceted Montessori mealtime intervention for people living with dementia would result in enhanced person-centred mealtime care practices and a more engaging and respectful dining experience for residents. As predicted, significant increases in staff and resident behaviours were demonstrated that reflected greater opportunity for choice and social interaction, as well as greater respect shown to residents during mealtimes. A significant change in occasions of feeding assistance were not evident post implementation, however, staff were observed to use more examples of tailored facilitation over time to promote independence. Overall, evidence of staff using a higher number of personal enhancing actions in the post-implementation videos, signified enhanced person-centred mealtime care practices. These care domains are elaborated below.
The Montessori approach and enhanced person-centred mealtime care
Promoting choice
Evidence of residents having greater opportunity for choice and demonstrating increased choice behaviours during mealtimes was reflected in where residents sat and who they dined with, as well as choices made in relation to menu items and portion sizes during the mealtime service. The higher incidence of choice was notably facilitated by structural and procedural changes made to the meal format (e.g. the introduction of the buffet and the tea/coffee station), however, increased opportunities for choice were also promoted by a shift in the quality of staff actions. That is, the way staff provided choice was enhanced over time, with evidence of more information and richer options being given to promote choice. This suggested that staff were placing greater value on residents’ autonomy, which is a critical contributor to quality of life and a central component of person-centred mealtime care (Reimer & Keller, 2009). This is important, with increasing recognition ‘that treating residents as active decision makers is a core task in dementia care’ (Kristiansen et al., 2018, p. 210).
Promoting the social side of eating
The frequency and quality of social interaction during mealtimes was also observed to increase over time, indicating that social aspects of the mealtime environment were enhanced by the Montessori mealtime intervention. Social interaction between staff and residents increased steadily and significantly across the mealtimes, with the number of instances of staff attending, listening and chatting with residents doubling post implementation. This was in conjunction with an increase in staff use of personal enhancing actions that promoted the social side of eating, with greater instances of holding, validation, belonging, celebration and fun. This depicted more balanced and genuine interactions between staff and residents that were more congruent with person-centred care principles. That said, the interactions remained more focused on the mealtime task itself (e.g. verbal encouragement and explanations of staff actions). While this demonstrated greater attention towards residents and their needs during the mealtime service, future studies could consider strategies to increase verbal engagement with a more social orientation to further enhance the social environment.
The social interactions between residents remained more stable during the intervention period, with a significant increase in interaction seen at the first maintenance time point only. On this occasion, an interaction between a female and male resident was observed, centred on a doll being held by the female resident. The male resident was observed to validate the reality of the ‘baby’ throughout the interaction. It is important to note that, prior to the intervention, male and female residents were seated at separate tables, so this interaction would not have taken place. Despite residents having increased control over where they sat in the dining room and whom they dined with, improvement in interactions between residents remained limited overall. Future studies should consider more targeted interventions to encourage and facilitate friendships and explore the unique physical, social and emotional needs of residents (Reimer & Keller, 2009; Watkins et al., 2017).
Promoting independence
Direct counts of staff providing feeding assistance, such as physical, verbal, or visual prompts during the mealtime service, remained relatively stable over time, with staff cutting up the meal for residents and providing verbal encouragement and prompts to eat during the mealtimes. The quality of assistance was, however, observed to change, with more examples of staff using personal enhancing actions, such as facilitation and empowerment, to promote independence and involvement in mealtime procedures and activities (e.g. laying the table and serving themselves at the buffet). This inclusion in the mealtime service was not evident at baseline and represents an important aspect of the Montessori model and person-centred mealtime care (Hung & Chaudhury, 2011; Reimer & Keller, 2009). Furthermore, this allowed staff to celebrate and promote the occupation and personhood of residents through recognition of their strengths and contribution.
Showing respect
In addition to the above findings, there was also evidence of staff showing greater respect towards residents during mealtime care in the post-implementation videos. Respect behaviours increased at each time point, with many more instances of staff showing warmth and genuineness through verbal and non-verbal communication, including tone of voice, and adopting a more relaxed pace during the mealtime service. Overall, the degree of positive person work was noted to increase, with evidence that staff had enhanced aspects of relational care and appeared less driven by institutional or task factors. Due to the integrated nature of the principles within a Montessori approach, it is not possible to determine which aspects of the innovation were responsible for the changes seen, nor is this important. The Montessori framework, however, appeared successful in enabling culture change. This provides further support for the potential of multi-faceted mealtime interventions to make more holistic and systemic changes to mealtime care practices. Many aspects of the Montessori mealtime intervention were clearly visible in the video footage; evident in the prepared environment and embodied through staff and resident behaviours. These changes reflect a more positive mealtime ambience, a more homelike environment and more enabling mealtime experience. Based on the results of this study, each element of the intervention appeared to play an important role in facilitating more person-centred mealtime care.
Challenges for culture change
Despite the positive conclusions drawn from this study, challenges to the implementation and culture change process were evident. A prominent challenge related to the variability in care practices that was evident across the two baselines and within the final maintenance mealtime. In the latter example, one staff member, who had received the Montessori training but was not recruited to the Memory Support Unit as a core member of the team, was observed to disrupt the mealtime service and demonstrate excessive use of personal detractors. As such, this staff member was delivering care that was in direct contrast to the other staff on duty who were embodying the Montessori intervention principles. This reflects the logistical challenges of rostering and retaining core staff over time, with a commitment required to keep building the team and the support of management who understand and prioritise staff who are responsive to training. Having staff working in discordant ways, created a less cohesive mealtime environment, and revealed differences in how individual staff responded to the training and culture change process. Previous studies have shown variability in mealtime care practices and called for appropriately trained staff in providing mealtime care to people with dementia (Bennett et al., 2015; Chang & Lin, 2005; Chaudhury et al., 2017; Murphy et al., 2017). This highlights the importance of continued staff education, mentoring and real-time feedback to ensure expectations of care quality are explicit. The novel coding tool used to measure change and identify care practices that reflect the Montessori approach could be used to track progress in culture change, as well as to provide individualised feedback to staff. Previous research has shown that staff value feedback structured in terms of personal detractors and personal enhancers, linked to the psychological needs and well-being of residents, rather than framed as a reprimand to staff (Brooker & Surr, 2006). Finally, the variability in care practices and the re-emergence of personal detractors at the final time point speaks to the complex and dynamic nature of mealtime care and the need to continuously monitor for re-emergence of more traditional, task focused care during the culture change process. This reinforces the need for a clear vision, strong leadership and continued efforts to maintain change and build on successes over time (Ducak et al., 2015).
Limitations of the current study
The current study provides evidence to support the feasibility of and potential for the Montessori mealtime intervention to enhance the four elements of person-centred mealtime care, acknowledging limitations in the study design and generalisability of the findings.
While the repeated sampling of baseline activity aimed to monitor the reliability of data collected prior to implementation, and the longitudinal design sought to control for location, nature of resident admission and staff training, future studies may consider more stringent experimental controls. In this study, the residents in each mealtime were not identified, which meant we could not control for the impact of dementia stage or severity of symptoms on care practices or interactions between staff and residents. This should be addressed in future studies, particularly given that cognitive ability has been found to influence a resident’s level of engagement in previous Montessori studies (Gaspar & Westberg, 2020). For example, a shorter time frame would reduce variability of the resident population to allow direct comparison and to control for continuity of staff. Future research should also explore the impact of the Montessori model on nutritional intake and nutritional status of residents. A greater number of time points, sampling across more than one mealtime service (e.g. breakfast, morning tea and lunch time), would also maximise inclusion and tracking of different staff members and other contextual factors that may influence mealtime care. Further, as the study aimed to evaluate the outcomes of employing Montessori principles in one residential facility, no other facilities were recruited to compare this approach to other multi-component approaches or person-centred care models. This could be explored in future to increase understanding of the critical ingredients of person-centred care approaches and whether Montessori principles provide additional benefits. Comparative information could also be addressed using standard measurement tools. The development of the novel coding tool for use in this study enabled focused measurement of behaviour, however, future research could consider using validated tools, such as, the Dining Environment Assessment Protocol (DEAP; Carrier et al., 2016; Iuglio et al., 2018) that can be used to quantify the physical environment of dining rooms in aged care homes, enabling comparison across studies and increasing validity of the findings. These could be considered in future research to help identify which residents may benefit most from the Montessori mealtime intervention and how intervention strategies might be further tailored to individual residents as the condition progresses over time.
Conclusion
This study provides promising evidence of the benefits of a Montessori mealtime intervention for people with dementia, presenting a possible pathway towards more person-centred and enabling care. The findings add to the growing body of evidence supporting multi-faceted mealtime interventions and the value of Montessori-based models of care for people with dementia. The intervention has potential to increase opportunities for choice, promote the social side of mealtimes and enhance independence and engagement, while fostering more respectful and dignified mealtime care. Further research is needed to extend the current findings and guide culture change for the aged care sector.
Footnotes
Acknowledgments
We would like to thank Catholic Homes Inc for supporting this research and for the staff, residents, and family members for their willingess to engage in the culture change and evaluation process. We would also like to acknowledge Anne Kelly, Aged Care Montessorian and Dementia Consultant, for providing the training and mentorship for staff.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received funding from Catholic Homes Inc to support the evaluation of the Care with Purpose model of care.
Ethical approval
The project had ethical approval through Curtin University Human Research Ethics Committee (APPNO//HRE2016-0056).