
Abstract
Intimate partner violence (IPV) impacts millions of adults and children every year and can result in homicide, legal proceedings, the involvement of child welfare, and the need for emergency shelter for survivors and their families. Survivors of IPV may develop psychological and somatic symptoms to the trauma, including anxiety, depression, and other mental health related disorders in addition to facing numerous safety, financial, and social challenges. To reestablish stability, effective short-term interventions are needed in order to address these issues survivors face. This systematic review and meta-analysis summarizes the extant literature on short-term interventions for survivors of IPV. Twenty-one studies are included in the analysis and overall effect sizes calculations and moderator analysis were conducted. On average, effects sizes were large (g = 1.02) suggesting that most sort-term interventions are effective, however CBT-based interventions that were tailored to IPV survivors achieved the largest effect sizes. Results of this study are presented in a question and answer format with the intent to guide practitioners, researchers and policy makers. IPV survivors access services in a variety of shelter and outpatient settings and present diverse needs. Although this study contributes a systematic review of the existing literature on IPV, there are relatively few rigorous outcome studies and even fewer that reflect the diversity in this population and the complexity of responding to IPV in real-world settings.
Introduction
According to the 2010 National Intimate Partner and Sexual Violence Survey, more than one in three women and one in four men in the United States have experienced rape, physical violence, and/or stalking by an intimate partner in their lifetime (Black et al., 2011). Intimate partner violence (IPV) includes physical, emotional, or sexual aggression as well as stalking and economic aggression directed at a partner. IPV is often believed to be motivated by a desire to maintain power or exert control over a partner.
Survivors of IPV suffer from a host of mental health problems including post-traumatic stress disorder (PTSD), substance use disorders, anxiety disorders, and depression (Zlotnick, Johnson, & Kohn, 2006). The negative impact of IPV is not limited to the adults in the relationship. Children who are exposed to IPV are more likely to experience both internalizing and externalizing problems (DeJonghe, von Eye, Bogat, & Levendosky, 2011). In the United States, child protective services will likely be involved if the police learn that children were exposed to IPV.
The negative impact of IPV is not limited to emotional, social, and psychological sequela for survivors and their children. Many survivors of IPV lose economic security and become functionally homeless because they are forced to leave the household to escape violence. Survivors who leave a perpetrator often go to a domestic violence (DV) shelter due to a lack of financial resources or because it is safer than alternative options. Survivors of IPV are likely to have experienced cycles of resource loss, which in turn exacerbates PTSD and other mental health problems. This can result in diminished functioning in multiple life spheres, including establishing safety and independence from abusers (Johnson & Zlotnick, 2009).
Breaking the cycle of IPV is important. The World Report on Violence and Health (2002) concluded that IPV is an important public health problem that requires the involvement of many sectors. Interventions targeting IPV have focused on the needs of survivors, issues surround those who perpetrate IPV, and community-based prevention efforts. As many IPV survivors become involved with a DV shelter, it is important to know which types of treatments might be applicable to this setting. Psychotherapy services for survivors are common in shelters and in community centers. However, little is known about the nature of interventions designed to help IPV survivors in shelters (Rhodes & Levinson, 2003). The present study sought to better understand the nature and effectiveness of short-term interventions in both community settings and shelters.
Traditionally designed and delivered psychotherapies may not be appropriate for IPV survivors given the complex concerns of survivors at the point of receiving services whether in a shelter or shortly thereafter. The complex needs of IPV victims include safety, ability to live and cope with communal living environments when entering shelters, substance use and abuse, mental illness, parenting, economic challenges, and complex grief while making or considering significant life changes such as staying or leaving the relationship. Brief therapies are often indicated for IPV survivors in shelter situations because they may not stay long in shelters.
This systematic review and meta-analysis focused on short-term psychotherapeutic modalities used when working with survivors of IPV. Two broad objectives guided our review. First, to identify and describe what short-term psychotherapy interventions have been delivered to IPV survivors and the nature of such interventions. This was done through a systematic review with a qualitative summary of identified studies. Second, to quantitatively synthesize targeted outcomes of short-term psychotherapy, interventions to both provide an overall estimate of the effect of such interventions and, where possible, explore possible moderator variables. This was done through meta-analysis. Findings from this study may guide decisions surrounding delivering short-term psychotherapies to IPV survivors.
Method
To promote confidence in outcomes, preferred reporting items for systematic reviews and meta-analyses guidelines were followed. To be included, studies must have provided a short-term psychotherapy to adult IPV survivors. Short-term psychotherapies or interventions included time-limited groups and individual treatment modalities that tended to be less than eight sessions. As there is a dearth of research in this area, study design was not a limiting factor. Thus, as long as an intervention designed to help IPV survivors was provided and supplied enough quantitative data to compute an effect size, the study was eligible for inclusion. Only dissertations and peer-reviewed reports were included. There were no language or date restrictions applied to the search. In an effort to avoid introducing systematic error (e.g., locating other reports, inconsistency associated with study authors responding to requests for information), only studies that could be identified and secured through electronic databases or the reference lists of identified studies were included. Exclusion criteria included studies that were purely qualitative or theoretical, single case scenarios, studies with less than five participants, studies where the main intervention was targeted to perpetrators of IPV, studies focused on sexual assault survivors (including adults molested as children), and single event trauma studies.
The following electronic databases were searched: Academic Search, Premier, Chicano Database, CINAHL, Criminal Justice Abstracts, Fuente Academica, MEDLINE, Medic Latina, PsychINFO, Psychology and Behavioral Sciences Collection, Women’s Studies International, and Family & Society Studies Worldwide. Three sets of search terms were created to encompass articles of interest to this study. Specifically, we identified terms surrounding the following three areas combined with “and” to narrow our search: “IPV,” “psychological interventions,” and “brief or short term.” The list of search terms used is shown in Table 1.
Search Terms Used to Identify Possible Studies.

Note. IPV = intimate partner violence.
aIndicates a wildcard.
A total of 223 possible studies were identified through our search strategy after duplicates were removed. We first reviewed titles and abstracts to ascertain relative fit, which left 44 articles that were secured and subjected to a full text review. Of these, 21 studies met our inclusion criteria. See Figure 1 for an overview. Each study that met inclusion criteria was independently coded by two of the authors to ensure accurate data extraction. Table 2 shows the information extracted from each study, some of the variables were eventually used as moderators in the meta-analysis.
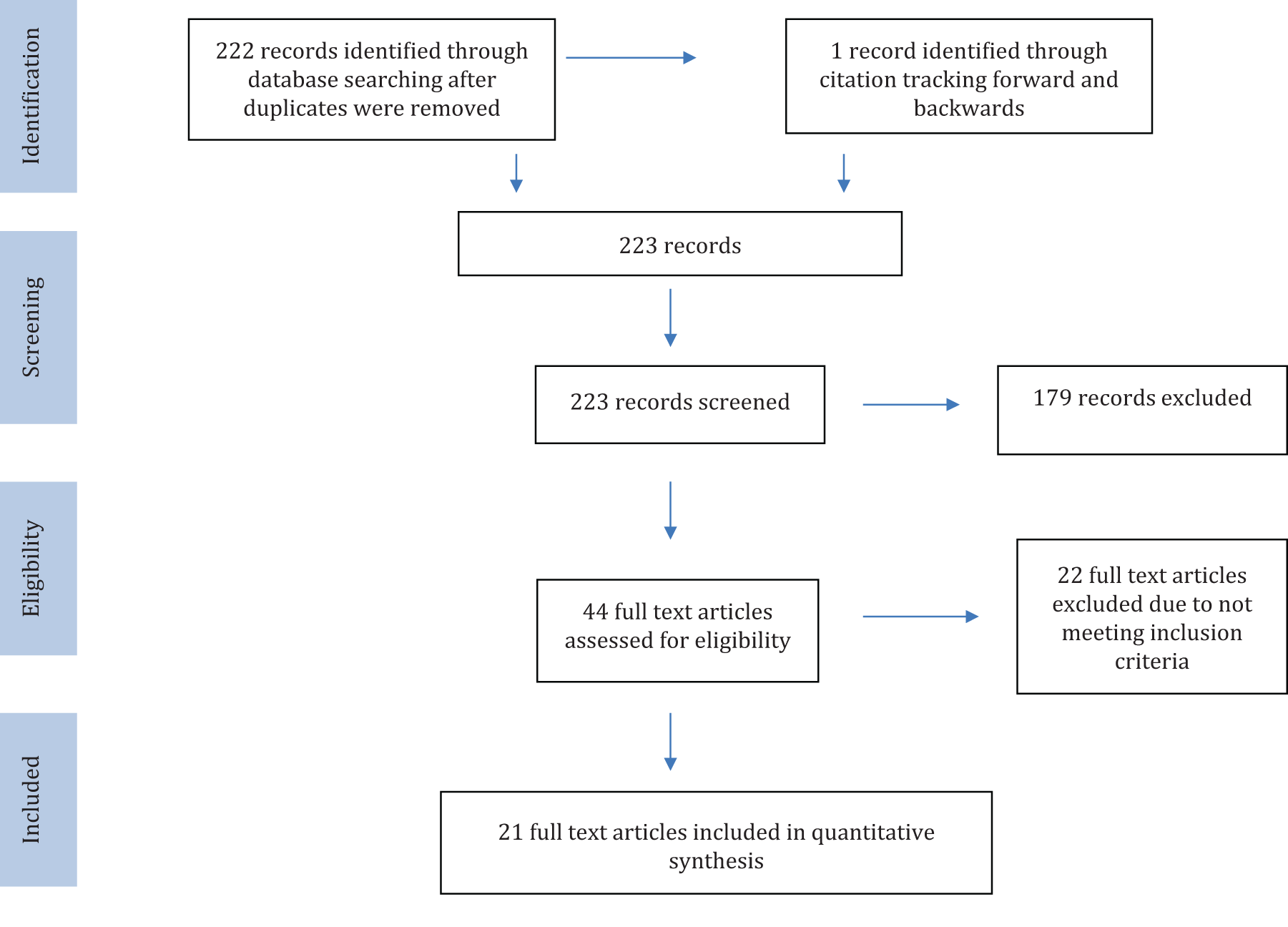
Preferred reporting items for systematic reviews and meta-analyses flow diagram.
Data Information Collected for This Review.

Note. ITT = intention to treat analysis.
Studies examined a range of targeted outcomes, too many to report independently in a meta-analysis or systematic review. Nine different categories were rationally developed to organize the many outcomes. Table 3 shows the nine categories with examples of outcomes measures that were included in each category.
Targeted Dependent Variables: Categories and Examples.
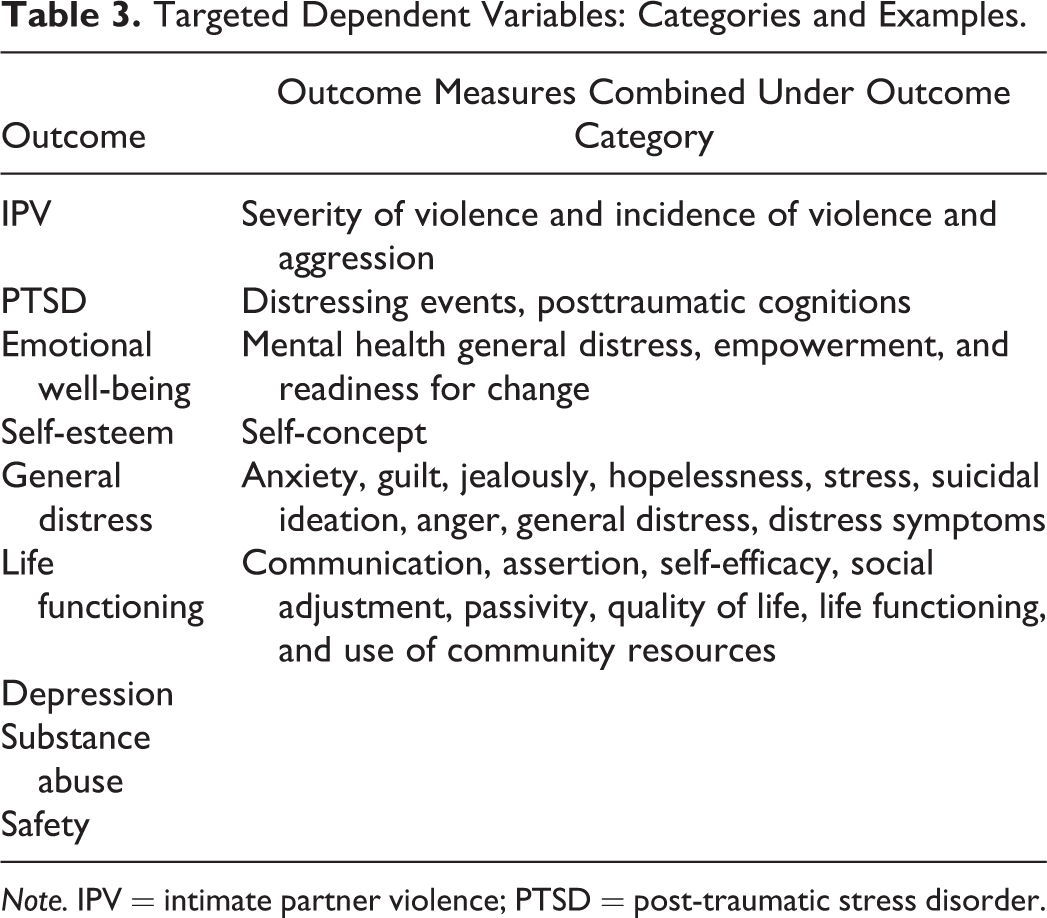
Note. IPV = intimate partner violence; PTSD = post-traumatic stress disorder.
Results
To provide a sense of context, we first provide brief narrative summaries of each of the 21 included studies. Next, we present the results from the meta-analyses.
Summary of Articles Included in the Review
Alonso and Labrador (2010). Efficacy of a Brief PTSD Intervention Program for Immigrant Women Victims of Intimate Partner Violence: A Pilot Study. Participants were 23 immigrant women, with an average age of 38.7 years, from Latin America, who had experienced IPV and meet the diagnostic and statistical manual of mental disorder fourth edition criteria for PTSD. Participants were assigned to a treatment or control group. The treatment intervention took place in outpatient clinics and the intervention consisted of 8 weekly group sessions. The treatment intervention used the “Programa de Tratamiento del TEPT para Mujeres Victimas de Violencia Domestica” curriculum developed by Labrador and Rincon (2002). The treatment intervention includes psychoeducation, cognitive–behavioral therapy, and exposure therapy. Dependent variables were PTSD, depression, self-esteem, guilt, life functioning, and posttraumatic cognitions, each measured following the intervention and at 1, 3, 6, and 12 months. Significant group differences were found for all variables at each of the measurement periods. There were no significant differences in the subscales of life functioning regarding family, work, and posttraumatic cognitions.
Cort et al. (2014). Interpersonal Psychotherapy for Depressed Women With Histories of Intimate Partner Violence. Participants were 32 women, with an average age of 39.8 years, who were receiving outpatient services at a community agency, were victims of IPV, and were experiencing moderate to severe symptoms of depression. The treatment intervention included 8 sessions of interpersonal psychotherapy (IPT) for designed for IPV survivors. This included a focus on current interpersonal problems and life events, targeting subjective emotional awareness, problematic communication, and maladjusted social responses. Dependent variables included interpersonal and psychiatric functioning, which were measured 1 week prior to treatment and 1 week and 3 months posttreatment following the intervention, and no comparison group was included. There were significant increases in interpersonal functioning and significant reductions in psychiatric symptom severity from pretreatment to posttreatment.
Crespo and Arinero (2010). Assessment of the Efficacy of Psychological Treatment of Women Victims of Violence by Their Intimate Partner. Participants were 53 Spanish women, with an average age of 41 years, who had a history of IPV and symptoms of PTSD (but not meeting full criteria). Participants were randomly assigned to two treatment conditions: exposure techniques and communication skills. Both treatment conditions took place in a community setting and included an 8-week cognitive–behavioral intervention. The first treatment condition included exposure techniques and the second included communication skills training. For both interventions, pre–posttests were used within each treatment condition. Dependent variables were PTSD symptoms, anxiety, depression, self-esteem, and anger; each was measured following the intervention and at 1, 3, 6, and 12 months. Significant group differences were found in general PTSD symptoms at 1 month, for reexperiencing symptoms following treatment; for avoidance symptoms at 1, 3, and 6 months; for hyperalertness following the intervention; for depression following the intervention and at 1 month; for anxiety following the intervention; and for anger expression following the intervention at 1, 3, 6, and 12 months. There were no significant differences in self-esteem. Many of the outcomes were greater the exposure group (general PTSD symptoms, avoidance, hyperalertness, depression, anxiety, and anger expression).
Franzblau, Echevarria, Smith, and Van Catfort (2008). A preliminary Investigation on the Effects of Giving Testimony and Learning Yogic Breathing Techniques on Battered Women’s Feelings of Depression. Participants were 40 African American (50%) and European American (50%) women between the age of 18 and 45 years, who experienced IPV within the previous year. Participants were randomized into four groups: testimony, yogic breathing, testimony and yogic breathing, and control. Each of the interventions took place in a community setting over 4 days and included 45 min each of training in testimony and/or yogic breathing. The control group did not receive any intervention. The dependent variable was depression. There were significant pre-to-post reductions in levels of depression in the three treatment groups and no difference in the control group.
Gilbert et al. (2006). An Integrated Relapse Prevention and Relationship Safety Intervention for Women on Methadone: Testing Short-term Effects on IPV and Substance Use. Participants were 34 women, with an average age of 41.8 years, who had both used illicit drugs and experienced IPV in the past 90 days and were undergoing methadone maintenance treatment. Most of the women were Latina (59.3%), followed by White (20.6), and African American (15.6). Participants were randomly assigned to treatment or control group. The treatment intervention was a twelve-session relapse prevention and relationship safety (RPRS) group that took place in a community setting. The control condition was a 1-hr presentation on community services and help-seeking tips. Dependent variables were “minor,” “severe,” or “any” IPV, substance use, depression, and PTSD symptoms. At three-month follow-up, participants in the intervention group reported significantly less minor “all of the above” (physical, sexual, and injurious IPV) and minor and severe psychological IPV. No difference was found in the report of minor or severe physical IPV, minor or server injurious IPV, and minor sexual IPV (serious sexual IPV was not calculated). No difference was found drug or alcohol use. Participants in the intervention group reported significantly less ‘sex while high on illicit drugs;’ however, no difference between groups was found on number of unprotected acts and having more than one sexual partner. Participants in the intervention group reported significantly lower depression scores. No difference between groups was found on PTSD symptomology.
Hamdan-Mansour et al. (2011). Evaluating the Mental Health of Jordanian Women in Relationships With Intimate Partner Abuse. Participants were 93 Jordanian women, with an average age of 32.4 years, who had experienced partner abuse. The intervention included eight cognitive–behavioral psychoeducational sessions that took place in a welfare center that provides services to intimate partner abuse survivors. Pre–posttests were used to measure change; no comparison group was included. Dependent variables were depression and stress. There was a significant reduction in pre-to-post level of depression. No difference was found in level of stress.
Hegarty et al. (2013). Screening and Counseling in the Primary Care Setting for Women Who Have Experienced Intimate Partner Violence (WEAVE): A Cluster Randomised Controlled Trial. Participants were 52 doctors and 137 women, with an average age of 48.1 years, who had experienced IPV or fear of partners in the past 12 months. Participants were randomized to treatment or control groups. The treatment intervention included the training of doctors on how to respond, notification of women who screened positive for IPV, and an invitation to between one and six counseling sessions, depending on client need. The intervention took place in community health clinic settings. Dependent variables were quality of life, safety planning and behavior, and mental health. No differences between groups were found on these variables following the intervention. However, at 12-month follow-up, the treatment group had lower levels of depression.
Iverson, Shenk, and Fruzzetti (2009). Dialectical Behavior Therapy for Women Victims of Domestic Abuse: A Pilot Study. Participants were 31 women, with an average age of 40.7 years, who had any history of DV victimization. Most of the women were Caucasian (97%). The intervention consisted of a 12-week dialectical behavior therapy program modified for DV and took place in a community setting. Pre–posttests were used to measure change; no comparison group was included. Dependent variables were depressive symptoms, hopelessness, social adjustment, and general distress. Significant pre-to-post change was found for each of these variables.
Johnson, Zlotnick, and Perez (2011). Cognitive Behavioral Treatment of PTSD in Residents of Battered Women’s Shelters: Results of a Randomized Control Trial. Participants were 70 women, with an average age of 32.5 years, who had experienced IPV in the prior month and had IPV-related PTSD. Half of the women were African American (50%), 42.9% were Caucasian, 4.3% were Hispanic, and 7.1 were listed as “other race.” Participants were randomly assigned to treatment or control group. The treatment intervention included Helping to Overcome PTSD through Empowerment (up to 12 sessions over 8 weeks covering psychoeducational, safety, cognitions, triggers, self-soothing, boundaries, anger management, and support systems) and standard shelter services (SSS; case management, supportive milieu, educational and support groups). The control group participated in SSS and given community referrals. Interventions took place at the shelters. Dependent variables were PTSD and reabuse. No differences were found between groups on PTSD diagnosis; however, the treatment group experienced a greater reduction in emotional numbing symptoms. Additionally, those in the treatment group reported significantly fewer incidents of reabuse.
Kaslow et al. (2010). Suicidal, Abused African American Women’s Response to a Culturally Informed Intervention. Participants were 208 African American women, with an average age of 34.7 years, with low socioeconomic status and who had experienced IPV and had a suicide attempt in the past year. Participants were randomly assigned to treatment or control group. The treatment intervention included a 10-week manualized-psychoeducation group that was empowerment focused and culturally informed which took place in a community setting. The control group consisted of medical and psychiatric care and weekly suicide and IPV support groups. Dependent variables were general distress, suicidal ideation, and depressive and PTSD symptoms. The treatment group experienced a quicker reduction of depressive symptoms and general distress and also a greater reduction in depressive symptoms at treatment end. There were no significant differences between groups on suicidal ideation and PTSD symptoms. Following the intervention, women from the treatment group experienced less psychological symptomology when exposed to IPV.
Kim and Kim (2001). The Effects of Group Intervention for Battered Women in Korea. Participants were 30 Korean women, with an average age of 35.8 years, recruited from two DV shelters in Seoul, Korea, funded and operated by the Korean government. Participants were randomized to treatment or control group. The intervention was conducted at the shelters and used in this study consisted of eight 90-min group sessions that involved the following topics: (1) assessment of trauma, (2) identification of major problems, (3) dealing with feelings, (4) understanding of self, (5) identifying batterer characteristics, (6) improving stress management strategies, (7) developing an action plan, and (8) promoting empowerment. Dependent variables were depression, anxiety, and self-esteem. There were no significant differences in changes to depression, state anxiety, or self-esteem between the two groups. There was significant difference between the groups on reduction of trait anxiety, with the treatment group experiencing a greater reduction.
Kubany, Hill, and Owens (2003). Cognitive Trauma Therapy for Battered Women with PTSD: Preliminary Findings. Participants were 37 women, with an average age of 36 years, who had experienced battering and were referred by agencies that provide services to battered women. Most of the women were White (49%), followed by Asian (27%), Pacific Islander (16%), and Black and Puerto Rican (8%). Participants were randomized to an immediate or delayed treatment condition. The treatment intervention was cognitive trauma therapy for battered women (CTT-BW), which included of 8–11 90-min individual therapy sessions conducted in an outpatient clinic. The CTT-BW intervention included psychoeducation, exposure exercises, cognitive restructuring, progressive muscle relaxation, and assertiveness skills. Dependent variables were PTSD, traumatic events, depression, guilt, self-esteem, and therapy satisfaction. PTSD remitted in 30 of 32 of the participants and gains were maintained at 3 month follow-up.
Kubany et al. (2004). Cognitive Trauma Therapy for Battered Women With PTSD. The intervention used in this study was CTT-BW (see description of Kubany et al., 2004). Study participants were 125 women with an average age of 42.2 years, who were have experienced battering and referred by victim services agencies. Most of the women were White (53%), followed by “other” or “mixed” (14%) Native Hawaiian (8%), Filipino (7%), Japanese (6%), Black (5%), Samoan (%), and American Indian (2%). Participants were randomized to an immediate or delayed treatment condition. The treatment intervention was CTT-BW, which included of 8–11 90-min individual therapy sessions conducted in an outpatient clinic. Dependent variables were PTSD, traumatic events, depression, self-esteem, guilt, and therapy satisfaction and were measured pretreatment, posttreatment, and 3 and 6 months follow-up. PTSD remitted in 87% of the participants and gains were maintained at 3 and 6 months follow-ups.
Labrador and Alonso (2007). Efficacy of a Brief PTSD Intervention Program for Mexican Women Victims of Intimate Partner Violence. Participants were 34 Mexican women, with an average age of 35 years, who were victims of IPV and met the criteria for a PTSD diagnosis. The treatment intervention took place in outpatient clinics and DV shelters. The intervention consisted of eight 100 min weekly group sessions using Programa de Tratamiento del TEPT para Mujeres Victimas de Violencia Domestica, a curriculum developed by Labrador and Rincon (2002). The treatment intervention used psychoeducation, cognitive–behavioral therapy (CBT), and exposure therapy. Pre–posttests were used to measure change, and no control group was included. Dependent variables were PTSD, depression, self-esteem, guilt, life functioning, and posttraumatic cognitions, and each was measured following the intervention and at 1 and 3 months postintervention. Significant pre-to-post change was found in all variables at each measurement time.
Labrador, Velasco, and Rincon (2006). Efficacy of a Brief PTSD Intervention Program for Women Victims of Intimate Partner Violence. Participants were 20 Spanish women, with an average age of 35 years, who were victims of IPV and met the criteria for a PTSD diagnosis. Participants were randomly assigned to treatment or control group, and the control group was defined as delayed treatment and began the interventions 60 days after pretest. The treatment intervention included eight 60 min weekly individual sessions at outpatient clinics and was based on the bi-process theory of Brewin, Dalgleish, and Joseph (1996). This treatment typically includes cognitive interventions first that are followed by exposure interventions. In this study, two experimental groups were used, one following the traditional method of cognitive interventions first and the second where the order was reversed. Dependent variables were PTSD, depression, self-esteem, life functioning, and posttraumatic cognitions. Significant group differences were found for all variables except posttraumatic cognitions in both experimental groups.
Lindquist, Telch, and Taylor (1983). Evaluation of a Conjugal Violence Treatment Program: A Pilot Study. Participants were eight couples (eight men and eight women) who were either married or cohabiting for at least 1 year, had experienced interpersonal violence, and were self-referred or court ordered to treatment. Participants ranged in age from 23 to 57 years. The treatment intervention included 9 weekly 2-hr group psychotherapy sessions at an outpatient clinic. The intervention focused on anger and stress management, with cognitive–behavioral interventions for self-talk, relaxation, and role-play. Pre–posttests were used to measure change at 6 weeks and 6 months posttreatment, and no comparison group was included. Dependent variables were anger, aggression, assertion, jealousy, communication, passivity, self-concept, and sex-role stereotypes; each measured before and after treatment and at 6 weeks and 6 months follow-up. Significant changes were observed on each of the variables, with the exception of passivity, self-concept, and sex roles.
Mancoske, Standifer, and Cauley (1994). The Effectiveness of Brief Counseling Services for Battered Women. Participants were 20 women who had an average age of 28.5 years and who requested services from a community-based battered women’s program. Over half of the women were White (65%), followed by African American (25%), Hispanic (1%), Native American (1%), and Asian (1%). Participants were randomized into two treatment conditions. The first intervention included standard crisis intervention followed by eight sessions of grief resolution. The second intervention substituted the grief resolution with eight sessions of feminist-oriented counseling. The feminist-oriented counseling approach involved an interpersonal focus rather than an intrapersonal focus. Dependent variables were self-esteem, self-efficacy, and attitudes toward feminism. Participants in the grief counseling intervention experienced statistically significant improvement in self-esteem and self-efficacy but not in attitudes toward feminism. Participants in the feminism approach did not experience significant changes on any of the variables.
McNamara, Ertl, March, and Walker (1997). Short-Term Response to Counseling and Case Management Intervention in a DV Shelter. Participants were 81 women who had an average age of 31.8 years and were receiving services at a DV shelter. Most of the participants were as Euro American (79%), followed by “minorities” (7%) and “missing data” (14%). Participants received either counseling (22%) or case management services (22%). Dependent variables were global improvement, global life satisfaction, ability to cope, and physical and psychological abuse. Participants in both counseling and case management services experienced increases in global improvement after the intake session, life satisfaction improved significantly after the three sessions. Both groups also experienced increases in coping ability and decreases in physical and psychological abuse.
McNamara, Tamanini, and Walker (2008). The Impact of Short-Term Counseling at a Domestic Violence Shelter. Study participants were 119 women, with an average age of 34.4 years, who requested services at a DV shelter. Most of the women were White (94%), the remaining 6% were Black, Asian, Hispanic, American Indian, and other. The intervention was described as eclectic counseling, involving elements of feminist theory, cognitive behavioral, existential, solution focused, and family systems theory. Pre–posttests were used to measure change, and no comparison group was included. Dependent variables were measured by the Outcomes Questionnaire (OQ) 45.5 (total OQ 45.5 score, symptoms of distress, interpersonal relationships, and social role) and the Life Coping Inventory (LCI; finance/employment, work/employment, family, partner/spouse, housing/living, and overall score). The participants experienced significant improvement on all of the OQ 45.5 subscales and total score. Additionally, significant changes were experienced the LCI total score and subscales, except work/employment and family.
Rassmusen, Hughes, and Murray (2008). Applying Motivational Interviewing in a Domestic Violence Shelter: A Pilot Study Evaluating the Training of Shelter Staff. Study participants were 20 women, with an average age of 37 years, who were residing in a DV shelter. Most of the women were White (45%), Latina (35%), African American (15%), and Asian American (5%). This was a quasi-experimental study that compared the women (10) who received regular treatment services with women who received regular treatment services from clinicians who were trained in motivational interviewing (MI). The dependent variable was readiness for changes. Participants in the treatment condition with the MI-trained clinicians experienced significantly greater readiness for treatment.
Zlotnick, Capezza, and Parker (2011). An Interpersonally Based Intervention for Low-Income Pregnant Women With Intimate Partner Violence: A Pilot Study. Participants were 54 women, with an average age of 23.8 years, who were pregnant, had low income, and had experienced IPV within the previous year. Most of the women were Hispanic (42%), followed by White (39%), Black (11%), and other (7%). Participants were randomly assigned to treatment and control groups. The treatment intervention took place at an outpatient pregnancy clinic included four 1-hr therapy IPT sessions, with a focus on enhancing social support and improving overall interpersonal functioning. The control group received standard medical care. Dependent variables in this study were PTSD, depression, and incidence of violence, which were measured pretreatment and posttreatment and 2 weeks and 3 months postpartum. Results indicated no significant reductions in any of three measures at immediate follow-up but significant reductions in PTSD and depression at follow-up. Table 6 provides detailed information on the studies and their treatment characteristics.
Meta-Analysis Results and Implications in Practice
In an effort to gauge the quantitative impact of programs targeting survivors of DV, we now turn to the meta-analytic results. In total, 21 articles reported data that allowed for effect size calculation. Of these, two studies involved multiple comparisons of a treatment group. Specifically, Franzblau et al. (2008) had three treatment conditions and Mancoske et al (1994) had two treatment conditions. Thus, a total of 24 separate study-wide effect sizes were available from the literature. Data for these effects can be found in Table 4.
Study Effect Sizes.
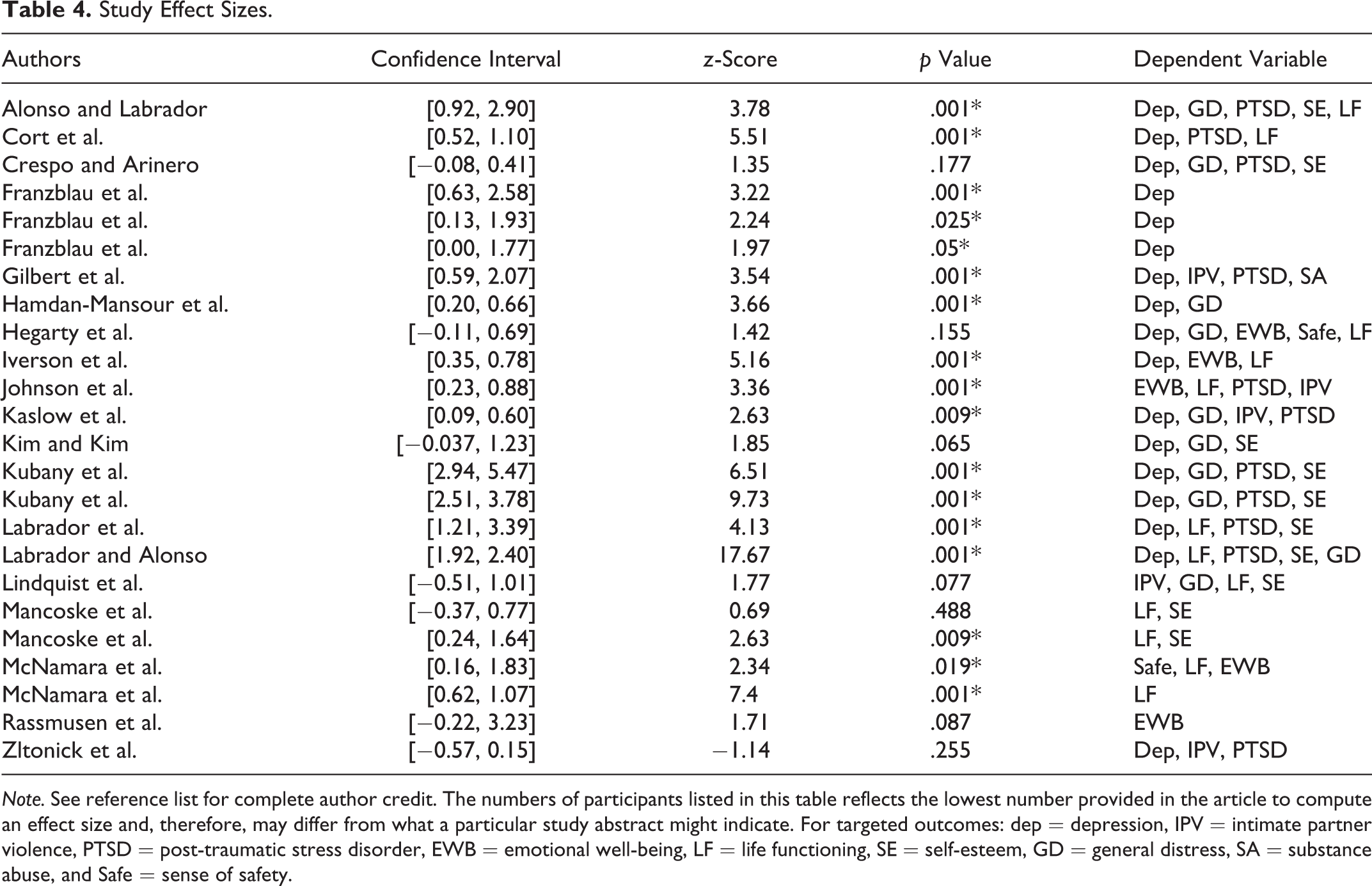
Note. See reference list for complete author credit. The numbers of participants listed in this table reflects the lowest number provided in the article to compute an effect size and, therefore, may differ from what a particular study abstract might indicate. For targeted outcomes: dep = depression, IPV = intimate partner violence, PTSD = post-traumatic stress disorder, EWB = emotional well-being, LF = life functioning, SE = self-esteem, GD = general distress, SA = substance abuse, and Safe = sense of safety.
For meta-analytic analyses, Comprehensive Meta-Analysis software version 3.3070 (Borenstein et al., 2005) was used to calculate the effect size, to calculate summary and descriptive statistics, and to conduct moderator analyses. Hedge’s g, similar to Cohen’s d, was used as the effect size measure to protect against overestimating the standardized mean difference. The software package allows for entry of multiple data entry formats. Where possible, the maximum amount of data was entered to provide a more reliable estimate of the effect. For example, if means and standard deviations (SDs) were available, they would be inputted even if p values were also available. A random effects model was used because our search strategy may not have captured the entire population of studies examining short-term treatment for IPV survivors (Lipsey & Wilson, 2001). Consistent with this approach, regression analyses for continuously distributed moderators utilized the “unrestricted maximum likelihood” method, which is similar to the random effects model (Morton, Adams, Suttorp, & Shekelle, 2004).
While multiple effect sizes derived from a single study are not technically independent, this is unlikely to cause biased estimates in meta-analyses. Hunter and Schmidt (2004, p. 432) state, “violations of independence cause no bias in estimates of mean values in meta-analysis.” Also, Borenstein, Hedges, Higgins, and Rothstein (2009) make a case that including multiple measures from a particular study often serves to produce a more conservative effect size estimate, as the variance is often underestimated. Other groups suggest analyses should be calculated at the effect size level to optimize statistical power to detect true differences in moderator analyses (Hedges & Pigott, 2004; O’Mara & Marsh, 2007). In this study, we report results at the effect size level and at the study level. Inclusivity of data and management of potential Type 1 error were the determining criteria for reporting at the effect size or study level. Thus, we reported summary statistics at the effect size level when this allowed all data to be captured. For example, because some studies reported on more than one outcome (e.g., depression, PTSD symptoms, and safety), analysis of the impact of short-term psychotherapies on outcomes was calculated at the effect-size level to allow all data to be captured. Conversely, most moderator analyses were run at the study level because a given moderator within a particular study was constant for all outcomes in that study.
As a guide to interpretation, Cohen (1988) suggests that effect sizes in the 0.20 range are statistically significant yet small, whereas effects in the 0.50 range are moderate and those near 0.80 are large. Further, as effect sizes are translated to SDs, it is estimated that an effect size of 1.0 suggests a 34% gain, an effect size of 0.80 suggests a 29% gain, an effect size of 0.50 suggests a 19% gain, and an effect of 0.20 suggests a gain of 8% (all assuming a starting point at the 50th percentile). Effect sizes are not linearly related to percentile gain, such that percentile gain tops out once effects are beyond the 2.0 or 2 SD units. For example, an effect size of 2.0 represents an approximate gain of 48%, which would correlate with the 98th percentile on the bell curve, and effect sizes beyond 2.20 all represent about a 49% gain once the 99% percentile is reached (see Lipsey et al., 2012).
We now turn to the results of the meta-analyses, guided by questions of possible interest to practitioners. See Table 4 and Table 5 for specific statistical findings.
Effect Sizes Organized Around Targeted Outcomes.

Note. PTSD = post-traumatic stress disorder.
Study and Treatment Characteristics.
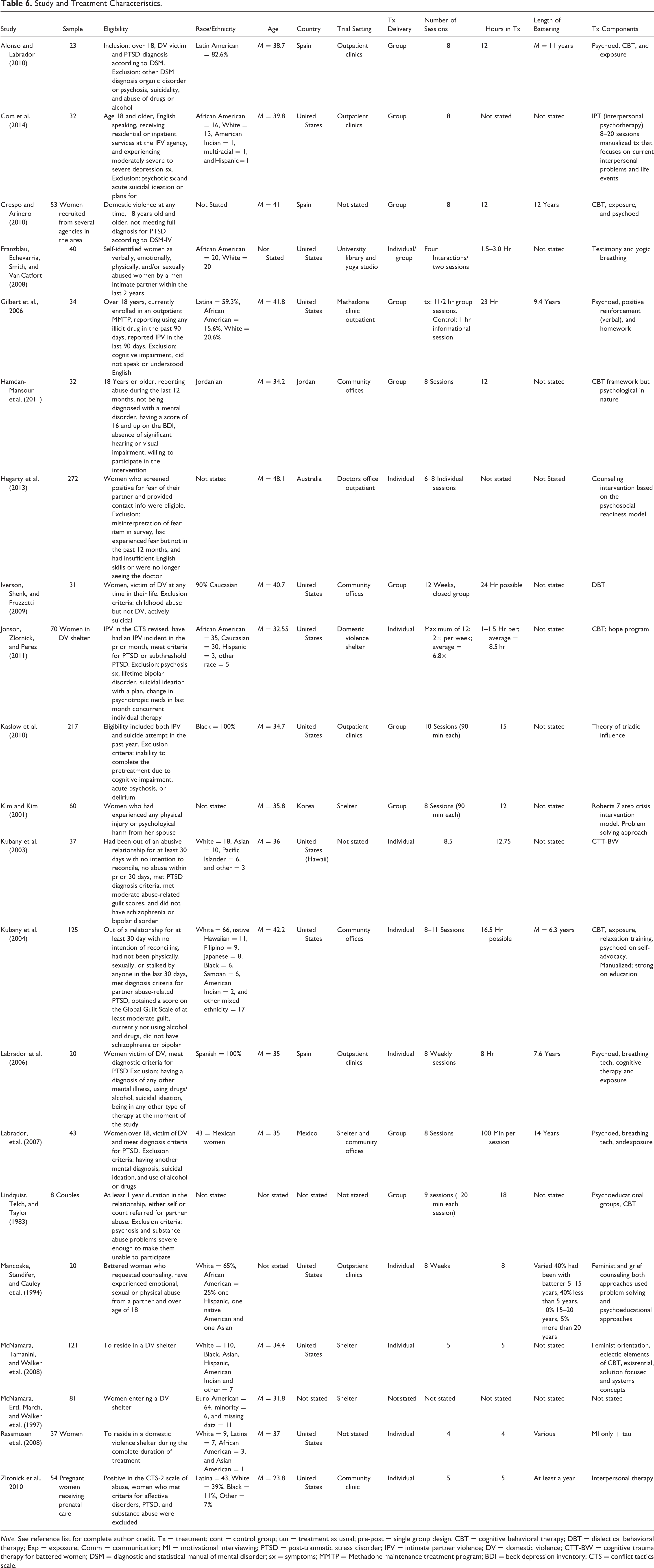
Note. See reference list for complete author credit. Tx = treatment; cont = control group; tau = treatment as usual; pre-post = single group design. CBT = cognitive behavioral therapy; DBT = dialectical behavioral therapy; Exp = exposure; Comm = communication; MI = motivational interviewing; PTSD = post-traumatic stress disorder; IPV = intimate partner violence; DV = domestic violence; CTT-BW = cognitive trauma therapy for battered women; DSM = diagnostic and statistical manual of mental disorder; sx = symptoms; MMTP = Methadone maintenance treatment program; BDI = beck depression inventory; CTS = conflict tactics scale.
Does short-term treatment help individuals who have suffered IPV? The overall effect, across all dependent variables and studies, shows an impressive outcome with an omnibus effect size in the large range, Hedge’s g = 1.02 (confidence interval [CI] = [0.71, 1.33]), z-value = 6.39, p < .001. Thus, across all of the variables, it appears that treatment is effective, resulting in about a 34% advantage. As is often the case in meta-analyses, the omnibus effect size in this study cannot be simply relied upon as a good estimate for all treatments and all outcomes as significant heterogeneity was present, Q-within = 317.53 (df = 21), p < .011. Thus, we examined some moderator effects in an exploratory manner given that no primary theory guides the various interventions in our sample.
How strong were effects across the different targeted outcomes? As can be seen in Table 5, five of the targeted areas had large effect sizes, including PTSD, self-esteem, depression, general distress, and life functioning. Four of the targeted areas had effects in the moderate range, including substance use/abuse, emotional well-being, safety, and recurrence of interpersonal violence. All nine targeted outcomes reached the level of statistical significance. Significant differences were present across the nine targeted variables (Q-between = 31.38, df = 8, p < .001), however as no theoretical basis exists for predicting, which variables would show the strongest effects we did not pursue subgroup comparisons. That said, it is promising that emotional symptoms expected to result from IPV, such as PTSD and depression, show strong responses to treatment. Of concern, is that potentially fatal outcomes like perceived safety and continued exposure to IPV had only moderate effects.
Did treatment type result in differential effects? Yes, CBT and interpersonal therapies that were specifically tailored to those who had experienced IPV were most effective. However, this is a difficult question to answer given the wide range of interventions being applied (see Table 4). Many studies employed interventions that included a nonspecific form of CBT or psychological education, which we combined into a “variety group.” Four studies employed a manualized form of CBT or interpersonal therapy that were specifically developed for IPV survivors based on theories of how IPV can impact individuals, these we combined into an “IPV-tailored” group. The remaining studies employed specific interventions that did not seem to logically group together. For example, Crespo and Arinero (2010) compared an exposure therapy program to a communication group, Franzblau et al. (2008) examined the effects of yoga and providing testimony on survivors’ sense of depression, and Iverson et al. (2009) utilized dialectical behavioral therapy to promote life functioning and emotional well-being. Other studies examined MI (Rassmusen et al., 2008) or education about feminism or grief (Mancoske, Standifer, & Cauley, 1994). The only study that showed a negative effect was Zltonick et al. (2010) that compared an intervention based on interpersonal therapy compared to a treatment as usual group. Across all studies, the IPV-tailored interventions (g = 2.04, k = 4, CI = [0.87, 3.21]) produced significantly higher results than all other intervention types combined (g = 0.84, CI = [0.51, 1.16]), Q-between = 5.81, p < .001, and more than the “variety” group (g = 1.01, CI = [0.59, 1.44]), which combined a seemingly nonspecific form of CBT and/or psychoeducation, Q-between = 5.00, p < .001. Said differently, the tailored interventions showed an approximate advantage of 69% were as those that were not tailored showed about a 29% advantage. The IPV-tailored interventions were reported on by three author groups: Cort et al. (2014; this study was also based on interpersonal therapy principles), Johnson et al. (2011; CBT based), and Kubany et al. (2003 and 2004; CBT based).
Did delivery type matter? Yes, individually delivered interventions (g = 1.21, k = 11, CI = [0.66, 1.77]) produced significantly stronger outcomes than group delivered interventions (g = 0.84, k = 10, CI = [0.39, 1.30]), Q-between = 5.51, p < .001.
Are effects durable? The strength of impact from interventions attenuated over time when examined at the target variable level (i.e., k = number of measured instances of a particular outcome vs. the number of studies, see Table 5). Most programs reported outcomes immediately following the intervention, but many programs reported follow-up outcomes at 1, 3, 6, and 12 months, although the number of studies reporting outcomes declined over time from 84 immediately following the intervention to 20 at 12 months postintervention. Immediately following treatment, Hedge’s g was 1.12 (k = 84, CI = [0.93, 1.30]); at 1 month beyond treatment, Hedge’s g was 1.38 (k = 11, CI = [0.73, 2.04]); at 3 months beyond treatment, Hedge’s g was 0.80 (k = 40, CI = [0.49, 1.10]); 6 months after treatment, Hedge’s g dropped to 0.23 (k = 26, CI = [0.09, 0.38]); and at 12 months after treatment, Hedge’s g was 0.28 (k = 20, CI = [0.10, 0.46]). While effects are still in the statistically significant range at the 12-month mark, there was a considerable drop from very large to small effects.
Does the amount of treatment influence outcomes? Yes, it appears that more treatment sessions and more overall time is linked to stronger outcomes based on meta-regression. Specifically, the number of sessions was positively associated with outcomes (z-value = 5.72, p < .001) as was the total amount of time spent in counseling (z-value = 8.11, p < .001).
Does location of intervention matter? Survivors of IPV did not differentially benefit if services were delivered within a shelter (g = 1.19, k = 7, CI = [0.55, 1.83]) or outside of a shelter (g = 1.06, k = 15, CI = [0.71, 1.40]). However, IPV interventions delivered from a doctor’s office was much less effective (g = 0.03, k = 2, CI = [−0.46, 0.52]).
What impact did study design have? A wide range of study designs were utilized. The strongest effect was when a control group was used against the intervention being studied (g = 2.20, k = 6, CI = [1.16, 3.23]). Those studies which did not have a comparison group (i.e., pre–post only) showed the next highest effect (g = 0.90, k = 12, CI = [0.51, 1.29]), followed by those that compared an experimental investigation to “treatment as usual” (g = 0.29, k = 5, CI = −[0.02, 0.60]), and lastly one study compared two competing treatments groups (g = 0.17, k = 1, CI = −[0.8, 0.41]). These finding are not surprising because we found strong effects across most interventions, so studies that compared an intervention to control (no treatment group) would be expected to have the largest effects and studies that compared one treatment to another demonstrate small effects between the interventions.
What is the likelihood of publication bias? This meta-analysis incorporates data from 24 separate analyses across 21 studies, which yield a z-value of 19.01 and corresponding two-tailed p-value of .001. The fail safe N is 2,234. This means that we would need to locate and include 2,234 “null” studies in order for the combined two-tailed p-value to exceed .050. Put another way, there would be need to be 62.3 missing studies for every observed study for the reported effect to be nullified. A more conservative estimate of publication bias is the Kendall’s S statistic, which suggests a total of 118 additional studies of null effect would be needed to show evidence of publication bias. Thus, publication bias seems unlikely, and the effect sizes reported reflect the actual effects of the intervention.
Discussion
A building literature has investigated the effectiveness of brief psychological interventions for individuals who have experienced IPV. A number of intervention approaches have been delivered in different methods targeting various outcomes. Meta-analytic results suggest that, on average, such interventions are effective in helping individuals who have experienced IPV. The omnibus or overall effect suggests an approximate 34% advantage of receiving brief psychological interventions compared to not receiving treatment. Such a gain is considerable and is evidence for supporting survivors of IPV with psychological services. Understandably, the gains from treatment varied. Below, we discuss such variation in a question and answer form.
Does treatment really make an impact? Yes. Studies that used a control group found the highest advantages. Individuals who received treatment enjoyed approximately 50% gains on targeted outcomes compared to those who did not. Across the 24 comparison groups in this study, 23 of the study level effects were positive and 17 reached statistical significance.
What outcomes are targeted and do all outcomes show equal gains? While we do not have a theoretical rationale for the different outcomes measured for the various interventions, statistical analysis showed that all interventions showed improvements in symptoms compared to control groups. We organized outcomes into nine broad areas as can be seen in Table 5. Participants seemed to gain most in the areas of decreased PTSD symptoms, increased self-esteem, decreased symptoms of depression and general distress, and increases in life functioning. Indeed, these effects were in the large range with percentile gains such that receiving intervention, versus not having the intervention, resulted in gains ranging from 27% to 30%. More moderate, yet meaningful, effects were found for outcomes such as substance abuse, emotional well-being, a sense of safety, and actual instances of subsequent IPV with gains 14–17% range.
Were some interventions better than others? Yes. In reviewing the articles, it was noted that several groups adapted established interventions to the theoretical needs of IPV survivors. Those that used these IPV adapted programs demonstrate significantly better outcomes than those that used more eclectic or nonspecific interventions. If we were asked to provide a recommendation on which interventions to consider as a frontline intervention based on the results of this study, we would recommend the CBT-based treatments designed and adapted by Kubany et al. (2003, 2004), Johnson et al. (2011), and secondarily the interpersonal therapy designed by Cort et al. (2014), as they showed significantly higher results than other studies. Of these four, Kubany and colleagues have replicated findings and used a comparison group. While Johnson and colleagues also used a control group, there is no evidence of a replication study. The results of Cort and colleagues seem to be preliminary, as only one study has been conducted and it was without a control condition. Further, another study that relied on interpersonal therapy (Zltonick et al., 2010) found untoward effects.
Does delivery impact outcome? Our results found that IPV survivors could benefit equally from treatment delivered in shelters or in the community. Our results also showed that treatment dosage matters and that generally more is better. Specifically, more sessions and more intervention time were linked to better outcomes. Of course, there may be many confounds that could explain this relationship; yet, at this point, the data suggest that very brief interventions may not be as effective as longer interventions. This is not surprising due to the complex nature of IPV and the multiple needs and barriers survivors face. Also, our results suggest that individually delivered interventions are superior to group interventions. While group interventions are effective, those receiving individual attention received more benefit. It could be that individual delivery allows for greater attention, increased ability to uniquely tailor the interventions to the needs of participants, or that the needs of IPV survivors are simply better addressed through individually delivered therapies. This is an important finding, as many programs may promote more group interventions because they are more cost-effective and based on the assumption that survivors need to hear from other survivors. While the “universalizing” experience of connecting with other survivors is surely valuable for many, an individualized approach may allow for more tailored and targeted interventions that meet the unique needs of the survivor. This finding may also highlight the heterogeneity among survivors of IPV. For example, not all survivors have poor self-esteem or depression, so programs that target these outcomes rather than the uniqueness of the survivor are unlikely to have strong effects.
How durable are the effects of the interventions? The benefits of treatment certainly diminished over time. Effect sizes immediately after treatment were in the large range immediately after treatment through about 3 months after treatment. Studies that measured outcomes at the 6 and 12 months mark found that effects were in the small range (though still meaningful and statistically significant range). This attenuation may be due to regression to the mean, as it could be imagined that individuals who first seek intervention are in a state of “crisis” or high problem levels upon entering treatment and these levels simply return to a normal level with the passage of time. Or, it could be that individuals return to more problematic behaviors, such that the original gains are lost. Our data do not provide an answer to why the gains diminish over time. Future research might attempt to describe and understand this phenomenon in greater depth. Such research might explore how booster sessions could help or what modifications to the therapies might promote retention of gains.
Are the findings generalizable? While the generalizability of the findings is “probable,” replication of treatments must occur including larger samples and a more standardized intervention and rigorous methodology. Replication of studies in multiple sites with careful consideration to demographic differences and physical settings (community center vs. shelter vs. medical office), as variables such as continuing exposure to violence, threats to violence, and contemplation of reuniting with abusive partner, may impact effectiveness and generalizability of treatment effects.
Limitations
One of the goals of our study was to identify and assess the effectiveness of short-term treatments for IPV survivors. Although sexual assault survivors and single event trauma survivors may benefit from this type of interventions, sexual assault and single event trauma treatments address events that took place in the past, while DV survivors in many cases are still under threat of ongoing abuse (Warshaw, Sullivan, & Rivera, 2013). Moreover, the literature regarding sexual assault includes victims with a more diverse relationship with the perpetrator, and this may include, fathers, brothers, acquaintances, and strangers, while IPV literature is specific to violence perpetrated by an intimate partner.
The effects of IPV impact not only the parent but also the children in the home, however the studies included in this review do not mention the incorporation of children or families as group as a component of the treatment. Future studies should incorporate into treatment of other family members who were exposed to the violence, especially children.
Participants across all studies were female. Although the overall pattern suggests that women, in particular, are heavily impacted by violence over their lifetime, recent studies also indicate that many men experience sexual violence, stalking, and, in particular, physical violence by an intimate partner (Breiding et al., 2014).
Based on the descriptions of the interventions used, we can say that most interventions work and that some interventions work better, those specifically tailored to IPV. However, very few of the studies show replicated effects. Indeed, only Kubany and colleagues (2003, 2004) and Labrador and colleagues (2006, 2007) seem to have published more than one article in which they are systematically examining how to best deliver a particular program to IPV survivors. The lack of replicated findings on specific interventions is symptomatic of a larger concern of a relative lack of rigorous research in this important area. For example, only about 50% of the studies employed a comparison group. Because of this, it is difficult to assess the interaction effects between these short-term interventions and the impact of larger system issues that surely effect the well-being of the survivors. Another possible limitation of the study which is common to all systematic reviews and meta-analyses is that of missing potential articles. It is possible that important studies contained in the “gray” literature were not captured in our search and thus not included in our analysis.
Implications of the Research and Recommendations
Short-term interventions for survivors of IPV are an important component of a coordinated community response to DV. This study demonstrates that most short-term interventions are effective in addressing some of the complex needs of these survivors, although there is significant heterogeneity in the relative impact of these programs. In addition, some of the most urgent and lethal outcomes like safety and subsequent IPV have only moderate effects. This reminds us that in addition to short-term psychotherapeutic programs, survivors need a system of care that can address not just their intrapsychic needs but the systematic, institutional, financial, and cultural barriers that survivors face. This research also provides evidence that the most effective short-term programs are grounded in traditional evidence-based interventions like CBT with specific adaptation to meet the needs of IPV survivors, like a trauma-informed or gender-specific approach.
This study also highlights the need for further research on interventions for IPV survivors. Few high-quality studies using strong experimental designs are present in the existing literature. While several showed strong effects, more research and particularly replication studies on the most promising interventions are needed to move toward establishing best-practice guidelines for this population. Furthermore, there remain questions about the theoretical basis for various treatment targets and approaches with survivors of IPV. More research is needed that informs the development of targeted interventions in various treatment settings and with different genders and ethnic groups. Finally, while this study focused on short-term interventions, these programs are embedded in larger system responses, so research is needed that examines the interaction effects between these short-term interventions and larger system issues things like access to community resources, awareness, and funding.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.