
Abstract
Aims:
Real-world evidence (RWE) data on the use of automated insulin delivery (AID) systems in the MENAT region (Middle East, North Africa, Türkiye) are limited. The aim of this article is to report RWE data on the use of the MiniMed™ 780G AID system in MENAT.
Materials and Methods:
CareLink™ personal data as of July 01, 2024, of MENAT users from countries with more than 25 users were included. Continuous glucose monitoring-based endpoints, system usage, and insulin delivery were examined in (1) the overall cohort, (2) users who reached 12 months of system use (longitudinal cohort), and (3) users having pre- to post-AHCL (advanced hybrid closed-loop) algorithm initiation data.
Results:
Seven thousand nine hundred and sixty-five users across 19 MENAT countries showed a mean glucose management index (GMI) of 6.9 ± 0.7%, time in range (TIR) of 71.7 ± 18.2%, time in tight range (TITR) of 48.9 ± 19.4%, time below range 70 mg/dL of 2.4 ± 3.9%, and time below range 54 mg/dL of 0.5 ± 1.7%. TIR and TITR were higher in users using optimal settings (glucose target = 100 mg/dL and an active insulin time = 2 h), being 76.3 ± 16.4% and 54.2 ± 18.8%, respectively. Consistent results were obtained analyzing different age groups, different countries, across the four seasons, between weekday/weekends, and day/night. Glycemic improvements began after AHCL algorithm initiation and sustained for 12 months, with a TIR and TBR70 that reached international targets in all months.
Conclusions:
MiniMed 780G system RWE data in the MENAT region showed a sustained glycemic control that achieved international target criteria across different age groups, countries, and climate extremes. These findings align with RWE data from other geographies, validate the broad applicability of the MiniMed 780G benefits, and may help expand access to AID systems in the region.
Introduction
Automated insulin delivery (AID) systems play a crucial role in managing type 1 diabetes (T1D) 1 offering substantial improvements in glycemic control for individuals affected by this condition. These advancements have led to the inclusion of AID systems in international guidelines for managing T1D in both adults and children.2–4
One such system, the MiniMed™ 780G system, has an advanced hybrid closed-loop (AHCL) algorithm that, according to the sensor value recorded, automatically administers basal insulin and delivers autocorrection boluses every 5 min as needed, aiming for a specified glucose target (GT). The MiniMed 780G system has been shown to safely achieve internationally recommended glycemic targets in both clinical trials and real-world settings.5–8
Over recent decades, the burden of T1D has escalated globally, with the MENAT region experiencing a notable increase in new cases.9–11 Between 1990 and 2019, the age-standardized incidence rate (per 100,000) increased from 5.8 (4.7–7.1) to 10.6 (8.6–13.0) (84.1% [80.2–88.4] increase in both sexes).12,13
Despite considerable heterogeneity in culture, development, income, ethnicity, urbanization, and health care, the region shares several significant commonalities. One of these is the widespread influence of Islam, the predominant religion, which shapes unique lifestyle adaptations, such as fasting during the holy month of Ramadan, structured prayer times throughout the day, and specific dietary customs. 14 Additionally, the population contends with some of the highest temperatures in the world, raising questions about the impact of extreme heat on blood glucose and the stability and integrity of insulin inside the pump for pump users. Moreover, the extreme heat necessitates further adaptations, such as shifting daily routines to make use of the cooler night hours (thus remaining active late into the evening).
Regions such as MENAT are underrepresented in clinical evidence related to T1D. Real-world studies are increasingly recognized as valuable sources of information on the effectiveness and safety of medical devices, offering complementary data to clinical trials by encompassing diverse and unbiased populations. This article provides a comprehensive overview of the performance and safety of the MiniMed 780G system in managing T1D in real-world user from MENAT.
Methods
Design
Data from the MiniMed 780G system, uploaded to the CareLink™ Personal software until July 1, 2024, were analyzed for users residing in MENAT. Metrics related to glycemic control, system usage, and insulin delivery were examined across three user cohorts. Cohort 1 represents the overall group, including data from all eligible users after initiating AHCL. Cohort 2 focuses on a 12-month longitudinal analysis to evaluate the sustainability of outcomes over time. Cohort 3 consists of a pre–post cohort for users with sufficient pre-AHCL data. Since AHCL initiation requires a minimum of 48 h of open-loop use, this allowed for a pre- and post-analysis of these users.
Data source
CareLink Personal is a software program that collects information directly from MiniMed systems and can be used by users to generate reports and monitor progress. The design, data quality, and data representativity have been extensively described in van den Heuvel et al. 15 In short, CareLink Personal contains data from all users who have created a CareLink Personal account. Users can upload either automatically (every night) or manually, based on the user’s preference. As the pumps have a 3-month storage capacity, upload gaps smaller than 3 months will not lead to missing data. Apart from device data, CareLink Personal also contains data on the self-reported age group. In addition to device data, CareLink Personal houses self-reported information such as gender (female or male) and age groups (≤15, 16–55, and ≥56 years).
Eligibility
Users who provided consent for their data to be aggregated and resided in MENAT countries with more than 25 users were included in the analysis. These countries specifically included Algeria, Bahrain, Egypt, Jordan, Kuwait, Lebanon, Morocco, Oman, Qatar, Saudi Arabia, the United Arab Emirates, and Türkiye. In addition, users needed to have a minimum of 10 days of sensor glucose (SG) data in each period evaluated; for cohort 1, this referred to the post-AHCL initiation period, for cohort 2, this referred to each month following AHCL initiation, and for cohort 3, this included both the pre- and post-AHCL period. This requirement (i.e., the minimum of 10 days of SG data) was based on a previous publication validating a similar duration of continuous glucose monitoring (CGM) metrics to estimate or determine long-term glycemic control. 16 All data available post-AHCL initiation were included, whether the system was in AHCL control or in open loop (e.g., following an AHCL exit triggered by either the system or the user).
Endpoints
Glycemic outcomes, including the mean percentage of time spent in 70–180 mg/dL (3.9–10.0 mmol/L) time in range (TIR), in 70–140 mg/dL (3.9–7.8 mmol/L) time in tight range (TITR), at less than 54 mg/dL (<3.0 mmol/L) (TBR54), at less than 70 mg/dL (<3.9 mmol/L) (TBR70), at more than 180 mg/dL (>10.0 mmol/L) (TAR180), and at more than 250 mg/dL (>13.9 mmol/L) (TAR250), were calculated. Additional endpoints related to glycemic outcomes, system usage, and insulin metrics were analyzed. Detailed information about these metrics can be found in Figure 1.
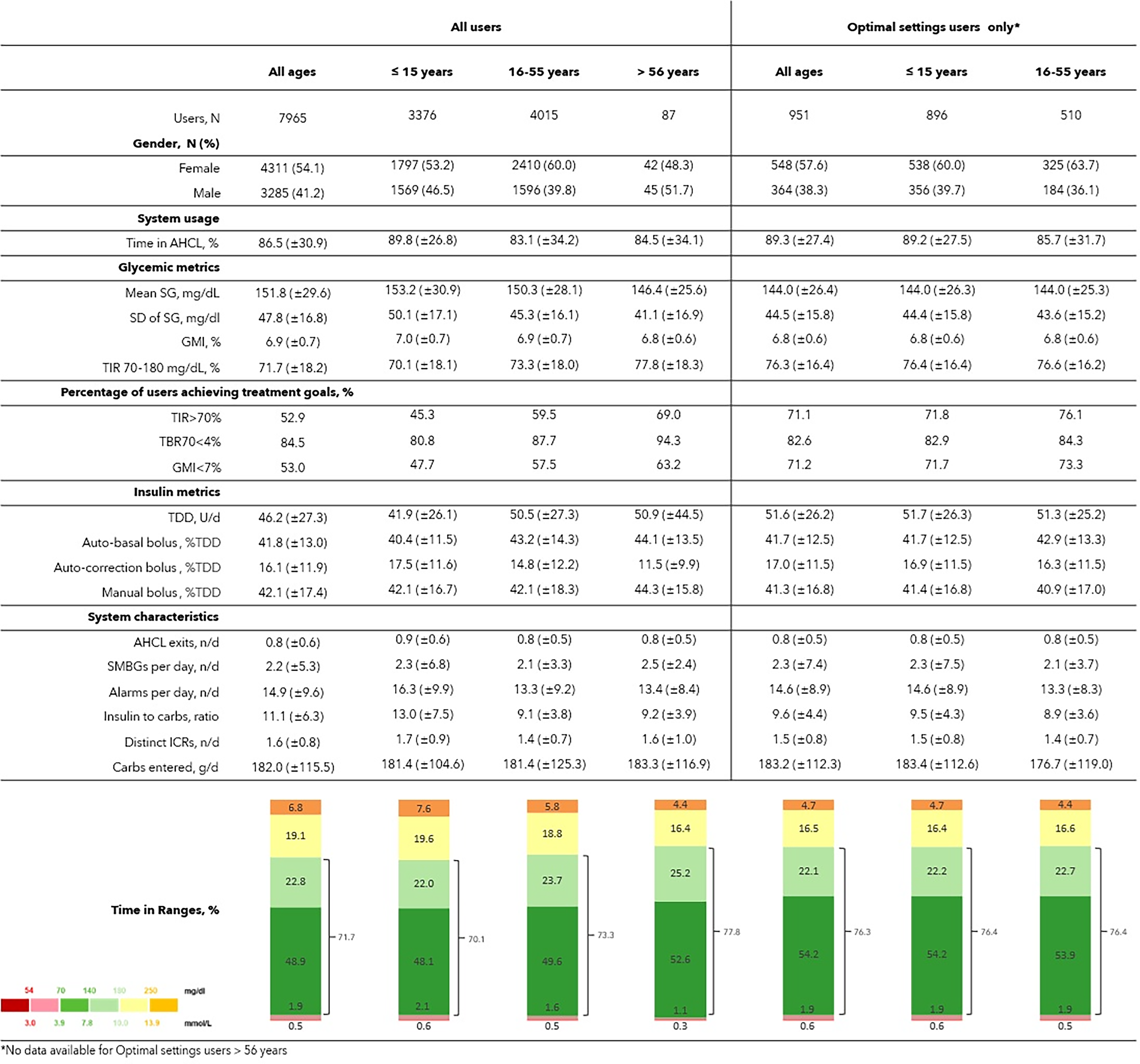
Glycemic control of real-world MiniMed™ 780G system users. Data are reported as mean (±SD), unless specified otherwise. Age groups are based on self-reported age in CareLink™ Personal (all ages, ≤15 years, 16–55 years, and >56 years). Overall cohort, sub-cohort per age, and sub-cohort on optimal settings are shown. Optimal settings are defined as a glucose target of 100 mg/dL for at least 95% of the time as well as an active insulin time of 2 h for at least 95% of the time. Note that data for elderly users (>56 years) with optimal settings are not shown due to insufficient numbers. Results are displayed as mean (SD) unless specified otherwise. AHCL, advanced hybrid closed loop; GMI, glucose management indicator; ICRs, insulin-to-carbohydrate ratios; SD, standard deviation; SG, sensor glucose; TBR, time below range; TDD, total daily dose; TIR, time in range; SMBGs, self-monitoring of blood glucose.
Statistics
Means and standard deviations were used for continuous variables, and the number of users and proportions for categorical variables. Endpoints were aggregated for each cohort. In addition, subanalyses were performed including users on optimal settings (those spending at least 95% of time with a GT of 100 mg/dL and at least 95% of time with active insulin time [AIT] of 2 h), for self-reported age groups (≤15, 16–55, and >56 years), and for separate countries. Also, subanalyses were done based on time windows such as day (06:01 AM to 11:59 PM) and night hours (12:00 AM to 06:00 AM), weekdays and weekends, and seasons.
Results
Cohort 1 (overall cohort)
Data from 7965 users across 19 countries in the MENAT region were analyzed (Fig. 1). The mean duration of the observation period was 300 days. The mean TIR and TITR were 71.7 ± 18.2% and 48.9 ± 19.4%, respectively. These were higher in users who consistently applied optimal settings (N = 951, 11.9% of the overall cohort), being 76.3 ± 16.4% and 54.2 ± 18.8%, respectively. The mean glucose management index (GMI) was 6.9 ± 0.7%, while TBR70 and TBR54 were low, at 2.4 ± 3.9% and 0.5 ± 1.7%, respectively. In terms of international glycemic targets, 53.0% of users achieved a GMI <7%, 52.9% achieved a TIR >70%, and 84.5% achieved a TBR70 <4%. Improved outcomes were observed in the subgroup consistently using optimal settings. Among users who consistently used a GT = 100 mg/dL and an AIT = 2 h, 71.2% achieved a GMI <7%, 71.1% achieved a TIR >70%, and 82.6% achieved a TBR70 <4%. In terms of insulin use, the mean total daily dose (TDD) of users was 46.2 units, of which 41.8% were automated basal and 16.1% were autocorrections.
In the age-specific subanalysis, 3376 users were reported to be 15 years old or younger, 4015 were between 16 and 55 years old, and 87 were older than 56 years. The mean TIR and TITR were 70.1 ± 18.1% and 48.1 ± 19.0% for users ≤15 years, 73.3 ± 18.0% and 49.6 ±19.8% for users between 16 and 55 years, and 77.8 ± 18.3% and 52.6 ± 20.5% for users ≥56 years. TIR and TITR were higher when optimal settings were used (for ≤15: 76.4 ± 16.4% and 54.2 ± 18.8% and for 16–55 years: 76.6 ± 16.2% and 53.9 ± 18.9%). For the three age groups, the average TBR70 and TBR54 were low (for ≤15 years: 2.7 ± 4.0% and 0.6 ± 1.7%, respectively; for 16–55 years: 2.1 ± 3.8% and 0.5 ± 1.7%, respectively; and for ≥56 years: 1.4 ± 3.0% and 0.3 ± 1.2%, respectively).
In the country-specific subanalysis presented in Figure 2, TIR ranged from 67.7% (Qatar) to 77.8% (Jordan); TITR spanned from 45.4% (Qatar) to 54.2% (Türkiye); GMI ranged from 6.7% (Türkiye) to 7.1% (Qatar and Bahrain); and TB70 fell between 1.9% (Bahrain and Jordan) and 3.0% (Lebanon). The overall percentage of users achieving a GMI below 7% ranged from 38.5% (Qatar) to 80.8% (Morocco), while those reaching a TIR above 70% varied between 38.9% (Qatar) and 76.9% (Morocco).
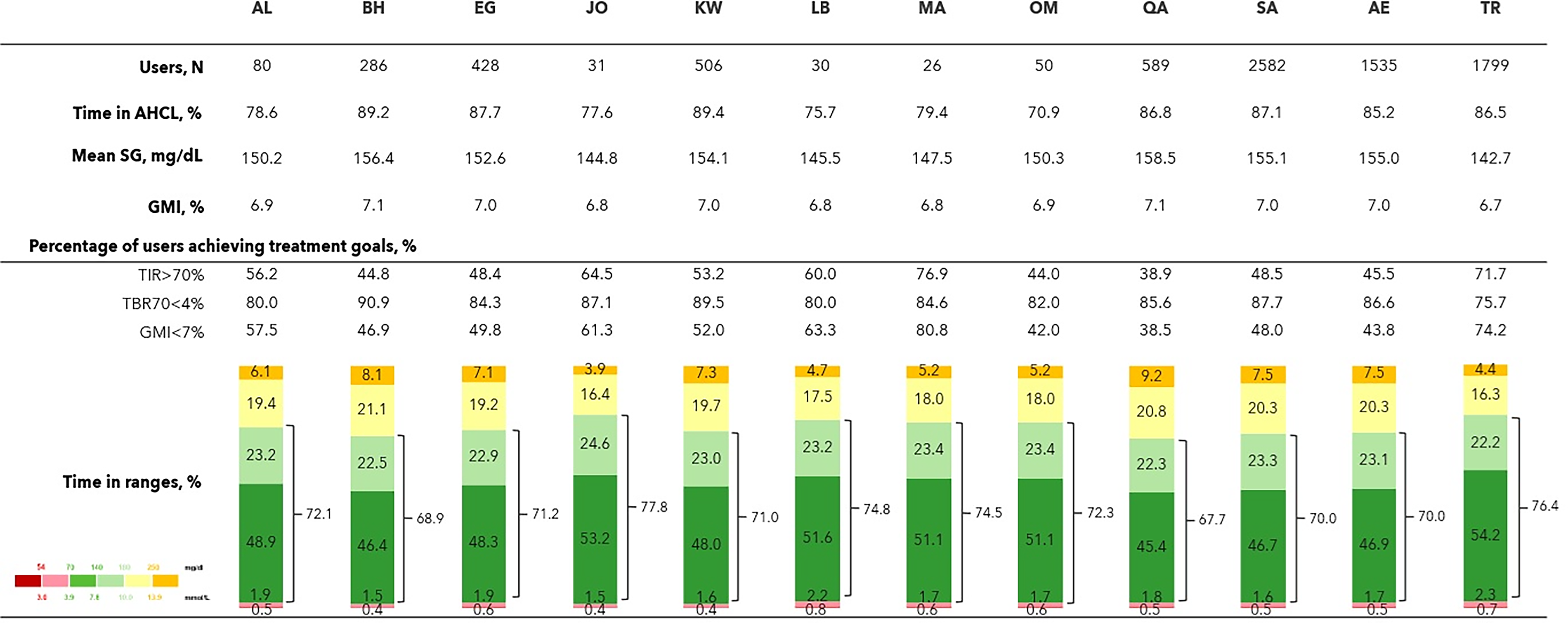
Continuous glucose monitoring outcomes from MiniMed™ 780G system users in MENAT (Middle East, North Africa, Türkiye) country-specific cohort. Results are displayed as mean for the following countries: AL, Algeria; BH, Bahrain; EG, Egypt; KW, Kuwait; LB, Lebanon; MA, Morocco; OM, Oman; QA, Qatar; SA, Saudi Arabia; AE, Union of Arab Emirates; TR, Türkiye.
In the time-specific subanalysis, all CGM metrics remained stable across the four seasons and between weekdays and weekends (Fig. 3). TIR remained above 71%, TITR exceeded 48.5%, GMI stayed at 7.0% or lower, and TBR70 was 2.5% or lower. In terms of international targets, over 52% of users achieved a GMI <7% and over 53% attained a TIR >70%. Regarding insulin, no meaningful changes were observed in the total daily insulin dose nor in the percentages of insulin delivered (by bolus [manually], by autobasal, or by autocorrection). In addition, glycemic control was comparable between daytime and nighttime. TIR was 71.1 ± 19.2% and 73.0 ±29.3%, respectively; TITR was 48.6 ± 20.2% and 49.3 ± 32.8%, respectively; TBR70 was 2.4 ± 4.4% and 2.3 ± 7.2%, respectively; and TAR180 was 26.5 ± 19.5% and 24.7 ± 29.4%, respectively.
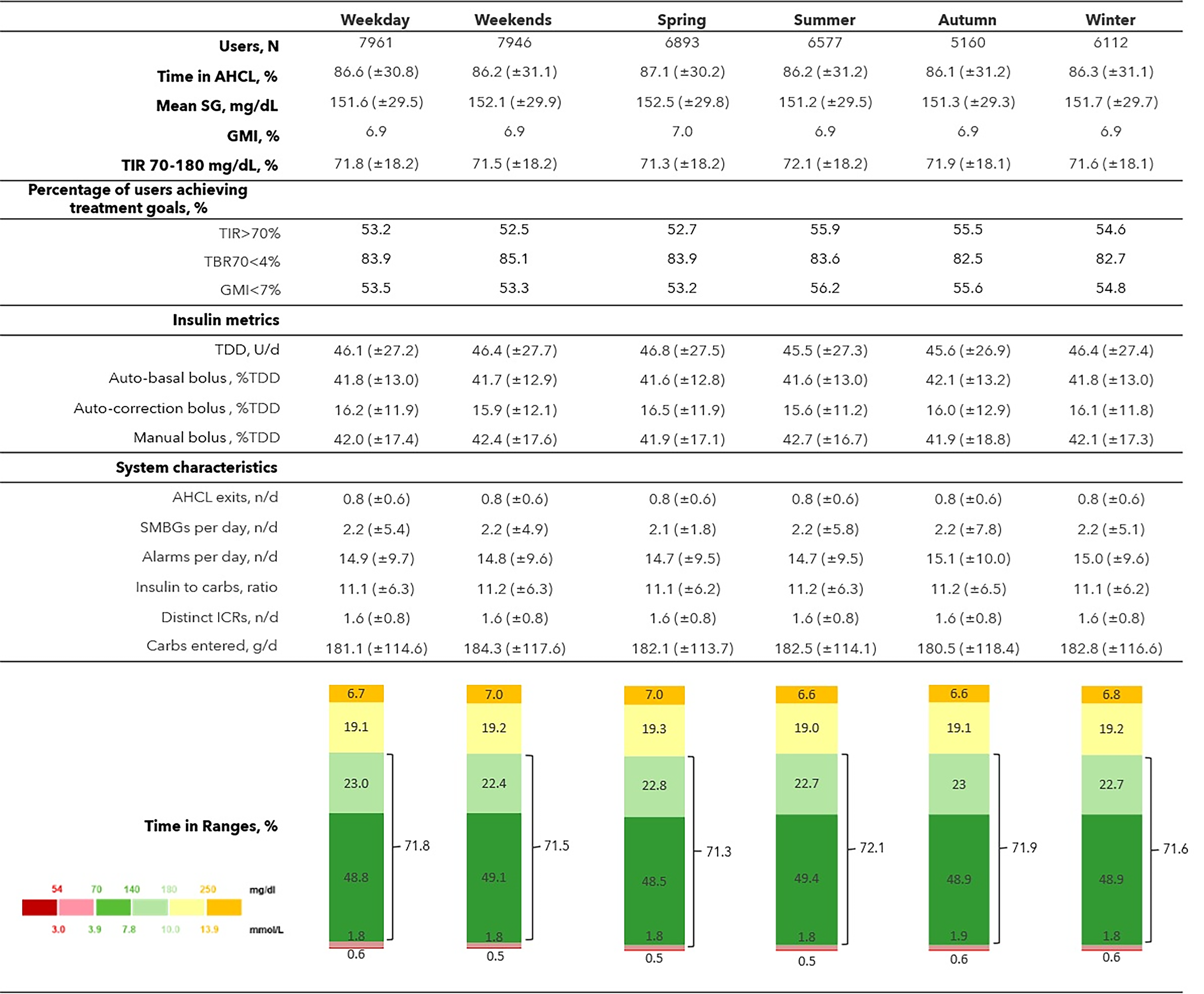
Continuous glucose monitoring outcomes in the MENAT region: day versus night hours, weekday versus weekends, and seasonal variations. Data are reported as mean (±SD), unless specified otherwise.
Cohort 2 (longitudinal cohort)
The sustainability of the MiniMed 780G system performance over 12 months (post-AHCL initiation) is presented in Figure 4. The 2303 users from this cohort on average had a GMI of 6.9 ± 0.6%, which was reached within the first month and sustained throughout the year. Their mean TIR in the first month was 73.7 ± 17.2% and remained above 70% over the 12 months. TBR70 and TBR54 remained below international targets in all months.
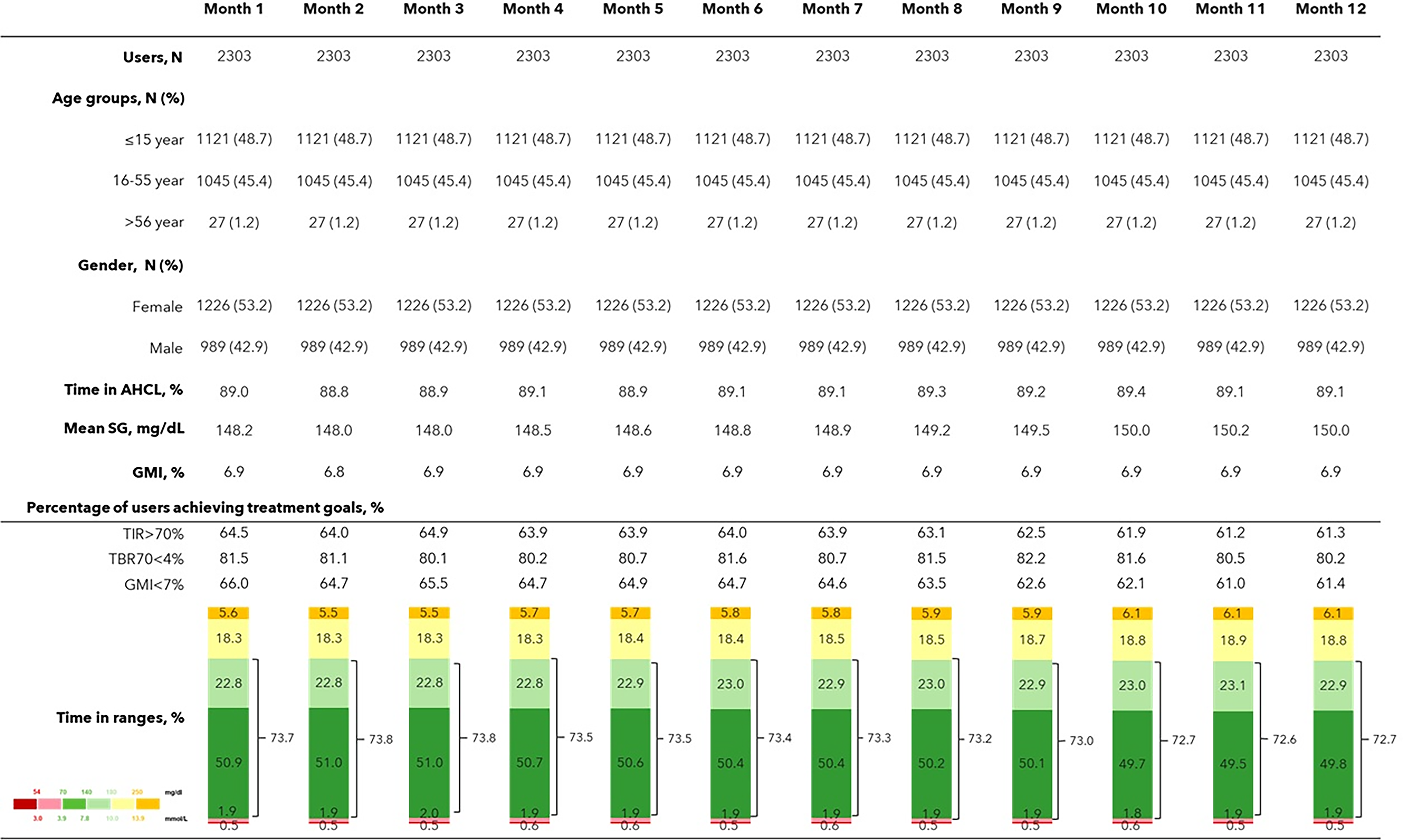
Glycemic control of real-world MiniMed™ 780G system MENAT users over 12 months. Data from users who have at least 10 days of SG data in each of the 12 months following AHCL initiation are considered and are displayed as mean (SD) unless specified otherwise.
Cohort 3 (pre–post cohort)
There were 1674 users who had at least 10 days of SG data both pre- and post-AHCL initiation. TIR and TITR improved from 56.1 ± 23.5% and 33.8 ± 20.7% to 71.3 ±18.1% and 48.5 ± 19.2%. GMI decreased from 7.5 ± 1.0% to 7.0 ± 0.7%. The percentage of users with GMI <7% increased from 24.5% to 51.6%, those with TIR >70% improved from 21.3% to 50.8%, and those with TBR70 <4% rose from 79.3% to 85.7% (Fig. 5).
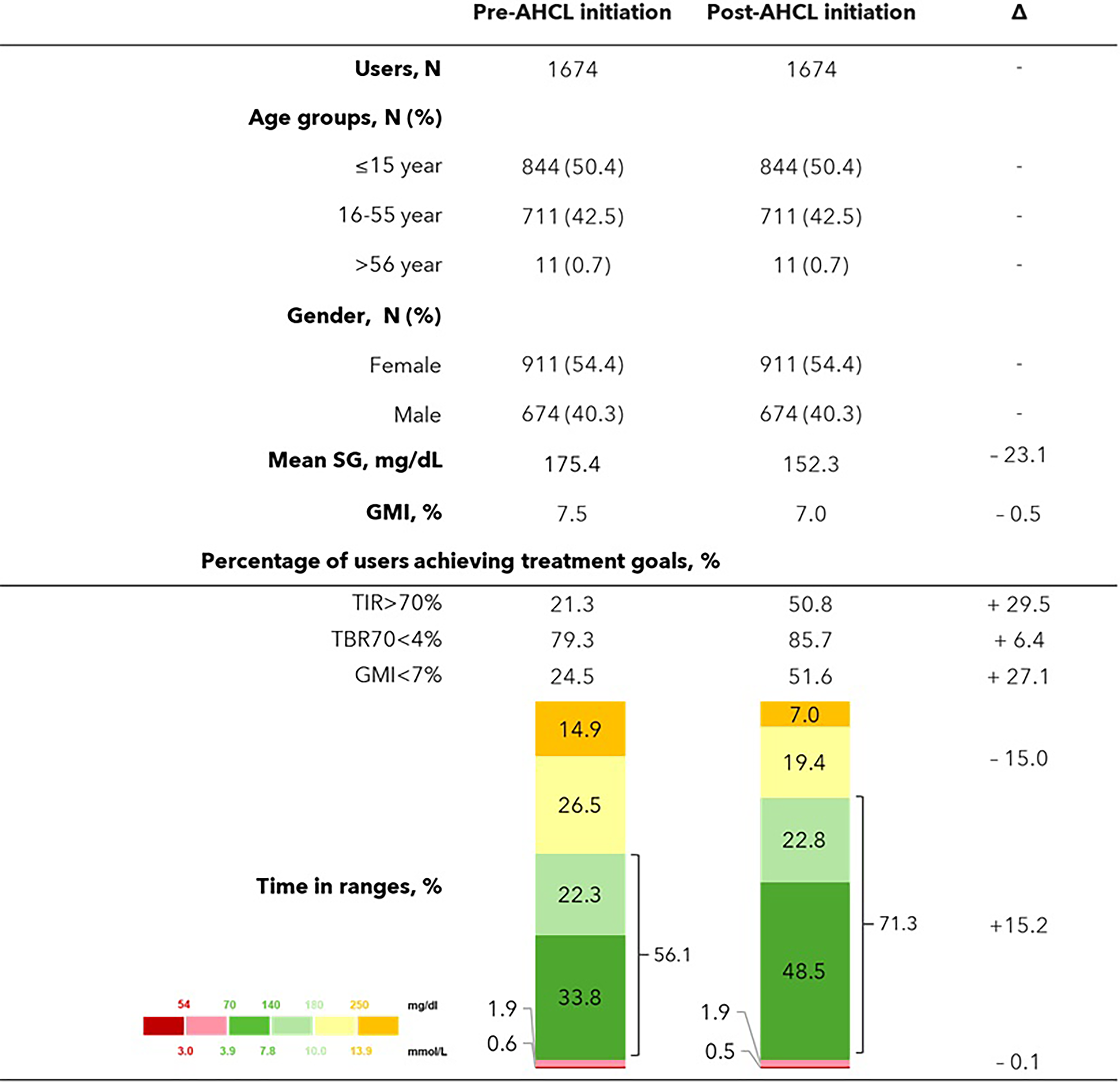
Glycemic outcomes and system use of Pre- and Post-AHCL initiation. Data from users who have at least 10 days of SG data both before and after transitioning to AHCL are considered and are displayed as mean. Mean change (Post-AHCL minus Pre-AHCL) is reported for all metrics and, specifically, for TAR, TIR, and TBR.
Discussion
The increasing adoption of the MiniMed 780G system has enabled comprehensive analyses of glycemic outcomes in real-world settings worldwide. In this study, we presented real-world evidence (RWE) on glycemic outcomes for 7965 MiniMed 780G system users from the MENAT region. The key findings were good glycemic control aligning with international targets (mean GMI of 6.9%, TIR of 71.7%, and TBR70 of 2.4%), and this was found to be consistent for at least 12 months.
Real-world data from Saudi Arabia indicate that people with T1D using FreeStyle Libre 1 with insulin pump therapy or multiple daily injections achieved a TIR of 50.5% at 12 months. 17 In a larger flash glucose monitoring cohort of 6097 users, those with high scanning frequency (≈32 scans/day) reached a TIR of 46.4%, compared with 32.8% among users with low scanning frequency (≈5 scans/day). 18 Similarly, a real-world study from Egypt during the COVID-19 pandemic reported that 42 children with T1D using insulin pumps and the Medtronic iPro2 CGM system achieved a median TIR of 57%, an improvement from 53% before the pandemic. 19 These comparisons highlight the additional glycemic benefit achieved with MiniMed 780G system relative to conventional treatment in the region.
The glycemic control in MiniMed 780G system users from the MENAT region is in line with that of other geographies. Choudhary et al., for instance, reported on over 100,000 users predominantly from Europe and found a mean TIR of 72.3%, a mean GMI of 7.0%, and a mean TBR70 of 2.0%. 7 Similar results were reported by Grassi et al. for Latin America. 20 The outcomes from the United States, as reported by Thrasher et al., were somewhat higher, with an average TIR of 77.0% and TBR70 of 1.6%. 21 This discrepancy may be attributed to the higher adoption rate of optimal settings within the U.S. region. Optimal settings are known to lead to a higher TIR, without compromising safety, and only 11.9% of MENAT users consistently used optimal settings (vs. 21.9% in the United States 21 ). This presents an opportunity to improve glycemic control through targeted initiatives aimed at understanding barriers to optimal pump settings and providing appropriate education. In some cases, such as during Ramadan fasting, both pump users and clinicians may feel more comfortable using lenient (suboptimal) settings to minimize risk of hypoglycemia. For instance, they may choose to raise the GT or increase the AIT during Ramadan and then forget to revert to the pre-Ramadan (optimal) settings afterward. Nonetheless, evidence shows that maintaining optimal settings is associated with improved glycemic outcomes even during Ramadan22–24 ; thus, educational efforts are required within the region to emphasize the importance of using optimal pump settings. The findings in this study also align with other real-world studies in terms of showing that glycemic control is sustainable for a long time and is better in older users.
The MiniMed 780G system seems capable of dealing with MENAT-specific cultural aspects. The study, for instance, found a high degree of consistency in TIR between daytime (71.1%) and nighttime (73.0%), which is not seen in RWE from other regions such as Europe and the United States. Arrieta et al., for instance, focusing mainly on European users of the system, reported substantial day–night variations; the nights were generally better controlled (81.9% vs. 73.7%), presumably due to rest and the absence of food intake overnight. 6 In many MENAT countries, it is common for individuals to consume larger or more frequent meals during the evening and nighttime hours, particularly during religious or social observances such as Ramadan. Moreover, the MENAT region is widely recognized as a climate “hot spot,” experiencing extremely high daytime temperatures, especially during the summer months. These conditions can discourage outdoor activity and heavy food consumption during the day, prompting a cultural shift toward eating and moving later in the evening or at night when temperatures are more tolerable. This adaptation may lead to a more even distribution of glycemic control in the 24-h cycle. Interestingly, changes in glycemic control were not observed between weekdays and weekend days nor between the seasons.
The findings from this study add to the growing body of evidence supporting the MiniMed 780G system’s ability to adapt to diverse and even abrupt lifestyle changes. A notable example is the study by Al-Sofiani et al., which monitored 449 real-world users before, during, and after Ramadan (in the Gulf region). 22 Glycemic control remained remarkably stable throughout, consistently achieving TIR levels above 70%, even during Eid al-Fitr. The system demonstrated rapid adaptability, maintaining good glucose control from the very first day of Ramadan and in the days following its conclusion. 22 Ramadan-specific (sub)-analyses were beyond the scope of this article.
The excellent and sustained glycemic control demonstrated in this study may help support broader adoption of diabetes technology in the MENAT region. Currently, only approximately ∼4%–5% of people with T1D in MENAT use an AID system, based on commercial data from Medtronic pump users and prevalence estimates by Gregory et al. 25 These adoption rates vary substantially between countries, due to differences in reimbursement systems. Several barriers contribute to the low uptake of diabetes technology in the region. Direct costs remain a major obstacle, as devices and consumables are often more expensive than conventional therapies, such as multiple daily injections combined with self-monitoring of blood glucose. Additionally, there is a lack of region-specific data on AID system performance, and few, if any, studies evaluate their (potential) cost-effectiveness in local health care settings. Furthermore, a shortage of trained adult and pediatric endocrinologists and diabetes educators across many MENAT countries exacerbates the situation. 26 Given the high prevalence of diabetes in the region, health care professionals are often overburdened, with limited time and resources for training in newer technologies.
Our analysis has several strengths, most notably the inclusion of a large cohort of users from multiple countries across the MENAT region and the use of a well-established and well-described methodology. To our knowledge, this is the first study of its kind conducted in the MENAT region. However, several limitations should be acknowledged. Data were obtained through the CareLink Personal platform, which introduces inherent constraints. First, the lack of baseline information regarding prior diabetes therapies limits our ability to comprehensively assess the incremental clinical benefit of transitioning to the MiniMed 780G system. Second, key sociodemographic characteristics—such as age, gender, and diabetes type—are self-reported. Given the lack of MiniMed 780G system reimbursement in some countries, we expect an overrepresentation of users from a good socioeconomic background. Third, the extent and potential impact of missing data remain uncertain. Fourth, HbA1c measurements were not available, necessitating reliance on CGM metrics as a surrogate metric for long-term glycemic control. Last, safety evaluation was limited, with no available data on acute complications such as severe hypoglycemia or diabetic ketoacidosis.
Conclusions
Real-world data from 7965 MiniMed 780G system users in MENAT showed a glycemic control that achieved international target criteria; was sustainable across different age groups, countries, extreme climates, and over time; and was comparable to real-world data from other geographies. The results from this study may help increase access to and adoption of advanced diabetes technology in MENAT.
Authors’ Contributions
All authors were involved in the design, analysis of data, writing, and review of the article.
Footnotes
Acknowledgments
This study was sponsored by Medtronic. The authors thank Fabrizio Fabbiano and Paola Cardano for their assistance with preparing this article in its final version. Both are Medtronic employees.
Author Disclosure Statement
M.E.A.-S. has served on advisory panels for Abbott, Medtronic, Insulet, VitalAire, and Sanofi and has received honoraria for speaking and consultancy from Abbott, Eli Lilly, Medtronic, Novo Nordisk, Sanofi, and VitalAire. W.C., T.v.d.H., O.C., and G.P. are employees of Medtronic.
Funding Information
The research was funded by Medtronic.