
Abstract
Adolescents and young people in sub-Saharan Africa (SSA) experience high rates of gender-based violence (GBV). The whole school approach (WSA) is an established benchmark of effective school-based interventions to address this issue. We conducted a systematic review of peer-reviewed literature using PubMed/Medline, EMBASE, Scopus, Web of Science, Cochrane Library, Clinicaltrials.gov, and Google Scholar (1) to determine the characteristics, measured outcomes, and effectiveness of school-based GBV interventions and (2) to examine each papers’ alignment with WSA and methodological quality. We developed a comprehensive intervention characteristics form for data extraction and analyzed the selected studies’ quality using the modified Methodological Quality Rating Scale. To measure alignment with WSA implementation standards, we expanded the application of the WSA by creating the Whole School Approach Rating Scale (WSARS) for assessing school-based GBV interventions. Most interventions (n = 14/16) we reviewed effectively addressed at least one of the three outcomes of interest (i.e., sexual violence, physical violence, and GBV-related knowledge/attitudes). Over half (n = 9/16) of the studies were rated high on the WSARS. However, we observed no significant differences in effectiveness between studies rated high and those rated low on the WSARS. Our results indicate that school-based GBV interventions could be an effective and sustainable strategy for addressing GBV in and around schools.
Keywords
In sub-Saharan Africa (SSA), 2018 regional estimates indicate that at least 33% of women (ages 15–49) had experienced gender-based violence (GBV), 20% of whom had experienced it in the past 12 months (World Health Organization [WHO], 2021). Troublingly, GBV rates are even higher among adolescent girls and young women (AGYW). Country-specific statistics show that the overall prevalence of GBV among AGYW (ages 10–24) in SSA was in Nigeria and Ethiopia, at 42.3% and 67.7%, respectively (Beyene et al., 2019). The same study found that, among the AGYW of different SSA countries, the lifetime prevalence of sexual violence ranged from 4.3% to 76.4%, physical violence ranged from 7.4% to 66.1%, and emotional violence ranged from 26.1% to 50.8%. Furthermore, an analysis of Demographic and Health Surveys from 27 SSA countries found that 33% of men (ages 15–64) reported that at least one form of physical intimate partner violence (IPV) was justified (Darteh et al., 2021). GBV, including IPV, constitutes a significant public health issue with well-documented deleterious effects on mental and physical health, including HIV vulnerability among adolescents and young women (Knaul et al., 2020; Mengo et al., 2019; Okumu et al., 2022).
In SSA, the lifetime prevalence of sexual, physical, and emotional violence—experienced in all facets of adolescents’ and young people’s lives from school to the home to the community—is high, particularly among adolescent girls who attend educational institutions (e.g., Beyene et al., 2019). To reduce the prevalence of GBV and the harmful gender norms in and around schools, the United Nations Girls’ Education Initiative (UNGEI) has recommended the use of a whole school approach (WSA) as a school-based intervention framework in the design and implementation of GBV prevention and mitigation interventions (UNGEI, 2018). The WSA was developed to promote greater gender awareness of the gender-based aspects in and around schools as part of achieving the UN’s Sustainable Development Goal 4 target of “safe, inclusive, and gender-sensitive learning environments” in schools and communities globally (UNGEI, 2018). It advocates for integrating social and emotional learning and GBV prevention into daily interactions between teachers and students and everyday practices in multiple school settings, including school staff, teachers, families, and school-going children (Oberle et al., 2016).
For this reason, the WSA draws from the socio-ecological model to define the entire school community as the unit of change and to promote the engagement of multiple stakeholders in schools to change harmful gender norms and reduce GBV (e.g., Cowie & Jennifer, 2007; Maxwell & Aggleton, 2014; McMahon et al., 2019; Parkes, 2016; Richard et al., 2012; Steiner & Spear, 2020; UNGEI, 2018). The key stakeholders identified by the WSA framework include teachers, families, and the broader community, who can serve as target participants, change agents, and allies (Oberle et al., 2016; UNGEI, 2018). The WSA also ensures that school-based GBV interventions target both boys and girls to comprehensively address core GBV risk factors to address core GBV risk factors and core GBV risk factors (e.g., harmful gender norms) (Elboj-Saso et al., 2020). Further, it adopts a broad understanding of school-related GBV that recognizes that men and boys and women and girls experience violence used to assert and reproduce gender roles and norms. In other words, WSA draws from empirical evidence to acknowledge the strong connection between different forms and victims of GBV.
In SSA, researchers, schools, governments, and communities are all increasingly recognizing that schools are a strategic and critical entry point for GBV prevention, reduction, and mitigation. Schools are considered essential settings for individuals’ socialization and positive development (Okumu et al., 2017, 2020), while teachers are seen as caregivers and agents of classroom development and change (Bhana et al., 2006; Pillay, 2017). Notably, in alignment with World Health Organization’s (WHO) recommendation to help learners by combating violence in and around schools may help SSA (WHO, 2019), a substantial amount of school-based GBV interventions have been tested in SSA (e.g., Baiocchi et al., 2017; Decker et al., 2018; Kilburn et al., 2018; Özler et al. 2020, among several others). Additionally, most of these interventions were designed to recognize the importance of critical stakeholders such as parents and communities (e.g., Devries et al., 2015; Jewkes et al., 2008; Jewkes et al., 2019; Mathews et al., 2016, among others).
Currently, the only synthesized evidence of school-based GBV interventions is from a review of 61 interventions conducted globally to prevent IPV and sexual violence among adolescents (ages 10–19) (Lundgren & Amin, 2015). To the best of our knowledge, no single systematic review exists that synthesizes knowledge on the relevance and effectiveness of these GBV interventions in SSA. Additionally, despite such calls for robust school-based violence prevention interventions that leverage the WSA in SSA, no synthesized evidence of the effectiveness of such programs exists. The only existing evidence of the effectiveness of WSA in school settings is from interventions conducted in high-income settings, and the focus was on social and emotional development and learning interventions among adolescents (Barry et al., 2017; Goldberg et al., 2018; Jones & Bouffard, 2012; Oberle et al., 2016; Weare & Nind, 2011). There is a need for synthesized knowledge on the extent to which school-based GBV interventions in SSA use the WSA and whether its use enhances intervention effectiveness.
Therefore, the current systematic review addresses the above-stated gaps in several ways: (1) examining the effectiveness of school-based GBV interventions in reducing GBV outcomes (i.e., sexual and physical violence and GBV-related knowledge/attitudes) in SSA; (2) evaluating the extent to which the implementation of these school-based GBV interventions align with the WSA; (3) establishing whether the extent of school-based GBV intervention alignment to the WSA has any significant impact in terms of effectiveness; and (4) assessing the extent to which school-based GBV interventions target and report outcomes for both boys and girls. The significance of this systematic review is that it addresses the persistent knowledge gap regarding the effectiveness of school-based GBV interventions in SSA.
Methods
Search Strategy and Information Sources
Using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Page et al., 2021), a reference librarian (K. L.) and one reviewer (T. N.) used a combination of standardized subject terms and keywords to systematically search six major databases including PubMed/Medline, EMBASE, Scopus, Web of Science Cochrane Library, Clinicaltrials.gov, and Google Scholar. We searched for articles published in English that assessed school-based GBV interventions in SSA aimed at preventing, mitigating, and/or reducing GBV and which targeted adolescents and young adults (ages 10–24 years). The published literature was searched using search strategies for the concepts of schools, universities, curriculum, high school, school curriculum, gender-based violence, violence, physical abuse, domestic violence, rape, intimate partner violence, sex offenses, Africa south of the Sahara, South Africans, Kenya, early intervention, educational, intervention(s), program development, programs, child, children, adolescent(s), and young adult. All searches were completed by October 19, 2021. The search strategy was marginally modified to ensure compatibility with each search engine. We also hand-searched the bibliographies of selected articles to identify relevant articles not identified through the search strategy. All the reviewers independently screened the titles, abstracts, and full text of the articles derived from the search to assess article eligibility for the review based on predefined inclusion and exclusion criteria. Discrepancies in study inclusion were resolved through discussion and consensus of three reviewers.
Eligibility Criteria
Identified texts were eligible for review if they were (1) conducted in SSA, (2) quantitatively evaluated GBV interventions in schools, (3) included adolescents and young adults between the ages of 10 and 24 years, (4) reported GBV and/or GBV-related attitudes, norms, and behaviors, and (5) were peer-reviewed journal articles. Journal articles were excluded if they were (1) not published in English, (2) were qualitative studies, meta-analyses, systematic reviews, or feasibility studies, (3) were not intervention studies (i.e., consisted of a letter, an editorial, a conference abstract, a presentation, or a study protocol), or (4) only included teachers.
Data Extraction and Synthesis
Each included study was reviewed to extract descriptive information on intervention characteristics (i.e., country, region, purpose, intervention name), characteristics of the target population included in the intervention (e.g., sample size, sex distribution, description), design features (e.g., randomization, study arms/conditions, and theoretical framework), violence prevention or mitigation strategies in the treatment condition (e.g., intervention components, intervention duration, follow-up time, and targets), outcomes measured, methodology for measurement, and overall reported findings or outcome of the evaluation. For articles providing such information, the details were extracted and recorded into a standard Excel data extraction worksheet (see Table 1). Three reviewers (T. N., J. S, and E. K. O.) independently extracted data and then met to adjudicate or clarify the content that was not interpreted. To synthesize data, all the reviewers conducted an iterative review of included intervention studies to identify commonalities in the main results and conclusions, intervention components, and outcomes that characterize the current state of the science for school-based GBV interventions for adolescents and young adults in SSA. Data extracted from each article were summarized and iteratively reviewed to identify common themes and limitations in the current evidence base by all the reviewers.
Intervention Study Characteristics.
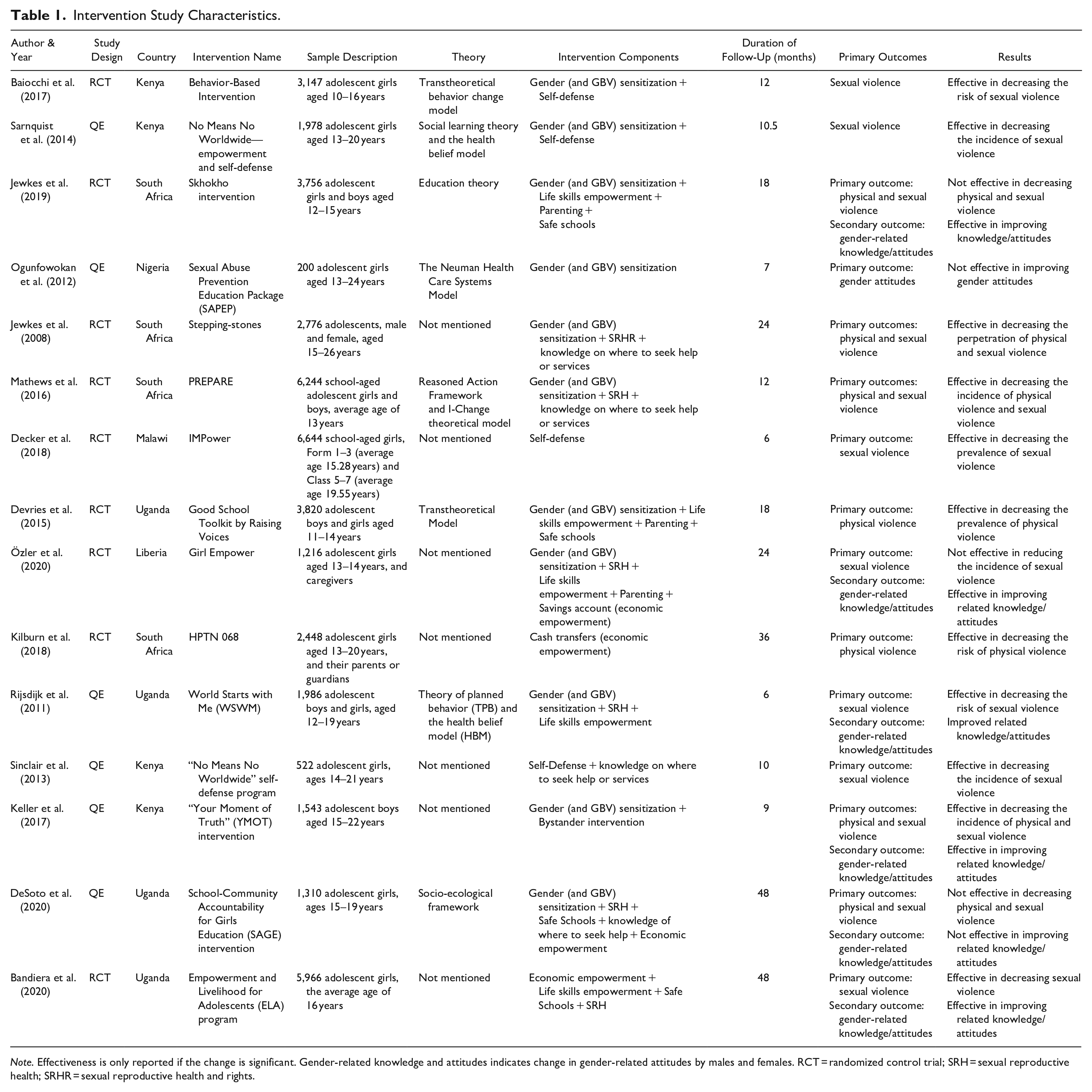
Note. Effectiveness is only reported if the change is significant. Gender-related knowledge and attitudes indicates change in gender-related attitudes by males and females. RCT = randomized control trial; SRH = sexual reproductive health; SRHR = sexual reproductive health and rights.
Methodological Quality Assessment
Three reviewers (T. N., J. S., and E. K. O.) assessed the extent of methodological rigor of the studies using a modified version of Miller et al.’s (1995) Methodological Quality Rating Scale (MQRS) in consultations with M. O. (Appendix 1). The original MQRS had 14 items: study design, quality control, follow-up rate, length of the follow-up period, reliability/validity of measures, contact, collaterals, objective verification, dropouts, attrition, blind follow-up, statistical analysis, multi-site, and generalizability (Miller et al., 1995). We made several modifications to the scale. First, we added three new items: theoretical basis, intervention intensity, and the use of multiple outcome measures. Second, we removed two items, contact, and collaterals, from the scale for lack of relevance. Third, we combined dropout and attrition, into one item because they provide similar information. Finally, we modified the study design scale to accommodate all available intervention study designs and has a score range of 0–3 instead of the original 0–2. Similar modifications were made in a prior systematic review and meta-analysis of HIV treatment adherence interventions (Nyoni et al., 2020). To fairly assess different studies with a wide range of intervention sites, we modified the multiple sites item so that a study gets a score of 0 if conducted in a single location or site, a score of 1 if conducted in locations ranging from 2–10, and a score of 2 was given for more than 10 locations. The modified MQRS scores were tallied to obtain an overall score for each study and each item. The highest attainable score for each study on the modified MQRS scale was 23.
Assessment of Study Compliance with WSA
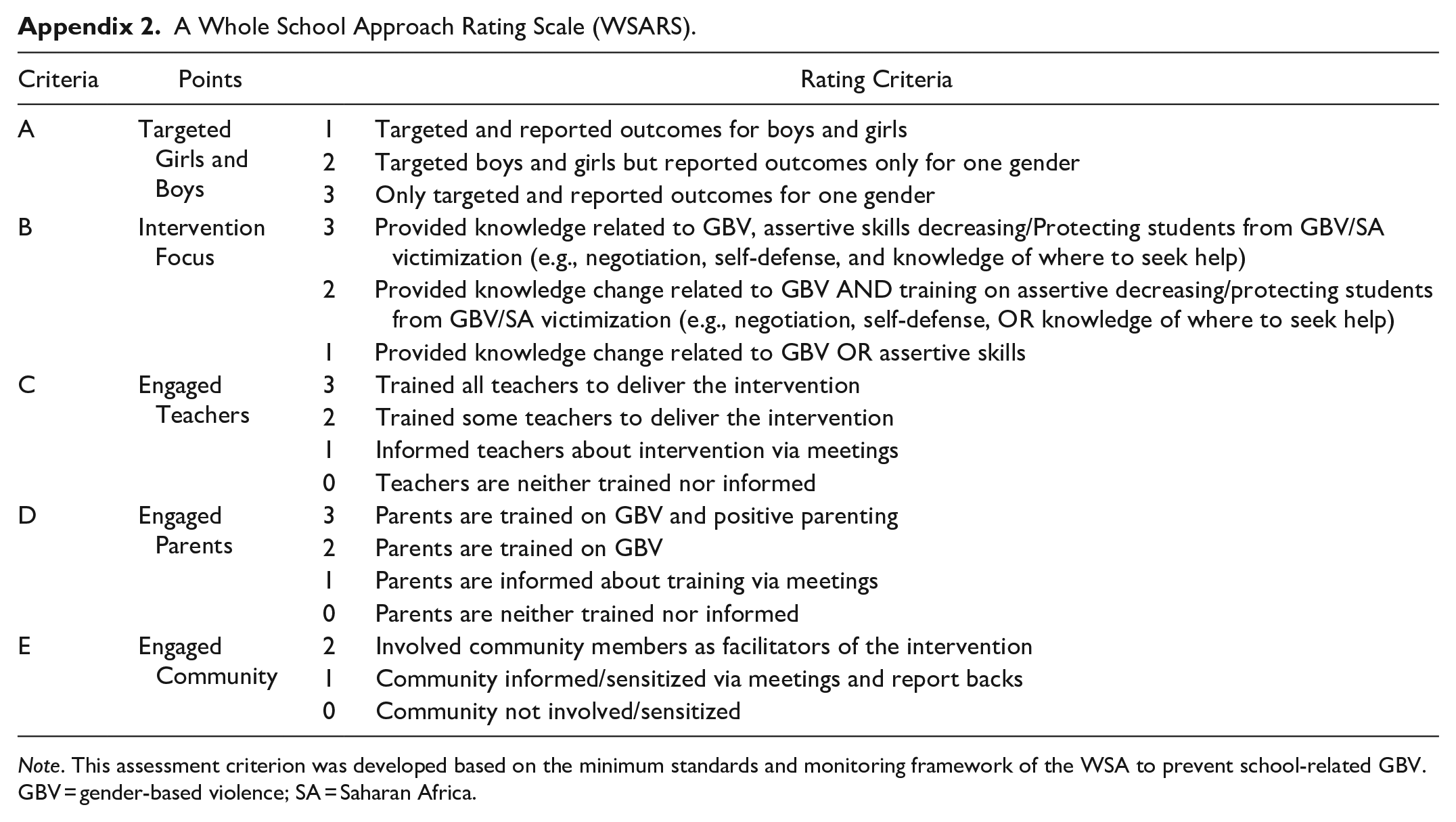
We developed a five-item Whole School Approach Rating Scale (WSARS to (1) assess the extent to which the selected school-based GBV intervention studies in SSA were using WSA and (2) establish whether the use of the WSA predicted greater intervention effectiveness. To develop the WSARS, we relied on prior empirical conceptualizations (e.g., Futures without Violence, n.d; Goldberg et al., 2018; UNGEI, 2018) (see Appendix 2). The WSARS had five items assessing (1) whether a given GBV intervention targeted and reported outcomes for boys or girls or both; (2) the intervention focus (i.e., the number of intervention components); and the extent to which the study engaged (3) teachers, (4) parents, and (5) the community. These five items were included in the WSARS because they were deemed feasible to be implemented within the timeframe of an intervention study. We used the WSARS to rate how each study scored on each of the five items to create the overall WSA score for each study. These scores indicated the extent to which each intervention study met the WSA implementation standards derived from various sources (e.g., Futures without Violence, n.d; Goldberg et al., 2018; UNGEI, 2018). The WSARS scores were tallied to obtain an overall score for each study. The overall scores for each study on the WSARS ranged from 0 (lowest score) to 14 (the highest score).
Results
Study Characteristics
As shown in the PRISMA diagram in Figure 1, 7,812 articles were identified through our initial database search. Forty-one articles were selected for a full-text review after screening for relevance based on titles and abstracts. The 6,037 titles and abstracts that were removed included observation studies, were not interventions of interest, were not conducted in SSA, were targeting school stakeholders (e.g., teachers, parents, community members) rather than students, or were duplicates. Of the 41 studies that were subjected to full-text review, 25 articles were excluded for several reasons, such as not having outcomes of interest, a population of interest, a study design of interest, or study protocols. A total of 16 studies met the inclusion criteria and were included in this systematic review. Detailed information on study characteristics appears in Table 1. Although we did not select any date range in our database search, our search output and study selection resulted in studies published from 2008 onward. These studies also reported on interventions conducted in six SSA countries: South Africa (n = 5), Kenya (n = 4), Uganda (n = 4), and one each in Liberia, Malawi, and Nigeria (Table 1). Interventions targeted school-going adolescents and young people aged between 10 and 24 years. Sample sizes ranged from 522 to 6,644 participants, and more than half (n = 9) of the included interventions only targeted girls. Post-intervention follow-up ranged from 6 months to 8 years.
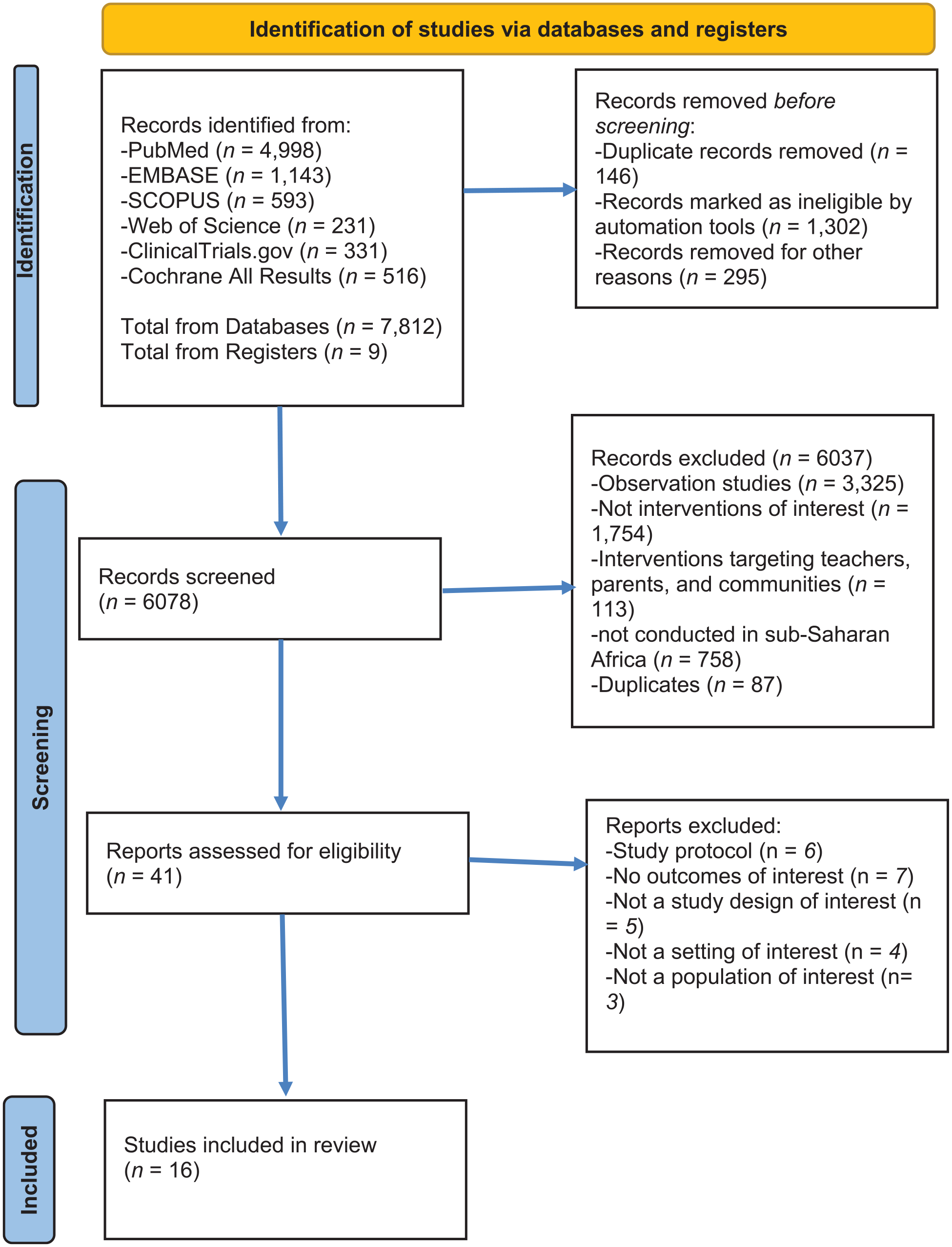
PRISMA 2020 flow diagram.
Study Quality
As shown in Figure 2, based on a modified MQRS score range of 11 to 19, the overall quality of studies included in this review ranged from moderate to high. The mean and the median modified MQRS scores of the 16 studies were 15 and 16 (SD = ±2.99), respectively (see Figure 2), reflecting moderate study quality differences. Half of the studies (n = 8) were rated as having high rigor. However, studies had several salient methodological weaknesses, such as using one outcome measure to assess intervention effectiveness (n = 6), not reporting the theoretical basis of the intervention (n = 7), and having a follow-up length <24 months (n = 10; mostly less than 12 months). A notable methodological strength of many intervention studies was the use of randomized control trials (RCTs) as the study design (n = 10)—the gold standard for measuring intervention effectiveness (Hariton & Locascio, 2018). A multi-site strategy also strengthened the external validity (generalizability; Weinberger et al., 2001) of several studies: 12 interventions were implemented in 11 or more sites. Other notable strengths were that all studies had a follow-up rate equal to or greater than the intervention phase and most reported quality control measures (n = 11).
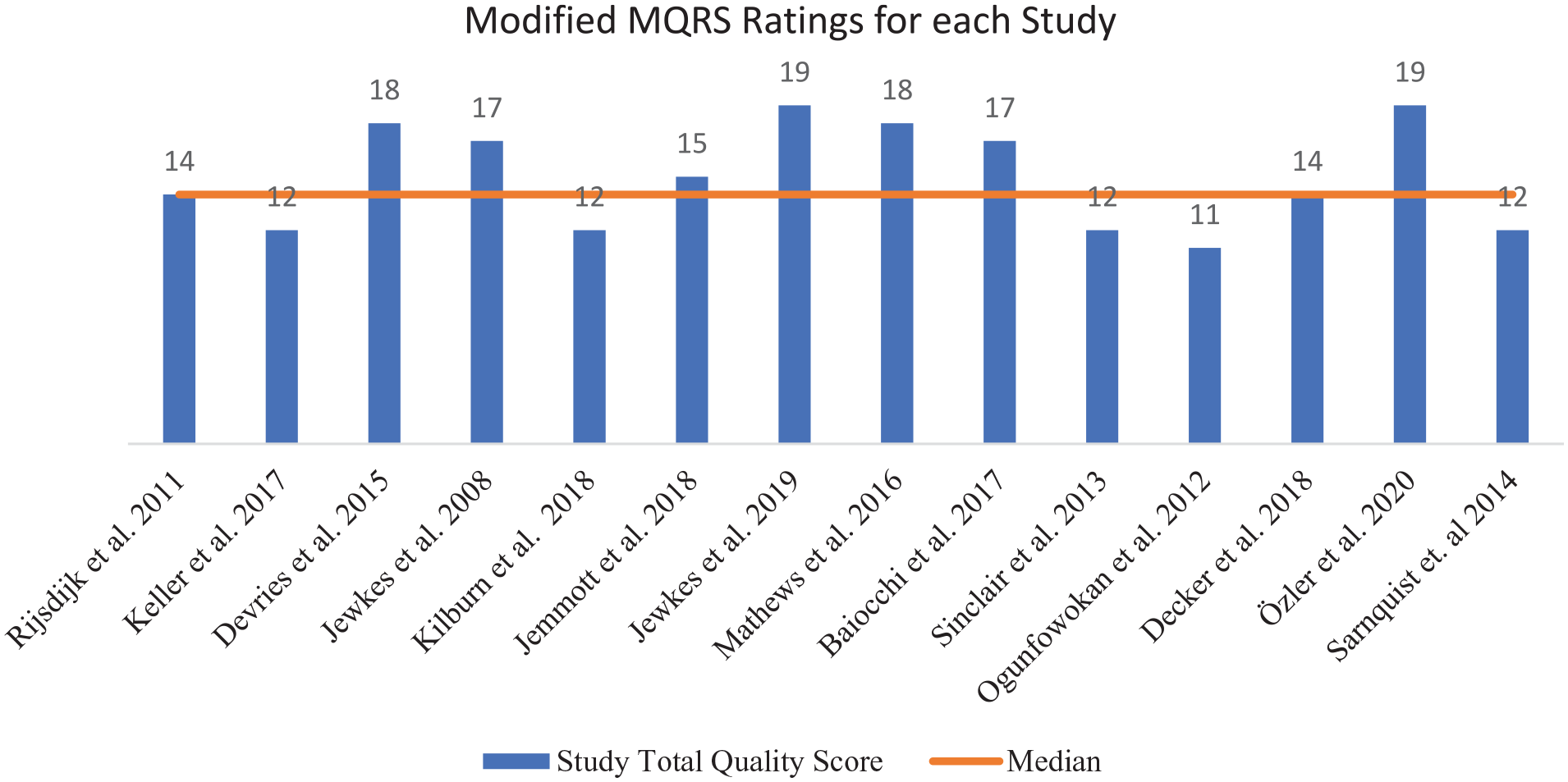
A methodological quality assessment for intervention studies.
Intervention Characteristics, Outcomes, and Effectiveness
Intervention Characteristics
As shown in Table 1, school-based GBV interventions had several components targeting girls and boys, including gender (and GBV) sensitization (n = 13), sexual reproductive health and rights (SRHR) (n = 7), safe schools (n = 4), and parenting (n = 3). However, life skills empowerment (n = 7), knowledge of where to seek help or services (n = 5), self-defense (n = 4), and economic empowerment (n = 4) components were specifically delivered to girls, while a bystander intervention was delivered to boys only (n = 1).
Intervention Outcomes and Effectiveness
As illustrated in Table 1, school-based GBV interventions addressed several GBV outcomes, including sexual and physical violence (i.e., primary outcomes) and GBV-related knowledge/attitudes (secondary outcomes). Most (81%; n = 13) of the interventions were evaluated using experiences of sexual violence, 50% (n = 8) were evaluated using experiences of physical violence, and 44% (n = 7) were evaluated using GBV-related knowledge/attitudes. Only 38% (n = 6) of the interventions were evaluated using a combination of primary and secondary outcomes (i.e., physical or sexual violence and GBV-related knowledge/attitudes). Even fewer interventions (31%; n = 5) were evaluated using both primary outcomes (i.e., physical and sexual violence). Of the 13 interventions that were evaluated for sexual violence, 76% (n = 10) were effective. Additionally, 63% (n = 5) were effective out of all the interventions that sought to reduce physical violence. Furthermore, of all the seven interventions that sought to improve GBV-related knowledge/attitudes, 71% (n = 5) were effective. Overall, 88% (n = 14) of all the interventions successfully improved at least one of the measured outcomes.
WSA Compliance Assessment
As shown in Figure 3, the WSARS assessment scores for the 16 intervention studies ranged from 2 to 12, while the mean and median scores were 6.8 and 7, respectively, reflecting moderate rating differences. More than half (56%; n = 9) of the interventions scored equal to or above the median, indicating a high rating on the WSARS, while the other 44% (n = 7) scored lower than the median, suggesting a medium to low rating. Of the two interventions that were ineffective in addressing at least one of the measured outcomes, one had a high WSA rating (12/16), and the other had a low WSA rating (2/16). Regarding specific WSA scale items, only 44% (n = 7) of the interventions targeted girls and boys; neither of the ineffective interventions among these. In addition, only 38% (n = 6) trained all or some teachers to deliver the intervention. About 56% (n = 9) engaged parents and communities via sensitization, mobilization, and feedback meetings or exhibitions. Of these nine interventions that engaged parents and community members, 77.7% (n = 7) effectively improved at least one of the measured outcomes. Regarding intervention focus, 81% (n = 13) of the interventions delivered at least two intervention components, while 44% (n = 7) delivered a comprehensive package of components, including knowledge related to GBV and assertive skills for decreasing the incidence of/protecting students from GBV/sexual assault victimization (e.g., negotiation, self-defense, and knowledge of where to seek help for GBV).
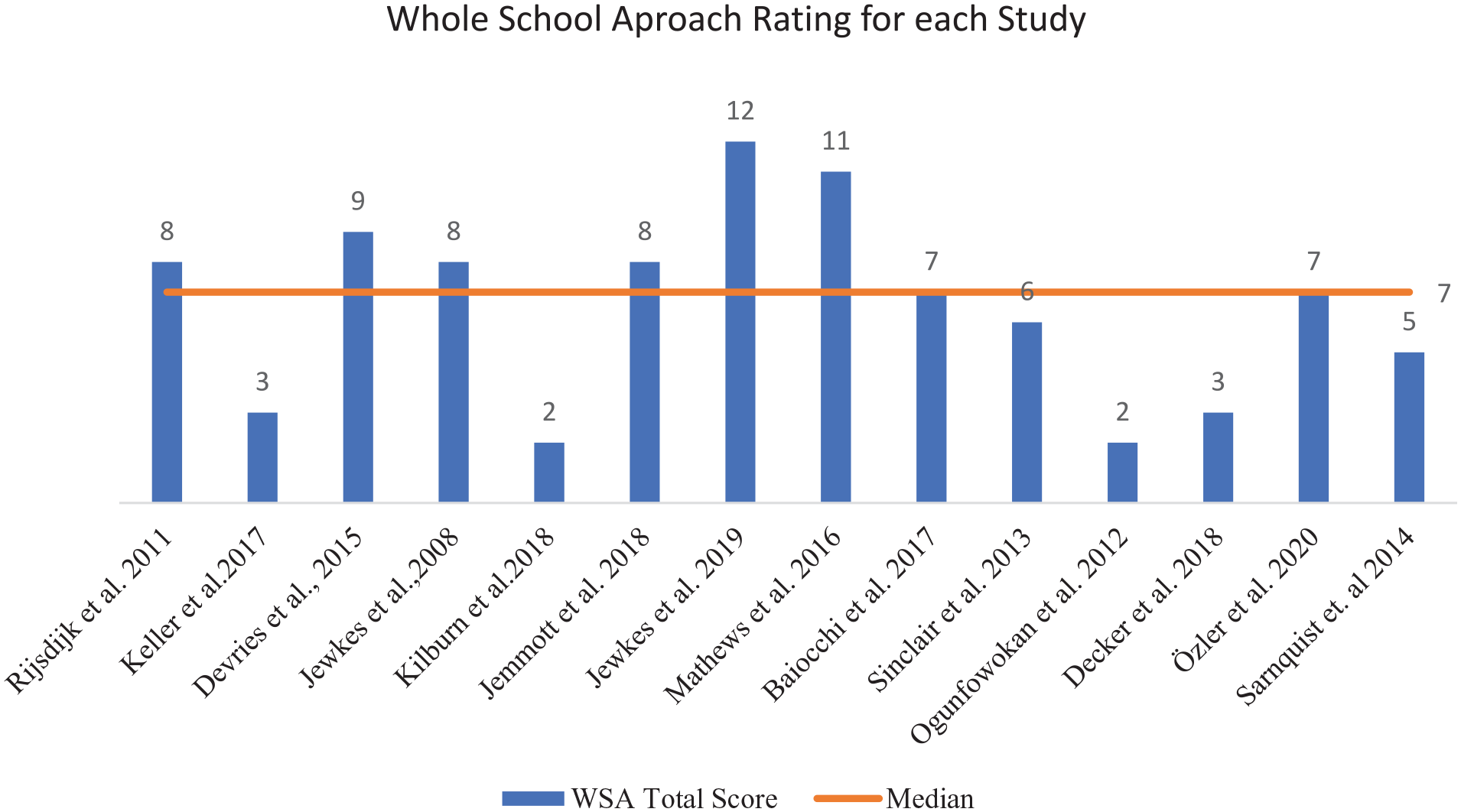
Whole school assessment for intervention studies using the WSARS.
Discussion
This systematic review synthesized and rigorously evaluated school-based GBV interventions to address four study aims. First, it examined the effectiveness of school-based GBV interventions in addressing GBV outcomes (i.e., sexual and physical violence and GBV-related knowledge/attitudes) in SSA. Notably, although targeting school settings indicates that the reviewed school-based GBV interventions sought to address GBV experienced by school-going adolescents, the data collected on prevalence and incidence of GBV did not often specifically focus on school-related GBV. Second, we evaluated the extent to which the design and implementation of these school-based GBV interventions aligned with the core tenets of WSA. Third, although our study established that the extent to which an intervention aligned with the WSA was not linked to greater effectiveness in addressing GBV, we found that most of the school-based GBV interventions engaging families (via parents) and community members were effective. Fourth, our study assessed how school-based GBV interventions targeted both boys and girls and reported GBV outcomes for both. To our knowledge, this review is the first study to address these questions. The only study that previously evaluated the effectiveness of the WSA was a meta-analysis targeting school-based interventions that sought to address the emotional skill development of adolescents on a global scale (Goldberg et al., 2018).
The authors found that most school-based GBV interventions (88%) effectively improved at least one of the three outcomes measured (i.e., sexual and physical violence and GBV-related knowledge/attitudes). This finding corroborates the results of previous global systematic reviews that found most school-based GBV interventions effectively reduce GBV and improve GBV-related knowledge and attitudes (De Koker et al., 2014; De La Rue et al., 2014). The effectiveness of most interventions in the current systematic review could be explained by the fact that intervention researchers conceptualized GBV outcomes as a product of coordinated action between curriculum, teaching, and learning, the school ethos and environment, and family and community partnerships (WHO, 1998).
Although none of the school-based GBV interventions were explicitly conceptualized based on the WSA, over half were rated high regarding their alignment with the WSA. This finding suggests that despite the encouraging results of many of the interventions, there remains a shortfall in the intentional uptake and utilization of the WSA, particularly with school-based GBV interventions. Evidence suggests that WSA is effective because it can address all forms and drivers of GBV (Futures Without Violence, n.d; Parkes et al., 2016). Thus, it is crucial to increase the adoption of WSA in such interventions because doing so ensures that the intervention design accounts for the interconnectedness of schools, communities, and families in creating a safe school environment for students, staff, and community members to help combat GBV in and around schools (UNGEI, 2018).
Notably, we found that school-based GBV interventions rated low on the WSA rating scale were just as effective as high-rated ones. This finding is consistent with results from prior reviews indicating that the full adoption of WSA in school-based social and emotional learning interventions failed to show impact (e.g., Durlak et al., 2011; Goldberg et al., 2018; Langford et al., 2015). The fact that most of the reviewed school-based GBV interventions engaged families (via parents) and community members as support systems to build awareness against harmful gender norms and to prevent or reduce GBV may explain the efficacy of those interventions that did not fully implement WSA. Engaging families and community members could be the most critical component of implementing school-based interventions, sufficient even to compensate for failing to conform to other elements of the WSA. This interpretation is consistent with findings from a meta-analysis by Goldberg et al. (2018). They found the inclusion of a community component as part of a WSA to be a significant moderator of intervention outcomes. Other empirical studies have indicated that by including family and community members, several interventions achieved a wider impact because these components helped to shift broader community attitudes on harmful gender norms (Abramsky et al., 2014; Barry et al., 2017; Jones & Bouffard, 2012; Oberle et al., 2016; Weare & Nind, 2011).
The current systematic review’s findings also reveal that while all school-based GBV interventions successfully addressed at least one assessed outcome, less than half specifically targeted both girls and boys. This is an important finding, given the dearth of knowledge about what effectively changes boys’ behavior and attitudes about GBV (Tappis et al., 2016). For instance, a 2016 integrative review of the effectiveness of interventions, programs, and strategies for GBV prevention among refugee populations found that none focused on engaging refugee men and boys (Tappis et al., 2016). Furthermore, a 2019 meta-analysis assessing the effectiveness of interventions designed to reduce GBV among young people living with or affected by HIV/AIDS in low-income and middle-income countries also concluded that limited knowledge was available about what works to change boys’ behavior and attitudes (Meinck et al., 2019). In our review, only one bystander intervention was delivered to boys only in the informal settlements of Nairobi, Kenya (Keller et al., 2017). In addition to bystander intervention skills, our findings also indicate that other interventions’ components that could work for boys include gender (and GBV) sensitization, SRHR education, and safe schools education (Jewkes et al., 2008; Jewkes et al., 2019; Rijsdijk et al. 2011). This finding also highlights the need for school-based GBV interventions to include boys in ways that still protect safe spaces for girls, especially given that harmful gender norms that drive GBV are hard to change without having all people who adhere to and act according to these norms (Tappis et al., 2016). The rationale for engaging men and boys in violence prevention is that to end violence against women and girls, interventions must also address the high levels of acceptability of IPV among men and boys as well as their greater likelihood of perpetrating such violence (Darteh et al., 2021).
Limitations
Using our modified MQRS, we found that half of the studies (n = 8) were of medium to low quality in terms of methodological rigor. Many interventions had low scores on some components considered essential to credible, evidence-based policy and practice. For instance, 62% (n = 10) of all interventions had a post-intervention follow-up period of few than 24 months. This short period may not be enough to assess the interventions’ effectiveness. Behavioral interventions, in particular, can take time to yield their full effect because they may hinge on changing attitudes and norms at the community level (Hayes et al., 2010).
Conversely, if impacts fade with time, the short follow-up period will not capture these multilevel changes. Researchers who conducted a prior systematic review and meta-analysis found that the effective interventions had a longer duration of follow-up, indicating the importance of the longer follow-up period for an accurate assessment of effectiveness (De Koker et al., 2014). Also, half of the interventions studied (n = 8) only used one outcome measure to assess intervention effectiveness, thereby necessarily failing to determine the co-occurrence of multiple victimization experiences (polyvictimization), which are common among adolescents and young people (Finkelhor et al., 2007; Logie et al., 2019; Okumu et al., 2022), and in turn missing the opportunity to target and mitigate these harms (Cid, 2017). Almost half of the studies did not report the theoretical basis of the intervention, making it challenging for researchers to test, validate, and improve existing behavior change theoretical frameworks (Sales et al., 2006). A final limitation was that our inclusion of study findings published in English only excluded studies conducted in French, Portuguese, and Spanish, even though such studies of school-based GBV interventions in SSA may exist.
Strengths
To the best of our knowledge, this is the first systematic review that assesses the effectiveness of school-based GBV interventions, their compliance with WSA, and the quality of their evidence in SSA, a region with high levels of GBV against school-going adolescents (WHO, 2021). Additionally, the quality of evidence reported in this review is substantial, given many included studies’ use of RCTs as their study design—the gold standard for measuring intervention effectiveness (Hariton & Locascio, 2018)—and their testing of interventions at multiple sites, which strengthens the external validity by increasing the generalizability of their findings (Weinberger et al., 2001). Moreover, by focusing on the SSA subregion, the present study sheds new light on multiple violence outcomes experienced by adolescents and young people in the region. Finally, these findings highlight the need for school-based engagement of students, families, and communities to mitigate GBV and improve the lives of youth and their future.
Implications for Research and Practice
Future research might augment the findings of this systematic review through a meta-analysis to establish the precise statistical effectiveness of school-based GBV interventions. Such an analysis could test the moderating effect of the WSA, as well as the impact of engaging families and communities in school-based GBV interventions. The current study treated the school-based GBV interventions—including gender (and GBV) sensitization, SRHR, life skills empowerment, self-defense for girls, knowledge of where to seek help or services, parenting, economic empowerment, and bystander intervention training—as a package or multi-component interventions without disambiguating the effects of the different components they included. Therefore, there is a need for more rigorous testing using the multiphase optimization strategy to assess the performance of individual intervention components and their interactions. Such analyses would enhance knowledge of which specific components contribute most to efficacy, informing the development of highly efficacious, efficient, scalable, and cost-effective interventions to reduce GBV.
Additionally, all school-based GBV programs must target both girls and boys and report outcomes for both to maximize the effectiveness of interventions in changing gender norms and reducing GBV. Future studies should also rigorously evaluate school-based GBV interventions with more extended follow-up periods to establish these interventions’ sustained effects and inform further investments in programming. Finally, researchers and practitioners need to pursue greater compliance with WSA tenets in designing and implementing school-based GBV interventions, with a specific focus on engaging parents, families, and communities to improve intervention effectiveness and to help shift gender norms to prevent and reduce GBV.
Conclusion
School-based GBV interventions that target both boys and girls and engage parents and communities may reduce GBV exposure among adolescent girls and adherence to harmful gender norms by both girls and boys. More research is needed to strengthen the evidence quality and rigorously test the effectiveness of including boys, parents, and communities in school-based GBV interventions. Finally, greater WSA principles—especially for families and communities—in school-based GBV intervention could increase the effectiveness and sustainability of programs’ impacts.
Footnotes
Appendix
A Whole School Approach Rating Scale (WSARS).
| Criteria | Points | Rating Criteria | |
|---|---|---|---|
| A | Targeted Girls and Boys | 1 | Targeted and reported outcomes for boys and girls |
| 2 | Targeted boys and girls but reported outcomes only for one gender | ||
| 3 | Only targeted and reported outcomes for one gender | ||
| B | Intervention Focus | 3 | Provided knowledge related to GBV, assertive skills decreasing/Protecting students from GBV/SA victimization (e.g., negotiation, self-defense, and knowledge of where to seek help) |
| 2 | Provided knowledge change related to GBV AND training on assertive decreasing/protecting students from GBV/SA victimization (e.g., negotiation, self-defense, OR knowledge of where to seek help) | ||
| 1 | Provided knowledge change related to GBV OR assertive skills | ||
| C | Engaged Teachers | 3 | Trained all teachers to deliver the intervention |
| 2 | Trained some teachers to deliver the intervention | ||
| 1 | Informed teachers about intervention via meetings | ||
| 0 | Teachers are neither trained nor informed | ||
| D | Engaged Parents | 3 | Parents are trained on GBV and positive parenting |
| 2 | Parents are trained on GBV | ||
| 1 | Parents are informed about training via meetings | ||
| 0 | Parents are neither trained nor informed | ||
| E | Engaged Community | 2 | Involved community members as facilitators of the intervention |
| 1 | Community informed/sensitized via meetings and report backs | ||
| 0 | Community not involved/sensitized | ||
Note. This assessment criterion was developed based on the minimum standards and monitoring framework of the WSA to prevent school-related GBV. GBV = gender-based violence; SA = Saharan Africa.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.