
Abstract
Attachment status in early childhood is a key yet modifiable contributor to the development of social–emotional competence. The security and organization of the infant–mother attachment bond is particularly susceptible to stressors in the caregiving environment. While the impacts of normative interparental conflict on infant attachment are increasingly understood, the potentially unique place of intimate partner violence (IPV) in this pathway has been under-researched. This study surveyed all empirical work in this area, including unpublished literature (k = 6, N = 3,394), to examine meta-analytic associations between maternal experiences of IPV and offspring attachment security (ages 1–5 years) measured at least 6 months post-IPV exposure. Mothers’ reports of IPV from pregnancy onward were inversely associated with offspring attachment security, r = −.23, CI [−0.42, −0.04], p = .02. Sample risk characteristics (e.g., clinical vs. community) moderated this association; child’s age at attachment measurement and method of assessing child attachment (e.g., observational, representational, parent report) also moderated at a trend level. Implications for early screening, intervention, and future research are discussed.
Introduction
Attachment security in early childhood is repeatedly found to contribute to the development of social–emotional competence, with small-to-moderate associations with other measures of socio-emotional functioning (Granqvist et al., 2017; Madigan, Atkinson, Laurin, & Benoit, 2013; Tharner et al., 2012). Rates of attachment insecurity increase as risk factors increase in the caregiving environment. Early attachment security is shown to have optimal impact on emerging brain structures and circuitry associated with regulatory capacity with a lasting positive developmental legacy for related social and emotional functioning (Feldman, 2017). A body of longitudinal research shows repeated associations between suboptimal attachment development, particularly attachment disorganization and perinatal risk exposure, including to caregiving stress (Bornstein, 2014; Groh, Fearon, van IJzendoorn, Bakermans-Kranenburg, & Roisman, 2017). Relative to the three organized forms of attachment, disorganized attachments are typified by intense contradictory behavioral strategies and/or relational incoherence in the infant during peak moments of stress for the child (Main & Solomon, 1990). Risk mechanisms include transmission via interparental trauma in the context of problematic interparental relationships (Behrens, Haltigan, & Bahm, 2016; Lieberman, Zeanah, & McIntosh, 2011). For example, higher rates of distorted or negative attributions by mothers to their infants have been found in samples of women diagnosed with post-traumatic stress disorder (PTSD) resulting from interpersonal violence trauma (Schechter, 2003). Long-term negative effects for the behavior of children exposed to intimate partner violence (IPV) prior to the age of 3 years are clear by school entry (Holmes, 2013; Levendosky, Bogat, Huth-Bocks, Rosenblum, & von Eye, 2011). Such findings are consistent with proposed cascade mechanisms of impact for infants, including the accruing developmental risks of early attachment insecurity (Fearon, Bakermans-Kranenburg, van IJzendoorn, Lapsley, & Roisman, 2010).
Despite the mounting evidence, the magnitude of influence of mother’s IPV exposure on offspring attachment development has yet to attract meta-analytic evidence. Research from related fields suggests an association is likely and worth examination. For example, significant effects on infant attachment insecurity are found for maternal depression (r = .18, Atkinson et al., 2000), maternal life stressors (r = .19, Atkinson et al., 2000), and caregiver insensitivity (r = .35, Verhage et al., 2016). Of direct relevance, non-IPV interparental conflict is significantly associated with offspring attachment insecurity (r = −.28, Tan, McIntosh, Kothe, Opie, & Olsson, 2018).
IPV Prevalence
Public health prevalence estimates underscore the importance of IPV research. The most recent national data reported by the U.S. National Intimate Partner and Sexual Violence Survey (Smith et al., 2018) showed 30.6% of 5,758 women experienced physical IPV during adulthood, 18.3% experienced sexual IPV, and 10.4% experienced stalking. In other countries, rates may vary and reflect definitional differences. Multiple studies found that more than half of women report having a child in their care at the time of an IPV incident and that violence was most often perpetrated by a former partner (Fleury, Sullivan, & Bybee, 2000; Ornstein & Rickne, 2013; Watts & Zimmerman, 2002).
Lifetime estimates of childhood exposure to IPV in the United States were approximately 16% (Finkelhor, Turner, Shattuck, & Hamby, 2015; McDonald, Jouriles, Ramisetty-Mikler, Caetano, & Green, 2006). Relative to intact two-parent households, rates of children’s exposure to IPV were 7 times higher in recently separated families and 6 times higher in sole parent families (McIntosh, Wells, & Lee, 2016; Zill, 2014). Robust population estimates for infants and preschoolers are not available, but research suggests exposures to interparental violence are highest for children under 5 years old (e.g., De Maio, Kaspiew, Smart, Dunstan, & Moore, 2013).
Sequelae for mother and child
The proportion of the preventable disease burden on women’s mental health of physical, sexual, and emotional IPV was estimated to be 2.2% with 24% of that burden resulting in fatal outcomes (Ayre, Lum On, Webster, Gourley, & Moon, 2016). IPV is a consistent risk factor for women’s suicide attempts after adjusting for common mental health disorders (Garcia-Moreno et al., 2006) and has been linked to increased risk for depression, anxiety, and PTSD (Lagdon, Armour, & Stringer, 2014).
Meta-analytic estimates show robust associations between young children’s exposure to physical IPV and a variety of psychological, emotional, and developmental problems (Evans, Davies, & DiLillo, 2008; Kitzmann, Gaylord, Holt, & Kenny, 2003; Vu, Jouriles, McDonald, & Rosenfield, 2016; Wolfe, Crooks, Lee, McIntyre-Smith, & Jaffe, 2003). Amassing evidence also finds exposures in the antenatal window linked to offspring regulatory outcomes, through the impacts of dysregulated cortisol reactivity (Levendosky et al., 2016; Martinez-Torteya, Bogat, Levendosky, & von Eye, 2016). Sleeper effects have been noted, indicating a long-term negative effect on the behavior of children who have been exposed to IPV prior to the age of 3 years, with effects of early IPV exposure most evident at school entry (Holmes, 2013), possibly reflecting accruing developmental risks of early attachment disorganization (Levendosky et al., 2011).
Background to Attachment and Its Classification
Infant attachment classification focuses on the patterning of the infant’s initiative in seeking proximity (psychological and physical) to the attachment figure under conditions of threat or stress for the purpose of psychological safety. The infant Strange Situation Procedure (SSP; Ainsworth, Blehar, Waters, & Wall, 1978) is the most highly validated approach to measurement of attachment in the infant and preschool years. It is a 21-min laboratory-based observation involving the infant and parent in play in a new environment, the introduction of a stranger, two separations of the infant and parent, and two reunions. The Cassidy and Marvin (1992) Preschool Attachment Classification System is an adaptation of the SSP infant classification system for 3–4 years old, and it remains the gold standard observational method for assessment of this age-group.
Using such observational systems, attachment classification defines the pattern of behaviors as either secure or one of the three forms of insecure attachment (i.e., avoidant, resistant, or disorganized). Young children whose attachment is classified as “secure” actively seek psychological or physical proximity on reunion, are relatively easily soothed by the parent, and display little if any avoidance or angry resistance when in need (Berlin, Zeanah, & Lieberman, 2008; Lyons-Ruth & Jacobvitz, 2008). Those classified as “insecure/avoidant” show minimal affect, ignore, or are neutral with respect to the caregiver and actively direct attention away from their emotional state rather than seeking restoration through proximity. The second insecure group is the “insecure/ambivalent” or “insecure/resistant” classification. These children show distress on separation yet are not readily soothed by the return of the parent, instead demonstrating a mix of proximity-seeking and angry behaviors toward the parent. Although both the avoidant and ambivalent groups are regarded as suboptimal to the secure group, the strategies in dealing with stress are nonetheless regarded as organized and predictable.
In contrast, disorganized attachment is marked by contradictory, oblique behaviors by the infant toward the parent at points of stress, particularly on reunion following a separation. Some characteristics of disorganized infant behaviors include simultaneous display of approach and avoidance, incongruous, misdirected, incomplete movements and expressions; redirecting need away from the attachment figure when stressed; and direct displays of disorientation around or apprehension of the parent such as the infant stumbling, freezing, or falling at reunion (Main & Solomon, 1990). The disorganized/disoriented attachment style was shown to be associated with anomalous parental behaviors regarded as confusing or traumatic including fearful and frightening stances toward the infant (Main & Hesse, 1990). Proportions of attachment disorganization vary from 15% in low-risk samples (Van IJzendoorn, Schuengel, & Bakermans–Kranenburg, 1999) to 77–90% in high-risk maltreated samples (Barnett, Ganiban, & Cicchetti, 1999; Carlson, Cicchetti, Barnett, & Braunwald, 1989; Cicchetti, Rogosch, & Toth, 2006; Van IJzendoorn, 1995). Disorganized attachment remains stable as a pattern across the early years for 36% of children from general population samples and for up to 80% of clinical samples (Groh et al., 2017; Opie, 2019).
Sequelae of early attachment insecurity
Across multiple studies, insecure attachment early in life is associated with altered regulatory capacity, manifest in problematic internalizing behaviors (e.g., depression, anxiety; 60 studies, 5,236 families; Madigan et al., 2013) and externalizing behaviors (e.g., conduct disorder; 69 studies, 5,947 families; Fearon et al., 2010). Attachment disorganization is a precursor to poor cognitive and socio-emotional outcomes for the child (Lyons-Ruth & Jacobvitz, 2008; Van IJzendoorn et al., 1999; Verhage et al., 2016), later psychopathology in middle childhood (Lyons-Ruth & Jacobvitz, 2008), and dissociative and borderline personality symptoms in adolescence and early adulthood, including suicidal ideation (Lyons-Ruth, 2008).
Transmission mechanisms
Elevated risk for attachment insecurity via impaired caregiving sensitivity has been established in meta-analyses and is moderated by maternal capacity for mentalization, meaning a mother’s capacity for reflection on her own mental experience, in the face of trauma (Van IJzendoorn & Bakermans-Kranenburg, 2019; Verhage et al., 2016) and the development of maternal representations of the parent–infant bond (Ammaniti, 1991; Huth-Bocks, Levendosky, Theran, & Bogat, 2004; Huth-Bocks, Levendosky, Bogat, & von Eye, 2004). The caregiving system becomes measurable during pregnancy with the development of maternal caregiving representations, which are related to later caregiving behaviors (Dayton, Levendosky, Davidson, & Bogat, 2010). After the baby is born, optimally, the mother responds promptly to infant signals, soothing and comforting in a manner reliable enough that the infant learns to predict and anticipate her responses. Reciprocal affective moment-to-moment communication gestures by the mother, including eye gaze, tone of voice, touch and body orientation toward the infant, are all part of this complex interplay (Beebe & Lachmann, 2002). In benign and “good-enough” conditions, the repetition of this experience reinforces neural networks associated with safety in the face of stress or threat, and over time, the mother comes to represent a secure base for the infant. Conversely, inconsistent or disturbed relational interactions led by the mother are characterized by affect dys-synchrony including unreliable, misattuned, and mistimed maternal responses (Beebe et al., 2010) and in turn elevated infant stress and confusion (Biringen, 2000).
Transmission in the context of IPV
Higher rates of distorted maternal representations or negative attribution by mothers to their infants have been found in samples of women diagnosed with PTSD related to trauma from intimate partner violence (Schechter, 2003). Evidence suggests that acute and chronic IPV experience commencing in the antenatal period impacts mother’s psychological functioning in the postnatal period through transmission of alarm, fear, numbing, and/or helplessness to her infant and an impeded capacity to recognize and respond to her child’s attachment needs (Huth-Bocks, Levendosky, Bogat, & von Eye, 2004; Levendosky, Huth-Bocks, Shapiro, & Semel, 2003; Levendosky, Lynch, & Graham-Bermann, 2000). In this context, IPV is understood not only as “an assault on women, but on the caregiving system as a whole” (Levendosky, Lannert, & Yalch, 2012, p. 402).
Meta-analytic evidence for a direct association between mother’s victimization from partner violence and the attachment security of her offspring has not yet been examined. While a recent meta-analytic study (Tan et al., 2018) confirmed a negative association (r = −.28) between exposures to normative interparental conflict and offspring attachment security at ages 0–5 years, that study excluded exposure to IPV. Given the significant potential of IPV to impair parental responsivity, the current study is a vital extension of that meta-analytic work.
While fathers’ experience of IPV victimization occurs, it is typically different than that of mothers in degree and type in both Eastern and Western societies, where women are at higher risk than men for financial control, and for dangerous, fear-inducing, or physically injurious outcomes from IPV (e.g., Australian Bureau of Statistics, 2017; Garcia-Moreno et al., 2006; Smith et al., 2018). Clearly, when fathers are victims of serious or chronic IPV, the attendant strain may impact the infant–father attachment relationship, and documentation of these processes will be an important direction in future research. Given that the existing research sufficient for meta-analytic examination comprises only mother–infant samples, our meta-analysis focuses on mothers.
Research on moderating factors
A broad set of variables that influence the transmission pathway between mothers’ experience of relational violence and child socio-emotional developmental outcomes has been studied. Mother’s experience of recent separation, intergenerational abuse, severity of post-traumatic stress, attributional style, and depressive symptomatology predict severity of her child’s symptoms (Berzenski, Madden, & Yates, 2019; Dallaire et al., 2008; Schechter et al., 2007). Protective influences are found in family support and sensitive parenting following mothers’ trauma exposures (Dallaire et al., 2008; Graham-Bermann, Gruber, Howell, & Girz, 2009). Within studies of IPV and offspring attachment, few moderating factors have been examined frequently enough to allow examination in the present meta-analysis. Therefore, we briefly review those where adequate data allowed inclusion in our analyses.
Type of IPV assessed
The type of IPV a mother has experienced is important to understand. Beyond early characterizations of IPV solely as acts of physical aggression (Evans et al., 2008; Kitzmann et al., 2003), the conceptualization of IPV has broadened in recent years to include psychological and/or sexual IPV, allowing for a more comprehensive understanding of the impacts of various IPV types on both mother and child (e.g., Huang, Wang, & Warrener, 2010; Jouriles, McDonald, Vu, & Sargent, 2016; Jouriles, Norwood, McDonald, Vincent, & Mahoney, 1996; Schnurr & Lohman, 2013; Vu et al., 2016; Zarling et al., 2013). Evidence from the attachment and caregiving literature suggests both emotionally and physically based trauma experiences impact adult attachment representations and caregiving states of mind (O’Connor & Elklit, 2008).
At-risk characteristics of sample
In other fields, severity of trauma exposure is found to differentially impact caregiving state of mind; thus, measurement of this influence is likely to be important in the study of offspring attachment outcomes (Schechter et al., 2007). Distinguishing the severity of trauma exposure in the available research has usually involved contrasting clinical and/or shelter samples with community samples (Nathanson, Shorey, Tirone, & Rhatigan, 2012; Seedat, Stein, & Forde, 2005). Thus, attending to sampling as an indicator of risk status seems key to meta-analytic enquiry of risk outcomes (Verhage et al., 2016) and equally to furthering our understanding of protective environments as important moderators.
IPV witnessed by child
A body of work highlights the importance of accounting for the nature of children’s exposure to IPV as a moderator in meta-analytic pathways (Margolin, 1998; Wathen & MacMillan, 2013). In an Australian sample of separated parents, Kaspiew et al. (2009) found that of 10,002 separated parents surveyed, 17% of fathers and 26% of mothers reported experiencing physical hurt from their partner before separation. Of these, 72% of mothers and 63% of fathers reported that their children had witnessed the violence. There were higher levels of reported behavioral problems in children aged between 1 and 3 years who on parent report had witnessed physical violence compared to children who had never witnessed violence.
Child age and time lag between assessments
Linked with this, children under 3 years are more likely to directly witness violent episodes between their parents than older children (Gewirtz & Edleson, 2007). The developmental sequelae of trauma exposures during the years 0–3, the peak period for the establishment of co-regulatory and self-regulatory functions, may be significant in their cascading influence (Perry, Pollard, Blakley, Baker, & Vigilante, 1995; Schore & McIntosh, 2011). The moderating role of child age or developmental stage at the time of IPV exposure and the lag between attachment assessment and IPV exposure may be important moderating influences.
Measurement heterogeneity
Assessment methods influence the predictive validity of both IPV and attachment status, and the significant measurement heterogeneity for both constructs needs careful methodological consideration. IPV victimization is measured variously using self-report questionnaires such as the well-validated Conflict Tactics Scale (Straus, 1979; Straus, Hamby, Boney-McCoy, & Sugarman, 1996), the Severity of Violence Against Women Scales (Marshall, 1992), the DOORS (McIntosh et al., 2016; Wells, Lee, Li, Tan, & McIntosh, 2018), and interview-based assessments such as the Partner Violence Interview (Zeanah, Hirshberg, Danis, Brennan, & Miller, 1995). Nonbehaviorally specific measures and interview formats underestimate parents’ reports of IPV experiences (Ballard, Holtzworth-Munroe, Applegate, & Beck, 2011; Rossi et al., 2015).
Although meta-analytic evidence (Tan et al., 2018; Van IJzendoorn, Vereijken, Bakermans-Kranenburg, & Riksen-Walraven, 2004) favors attachment measurement by an independent, reliable observer, parent report methods still appear in the literature. The SSP and its preschool adaptation (Ainsworth et al., 1978; Cassidy & Marvin, 1992), and the Attachment Q-Sort (AQS; Waters & Deane, 1985) remain the gold standard methods. The latter (AQS) may also be parent rated. Representational procedures administered directly to the child may also be used, such as the Attachment Story Completion Task (Bretherton, Ridgeway, & Cassidy, 1990).
Publication information
Finally, given advances in methodology, it is good practice to account for the recency of findings (year of publication) and for potential cross-cultural differences (country of publication; Lin & Chu, 2018).
The Current Study
Given the centrality of the mother–infant relationship in the prediction of multiple developmental outcomes, the need to examine meta-analytic evidence in this domain is clear. We survey and examine all available longitudinal data sources reporting on mother’s IPV victimization and the subsequent offspring attachment relationship for children aged 1–5 years. We first examine the direct relationship between mother’s IPV experience and offspring attachment security. In addition, while limited by variables included in the compiled research, we were able to examine potential moderation of effect sizes by type of IPV assessed, at-risk characteristics of sample, IPV witnessed by child, child age and time lag between assessments, measurement forms of IPV and attachment, and publication information.
Method
A systematic literature search following PRISMA guidelines was completed in February 2019. The search aimed to identify studies examining mothers’ experience of IPV victimization in the ante- or perinatal periods and subsequent mother–offspring attachment security in early childhood (i.e., 5 years and under). Parallel literature searches were conducted in four EBSCOhost databases (PsycINFO, MEDLINE Complete, CINAHL Complete, and Social Work Abstracts), Informit, and Embase. We selected these databases for their quality and depth of coverage of social science literature (Taylor, Wylie, Dempster, & Donnelly, 2007). Search terms selected through team collaboration encompassed three major concepts: (1) intimate partner violence, (2) child attachment outcomes, and (3) young children. A search for gray literature was conducted in Google (i.e., the first 10 pages of results were reviewed) and ProQuest for unpublished dissertations and theses. We included empirical research studies that assessed intimate partner violence in the ante- or perinatal periods and later child (1–5 years) attachment outcomes. We had aimed to confine the study to longitudinal studies only. Given the dearth of such studies, criteria were expanded to also include cross-sectional studies that used retrospective reports by mother of IPV in the last 6 or 12 months. Studies that examined nonviolent forms of interparental conflict and relationship dissatisfaction were excluded.
The initial search from the EBSCOhost databases, Informit, and Embase yielded 1,234 studies with 10 further gray literature papers identified. This resulted in a total of 802 articles after the removal of duplicate records. See Figure 1 for a PRISMA diagram outlining the identification, screening, eligibility, and inclusion process of the reviewed literature.

PRISMA diagram. Source. Moher, Liberati, Tetzlaff, Altman, and The PRISMA Group (2009); for more information, visit www.prisma-statement.org
One researcher completed title and abstract screening of all articles, and 25% were checked by a second researcher (96.1% agreement, κ = .65). As a result, 772 records did not meet the inclusion criteria. Of the remaining 30 articles, two thirds of the full texts were assessed independently by two researchers with 95.0% agreement (κ = .90). Disagreements were resolved by conferencing.
Next, studies were excluded if they (a) assessed attachment over 5 years old, (b) did not assess attachment or assessed attachment using unvalidated measures (e.g., measures which were study-derived and/or not externally validated), (c) did not assess intimate partner violence, (d) did not have an empirical research design, (e) did not have a quantitative component, (f) were not available in English, (g) utilized the same sample and measures as another full-text study, and (h) did not have data available despite authors being contacted. This resulted in six remaining studies.
Data were extracted from the included papers by two researchers (see Tables 1 and 2). Studies identified through this systematic review were predominantly from the United States of America (83.3%) with one study from France. All studies were peer-reviewed journal articles. Study characteristics and potential risks of bias are discussed in the reporting of results.
Study Characteristics.
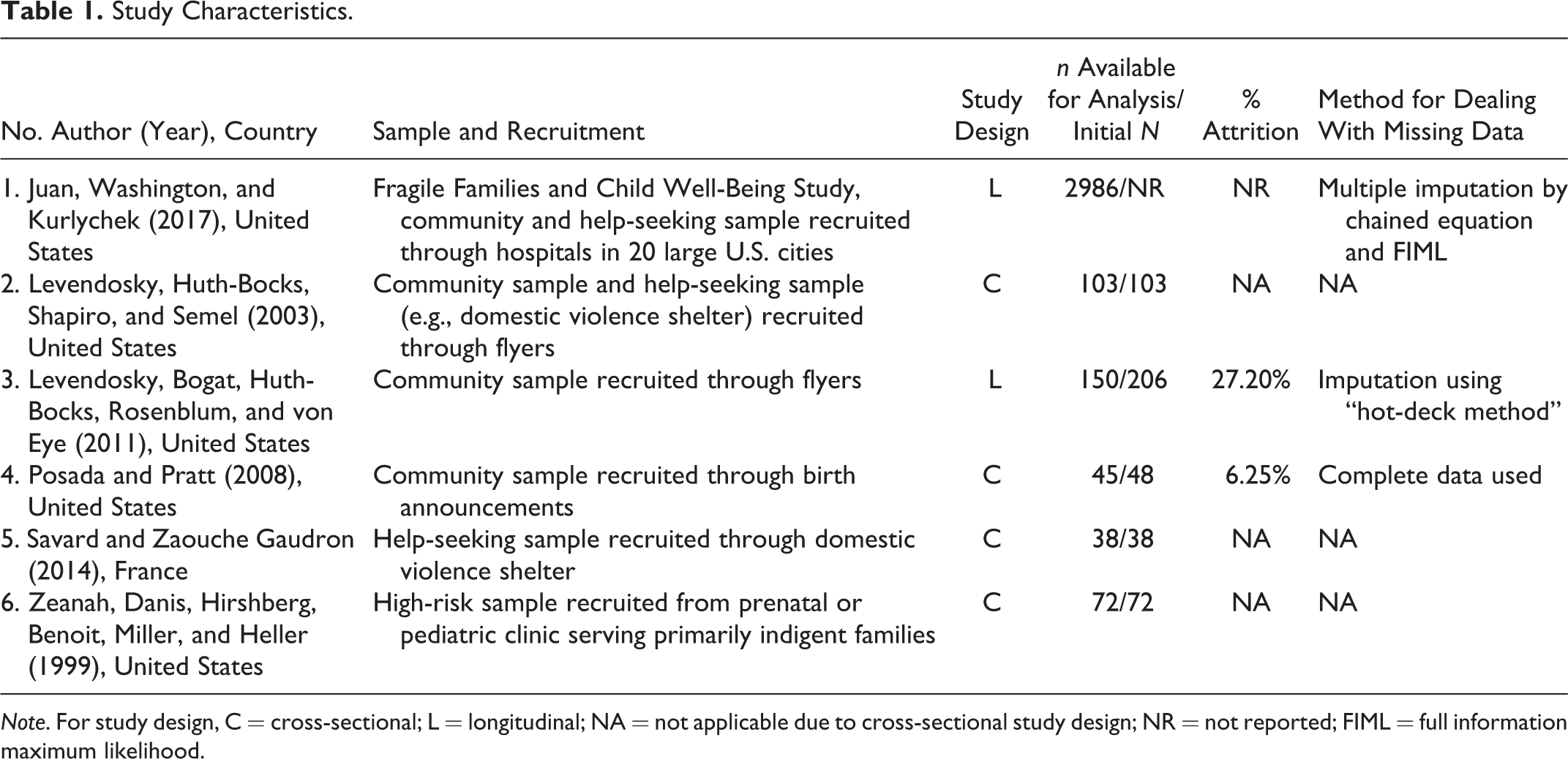
Note. For study design, C = cross-sectional; L = longitudinal; NA = not applicable due to cross-sectional study design; NR = not reported; FIML = full information maximum likelihood.
Study Measures.
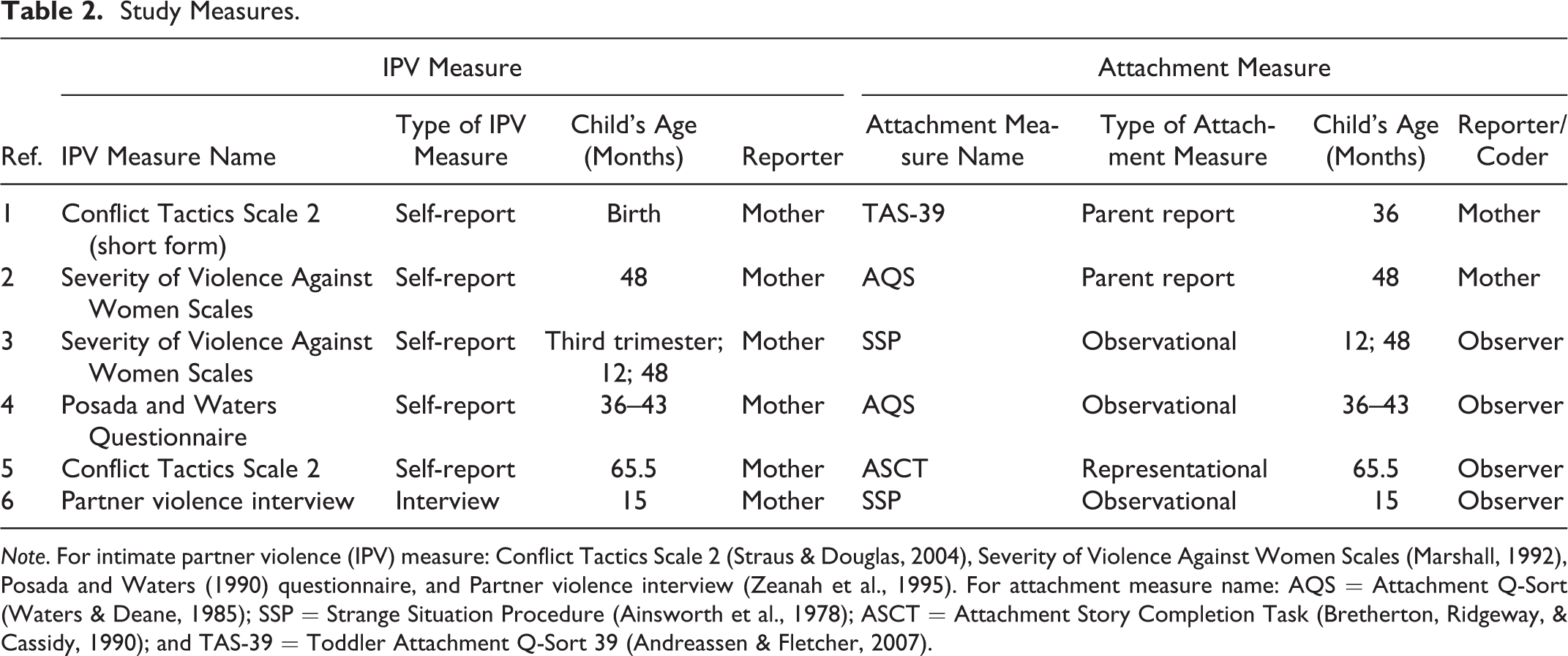
Note. For intimate partner violence (IPV) measure: Conflict Tactics Scale 2 (Straus & Douglas, 2004), Severity of Violence Against Women Scales (Marshall, 1992), Posada and Waters (1990) questionnaire, and Partner violence interview (Zeanah et al., 1995). For attachment measure name: AQS = Attachment Q-Sort (Waters & Deane, 1985); SSP = Strange Situation Procedure (Ainsworth et al., 1978); ASCT = Attachment Story Completion Task (Bretherton, Ridgeway, & Cassidy, 1990); and TAS-39 = Toddler Attachment Q-Sort 39 (Andreassen & Fletcher, 2007).
Meta-Analytic Procedures
The metafor package in R (Viechtbauer, 2010) was utilized for meta-analysis. Studies varied in the effect size metric reported, and all effects were converted to correlation coefficients (Pearson’s r) to facilitate cross-study comparison using an interpretable metric with good statistical properties (Rosenthal & DiMatteo, 2001). Effect sizes and relevant demographics were extracted from each paper and tabulated in R. In longitudinal studies with various time points, effect sizes for each time point were treated separately. A multilevel modeling approach was utilized to obtain estimates of average effect sizes across all studies while controlling for the nonindependence of multiple estimates within the same study (Hox, 2010). Effect sizes were weighted by sample size. Within this multilevel modeling framework, random effects modeling was undertaken to assess the extent to which effect sizes were heterogeneous across papers. Cochran’s Q statistic reflects the total amount of variance in the meta-analysis and is sensitive to the number of associations considered with a statistically significant Q statistic indicating substantial heterogeneity. Duval and Tweedie’s (2000) trim-and-fill method was used to estimate potential publication bias.
Intra-class correlations (ICCs) greater than 0.25 were followed up with meta-regression analyses that examined various moderated effects independently. These separate analyses examined the following predictors: type of IPV assessed, at-risk characteristics of sample, IPV witnessed by child, child age and time lag between assessments, measurement forms: IPV and attachment, and publication information. While our hope was to analyze attachment classification by organization and disorganization, no studies reported these data, and data could only be extracted for the secure/insecure distinction. See Table 3 for information on how variables were coded.
Results of Moderator Analyses in Association Between IPV and Offspring Attachment Security.
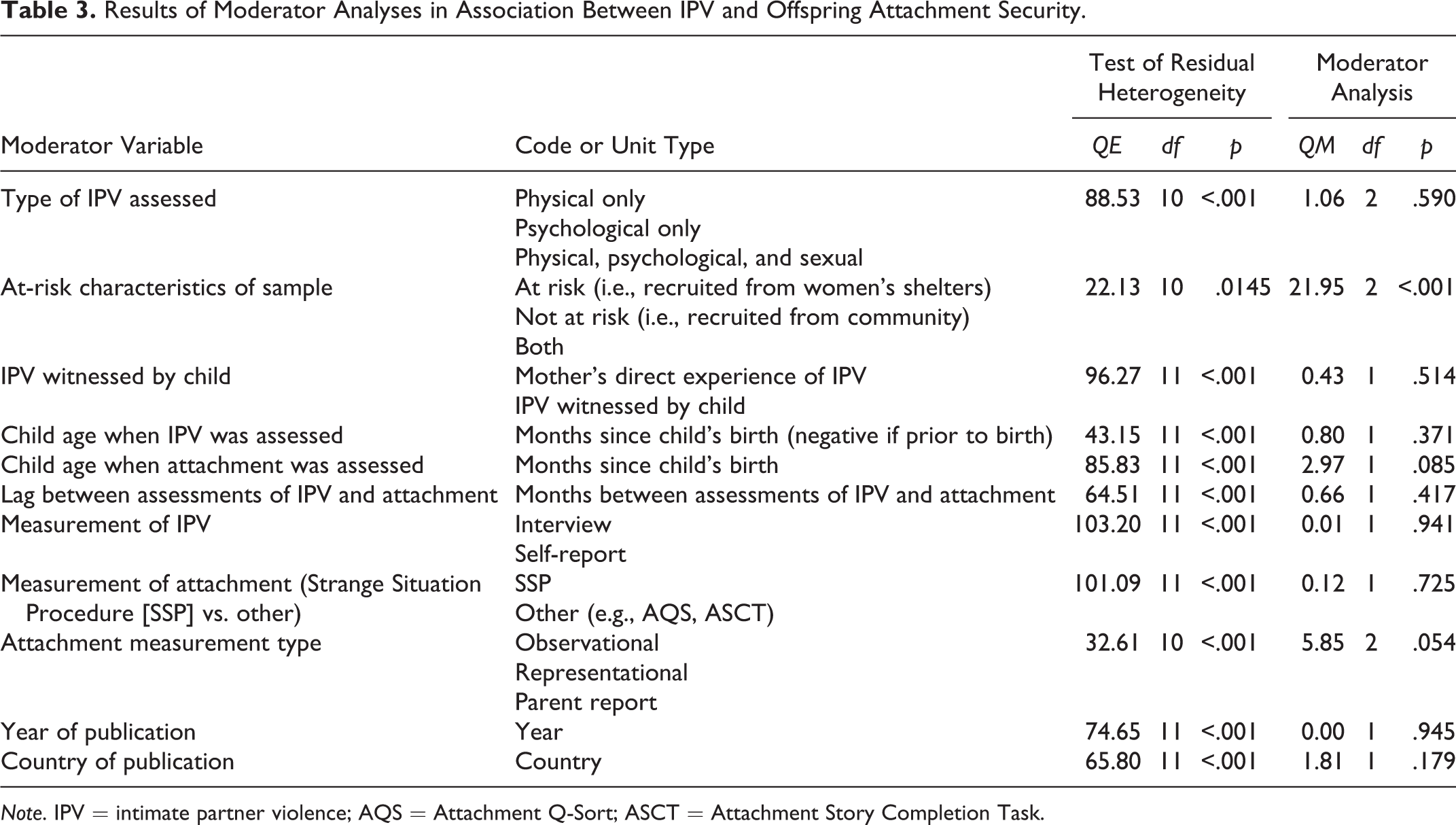
Note. IPV = intimate partner violence; AQS = Attachment Q-Sort; ASCT = Attachment Story Completion Task.
Results
Multilevel random effects meta-analysis was conducted on six studies reporting the association between intimate partner violence and offspring attachment security at 5 years and under. A total of 12 effects were included in the model, clustered by study. Intimate partner violence was inversely associated with offspring attachment security, r = −.23, CI [−0.42, −0.04], SE = .10, p = .02, ICC = .87. See Figure 2 for a graphical display of the results as a forest plot. See Figure 3 for the Duval and Tweedie procedure regarding publication bias. The test for heterogeneity was statistically significant, k = 13, Q(12) = 106.14, p < .01.
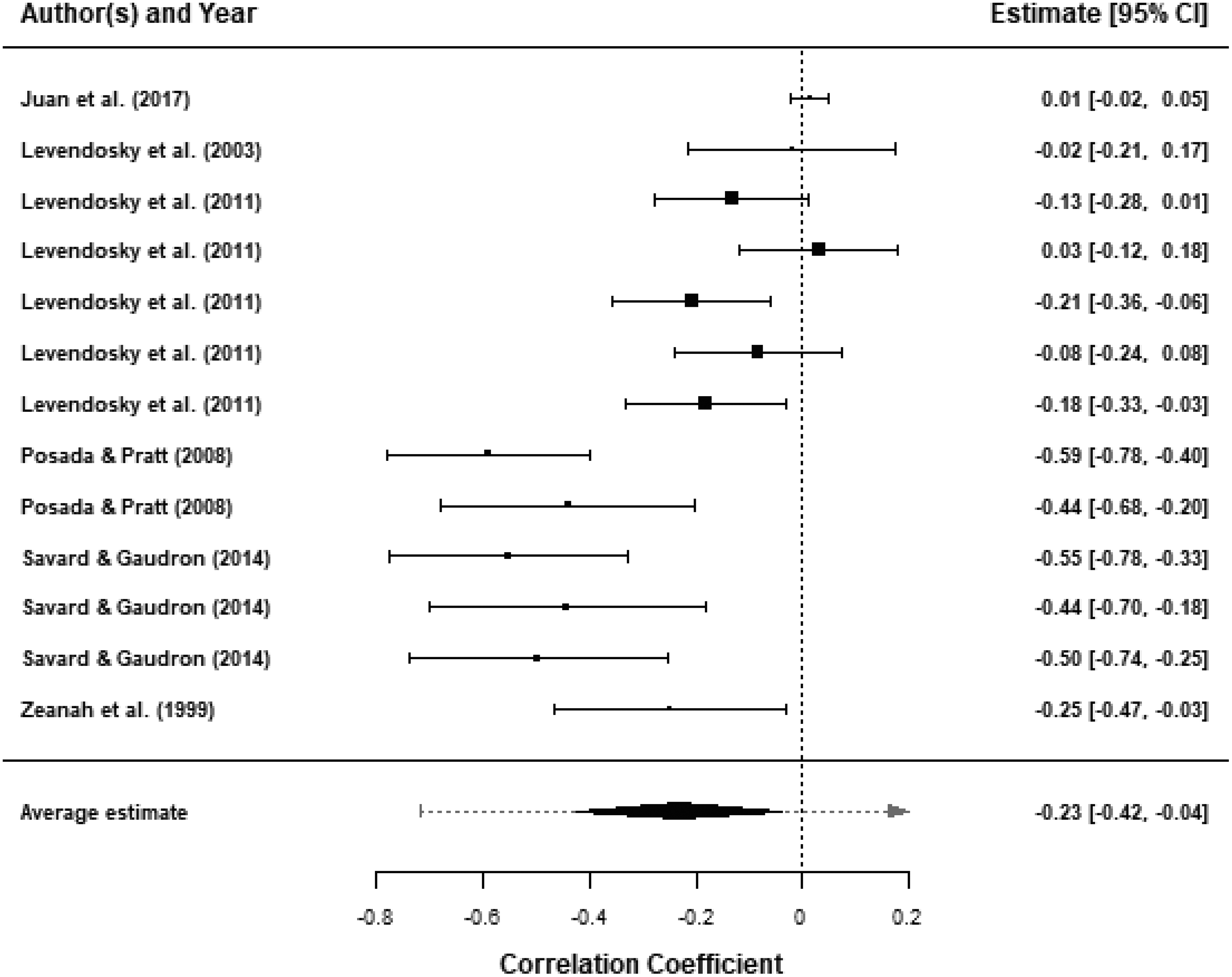
Forest plot.
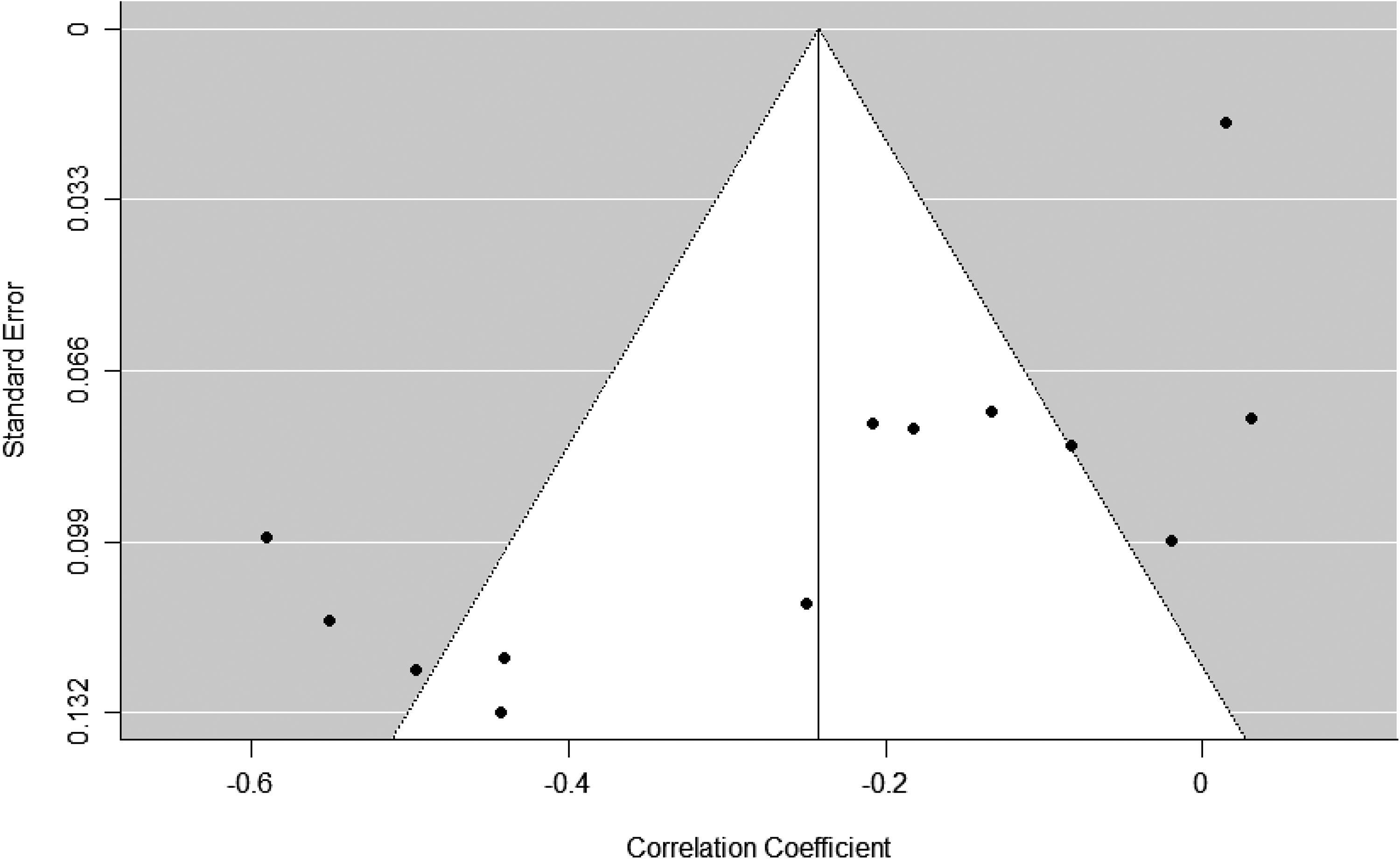
Funnel plot.
Potential moderators were examined in the association between intimate partner violence and offspring attachment security. Due to limited power, separate meta-regression analyses were conducted independently (see Table 3). Risk status of the sample (e.g., clinical vs. community samples) was a significant moderator in the relationship between mother’s IPV exposure and offspring attachment security. Studies which recruited both at-risk and not-at-risk participants (n = 3, k = 7, r = −.04, p = .391) reported weaker associations with offspring attachment security than studies which recruited only clinical samples (n = 2, k = 4, r = −.39, p = .002) or only community samples (n = 1, k = 2, r = −.53, p < .001). Type of attachment measurement also moderated the association at a trend level. Studies which utilized parent-report measures of attachment (n = 2, k = 2, r = .01, p = .474) tended to report weaker associations with offspring attachment security than studies which utilized observational (n = 3, k = 8, r = −.29, p = .02) or representational measures (n = 1, k = 3, r = −.50, p < .001). Child age at attachment assessment neared significance as a moderator. As child age at attachment assessment increases, the link between mother’s IPV experience and child attachment security tends to be weaker.
Discussion
This meta-analytic study is the first to examine and confirm an inverse link between mother’s experience of intimate partner violence in the perinatal window and subsequent attachment security in children aged 1–5 years (r = −.23). The relationship was moderated by sample risk or clinical status and at a trend level by both type of attachment measurement and the child’s age at the time of attachment assessment. This effect size exceeds effects found for attachment insecurity and marital quality, maternal depression, and maternal life stressors (Atkinson et al., 2000); is comparable to the effects found for non-IPV interparental conflict (Tan et al., 2018); and is close to those consistently found for caregiver insensitivity (Verhage et al., 2016).
Importantly, these findings are consistent with prior findings of a strong relationship between maternal caregiving behavior and offspring attachment (Bakermans-Kranenburg, van IJzendoorn, & Juffer, 2003; George & Solomon, 2008) and with propositions as described in the Introduction that caregiving is, itself, directly affected by assault on a mother (Levendosky et al., 2012). Our evidence supports broader evidence that maternal adverse experiences, including abusive trauma and unresolved loss during pregnancy and the postpartum period, impact on the emotional aspects of caregiving. The suggestion from the clinical literature is that traumatic preoccupation and depression resulting from IPV interfere with the accuracy of the mother’s interpretation of her infant’s cues (Baradon & Steele, 2008; Solomon & George, 2011) and damage the development of her caregiving representations (Huth-Bocks, Levendosky, Theran, & Bogat, 2004). In a climate of domestic violence, the preoccupied and frightened mother may misread the infant’s distress and behave in a subtle or overt manner that is confusing, and otherwise disorganizing for the infant, including helpless, or anomalous gestures, withdrawal, sudden shifts in mood, intrusiveness, or mistimed contingencies (Beebe et al., 2010; Biringen & Easterbrooks, 2012; Judd, Newman, & Komiti, 2018; Lyons-Ruth & Spielman, 2004).
We found the relationship between IPV and insecure attachment is attenuated over the course of early development. This may reflect the slowly increasing importance of other relational figures in the child’s life as they grow, such that the assaults to the maternal caregiving system itself are somewhat less significant, or their impacts are diluted through surrounding supportive relationships with early childhood teachers and other carers. The finding may also be related to changes in the nature of IPV or decreasing violence over time. Measurements of attachment also vary with age, moving from observational to representational forms of assessment. This may introduce an additional confounding factor which we were unable to account for in our analyses. While we could not examine these possibilities in the current meta-analysis, future researchers may.
The nature of studies included in our meta-analysis precluded close examination of other variables that theoretically influence the link between mother’s experience of IPV and child attachment and prevent us from offering a view on the extent to which attachment status following a child’s exposure to IPV is fully moderated or otherwise by parental responsiveness. A lack of significant findings for other potentially relevant moderator variables in the current meta-analysis likely reflects the limited number of studies available. For example, where we found “IPV witnessed by the child” was not a significant moderator, other research (e.g., Gewirtz & Edleson, 2007; Renner & Slack, 2006) suggests that children who witness parental IPV are at greater risk for several forms of maltreatment by attachment figures, including physical and sexual abuse, and these potentially traumatic experiences could also be linked to attachment insecurity and negative developmental outcomes. This level of disaggregation is an important focus for future research.
The reviewed research did allow us to test some moderators, and the results highlight methodological and theoretical considerations for future studies. First, we found studies that included participants recruited from both clinical and community samples reported weaker associations than studies which had only clinical or community samples. Sampling disaggregation clearly remains important to future studies. We also found at a trend level that the type of attachment measure used impacted the link between mother’s IPV and child attachment security such that studies utilizing parent-report measures of attachment reported weaker associations with offspring attachment security than studies with observational or representational measures. This has been found elsewhere (Tan et al., 2018; Van IJzendoorn et al., 2004), suggesting that parent-rated and observational measures of attachment may be measuring different constructs. Our finding regarding type of attachment measurement may be related to another trend-level finding that the older the child, the weaker the link between mother’s IPV and child attachment security. Attachment for younger children is more frequently assessed through gold standard observational means (i.e., the SSP), and this may have yielded more accurate results. Greater impact on attachment for younger children remains consistent with other findings of a sleeper effect across childhood of violence exposure, wherein compromised attachment security becomes a critical domino in a downward cascade of internalizing and externalizing symptomatology for children by school entry (Holmes, 2013).
Our study also underscores the importance of close attention in the future to specificity within attachment measurement. Inclusion of four-way attachment classification (i.e., secure, avoidant, ambivalent-resistant, disorganized) above the two-way secure/insecure attachment classification would allow more nuanced examination of findings, including the transmission of disorganized attachment outcomes from maternal trauma. Attachment disorganization is thought to reflect a young child’s experience of fear without solution (Main & Solomon, 1990), linked to frightening or frightened behaviors in the caregiver. Given the IPV context in which mother is often frightened of the partner, with potential spillover into helpless or frightening interactions with her infant, there are likely to be stronger links with mother’s IPV experiences and offspring attachment disorganization than with attachment insecurity in general.
Equally important, limitations within current methodologies include the understudied nature of father–child attachment in the context of IPV. While it remains easier for social scientists to recruit mothers for these forms of research (Newington & Metcalfe, 2014), doing so increases the risk that we will focus on mothers’ parenting as the problem and the solution, ignoring the role of fathers in both risk and protective offsets for children’s outcomes. In this, it is important to note that female IPV victimization does not predetermine parenting problems for the mother (Levendosky, Bogat, Bernard, & Garcia, 2017). Of import, we were also unable to examine recency of IPV exposures or ongoing trauma in the home. Related to this, we were unable to explore variation of mental and behavioral impacts of IPV experiences for mothers or the extent to which any trauma experienced was resolved and integrated. Assuming variability of recovery, including mothers who restored mental health and behavioral competencies, it is noteworthy that direct effects of IPV on the attachment bond remained. Finally, we note that we have considered socioeconomic, racial, ethnic, and gender diversity in the literature review but that this level of diversity was not well represented in the studies included for meta-analytic examination. Sexual orientation, religion, ability, and culture are particularly under-represented to date in studies examining the connections between attachment and IPV experiences.
For now, what is clear is that a mother’s experience of IPV victimization during pregnancy and in the months following birth increases risk of offspring forming an insecure attachment with her. The finding underscores the need for earliest recognition by frontline health services of IPV experiences and their potential to compromise security in the mother–infant dyad. Some initiatives for workforce training in this arena are underway (McIntosh & Newman, 2018). Earliest identification of IPV with mothers would enable preventive interventions to promote safety in relationships and to support mothers’ parenting responsiveness in the face of stress and distress, in turn potentially helping to safeguard the developmental trajectory for offspring. Given the recurrent nature of IPV for many women, such assessments would optimally be repeated by pediatricians and public health nurses at routine child wellness appointments. Early recognition of infant attachment difficulties may also alert clinicians to assess for IPV, providing opportunities for early intervention.
The child welfare implications of IPV for legislation are significant. We note debate is underway on legislative change to acknowledge child exposure to domestic violence as a form of child maltreatment warranting state intervention (Henry, 2018). We caution against the mistranslation or misuse of our findings, especially in the context of the individual case. Specifically, our findings do not imply that infants should be removed from a mother experiencing IPV on the grounds of likely attachment disorganization. Such misuses of attachment research, particularly in family court and child protection arenas, have been documented elsewhere (Duschinsky, 2018; Pruett, McIntosh, & Kelly, 2014). On the contrary, our findings support the social imperative to give increasing attention and resources to the support of mothers who have experienced IPV, in safeguarding attachment security in their children, and de-escalating the negative impact of IPV on developmental pathways. This may include new psychoeducational approaches to enhancing parent awareness of the associations that IPV exposure may have with the development of their child’s attachments (McIntosh, 2015; McIntosh & Tan, 2017) as well as implementing attachment-based parenting interventions in cases where IPV has been identified (Lieberman, Chu, Van Horn, & Harris, 2011). Given the strong intergenerational transmission of IPV risk, doing so may improve the social–emotional health of generations to come.
Critical Findings
Intimate partner violence was inversely associated with offspring attachment security, r = −.23, CI [−0.42, −0.04], SE = .10, p = .02, ICC = .87.
Risk status of the sample (e.g., clinical vs. community samples) was a significant moderator in this relationship. Studies which recruited both at-risk and not-at-risk participants (n = 3, k = 7, r = −.04, p = .391) reported weaker associations with offspring attachment security than studies which recruited only clinical samples (n = 2, k = 4, r = −.39, p = .002) or only community samples (n = 1, k = 2, r = −.53, p < .001).
Type of attachment measurement moderated the association at a trend level. Studies which utilized parent-report measures of attachment (n = 2, k = 2, r = .01, p = .474) tended to report weaker associations with offspring attachment security than studies which utilized observational (n = 3, k = 8, r = −.29, p = .02) or representational measures (n = 1, k = 3, r = −.50, p < .001).
Child age at attachment assessment neared significance as a moderator. As child age at attachment assessment increases, the link between mother’s IPV experience and child attachment security tends to be weaker.
Implications for Practice, Policy, and Research
Our findings suggest the significant potential of IPV to impact the maternal state of mind, sufficient to disrupt the security of the infant–mother attachment relationship. Earliest identification of IPV with mothers may allow preventive interventions to promote safety and to support mother’s parenting capacity and responsiveness in the face of IPV, in turn potentially helping to safeguard the developmental trajectory of the child.
Recognizing signs of children’s attachment difficulties and maternal struggles with responsiveness may alert clinicians to assess for IPV, providing opportunities for early intervention.
Our findings note the need for replication of studies and underscore the importance of close attention in the future to type of attachment measure.
Limitations within current methodologies were identified, including the understudied nature of father–child attachment in the context of IPV.
Our findings underscore the need for earliest recognition by frontline health services of IPV experiences and their potential to compromise security in the mother–infant dyad.
Footnotes
Acknowledgment
We thank Bi-Xia Ke and Claire Lubotzky, Deakin University, for their research assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a University–Industry partnership project between Relationships Australia South Australia and Deakin University Centre for Social and Early Emotional Development (SEED).