
Abstract
Introduction and Objective:
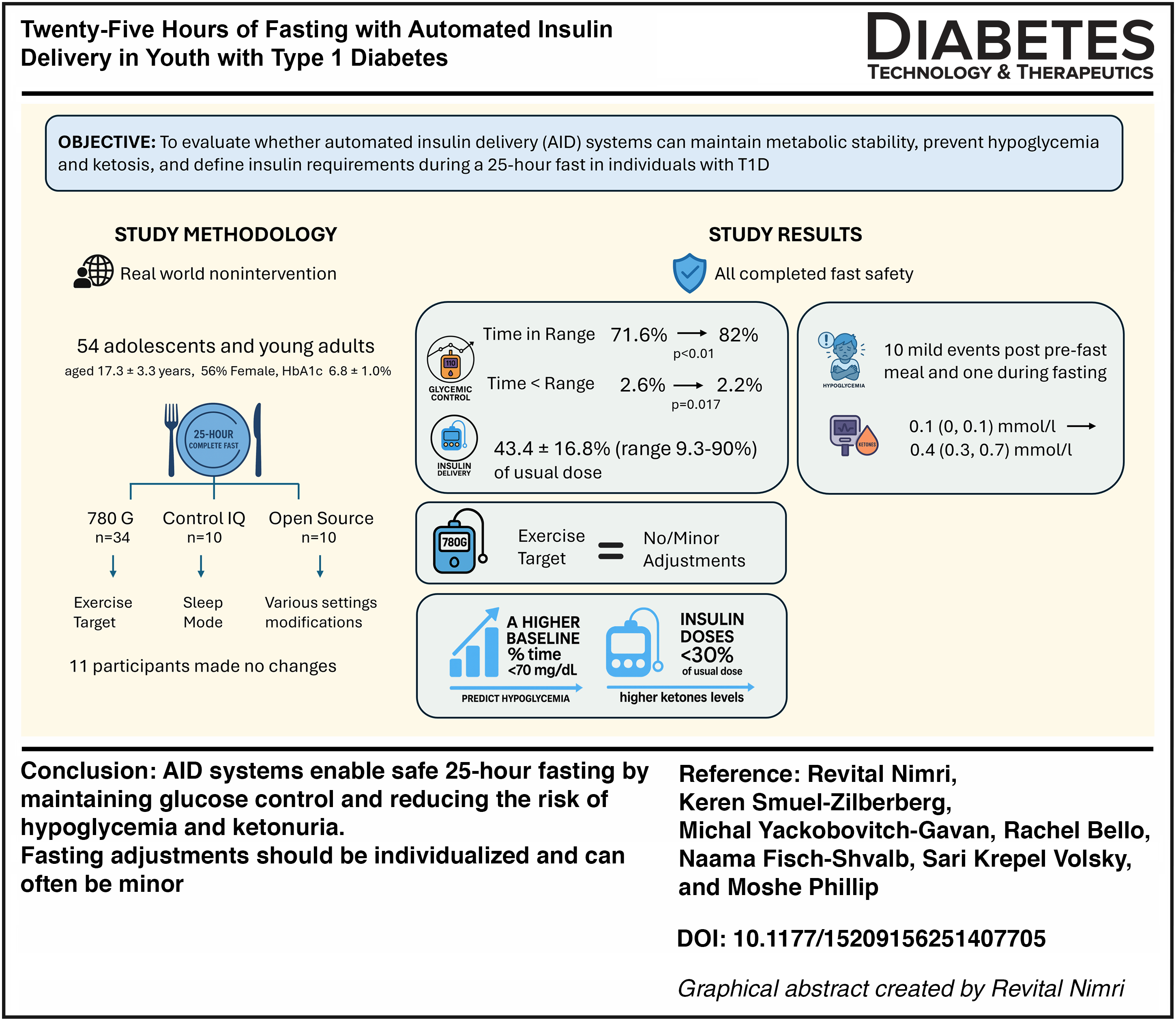
Fasting presents unique metabolic challenges for individuals with T1D. The 25-h Yom Kippur complete fast provides an opportunity to evaluate whether automated insulin delivery (AID) systems can maintain metabolic stability, prevent hypoglycemia and ketosis, and determine basal insulin requirements during prolonged fasting.
Methods:
This real-world, noninterventional study included 54 adolescents and young adults with T1D (mean age 17.3 ± 3.3 years, HbA1c 6.8 ± 1.0%). Participants used MiniMed 780 G (n = 34), Control-IQ (n = 10), or open-source AID systems (n = 10). Common system-specific adjustments included setting a 150 mg/dL exercise target, activating sleep mode, and modifying basal or glucose targets, while 11 participants made no changes. Ketone levels were measured after the 25-h fast and a routine overnight fast. Analyses compared glucose and insulin across fasting periods and different 780 G settings and assessed predictors of hypoglycemia and ketone levels.
Results:
All participants successfully completed the fast. Mean TIR increased from 71.6 ± 13.9% during routine days to 82 ± 13.2% during fasting (P < 0.01), while time <70 mg/dL decreased from 2.6% to 2.2% (P = 0.017). Ten mild hypoglycemic events occurred after the pre-fast meal and one during fasting. A higher baseline percentage of time <70 mg/dL was the only predictor of hypoglycemia. No significant difference was found between 780 G users with exercise mode and those with no or minor changes. Participants received 43.4 ± 16.8% (range 9.3%–90%) of their usual insulin dose. Median (IQR) end-of-fast ketone levels were 0.4 (0.3, 0.7) mmol/L vs 0.1 (0, 0.1) mmol/L on a regular morning (n = 31); insulin doses <30% of usual dose were associated with higher ketone levels. No severe hypoglycemia or serious adverse events occurred.
Conclusion:
AID systems enable safe 25-h fasting by maintaining glucose control and reducing the risk of hypoglycemia and ketonuria. Fasting adjustments should be individualized and can often be minor.
Graphical Abstract
Introduction
Fasting has long been practiced across diverse religious traditions and, in recent years, has also gained prominence as a lifestyle choice associated with health benefits. In Judaism, Yom Kippur, the Day of Atonement and the holiest day of the year, is marked by a complete 25-h fast (abstinence from both food and fluids) observed not only by strictly religious individuals but also by many secular Jews who choose to fast on this day.1,2
In individuals with type 1 diabetes (T1D), fasting poses substantial risks owing to the difficulty of maintaining euglycemia and appropriately adjusting insulin therapy. The absence of caloric intake increases susceptibility to hypoglycemia, and evidence shows that short-term fasting impairs glucagon counter regulation and endogenous glucose production, further amplifying this risk. 3 At the same time, fasting promotes dehydration and activation of gluconeogenic and ketogenic pathways. When circulating insulin levels are insufficient to suppress lipolysis and ketogenesis, fatty acid oxidation predominates, resulting in ketone accumulation. The convergence of insulin deficiency, rising ketones, and dehydration substantially increases the risk of diabetic ketoacidosis (DKA), a life-threatening emergency.4,5 Although rare, fasting combined with dehydration may also precipitate euglycemic DKA. 6
Given these risks, the safety and feasibility of fasting in individuals with T1D remain an ongoing clinical concern. Accordingly, professional guidelines and diabetes care centers generally advise against fasting in this population. In situations where fasting is undertaken, expert consensus emphasizes the need for strict medical supervision, individualized insulin adjustments, frequent glucose and ketone monitoring, and readiness to terminate the fast if metabolic instability develops.2,7,8 Therefore, many diabetes clinics and centers, including ours at Schneider Children’s Hospital diabetes clinic, do not recommend fasting for people with diabetes. However, some individuals elect to fast despite these recommendations.
The introduction of advanced diabetes technologies, particularly automated insulin delivery (AID) systems, has the potential to mitigate glucose excursions and reduce risk of hypoglycemia by dynamically adjusting insulin delivery based on real-time continuous glucose monitoring (CGM) data. However, clinical evidence on the safety and effectiveness of AID systems during prolonged fasting remains limited. Furthermore, evaluating their use in this setting may yield valuable insights into minimum insulin requirements for suppressing ketogenesis, changes in insulin sensitivity, and the safety thresholds for preventing both hypoglycemia and ketosis. Such findings could inform clinical guidelines for managing insulin delivery during planned fasting periods, including medical procedures, diagnostic testing, or surgery.
In this study, we aim to evaluate the safety, glycemic outcomes, and insulin delivery in individuals with T1D who elect to fast during Yom Kippur while routinely using an AID system for diabetes management. In addition, the study examined the presence and extent of ketonuria at the conclusion of the 25-h complete fast.
Research Design and Methods
This study was approved by the Institutional Review Board of the Rabin Medical Center, number 0494-24-RMC, and conducted in accordance with the ethical standards of the 1964 Helsinki Declaration and its later amendments. The study was conducted at the institute for endocrinology and diabetes at Schneider children’s medical center of Israel.
Study design and participants
This was a non-interventional study of youth with T1D fasting during Yom Kippur in October 2024. The study included 19 participants prospectively, and data from 35 additional participants were collected retrospectively. Approximately 1 month before Yom Kippur, potential participants were identified during routine clinic visits, through the clinic mailing list, and by telephone contact with known religious individuals to determine their intention to fast. Of these, 19 participants were prospectively enrolled when they attended the clinic and provided written informed consent, or parental consent and participant assent, where applicable. In addition, as part of an initiative to reduce fasting risks, in two clinics located in religious areas, blood glucose and ketone meters were made available so that individuals who wished to fast could use them for safety as part of routine care.
Included in the study were individuals with T1D, aged 10 years and above, and using AID system, who declared that they intended to fast on Yom Kippur and agreed to participate in the study. Excluded from the study were individuals with a comorbidity or condition that, in the judgment of the study physician, prohibited fasting; had a history of severe hypoglycemia or diabetes ketoacidosis within the last 3 months; and pregnant women.
Participants used FreeStyle Optium Neo meter (Abbott Diabetes Care Ltd, UK) to measure capillary β-hydroxybutyrate levels at the end of the fasting period and after an overnight fast on a regular day. Under standard (non-fasting) conditions, plasma ketone concentrations are typically below 0.6 mmol/L and are considered within no particular risk for DKA.9,10
The participants received no instructions regarding fasting practices or insulin pump adjustments as part of the study protocol. Accordingly, data from individuals who undertook fasting independently, outside the formal study setting, were incorporated and analyzed together with those who were included prospectively.
Data collection
CGM and pump data were collected from cloud-based platforms when available or uploaded during the subsequent clinic visit for participants who were not connected. Glucose levels were calculated from raw Comma-Separated Values (CSV) file exports, and insulin delivery was derived from either the CSV files data or the platforms’ summary reports. Three periods were analyzed: the 2 weeks most proximal to the fasting day (generally the 2 weeks preceding the fast), referred to as baseline; the entire 25-h fast; and the final 12 h of the fast. The last 12 h were additionally analyzed, as this period represents a true fasting state, unaffected by postabsorptive effects of the pre-fast meal or associated insulin, thereby allowing evaluation of basal insulin requirements. Only participants with ≥70% CGM and AID data availability during the fasting period were included in this analysis.
Data on participant demographics and study cohort characteristics were retrieved from electronic medical records. Data on participants’ fasting experiences (e.g., symptoms, hypoglycemia, fast interruption, and other clinical or behavioral observations) were collected from medical records and self-reports.
Outcomes and statistical analysis
CGM data were used to assess glycemic control during the fasting period. A hypoglycemia event was defined as glucose levels below 70 mg/dL or 54 mg/dL for more than 15 min. 11
Descriptive statistics were used to summarize cohort characteristics and outcome measures. Continuous variables were expressed as mean ± standard deviation for normally distributed data or as median with interquartile range (IQR) for skewed data, while categorical variables were presented as counts and percentages. To identify predictors of hypoglycemic events during the fasting period, a forward likelihood ratio (LR) Cox regression model was applied.
Ketone concentrations at the end of the 25-h fasting period were compared with those obtained following an overnight fast on a routine day using the Wilcoxon signed-rank test, due to the skewed distribution of the data. Potential determinants of ketone levels at the end of the fasting period were examined with a forward stepwise linear regression model. Insulin doses and glucose levels were compared between baseline (approximately 2 weeks prior to fasting), 25 h of fasting, and the final 12 h of the fast using a general linear model with repeated measures.
Glucose and insulin data in participants using the MiniMed™ 780 G system were compared between those maintaining their usual settings with no or minor changes during the fast and those who used the exercise mode. For variables with normal distributions, an independent samples t-test was applied, while the Mann–Whitney U test was used for skewed variables.
All statistical tests were two-tailed, and a P value < 0.05 was considered statistically significant.
Results
A total of 54 adolescents and young adults were included in the study. Demographic characteristics of the participants are presented in Table 1. The cohort had a mean age of 17.3 ± 3.3 years and had been using AID systems for an average of 1.5 ± 0.8 years. Most participants were well controlled, with a mean baseline TIR of 71.2 ± 13.7% and a mean HbA1c of 6.8 ± 1.0%. Nineteen participants (35%) had HbA1c levels above the target of 7%. Regarding device distribution, 34 participants used MiniMed 780 G, 10 used Control-IQ, and 10 used open-source systems.
Demographic Characteristics of Study Participants (n = 54)
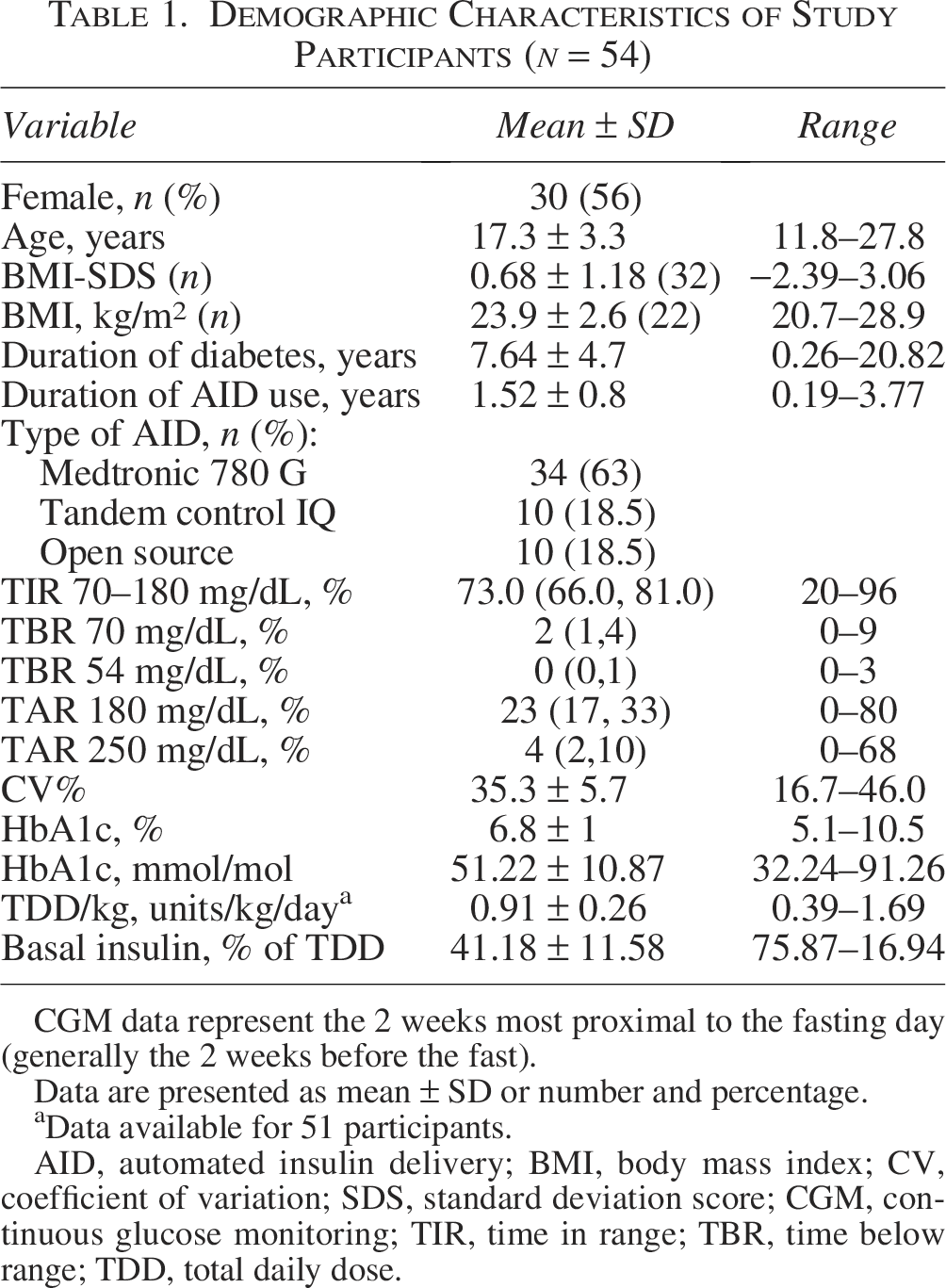
CGM data represent the 2 weeks most proximal to the fasting day (generally the 2 weeks before the fast).
Data are presented as mean ± SD or number and percentage.
Data available for 51 participants.
AID, automated insulin delivery; BMI, body mass index; CV, coefficient of variation; SDS, standard deviation score; CGM, continuous glucose monitoring; TIR, time in range; TBR, time below range; TDD, total daily dose.
Fasting-related adjustments to AID system parameters
Participants received no specific instructions regarding fast-related adjustments and therefore employed individual strategies, resulting in heterogeneous practices. Among all participants, 11 (20.4%) made no adjustments to any device parameter throughout the fasting period. Of the 34 participants using the MiniMed 780 G system, 19 (56%) enabled the exercise target of 150 mg/dL as their primary glucose target throughout the fasting period. Within this group, 11 maintained exercise mode for the entire fasting duration, 5 used it continuously but exited 1 to 2 h before the end of the fast, and 3 activated it at varying times during the fasting. 10 participants did not make any adjustments to their settings, while four did not change targets but applied exercise mode intermittently for up to 7 h. Two participants adjusted their glucose target from 100 mg/dL to 120 mg/dL. No modifications were made to the default active insulin time in any participant.
Of the 10 participants using Control-IQ technology, most (n = 8) activated Sleep Mode during the fasting period. Two used it only at night, as they typically did on non-fasting days, along with reductions in basal insulin and correction factor (CF). Five activated Sleep Mode for the entire fasting period, with one of them additionally reducing basal insulin and CF. One participant used Exercise Mode throughout, and one made no changes to the pump settings. Basal profile reductions were in the range of 15%–35%.
Among the 10 participants using open-source AID systems, data were available for 9, who tended to make the most extensive adjustments. Most participants who reduced their basal profiles by 20%–50% (n = 8) also raised their glucose targets (n = 7), and some (n = 3) additionally increased the CF by 30%–50%, thereby lowering insulin delivery for corrections.
Glycemic control
The average sensor glucose level at the start of fasting was 204 ± 66 mg/dL (after the pre-fast meal) and 112 ± 29 mg/dL at the end of the fast, based on 46 paired values (P < 0.001). During the fasting period, 67% of participants achieved the composite CGM targets recommended internationally: TIR between 70 and 180 mg/dL >70%, time between 70 and 54 mg/dL <4%, and time <54 mg/dL <1%. 11 Complete insulin and glucose data were available for 47 participants using the AID system and are summarized in Table 2, which presents metrics at baseline (approximately 2 weeks before fasting), at 25 h of fasting, and during the final 12 h of the fasting. The overall glucose profile during the 25-h fast is shown in Figure 1.
Insulin and Glucose Data at Baseline, During the 25-h, and During the Last 12-h of the Fast (n = 47)
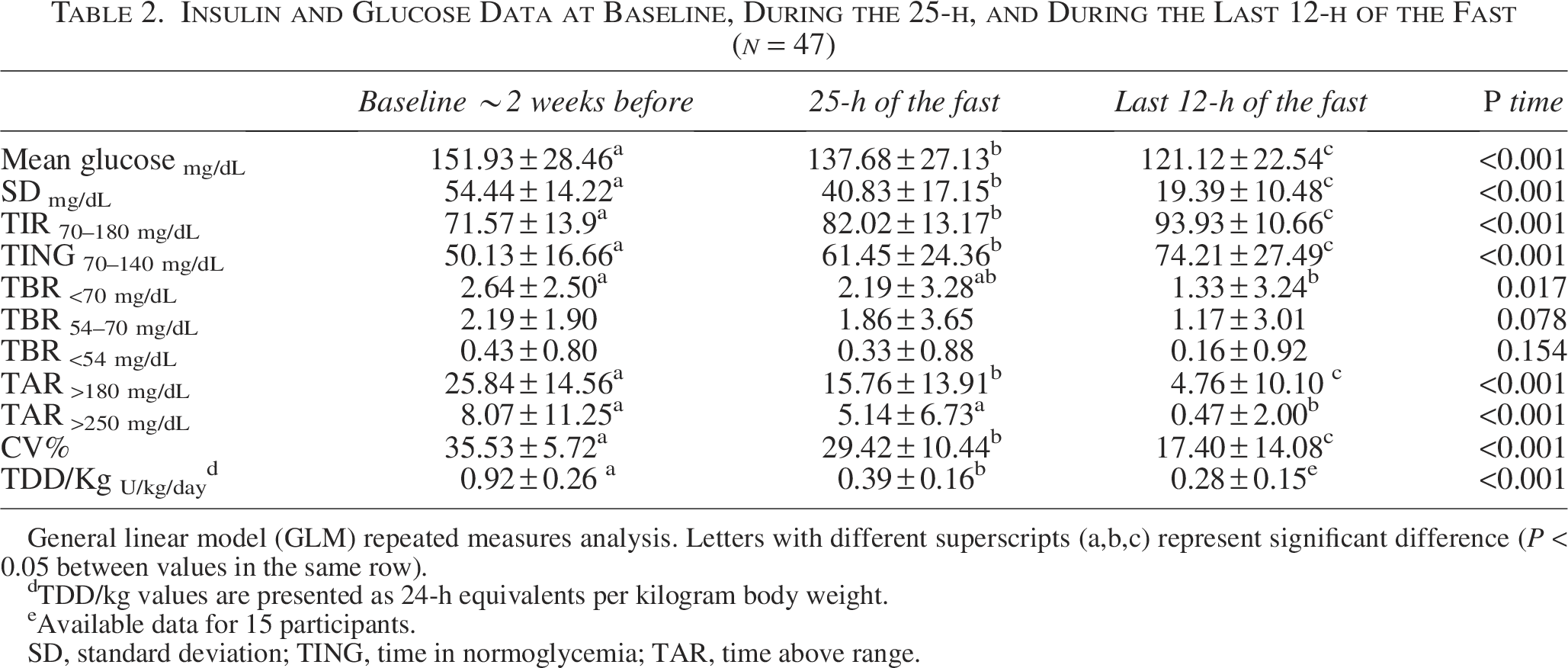
General linear model (GLM) repeated measures analysis. Letters with different superscripts (a,b,c) represent significant difference (P < 0.05 between values in the same row).
TDD/kg values are presented as 24-h equivalents per kilogram body weight.
Available data for 15 participants.
SD, standard deviation; TING, time in normoglycemia; TAR, time above range.
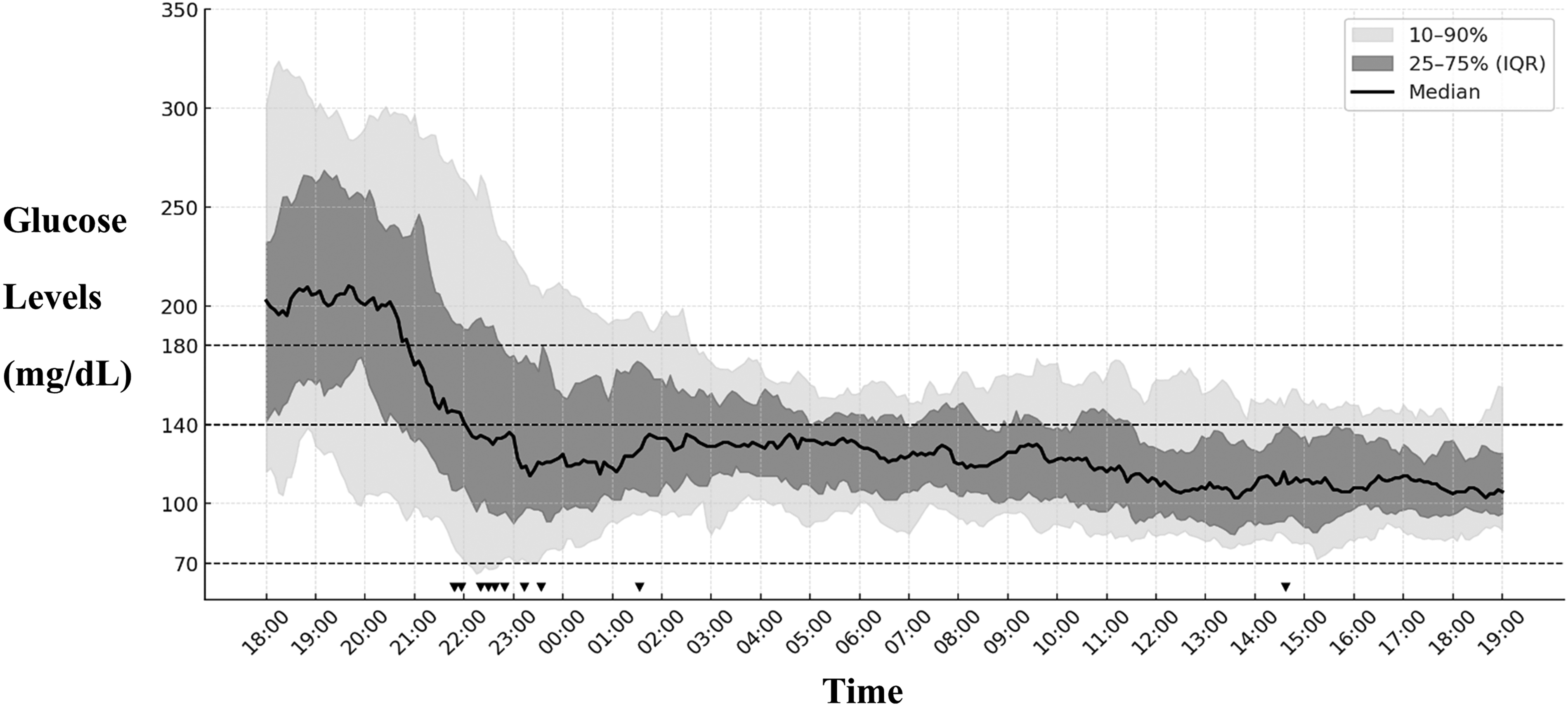
Twenty-five-hour glucose profile during fasting (n = 47). The solid black line represents the median CGM glucose during the 25-h fasting period, with the dark gray band showing the interquartile range (25th–75th percentile) and the light gray band representing the 10th–90th percentile range. Black triangles on the time axis mark hypoglycemia events (n = 11) observed in the entire cohort. CGM, continuous glucose monitoring.
Mean glucose, hyperglycemia, and glycemic variability were significantly lower during fasting, while TIR and Time In NormoGlycemia (TING) were significantly higher, with additional improvements in the last 12 h. TIR (70–180 mg/dL) increased from 71.6 ± 13.9% before fasting to 82.0 ± 13.2% at 25 h and 93.9 ± 10.7% in the final 12 h (P < 0.001), without an increase in hypoglycemia. Notably, time <70 mg/dL was significantly reduced during fasting and again in the last 12 h, accompanied by lower insulin delivery rates.
As the number of participants using the MiniMed 780 G was sufficient, we compared glucose and insulin data between those maintaining their usual settings with no or minor changes during the fast and those using the exercise mode, as presented in Table 3. As expected, the exercise group received less insulin than the usual settings group. No differences were observed between the groups in overall glycemic control, hypoglycemia, or hyperglycemia; however, TING was significantly greater in the usual settings group.
Comparison of Glucose and Insulin Data Between Usual Settings and Exercise Mode Strategies in MiniMed 780 G Users (n = 31)
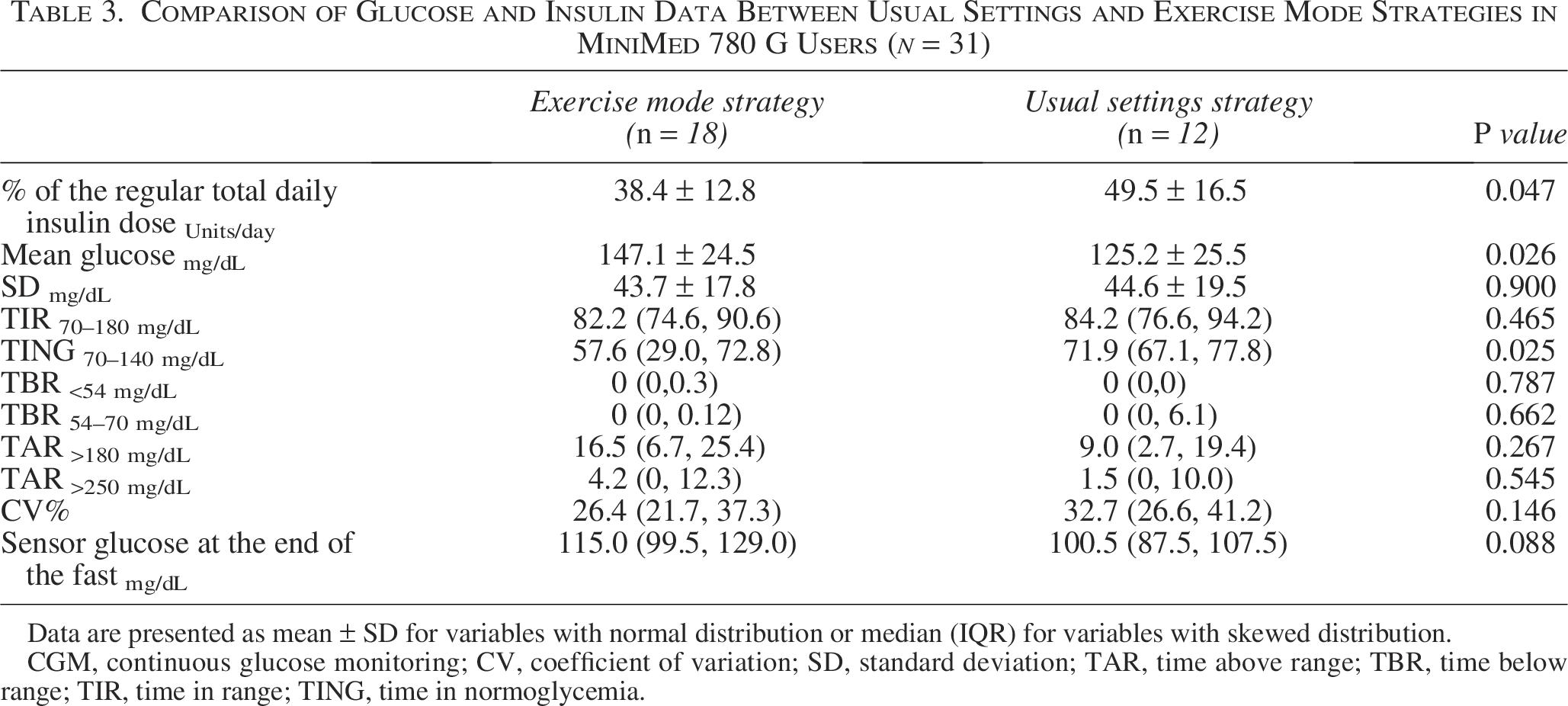
Data are presented as mean ± SD for variables with normal distribution or median (IQR) for variables with skewed distribution.
CGM, continuous glucose monitoring; CV, coefficient of variation; SD, standard deviation; TAR, time above range; TBR, time below range; TIR, time in range; TING, time in normoglycemia.
Insulin dose
On average, insulin delivery during the fasting day was 43.4 ± 16.8% (range 9.3%–90%) of the regular total daily insulin dose. Insulin data were available for 47 participants at baseline and at 25 h of fasting, and for 15 participants during the final 12 h (Table 2). The mean total daily insulin delivery was 0.39 ± 0.16 U/kg/day during the fasting period and was lower, at 0.28 ± 0.15 U/kg/day, in the final 12 h.
Adverse events
Hypoglycemic events were assessed using data from both CGM and participant self-reported experiences. Complete data were available for all participants except one. A total of 11 hypoglycemic events were reported among 10 participants. The distribution of these events across the fasting period is shown in Figure 1.
Ten mild hypoglycemic events occurred postprandially after the pre-fast meal, treated with 10.4 ± 7.1 g of carbs, with all continuing fasting. Notably, two individuals did not consume carbohydrates despite hypoglycemia. Of these events, five were between 54 and 70 mg/dL, four events were below 54 mg/dL, and there was one only symptomatic event with glucose level of 73 mg/dL. One participant had two events, one postprandial (included among the 10 events described above) and one on the second day of fasting, with glucose levels of 54–70 mg/dL. No instances of severe hypoglycemia or other serious adverse events were reported during any of the fasts.
A forward LR Cox regression model was performed to identify predictors of hypoglycemia events during the fasting period. Covariates included age, gender, duration of AID use, percentage of the regular total daily dose (TDD) delivered during the fasting period, time below range (TBR <70 mg/dL and <54 mg/dL), and glucose level at the start of fasting. Of these variables, only the baseline percentage of time spent below 70 mg/dL entered the final model. A higher baseline TBR <70 mg/dL was associated with an increased risk of hypoglycemia (HR = 1.219; 95% CI: 0.994–1.494; P = 0.057).
Ketones measurements
Capillary ketone levels at the end of the 25-h fast were recorded by 31 participants. The median and IQR of the ketone level measurement was 0.4 (0.3, 0.7) mmol/L, range 0.1–1.6 mmol/L, compared with 0.1 (0.1, 0.1) mmol/L, range 0–0.2 mmol/L, measured on the morning of a regular day (P < 0.001).
A forward linear regression model was used to identify predictors of higher ketone levels at the end of the fast, including age, gender, duration of AID use, percentage of the regular TDD delivered during the fasting period, baseline TIR, and glucose levels at the start of fasting. The only variable that entered the final model was the percentage of insulin dose delivered during the fast of the usual TDD. A higher percentage of insulin delivery during the fast was significantly associated with lower ketone levels (β = –0.014, SE = 0.005, P = 0.017). Specifically, every 10% increase in insulin delivery during fasting was associated with a 0.14 mmol/L decrease in ketone levels. The ketone levels vs. percentage of insulin dose delivered during fasting relative to the usual TDD is presented in Figure 2.
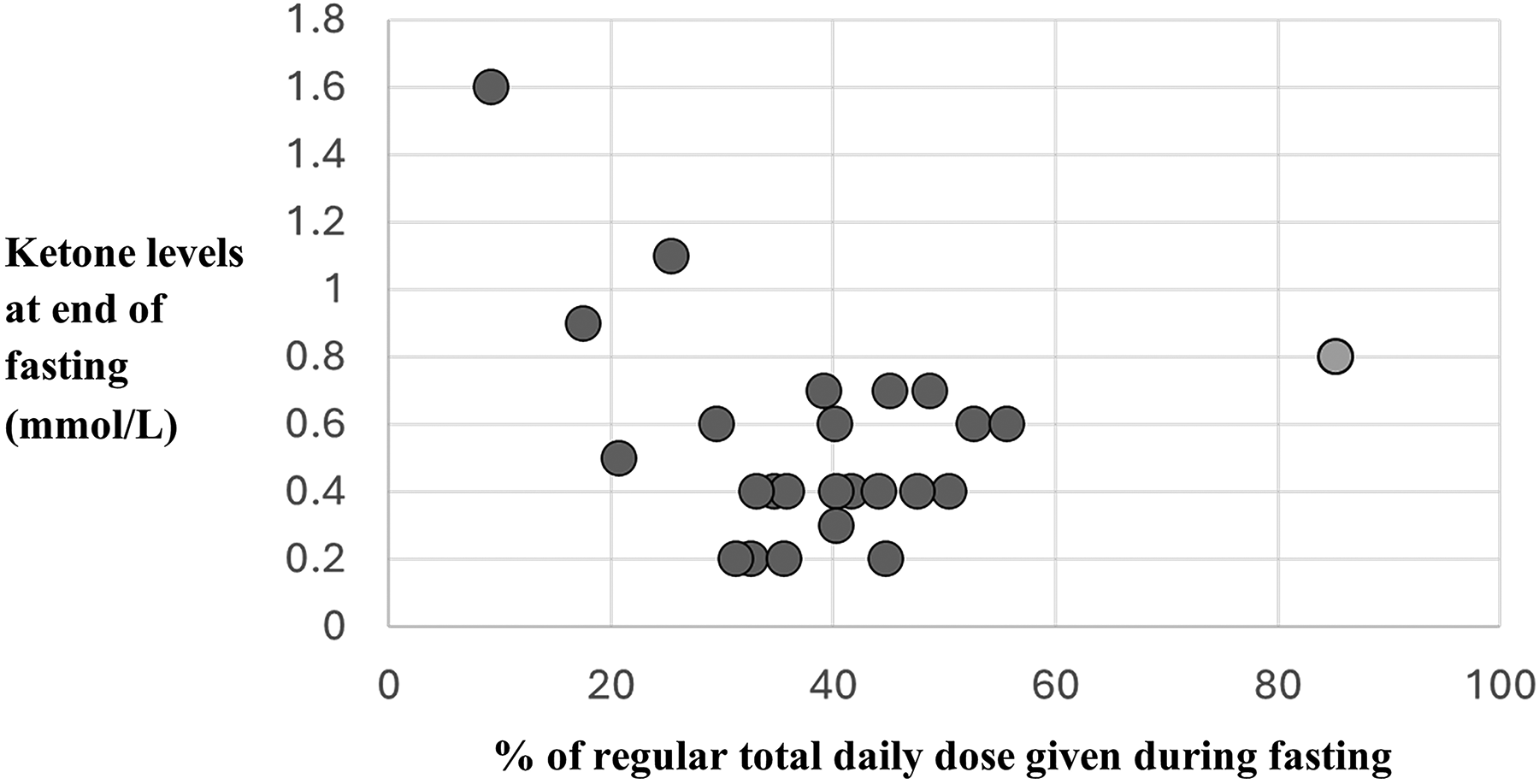
Ketone levels vs. insulin dose on fasting day (%) of regular total daily dose (n = 25*). * n = 25 participants with available insulin and ketone data. [GRAPHIC] Participant with poor baseline TIR. TIR, time in range.
Conclusions
This study demonstrates that AID systems can facilitate safe fasting in individuals with T1D by maintaining glucose levels within target range, ensuring adequate insulin delivery to suppress ketonuria, and minimizing the risk of hypoglycemia. Through individualized adjustments, AID systems offer a reliable and effective approach to mitigating metabolic risks associated with fasting.
The fasting period began with a mean postprandial glucose level of approximately 200 mg/dL and gradually transitioned into the target range, reaching a final TING of 74.2 ± 27.5%. The percentage of time spent in hypoglycemia (<70 mg/dL) was significantly lower during the prolonged fasting period than during regular daily routine. We found no other published data on Yom Kippur fasting using AID. However, in a small study of eight insulin pump users monitored with blinded CGM during Yom Kippur, participants with a similar baseline HbA1c (7.3%) had a mean glucose of 185 ± 69 mg/dL and 5% of readings below 70 mg/dL, 12 compared with 138 ± 27 mg/dL and 2.2% in our study. Considerably more data exist for Ramadan fasting, which differs in everal respects from Yom Kippur fasting in structure and metabolic impact. Ramadan involves daily fasts of approximately 14–16 h, typically followed by one or more substantial evening meals, and is repeated for 29 to 30 consecutive days. In contrast, Yom Kippur is a single, continuous fast of about 25 h, during which no food or fluids are consumed, eliminating the confounding effects of intermittent refeeding and posing greater potential for dehydration and prolonged insulin deprivation. In a real-world Ramadan study of 62 AID users (baseline TIR 71.7%, TBR of 2.7%), fasting TIR was 73% with TBR 2.0%. 13 With a comparable baseline profile, our cohort achieved a higher TIR of 82% and a similar TBR of 2.2% during the 25-h Yom Kippur fast, possibly due to the longer continuous fasting without intermittent meals.
The ability of AID systems to modulate insulin delivery in response to glucose real-time levels enables estimation of continuous background insulin requirements for metabolic stability. Importantly, the final 12 h of the fast, devoid of food and fluid intake and uninfluenced by the pre-fast meal, provided a controlled period for reliable evaluation of insulin delivery. During this time, total insulin delivery averaged approximately 0.28 units/kg/day, reflecting the reduced insulin requirement under prolonged fasting. Corresponding glycemic control was optimal, with a mean TIR of 94% and 1.3% time spent in hypoglycemia below 70 mg/dL, both significantly better than the already favorable results observed over the entire 25-h fast, which were 82% and 2.2%, respectively. Our mean insulin delivery was slightly higher than the 0.20 U/kg/day reported by Strich et al., who examined individuals treated with MDI or CSII. The difference is likely due to more cautious dosing with Multiple Daily Injections (MDI) or CSII compared with automated modulation and acceptance of higher glucose levels. 14
AID enabled successful fasting in all participants, although 8 of 56 required carbohydrates for a hypoglycemic event and then continued fasting. In comparison, in populations using older technologies (MDI or CSII without CGM), Strich et al. reported a 22% termination rate (27% pump, 16% MDI) across 88 fasting events, with most cases due to hypoglycemia, 14 and Reiter et al. reported 35% early termination among 56 individuals 15 despite insulin dose reductions of up to 50%. Thus, AID systems appear safer for fasting than other modalities reported to date, although this was not tested directly in the present study. The advantage of AID over other modalities has been reported in intermittent fasting studies.13,16
As all but one hypoglycemic event occurred after the pre-fast meal, our findings suggest that in the context of Yom Kippur fasting, AID systems can prevent prolonged fasting-related hypoglycemia and be used safely, with glucose management following the pre-fast meal identified as the main area requiring attention. A reduction of the pre-fast meal bolus by approximately 10%–20% may help to minimize postprandial hypoglycemia during fasting. A higher percentage of TBR <70 mg/dL at baseline was found to be a predictor of an increased risk of hypoglycemia during the fast (HR = 1.219; 95% CI: 0.994–1.494; P = 0.057). This may help in planning and guiding individualized strategies for safe fasting. Similar findings were reported in a Ramadan study by Al-Sofiani et al., in which hypoglycemia risk was also predicted by pre-fasting glycemic metrics. In their analysis, the pre-Ramadan Glycemia Risk Index demonstrated greater sensitivity than pre-Ramadan TIR in identifying individuals with T1D who were likely to fast most days. 13
Importantly, all participants maintained ketone concentrations well below the threshold for ketoacidosis. Median ketone levels were 0.4 mmol/L (IQR 0.3–0.7) after the 25-h fast, compared with 0.1 mmol/L (IQR 0–0.1) following overnight fast. One participant ended the fast with a ketone level of 1.6 mmol/L following substantial reductions in insulin delivery due to multiple pump adjustments (reduced basal insulin, CF, and increased glucose target, all contributing to lower overall insulin delivery) as well as more than 3 h without pump use. No cases of DKA or ketonuria-related symptoms occurred; the mild ketosis observed in our study was likely due to fasting and, in a few cases, disruptions in insulin delivery. These mild elevations in ketone levels reflect a normal physiological response, characterized by enhanced fat oxidation and ketone production, rather than a pathological process. Our findings are consistent with those of Moser et al., who conducted a supervised study in 20 adults with T1D. In that study, participants were permitted water intake during fasting and mild ketosis was observed, with mean ketone levels rising to 0.54 mmol/L after 36 h compared with 0.15 mmol/L after 12 h. 17 In our study, the only variable associated with ketone levels was the percentage of insulin delivered during fasting relative to the usual TDD. Higher insulin delivery during fasting was significantly correlated with lower ketone concentrations (β = –0.014, SE = 0.005, P = 0.017), with each 10% increase in insulin delivery corresponding to a 0.14 mmol/L reduction in ketone levels. This finding underscores the importance of maintaining adequate insulin delivery during fasting to prevent excessive ketone accumulation. While no participant developed DKA and almost all exhibited only mild ketosis, receiving less than 30% of the usual daily insulin dose during fasting was associated with higher ketone levels.
In the absence of standardized guidance on system adjustments, participants adopted diverse strategies, ranging from modification of all adjustable parameters to completing the fast without any alteration of device settings. Most MiniMed™ 780 G users activated exercise mode for the entire fasting period. As MiniMed™ 780 G users constituted the largest group in our cohort, we were able to compare those who used exercise mode almost exclusively with those who made minimal or no parameter changes. The latter group achieved significantly better glycemic control, with higher insulin delivery and no increase in hypoglycemia. This subgroup delivered approximately 50% of their regular daily insulin dose, compared with 38% of those using exercise mode. While both groups had similar TIR and rates of hyperglycemia, the minimal/no-modification group achieved significantly better TING and lower mean glucose without an increase in hypoglycemia. In our population, AID use was safe during prolonged fasting even with minimal or no parameter adjustments. Similar outcomes were reported by Elbarbary et al. in a prospective study of 42 youth with T1D fasting during Ramadan, which compared adjusted versus unchanged MiniMed 780 G settings. The study demonstrated that even with the default optimal configuration (100 mg/dL target, 2-h active insulin time), participants maintained excellent glycemic control (TIR ∼82%) without increasing hypoglycemia and with no severe adverse events. 18 The Control-IQ and open-source AID groups were too small to allow for a meaningful comparison and to determine the preferred strategy, which remains to be established in future studies.
These findings demonstrate that there is more than one safe strategy for fasting and that adaptations in AID settings can be mild while still achieving improved control with safety. As with all aspects of diabetes management, the optimal strategy should be individualized and guided by the baseline glycemic profile and the pre-fasting hypoglycemia rate.
A key strength of this study is that it provides novel data from a 25-h fast in individuals using AID systems in real-world settings, including measurement of blood ketone levels in participants who fasted, compared with levels measured during a usual overnight fast. Nevertheless, this study has several limitations. First, most participants had good glycemic control and voluntarily chose to fast with adjustments to device settings made at their discretion. This may limit the generalizability of our findings to the broader population. Second, we lacked a reference group of healthy, age-matched individuals fasting for comparison of ketone levels. However, previous data indicate that in healthy individuals plasma ketone concentrations generally range from 0 to 0.3 mmol/L under normal conditions but may rise to approximately 1 mmol/L after 24 h of fasting or prolonged exercise. 9 In addition, ketone data were incomplete in a portion of participants, limiting full assessment.
In addition, the study included both prospective and retrospective cohorts, which may have introduced variability in data collection. However, as no specific fasting instructions were provided, the data could be combined to reflect real-world practices. The heterogeneity of AID systems represents another limitation, as differences in algorithms and settings may have influenced glycemic outcomes, yet also allowed assessment of fasting-related adjustments across diverse systems. Finally, the study was designed to descriptively assess real-world AID system performance during fasting, without formal hypothesis testing.
In Summary
AID systems support safe fasting by providing effective insulin delivery even with minor individualized adjustments and are associated with a low risk of hypoglycemia and an absence of significant ketonuria. These findings underscore the need to revise practical guidelines to classify individuals with T1D using AID as having lower metabolic risks while fasting compared with those managed by alternative therapies.
For fasting periods such as Yom Kippur or similar fasts for medical procedures, suggested adjustments include pre-fast meal bolus reduction; for the MiniMed 780 G, use of exercise mode or a higher glucose target with or without extending insulin action time; for Control-IQ, use of sleep mode or reduced basal with or without adjusting the CF; and for open-source systems, a higher glucose target with or without basal profile reduction. All adjustments should be individualized and selected in accordance with glycemic control and hypoglycemia risk, with close CGM monitoring.
Authors’ Contributions
R.N. contributed to the study design, data collection, data interpretation, and writing the first draft of the article. K.S.Z., R.B., N.F.S., and K.V.S. contributed to the study conduct and data collection. R.N. and M.Y.G. contributed to the statistical analysis. M.P. contributed to the study conduct and data interpretation. All authors reviewed and approved the last version of the study. R.N. is the guarantor of this work and, as such, has full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Footnotes
Acknowledgments
The authors would like to thank Geffen Medical for their provision of Neo glucometers and ketone test strips, free of charge. The authors thank the following colleagues for assistance in the study: Ayelet Parnas, Orna Hermon and Galit Shiovitch-Mantzuri.
Author Disclosure Statement
Revital Nimri served on advisory board of Tandem Diabetes and DreaMed Diabetes and received honoraria for participating in the speaker’s bureau of Novo Nordisk, Pfizer, Sanofi, Medscape, and Insulet. Revital Nimri is a shareholder of DreaMed Diabetes and has an active position in DreaMed Diabetes. Revital Nimri’s institution received research grant support from Abbott Diabetes, Eli Lilly, Geffen Medical, Medtronic Diabetes, Novo Nordisk, Pfizer, and Sanofi. Moshe Phillip has participated on advisory boards for AstraZeneca, Eli Lilly, Insulet, Mannkind, Medtronic Diabetes, Pfizer, Sanofi, Bayer, Ascensia, ProventionBio, embecta, Dompe, and Tandem. He has received consulting fees from Qulab Medical and ProventionBio and received, through his institute, research grants from Eli Lilly, Medtronic Diabetes, Novo Nordisk, Pfizer, Sanofi, DreaMed Diabetes, NG Solutions, Dompe, Lumos, GWAVE, OPKO, ProventionBio, AstraZeneca, and Omega Galil. Moshe Phillip owns stocks in DreaMed-Diabetes and NG Solutions. Keren Smuel-Zilberberg, Michal Yackobovitch-Gavan, Rachel Bello, Naama Fisch-Shvalb, and Sari Krepel Volsky have no disclosure.
Funding Information
No funding was received for this article.