
Abstract
Objective:
To assess postprandial glucose excursions following a meal bolus of inhaled technosphere insulin (TI) in youth with type 1 diabetes.
Methods:
As part of a multicenter randomized controlled trial, 217 youth 4–17 years old with type 1 diabetes using multiple daily injections (MDI) completed an in-clinic standardized meal challenge with their first TI dose. Glucose levels were monitored for 2 h. Outcomes were compared with outcomes in MDI-using adults with T1D who received a TI (N = 51) or a rapid-acting analogue (RAA, N = 25) bolus for a similar meal challenge in a separate trial.
Results:
Following TI inhalation, the glucose excursion and glycemic metrics were similar in the pediatric cohort to those of the adult TI cohort. In contrast, compared with the adult RAA cohort, the pediatric TI cohort had a smaller glucose excursion (P < 0.001), lower peak glucose (P < 0.001), smaller AUC180 (P < 0.001), and higher time-in-range 70–180 mg/dL (P = 0.002). A glucose value < 70 mg/dL occurred in 14 (6%) of the pediatric TI cohort versus 1 (2%) of the adult TI cohort. Children 4–12 years old had a significantly higher peak glucose and excursion (P < 0.001) than those 13–17 years old. No significant difference in response to meal challenges was observed between groups with baseline HbA1c < 8.5% and HbA1c ≥ 8.5%. The mean ratio of TI inhaled units to the calculated RAA bolus that would be given for the number of carbohydrates was 1.9 ± 0.6 in the pediatric cohort and 1.9 ± 0.2 in the adult cohort.
Conclusions:
In children with type 1 diabetes, the postmeal glucose excursion following a TI bolus was similar to the postmeal glucose excursion that occurs with TI in adults and significantly lower than the excursion that has been observed with RAA in adults. These findings are consistent with the known pharmacokinetic profile of TI.
Introduction
In individuals with type 1 diabetes (T1D), postmeal hyperglycemia is common, even with automated insulin delivery systems. This glucose rise is difficult to prevent due to the delay in effect following a meal bolus using a subcutaneous injection of rapid-acting analogue (RAA) insulin. Technosphere insulin inhalation powder (TI, Afrezza®, MannKind Corporation, Danbury, CT) has a more rapid onset of action and more rapid dissipation than with RAA insulin,1,2 which may reduce the postmeal glucose excursion.
TI was approved by the Food and Drug Administration (FDA) for use in adults with diabetes in 2014, with a recommended starting TI dose equal to the calculated RAA dose. 3 A recent randomized controlled trial (RCT, INHALE-3) in 123 adults with T1D using a higher TI dose than in the FDA label demonstrated promising efficacy results, without safety concerns over 30 weeks of TI use.4–6 As part of that study, an in-clinic meal challenge showed reduced postmeal glucose excursions with TI compared with RAA. 7
In children, a pharmacokinetic study has demonstrated a highly favorable insulin action profile for TI with no safety concerns. 8 These promising results preceded the conduct of an RCT (INHALE-1) in 230 youth 4–17 years old with diabetes, comparing TI versus RAA used in conjunction with basal insulin over 26 weeks, followed by a 26-week extension phase in which both groups used TI + basal insulin. 9 As part of the trial, an in-clinic standardized meal challenge was performed for the first TI dose received by the participants. In order to evaluate postprandial glucose excursion following inhaled TI insulin during a meal challenge in children with type 1 diabetes, we compare the results in T1D youth to both TI and RAA meal challenges performed in T1D adults in INHALE-3.
Methods
The INHALE-1 study was conducted at 38 endocrinology practices in the United States. The protocol was approved by a central institutional review board. Informed consent was obtained from the parent or guardian of each participant and assent from participants ≥7 years old. Study participants included in the current analysis were children 4 to <18 years old living with T1D for ≥6 months treated with multiple daily injections (MDI) of insulin who had baseline HbA1c 6.3%–11.0% as measured by the central laboratory (screening point-of-care testing required HbA1c of 7.0%–11.0% for eligibility). Study methods, including complete participant eligibility criteria, have been previously published and appear on clinicaltrials.gov (NCT04974528). 9
INHALE-1 meal challenge procedures
The first TI dose was received during an in-clinic meal challenge at the baseline visit for participants randomly assigned to the TI group and at the RCT 26-week visit for participants assigned to the RAA group (who switched to TI at this visit). Participants were fasting for at least 8 h prior to the meal challenge. The TI inhalation was given at the start of the meal in which participants ingested either a Clif Bar (250–260 calories, 40–43 g of carbohydrate, 10–11 g of protein, 6–8 g of fat depending on the flavor of the bar) or drank a bottle of BOOST nutritional shake (240 calories, 37 grams of carbohydrate, 10 g of protein, 6 g of fat).
The dose of inhaled insulin was determined by rounding the usual RAA dose to the nearest whole number, multiplying by 2, and then rounding down to the nearest 4-unit dose of TI (not to exceed 16 units). This starting dose for TI was intended to guide the initial conversion from injection. Dose determinations were made without glucose level correction. At the investigator’s discretion, a second TI dose, typically 4 units, was inhaled 60–90 min after the initial dose if the glucose level was >160 mg/dL.
Real-time continuous glucose monitoring (CGM) using a Dexcom G6 sensor was used for safety monitoring and for analysis if available. When CGM was not available, blood glucose (BG) measurements were made using a Contour Next One BG meter 15 min before and immediately prior to the TI inhalation and 15, 30, 45, 60, 90, and 120 min after inhalation.
For a BG value <70 mg/dL during or at the completion of 2 h postmeal, oral carbohydrate was ingested.
INHALE-3 meal challenge procedures
The analyses included data from meal challenges performed on the adult MDI users with T1D in INHALE-3. The INHALE-3 meal challenge procedures followed have been detailed in a prior publication. 7 Participants assigned to the TI group had a TI meal challenge at the baseline visit, whereas participants assigned to the RAA group had an RAA meal challenge at baseline and a TI meal challenge at 17 weeks when they switched to TI.
For the INHALE-3 meal challenges, participants were fasting with no manual insulin boluses for 4 h. The glucose level was expected to be 91–219 mg/dL 15 min prior to the consumption of BOOST® nutritional shake (240 calories, 37 g of carbohydrate, 10 g of protein, 4 g of fat). For the TI meal challenge, the TI dose was determined by the method described above for INHALE-1 and given at the start of the meal (maximum 24 units). For the RAA meal challenge, the insulin dose was based on the participant’s usual bolus for that amount of carbohydrate and was given 10 ± 5 min before the start of the meal. For a glucose measurement >400 at any time or >300 mg/dL for 1 h, additional insulin was administered (TI for the TI meal challenges and RAA insulin for the RAA meal challenges).
Participants wore a blinded Dexcom G6 Pro sensor and were monitored using BG measurements obtained with a McKesson TRUE METRIX® PRO Professional Monitoring Blood Glucose Meter by the schedule described for INHALE-1. For a BG value <70 mg/dL during or at the completion of 2 h postmeal, oral carbohydrate was ingested.
Statistical methods
Glucose data from the 2 h after the start of the meal were used in the analyses. The outcome considered most relevant was area under the curve >180 mg/dL (AUC180). Other outcomes included maximum glucose excursion from baseline, peak glucose, time to peak glucose, and percent time in standard glucose ranges.
Outcomes were compared between INHALE-1 TI and INHALE-3 TI and between INHALE-1 TI and INHALE-3 RAA using linear regression models adjusted for starting glucose. Outcomes were also compared between groups based on age and baseline HbA1c for the INHALE-1 study using similar methods. P-values were adjusted to control the false discovery rate using the Benjamini-Hochberg procedure method adapted using the two-stage test.
To convert glucose values from mg/dL to mmol/L, multiply by 0.05551. SAS version 9.4 was used for the analyses.
Results
The analyses compared the results of a meal challenge in 217 youth who received a TI meal bolus in INHALE-1 with the results in 51 adults who received a TI meal bolus and 25 who received an RAA meal bolus in INHALE-3. All participants used MDI for insulin delivery. Characteristics of the three cohorts are shown in Table 1.
Participant Characteristics at Baseline
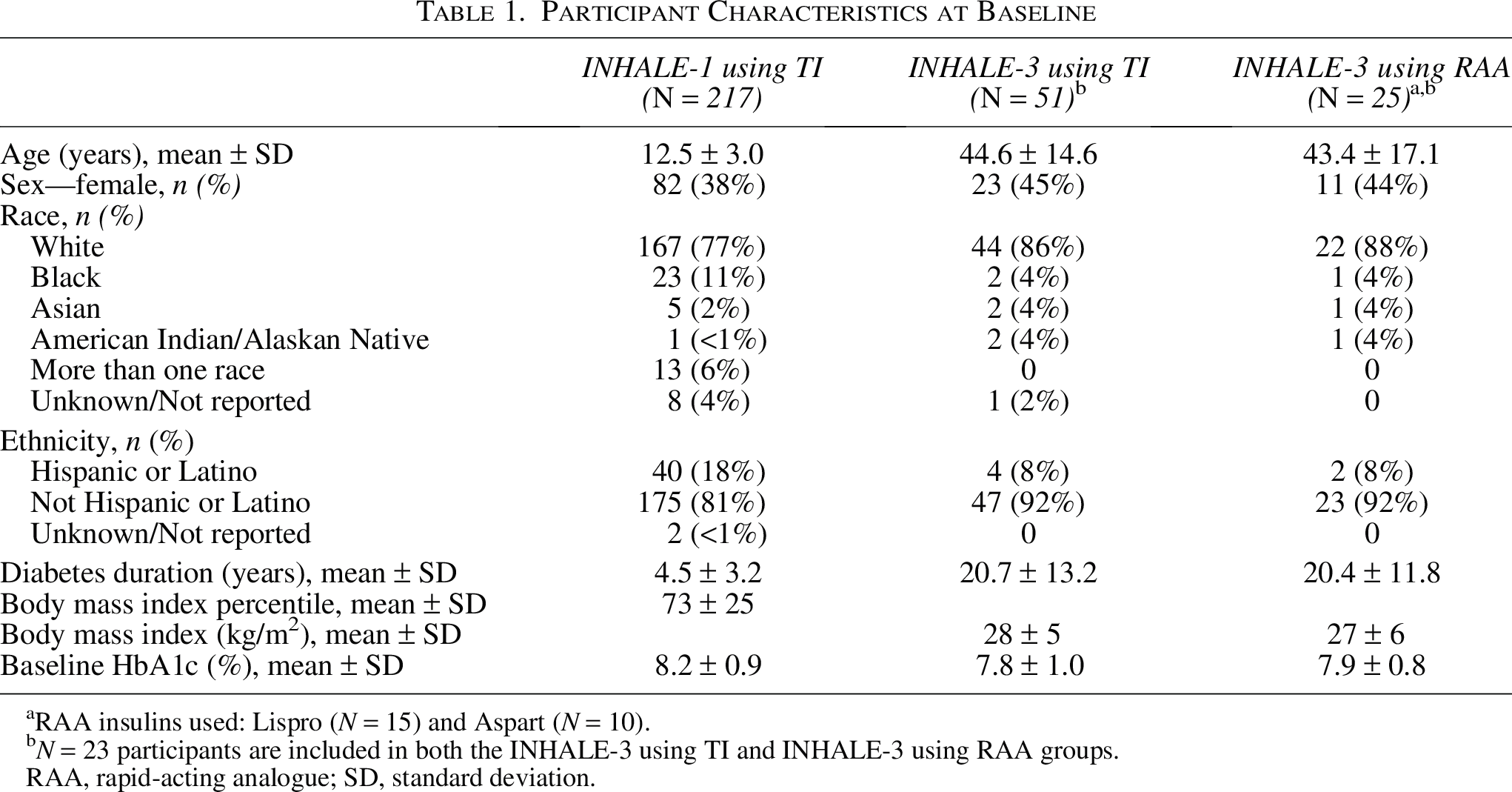
RAA insulins used: Lispro (N = 15) and Aspart (N = 10).
N = 23 participants are included in both the INHALE-3 using TI and INHALE-3 using RAA groups.
RAA, rapid-acting analogue; SD, standard deviation.
The dose of TI or RAA insulin received at the start of the meal challenge is shown in Table 2. For the pediatric TI cohort, the mean ratio of TI inhaled to the calculated RAA bolus that would be given for the number of carbohydrates ingested was 1.9 ± 0.6 (median 2.0, interquartile range [IQR] 1.6–2.0). For the adult TI cohort, the mean ratio was 1.9 ± 0.2 (median 2.0, IQR 1.7–2.0). A correction dose was given after 60–90 min in 53% of the pediatric cohort for a glucose level >160 mg/dL. In the adult cohort, 3 (6%) received a second TI dose, and none received a second RAA dose.
Features of the Meal Challenges
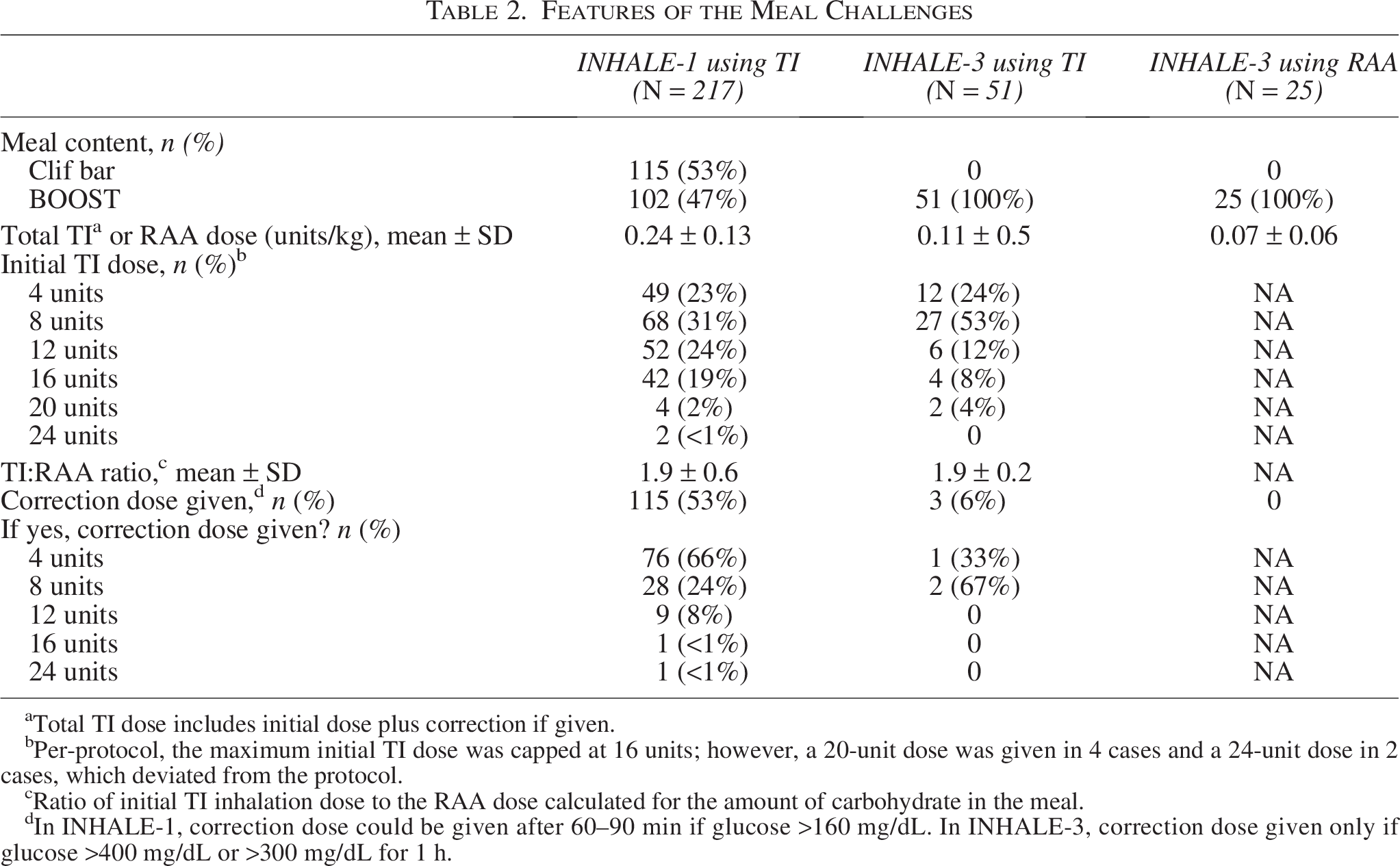
Total TI dose includes initial dose plus correction if given.
Per-protocol, the maximum initial TI dose was capped at 16 units; however, a 20-unit dose was given in 4 cases and a 24-unit dose in 2 cases, which deviated from the protocol.
Ratio of initial TI inhalation dose to the RAA dose calculated for the amount of carbohydrate in the meal.
In INHALE-1, correction dose could be given after 60–90 min if glucose >160 mg/dL. In INHALE-3, correction dose given only if glucose >400 mg/dL or >300 mg/dL for 1 h.
Following TI inhalation, the glucose excursion appeared quite similar in the pediatric and adult TI cohorts. In contrast, the pediatric TI cohort had a substantially smaller excursion than the adult RAA cohort (P < 0.001) and a significantly lower peak glucose (P < 0.001) and AUC180 (P < 0.001) (Fig. 1A, Table 3). Average change per minute over the first hour using TI was 0.4 ± 1.0 mg/dL in the pediatric cohort and 0.8 ± 0.9 mg/dL in the adult cohort compared with 1.3 ± 0.8 mg/dL in the adult cohort using RAA. Mean time-in-range 70–180 mg/dL during the 2 h of the meal challenge was 41 ± 38% in the pediatric TI cohort, 44 ± 39% in the adult TI cohort, and 23 ± 32% in the adult RAA cohort (P = 0.002 comparing pediatric TI versus adult RAA). Participants younger than 13 years old (N = 100) had significantly higher peak glucose, excursion, and AUC180 mg/dL (P < 0.001, P < 0.001, and P = 0.02, respectively) compared with 13- to 17-year olds (N = 117) (Fig. 1B, Table 4). Mean baseline HbA1c was 8.3 ± 0.9% in the younger versus 8.1 ± 0.9% in the older participants. A TI correction dose was received by 57% of the younger subgroup and by 50% of the older subgroup. Among participants receiving a correction dose, the mean time to redosing after the start of the meal was 70 ± 19 min in the younger subgroup and 70 ± 18 min in the older subgroup. There were no significant differences in postmeal metrics with baseline HbA1c < 8.5% versus HbA1c ≥ 8.5% (Fig. 1C, Table 4).
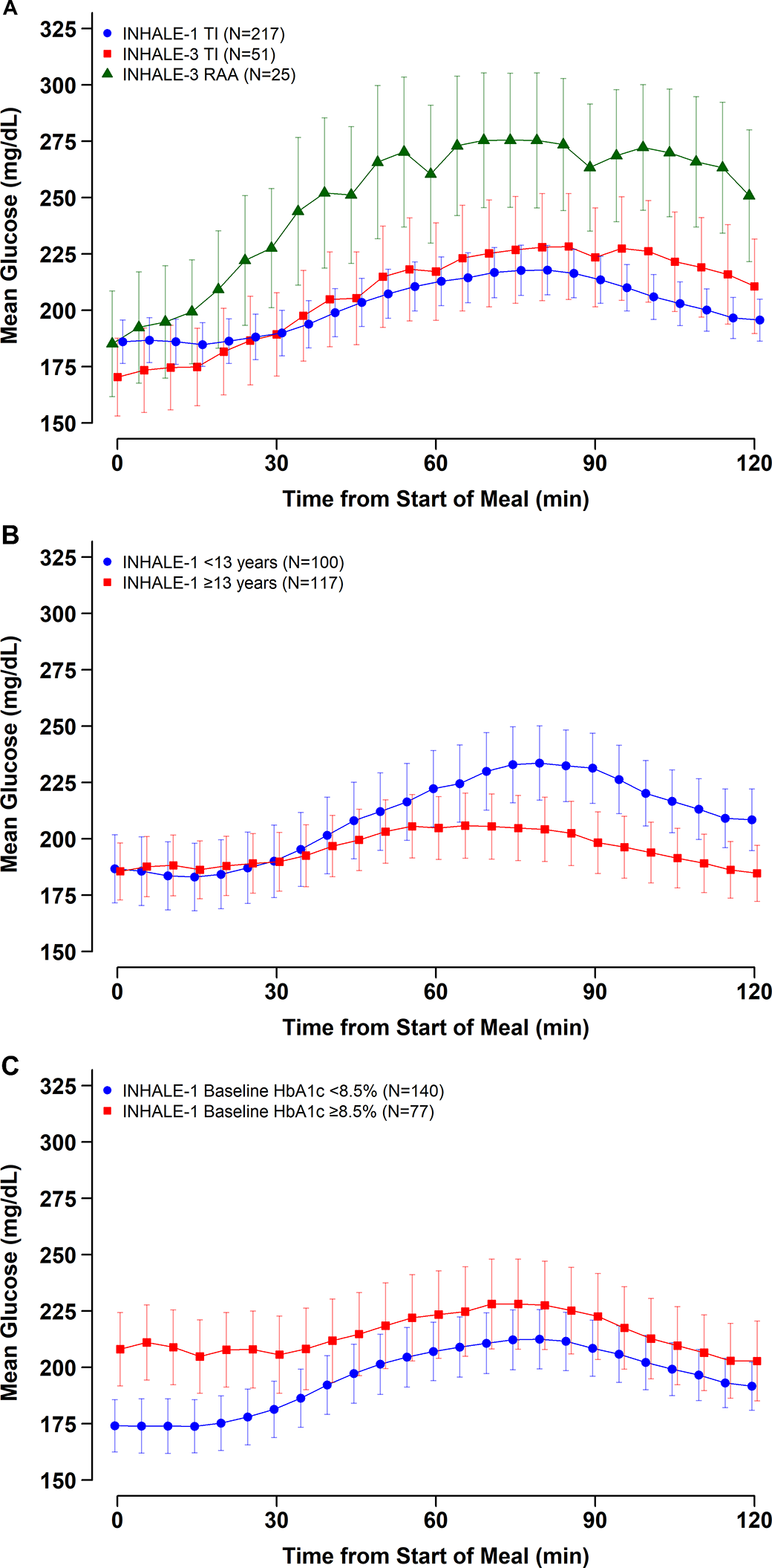
Postprandial glucose levels following standardized meal. Mean glucose and error bars representing 95% confidence interval around the mean at 5-min intervals following a standardized meal.
Postprandial Glycemic Metrics in First 2 h After Start of Meal Challengea
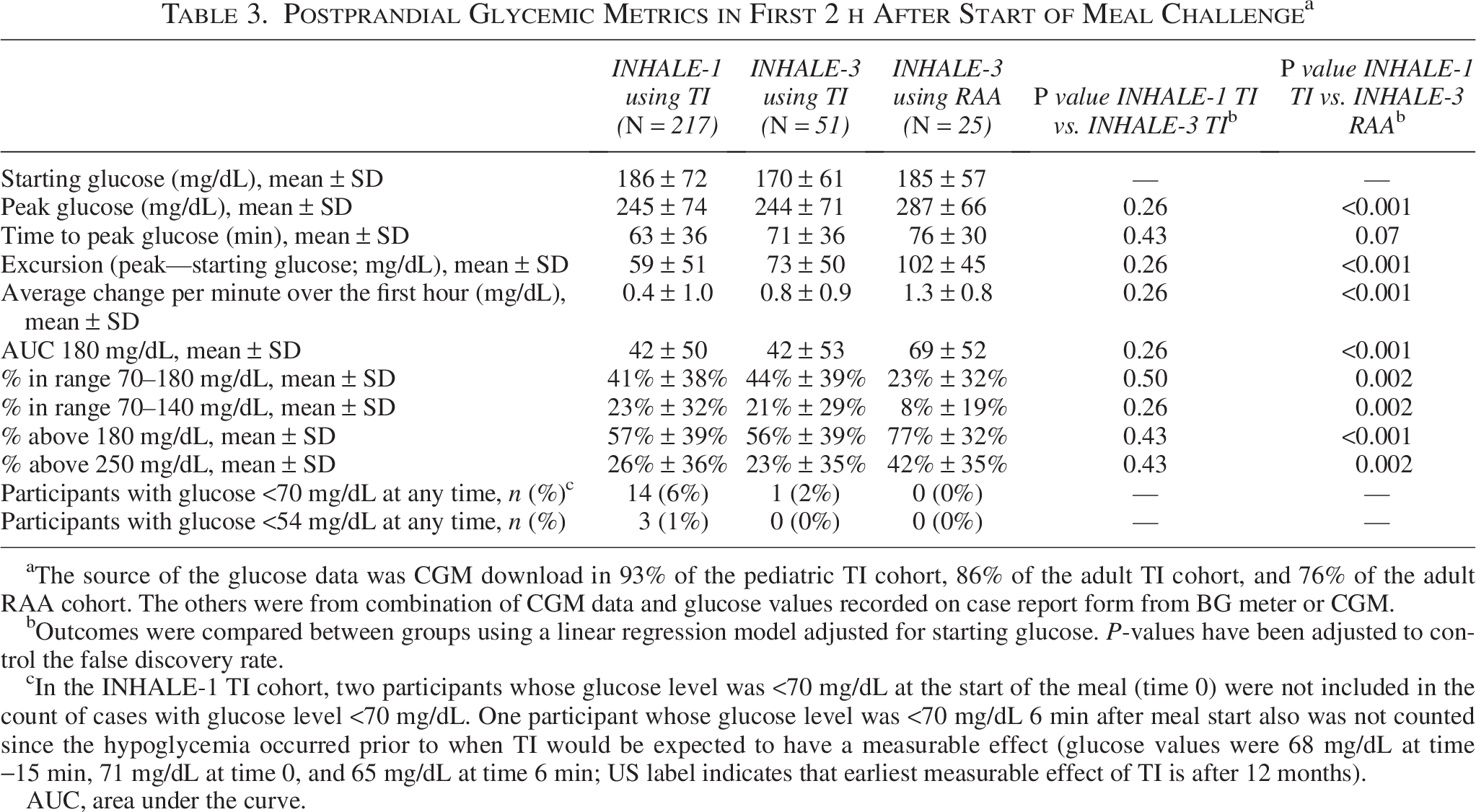
The source of the glucose data was CGM download in 93% of the pediatric TI cohort, 86% of the adult TI cohort, and 76% of the adult RAA cohort. The others were from combination of CGM data and glucose values recorded on case report form from BG meter or CGM.
Outcomes were compared between groups using a linear regression model adjusted for starting glucose. P-values have been adjusted to control the false discovery rate.
In the INHALE-1 TI cohort, two participants whose glucose level was <70 mg/dL at the start of the meal (time 0) were not included in the count of cases with glucose level <70 mg/dL. One participant whose glucose level was <70 mg/dL 6 min after meal start also was not counted since the hypoglycemia occurred prior to when TI would be expected to have a measurable effect (glucose values were 68 mg/dL at time −15 min, 71 mg/dL at time 0, and 65 mg/dL at time 6 min; US label indicates that earliest measurable effect of TI is after 12 months).
AUC, area under the curve.
Postprandial Glycemic Metrics in First 2 h After Start of Meal Challenge in the INHALE-1 Study According to Age Group and HbA1c Level
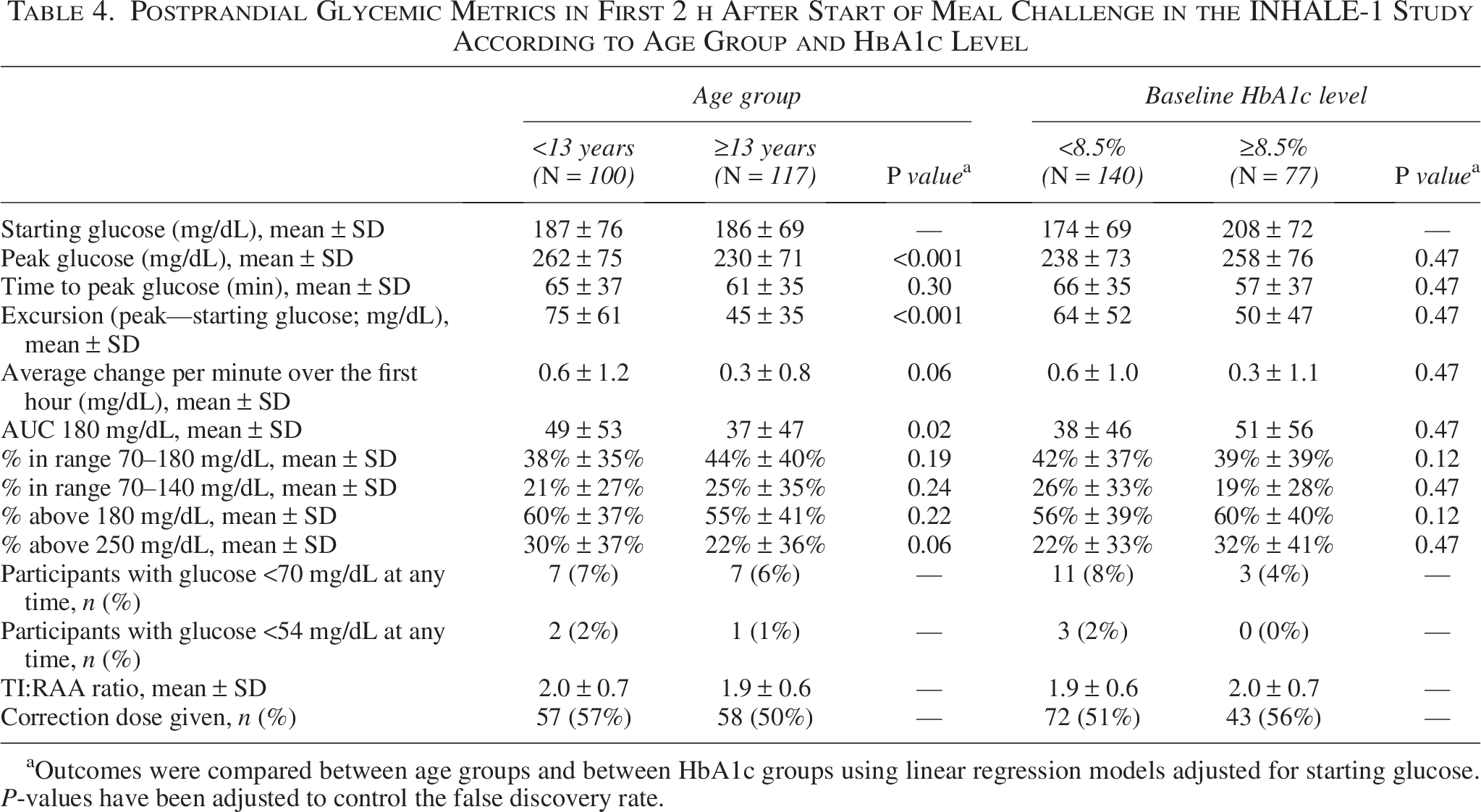
Outcomes were compared between age groups and between HbA1c groups using linear regression models adjusted for starting glucose. P-values have been adjusted to control the false discovery rate.
A glucose value <70 mg/dL occurred during the meal challenge in 14 (6%) of the pediatric TI cohort, 1 (2%) of the adult TI cohort, and in none of the adult RAA cohort. In the INHALE-1 TI cohort, mean glucose at the start of the meal was 109 ± 35 mg/dL in the 14 participants who developed hypoglycemia compared with 193 ± 69 mg/dL in the 200 participants who did not develop hypoglycemia (P < 0.001). The time of the first glucose measurement <70 mg/dL was within 20 min of the start of the meal in 5, 21–40 min in 5, 41–60 min in 1, 61–80 min in 2, 83 min in 1, and 120 min in 1. None of the 14 episodes occurred after a TI correction dose.
Discussion
In standardized in-clinic meal challenges using inhaled TI, postprandial glucose excursions in the INHALE-1 MDI-treated pediatric type 1 diabetes cohort were similar to those reported in the comparable INHALE-3 adult cohort. In contrast, there was a substantial reduction in the glucose excursion, peak glucose, and time to peak glucose in the INHALE-1 pediatric cohort following TI inhalation compared with an RAA bolus in the INHALE-3 adult cohort. This is consistent with the pharmacodynamics of inhaled insulin.1,8
Previous studies have shown the safety of a starting TI dose approximately twice the RAA dose.6,10 This was confirmed during the 26 weeks of the INHALE-1 RCT, where the dose was titrated in many participants to about three times the baseline RAA dose by week 26, without observing any increase in hypoglycemia. 9 During the INHALE-1 pediatric cohort meal challenges, more participants’ glucose values dropped to <70 mg/dL than was observed in the INHALE-3 adult cohorts. This difference between the pediatric and adult cohorts does not appear to be related to TI dose, as the mean ratio of TI to RAA was similar in both the pediatric and adult cohorts, and does not appear to be related to postmeal correction doses being received in the pediatric cohort, as none of the cases of hypoglycemia occurred after a correction dose. Within the pediatric cohort, there was no consistent pattern of hypoglycemia across the age range, yet there was a prominent association with baseline glucose level, as the participants developing hypoglycemia on average had a substantially lower glucose level at the start of the meal compared with those who did not develop hypoglycemia.
The postmeal glucose excursion was lower in adolescents than in younger participants, despite the TI dose to calculated RAA bolus ratio being similar between the two age groups. There was no optimization period, and therefore the insulin-to-carb ratios could have been less aggressive, perhaps due to concern about hypoglycemia, in younger children compared with adolescents; or the younger children might have had greater difficulty with full inhalation, as this was their initial TI inhalation after training. Also, basal insulin doses were not optimized for inhaled insulin.
Although the meal challenge results in the INHALE-1 pediatric cohort demonstrated a substantial benefit of TI in reducing postmeal hyperglycemia, this did not translate to better glycemic outcomes in the RCT comparing TI versus RAA combined with basal insulin for 26 weeks. In the trial, mean HbA1c was 8.22 ± 0.87% at baseline and 8.41 ± 1.38% at 26 weeks with TI and 8.21 ± 0.96% and 8.21 ± 1.10%, respectively, with RAA. HbA1c improved from baseline by >0.5% in 15% in the TI group versus 23% in the RAA group. 9
There are several possible reasons for this discordance between the meal challenge results and the RCT findings. First, the in-clinic standardized meal was characterized by relatively low fat and protein content and therefore may not reflect the composition of typical meals for many children. It is well studied that the fat and protein content of meals can increase insulin requirements and lead to late hyperglycemia.11–13 For optimal effect from TI, redosing may be needed 1–2 h after a prior dose when hyperglycemia is present, and during the in-clinic meal challenge, about half of the pediatric cohort required a correction dose after 60–90 min. Such correction dosing is not done following an RAA meal bolus due to its prolonged duration of action and risk of stacking if done. We speculate that many participants may not have fully understood the need to redose TI following most meals to optimize control or simply found doing so challenging and at times not feasible. In addition, there may have been a tendency towards underdosing for meals and corrections and at bedtime due to concerns about hypoglycemia resulting from the 2–3× conversion from RAA units to TI units.
The strength of this study is the use of data gathered from a large, multicenter clinical investigation. The main limitation is that the pediatric study did not compare TI versus RAA. Thus, the statistical comparison was made with an adult cohort from the INHALE-3 trial. The finding that the TI results from the pediatric and adult cohorts were similar supports the validity of comparing the pediatric TI results in INHALE-1 to the adult RAA results in INHALE-3. An additional limitation was that while the glucose data source was primarily CGM, some participants did not have CGM data during the meal challenge, and BG data were used instead. The duration of BG monitoring was also only 2 h, and with a 4-h period, we would have been better able to assess the full effect of the TI and RAA insulin boluses. Finally, results might differ for meal compositions different from those ingested in the study.
In summary, in children with type 1 diabetes, the postmeal glucose excursion following a TI bolus was similar to the postmeal glucose excursion that occurs with TI in adults and significantly lower than the excursion that has been observed with RAA in adults. These findings are consistent with the known pharmacokinetic profile of TI and support similar dosing for pediatric and adult meal challenges.
Authors’ Contributions
L.E.: Investigation and writing—original draft, review, and editing. L.K.: Formal analysis and writing—review and editing. A.D.: Investigation and writing—review and editing. L.A.D.: Investigation and writing—review and editing. M.K.: Investigation and writing—review and editing. M.A.W.: Investigation and writing—review and editing. M.J.H.: Investigation and writing—review and editing. T.J.M.: Project administration and writing—review and editing. R.W.B.: Funding, supervision, and writing—original draft, review, and editing.
Footnotes
Author Disclosure Statement
L.E. has served on the advisory board of Sanofi, Abbott, Diabetes Center Berne, Sequel, MannKind, and Medtronic; received consulting fees from Jaeb and Tandem Diabetes Care, Ypsomed, and honorarium fees from American Diabetes Association, Med Learning Group (Sanofi-sponsored grant), Children with Diabetes (MannKind-sponsored educational event), cgmEducation.net (education grant sponsored by MannKind), Tandem Diabetes Care, Medtronic, and Insulet. Her institution has received research support from Breakthrough T1D, The Leona M. and Harry B. Helmsley Charitable Trust, Medtronic, Tandem Diabetes Care, MannKind, and Abbott. She receives salary support from NIH. L.A.D. reports research support to her institution from Lilly, Sanofi, and Zealand and consulting fees from Tandem Diabetes. M.K. reports receiving research grants from 89bio, Medtronic, Abbott, Akero Therapeutics, Biomea Fusion, Carmot, Dexcom, AbbVie, Amgen, Biolinq, Diamyd, Endogenex, Insulet, IONIS Pharmaceuticals, Kowa, Novo Nordisk, Tandem, Zucara Therapeutics, Zydus, Sinocare, Boehringer Ingelheim, Corcept, Eli Lilly, and advisory board fees from AP stem and Corcept. M.A.W. reports receiving speaker fees from Alexion, Sanofi, and MannKind. M.J.H. reports receiving consultancy fees and serving as a scientific advisory board member for MannKind and SAB BIO, and consultancy fees from Sanofi. R.W.B. reports no personal financial disclosures but reports that his institution has received funding on his behalf as follows: grant funding, study supplies, and consulting fees from Insulet, Tandem Diabetes Care, and Beta Bionics; grant funding and study supplies from Dexcom and Abbott; grant funding from Bigfoot Biomedical, Embecta, Sequel Med Tech, and MannKind; study supplies from Medtronic; consulting fees and study supplies from Novo Nordisk; and consulting fees from Vertex, Hagar, DreaMed, Ypsomed, Abata Therapeutics, Eli Lilly, and Zucara. The following authors report no disclosures: L.K., T.J.M., and A.D.
Funding Information
Funding for the study was provided by MannKind. The conduct of the study at the University of California, San Francisco, was supported in part by the National Center for Advancing Translational Sciences, National Institutes of Health, through UCSF-CTSI grant number UL1 TR001872. Article contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.