
Abstract
Background:
On completion of the INHALE-1 randomized controlled trial (RCT), an extension phase was completed to provide longer term safety data on use of technosphere insulin (TI) in children with diabetes.
Methods:
In the RCT, 4- to 17-yr-olds with type 1 (98%) or type 2 (2%) diabetes treated with multiple daily injections of insulin were randomly assigned to TI or rapid-acting analog (RAA) plus continuation of long-acting basal insulin and continuous glucose monitoring (CGM). After 26 weeks, participants were provided the option to continue in an extension phase through 52 weeks in which TI was used by both treatment groups.
Results:
In the TI group (N = 80), mean HbA1c was 8.1 ± 0.8% at the start of the RCT, 8.2 ± 1.2% at 26 weeks, and 8.6 ± 1.2% at 52 weeks (mean change from 26 to 52 weeks = 0.38%, 95% confidence interval [95% CI] 0.08%–0.67%, P = 0.003). In the RAA Crossover group (N = 88), mean HbA1c was 8.1 ± 1.1% at TI initiation (RCT week 26) and 8.4 ± 1.4% at 52 weeks (mean change = 0.31%, 95% CI −0.02%–0.64%, P = 0.08). There were no serious or unexpected pulmonary-related adverse events. The change in mean percent predicted forced expiratory volume in 1 s from the start of TI to 4 weeks after discontinuation was −0.5 (95% CI −1.9–0.9, P = 0.52) when combining the entire periods of TI exposure for both groups. CGM-measured time < 54 mg/dL was very low during TI use (TI group: 0.39 ± 0.61%; RAA Crossover group: 0.45 ± 0.59%).
Conclusions:
The INHALE-1 extension phase showed no safety concerns. Although HbA1c levels deteriorated slightly during the study, in view of the safety profile and increased patient satisfaction in the RCT portion of the trial, TI may be a useful treatment option for some pediatric patients with diabetes, particularly for those who choose not to or are unable to use an AID system.
Introduction
Mean HbA1c remains >8.5% in youth with diabetes, and only a minority meet the American Diabetes Association target of HbA1c <7.0%. 1 The delayed onset of action of rapid-acting analog (RAA) insulin impacts the postmeal glucose rise, especially if not dosed 10–15 min before meal consumption. This rise is an important contributor to elevated HbA1c levels, and the prolonged duration of action of RAA insulin limits the ability to administer postprandial correction doses due to the risk of stacking and subsequent hypoglycemia.
Technosphere insulin (TI) inhalation powder (Afrezza®, MannKind Corporation, Danbury, CT) has been shown in pharmacokinetic studies to have both a more rapid onset of action and more rapid dissipation of effect than subcutaneous RAA insulin.2,3 Thus, inhaled TI can potentially reduce the risks of both postmeal hyperglycemia and subsequent hypoglycemia.4,5 A pharmacokinetics study in children demonstrated no safety concerns of TI and an insulin action profile similar to what has been reported for adults. 6 TI was approved by the Food and Drug Administration for adults with diabetes in 2014; in recent years regulatory approval has also been received in Brazil and India.
To evaluate the efficacy and safety of TI in children, we conducted a multicenter 26-week randomized controlled trial (RCT) in 230 4- to17-yr-olds with diabetes who were using multiple daily injections (MDI) for insulin delivery. Participants were randomly assigned to either TI or RAA, with continuation of basal insulin and use of real-time continuous glucose monitoring (CGM). At 26 weeks, changes in HbA1c and time-in-range (TIR) 70–180 mg/dL were not significantly different between groups. However, the prespecified criteria for noninferiority of TI to RAA were not met in the intent-to-treat analysis, although it was met in a prespecified per-protocol analysis. TI use was safe over 26 weeks without impacting pulmonary function and was associated with significantly greater treatment satisfaction and less weight gain compared with RAA.
On completion of the 26-week RCT, participants continued in a 30-week extension study in which the TI group continued to use the TI insulin regimen and the RAA group switched to use of the TI regimen for 26 weeks, followed by a 4-week off-treatment safety visit. The objectives of the extension phase were to assess the safety of TI over 52 weeks in the RCT TI group and to provide additional safety and efficacy data using TI by the RCT RAA group.
Methods
The study was conducted at 38 pediatric diabetes centers in the United States. The protocol (clinicaltrials.gov NCT), which included both the 26-week RCT and the subsequent 30-week extension phase, was approved by a central institutional review board. Informed consent was obtained from the parent or guardian of each participant and assent from participants ≥7 yrs of age.
The methods of the RCT have been previously published. 7 In brief, the study cohort included youth aged 4 to <18 yrs old with a clinical diagnosis of type 1 diabetes (T1D) for ≥6 months or type 2 diabetes (T2D) for at least 3 months using an MDI insulin regimen and HbA1c of 7.0%–11.0%. Following the collection of baseline CGM data, participants were randomly assigned 1:1 to TI or RAA insulin for meal boluses and corrections plus continuation of long-acting basal insulin for 26 weeks. Participants were provided with Dexcom G6 sensors to use throughout the study.
During the 26-week treatment period of the extension phase, the TI group continued to use TI for meals and corrections, and the RAA group switched to use TI, along with basal insulin and continued use of CGM. For the RAA group, the protocol paralleled that followed by the TI group in the RCT for initiating TI and titrating the TI and basal insulin doses. 7 CGM alarms were set at investigator discretion.
For both groups, clinic visits were held during the extension phase after 13 weeks (study week 39) and 26 weeks (study week 52) with a virtual visit after 19 weeks (study week 45). The TI group had an additional virtual visit after 6 weeks (study week 32). The RAA group initiating TI had an additional clinic visit after 1 week (study week 27) and virtual visits after 2, 4, and 6 weeks (study weeks 28, 30, and 32). Both groups discontinued TI at the 52-week visit and were transitioned back to their prestudy insulin regimen or an alternative regimen. A final safety visit was conducted 4 weeks post-TI discontinuation in study week 56.
The occurrence of adverse events was solicited at each visit or contact. At the study weeks 39 and 52 visits, HbA1c was measured at a central laboratory, and spirometry was performed to assess forced expiratory volume in 1 s (FEV1). FEV1 was also measured at study week 56 (4 weeks after discontinuation of TI). Participants ≥13 yrs old completed the Diabetes Treatment Satisfaction Questionnaire (DTSQs) and the DTSQc at study week 52. A parent or guardian of participants <13 yrs old completed the parent version of the surveys. Participants discontinuing TI before study week 52 had a final study visit with completion of the testing specified for week 52.
Study outcomes and statistical methods
HbA1c at study week 52 was the primary outcome. Additional outcomes included binary HbA1c outcomes, CGM metrics, and DTSQ(c) scores. Safety outcomes included all reported adverse events, severe hypoglycemia (defined as severe neuroglycopenia usually resulting in loss of consciousness, coma, or a seizure requiring external assistance by another person to actively administer carbohydrates or glucagon or take other corrective actions), diabetic ketoacidosis (DKA), other serious adverse events, and change in percent predicted FEV1 on pulmonary function testing.
The two treatment groups were analyzed separately. For the TI group, statistical comparisons were made between RCT baseline and 52 weeks and between 26 and 52 weeks.
For the RAA group, baseline was considered to be the RCT 26-week visit, with statistical comparisons made between this baseline and study week 52 (after 26 weeks in the extension phase). FEV1 comparisons were made between baseline and week 56 and between week 52 and week 56. Continuous end points were analyzed using paired t-tests; if the outcome change was not normally distributed, a generalized linear regression model with the t-distribution was used instead. Binary end points were analyzed using McNemar’s tests.
Only participants completing the extension phase who did not discontinue TI were included in the efficacy analyses; all participants who initiated the extension phase were included in the safety analyses. CGM metrics were calculated at baseline, 26 weeks, and 52 weeks for the TI group and 26 weeks and 52 weeks for the RAA group by pooling all available data in the 30 days before the visit date. A minimum of 168 h of data was required to calculate metrics.
For all comparisons, the false discovery rate was controlled using the adaptive Benjamini–Hochberg procedure, separately for the two treatment groups. SAS version 9.4 was used for the analyses.
Results
Among the 117 participants randomly assigned to the TI group, 105 completed the 26-week RCT visit, and 88 continued using TI in the extension phase. Among the 113 participants randomly assigned to the RAA group, 108 completed the 26-week RCT visit, and 104 initiated TI in the extension phase (Supplementary Fig. S1). Characteristics of the participants in the extension phase are shown in Table 1.
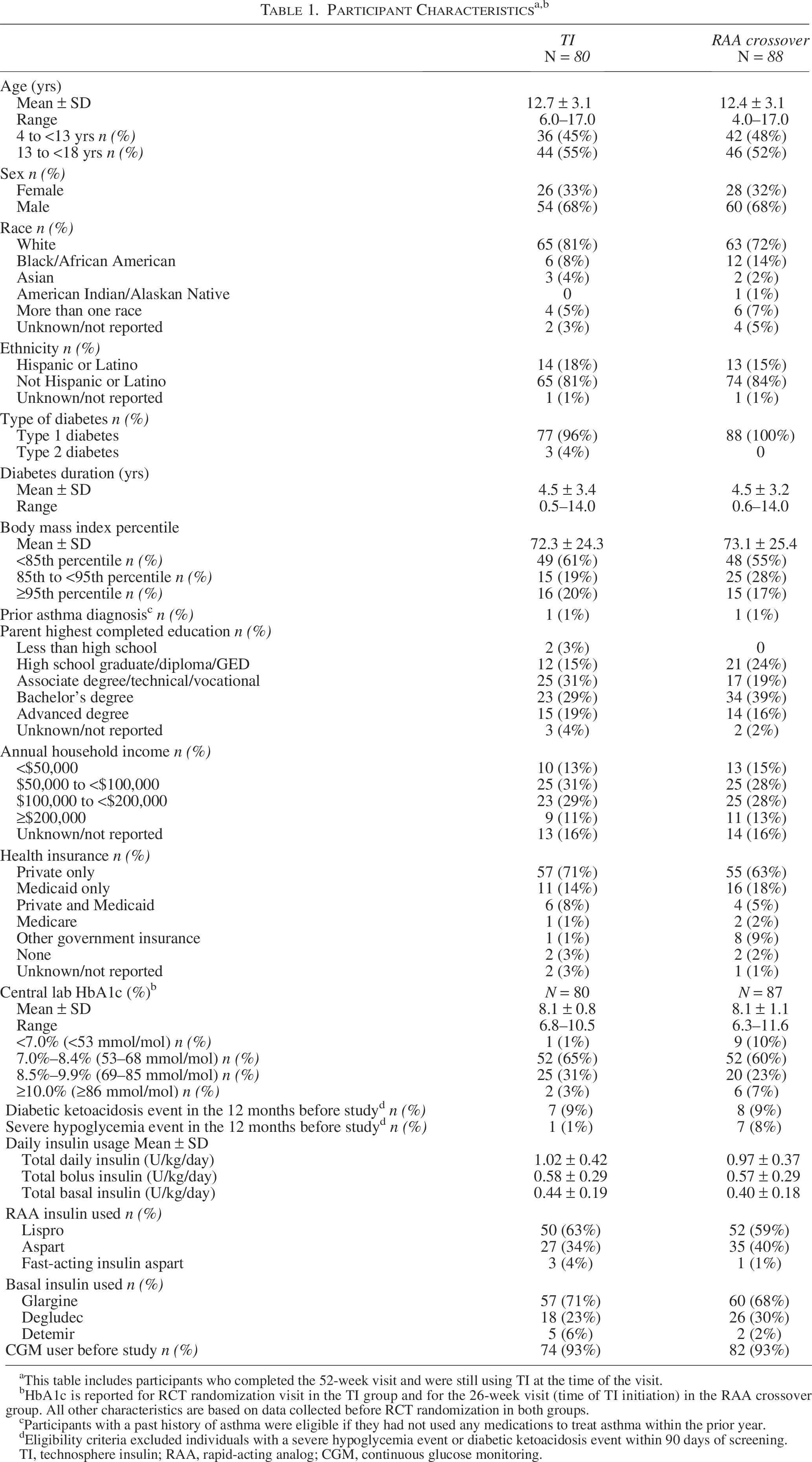
This table includes participants who completed the 52-week visit and were still using TI at the time of the visit.
HbA1c is reported for RCT randomization visit in the TI group and for the 26-week visit (time of TI initiation) in the RAA crossover group. All other characteristics are based on data collected before RCT randomization in both groups.
Participants with a past history of asthma were eligible if they had not used any medications to treat asthma within the prior year.
Eligibility criteria excluded individuals with a severe hypoglycemia event or diabetic ketoacidosis event within 90 days of screening.
TI, technosphere insulin; RAA, rapid-acting analog; CGM, continuous glucose monitoring.
The 52-week visit was completed by 85 (97%) of the 88 in the TI group who continued in the extension phase and by 99 (95%) of 104 in the RAA Crossover group who initiated TI at the 26-week visit. An additional 5 in the TI group and 11 in the RAA Crossover group discontinued TI prior to their completing the 52-week visit. Reasons for early study or TI discontinuation for 24 (12.5%) of 192 participants who used TI in the extension phase included an adverse event related to inhalation in 6, adverse event unrelated to TI in 4, dissatisfaction with glucose control or switching to an insulin pump in 11, a positive cotinine test in 1, site withdrawal for safety in 1, and loss to follow-up in 1 (Supplementary Table S1).
Glargine was the most frequent basal insulin that was used. At the end of the trial, basal insulin use in the TI group was 59% glargine, 36% degludec, and 5% detemir, and in the RAA Crossover group, it was 67%, 32%, and 1%, respectively. Among glargine users, U100 was used by 96% in the TI group and by 98% in the RAA Crossover group, and U300 by 4% and 2%, respectively; glargine was injected once a day by 85% in the TI group and 86% in the RAA Crossover group and twice a day by 15% and 12%, respectively (missing data for one participant).
Glycemic outcomes
In the TI group, mean HbA1c was 8.1 ± 0.8% at the start of the RCT, 8.2 ± 1.2% at 26 weeks, and 8.6 ± 1.2% at 52 weeks (Table 2, Fig. 1, Supplementary Fig. S2). Mean change in HbA1c from RCT baseline to 52 weeks was 0.46% (95% confidence interval [95% CI] 0.22%–0.71%, P = 0.001), with most of the worsening occurring between 26 weeks and 52 weeks, where the mean change was 0.38% (95% CI 0.08%–0.67%, P = 0.003). Between baseline and 52 weeks, 13 (16%) participants improved HbA1c by >0.5% and 32 (41%) worsened by >0.5% (Supplementary Table S2). The HbA1c level was <7.0% in 1 (1%) at baseline, 9 (11%) at 26 weeks, and 5 (6%) at 52 weeks (Supplementary Table S3). Mean TIR was 44 ± 14% at RCT baseline, 42 ± 15% at 26 weeks, and 38 ± 15% at 52 weeks (Table 2). CGM outcomes during daytime and nighttime are shown in Supplementary Table S4.
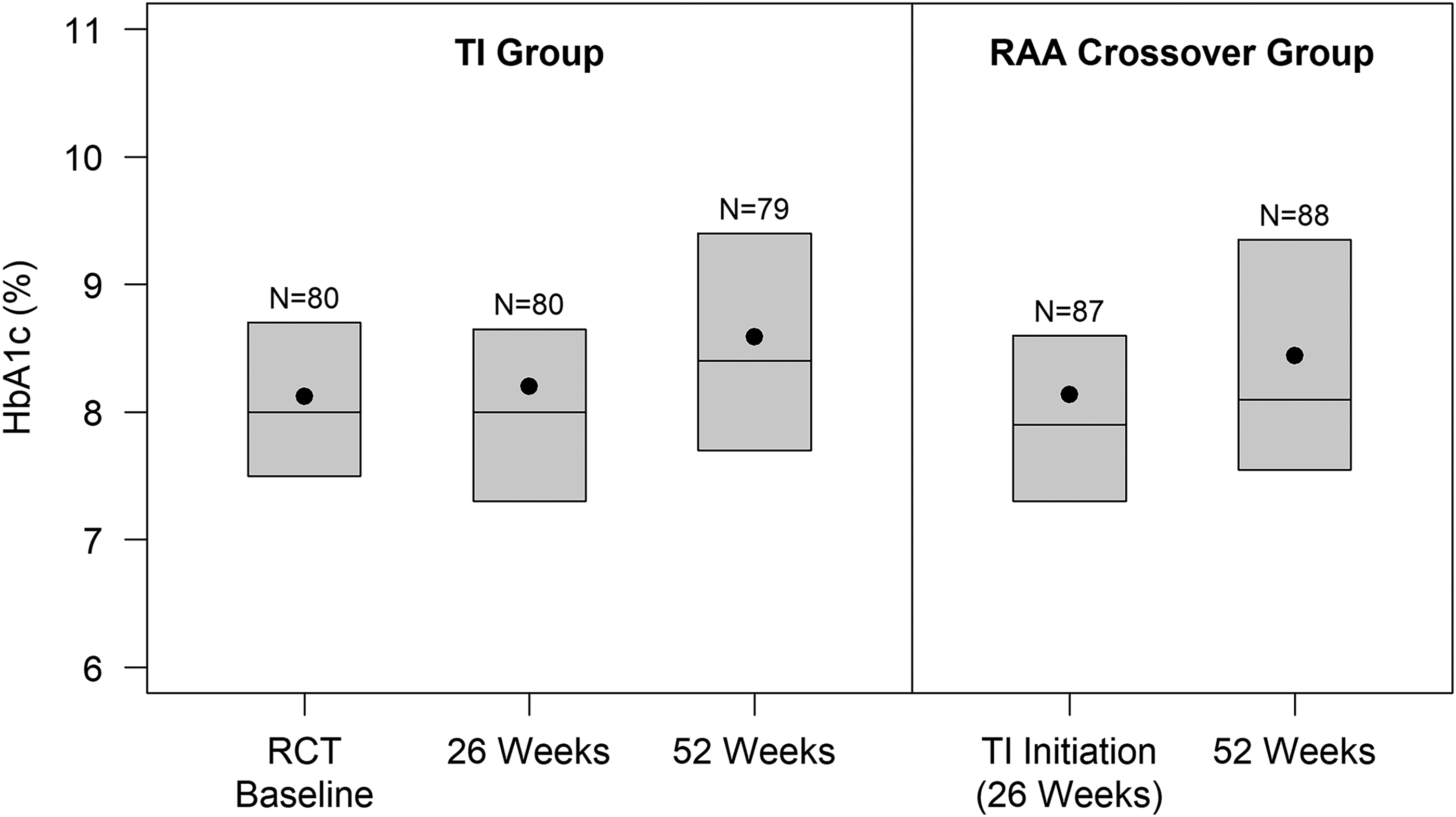
Boxplots of HbA1c by visit.
HbA1c and Continuous Glucose Monitoring Outcomes in the Technosphere Insulin Group
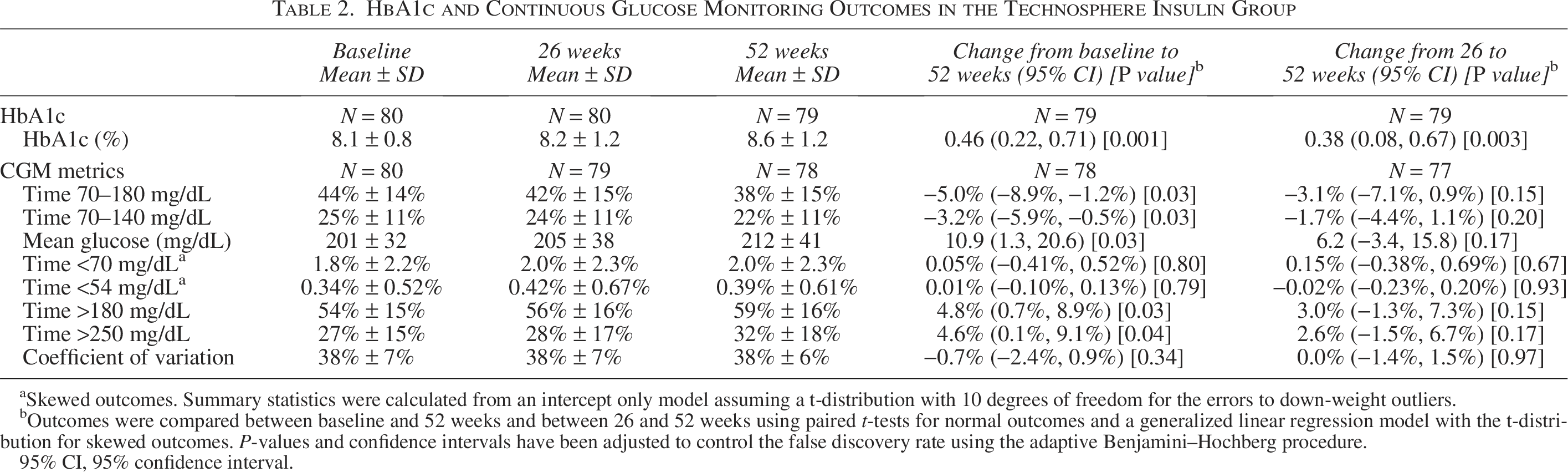
Skewed outcomes. Summary statistics were calculated from an intercept only model assuming a t-distribution with 10 degrees of freedom for the errors to down-weight outliers.
Outcomes were compared between baseline and 52 weeks and between 26 and 52 weeks using paired t-tests for normal outcomes and a generalized linear regression model with the t-distribution for skewed outcomes. P-values and confidence intervals have been adjusted to control the false discovery rate using the adaptive Benjamini–Hochberg procedure.
95% CI, 95% confidence interval.
In the RAA Crossover group, mean HbA1c was 8.1 ± 1.1% at the start of the initiation of TI (RCT week 26) and 8.4 ± 1.4% at 52 weeks. Mean HbA1c change from RCT week 26–52 was 0.31% (95% CI −0.02%–0.64%, P = 0.08) (Table 3, Fig. 1, Supplementary Fig. S2). HbA1c improvement from 26 to 52 weeks >0.5% occurred in 15 (17%), and HbA1c worsening >0.5% occurred in 34 (39%) (Supplementary Table S5). The HbA1c level was < 7.0% in 9 (10%) at 26 weeks and 11 (13%) at 52 weeks (Supplementary Table S6). Mean TIR was 42 ± 14% at 26 weeks and 40 ± 14% at 52 weeks (Table 3). CGM outcomes during daytime and nighttime are shown in Supplementary Table S7.
HbA1c and Continuous Glucose Monitoring Outcomes in the Rapid-Acting Analog Crossover Group
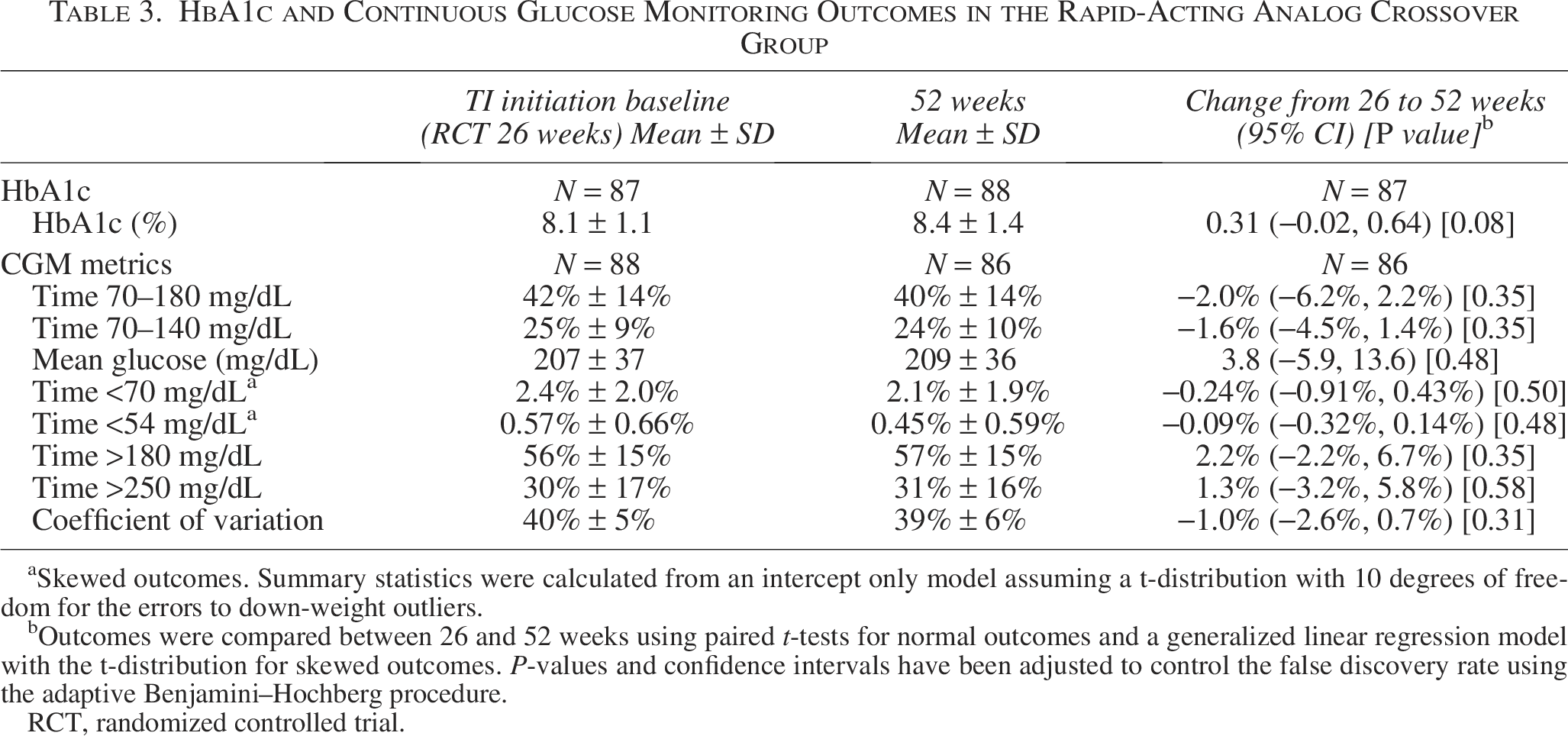
Skewed outcomes. Summary statistics were calculated from an intercept only model assuming a t-distribution with 10 degrees of freedom for the errors to down-weight outliers.
Outcomes were compared between 26 and 52 weeks using paired t-tests for normal outcomes and a generalized linear regression model with the t-distribution for skewed outcomes. P-values and confidence intervals have been adjusted to control the false discovery rate using the adaptive Benjamini–Hochberg procedure.
RCT, randomized controlled trial.
In both the TI and the RAA Crossover groups, a slight worsening in mean HbA1c was observed in all subgroups. There was a suggestion of greater worsening in participants with body mass index (BMI) in the obese range (Figs. 2 and 3).
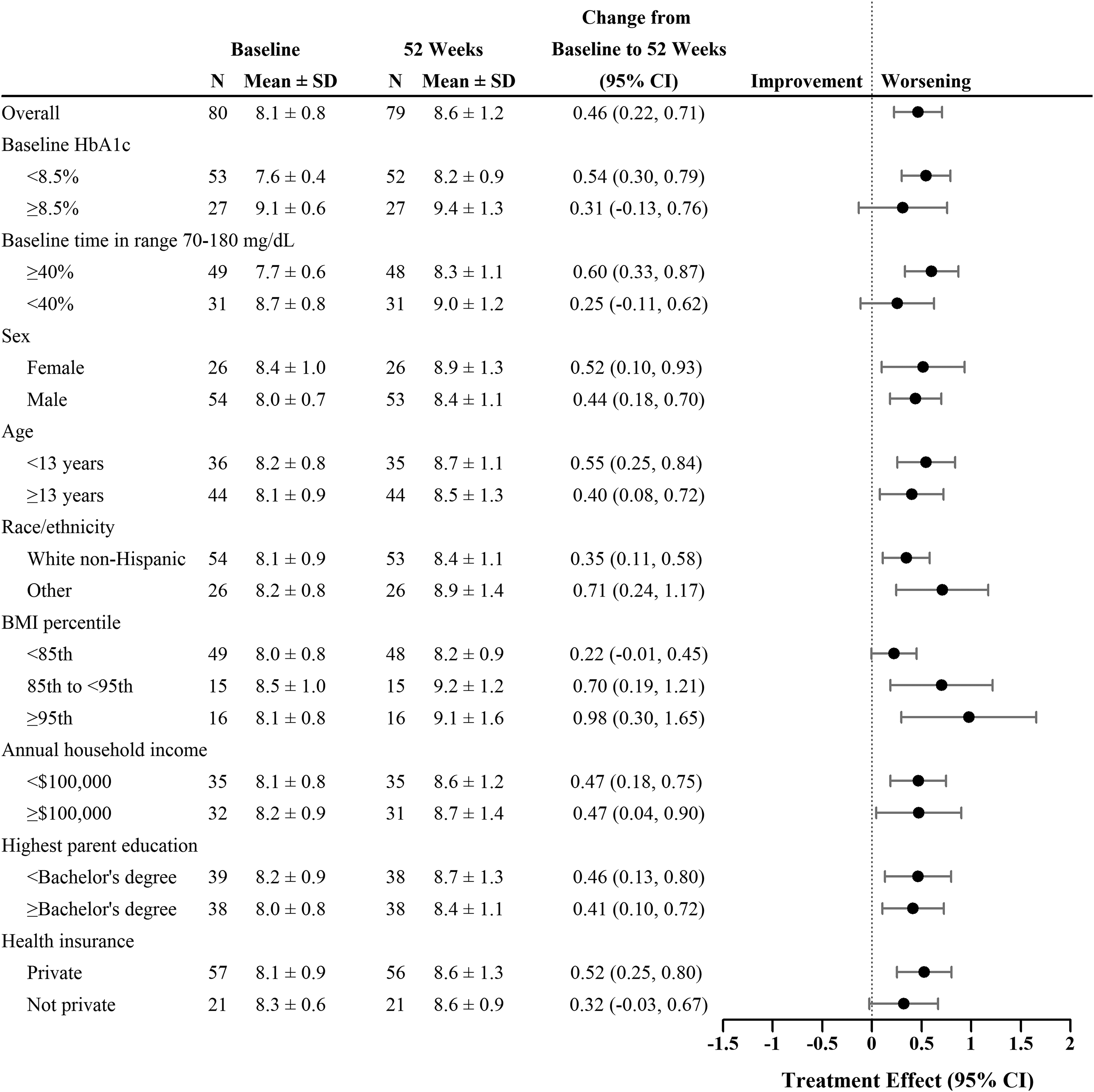
Forest plot of HbA1c according to participant characteristics in the TI group. TI, technosphere insulin.
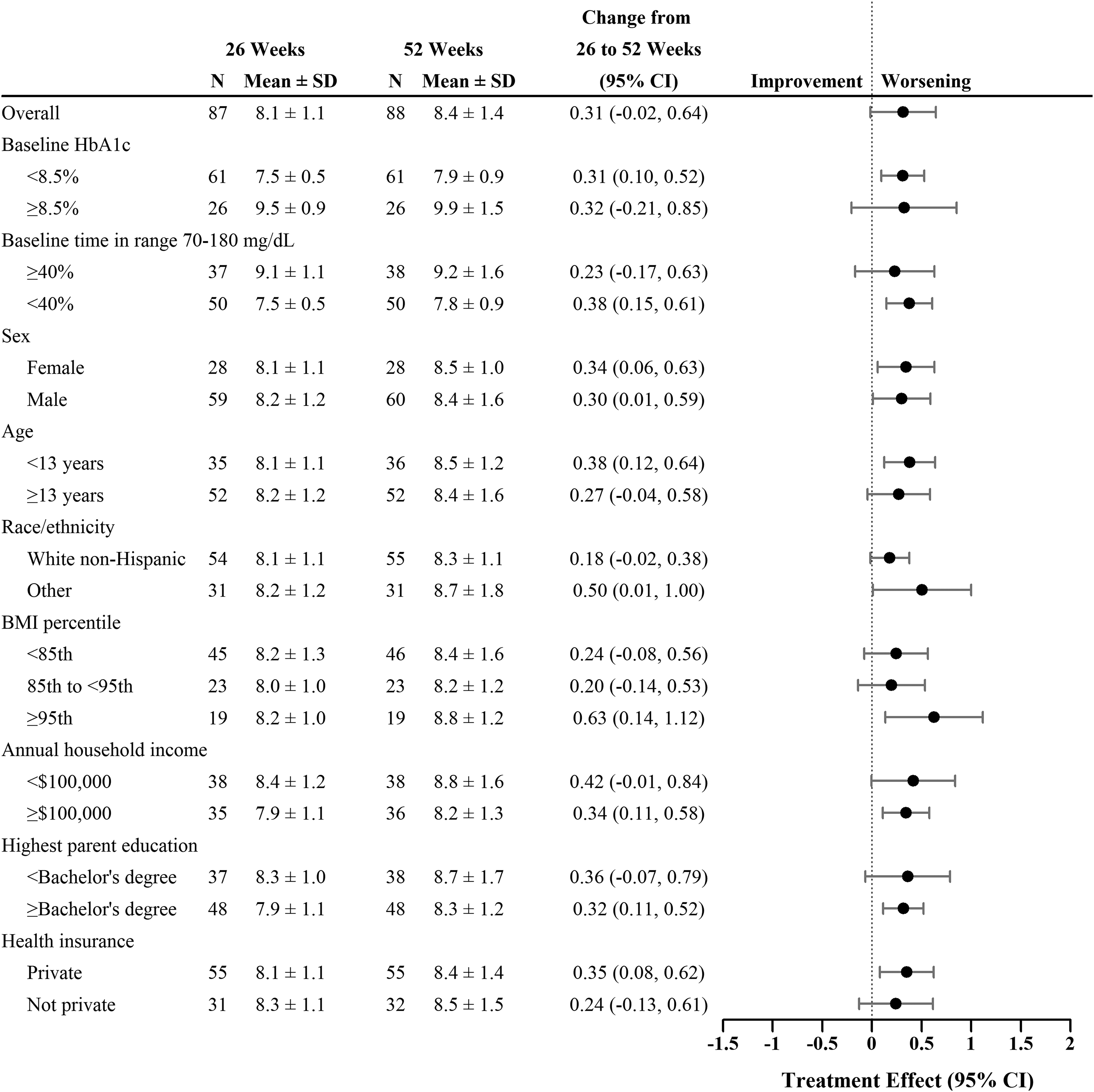
Forest plot of HbA1c according to participant characteristics in the RAA Crossover group. RAA, rapid-acting analog.
Insulin dosing and weight change
In the TI group, median daily TI dose was 1.33 units/kg/day at week 26 and 1.32 units/kg/day at week 52. The median ratio of the TI dose at 26 weeks to the RAA dose at RCT baseline before switching to TI was 2.61, and the ratio of the 52-week TI dose to RCT baseline RAA dose was 2.86. Median total daily basal insulin dose was 0.45 units/kg/day at week 26 and 0.51 units/kg/day at week 52 (Supplementary Table S8). In the RAA crossover group, the median total TI dose at 52 weeks was 1.16 units/kg/day. The ratio of the 52-week TI dose to 26-week RAA dose was 2.41. Median total daily basal insulin dose was 0.40 units/kg/day at week 26 and 0.42 units/kg/day at week 52 (Supplementary Table S9).
The clinical site assessed that the participant was adherent with the prescribed TI regimen at all visits between weeks 26 and 52 in 64 (80%) of the 80 participants in the TI group and in 63 (72%) of the 88 participants in the RAA Crossover group (Supplementary Table S10).
In the TI group, mean BMI percentile was 72 ± 24 at the RCT baseline, 70 ± 26 at 26 weeks, and 72 ± 26 at 52 weeks (mean change from baseline to 52 weeks −0.4, 95% CI −2.9–2.2, P = 0.78), whereas in the RAA Crossover group, mean BMI percentile was 76 ± 24 at 26 weeks when TI was initiated and 73 ± 27 at 52 weeks (mean change from 26 weeks to 52 weeks −2.8, 95% CI −4.6 to −1.1, P = 0.002). An analysis using BMI z-scores produced similar results (Supplementary Table S11).
Participant-reported outcomes
In the TI group, treatment satisfaction subscale scores suggested an increase in treatment satisfaction from RCT baseline to 52 weeks for both the teenagers (13–17 yrs old) and parents of younger participants (P = 0.02), with the increase being observed between the RCT baseline and 26 weeks, followed by little change between 26 weeks and 52 weeks (Supplementary Table S12). No significant or meaningful changes were present for the perceived diabetes control and the perceived frequency of hypoglycemia subscales.
In the RAA Crossover group, there were no significant changes in any of the three subscales between 26 weeks (when TI was initiated) and 52 weeks (Supplementary Table S13).
Safety outcomes
During the extension phase, 151 adverse events were reported for 60 (68%) of the 88 participants in the TI group (Supplementary Table S14), of which 12 were considered possibly related to TI (10 of 12 were asymptomatic reductions in pulmonary function test results that met the definition of a reportable adverse event). In the RAA Crossover group, 254 events were reported for 79 (76%) of 104 participants, of which 45 were considered possibly related to TI (Supplementary Table S15). Inhalation-related cough was the most common of these adverse events, reported by 18 (17%) of the 104 participants in the RAA Crossover group.
Severe hypoglycemia events occurred in 1 participant in the TI group (3 events) and 1 participant in the RAA Crossover group (1 event). In three of the four events, severe hypoglycemia occurred many hours after the last TI dose and may have been related to too high a basal insulin dose. In one case, the event occurred shortly after a TI correction dose, but the amount of TI received on the day of the event was no different than prior days. Mean percent time < 54 mg/dL was very low in both groups throughout the course of TI use. Mean change from RCT baseline to 52 weeks was 0.01% in the TI group, and from TI initiation to 52 weeks in the RAA Crossover group, it was −0.09%.
One DKA event occurred in each of two participants in the RAA Crossover group (HbA1c at time of TI initiation 9.1% and 8.6%). In neither case was a concomitant illness present, and there was no precipitating cause identified, suggesting that the cause may have been nonadherence with their insulin regimen.
Other serious adverse events occurred in three participants in the RAA Crossover group but in none of the participants in the TI group (Supplementary Table S16).
As shown in Table 4, there was little change in percent predicted FEV1 in both the TI group and the RAA Crossover group. Combining the entire periods of TI exposure for both groups, mean change from the start of TI to 4 weeks after discontinuation was −0.5% (95% CI −1.9%–0.9%, P = 0.52).
Percent Predicted Forced Expiratory Volume in 1 s in Both Groups
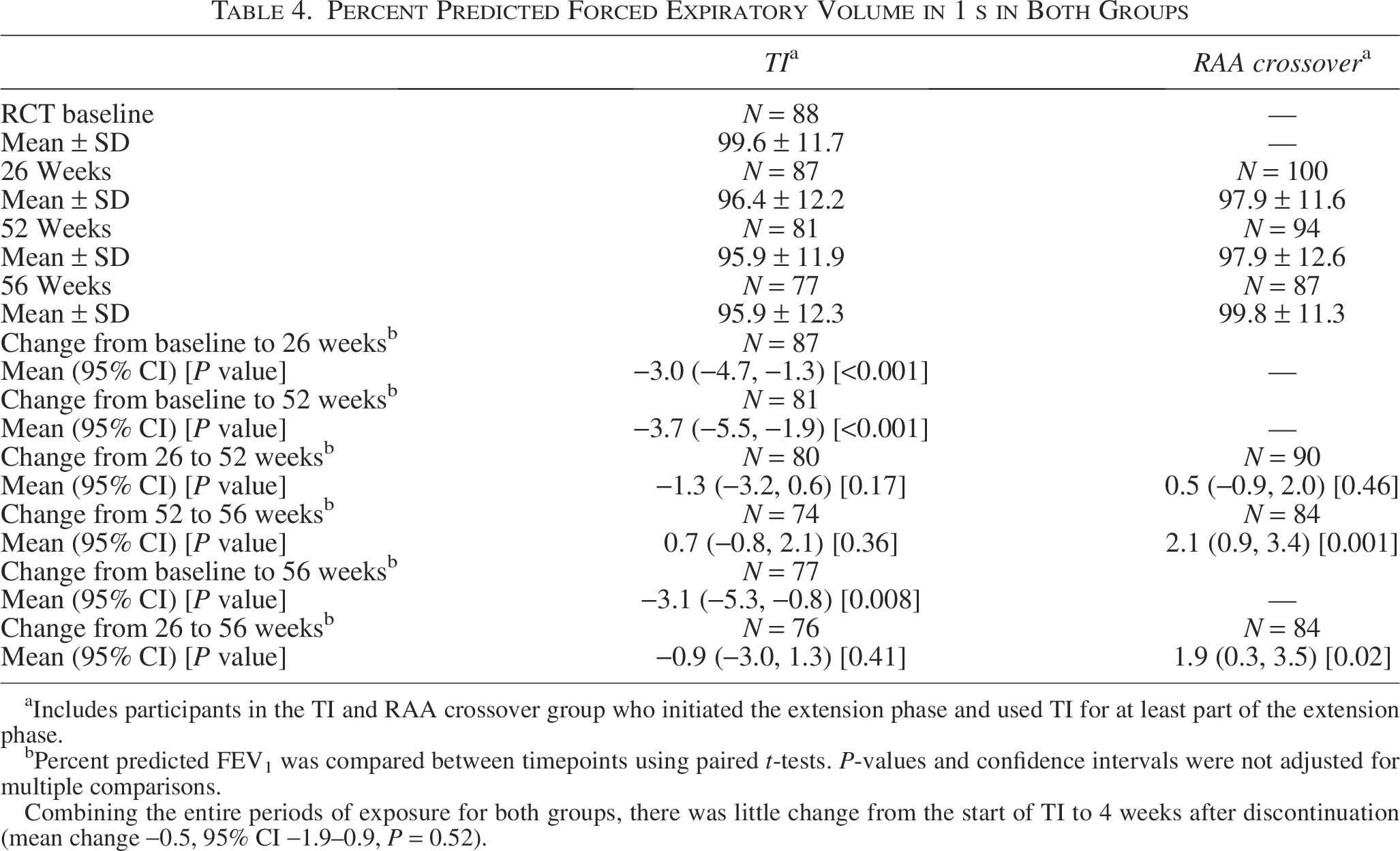
Includes participants in the TI and RAA crossover group who initiated the extension phase and used TI for at least part of the extension phase.
Percent predicted FEV1 was compared between timepoints using paired t-tests. P-values and confidence intervals were not adjusted for multiple comparisons.
Combining the entire periods of exposure for both groups, there was little change from the start of TI to 4 weeks after discontinuation (mean change −0.5, 95% CI −1.9–0.9, P = 0.52).
Discussion
During this 26-week extension following the 26-week INHALE-1 RCT, there was slight glycemic worsening in both the RCT TI group that continued use of TI and the RAA Crossover group that initiated TI at the commencement of the extension phase. In the TI group, mean HbA1c, after showing little change during the first 26 weeks, worsened between 26 and 52 weeks by 0.38%. For the RAA Crossover group, mean HbA1c worsened by 0.31% from 26 to 52 weeks. These findings were consistent in multiple subgroups based on participant characteristics. Changes in TIR and other CGM metrics reflective of hyperglycemia paralleled the HbA1c results.
Given the favorable pharmacokinetic and pharmacodynamic profile of TI compared with RAA2,6 which was confirmed in children in an in-clinic meal challenge performed as part of INHALE-1, 8 the glycemic results were disappointing and not consistent with the glycemic benefit demonstrated in many adult MDI users in the INHALE-3 trial. 9 For meals, inhalation of multiple cartridges was required if the bolus requirement was more than 12 Afrezza units; it is possible that some participants underdosed rather than inhaling multiple doses. For optimal effect from TI, redosing may be needed 1 to 2 h after a prior dose when hyperglycemia is present. Even though they were trained to do so, we speculate that many participants may not have fully appreciated the need to redose TI following most meals to optimize control or simply found doing so challenging and at times not feasible. In addition, there may have been a tendency toward underdosing for meals and corrections and at bedtime due to concerns about hypoglycemia resulting from the 2 to 3× conversion needed to approximate glycemic lowering capacity of RAA units to TI units.
With respect to safety, CGM-measured hypoglycemia (<54 mg/dL) was minimal in both groups at the start of the Extension Phase and remained unchanged at 52 weeks. Inhalation-related cough was the most common adverse event reported by 18% of the RAA Crossover group, a frequency that is consistent with what was reported by the TI group during the 26-week RCT and in prior adult studies.9,10 There were no serious or unexpected pulmonary-related adverse events, and pulmonary function test results did not indicate any decline in lung function. In the 26-week RCT, there was a slight reduction in percent predicted FEV1 in both the TI group and the RAA control group (2.9 vs. 4.2). During an additional 26 weeks of TI use by the TI group, there was no statistically significant or clinically meaningful change in FEV1. In the RAA Crossover group, there was actually a small increase in FEV1 with the use of TI during the extension phase. Combining the entire periods of exposure for both groups, there was little change from the start of TI to 4 weeks after discontinuation.
Although the current U.S. labeling of TI indicates that the starting initial dose should be 1.0–1.3 times the RAA dose for most of the dose range, the current study in a pediatric population and INHALE-39 in an adult population have demonstrated that for bioequivalence the TI dose needs to be two to three times higher than the RAA dose. Both studies provide support for the safety of an initial conversion of approximately 2:1 followed by subsequent dose titration generally to a higher dose. In the current study, the median ratio of TI dose at 52 weeks to the pre-TI RAA dose was 2.86 in the TI group and 2.41 in the RAA Crossover group.
The RAA Crossover group showed a reduction in BMI between 26 and 52 weeks, which paralleled what was observed in the TI group after its first 26 weeks of TI use. Despite the lack of benefit observed in glycemic outcomes, treatment satisfaction increased over the 52 weeks of TI use in the participants in the TI group who continued in the extension phase. A similar increase in satisfaction was not observed in the RAA Crossover group, although scores were nevertheless quite high at 52 weeks.
The preponderance of youth in the United States with T1D use an insulin pump with automated insulin delivery. For such individuals, there are circumstances where adjunctive TI may be beneficial, including as a meal bolus, particularly for a high-carbohydrate meal or before planned postmeal exercise to minimize the risk of hypoglycemia.
This extension study has limitations that should be acknowledged. First, there was no concurrent control group, as the RCT RAA control group was switched to TI for the extension phase. Second, not all participants in the TI group elected to continue in the extension phase, which could be a source of bias, particularly with regard to the assessment of treatment satisfaction. Third, assessment of adherence to TI dosing relied on self-report, which may not have provided an accurate representation and limited our ability to understand dosing patterns and their impact on glycemic outcomes. A dose tracking device reportedly in development by the company may help to provide more data for patients and clinicians regarding dosing frequency and amount in the future. Fourth, although the study did not identify safety concerns, there was only 1 yr of exposure to TI; thus, we were unable to assess long-term safety.
In summary, the INHALE-1 extension phase showed no safety concerns. Although HbA1c levels worsened slightly during the study, in view of the safety profile and increased patient satisfaction in the RCT portion of the trial, TI may be a useful treatment option for some pediatric patients with diabetes, particularly for youth who choose not to or are unable to use an AID system.
Authors’ Contributions
R.W.B.: Funding, supervision, and writing—original draft, review, and editing. L.K.: Formal analysis and writing—review and editing. R.M.: Investigation and writing—review and editing. S.M.W.: Investigation and writing—review and editing. M.T.: Investigation and writing—review and editing. J.R.W.: Investigation and writing—review and editing. A.C.: Investigation and writing—review and editing. R.F.-S.: Investigation and writing—review and editing. K.E.B.: Investigation and writing—review and editing. K.C.: Investigation and writing—review and editing. P.C.W.: Investigation and writing—review and editing. P.C.H.: Investigation and writing—review and editing. T.J.M.: Project administration and writing—review and editing. M.J.H.: Investigation and writing—review and editing.
Footnotes
Author Disclosure Statement
R.W.B. reports no personal financial disclosures but reports that his institution has received funding on his behalf as follows: grant funding, study supplies, and consulting fees from Insulet, Tandem Diabetes Care, and Beta Bionics; grant funding and study supplies from Dexcom and Abbott; grant funding from Bigfoot Biomedical, Embecta, Sequel Med Tech, and MannKind; study supplies from Medtronic; consulting fees and study supplies from Novo Nordisk; and consulting fees from Vertex, Hagar, DreaMed, Ypsomed, Abata Therapeutics, Eli Lilly, and Zucara. J.R.W. reports being on advisory boards for MannKind and Sanofi and receiving research funding from Insulet. M.J.H. reports being a consultant for MannKind, Sanofi, and SAB Bio and holding stock options for SAB Bio. The following authors report no disclosures: L.K., R.M., S.M.W., M.T., A.C., R.F.-S., K.E.B., K.C., P.C.W., P.C.H., and T.J.M.
Funding Information
Funding for the study was provided by MannKind.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.