
Abstract
Written patient education material, for example, discharge-information is commonly used in hospital settings. Despite following guidelines on how to best present text and using patients as consultants, improvements can still be made from a patient’s perspective.
Here, we describe the process of developing patient education material using a participatory design methodology, with patients, clinicians, researchers and designers working as co-designers following a structured process map. The method emphasises coping with conflicting interests and using this as a source of development. The philosophies behind action research and person-centred care were combined in a practical setting, enhancing both perspectives and generating actionable knowledge to be further used in patient involvement projects. The results reveal that predominant areas of tensions focused on power, organization, content and clinical usability. This study is one of the first to involve patients as co-designers of education materials in the health care context, and not only as consultants. Working as co-designers was found to be productive and in line with person-centred care philosophy, with focus on partnership and equality. The results of this study can therefore benefit both patients and other relevant stakeholders in the healthcare system in developing written patient education materials.
Keywords
Background
In this paper we describe the results from the process of using participatory design methodology to develop written patient education material used as complementary information before and after colorectal cancer surgery. Person-centred principles were used as a theoretical and philosophical frame. Having a participatory approach in health care research is argued to be beneficial for both professionals and the community involved by integrating the knowledge gained and shared with action (Israel, Schulz, Parker, & Becker, 2001). Here, in particular, we present the negotiations experienced between stakeholders such as patients, clinicians, researchers and designers during the development process. There is previous knowledge of how participatory design can create or enlighten conflicts of interest (Pilemalm & Timpka, 2008; Weng, McDonald, Sparks, McCoy, & Gennari, 2007), and even find it beneficial (Steen, 2013), but there is a lack of discussion in the action research literature regarding what, how and when negotiations could emerge in the process of co-designing education materials. Many studies report how new materials in health care have been developed from the perspective of patients (Jefford & Tattersall, 2002; Joshi et al., 2001; Paul, Hendry, & Cabrelli, 2004), or clinicians (Bolejko, Sarvik, Hagell, & Brinck, 2008; Jefford & Tattersall, 2002) and how researchers have used patients as consultants (Cleary, McCarthy, & Hegarty, 2012; Vallance, Courneya, Taylor, Plotnikoff, & Mackey, 2008). However, being partners, here as co-designers, is particularly significant when developing tools to support person-centred communication, but co-designing also involves new challenges (Scariot, Heemann, & Padovani, 2012). Our findings are of interest to a broader public in making future users of participatory design in collaboration with patients aware of the challenges involved. They may also contribute to theoretical development of person-centred communication (Öhlén, Carlsson, Jepsen, Lindberg, & Friberg, 2015) and add another dimension to the development of materials. The results can be of benefit for both patients and other relevant stakeholders in the healthcare system.
Written information
Written information such as patient education material is commonly used in hospital settings, particularly at discharge. It also prepares patients before or after procedures and diagnosis (Johnson & Sandford, 2005). Patients both need and ask for written information as a complement to oral information (Semple & McGowan, 2002). How the material is designed from a readability and comprehensibility point of view is of great importance to how relevant a supplement they will become (Helitzer, Hollis, Cotner, & Oestreicher, 2009; Hoffmann & Worrall, 2004). Features that need to be considered when designing new material can be grouped under the categories content, language, organization, layout and typography, illustrations and learning and motivation (Hoffmann & Worrall, 2004). Text should preferably be as simple as possible, gauged at the lowest level of reading skills to be comprehensible (Hoffmann & Worrall, 2004) and with both word- and sentence length sufficiently short (Mühlenbock & Johansson Kokkinakis, 2009).
Written information production and patient participation
Most written information is internally produced by clinicians (Payne, Large, Jarrett, & Turner, 2000; Smith et al., 2014), but Smith et al. (2014) demonstrates, by using a validated instrument, that only materials produced with the help of professional writers are rated superior. There is evidence that written information developed after consultation with consumers (patients) become more relevant, readable and understandable (Carney, Jones, Braddon, Pullyblank, & Dixon, 2006; Nilsen, Myrhaug, Johansen, Oliver, & Oxman, 2006). Further, when patients had been involved in developing written information, twice as many considered the material to be easy to understand compared to when they had not been involved (Chumbley, Hall, & Salmon, 2002). However, no studies were found with patients actively involved in the initial design of material – only as consultants in later stages. Even when guidelines and toolkits on how best to present text in a healthcare context were used, McCarthy et al. (2012) found that these guidelines did not completely consider the patients’ perspectives. This meant that text and illustrations had to be considerably changed after consulting the intended readers, i.e. the patients. When using participatory design in the development of web-based information for pregnant women with type-2 diabetes, the method proved to be effective in ensuring that the users’ needs and wishes were included from the beginning, but it was also time consuming. Input from both clinicians and mothers with experience gave invaluable insights to the team (Linden, Berg, & Sparud-Lundin, 2012). Using a well-defined process model is also recommended for collaborative working, such as co-design (Scariot et al., 2012).
Power, knowledge and reflection
Power and knowledge and how they relate can be seen from at least three views, firstly: knowledge as resources owned by the powerful experts and transformed to the powerless as the truth yielded by objective research; secondly: knowledge as controlled by the powerful, where the powerless are sometimes invited to produce and act upon the set agenda of knowledge creation; and thirdly: emphasis on shaping consciousness of the agenda where participation in knowledge production in itself builds greater awareness and self-consciousness of capacities for action (Gaventa & Cornwall, 2015). This third take on power and knowledge can be related to the development of action research in South and Latin America with Freire’s (1970) process “conscientizacao”, used to liberate awareness of oppressing dimensions. In this process, the stakeholders are given opportunities to be responsible subjects by using their reflections in dialogue with the researcher. Beside this, the systematisation of experience methodology was also developed, with an endeavour to create a new relationship between theory and action, where knowledge was produced from the practice itself. Both originate from a desire to challenge social injustice and develop people’s capacity to pronounce their world and exercise the right to have their say (Streck & Jara Holiday, 2015).
In participatory design, as well as in other action research methods, ethics can be problematic and must be considered throughout the process (Boser, 2006). In particular, the risk of asymmetrical patterns of power must be documented and transparent in all stages of the iterative cycle. By doing this, protection and evaluation of the intended democratic knowledge-sharing and generating can be facilitated. Eikeland (2006) expresses this ethical question as a transformation from “How should we relate to them” to “How should we relate to each other?” and points out that action research is often torn between externally based academic research and the internal indigenous standards. By considering the three views on power and knowledge in the reflection cycle and also promoting “conscientizacao”, tensions and negotiations will be regarded productive driving forces in action research. Both awareness of asymmetrical patterns of power and the possibility of all stakeholders’ knowledge need to be shared and enhanced in the project. Thus, action research (Bradbury-Huang, 2010) encompasses an endeavour to achieve reflexivity, described as “the extent to which the authors explicitly locate themselves as change agents”. This means that the researcher must have a plan, not only for action, but also reflection; i.e. be reflexive about the change process and the researchers’ impact on the intervention. Levin (2012) describes it as action being followed by reflection, as reflection has to be accompanied by action and the rigor of action research depending on the capability to both solve problems but also scrutinize the experiences gained in order to communicate new knowledge. According to Johansson and Lindhult (2008) there are two orientations of action research influencing power and reflection: a pragmatic one which is more suited to contexts dealing with immediate action where power to act is a desired outcome, and a critical one focusing more on critical thinking and reflection, aiming at unveiling unequal and invisible power relations. These orientations can also be seen as a north and south tradition, where north is more pragmatically problem-solving oriented, possibly due to often being performed in principally democratic contexts such as Scandinavia and North America. The south tradition orients from South America, with strong connections to Freire (1970) and the emancipation of underprivileged groups (Johansson & Lindhult, 2008; Streck, 2014). North (pragmatic) is thereby more focused on participation, exchange and collaboration, whereas south (critical) gives more room for dissension and reflection. This study can relate to both since it has a pragmatic purpose (developing a new material), but also a desire to promote a person-centred approach in the process, hence emancipating the patients’ knowledge in a hierarchical structure such as health care.
Aim
The aim was to present the negotiations derived by areas of tension when stakeholders were involved as co-designers in the process of developing patient education materials.
Study context
This study utilizes the Swedish PINCORE (Person-centred Information and Communication in Colorectal Cancer Care) project. The aim of the PINCORE project is to investigate whether tailored information material and person-centred communication for patients diagnosed with colorectal cancer undergoing elective surgery can enhance their preparedness and improve the patients’ recovery following diagnosis and initial treatment. The study was approved by the Regional Ethical Review Board in Gothenburg (Ref. No. 545-10).
In the care and treatment process for serious conditions such as colorectal cancer, a lot of information is shared between patients and clinicians. In the guidelines for enhanced recovery after surgery, preoperative counselling is an essential part for successful results (Gustafsson et al., 2012; Nygren et al., 2012). This evidence-based best practice protocol states that personal counselling, leaflets or multimedia information about the procedure, with particular stress on what tasks the patients can do themselves before surgery and during recovery plays a significant role in decreasing complications.
Person-centred care principles build on the belief that a patient is not reduced to their diagnosis but is the person they are: their context, their history, their family and loved ones, their individual strengths and weaknesses (Leplege et al., 2007). Narratives should be actively used and, along with the patients’ capacities, be transformed into a partnership (Ekman et al., 2011). Participatory design adheres to a constructivist paradigm, with emphasis on knowledge-making through interaction. It also strives to describe stakeholders’ tacit knowledge so that it can be used to design new tools that can empower users (Spinuzzi, 2005).
The combination of working in collaboration with different stakeholders (patients, clinicians and designer) from an early design stage thereby seems a fruitful method for developing person-centred, suitable, comprehensible and readable materials. In the enhanced recovery after surgery guidelines (Gustafsson et al., 2012; Nygren et al., 2012) it is stated that dedicated preoperative counselling, including written material, can only be beneficial and not harmful. The recommendation grade of this is high even if the evidence level is considered low. The PINCORE program and this study in particular fill some of these knowledge gaps.
Method
Participatory design
Participatory design (Spinuzzi, 2005) was used complemented by a process map developed by Elwyn et al. (2011). This process map provides a systematic tool to describe and structure the work and reflect during the process. It was originally designed for web-based support programs, and was therefore adapted to fit the process of developing printed written information materials.
In participatory design, the outcome typically consists of designed artefacts, work arrangements or work environments cooperatively designed in an iterative partnership with researcher and participants. This is also in line with person-centred care (Ekman et al., 2011). The method is suggested to follow three basic steps: Initial exploration of work, Discovery process and Prototyping (Spinuzzi, 2005).
Emphasis is also on coping with conflicting interests, where there needs to be a negotiation between how a current situation and a future vision can complement each other. It is also concerned with how the researcher can deal with the ambition to focus on other people’s knowledge and ideas instead of his or her own (Steen, 2013). Conflict is therefore seen as a source of development and not a negative in the research process, and participants’ co-interpretation of the research is an essential part of this process. Tacit knowledge from stakeholders is used in a constructionistic paradigm in which a goal can be achieved when researchers use this knowledge in conjunction with their own academic knowledge.
During the process, data were documented by audio-recordings, field notes and e-mails.
Work process
The process of developing a new patient education material started in autumn 2012 and lasted approximately a year. A flow-chart of the work process is presented in Figure 1.
Flowchart of work process.
Stage 1: In the initial exploration of work, the researchers designing the study met the stakeholders to make a “needs assessment” (Elwyn et al., 2011). This was described in a protocol document, which was also used as a design for the study, containing background information, the rationale for developing the material and the process and methods for collecting and analysing data.
Five focus groups were conducted with former patients (six women and nine men) operated for colorectal cancer within a year at a University hospital in Sweden (Smith et al., 2014). Participants were asked to share their experiences of how they considered written information to be helpful and how they preferred it to be designed. They were also asked when and how they would like it to be delivered in the colorectal cancer care process. Two members of the research team participated, one as a discussion leader (FS) supported by another team member taking notes. All group sessions lasted two hours and were audio recorded and transcribed verbatim. These groups met once and were not further involved in the process of developing the new material. In addition to known quality aspects of material, the results identified new subject areas: general and personal care, personal implications, Internet, significant others, accessibility to health care, usability, trustworthiness and patient support groups (Smith et al., 2014). These areas, in connection to the categories content, language, organization, layout and typography, illustrations and learning (Hoffmann & Worrall, 2004) were used in the Protocol document as a baseline and ideal for what could constitute design and subject areas of new material for patients with colorectal cancer.
After conducting a literature review, the laws and guidelines regarding written information for patients in Sweden were examined and a literature scope was performed as to how best to produce and present written information. This led to an evidence synthesis, with relevant literature being identified in the process and added to the evidence synthesis as appropriate. In this way, literature was treated as data and used to define the extent to which the emerging theory can be generalized (Dick, 2011).
Overview of included stakeholders.

An advisory group was formed to support the project management group (Table 1). This group consisted of two RNs, one working in the surgical ward for colorectal cancer and one working in the outpatient clinic as a contact nurse for patients with colorectal cancer. Three former patients treated for colorectal cancer were included: one young woman, one recently retired woman, and one retired man. These individuals were asked to participate as they had expressed an interest in written information in previous studies. Each group member was interviewed individually, met together in a workshop and had e-mail correspondence throughout the process.
All five members of the advisory group were individually asked to give their thoughts, feelings and preferences regarding what information should be given at four points in time in the colorectal cancer care process. The four information time-points identified as most crucial in the five focus groups performed in stage one were: medical investigation before diagnosis is set, being diagnosed with colorectal cancer, preparing for surgery and going home. Responses were documented in note form and reflections made and discussed within the project management group and advisory group. These were then compared (Dick, 2011) with data and results from the five focus groups, after which a first draft was made for new material in four parts (chapters).
Stage 2: In the discovery processes, the interaction between researchers and users was intensified (Spinuzzi, 2005). A workshop with the project management group and the advisory group was conducted concerning the first draft. Since one of the former patients in the advisory group had volunteered to be active in the writing process, the drafts were handed over for suggestions as regard text and person-centred application. This was part of the participatory design methodology described as continual participation, where users should be involved repeatedly and not only as advice-givers, but also as co-designers (Spinuzzi, 2005). In this case, the participant’s knowledge consisted of having experience both as a professional writer and as a patient who had undergone colorectal cancer treatment. The new suggestions for the information materials were discussed within the project management group and the advisory group and compared with an earlier draft, after which a second draft was made.
A scientific reference group was then formed (Table 1), the members of this group having been invited because of special interests or expertise, or because they represented key relevant organizations (Elwyn et al., 2011). The members of the scientific reference group met with the other process groups in a workshop where they had been asked to give comments on the material from their specific area of knowledge. This workshop was audio-recorded and notes were taken during the discussion. From this, a new draft was made in collaboration with the project management group and the writing member of the advisory group. This draft was then changed according to comments and negotiations of conflicting interests within the groups (draft 3-6).
Stage 3: The prototyping design stage involved a designer with a Masters in transdisciplinary design (Table 1) who had previously specialized in how the design of objects and visualizations influences understanding, communication and behaviour in health care. The designer made suggestions for the design and illustrations, which were then viewed by the process groups. Eight new stakeholders (patients) were also asked for their opinions on the design and illustrations. These patients were evenly distributed in the four stages of the colorectal cancer care process used as chapters in the material (investigation, diagnosis, surgery and rehabilitation) and the interviews took place either on the ward or in the outpatient clinic. Changes were made several times in negotiations with all the stakeholders involved in the process, after which a final draft was then printed to be tested in an intervention study as part of the PINCORE project.
Analysis
Throughout the process, constant comparative analysis was applied as an action research cycle, considered the “data engine” (Dick, 2007, 2011). It was used on all sets of data to inductively find agreements and disagreements which needed to be negotiated. The process can be viewed as dialectic, using apparent disagreement to generate agreement at a deeper level.
Data (audio-recordings, transcriptions, field notes and e-mails) were compared with each other and added to the study documentation in the process. Overlaps between data were noted as agreements or disagreements. Disagreements also included when the same topic was mentioned but incompatibly. Where there was agreement, exceptions were explored and if found, treated like a disagreement. Where there was disagreement, explanations for these were explored and the disagreements were negotiated within the process groups.
The three basic steps in the participatory design methodology were applied, integrating the Elwyn process map (2011) accordingly. Throughout the whole process, the cooperation, curiosity, creativity, empowerment and reflexivity (Steen, 2013) of the stakeholders were reflected on by the project management group. Particular focus was given to how the researchers in the project management group discovered and negotiated conflicting interests and areas of tension arising in the process.
Results
Overview of agreements, disagreements and negotiations.
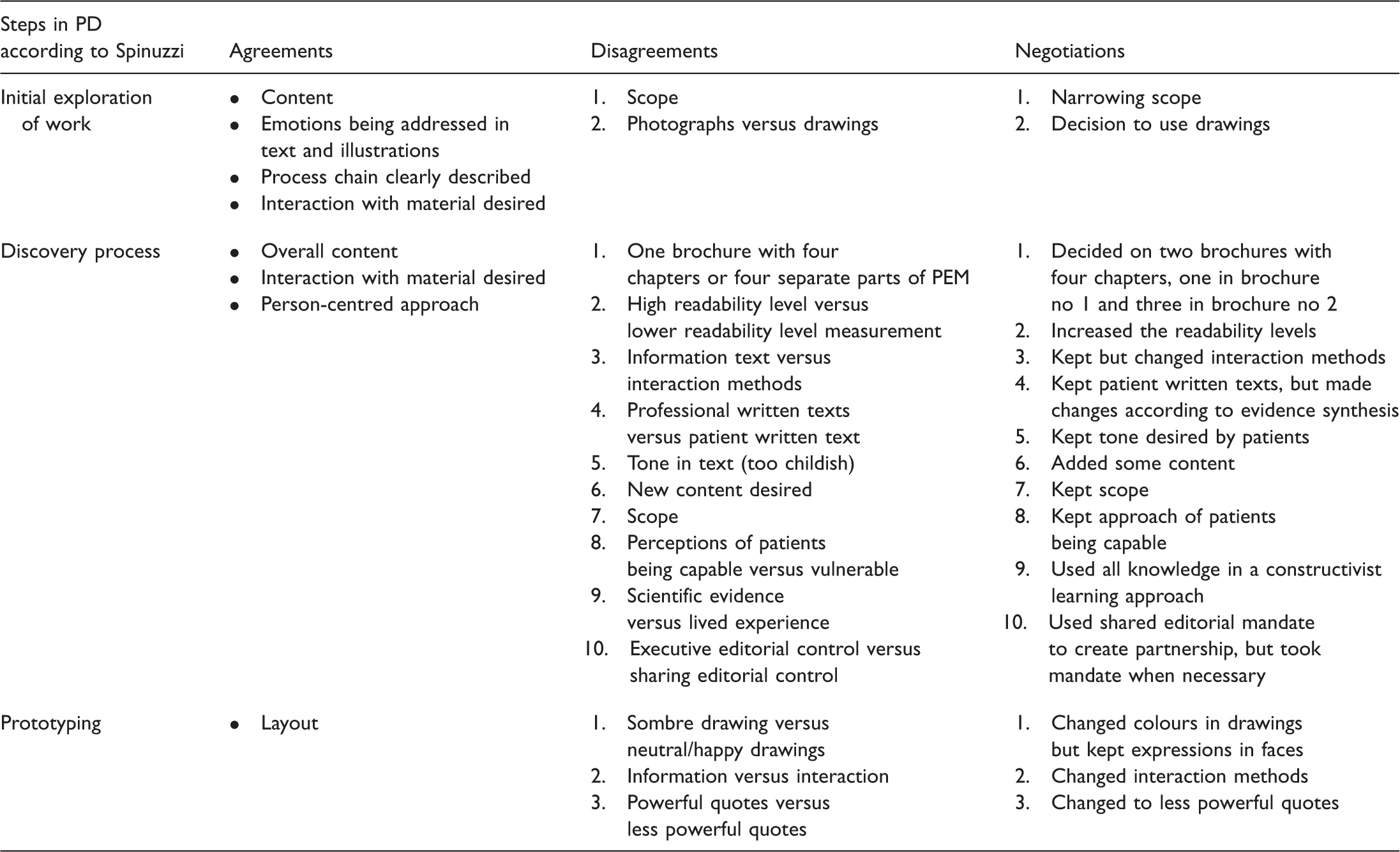
Mandate to decide
During the first stage of the process, the project management group was given the mandate from the rest of the research group within the PINCORE project to develop the new material. How this mandate was interpreted became a source of insecurity within the PINCORE group at certain stages of the process. Since the intended material was a part of a larger intervention, its development was closely related to the development of the whole intervention, which aimed to promote person-centred communication with patients before and after surgery. Members of the PINCORE research group were also part of the scientific reference group from their specific area of expertise (Table 1). This became somewhat problematic as they participated in the whole intervention design. According to the Elwyn protocol, the project management group has editorial control and makes the final decisions on content specification, design and testing phases.
One of the participants in the advisory group was a former patient who also worked within the field of writing information materials. This person volunteered and tried very hard to use a different approach in writing to enhance person-centred expression in the text. When draft number three was presented to the scientific reference group, several stakeholders of this workshop rejected this style of writing, which was different from their expectations. Moreover, in certain aspects it was not in congruence with the evidence synthesis on how to best write information for patients. The project management group had to use its editorial mandate to try to incorporate both the proposed text with suggestions made by the scientific reference group, but in so doing they lost the patient as a co-writer as he felt he was being resisted in his attempt to be innovative in the text. This was expressed in an e-mail to the project management group: “At the workshop, there was a lot of: we can’t say that, we can’t write that. I’m not saying that’s wrong, but it tells me that all the guidelines and demands on what and how to write may lead to a far less person-centred text than was the intention from the beginning. It also seems to be a very hierarchical group, with you at the bottom and the professor at the top.”
Although the PINCORE research group largely questioned how the patient co-writer had decided to go about his mandate, they felt uncomfortable criticizing him because he was a patient and had volunteered. Nevertheless, it was never promised that the patient’s text would be immune to revision, and he gave us permission to use whatever we wanted from his contribution in the final production of the new material. The final draft was also sent to him and his opinions were brought to the process protocol. Upon reflection, he felt the task had been difficult to complete, and that he had been trapped in a traditional way of presenting written information. Nevertheless, his feedback was positive overall and he was glad to have contributed to the process.
Designing evocative illustrations
A few specific issues of disagreements occurred during the work process, illustrations clearly being the biggest of these (Table 2). During the initial exploration of work, members of the advisory group inspired the project management group to use illustrations as stimuli to express emotions that can arise when a patient is diagnosed and treated for colorectal cancer. Within the advisory group there were different opinions as to how these illustrations should be presented, with younger participants wanting photographs they could relate to while older ones preferred drawings. Enhanced by the knowledge gleaned from the evidence syntheses, it was agreed that any drawings used should be age-neutral.
The stakeholders had different opinions on how the design of the illustrations was best suited to the aim of the material, and it became obvious that art is not only a subjective matter but also a strong trigger for emotions. Throughout the process, negotiations took place, as exemplified by the following exchange of expressions: “The drawings are too sad – it might make it feel more scary. You have to feel hope. The drawings are very nice and you understand what they want to convey, but they need to be a bit brighter” (Patient). “I like the expression. Nice. Gives a hint of being something serious. Could be important as a counterbalance for the staff who meet people with cancer everyday” (Researcher). And “You know, it is frightening and upsetting to get cancer, and you
The designer and the project management group consequently struggled to find the right amount of emotion in the illustrations and to agree on whose mandate it was to decide when a drawing needed changing or not. Drawings of people with emotional expressions on their faces were used in the final version, and it was agreed that these expressions would be subtler but that the colour would be brighter than the first versions. When the stakeholders (eight patients) were shown the illustrations in the latter part of the design phase (Figure 1) they all said they liked the idea of the emotions being expressed, and were happy with them now.
Scientific evidence and professional knowledge vs. individual patients’ lived experience
Throughout the process there was tension between the researchers’ wish to rely on scientific evidence as the most important source of information, the clinicians’ preconception of how patients should be involved and informed, and the lived experience of the patients. On the one hand, the patients were not fully aware of the latest scientific evidence on how to best present written information and did not know what guidelines and legislation guided the clinicians’ information. On the other hand, the researchers and clinicians sometimes struggled with their role as co-designers, which equally impacted on the end result. In all stages, the project management group had to reflect on this matter and tried to incorporate all types of knowledge into the creation of the material.
Although most of the topics were suggested and written by patients, the clinicians and researchers regarded some aspects as less valuable for patients, thereby giving them less of a mandate in knowing what was important to them. Examples of this were emotions, sexuality and “what can I do myself to feel better”, something that had already been discovered in the evidence synthesis from previous studies. Patients felt these issues were not sufficiently expanded upon and wanted to know more about them. Throughout the process, the clinicians gave the impression that they were used to knowing what was best for the patients and wanted to protect them from what they considered too much to deal with in a difficult situation. The project management group had to constantly remind themselves and the rest of the process groups that tacit knowledge and lived experience have just as much validity as their research-based knowledge and clinical experience. An example of conflicting interest is highlighted in the sentence: “You are allowed to eat whatever you want, and it is not dangerous to eat.” The word ‘dangerous’ was something that the designer specifically thought inappropriate but that the patients approved and wanted to be included. As a result, the sentence retained its original formulation.
Expression and form of language in text
The text was also a matter of disagreement within the group. All members of the research group were not only members of the scientific reference group but also experienced writers of both scientific literature and popular texts and thus suggested several changes to the text. The project management group also asked for comments on the text, thereby somewhat stepping out of the Elwyn-protocol, since the scientific reference group was only supposed to bring their specific area of expertise to the process and none of the members were experts in text production (Table 1).
The project management group took great effort in their editing to ensure a use of language that would be deemed appropriate according to the evidence synthesis protocol. Health literacy was also considered throughout the writing process by using the patients’ tacit knowledge of how and when information should be presented in a turbulent life situation. When the clinicians in the advisory group – especially nurses – read the text, they thought the language was too simple or even childish. Spontaneously, they wanted to use more medical and colloquial expressions, and were not in favour of the different style of writing, sometimes commenting that it was disrespectful to patients’ ability. “The language borders on being childish, we are almost treating people like idiots writing like this!” (Nurse in workshop). Further, it was decided that the medical text written by the surgeon had to be changed, since this too had a medical rather than a popular expression. Moreover, suggestions made by the research group were sometimes not in line with the evidence synthesis protocol on how to write information text, and the project management group spent several hours trying to negotiate around the text to take in the preferences of researchers and clinicians, as well as that of the patients.
The patient in the advisory group who was a professional writer had strong opinions on the matter of using readability measures, and thought it old-fashioned. It also led to shorter sentences, which made the text less fluent and interesting to read. As a result, the project management group changed their initial goal of using very simple text for high readability.
When the designer was given the text, she initially found it difficult to add pictures and suggested several changes to the text. As with the clinicians’ suggestions, however, some of the designer’s suggestions were not in line with the evidence synthesis or with the patients’ wishes. Since the designer was not used to the surgical context and pointed out things that were unclear, many of her suggestions were nevertheless considered valuable and used. The text was also sent to a language specialist and minor editorial changes were made.
The use of patient quotes as inspiration
Using quotes to inspire readers to express their own feelings and concerns was one way of promoting a person-centred approach. The quotes were picked from the initial five focus group interviews (Stage 1), and depicted the feelings often expressed in the four time-points of information transformed into the chapters of the material. The designer and the project management group did, however, have conflicting opinions about which quotes to use. For example, the designer considered the initial quote chosen in connection with waiting for test results to be too strong since it contained the phrase “living in terror”. After consulting the rest of the process groups, this quote was exchanged for another, less powerful one. The desire of the project management group to use strong quotes was thereby renegotiated to make the text less frightening, and the quote used in the final draft was: “It was hard…. Somewhere in the back of my head I knew that there could be some bad news.”
Reader interaction
From the very beginning, the project management group had the intention of making the text as interactive as possible. The idea was that this would create a person-centred approach to support patient preparedness, where the patient is encouraged to recognise his or her capabilities to overcome various obstacles and decrease distress. When first presented to the advisory group, participants had various preferences for how this would be applied in the text. The patient involved in the writing process wanted more clarity on what the patients needed to do and advocated a clear push for the reader to take action. “One of the most important missions for such information is to make the patients realize and accept that they are active partners in the process and should not see themselves as just passive victims” (Patient during needs assessment). Another patient was at first provoked by the suggestion that the patients’ responsibility throughout the process should be clearly stated, but after reflection, changed her mind. She saw this as a way of incorporating patients in the team and making them feel more empowered. “Interaction is important; it makes you as a reader take responsibility for what you have read to take necessary actions” (Patient during needs assessment).
In the needs assessment, some of the patients in the advisory group had expressed a strong wish to be better helped to express feelings after being diagnosed with cancer: “I want the staff to say: I care about more than just curing your cancer, that they say that I’m a person, not just a patient” (Patient during needs assessment). The patients felt that, particularly after discharge, there was an enhanced need for social support for those who lived alone. They felt this issue was absent from the discussions raised by the clinicians during the process and that this was an area for improvement in the new material.
In the workshop including scientific reference group participants, many commented on how much responsibility could be transferred to the patients from an ethical point of view. After this workshop, there was quite a lot of negotiation in the project management group regarding the patients’ and the clinicians’ comments, particularly regarding how these were congruent with the evidence-synthesis protocol, in which interaction was clearly pointed out as important for improving the material.
Content, structure and scope of care process
The process groups mostly agreed on the topics to be included in the material. However, in the latter part of the process, when the scientific reference group became more involved, additional topics and areas of content were brought up and negotiated. Mostly, it was only a matter of adding more content and then agreeing within the groups that this had been missing, but some of the members wanted more specifics about their own area of expertise. This was not always included, since it may have become disproportionate compared to other level of details.
The structure of the material was changed several times during the process, rarely because of disagreement, but more frequently the result of discovery after every change made to the draft. The ambition to keep the material as short as possible turned out to be a difficult task. Both stakeholders (patients and clinicians) shared this ambition, but when it came down to omitting certain areas, there were a few disagreements. Specifically, possible risks and side effects was something the patients had requested but felt intimidated by when confronted with a detailed description. “I’m not sure I would have turned up for surgery knowing all these risks …” (Patient after reading about risks and complications). The surgeon in the project management group had directives from the National Board of Healthcare to give better information about this, and wanted the text to be fairly long. Several drafts were made and negotiated to maintain readability and suitability for the patients.
The scope of the material was also negotiated as regard when the process should start and end. Some members of the advisory group wanted the whole follow-up and possible chemotherapy treatment to be included, but the project management group wanted to leave this out and concentrate on the surgical process alone. This was also negotiated and agreed upon.
Usability in clinical work
Originally, the project management group intended to make four separate chapters that would build on the previous ones, as the needs assessment had revealed that giving the information all at once might be too much. However, some patients wanted all the information from the beginning so they could decide when to read what, and in what order. During the process, a practical issue also arose in having too many parts of the text to hand out. There was a risk of not having an updated version or not having all four separate parts printed at the clinic to hand out at the right time. It was also considered inappropriate to distribute only one part, since the patients were actually not diagnosed with cancer until later in the process. For these reasons, the decision was made to divide the material in two parts – one to be delivered during the first stage of investigation, before cancer diagnosis had been established, and one part with three chapters: diagnosis, surgery and recovery. In this way, patients could choose what to read and when, and the word ‘cancer’ was not used until part two.
During the workshop with the scientific reference group, the manager of the surgical department raised the question of how the new material would actually be used by the professionals and patients in “real life”. “It will take a lot of time and engagement to make this work. I know – we have tried many times before to improve information and communication and failed” (Member of scientific reference group in workshop). She was concerned about the model being too time-consuming and that it would be viewed as something new and suspicious within the workgroup. This was not only negotiated both within the process groups, but also on a different level, when the complete intervention was discussed. In a parallel process, it was decided to perform workshops with the staff to process how the new material could support patients in preparing for surgery and recovery and thereby save time instead of consuming time.
Discussion
The results reveal that the predominant areas of tensions focused on power (mandate to decide), organization (content, structure and scope of process, reader interaction), content (designing evocative illustrations, types of knowledge, expression and form of language in text, the use of powerful patient quotes as inspiration) and application (usability in clinical work). These areas of tensions appeared and reappeared throughout the work process, varied in intensity and had to be consistently negotiated through dialogue with different stakeholders and/or literature.
During the process, a number of tensions became visible, but were consequently defused through negotiation. This can be interpreted as an attempt by the project management group to be open and willing to work with all included stakeholders and trying to promote “conscientizacao” (Freire, 1970) whilst also reflecting on the process and holding on to the design goal. This can also be seen as a combination of the north and south perspectives on action research, but with an upper hand of the pragmatic, north perspective. Johansson and Lindhult (2008) state that there is no rule against eclectically mixing the two, here probably presented as pragmatic-critical orientation. Producing education material in the context of health care with multiple stakeholders was not an uncomplicated task, a result supported by Braye and McDonnell (2013). In this paper, one of the most palpable areas of tension was power and the negotiation regarding balancing the editorial power towards lived experiences of stakeholders and between stakeholders. According to Elwyn et al. (2011), the project management group has exclusive editorial power to make the final decision about the new design product, but as Freire (1970) emphasises, this is not about producing something for the people or without them but with those who are concerned. This is also stressed by Eikeland (2006) and Scariot, Heemann, and Padovani (2012). For example, in our study, it became clear that the researchers were more familiar with maintaining distance to patients’ views, and principles in research ethics were sometimes referred to as a way of protecting patients from being harmed while they were participating in the process. The clinicians also emphasised patient safety, expressing a desire to avoid hurting them. We discovered that it was difficult for both clinicians and researchers to abandon established ways of working with patients, a finding that is described by Jacobs (2010, p. 377) as “the clashes between empowerment, academic quality and practical usefulness.” We also found behaviour that showed traces of old models, i.e. working for or without patients, and a tendency to withdraw to familiar routines, tasks and roles and thereby protect themselves from the anxiety of working in different power structures. These behaviours among professionals are well known (Minkler et al., 2002) and also strongly linked to the three views of power and knowledge (Gaventa & Cornwall, 2008). Health care professionals, and researchers in particular, are used to being in charge and being more knowledgeable than (in this case) the patients. According to Freire (1970), this manner can be explained by the clinicians’ and researchers’ (oppressors) perception of the patients (the oppressed) as objects. An object waits for instruction and direction while a subject is a person who can reflect and act. The project management group consequently had to work hard to facilitate cooperation between patients, clinicians and researchers and to remind all stakeholders (including themselves and the patients) that patients are not passive objects but active subjects who have the capacity to reflect on and make good decisions. This is an activity in line with how person-centred care is conducted (Ekman et al., 2011) but not a characterising feature in discourses identified in existing materials (Öresland, Friberg, Määttä, & Öhlen, 2015). Despite emphasising this, our project lost one patient in the work process, possibly due to power structures that were not resolved from both perspectives: he was a professional writer with strong views on text, and the research group not prepared to completely accept his knowledge both as a writer and a patient. Aas (2014) and Weng, McDonald, Sparks, McCoy, and Gennari (2007) nevertheless see negotiating iteratively during the design process as helpful and an important factor for the adoption of a new system. They report tensions are driving forces for development if made visible. As a result, the project management group learned to surrender some of their editorial power, thus stepping aside from the recommendation of the Elwyn et al. (2011) protocol. Nevertheless, we still consider this protocol useful in future research as a theoretical frame for developing material in the context of health care, but the project management group’s editorial power should exist in cooperation with stakeholders. Having a structured process map was also helpful in keeping track of the process, as recommended by Scariot et al. (2012), even while it is being changed during the action research cycles. Further, in regard to the balancing of power between stakeholders, we would like to suggest future research increases the number of patients in working groups and really emphasises them as capable individuals contributing to the design process. Having the designer included earlier in the work process may have sped up the design phase and added valuable knowledge earlier, but then the process map would not have been followed.
The appearance and reappearance of negotiations may be interpreted as the project management group trying to empower, i.e. to share power with the stakeholders in all steps of the work process, from initiation to design and production as well as utilization. According to Bradbury-Huang’s (2010) description of “good action research”, one thing to consider is how the project reflects or enacts stakeholders’ values and concerns for the relational components of research. By using the participatory design method and following the Elwyn protocol (2011), the project management group of this study could promote the collaboration and work process but it was the stakeholders who led it forward. It is well known that stakeholders can be used in the continuum from consultant to full co-researcher (Rudd & Comings, 1994; Steen, 2013). However, when it comes to patients, they are most often only used as consultants when developing materials in health care, while the clinicians and researchers are included as full co-researchers (Buckley et al., 2013). In this study, however, the patients were seen neither as consultants nor co-researchers but as co-designers, and this put them in the middle of the continuum. The reason for this was that the project management group collaborated with patients in the phase of the needs assessment, writing process and creation of the design but did not ask them how they wanted to improve care before and after surgery or whether they would like to be actively involved in the analysis process, although this issue frequently came up in the different stages of the action cycle. The patients were nevertheless continually informed of the progression of the analysis and their comments and suggestions were recorded and kept as data.
Data in this present study were generated by focus group interviews, workshops, e-mail, individual interviews and review of literature. The common thread of the process was dialogue, which was used to pledge all stakeholders’ opportunity to rename the world. This is in line with Freire (1970), who commented that humans do not grow in silence, but in words, work, reflection and action. In this study, however, stakeholders sometimes recommended suggestions that were the opposite of the scientific evidence in our literature scope. For example, one of the patients wanted to use photographs instead of drawings and the project management group had to negotiate with this stakeholder. By doing so, we started to balance her point of view, i.e. “self-absorption” (Steen, 2013, p. 953) and our protocol document, and during this act of balance she started to communicate her understanding that other patients might find photographs to be too detailed and interpretative. The negotiation therefore led to the use of drawings instead of photographs in the final designed product. As a result, we learned the power of dialogue and how to use our “virtue of cooperative curiosity” as stated by Steen (2013) but also that using dialogue is a time-consuming approach, an experience in line with the action research study by Goins, Garroutte, Fox, Dee Geiger, and Manson (2011).
The contribution to both participatory design and person-centred care can be seen as a fusion used in a practical setting (such as developing material) which seemed to enhance both perspectives. Using scientific evidence from both patient participation and medical and other guidelines as well as tacit knowledge when negotiating during a development process may enhance the possibility of working in partnership and not only in a patient-provider encounter. Health care has a strong framework of regulations and traditions but introducing new ways of collaboration in a research context may contribute to both theory development and clinical development, something that has been done successfully in other areas of participatory research but not found in the development of health care materials. The same research reveals issues similar to those we have found, namely that action research is time-consuming (Linden et al., 2012), staff are insecure about viewing patients as capable (Bengtsson, Kasperowski, Ring, & Kjellgren, 2014) and shared involvement is possible between stakeholders through synthesizing conflicting views (Berg et al., 2014). This needs to be addressed and further researched.
By using action research methodology person-centred care philosophy can be transformed into actionable knowledge (Coghlan & Brannick, 2014) and presented in a transparent way. It can also be seen as a way of actively using the narratives of both patients and staff, uniting all stakeholders’ capacities in a partnership and documenting this, thereby adhering to Ekman et al.’s (2011) description of person-centred care and McCormack and McCances’ (2010) call to develop creative strategies for evaluating person-centred care in practice. The risk of bias is minimized by the researchers taking a focused and structured stance not only in following the process protocol (Elwyn et al., 2011) but also in reflecting and describing the tensions and how they were negotiated between stakeholders, mainly from a second-person perspective encouraged in action research methodology (Chandler & Torbert, 2003). Reflexion is a key choice-point in promoting high quality action research (Bradbury-Huang, 2010). However, the methodology used in this study has more emphasis on reaching consensus and describing the process. Alvesson, Hardy, and Harley (2008) highlight a risk of “reflexion becoming a dead end rather than a route to more thoughtful and interesting research” if it is mystified instead of used to show rigour in research.
In this way, the focus of this study on tensions can be taken as an expression for considering critical reflection on how the development process evolved.
The project management group tried to take steps to introduce the third person perspective, here evidence on how to present written information and the medical guidelines about the specific medical procedures (i.e. colorectal cancer surgery) to all stakeholders involved. When necessary, this was discussed within the groups, particularly when it was not in congruence with the stakeholders’ beliefs. Even if reflexion is clearly elaborated on, the community the researchers come from may colour their view of the “truth” and how and on what is being reflected upon (Alvesson, Hardy, & Harley, 2008). All the researchers came from the health care sciences, and one of the researchers (FS) was also knowledgeable in colorectal cancer care and may have had preconceptions of which she was unaware. Since the other researchers (CW, JÖ) did not have this previous knowledge, this possible bias was seldom noticed but critically reflected upon. Further, the third researcher (JÖ) was not involved in the project management group but had previous experience in action research, which contributed to the critical stance in the process. However, the reflexivity here may not have been as critical as it could have been, partly due to the method chosen (Spinuzzi, 2005), and partly due to the pragmatic goal of designing a product within a set time limit. This meant that workability may have been established prior to reflexion, but since this was the reason for the methodology and the process was transparently described, this study can nevertheless add valuable insight and knowledge to others, particularly on tensions related to power.
Conclusion
Using participatory design and person-centred care in a fusion when co-designing a new education material in the context of health care with stakeholders such as patients, clinicians, researchers and a designer was productive but time-consuming and sometimes challenging. Negotiated areas of tension appeared and reappeared during the process and were predominantly related to power, i.e. mandate to decide, organization; content, structure and scope of process, reader interaction, content; designing evocative illustrations, types of knowledge, expression and form of language in text, the use of powerful patient quotes as inspiration and application; usability in clinical work. These tensions functioned as a productive driving force, which actually improved the design process. Thus, a critical sensitivity towards such tensions and using all stakeholders’ knowledge throughout the design process might be critical for participatory design researchers. Often, materials have been produced in a power setting with the clinicians, and sometimes researchers, as the ones with the both the right and knowledge to develop materials without involving patients. This has sometimes led to inappropriate rather than person-centred materials. Constant reflection on democratic knowledge-sharing related to power is therefore important in achieving success, and the process needs to be transparent for all stakeholders in order to make them feel like partners and co-designers, and not just consultants. Learning to manoeuvre between existing evidence and creating new evidence in on-going knowledge-sharing was found to be elaborative. The findings of this study can benefit both patients and other relevant stakeholders in the health care system for the development of written patient education materials.
Footnotes
Acknowledgements
Our sincere thanks to all stakeholders involved in the process. We would also like to thank Dr. Svante Lifvergren for leading the review process of this article. Should there be any comments/reactions you wish to share, please bring them to the interactive portion (Reader Responses column) of the website: ![]() .
.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the University of Gothenburg Centre for Person-centred Care (GPCC).